Forensic Toxicology Analytical Toxicology Fall 2007 Analytical Toxicology Fall 2007.
Upload
gomathi-gomuCategory
view
458download
2description

TOXICOLOGY
GOMATHI’S

TOXICOLOGY – STUDY OF POISONS(GREEK WORDS)
TOXICAN – POISON LOGOS – STUDY
?

IRRITANT
BIOHAZARD
RADIOACTIVE HAZARDS


அளவுக்குமி�ஞ்சினா�ல்அமி�ர்தமும்………நஞ்சு ..
“All substances are poisons; there is none which is not a poison. The right dose differentiate a poison and a remedy”
- Paracelsus (Grand Father of Toxicology)

INTRODUCTION
Toxic – the chemical/physical agent/substances having the characteristic of producing an undesirable or adverse health effects.
Toxicity – the ability of a toxic to cause adverse effects in living organisms.

DEFINITION - TOXICOLOGY The science that deals with the study of
the adverse effects chemicals/physical agents may produce in living organisms under specific conditions of exposure.
It is the science that attempts to qualitatively identify all the hazard as well as to quantitatively determine the exposure conditions.

“The science that experimentally investigates the occurrence, nature, incidence, mechanism and risk factors for the adverse effects of toxic
substances.”

HISTORY The knowledge of poison substance
(venom & plant extracts) –ancient periods – hunting.
Poisons such as Hemlock (blood of Socrates)

4,000 BC – Opium poppy – alkaloids such as morphine, codeine, Laudanum are all narcotics.
Morphine the very first medicinal compound ever isolated in pure form.

In 9th century Dioscorides, a Greek physician – classified poison
1. Plant poisons2. Animal poisons3. Mineral poisons

Paracelsus (1493) - contributed greatly to the fields of medicine and toxicology - the use of chemicals and minerals in medicine, (First Coined “Zinc”)
Certain illnesses of the body had chemical remedies that could cure them.
He was, therefore, a precursor to modern-day medicine and to the use of vitamins and minerals to maintain health.

Mathieu Orfila - Modern father of toxicology
First formal treatment – experimental toxicology laid down great success to pharmacology in 1813.
In 1815 Magendia - done atopsy & chemical toxicants and explain the mechanism of action of emitine & strychine – absorption, distribution of the compounds.

1850’s- advent of anesthetics & disinfectants began to understand.
During 1900, discovery of radioactivity & vitamins.
NIH- National Institute of Health assigned NIDA – National Institute of Drug Abuse.
FDA ASSIGNED U.S PESTICIDE ACT – 1947 1950’S additives of food, drugs, cosmetics
Act passed. Many toxicological journals, professional,
governmental & other scientific organizations begins to broadcast representation to toxicology as well as applied pharmacology.

TOXICOLOGIST
Identify the toxic materials Mechanism of toxins Exposure assessment Experimentally prove the toxicants Risk characterization Safety measures
IMPLEMENTATION / AWARENESS
RESEARCH

TOXICITY DEPENDS UPON,
PHYSICAL FORMS
DOSE
EXPOSUREROUTES OF
ENTRY

MEASURES OF TOXICITY
Toxicity is measured as clinical “endpoints” which include Mortality (death) Teratogenicity (ability to cause birth
defects) Carcinogenicity (ability to cause
cancer) Mutagenicity (ability to cause
heritable change in the DNA)

Toxic dose low (TDLO): The lowest dose of a substance introduced by any route, other than inhalation, over any given period of time, and reported to produce any toxic effect in humans or to produce tumorigenic or reproductive effects in animals.
Toxic concentration low (TCLO): The lowest concentration of a substance in air to which humans or animals have been exposed for any given period of time that has produced any toxic effect in humans or produced tumorigenic or reproductive effects in animals.
Lethal dose low (LDLO): The lowest dose, other than LD50 of a substance introduced by any route, other than inhalation, which has been reported to have caused death in humans or animals.
Lethal dose fifty (LD50): A calculated dose of a substance which is expected to cause the death of 50 percent of an entire defined experimental animal population. It is determined from the exposure to the substance by any route other than inhalation.
Lethal concentration low (LCLO): The lowest concentration of a substance in air, other than LC50, which has been reported to cause death in humans or animals.
Lethal concentration fifty (LC50): A calculated concentration of a substance in air, exposure to which for a specified length of time is expected to cause the death of 50 percent of an entire defined experimental animal population.

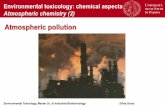
ROUTES OF ENTRY
ABSORPTION
INHALATION
DERMAL CONTACT
INGESTION
INJECTION

Example: The cyanide ion (CN−) blocks cellular respiration by inhibiting an enzyme in the mitochondria called cytochrome c oxidase.
MECHANISM OF TOXICANTS
Allergic response or
Hypersensitivity
Organ directed toxicity
MutagenesisCarcinogenesisTeratogenesis
Biological pathways changes,
Receptors, Ion channel, Enzyme mediated
toxicity

R

INGESTION INHALATION
DERMAL CONTACT
ABSORPTION
Gastrointestinal tract
FAECES
LUNGS
BILE
LIVER
BLOOD & LYMPH
KIDNEY LUNGS
BLADDER
URINE EXPIRED AIR
EXTRACELLULAR FLUIDS
FATSORGANS OF BODY
SOFT TISSUES OR BONES
SECRETION OF
GLANDS
SECRETION
METABOLISM
DIS
TR
IBU
TI
ON
EXCRETION


ABSORPTION
Passive diffusion - Diffusion occurs through the lipid membrane.
Filtration - Diffusion occurs through aqueous pores. Special transport - Transport is aided by a carrier
molecule. Endocytosis - Transport takes the form of
pinocytosis for liquids and phagocytosis for solids.

Large surface are for absorption of toxicants in small intestine.
Lipophilic toxicants highly absorbed than hydrophilic substances

LUNGS – ALVEOLAR ABSORPTION

EXAMPLES OF RESPIRATORY TRACT TOXICANTS

SKIN Absorbs
lipophilic compounds of low molecular weight very quickly and also hydrophilic substances.

KINETICS OF ABSORPTION
Rate of absorption of toxic depends upon the nature of chemicals and their site of administration.
Rate of absorption more for lipid – soluble molecules and slow for strong acids and bases.
First order process: at low doses, rate of reaction is directly proportional to the amount of toxicant present.
Zero order process: as the concentration of substances increase, a point may be reached at which there is no further increase in rate of absorption.
Extent of absorption depends on the bioavailability of the substance.

INGESTION INHALATION
DERMAL CONTACT
ABSORPTION
Gastrointestinal tract
FAECES
LUNGS
BILE
LIVER
BLOOD & LYMPH
KIDNEY LUNGS
BLADDER
URINE EXPIRED AIR
EXTRACELLULAR FLUIDS
FATSORGANS OF BODY
SOFT TISSUES OR BONES
SECRETION OF
GLANDS
SECRETION
METABOLISM
DIS
TR
IBU
TI
ON
EXCRETION

DISTRIBUTION
Rate of distribution is rapid in plasma but slow in tissues.
Extent of distribution related to apparent volume of distribution (V).
V = AbC
Ab – total quantity of toxicants in the body C – plasma concentration Volume of distribution actual space in which
toxicants distributed. Vd = D (dose administered)
Cp

INGESTION INHALATION
DERMAL CONTACT
ABSORPTION
Gastrointestinal tract
FAECES
LUNGS
BILE
LIVER
BLOOD & LYMPH
KIDNEY LUNGS
BLADDER
URINE EXPIRED AIR
EXTRACELLULAR FLUIDS
FATSORGANS OF BODY
SOFT TISSUES OR BONES
SECRETION OF
GLANDS
SECRETION
METABOLISM
DIS
TR
IBU
TI
ON
EXCRETION

EXCRETION
Rate of excretion is determined by apparent volume of distribution (V) and clearance (CL).
Rate of elimination of chemicals CL = Plasma concentration Plasma clearance = sum of the
clearance of metabolism (CLM), renal excretion (CLR), biliary excretion (CLB).
Metabolic clearance cannot measured easily so the total clearance(CL) = CLM +
CLR CLM = CL - CLR

WHY WE NEED TO STUDY TOXICOLOGY


NOT FOR………….




THANK
YOU……