Toxic Epidermal Necrolysis by Ceftriaxone in Patient with Newly … · 2014-02-04 · Toxic...
4
Journal of Rheumatic Diseases Vol. 20, No. 6, December, 2013 http://dx.doi.org/10.4078/jrd.2013.20.6.374 □ Case Report □ 374 <Received:September 26, 2012, Revised (1st: December 21, 2012, 2nd: January 10, 2013), Accepted:January 10, 2013> Corresponding Yeon-Sik Hong, Division of Rheumatology, Department of Internal Medicine, School of Medicine, The Catholic University of Korea, Incheon St. Mary’s Hospital, 56, Dongsuro, Bupyeong-gu, Incheon 403-720, Korea. E-mail: [email protected] pISSN: 2093-940X, eISSN: 2233-4718 Copyright ⓒ 2013 by The Korean College of Rheumatology This is a Free Access article, which permits unrestricted non-commerical use, distribution, and reproduction in any medium, provided the original work is properly cited. Toxic Epidermal Necrolysis by Ceftriaxone in Patient with Newly Diagnosed Systemic Lupus Erythematosus Jae Ho Lee, Il Nam Ju, Hyung Jun Cho, Hong Ki Min, Yeon-Sik Hong Division of Rheumatology, Department of Internal Medicine, School of Medicine, The Catholic University of Korea, Incheon, Korea Toxic epidermal necrolysis (TEN) is a rare disease in abso- lute numbers with an incidence of 2 cases per million peo- ple per year. Most cases of TEN are caused by drugs, but certain infectious diseases may have an impact on the risk. There are rare reports of TEN occurring without history of drug ingestion in systemic lupus erythematosus (SLE), appearing similar to cutaneous lupus and early TEN mani- festations, such as erythema multiforme. This report de- scribes a patient with SLE who presented with manifes- tations of TEN after ceftriaxone treatment. The patient was newly diagnosed with SLE and TEN occurring eight days after cessation of ceftriaxone. Considering possible etiol- ogies, we could not exclude ceftriaxone as the cause of TEN. After intravenous immunoglobulin with glucocorti- coid, clinical symptoms improved. Key Words. Systemic lupus erythematosus, Toxic epi- dermal necrolysis, Ceftriaxone, Hydroxychloroquine, IV immunoglobulin Introduction Toxic epidermal necrolysis (TEN) is an acute, rapidly evolv- ing mucocutaneous reaction, frequently associated with medi- cation use characterized by extensive painful cutaneous and mucosal exfoliation, and systemic involvement that may be life-threatening (1). Common triggers of TEN are anti- epileptic drugs such as carbamazepine. Also, allopurinol is the most common cause of Stevens- Johnson syndrome (SJS)/TEN in Europe and Israel (2). However, several drugs except the following drugs can be a cause of TEN (3). One of them is cephalosporin, such as ceftriaxone. Moreover, SLE can present as SJS and TEN, too (4-6). The mortality of TEN approximates 30%. Therefore, differential diagnosis about the cause of TEN is important in SLE patients. We experienced a case presenting TEN in a new diagnosed SLE patient after ceftriaxone administration. Case Report A 37 year-old female patient who had facial rash, febrile sense for 2 weeks was admitted to the emergency room. The patient was treated by local dermatologic clinic regarding fa- cial rash using steroid ointment. There was no facial rash im- provement; therefore, laboratory tests were checked. She was transferred to our hospital because the test showed elevated liv- er enzymes. At that time, blood pressure was within normal limit, but the pulse rate 119 bpm and body temperature 38.1 o C were increased. In past history, it was non-specific except herbal medication for 4 days before 2 weeks. Nothing unusual was found in familial history. Oral ulcer and mild abdominal tenderness without rebound tenderness were observed. Complete blood count showed decreased white blood cell (WBC) 1,560/mm 3 (absolute neutrophil count (ANC) 790), he- moglobin 10.4 g/dL and platelet count 113 K, pancytopenia. It was showed an increased aspartate transaminase/alanine transaminase (AST/ALT) 457/238 (0∼40) U/L, γ-GTP 44 (0
Transcript of Toxic Epidermal Necrolysis by Ceftriaxone in Patient with Newly … · 2014-02-04 · Toxic...

J o u r n a l o f R h e u m a t i c D i s e a s e sV o l . 2 0 , N o . 6 , D e c e m b e r , 2 0 1 3http://dx.do i.org/10.4078/jrd .2013.20.6 .374
□ Case Report □
374
<Received:September 26, 2012, Revised (1st: December 21, 2012, 2nd: January 10, 2013), Accepted:January 10, 2013>Corresponding Yeon-Sik Hong, Division of Rheumatology, Department of Internal Medicine, School of Medicine, The Catholic
University of Korea, Incheon St. Mary’s Hospital, 56, Dongsuro, Bupyeong-gu, Incheon 403-720, Korea. E-mail:[email protected]
pISSN: 2093-940X, eISSN: 2233-4718Copyright ⓒ 2013 by The Korean College of RheumatologyThis is a Free Access article, which permits unrestricted non-commerical use, distribution, and reproduction in any medium, provided the original work is properly cited.
Toxic Epidermal Necrolysis by Ceftriaxone in Patient with Newly Diagnosed Systemic Lupus Erythematosus
Jae Ho Lee, Il Nam Ju, Hyung Jun Cho, Hong Ki Min, Yeon-Sik Hong
Division of Rheumatology, Department of Internal Medicine, School of Medicine, The Catholic University of Korea, Incheon, Korea
Toxic epidermal necrolysis (TEN) is a rare disease in abso-
lute numbers with an incidence of 2 cases per million peo-
ple per year. Most cases of TEN are caused by drugs, but
certain infectious diseases may have an impact on the risk.
There are rare reports of TEN occurring without history
of drug ingestion in systemic lupus erythematosus (SLE),
appearing similar to cutaneous lupus and early TEN mani-
festations, such as erythema multiforme. This report de-
scribes a patient with SLE who presented with manifes-
tations of TEN after ceftriaxone treatment. The patient was
newly diagnosed with SLE and TEN occurring eight days
after cessation of ceftriaxone. Considering possible etiol-
ogies, we could not exclude ceftriaxone as the cause of
TEN. After intravenous immunoglobulin with glucocorti-
coid, clinical symptoms improved.
Key Words. Systemic lupus erythematosus, Toxic epi-
dermal necrolysis, Ceftriaxone, Hydroxychloroquine, IV
immunoglobulin
Introduction
Toxic epidermal necrolysis (TEN) is an acute, rapidly evolv-
ing mucocutaneous reaction, frequently associated with medi-
cation use characterized by extensive painful cutaneous and
mucosal exfoliation, and systemic involvement that may be
life-threatening (1). Common triggers of TEN are anti-
epileptic drugs such as carbamazepine. Also, allopurinol is
the most common cause of Stevens- Johnson syndrome
(SJS)/TEN in Europe and Israel (2). However, several drugs
except the following drugs can be a cause of TEN (3). One
of them is cephalosporin, such as ceftriaxone. Moreover, SLE
can present as SJS and TEN, too (4-6). The mortality of TEN
approximates 30%. Therefore, differential diagnosis about the
cause of TEN is important in SLE patients. We experienced
a case presenting TEN in a new diagnosed SLE patient after
ceftriaxone administration.
Case Report
A 37 year-old female patient who had facial rash, febrile
sense for 2 weeks was admitted to the emergency room. The
patient was treated by local dermatologic clinic regarding fa-
cial rash using steroid ointment. There was no facial rash im-
provement; therefore, laboratory tests were checked. She was
transferred to our hospital because the test showed elevated liv-
er enzymes. At that time, blood pressure was within normal
limit, but the pulse rate 119 bpm and body temperature 38.1oC
were increased. In past history, it was non-specific except
herbal medication for 4 days before 2 weeks. Nothing unusual
was found in familial history. Oral ulcer and mild abdominal
tenderness without rebound tenderness were observed.
Complete blood count showed decreased white blood cell
(WBC) 1,560/mm3 (absolute neutrophil count (ANC) 790), he-
moglobin 10.4 g/dL and platelet count 113 K, pancytopenia.
It was showed an increased aspartate transaminase/alanine
transaminase (AST/ALT) 457/238 (0∼40) U/L, γ-GTP 44 (0

Toxic Epidermal Necrolysis in a Systemic Lupus Erythematosus Patient 375
Figure 1. It shows blistered skin
lesions in back (A) and upper
abdomen (B).
Figure 2. It shows skin detach-
ment and new epidermis regenera-
tion. Skin detachment start in back
at hospital day 22 (A). Around
hospital day 30, almost skin de-
tachment is over and new epide-
rmis go into new regeneration (B).
∼38) U/L, and LDH 1,607 (208∼450) IU/L in blood chem-
istry, but otherwise within normal limit, including urine
analysis. The patient was hospitalized in the division of hep-
atology for evaluation and treatment about hepatitis. Empirical
ceftriaxone was started considering infectious fever, and raniti-
dine, ornithine oxoglurate, and oral prednisolone 10 mg were
administered in the light of autoimmune diseases. However,
AST/ALT was on the increase continuously. The results of
hepatitis viral examination (HAV, HBV, HCV, EBV, and
CMV) and autoimmune hepatitis (anti-liver kidney microsomal
antibody, anti-smooth muscle antibody, anti-mitochondrial anti-
body) were all negative. In immunologic test, rheumatoid fac-
tor was negative, but anti-nuclear antibody 1:640 homoge-
neous, anti SS-A antibody was positive and anti-dsDNA anti-
body was over 600 IU/mL. Complements were both decreased:
C3 was 20.3 (90∼180 mg/dL) and C4 12.2 (14∼50 mg/dL).
At hospital day 7, ceftriaxone was stopped since fever is not
infectious origin. Liver biopsy showed focal macrovesicular
steatosis with intralobular degeneration and focal necrosis.
Moreover, Masson-Trichrome stain was positive in collagen
tissue of the portal tract and reticulin was positive in reticulin
framework, too. The result of liver biopsy may be present in
SLE. She was diagnosed SLE based on clinical symptoms and
laboratory test, and transferred to the division of rheumatology
on hospital day 12. At that time of transfer, ANC was de-
creased to 330/mm3, therefore an increase of prednisolone dos-
age of up to 50 mg was decided. Three days later, although
reduction of AST/ALT was not significant, ANC was elevated
to 3,330/mm3. A dose of 400 mg of hydroxychloroquine
(HCQ) was prescribed. Confluent erythematous plaques with
target lesions developed on the whole abdomen and back with
itching sense on the same evening. The rash extended to the
extremities, face and neck over 4 days, and then multiple blis-
ters arose on the patient’s abdomen and back (Figure 1). This
376 Jae Ho Lee et al.
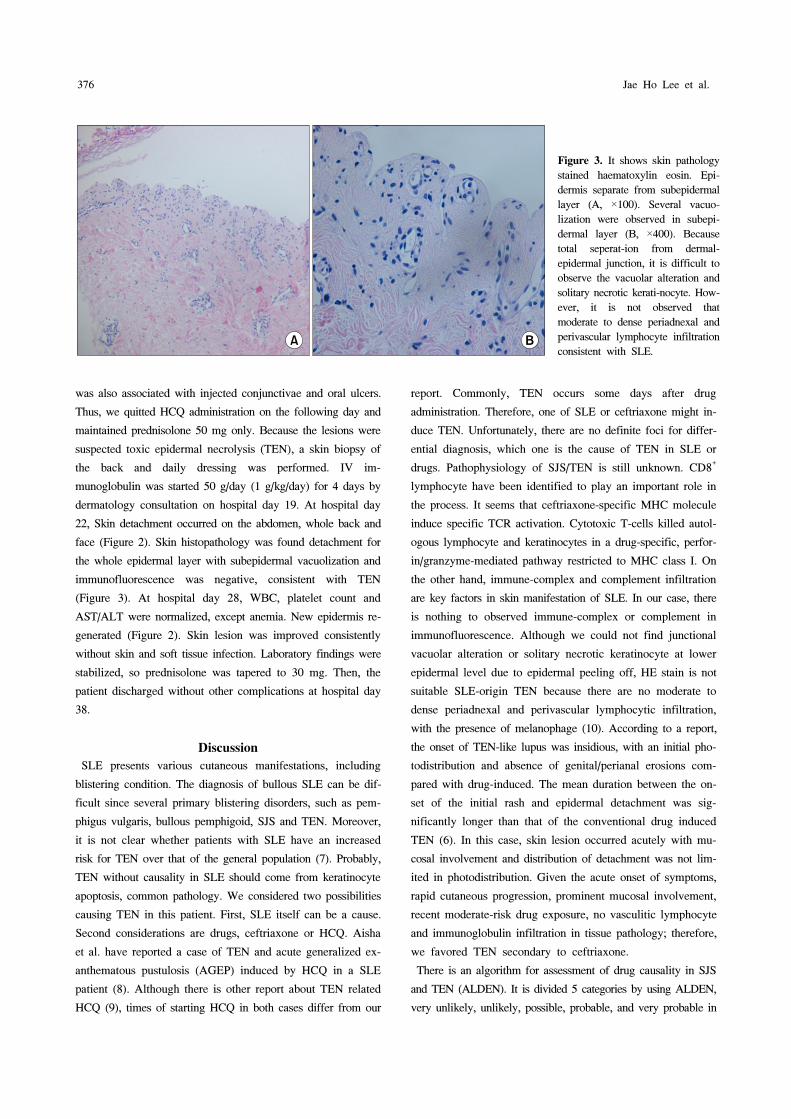
Figure 3. It shows skin pathology
stained haematoxylin eosin. Epi-
dermis separate from subepidermal
layer (A, ×100). Several vacuo-
lization were observed in subepi-
dermal layer (B, ×400). Because
total seperat-ion from dermal-
epidermal junction, it is difficult to
observe the vacuolar alteration and
solitary necrotic kerati-nocyte. How-
ever, it is not observed that
moderate to dense periadnexal and
perivascular lymphocyte infiltration
consistent with SLE.
was also associated with injected conjunctivae and oral ulcers.
Thus, we quitted HCQ administration on the following day and
maintained prednisolone 50 mg only. Because the lesions were
suspected toxic epidermal necrolysis (TEN), a skin biopsy of
the back and daily dressing was performed. IV im-
munoglobulin was started 50 g/day (1 g/kg/day) for 4 days by
dermatology consultation on hospital day 19. At hospital day
22, Skin detachment occurred on the abdomen, whole back and
face (Figure 2). Skin histopathology was found detachment for
the whole epidermal layer with subepidermal vacuolization and
immunofluorescence was negative, consistent with TEN
(Figure 3). At hospital day 28, WBC, platelet count and
AST/ALT were normalized, except anemia. New epidermis re-
generated (Figure 2). Skin lesion was improved consistently
without skin and soft tissue infection. Laboratory findings were
stabilized, so prednisolone was tapered to 30 mg. Then, the
patient discharged without other complications at hospital day
38.
Discussion
SLE presents various cutaneous manifestations, including
blistering condition. The diagnosis of bullous SLE can be dif-
ficult since several primary blistering disorders, such as pem-
phigus vulgaris, bullous pemphigoid, SJS and TEN. Moreover,
it is not clear whether patients with SLE have an increased
risk for TEN over that of the general population (7). Probably,
TEN without causality in SLE should come from keratinocyte
apoptosis, common pathology. We considered two possibilities
causing TEN in this patient. First, SLE itself can be a cause.
Second considerations are drugs, ceftriaxone or HCQ. Aisha
et al. have reported a case of TEN and acute generalized ex-
anthematous pustulosis (AGEP) induced by HCQ in a SLE
patient (8). Although there is other report about TEN related
HCQ (9), times of starting HCQ in both cases differ from our
report. Commonly, TEN occurs some days after drug
administration. Therefore, one of SLE or ceftriaxone might in-
duce TEN. Unfortunately, there are no definite foci for differ-
ential diagnosis, which one is the cause of TEN in SLE or
drugs. Pathophysiology of SJS/TEN is still unknown. CD8+
lymphocyte have been identified to play an important role in
the process. It seems that ceftriaxone-specific MHC molecule
induce specific TCR activation. Cytotoxic T-cells killed autol-
ogous lymphocyte and keratinocytes in a drug-specific, perfor-
in/granzyme-mediated pathway restricted to MHC class I. On
the other hand, immune-complex and complement infiltration
are key factors in skin manifestation of SLE. In our case, there
is nothing to observed immune-complex or complement in
immunofluorescence. Although we could not find junctional
vacuolar alteration or solitary necrotic keratinocyte at lower
epidermal level due to epidermal peeling off, HE stain is not
suitable SLE-origin TEN because there are no moderate to
dense periadnexal and perivascular lymphocytic infiltration,
with the presence of melanophage (10). According to a report,
the onset of TEN-like lupus was insidious, with an initial pho-
todistribution and absence of genital/perianal erosions com-
pared with drug-induced. The mean duration between the on-
set of the initial rash and epidermal detachment was sig-
nificantly longer than that of the conventional drug induced
TEN (6). In this case, skin lesion occurred acutely with mu-
cosal involvement and distribution of detachment was not lim-
ited in photodistribution. Given the acute onset of symptoms,
rapid cutaneous progression, prominent mucosal involvement,
recent moderate-risk drug exposure, no vasculitic lymphocyte
and immunoglobulin infiltration in tissue pathology; therefore,
we favored TEN secondary to ceftriaxone.
There is an algorithm for assessment of drug causality in SJS
and TEN (ALDEN). It is divided 5 categories by using ALDEN,
very unlikely, unlikely, possible, probable, and very probable in

Toxic Epidermal Necrolysis in a Systemic Lupus Erythematosus Patient 377
turn. Data from the report showed lower etiologic fraction of
cephalosporin related epidermal necrolysis, 4.3% (11).
TEN remains a potentially fatal disorder. The typically quot-
ed mortality rate of 20% and 30% was confirmed (12).
Established therapies are controversial up to now, and treat-
ments are not different regardless of the etiology. In aspect
of the topical treatment, appropriately placed wet dressing
may help to avoid adhesion or stricture and infection via skin
or mucosa. Also, supportive care in intensive unit is im-
portant, such as maintain room temperature, avoiding dehy-
dration and electrolyte imbalance. In addition, various im-
munomodulating therapies are discussed for SJS/TEN, includ-
ing IVIG. It is unclear IVIG mechanism to improve SJS/TEN
survival. Antibodies in pooled human IVIG block in vitro
FAS-mediated keratinocyte necrosis, which is why IVIG is
used in the treatment of SJS and TEN (13). Nothing has been
decided yet regarding proper dosage of IVIG. The dose has
varied from one author to the next (1). There have been argu-
ments against systemic glucocorticoid treatment due to in-
creased mortality related infection (13,14). On the other hand,
some reports have shown effects of steroid pulse therapy, pre-
venting ocular complication or not increased mortality (15).
We administered prednisolone 1 mg/kg to control SLE activity
not TEN. IVIG was prescribed by 50 g/day (1 g/kg/day). We
considered ethnic distinctions to decide the dose. Otherwise,
there are many immunomodulators to treat TEN, TNF antago-
nist, thalidomide, cyclophophamide, cyclosporine A, and etc.
Summary
Our patient recovered rapidly after IVIG treatment. We are
following her for 6 months, and she takes HCQ before several
months without adverse effects.
References
1. Harr T, French LE. Toxic epidermal necrolysis and
Stevens-Johnson syndrome. Orphanet J Rare Dis 2010;5:
39.
2. Halevy S, Ghislain PD, Mockenhaupt M, Fagot JP,
Bouwes Bavinck JN, Sidoroff A, et al; EuroSCAR Study
Group. Allopurinol is the most common cause of
Stevens-Johnson syndrome and toxic epidermal necrolysis
in Europe and Israel. J Am Acad Dermatol 2008;58:
25-32.
3. Heymann WR. Toxic epidermal necrolysis 2006. J Am
Acad Dermatol 2006;55:867-9.
4. Mandelcorn R, Shear NH. Lupus-associated toxic epi-
dermal necrolysis: a novel manifestation of lupus? J Am
Acad Dermatol 2003;48:525-9.
5. Obermoser G, Sontheimer RD, Zelger B. Overview of
common, rare and atypical manifestations of cutaneous
lupus erythematosus and histopathological correlates.
Lupus 2010;19:1050-70.
6. Lee HY, Tey HL, Pang SM, Thirumoorthy T. Systemic
lupus erythematosus presenting as Stevens-Johnson syn-
drome and toxic epidermal necrolysis: a report of three
cases. Lupus 2011;20:647-52.
7. Horne NS, Narayan AR, Young RM, Frieri M. Toxic epi-
dermal necrolysis in systemic lupus erythematosus.
Autoimmun Rev 2006;5:160-4.
8. Lateef A, Tan KB, Lau TC. Acute generalized ex-
anthematous pustulosis and toxic epidermal necrolysis in-
duced by hydroxychloroquine. Clin Rheumatol 2009;28:
1449-52.
9. Callaly EL, FitzGerald O, Rogers S. Hydroxychloroquine-
associated, photo-induced toxic epidermal necrolysis. Clin
Exp Dermatol 2008;33:572-4.
10. Ziemer M, Kardaun SH, Liss Y, Mockenhaupt M.
Stevens-Johnson syndrome and toxic epidermal necrolysis
in patients with lupus erythematosus: a descriptive study
of 17 cases from a national registry and review of the
literature. Br J Dermatol 2012;166:575-600.
11. Sassolas B, Haddad C, Mockenhaupt M, Dunant A, Liss
Y, Bork K, et al. ALDEN, an algorithm for assessment
of drug causality in Stevens-Johnson Syndrome and toxic
epidermal necrolysis: comparison with case-control
analysis. Clin Pharmacol Ther 2010;88:60-8.
12. Mockenhaupt M. The current understanding of Stevens-
Johnson syndrome and toxic epidermal necrolysis. Expert
Rev Clin Immunol 2011;7:803-13.
13. Mockenhaupt M. Severe drug-induced skin reactions:
clinical pattern, diagnostics and therapy. J Dtsch Dermatol
Ges 2009;7:142-60.
14. Ghislain PD, Roujeau JC. Treatment of severe drug re-
actions: Stevens-Johnson syndrome, toxic epidermal nec-
rolysis and hypersensitivity syndrome. Dermatol Online J
2002;8:5.
15. Araki Y, Sotozono C, Inatomi T, Ueta M, Yokoi N, Ueda
E, et al. Successful treatment of Stevens-Johnson syn-
drome with steroid pulse therapy at disease onset. Am J
Ophthalmol 2009;147:1004-11.