
Rapid Response Team Utilization of Modified Early Warning ...

Towards Climate Based Early Warning and Response Systems for Malaria
Maquins Odhiambo Sewe
Department of Public Health and Clinical Medicine
Epidemiology and Global Health
Umeå University, Sweden 2017

Responsible publisher under Swedish law: the Dean of the Medical Faculty
This work is protected by the Swedish Copyright Legislation (Act 1960:729)
ISBN: 978-91-7601-641-1
ISSN: 0346-6612
Electronic version available at http://umu.diva-portal.org/
Tryck/Printed by: UmU Print Service, Umeå UniversityUmeå, 2017

I dedicate this dissertation to my parents


“The future never takes care of itself; it is taken care of, shaped, molded, and
colored by the present. Our todays are what our yesterdays made them; our
tomorrows must inevitably be the product of our todays.” ~Dennis Kimbro

i
Table of Contents
Table of Contents i Abstract iii Abbreviations v Contributing Papers vii Preface ix Introduction 1
Malaria and how its transmitted 1 Malaria burden 4 Risk factors for malaria transmission 9 Malaria surveillance 15 Malaria early warning and detection 16 Evaluating economic benefit of early warning systems 17 Summary 20 Objectives 21
Materials and methods 22 Study setting 22 Verbal autopsy 24 Hospital surveillance 25 Environmental data 26 Statistical analysis 29 Methodologies paper by paper 33
Results 41 Distribution of malaria health outcomes 41 Distribution of weather variables 41 Seasonality of malaria deaths and environmental variables 44 Relationship between environmental factors and malaria mortality 46 Prediction of monthly malaria admissions 53 A framework for economic evaluation of early warning and response system
benefits 56 Discussion 60 Conclusions 71 Acknowledgements 72 References 74

ii

iii
Abstract
Background: Great strides have been made in combating malaria, however, the
indicators in sub Saharan Africa still do not show promise for elimination in the
near future as malaria infections still result in high morbidity and mortality
among children. The abundance of the malaria-transmitting mosquito vectors in
these regions are driven by climate suitability. In order to achieve malaria
elimination by 2030, strengthening of surveillance systems have been advocated.
Based on malaria surveillance and climate monitoring, forecasting models may
be developed for early warnings. Therefore, in this thesis, we strived to illustrate
the use malaria surveillance and climate data for policy and decision making by
assessing the association between weather variability (from ground and remote
sensing sources) and malaria mortality, and by building malaria admission
forecasting models. We further propose an economic framework for integrating
forecasts into operational surveillance system for evidence based decision-
making and resource allocation.
Methods: The studies were based in Asembo, Gem and Karemo areas of the
KEMRI/CDC Health and Demographic Surveillance System in Western Kenya.
Lagged association of rainfall and temperature with malaria mortality was
modeled using general additive models, while distributed lag non-linear models
were used to explore relationship between remote sensing variables, land surface
temperature(LST), normalized difference vegetation index(NDVI) and rainfall
on weekly malaria mortality. General additive models, with and without
boosting, were used to develop malaria admissions forecasting models for lead
times one to three months. We developed a framework for incorporating forecast
output into economic evaluation of response strategies at different lead times
including uncertainties. The forecast output could either be an alert based on a
threshold, or absolute predicted cases. In both situations, interventions at each
lead time could be evaluated by the derived net benefit function and uncertainty
incorporated by simulation.
Results: We found that the environmental factors correlated with malaria
mortality with varying latencies. In the first paper, where we used ground
weather data, the effect of mean temperature was significant from lag of 9 weeks,
with risks higher for mean temperatures above 25C. The effect of cumulative
precipitation was delayed and began from 5 weeks. Weekly total rainfall of more
than 120 mm resulted in increased risk for mortality. In the second paper, using
remotely sensed data, the effect of precipitation was consistent in the three areas,
with increasing effect with weekly total rainfall of over 40 mm, and then declined
at 80 mm of weekly rainfall. NDVI below 0.4 increased the risk of malaria
mortality, while day LST above 35C increased the risk of malaria mortality with
shorter lags for high LST weeks. The lag effect of precipitation was more delayed

iv
for precipitation values below 20 mm starting at week 5 while shorter lag effect
for higher precipitation weeks. The effect of higher NDVI values above 0.4 were
more delayed and protective while shorter lag effect for NDVI below 0.4. For all
the lead times, in the malaria admissions forecasting modelling in the third
paper, the boosted regression models provided better prediction accuracy. The
economic framework in the fourth paper presented a probability function of the
net benefit of response measures, where the best response at particular lead time
corresponded to the one with the highest probability, and absolute value, of a net
benefit surplus.
Conclusion: We have shown that lagged relationship between environmental
variables and malaria health outcomes follow the expected biological
mechanism, where presentation of cases follow the onset of specific weather
conditions and climate variability. This relationship guided the development of
predictive models showcased with the malaria admissions model. Further, we
developed an economic framework connecting the forecasts to response
measures in situations with considerable uncertainties. Thus, the thesis work has
contributed to several important components of early warning systems including
risk assessment; utilizing surveillance data for prediction; and a method to
identifying cost-effective response strategies. We recommend economic
evaluation becomes standard in implementation of early warning system to
guide long-term sustainability of such health protection programs.
Key words: Malaria, Mosquito, Lead time, Early Warnings, Forecasts,
Economic Evaluation, Rainfall, KEMRI/CDC HDSS, Kenya, Temperature, LST,
NDVI, Climate, HDSS, GAM, GAMBOOST, DLNM, Remote Sensing, Net
Benefit, Cost-Effectiveness, Boosting Regression, Weather, Public Health,
Infectious Diseases

v
Abbreviations
AS- AQ Artesunate – Amodiaquine
ACF Autocorrelation Function
ACT Artemisinin Combination Based Therapy
An. Anopheles
AR Autoregressive Term
AVHRR Advanced Very High Resolution Radiometer
CDC Centre for Disease Control
DDT Dichlorodiphenyltrichloroethane
DLM Distributed Lag Models
DLNM Distributed Lag Non-Linear Models
EIP Extrinsic Incubation Period
ETA Evapotranspiration
EVI Enhanced Vegetation Index
GAM General Additive Model
GAMLSS General Additive Models for Location, Scale and Shape
HDF-EOS Hierarchical Data Format- Earth Observing System
HDSS Health and Demographic Surveillance System
INDEPTH International Network for The Demographic Evaluation of
Populations and Their Health
InterVA Interpreting Vas
IPTp Intermittent Preventive Treatment for Pregnant Women
ITN Insecticide Treated Nets
KEMRI Kenya Medical Research Institute
KIMS Kenyan Malaria Indicator Survey
LLINs Long Lasting Insecticidal Nets
LST Land Surface Temperature
MAE Mean Absolute Error
MCMC Markov Chain Monte Carlo
MEW Malaria Early Warning System
MODIS Moderate Resolution Imaging Spectro-Radiometer
MVC Maximum Value Compositing
NASA National Aeronautics and Space Administration
NASDA National Space Development Space Agency of Japan
NDVI Normalized Difference Vegetation Index
NMAE Normalized Mean Absolute Error
NMCP National Malaria Control Program
NMSE Normalized Mean Squared Error
NN Nearest Neighbour
NOAA National Oceanic and Atmospheric Administration
P. falciparum Plasmodium falciparum
PACF Partial Autocorrelation Function
vi
pfPR P. falciparum prevalence rate
PSA Probability Sensitivity Analysis
RH Relative Humidity
RMSE Root Mean Squared Error
SP Sulfadoxine/Pyrimethamineÿ
TRMM Tropical Rainfall Measuring Mission
VA Verbal Autopsy
VI Vegetation Index
WHO World Health Organization
WMO World Meteorological Association

vii
Contributing Papers
This thesis is based on the papers I-IV. The papers I and II were published in
open access journals so no permission was required to reprint.
I. Sewe, M., Rocklöv, J., Williamson, J., Hamel, M., Nyaguara, A.,
Odhiambo, F., & Laserson, K. (2015). The association of weather
variability and under five malaria mortality in KEMRI/CDC HDSS in
Western Kenya 2003 to 2008: a time series analysis. Int J Environ
Res Public Health, 12(2), 1983-1997. doi:10.3390/ijerph120201983
II. Sewe, M. O., Ahlm, C., & Rocklöv, J. (2016). Remotely Sensed
Environmental Conditions and Malaria Mortality in Three Malaria
Endemic Regions in Western Kenya. PLoS One, 11(4), e0154204.
doi:10.1371/journal.pone.0154204
III. Sewe, M. O., Tozan, Y., Ahlm, C., & Rocklöv, J. (Submitted). Using
remote sensing environmental data to forecast malaria incidence at a
rural district hospital in Western Kenya.
IV. Sewe, M. O., Tozan, Y., Ahlm, C., & Rocklöv, J. (Manuscript). A
methodological framework for economic evaluation of operational
response to vector-borne disease forecasts.

viii

ix
Preface
The control and prevention of malaria is very important in countries in Sub-
Saharan Africa where malaria contributes to high levels of morbidity and
mortality. Children under the age of five are the most vulnerable with most of
the mortality occurring in this age group. Great progress has been observed in
taming the scourge of malaria, but in countries with higher prevalence the
progress has not been as expected and thus malaria still contributes to high
child mortality plunging communities affected to great suffering and
economic burden. In malaria prevalent areas, reducing malaria deaths in
children would yield huge gains in reducing the overall under five mortality
rates. The world health assembly in 2015, through the sustainable
development goals framework, has targeted the elimination of malaria in
countries reporting malaria transmission by 2030. The new set of sustainable
development goals continues and replaces the millennium development goals
that ended in 2015. To achieve the goal of elimination, improved malaria
surveillance technologies has been cited as one of the key strategies.
In Kenya, about 40% of the population is at risk of malaria. Endemic malaria
transmission is concentrated around the Lake Victoria region and part of the
coastal regions, while highland and semi-arid regions only occasionally
experience epidemics. The use of interventions in the control of malaria can
have great impact if they are implemented in a timely manner before
epidemics, or before anomalous increase in the cases beyond the seasonal
mean occurs. To have enough time to implement interventions, the routine
monitoring of malaria cases reported through active surveillance can provide
information regarding seasonal changes and epidemic anomalies in disease
transmission and provide a foundation for forecasting forthcoming
transmission in communities.
Malaria surveillance used in conjunction with environmental monitoring can
provide early warning alerts if aberrations are observed in comparison to
seasonal transmission patterns. WHO have advised the use of early warning
for the control of epidemics. Early detection using thresholds derived from
malaria surveillance, risk assessment and predictive models, form part of
malaria early warning system. In this thesis, we contribute to informing on the
feasibility and strategies to the development of a malaria early warning system
in an endemic region that is part of an ongoing health and demographic
surveillance system in Western Kenya. We do this, by assessing temporal
lagged risk associations between ground weather data as well as remotely
sensed data to malaria mortality. We use the information from the risk
assessment studies to develop early warning prediction models comparing

x
different lead times to single out the predictive skill and uncertainty. Alerts
emanating from early warning systems often fail to be utilized by decision
makers to initiate response actions due to the inherent possibility of false
alarms, and the lack of technical and strategic response capacity. To aid
decision makers on the timing of appropriate actions, we propose an economic
evaluation framework that integrates response actions with disease forecasts
and able to handle uncertainty in the prediction and response.

1
Introduction
Malaria and how its transmitted
Malaria parasite development in human host
Malaria infections occur when human blood is infected by protozoan parasite
called sporozoites of the genus Plasmodium which is transmitted by female
Anopheles mosquitoes when they take a blood meal from a host [1]. The
sporozoites invade the hepatocytes and proliferate into merozoites. Some
sporozoites differentiate into hypnozoites that remain in the liver for months
to years before dividing and developing into merozoites. It takes around six
days for P. falciparum sporozoites to develop into 40,000 merozoites per liver
cell. Malaria infection begins when the merozoites invade the erythrocytes [2].
A summary of the life cycle of malaria parasite in the human host is displayed
in Figure 1. It has been postulated that the malaria parasites originated from
gorillas [3].
There are five main malaria parasites namely P. vivax, P. malariae, P. ovale
and P. falciparum and more recently discovered P. knowlesi [4]. Currently P.
falciparum and P. vivax are the mostly encountered malaria parasites with P.
falciparum accounting for over 79% of the malaria parasites in East African
countries in Sub-Saharan Africa. P. falciparum malaria is responsible for high
morbidity and mortality in younger children below five years and responsible
for episodes of severe malaria in children [5, 6].
P. ovale has very limited distribution. P. falciparum malaria is characterized
as “subtertian, malignant persistent fevers”. Malaria infections are
characterized with febrile episodes, paroxysm with chills, rigors and sweating.
Malaria shares similar symptoms with other febrile illnesses, which include
body aches, headache, nausea, general weakness and prostration. This has
resulted in treatment of most febrile cases for which not all maybe malaria
related with antimalarial in countries such as Kenya [5].

2
Figure 1. Malaria parasite life cycle, (source: [7])
Malaria parasite development in mosquito
When the mosquito vector takes a blood meal from a human host it ingests
gametocytes which triggers the formation of gametes in the mosquito’s midgut
lumen [8]. In a process called exflagellation, the male microgametes fertilize
the female macrogametes to form a ‘zygote’. Temperature and PH levels of the
xanthurenic acid influence the rate of ‘zygote’ development. After the ‘zygotes’
are formed, meiosis happens and genetic recombination occurs. The spherical
‘zygote’ transforms into an ookinete. The ookinetes uses motility to leave the
blood meal bolus to penetrate the peritrophic matrix that encloses the blood
meal after which it penetrates the apical end of the mosquito midgut
epithelium [8]. The ookinete then transforms into oocysts, a process that takes
about 10-12 days and subsequently develops into sporozoites that burst into
the hemocoel. The sporozoites are then carried by circulation of haemolymph
to all tissues of the mosquito and eventually to the salivary glands [8].
Mosquito life cycle
Mosquitoes go through four distinct stages during their life. The stages are
egg, larva, pupa and adult as shown in Figure 2. The first three stages occur in
water while the adult is an active flying insect. Only the female mosquito bites
and feeds on bloods from humans or animals. After the female mosquito

3
obtains a blood meal, she lays the eggs directly on or near water. The eggs
hatch in water and mosquito larva or “wriggler emerges”. The development
of larva depends on temperature, type of mosquito and availability of food.
The larva lives in the water, feeds and develops into pupa or “tumbler”. The
pupa also lives in water but does not feed. Finally, the mosquito emerges from
the pupal case after 2 - 7 days in the pupal stage. The life cycle takes about two
weeks but depending on environmental conditions, it can take from 4 days to
1 month. The adult mosquito emerges onto the surface of the water and flies
away.
Figure 2. Mosquito development cycle (source: http://www.mosquito.org/life-cycle)
Malaria endemicity
There are three levels of malaria transmission zones. In areas with stable
endemic transmission, populations are continuously exposed to malaria
inoculations due to mosquito bites, however, with seasonal fluctuations. Due
to this persistent exposure, the population usually gets immunity from ages 4
to 5 years. The others are unstable endemic malaria and epidemic malaria
zones [1]. In unstable endemic malaria transmission setting, there is less
permanent transmissions and a huge fluctuation in transmission over time.
This affects immunity as individuals can be exposed to inoculations ranging
from intervals of one year to several years. Epidemic malaria is an extreme
form of unstable malaria where populations or groups of individuals are
subjected to an increase in transmission, not previously or normally
experienced. P. falciparum malaria epidemics usually results in very high
morbidity and mortality [1].

4
Malaria burden
Global burden
World Health Organization’s(WHO) 2015 world malaria report confirms that
concerted efforts towards the prevention and control of malaria has resulted
in significant gains in reducing global malaria burden. Since the year 2000, 57
countries have achieved millennium development goal 6C of over 75%
reduction in incidence while 18 countries achieved reduction of between 50-
75% in incidence by 2015 [9]. However, malaria endemic countries in Sub-
Saharan African, contributing over 88% in global malaria disease burden,
have registered below average decline, blamed on the weak health systems.
For example, Nigeria and Democratic Republic of Congo characterized as very
high stable endemic malaria transmission areas, with a parasite prevalence of
over 40%, together contributed 35% of the global estimated malaria deaths
[10]. Malaria still poses a major burden in most parts of the world with an
estimated 3.2 billion people at risk of infection [9].
European countries reported no malaria infections in 2015 while Southeast
Asia contributed 10% to the global incidence. By 2015, of the 106 WHO
countries, 33 registered less than 1000 malaria cases in 2015, suggesting that
most countries are progressing towards elimination [9].In 2000, 262 million
infections were reported compared to 214 million in 2015, resulting in an
overall decline of 18% over the 14-year period. In the same period malaria
incidence decreased by 37% with parasite prevalence among children 2 to 10
years decreasing from 33% in 2000 to 16% in 2015 [9].
In the same period, malaria deaths for all age groups declined by 48% from
839,000 in 2000 to 438,000 in 2015 and for children under five years, the
mortality reduced by 50% from 723,000 deaths in 2000 to 360,000 deaths in
2015. The WHO African region, which contributes to 90% of malaria deaths
in just 15 countries, registered 57% reduction in malaria mortality among
children from 694,000 in 2000 to 292,000 deaths in 2015. These reductions
represents huge gains in combating malaria contributing significantly towards
the achievement of millennium development goal 4 [9]. Overall, factoring in
changes in population, malaria mortality rate declined by 60% between 2000
and 2015, with a 66% reduction in African region for all ages and a 71%
reduction among children under five years [9].With the reductions achieved
in mortality, malaria was no longer the leading cause of mortality in children
in Africa having been relegated to position 4 contributing 10% to the mortality
burden in that age group and $900 million dollars saved through prevention
strategies over the 14 years [9].

5
Some challenges have been cited in relation to the fight to eliminate malaria
worldwide. As such are the report that 269 million of the 834 million people
at risk are not sleeping under mosquito nets, weaknesses in health systems,
insecticide resistance and anti-malaria drug resistance [9].
Malaria burden in Kenya
In Kenya 75% of the population, live in malaria prone regions. P. falciparum
is the major malaria Plasmodium parasite prevalent in Kenya. The malaria
risk in Kenya is not homogenous, the endemic lake region and coastal areas
are leading in malaria prevalence, and the children under five and pregnant
women at greatest risk due to low immunity [11]. A map of estimated malaria
prevalence for Kenya is shown in Figure 3. Over 50% of the households in the
country at risk of malaria use ITNs. Artesunate (AS)- Amodiaquine (AQ) is the
first-line medical treatment for malaria [9].
Figure 3. Map of Kenya showing spatial distribution of PfPR2-10. CE = Central province; CO =
Coastal province; EA = Eastern province; NA = Nairobi province; NE = North Eastern province;
NY = Nyanza province; RV = Rift Valley province; and WE = Western province. (Source: [12])

6
The national malaria control program (NMCP) under the Kenyan ministry of
health is responsible for the control of malaria in line with the country’s vision
for the year 2030. NMCP has several strategies to combat malaria prioritizing
certain interventions. These interventions include: the use of long lasting
insecticidal nets (LLINs), intermittent preventive treatment for pregnant
women (IPTp), prompt diagnosis and treatment of all malaria cases,
improving the capacity of health care providers, strengthening supply chain of
diagnostic tests and medicines, advocacy and communication to enhance
demand and uptake by communities at risk and also providing malaria policy
guidelines [11].
In the years 2007, 2010 and recently 2015, the Kenyan malaria indicator
survey (KIMS) has been conducted to monitor progress in malaria control
efforts. The 2015 KIMS was conducted to determine progress of important
malaria interventions contained in the Kenya malaria strategy 2009-2018,
which was updated in 2014. The 2015 survey was based on a national
representative sample comprising children 6 months to 14 years and women
of reproductive age 15-49 years in 6,481 households [11]. The survey is also
conducted to assess changes in parasite and anemia prevalence among
children 6 months to 14 years. Obonyo et al. showed that anemia contributes
greatly to mortality in children admitted with malaria [13], and that children
below 10 years serve as the reservoir for P. falciparum malaria [14]. The
parasitemia prevalence among children 6 months to 14 years decreased from
11% in 2010 to 8% in 2015. The prevalence was highest among children 10-14
years at 11% followed by 4-9 year olds at 10%. Among children 6 to 59 months,
prevalence decreased from 8% in 2010 to 5% in 2015. The endemic lake region
characterized by high parasitemia with pfPR2-10 at over 40% [12] had the
highest prevalence at 38% in 2010 compared to 27% in 2015 among children
6 months to 14 years. In the coastal areas, prevalence increased from 4% in
2010 to 8% in 2015. The lake region registered the highest anemia prevalence
at 38% compared to 20% in the malaria low risk areas [11].
Malaria in Western Kenya
The areas around Lake Victoria in Western Kenya have endemic malaria with
transmission throughout the year. Asembo region, which borders Lake
Victoria in Rarieda district and Gem in Gem district, have been part of malaria
research conducted by the collaborative work between the United States’
Centre for Disease Control (CDC) and Kenya Medical Research Institute
(KEMRI) since 1979. To evaluate the impact of Insecticide Treated Nets (ITN)
use on health outcomes such as malaria mortality, a health and demographic
surveillance system (HDSS) was established to provide demographic
information, mortality data and person years of observation [15-19].

7
In 2001, the HDSS was revitalized to monitor socio-demographic changes,
first in Asembo and then expanding to Gem in 2002 [20]. Adazu et al.
presented the mortality profile for the demographic study area for the year
2002 just after the HDSS had been started. They found that the under-five
mortality ratio was 227 per 1000 live births, and malaria contributed 75% of
all sick visits at the health facilities. Malaria and anemia were the main cause
of death in children 1 month to 11 years with mortality fractions of 28.9% and
19.8%, respectively [20]. The main anopheles vector was An. gambiae
constituting 95.6% of all mosquitoes collected between 2002 and 2003 with
7.2 infectious bites per person [20]. In the period 2002 to 2004 in the study
area, Amek et al. reported the prevalence of An. gambiae mosquitoes species
at 86% with entomological inoculation rates of 6.7, 9.3 and 9.6 infectious bites
per year for years 2002 to 2004 [21]. An. gambiae has been the dominant
Anopheles vector in the study area, but since the 2005, its population has
declined due to high ITN use. The dominant species currently is An.
arabiensis [22].
The age–specific mortality fractions were 30.6%, 26.8% and 30.2% for the age
groups 1-11 months, 1 to 4 years and 5 to 11 years respectively [20]. Amek et al
explored the childhood causes of death in the same setting for the period 2003
to 2010 [23]. In general, malaria was the leading cause of death for children
under five with a proportion of 28.2%. Figure 4 shows trends in the under-five
malaria mortality fraction. There was a decrease in the proportion of deaths
due to malaria between 2004 and 2007 and then an increase from 2008. For
example, for the 1 to 4-year age group, malaria mortality fraction decreased to
25.9% in 2007 from 41% in 2004 followed by an increase to 46% in 2008 [23].
Figure 4. Trends in malaria mortality fractions by age group 2003 to 2010 in Asembo and Gem
areas in Western Kenya. (Data source: [23])

8
Hamel et al aptly described the changing trends in mortality in the
KEMRI/CDC HDSS as “a reversal in reduction of child mortality” [24]. In this
study, they explored the trends in childhood mortality among children for the
period 2003 to 2008 with malaria as the leading cause of death for children.
They reported a decrease in malaria parasitemia prevalence from 60% in 2003
to 26% in 2008 resulting in annual relative decrease of 14% [24]. Similar
trends in malaria burden have been documented for other areas in sub-
Saharan Africa [25]. The trend, however, reversed after 2009 with a reported
increase to 41%. Moderate anemia decreased from 11% in 2003 to 4% in 2007
but then increased again to 19% in 2009. The reported ITN use fluctuated
during this period and was 56% in 2006, 69% in 2007, 49% in 2008, and 64%
in 2009 [24].
The reversal in reduction in mortality was also observed when Desai et al.
computed age specific malaria mortality rates for the period 2003 to 2010 in
Asembo and Gem regions [26]. The under-five malaria mortality rate
decreased from 15.8 per 1000 person years in 2004 to just 4.7 per 1000 person
years in 2007. However, the rate increased again to 5.6 in 2008. Malaria
mortality rates among children 5 to 14 years was low with less than 1 per 1000
person years in all the years monitored [26]. In the same period, the
proportion of under five deaths from total annual malaria deaths decreased
from 71% in 2003 to 61% in 2010 [26]. The malaria mortality fraction among
children below five years decreased from 29% in 2003 to 16% in 2010 while
the fraction in the 5 to 14 years’ age group increased from 16% to 21% in the
same period [26]. The decrease in child mortality observed up to 2007 was
attributed to the use of well-proven child survival interventions, marginal
improvement in social economic status and change of first line malaria
treatment from SP to AL [24]. Malaria contributed to the high mortality rate
observed in 2008, which has been pinned on the widespread stock out of
antimalarial drugs that began in September 2007 and persisted for most of
2008 in which drugs were out of stock for 7 months including three months
during the high transmission months [24]. The influx of people into the study
area after the post-election violence may have also resulted in the peak in
observed mortality in 2008 [27].
Streatfield et al. analyzed verbal autopsy (VA) data for HDSS sites globally to
document malaria specific mortality [28]. The Kisumu [29], Nairobi [30] and
Kilifi [31] HDSS sites in Kenya contributed to the cohort. Malaria mortality
rate among infants was 0.38, 0.17 and 0.8 per 1000 person years for Kisumu,
Kilifi and Nairobi respectively. The malaria mortality rate among under-fives
was highest in Nairobi site at 0.18 per 1000 person years and lowest in Kilifi
at 0.04 per 1000 person years [28].

9
Risk factors for malaria transmission
Physical environment
Temperature
The development and survival of the mosquito vector that transmits malaria
depend on environmental factors such as temperature and precipitation. The
spatial limits of distribution of malaria is affected by environmental suitability
of malaria vectors where temperature plays a pivotal role [32, 33].
Temperature modulates endemicity in some areas and prevents transmission
in others [10, 32, 34]. This explains why stable malaria transmission is
restricted to the tropics [35-37]. Future climate scenarios show a warming
planet with changes in length of transmission season for malaria. The
highland regions in East Africa are projected to see an increase in the persons
at risk of malaria with increasing temperature [35, 38-40]. Temperatures
above 220C has been shown to be suitable for stable malaria transmission
while temperature above 320C result in high vector mortality [36].
Since insects are ectothermic, their development greatly depends on
temperature. They are also poikilothermic meaning their metabolic rates are
determined by temperature. Low temperature results in larger insects as they
take long to develop to adult stage. Bayoh et al. evaluated the effect of
temperature on the aquatic stages of An. gambiae from egg to larva. They
found that the optimal development temperature was between 28-320C and
for mosquito production between 22 -260C. Below 160C and above 340C no
vector could develop [41-43]. In the coastal and western regions of Kenya,
temperature was found to negatively correlate with populations of An.
gambiae and An. arabiensis [21, 44]. Kirby also showed that vector survival
decreased with increasing temperatures and larval stage duration decreased
with increasing temperature. The survival of An. arabiensis was 65%, 59% and
below 40% at 250C, 300C and 350C respectively and larval stage duration was
12.2,10.5, and 10.5 days for the same temperature ranges [45]. Higher mean
water temperature has been shown to lower larval duration by four days in
two sites in Kenya [46].
Malaria parasite sporogony cycle, the time it takes for sporozoites to appear
in salivary glands of the mosquito after an infected blood meal, is also affected
by temperature. Blanford et al used thermodynamic parasite model to assess
temperature effect on extrinsic incubation period (EIP) of malaria parasite at
four sites in Kenya with varying climatic conditions [47]. EIP is the time it
takes the parasite to develop inside the mosquito after an infected blood meal
to the time of transmission to another host. They used different time

10
resolution for temperature, monthly, daily and hourly means. In all the four
areas, the temperature parasite development relationship was non-linear with
an inverted U-shape. For Kisumu the parasite development increased linearly
from 160C peaking at 310C then steadily declining [47]. In warmer
transmission areas, EIP increased with the finer the temporal resolution of
mean temperature. For example, in Kisumu, using the monthly temperature
EIP took 12.5-16.5 days while using hourly temperature, EIP took longer (15-
18) days [47]. Diurnal temperature fluctuations can also alter incubation
period of parasites [48], mean temperature of below 210C has been shown to
speed parasite development while one above 210C slowing development [49].
Minimum and maximum temperature was shown to correlate with
entomological inoculation rates. A correlation of -0.36 and 0.24 was found for
maximum and minimum temperatures with An. gambiae human biting rate.
The effect was pronounced when lags of temperature indicators were taken
into consideration [50].
Rainfall and humidity
Rainfall provide breeding sites for mosquitoes to lay their eggs. For example,
rainfall frequency and intensity determine pond stability for vector breeding
[51]. The amount of rainfall, in combination with wind and temperature, also
determines the levels of relative humidity (RH). RH, which is the amount of
water vapor in the air, influences mosquito vector relative abundance [42, 52,
53]. RH of above 55% was shown to determine malaria survival [53], while
Bayoh et al. showed that vector survival increased with high levels of RH. The
peak vector life expectancy was determined for RH of 100%. 40% was the
minimum RH necessary for vector survival [42].
An. gambiae vectors breed in temporary and turbid water provided by rain
[36]. Mosquito densities have been show to increase during the rainy season
[54], followed by more malaria associated febrile illnesses [55]. Malaria
incidence was shown to be higher in areas with high water accumulation [56]
High water accumulation has been depicted as having strong linear
relationship with malaria presentation [57], and to be significantly associated
with occurrence of malaria parasites [58]. However, excessive rainfall can
flush existing mosquito larvae temporally resulting in reduced vector
population and, thus, malaria incidence. This results in a non–linear
relationship between rainfall and malaria health indicators as shown in [59-
61] where malaria increases with increasing rainfall, peaks then falls at the
extremes
In permanent water environments, predation determines water malaria
vector populations. The larvae of mosquitos stay at the surface of water where

11
they are adapted to feed and obtain atmospheric oxygen [42]. Craig et al.
determined that five months of rainfall above 80 mm in a year was sufficient
for malaria to occur if all the other requirements are met, and when
temperatures are high, only three months of rainfall above 80 mm was
sufficient for stable malaria transmission [36]. Vector biting rates have also
been found to correlate with the amount of precipitation [50, 62]. Patz et al.
found a correlation between the amount precipitation and An. gambiae
human biting rate with a lag of up to four weeks [50]. Amek et al found no
significant relationship between precipitation and mosquito density; however,
mosquito density peaked in the month of May during the rainy season [21]. In
drier savannah region where annual rainfall amounts fall below 1000 mm, An.
arabiensis species of mosquitoes proliferate [63]. In these regions, the peak
of mosquito density has been determined to correlate with rainfall seasons
with significant correlations observed with a six week lag [64]. Further, a
correlation of 0.87 has been found with five months of rainfall in a year [65],
and two months lag of rainfall in east African highlands [66]. Moisture index
also determines mosquito species composition with an index above 0.7 found
suitable for An. gambiae while index below 0.7 are suitable for An. arabiensis
[67].
Land cover
Satellite derived data has been used widely in malaria epidemiology. The most
commonly used remote sensed land cover proxy is normalized difference
vegetation index (NDVI) [68, 69]. Vegetation is very reflective in the near
infrared and absorptive in the visible red. The ratio of these can be used as an
indication of the status of vegetation [70]. This ratio ranges between -1 and 1,
with higher values showing denser vegetation, 0 signifies lack of vegetation
and -1 representing water bodies. A decrease in vegetation index may mean a
decrease in vegetation density thus water availability. It could also mean
suppression of vegetation due to flooding [71].
Land cover especially vegetation, provide suitable resting and sugar feeding
places for adult mosquitoes and creates the right microclimatic conditions for
mosquito proliferation. Vegetation state monitoring and mapping of water
bodies is crucial in identifying sources of malaria vectors [72]. Many studies
have explored the correlation between NDVI and malaria transmission
factors. For example, in Nigeria NDVI was singled as an important variable
for malaria risk assessment [73], shown to positively correlate with mosquito
density [21, 74-76]. NDVI is also correlated with mosquito biting rates, with
biting rate transient in high NDVI areas [62] and negatively associated with
mosquito larval densities in and around ponds [77].

12
NDVI has been used to develop malaria predictive models showing different
lag patterns [78] between NDVI levels and malaria incidence. In Kenya,
Burundi and Ethiopia, malaria in a given month was best predicted by average
NDVI of the previous month [57, 79-81]. Malaria has been shown to correlate
highly with low levels of NDVI; low NDVI was associated with abundance of
mosquito vectors along the coast of Kenya [44], a threshold of 0.3-o.4 resulted
in 5% increase in malaria presentation in Kenya [57], and low NDVI was
associated with increased number of malaria cases in Bangladesh [82].
However, in West Africa higher NDVI were associated with malaria infections
in children [83]. Distance to vegetation has also been associated with
Anopheline aggressiveness [84]. Exposure to forest areas has also been linked
with upsurge of malaria infections [85], and high risk has been reported for
houses surrounded by green vegetation [86].
Socio-economic factors
Education and economic status
Education, economic status and outdoor activities in endemic areas [87] also
affects the odds of one being at risk of malaria. It has been proven that low
education and economic means increases the risk of malaria infection [88]
and working outdoors [89], having high household wealth [90-92], and high
education level for the caregiver [93, 94], provide protective effects. High
social economic ability is associated with high mosquito control [95] and,
thus, the low risk observed.
Human practices
Human activities that alter land cover affect the mosquito population levels.
In highlands and lowlands of Western Kenya, an increase in farmland use
provided suitable environment for An. gambiae larva development [96, 97].
Mature maize fields, newly cultivated fields, grassland [97] and agro-
ecological zones [76] were correlated with presence of mosquito larval
habitats and irrigated fields associated with malaria parasitemia [98]. It has
been shown that areas where land cover has changed due to deforestation
experience high rates of malaria [99, 100] as new breeding sites are created .
Malaria transmission risk increases among those living in proximity to
stagnant water (OR=2.1) [101], permanent ponds [102] or near breeding sites
[100, 103, 104] and in areas with irrigated land (RR=2.68) [105] and wet
lowland (OR=4.45) [106].

13
Housing conditions
Housing characteristics also affect malaria risk. Living in houses with
thatch/mud roof and mud floors increased the odds of malaria risk [107]. In
Uganda, it was shown that houses with earth/sand floors increases odds of
malaria (OR=2.65) and sand/dung floor having odds of (OR=1.8) [93] as
compared to finished surfaces. In Burkina Faso, having earth brick floor
protected (OR=0.2) households against malaria infection while stone floor
increased risk [108]. It has been shown that living in earthed roofed houses
and sleeping in same room with animals increased risk of malaria infection by
a magnitude of 2.5 and 1.8 respectively [105]. The type of house wall material
and living in areas with high housing density has also been shown to amplify
risk to malaria [89, 109]. Having a wooden or mud house has been associated
with increased risk (OR=1.32) in Rwanda [86] and OR=1.63 in Eritrea [106].
Houses with holes also increase odds of malaria (OR=1.59) as shown by
Woyessa et al [110]. Household size has been shown to negatively correlate
with malaria [111].
Prevention measures
The huge gains in the global malaria burden reduction can be attributed to
significant increase in access and utilization of malaria prevention strategies.
For example, in 2015, 67% of households in sub-Saharan African had access
to ITN compared to 56% in 2014 with 82% of the households with access
actually using them. The proportion of the population sleeping under ITNs
increased from 46% in 2014 to 55% in 2016 with the proportion of under-fives
sleeping under ITN seeing a major leap from <2 % in 2000 to 68% in 2015 [9].
In Kenya, through the KIMS, it was reported that 63% of the households had
at least one long lasting insecticidal nets (LLINs) in 2015 compared to 44% in
2010. 40% of the households had 1 net for two people. 48% of the people in
the households slept under a LLIN the previous night prior to interview. LLIN
usage depended greatly on ownership with 71% of the households with at least
one LLIN sleeping under LLIN. There was an increase in the proportion of
children sleeping under LLINs from 39% in 2010 to 56% in 2015. The
percentage of pregnant women sleeping under LLINs also saw an upward
trajectory with an increase of 22% from 36% in 2010 to 58% in 2015. The
increase in net coverage was observed in high risk areas including the lake,
coastal and epidemic highland regions [11].
The Kenya malaria control strategy recommends pregnant women to receive
intermittent preventive treatment (IPTp) as prophylaxis against malaria
during antenatal care. From KIMS 2015, 75% of the pregnant women who

14
delivered two years preceding the survey received at least 1 dose of
Sulfadoxine/Pyrimethamine (SP)/FANSIDAR, 56% received at least 2 doses,
while 37% received the three recommended doses [11].
One of the pillars of the Kenya malaria control strategy includes prompt
parasitological diagnosis and treatment within 24 hours of onset of symptoms.
In the 2015 survey, 7 out of 10 children presenting with fever were taken to
health facilities for medical advice with 72% receiving treatment. 39% of the
children had their blood taken for testing while 25% got the recommended
Artemisinin combination based therapy (ACT) [11].
Prevention in epidemic situations
The control measure to be used when in epidemic malaria situation depend
on the time window to act. Early detection of epidemics provide shorter lead-
times, and consequently individual case management is preferred to reduce
mortality and morbidity. The drugs used in individual case management
should have at least 95% efficacy. Currently ACT has been widely used in
treating uncomplicated P. falciparum malaria [112] and intramuscular
injectable Artemether for severe presentation of malaria. ACT can also be used
for mass fever treatment [113]. The huge reduction in malaria burden in sub-
Saharan African has been attributed to ACT [114]. In Kwazulu Natal in south
Africa Artemether/Lumefantrine (AL) was used to control epidemic malaria
with significant reduction in both outpatient and inpatient admission due to
Malaria [114]. AL was also instrumental in reducing mortality due to malaria
in Tigray region of Ethiopia during the May–October malaria epidemic [114].
In regions with medium to high levels of transmission, mass screening and
treatment (MSAT) can result in lower malaria burden as shown by Crowell et
al in Sub–Saharan countries [115]. Mass screening of the community and
treatment with AL can reduce transmission in high malaria endemic regions
[116].
If an epidemic has been predicted and there is sufficient time to act, vector
control measures provide better option to curb the high risks of mortality and
transmission associated with epidemics [113]. The vector control activity
should be well planned, targeted and timely. Vector control as an intervention
is most effective when used at beginning of an epidemic and with high
coverage >85% of the epidemic risk region.
Vector control works to curtail the reappearance of malaria in a previously
controlled area and to prevent gradual transmission increase over the years or
increase in annual seasonal transmission. The most widely used vector control
strategy is Indoor Residual Spraying (IRS). It is recommended that the spray

15
chemical used in IRS campaigns should have a residual action beyond 6
months. Synthetic pyrethroids have been shown to be effective and provide
residual action of between 2-6 months. The spraying of houses to get rid of
mosquitoes has been shown to lower risk of malaria infection [93]. Spraying a
household in the last six months reduced the odds of malaria infection
(OR=0.26) in Eritrea [106].
The use of ITNS may not be very effective in epidemic situations but could be
useful to reduce morbidity in endemic regions where coverage is high. In
Ethiopia Alemu et al showed that the odds of malaria infection increased for
those not using ITN [88, 101, 109, 117, 118] with an odds ratio of 13.6 [101].
Larval control is another intervention that may be less useful in epidemics but
may prove effective when breeding sites are fewer, known, permanent and
accessible [113]. Several studies have shown the efficacy of using both IRS and
ITN in malaria control. In Western Kenya highlands characterized by malaria
epidemics, IRS was shown to reduce parasitemia by up to 64% in intervention
areas with effect persisting for six months [119].
In the countries with high malaria transmission burden, a combination of
both IRS and ITN significantly reduced malaria parasitemia prevalence [120-
126]. It has also been shown that using a combination of IRS with rounds of
Dichlorodiphenyltrichloroethane(DDT) and MSAT, it is feasible to lower
parasitemia prevalence in moderate transmission settings in Africa, however
higher coverage levels of over 90% is necessary to achieve similar reductions
in high transmission environments [127].
Malaria surveillance
Public health malaria surveillance systems comprise detection, registration,
confirmation, reporting, analysis and feedback [128]. The main purpose of the
surveillance is to inform policy and improve timely response [129].
The action included in surveillance system includes acute response and
planned responses, which are supported by communication, training,
supervision and resource provision [128]. Activities included in the response
system include confirming diagnosis through laboratory testing, active case
finding, collection of clinical and environmental data, synthesis and
interpretation of data [129].

16
Malaria early warning and detection
Malaria epidemics affect populations with less immunity in highlands and
semi-arid areas of Africa and occur due to increase in temperature which is
normally low [130]. One of the targets of the Roll Back Malaria initiative is to
detect malaria epidemics within two weeks of onset. Early detection and
prevention of malaria outbreaks is a key pillar in malaria control strategy. An
early warning system has been aptly defined as “The provision of timely and
effective information, through identified institutions, that allow individuals
exposed to hazard to avoid or reduce the risk and prepare for effective
response” [131].
An early warning system for malaria control in Africa has been formulated by
WHO through a framework [132]. The malaria early warning (MEW)
framework involves the use of vulnerability, transmission risk, and early
detection indicators. Vulnerability factors include immunity levels, migration,
malnutrition and HIV while transmission risk may include factors such as
rainfall and temperature. Early warning indicators can be obtained through
routine case reporting and using set thresholds to issue alerts [132]. The use
of malaria early warning system in epidemic prone regions has been
recommended in order to optimize lead times for control managers to act
[133-135]. Abeku et al have advocated for improved malaria surveillance to
beef up early detection capacity in malaria epidemic prone regions in Africa
[130] in current focus to achieve targets set for malaria in the Sustainable
Development goals [9]. Lindblade showed that monitoring mosquito density
can also be used for early warning [136]. With improvement in surveillance, it
would be possible to precisely determine when an epidemic begins.
Combining surveillance data and malaria risk factors, predictive models can
be developed to provide early warnings for effective responses.
Early detection
Early detection techniques with thresholds computed from baseline data have
been used in malaria control in different epidemiological settings. Cullen
showed that using historical malaria patterns, it was possible to detect
departures from normal transmissions in Thailand. Any incidence greater
than two standard deviations from normal mean were flagged as anomalous
[137]. The Cullen method above for early detection was used also in endemic
areas in Zambia where upper confidence limit was used as threshold for
detection [138].
The highland malaria project set up surveillance in 20 sites in Kenya and
Uganda to detect abnormal malaria incidence in these sites [139]. Utilizing an

17
automated system, aberrations were detected based on weekly and region
specific levels of malaria incidences compared to baseline values from the
previous seven years of data. The anomalous weekly incidences were
computed by taking a difference of particular week from the de-trended mean
and dividing by the baseline standard deviations [139].
Malaria forecasts
Historical malaria case surveillance data can be modelled to make short-term
predictions. In Ethiopia, a seasonal adjustment method was used to make
forecast with one-month lead using historical data [140]. The relationship
between malaria incidence and climatic factors [78, 141, 142] has also been
exploited to develop prediction models that could act as early warning systems
with varied lead times. For example, remote sensing derived precipitation was
shown to correlate with malaria incidence anomalies in Eretria with a lead-
time of two to three months [143], real time rainfall monitoring has been used
as an operational epidemic warning system [144], remote sensing data used
to predict malaria incidence in epidemic prone areas in Kenya [145]. Hay
showed that rainfall data gave timely and reliable early warning for the 2002
malaria epidemic in Kericho, Kenya [146]. In Ethiopia, rainfall, vegetation
index (VI) and evapotranspiration (ETA) provided prediction lead times of
one to three months [81], and use of weather factors and including previous
malaria cases provided a lead time of one month [147]. Thomson et al
parameterized a non-linear quadratic relationship between rainfall and
malaria to predict anomalous malaria months. The rainfall data provided
warning on high transmission years before the peak seasons [61].
Longer lead times for predictions can be achieved using seasonal climate
forecasts [148-151]. Using seasonal climate forecasts in India, the model was
able to identify high and low malaria years with high skill with three month
forecast lead time [149]. In Botswana, a four-month lead time was achieved
using seasonal climate forecasts data to forecast probabilities of high and low
malaria incidences with high precision [151].
Evaluating economic benefit of early warning systems
In most areas that experiences malaria epidemics, MEWS are not yet fully
functional. Because of this, it is possible to evaluate only certain components
of their roles such in reduction of number of cases by use of interventions such
as vector control strategies. The type of information used in providing forecast
determine the timing of interventions that is crucial in assessing economic
benefit of MEWS. Making comparisons between different intervention

18
strategies with and without MEWS, offer means to measure the economic
benefit of having a MEW in place.
Drummond defines economic evaluation as “the comparative analysis of
alternative courses of actions in terms of their costs and consequences”. Some
of the methods used in economic evaluation includes, cost minimization
analysis, cost effectiveness analysis, cost utility analysis and cost benefit
analysis. In the assessment of economic value of early warning systems, either
of the following two approaches can suffice. One is analyzing users of the
systems willingness to pay referred to as contingent valuation. The other is
cost avoidance calculations which utilizes statistical procedures to perform
cost estimations to evaluate damage prevented if warning is in place and
compares with resources needed set in place and operationalize the system
[152]. To perform an economic evaluation of an early warning system we
would need to know the investment costs, maintenance and repair costs and
operating costs [153].
Some of the factors that affect effectiveness of MEWS include personal and
cultural factors, prediction related factors and dissemination related factors.
The prediction related factors include type I errors which are missing alerts,
type II errors which are false alerts [152]. The overall operational cost of the
system, societal economic losses arising from false alerts an societal savings
should be computed to appreciate the cost benefit of the early warning system
[154].Worrall et al. performed a cost effectiveness analysis to determine the
effectiveness of using A MEW with insecticidal residual spraying program for
Zimbabwe [155, 156]. They compared different levels of coverage of IRS with
varied timing to the do nothing strategy which was taken as having no MEW
in place. The do nothing assumed a coverage of 0% thus representing situation
with warning [156]. The indicators used for economic evaluation were, the e
total number of cases each year per intervention scenario, the incremental
cost of spraying compared to do nothing, the incremental cost per case
prevented compared to do nothing, the total cost of malaria control and the
net incremental cost per case prevented compared to do nothing [156].
Economic evaluation of early warning with uncertainties in
prediction
Predictive information emanating from early warnings are seldom used by
disease control managers due to the level of uncertainty associated with the
forecasts. With low prediction accuracies, the benefits of interventions could
be hard to tease out and thus public health officials not use the information to
take preventive measures [157]. Decision makers that act based on predicted

19
events may suffer if the alarm is false. It has been shown that this information,
however uncertain could still be very useful to decision makers [157].
Early warnings should be provided well in advance to allow sufficient lead
time to take action. However, as the lead time increases, the uncertainty
associated with the predictions increases [131] such as the uncertainties
inherent in seasonal weather forecast that provide longer lead times. Schröter
et al illustrate the interplay between lead time and warning reliability in Figure
5. in its application to early warning for flash floods [153].
Figure 5. Warning reliability as a function of lead time (source: [158])
Every prediction given has some error attached to it that would either result
in a false negative, a false positive or difference in predicted and observed
cases. Every warning message should include the level of uncertainty and the
expected cost of taking action [131]. To improve the performance of EWS,
decision-making should include the expected consequences of taking action
in terms of probability of a false and a missed alarm. An acceptable level of
probability of false alarm should be set using a threshold and included in the
economic evaluation. The incidence of false and missed alarms can be greatly
reduced by factoring in uncertainty and the corresponding action taken [131].

20
Summary
We have seen that several factors act together to modify populations risks to
malaria infections. Environmental risk factors; including rainfall,
temperature and land cover characteristics; vector control methods such as
IRS and use of LLINs affect vector abundance and competency to transmit
malaria. Human behavior such agricultural practices, health seeking patterns
and economic means determine the malaria burdens experienced by
households. Monitoring these indicators through robust surveillance system
provide mechanism to quantify the relationships and improve management of
risks. In order to have better control and effective use of available
interventions, understanding these dynamics and using the information in
developing systems that help predict levels of expected future caseloads can
result in progress towards achieving malaria elimination especially in areas
burdened by malaria. To increase the sustained utilization of predictive
systems among public health officials, uncertainties in predictions and
intervention effectiveness should be considered jointly and strategically.

21
Objectives
The main aim of this study was to assess the prospects and feasibility of using
climate and environmental information to forecast malaria incidence in
Western Kenya, and to develop a methodological economic framework
assisting decision making of time sensitive counter measures responding to
forecasts. Our contribution to an early warning system is illustrated in Figure
6. The specific objectives were to:
I. Determine the association of weather variability and under five
malaria mortality using data from KEMRI/CDC HDSS
II. Evaluate the association of remotely sensed environmental conditions
and malaria mortality in three malaria endemic regions in Western
Kenya
III. Use remote sensing environmental data to forecast malaria incidence
at a rural district hospital in Western Kenya and evaluate forecast
accuracy
IV. Develop a methodological framework to integrate economic impact
models of operational response to forecasts and their uncertainty
Figure 6. How the thesis papers contribute to core components of early warning systems.

22
Materials and methods
Study setting
We extracted the health outcome data was from the KEMRI/CDC Health and
Demographic surveillance system (HDSS). In most poor countries, vital
registration data such as births and deaths are often incomplete, thus the
HDSS framework provides complete data by collecting demographic
information from all residents in geographically defined regions in a country
[159-161]. There are several HDSS sites in Africa and Asia under the umbrella
body INDEPTH network [160] with a systematic collection of health and
demographic data. The database is available online for researchers [162].
The KEMRI/CDC HDSS [20, 29] is conducted at three contiguous sites in
Western Kenya about 60km away from KISUMU County. Today, the
KEMRI/CDC HDSS follows a population in three geographically defined
areas. The first site to be enumerated was Asembo in 2001, followed by Gem
in 2002 and Karemo in 2007. The HDSS covers an area of about 700 km2
located at latitudes ranging from -0.210 to 0.130 and longitudes ranging from
34.16o to 34.520. The topography of the HDSS area comprises gentle hills and
valleys with a number of streams and rivers. The map of the HDSS area is
shown in Figure 7. The surveillance commences with a baseline census, after
which regular census are conducted to update the population. Residency
status in the surveillance is gained by staying in the study area for four
calendar months or being born to a resident [20, 29].
Figure 7. Maps of Africa, Kenya, Western Kenya and the KEMRI/CDC HDSS Study sites Karemo,
Gem and Asembo (source: [29]).

23
The population changes through demographic processes such as births,
deaths and migrations. In the KEMRI/CDC HDSS, three censuses are
conducted in a year. Besides births, deaths and migrations, a myriad of other
information is collected from the residents. These include education levels,
ownership of household assets used to construct wealth quintiles [163], house
structures, marital status, immunization status for children and cause of death
data derived using verbal autopsy [20, 29]. The HDSS has provided a
sampling frame for conducting several surveys for other research projects
using the population data. The KEMRI/CDC HDSS supports TB, Malaria, and
HIV projects within the KEMRI/CDC public health collaboration. The health
component of the HDSS also involves collecting data on morbidity at health
facilities in the HDSS areas. Inpatient information is collected at Siaya district
hospital located in Karemo area while outpatient data are collected at Ting’
Wangi and Njenjra Health facilities located in Karemo and Gem respectively
[20, 29].
From the 2012 annual report, there were 42,569 compounds with 58,720
households in the study area. The median number of individuals in a
household was four. Each compound has at least one house separated by
agricultural field. The total population under surveillance was 240,633
residents. The residents by area were 69,472, 86,279 and 84,882 in Asembo,
Gem and Karemo respectively. 53% of the population were females while
children below 15 comprise 45% of the population. Children below 5 years
comprise 15% of the population while the elderly, those 65 years or above,
formed only 5% of the population. There were 7,205 births in 2012. The
population structure is typical for a developing country (Figure 8).
The crude death rate, under five mortality rate and infant mortality rate were
10, 18 and 50 per 100o person years respectively with a life expectancy of 59
years at birth. The general fertility rate was 132 per 1000 women in
reproductive age group with a total fertility rate of 4 children per woman. 87%
of children 6-10 years are enrolled in school in the study area. The houses in
the study area are made of mud, brick or cement with thatched or iron sheet
roofs [20]. Subsistence farming is the main economic activity. During normal
years, the normal annum is characterized by two rainy seasons stretching from
March to May and November to December.

24
Figure 8. Population pyramid for the KEMRI/CDC HDSS Study sites (Asembo, Gem and Karemo
2012)
Verbal autopsy
Poor countries often lack complete reporting of vital statistics such as deaths
and births. Autopsies are often not conducted on all deaths, thus getting
reliable estimates on causes of death at population levels is impeded. To
circumvent this shortfall, verbal autopsy (VA) has been recommended for use
in poor resource setting [164-167]. Verbal autopsy involves the collection of
signs and symptoms the diseased suffered prior to death. This information is
then used to prescribe a probable cause of death. Deaths in the KEMRI/CDC
HDSS are collected using a dual system. One involves the use of village
reporters who report all deaths that happen even for non-resident members
as soon as they occur. The other is the usual surveillance conducted by
community interviewers who visit the households every four months. The
prior was included to provide timely reporting of both deaths, births and
currently pregnancies to capture neonatal deaths. When a death occurs, one-
month mourning period is allowed and then VA interviewers are sent to
conduct interview with the caregiver of the diseased prior to death. The VA
questionnaire is a standardized questionnaire such as [168, 169] collecting
symptoms for different demographic categories such as age and gender. The
VA process in the HDSS has been described in previous studies [20, 23].

25
Assigning cause of death
There are two main ways of assigning probable cause of death to signs and
symptoms collected using VA. The first one is physician coding where the VA
questionnaire is given to two or more physicians to review and come up with
a probable cause. The second system, which has increased in popularity in the
recent years, is the use of computer based statistical methods to proffer
probable causes of death from VA. The most used is the INTERVA method
[170-172]. In the KEMRI/CDC HDSS physician coding was used up to 2008
after which INTERVA method was adopted. The physician coding involved
giving two clinicians the VA questionnaires to review. They would come up
with three probable causes of death, which would be compared using a
computer algorithm. The cause that matched from the two clinicians would
be assigned as the probable cause of death. If no match was found, a third
clinician would be asked to also review the VA questionnaire and come up with
a cause of death, which would again be compared. If still no match, an expert
panel would be setup to come to an agreement. From, 2009, all the data from
the VA questionnaires were converted to INTERVA format, which is a series
of variables in binary format detailing presence or absence of symptoms. The
INTERVA methods is more systematic [170] and not prone to biases
encountered with the physician coding which would depend on experiences
and qualifications of the people reviewing the VA questionnaires. The
INTERVA methods uses the Bayesian framework that incorporates expert
opinion to give prior probabilities of certain diseases given presence of a set of
symptoms [170, 171]. The INTERVA methods includes toggle buttons to cater
for areas with high prevalence of HIV and Malaria such as the KEMRI/CDC
HDSS.
Hospital surveillance
The KEMRI/CDC collects information on morbidity at different health
facilities in the study area. The inpatient data is currently collected at Siaya
district hospital while outpatient data is collected at two health facilities,
Njenjra and Ting’ Wangi. All children admitted at Siaya district hospital have
their blood samples taken and tested for malaria parasites.

26
Environmental data
MODIS Remote sensing data
Two Moderate resolution imaging spectro-radiometer (MODIS) satellite
sensors were deployed by international earth observing system run at NASA
to aid in the global studies of the atmosphere, land and ocean processes. The
morning platform with overpass times of 10.30 am and 10.30 pm in
descending and ascending modes respectively called terra was the first to be
launched in December 1999. The second afternoon platform called aqua was
launched in May 2002 with overpass times of 1.30 pm and 1.30 am in
ascending and descending modes respectively [173]. The MODIS instruments
sweep the earth at ±55 nadir in 36 bands. Bands 1-19 and 26 are in visible and
near infrared ranges while the rest of the bands are in thermal infrared from
3-15µm [174]. The sensors take images of reflections during the day and
emissions at night or day every one to two days. Due to global coverage and
great radiometric resolution, the MODIS satellites are very useful in the study
of earth processes.
MODIS Land surface temperature
Land surface temperature (LST) is a crucial indicator of physical processes in
surface energy and water’s spatio-temporal equilibrium. LST has been used in
the study of evapotranspiration, climate change, hydrology and vegetation
monitoring[175]. LST is computed from the radiations emitted from the land
surface such as vegetation or soil surfaces at instant viewing angles [173]. The
single infrared channel and split window [174, 176] methods are used to
estimate LST from satellites. The split window method corrects for the effect
of atmosphere and been used to compute MODIS LST products [177]. The
MODIS LST products are created through spatial and temporal
transformations to daily and 8-day gridded product.
The datasets are archived in hierarchical data format- earth observing system
(HDF-EOS) [177]. The MOD11A1 daily LST product at 1km resolution is
generated from the MOD11_l2 product by mapping the pixels to a day in a
earth location on sinusoidal projection [177]. The datasets are generated at tile
level, which is 1113 km by 1113 km with 1200 rows, by 1200 columns. The
MODIS tiles downloaded for this study are h21v08 and h21v09 that covered
the KEMRI/CDC HDSS area. The MODIS MOD11A1 LST product scientific
datasets extracted for this study were lss_day_1km, qc_day, lst_night_1km
and qc_night. The variables with qc prefix are for quality assurance [177].

27
MODIS Vegetation Index
Vegetation indices (VI) are transformations of two or more spectral bands that
can aid in the robust spatial and temporal comparisons of photosynthetic
activity and canopy variation[178]. They are indicators of vegetation growth
and vigor [179]. The MODIS VI are designed to provide consistent spatial and
temporal comparison of global vegetation conditions. The two VIs are NDVI
and Enhanced vegetation index (EVI). While NDVI is sensitive to chlorophyll
characteristics, EVI is more correlated to canopy variations. The MODIS
NDVI has been described as the ‘continuity index’ [180], it increases the
temporal extent of the NOAA-AVHRR derived NDVI time series. NDVI is the
normalized ratio of the near infrared (NIR) and the red bands.
𝑁𝐷𝑉𝐼 =𝜌𝑁𝐼𝑅 − 𝜌𝑟𝑒𝑑
𝜌𝑁𝐼𝑅 + 𝜌𝑟𝑒𝑑
Where 𝜌𝑁𝐼𝑅 and 𝜌𝑟𝑒𝑑 are the surface bidirectional reflectance factor in their
respective MODIS bands. NDVI has been used widely because of its stability
in the identification of seasonal and inter-annual changes in vegetation
growth and activity. However, the NDVI ratio is non-linear and prone to
additive noise effects like cloud cover [178]. Gridded VI maps are generated
using surface reflectance corrected for molecular scattering, ozone absorption
and effects of aerosols [180]. The VI algorithms use the upstream surface
reflectance (MOD09) product to temporally composite the images to create
the VI products [181]. Maximum value compositing (MVC) method is used to
create the composite VI products. In the MVC algorithm, several images over
a given time interval are merged by taking the input pixel with the highest
NDVI value to create a single cloud free image [180-182]. Some of the
objectives of compositing include; depiction and reconstruction of
phenological variations and to maximize global and temporal coverage [182].
The MODIS VI are produced at 250 m, 500 m, 1 km and 0.05 degrees spatial
resolution. The MODIS VI are also produced in tiles which measure about
1200 km by 1200 km and mapped in the sinusoidal grid projection [181].
There are six MODIS VI products but for our purposes, we used the MOD13Q1
16 day 250 m VI product. The MOD13Q1 is generated using the daily MODIS
level 2G surface reflectance product. The MODIS VI data products are stored
in HDF-EOS format [181].
28
MODIS data for the study area
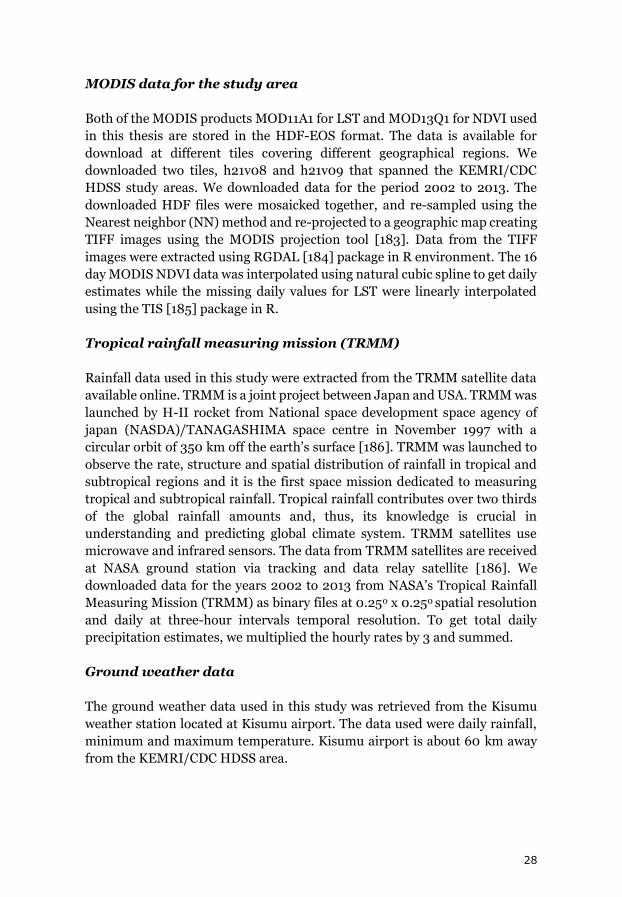
Both of the MODIS products MOD11A1 for LST and MOD13Q1 for NDVI used
in this thesis are stored in the HDF-EOS format. The data is available for
download at different tiles covering different geographical regions. We
downloaded two tiles, h21v08 and h21v09 that spanned the KEMRI/CDC
HDSS study areas. We downloaded data for the period 2002 to 2013. The
downloaded HDF files were mosaicked together, and re-sampled using the
Nearest neighbor (NN) method and re-projected to a geographic map creating
TIFF images using the MODIS projection tool [183]. Data from the TIFF
images were extracted using RGDAL [184] package in R environment. The 16
day MODIS NDVI data was interpolated using natural cubic spline to get daily
estimates while the missing daily values for LST were linearly interpolated
using the TIS [185] package in R.
Tropical rainfall measuring mission (TRMM)
Rainfall data used in this study were extracted from the TRMM satellite data
available online. TRMM is a joint project between Japan and USA. TRMM was
launched by H-II rocket from National space development space agency of
japan (NASDA)/TANAGASHIMA space centre in November 1997 with a
circular orbit of 350 km off the earth’s surface [186]. TRMM was launched to
observe the rate, structure and spatial distribution of rainfall in tropical and
subtropical regions and it is the first space mission dedicated to measuring
tropical and subtropical rainfall. Tropical rainfall contributes over two thirds
of the global rainfall amounts and, thus, its knowledge is crucial in
understanding and predicting global climate system. TRMM satellites use
microwave and infrared sensors. The data from TRMM satellites are received
at NASA ground station via tracking and data relay satellite [186]. We
downloaded data for the years 2002 to 2013 from NASA’s Tropical Rainfall
Measuring Mission (TRMM) as binary files at 0.250 x 0.250 spatial resolution
and daily at three-hour intervals temporal resolution. To get total daily
precipitation estimates, we multiplied the hourly rates by 3 and summed.
Ground weather data
The ground weather data used in this study was retrieved from the Kisumu
weather station located at Kisumu airport. The data used were daily rainfall,
minimum and maximum temperature. Kisumu airport is about 60 km away
from the KEMRI/CDC HDSS area.

29
Statistical analysis
Distributed lag nonlinear models
When assessing the effect of environmental factors on health outcomes, there
is usually, a period preceding observed health effects after the occurrence of
the exposure. This elapsed time between exposure and outcome is called lag
time and can be interpreted as latencies in the ecological & biological systems
of exposure and effect. The lag association will adjust for the timing and
intensity of previous (and other) exposures while estimating the exposure-
response relationship [187].
Distributed lag models (DLM) have been developed to factor in the lag
component in statistical regression modelling handling the fact that lag
variables if included directly in regression models could yield instability in the
statistical estimates due to the high temporal correlation, so called
collinearity. In the DLM framework, the latency processes of exposures on the
response is assumed to be distributed over a period of time [188]. To capture
lag and nonlinear effects, a family of models called distributed lag nonlinear
models (DLNM) have been developed [188]. The DLNM models
simultaneously describes associations along the space of the predictor and in
its lag dimension [188]. DLNMs have been shown to provide robust estimates
of effects compared to DLMs [189]. Time series of ouctome 𝑌𝑡 (𝑡 = 1, … … , 𝑛 ) is often represented by the equation below adapted from [188].
𝑔(𝜇𝑡) = 𝛼 + ∑ 𝑠𝑗
𝐽
𝑗=1
(𝑥𝑡𝑗; 𝛽𝑗 ) + ∑ 𝛾𝑘𝜇𝑡𝑘
𝐾
𝑘=1
Where μt = E(Y) and are Y assumed to arise from exponential family distribution. sj denotes smooth function of xj with parameter βj while μk
represents additional variables included in the model with coefficients γk. In
time series analysis of environmental factors to disease registries, Yt are often
counts assumed to originate from over-dispersed Poisson distribution. In
these models, smooth function of time is often included to capture effects of
confounders [188], and an offset of population at risk can sometimes be
combined with the time trends yielding and incidence model. In models
without an explicit offset the time trends will adjust for population size
changes at the time scale of the time function making parameters
approximating incidence estimates assuming population fluctuations is not
faster than the time trend adjustments.

30
Basis
The relationship between g(μ) and x can be defined by a smooth function s(x)
and included in the model as a sum of linear terms. This is done by choosing
a space of functions called basis containing s [188]. The basis functions
transform x to form basis variables. The assumption on the shape of
relationship between exposure and outcome determines the basis function to
use. Some of the basis functions used include polynomials or spline functions.
DLNM extends the basis definition by introducing a crossbasis function,
which is a bi-dimensional space of functions describing the shape along x and
its distributed lag association [188]. This involves choosing two sets of
functions, which are then combined to form the cross-basis functions [188].
The DLNM models have been implemented in the R environment and its
application is described in detail in Gasparrini et al. [190].
Interpretation of risk
The estimated relative risk contributions in the lag-response curve can be
interpreted using a forward or backward approach [187]. β̂ℓp can be the
relative risk contribution at time 𝑡 + ℓ𝑝 in the future from a unit increase in
exposure x at time t, or the contribution of a unit increase in exposure x occurring at time 𝑡 − ℓ𝑝 in the past to a given risk measured at time t [187].
Attributable Risks can be derived from DLNMs as described by Gasparrini et
al. [191].
General additive models
A generalized additive model replaces the linear part of generalized linear model with smooth functions [192]. The linear part ∑ 𝛽𝑗𝑋𝑗 in the GLM is
replaced by a sum of smooth functions ∑ 𝑠𝑗(𝑋𝑗) called the additive predictor
and thus the name. GAMs are useful in teasing out non-linear covariate
effects. The models allow flexibility on structure of response and covariates by
allowing specification of smooth functions[193]. An example of a univariate
smooth is described in the book by Wood, 𝑦𝑖 = 𝑓(𝑥𝑖) + 𝜖𝑖 adapted from[193].
In this simple model, yi is a response variable, xi is a covariate, f is a smooth
function and 𝜖𝑖 are random variables. The function f can be defined by
choosing a basis assumed to take the form:
𝑓(𝑥) = ∑ 𝑏𝑖𝑞𝑖=1 (𝑥)𝛽𝑖 from [193].
For example, for a 4th order polynomial, the space of polynomials of order 4
contains f. Expanding the 4th order polynomial results into a model of the
structure as evaluated in[193] : 𝑦𝑖 = 𝛽1 + 𝑥𝑖𝛽2 + 𝑥𝑖2𝛽3 + 𝑥𝑖
3𝛽4 + 𝑥𝑖4𝛽5 + 𝜖𝑖 . The

31
basis function can also be represented using cubic spline. Wood in the
book[193] describes cubic splines as a combination of cubic polynomials
joined forming a continuous a curve. The points where the polynomials join
are called knots, which are spaced equally in the range of x and form the basis
dimension. The number of knots determine the degree of smoothing [193].
The value of the smoothing parameter 𝜆 should be chosen to approach the true
function f. There is over smoothing when the value of 𝜆 is too high and under
smoothing when it is too low. One of the methods used is penalized regression
splines to choose 𝜆. In this method , the smoothness is controlled by fixing the
basis dimension at large size and imposing a ‘wiggliness’ penalty [193].
Generalized cross validation is one method used to choose the smoothing
parameter. This is done by leaving each data point successively and fitting
model to remaining data and calculating squared differences between left out
data and their predicted values which are then averaged across all data [193].
A very detailed introduction to GAMs and its implementation in R using the
mgcv package[194] are illustrated in the book by Wood [193].
General additive models for location, scale and shape (GAMLSS)
GAMLSS models provides a flexible framework to model the outcome
distribution called location and its distribution functions such as mean and
standard deviation together [195]. GAMBOOSTLSS [195] provides boosting
algorithm to fit GAMLSS models which are an extension of the GAM [192]
models.
Boosting
GAMBOOSTLSS fits a GAMLSS model by adopting the component wise
gradient boosting. Regression boosting methods emanated from supervised
machine learning discipline and involves iteratively fitting various predictors
using simple regression functions called base learners and then combining the
estimates at each iteration to the additive predictors. In gradient boosting,
base learners are fitted to the negative gradient of the loss function. The
algorithm sweeps through a series of parameter dimensions and
implementing boosting for each dimension and the corresponding additive
predictor updated [195]. A tiny proportion of the fit of the included base
learner called step length is added to a current additive predictor. A typical
step length value is 0.1 [195]. This approach then permits a data driven variable selection controlled by the stopping iteration 𝑚𝑠𝑡𝑜𝑝, which is tuning
parameter that can be determined using cross-validation. The boosting
algorithm for GAMLSS models have been exhaustively explored in the work
by Hosfer [196] and has been implemented in an R-package [195].

32
Dealing with uncertainty in predictions in economic evaluation
Statistical methods have been used to deal with uncertainty in predictions and
how to integrate them in economic health evaluation of early warnings. In
particular stochastic dominance has been suggested in evaluating role of
predictive information [157]. With stochastic dominance, you can rank
outcome distributions based on assumptions on preferences. These
distributions are depicted as cumulative distribution functions which are
conditional on warning or safe signal [157]. These distribution functions are
used to create bounds to assess policy effectiveness [157]. A prediction system
that is able to classify accurately epidemic and non-epidemic episodes would
result in optimal policy of no intervention when no epidemic occurs while with
epidemic the maximum cost changes. Predictive information tends to be more
useful with low probabilities of intervention failure.
Another statistical method involves modelling the prediction error using a
Gaussian distribution having mean equal to the prediction and standard
deviation as the uncertainty. The potential probability of false alarm is taken
as less or greater than the critical threshold. This becomes the probability of
false alarm with no alarm. The tolerable level for response is derived using
cost benefit analysis by minimizing the cost of taking action:
𝑃𝑓𝑎 ≤ 𝛽 =𝐶𝑠𝑎𝑣𝑒
𝐶𝑓𝑎+𝐶𝑠𝑎𝑣𝑒
𝑃𝑚𝑎 < 𝛼 =𝐶𝑓𝑎
𝐶𝑓𝑎+𝐶𝑠𝑎𝑣𝑒
From [131].
Where 𝐶𝑠𝑎𝑣𝑒 are savings due to mitigation actions and 𝐶𝑓𝑎 is the cost of false
alarm. The tolerable levels α and β sum upto 1, which directly exhibits
tradeoffs between the tolerable threshold probabilities for false and missed
alarms.
Sensitivity analysis can be used factor in uncertainty during economic
evaluation. There is one-way, multi-way and probabilistic sensitivity analysis
(PSA) [197]. PSA has advantage over the other methods as it allows us to
consider the joint uncertainty of all the parameters at the same time. PSA
models the uncertainty around a parameter, which is called the second order
uncertainty. The uncertainties are assumed to follow probability distribution
functions. The appropriate probability distribution is chosen depending on
the characteristics of the parameter.

33
Methodologies paper by paper
Paper I
The aim of the Paper I was to model the association between weather
variability and malaria/anemia related mortality in Asembo and Gem areas
taking into account exposure lag response relationship.
Malaria or anemia as causes of death used in this analysis are derived from
physician coded Verbal Autopsy data. We combined malaria and anemia
deaths because anemia deaths in the KEMRI/CDC HDSS frequently have
malaria as the underlying cause [24]. Synoptic weather data derived from the
National Oceanic and atmospheric administration (NOAA) online data portal
was used in this analysis. The meteorological data was monitored as part of
the World Meteorological Association (WMO). We used data for the Kisumu
area, which is approximately 60 km from the KEMRI/CDC HDSS study area.
Daily mean surface temperature and 24-hour cumulative precipitation were
included as predictors in the model.
We used data on malaria and anemia deaths for children under five in Asembo
and Gem areas of the KEMRI/CDC HDSS together with Kisumu rainfall and
temperature data for the period 2003 to 2008 to build the model. The
malaria/anemia mortality data was aggregated weekly from the
KEMRI/HDSS verbal autopsy data. Lag strata of weekly mean temperature
and cumulative rainfall were computed for 1 to 16 weeks. A lag maximum of
16 weeks was chosen taking into account the biological mechanism of malaria
transmission and checking cross correlation coefficients between the malaria
deaths and the lagged weather variables. The lag strata were grouped as lag1-
4, lag5-8, lag9-12 and lag13-16 corresponding to weeks 1 to 4, weeks 5 to 8,
weeks 9 to 12, and weeks 13 to 16, respectively.
The mean, median, minimum, maximum, range and inter-quartile range of
the weather and mortality variables we estimated overall and for each year.
Two percent of the weather data were missing or considered incorrect data
input. The missing observations were linearly imputed based on the closest
temporally present observations before and after the missing observation.
Poisson regression, allowing for over dispersion, was used to model the
expected number of malaria/anemia deaths for each week. A time trend was
included in the model to capture changes in malaria/anemia deaths over time
not explained by weather variability. Auto regressive terms of malaria/anemia
deaths were included in the model to reduce auto-correlation and increase
generalization of model estimates. The autoregressive terms were estimated

34
using lags of 1 to 16 weeks of the malaria/anemia deaths. Both the time trend
and the lagged meteorological variables were modeled using a penalized cubic
regression splines basis. For the latter we allowed 3 degrees of freedom for the
smooth function while we used 2 degrees of freedom per year for the time
trend. The time trend function was set to fixed degrees of freedom, and thus
not penalized.
The model fit was:
𝑙𝑜𝑔[𝐸(𝑌𝑡)] = 𝛽0 + 𝛽1𝐴𝑅[𝑀𝑎𝑙𝑡 ] + ∑ 𝑆[𝑡𝑒𝑚𝑝𝑖 , 𝑑𝑓] + 𝑆[𝑐𝑢𝑚𝑝𝑟𝑐𝑝𝑖 , 𝑑𝑓]
4
𝑖=1
+ 𝑆[𝑡𝑟𝑒𝑛𝑑, 𝑑𝑓]
where 𝑌𝑡~Poisson, 𝛽0 𝑎𝑛𝑑 𝛽1 are parameter estimates; t=time in weeks;
AR(mal)=auto regressive term of malaria/anemia deaths; s=cubic smoothing
function with corresponding degrees of freedom (df), 𝑡𝑒𝑚𝑝𝑖 =weekly mean
temperature at lag strata i, and 𝑐𝑢𝑚𝑝𝑟𝑐𝑝𝑖 =weekly cumulative precipitation at
lag strata i . There were four lag strata corresponding to weeks 1-4, 5-8, 9-12
and 13-16.
We used the Partial Autocorrelation function (PACF) to determine the degrees
of freedom for the smoothing function of the time trend. We chose the degrees
of freedom that minimized the absolute sum of the PACF of the residuals of
the first 10 lags of the model [198]. The degrees of freedom compared were 1,
2, 3, 4 and 5 per year of data in the time series. We used backward elimination
to produce the final model. We used data for the period 2003-2007 to initially
fit the model while 2008 data were used to test model predictions. We
assessed model fit by examining the ACF, PACF, and the cumulative
periodogram of the model residuals. We also checked the normality
assumption of the residuals by examining normal q-q plots and the plot of the
residuals versus the predicted values of the response. The analysis was done
using mgvc package in R [194].
Paper II
The objective Paper II was to study the association between remote sensing
variables: day LST, precipitation and NDVI, on malaria mortality over time in
KEMRI/CDC HDSS areas with a higher resolution to better understand to
what extent weather variability is driving the malaria mortality patterns in the
regions. We used Inter-VA4 derived malaria cause of death data from verbal
autopsies in KEMRI/CDC HDSS for the period 2003 to 2012 for Asembo and
Gem areas while 2008 to 2012 for Karemo region. The daily data was

35
aggregated to weekly temporal resolution for each of the three areas and all
areas combined. The remotely sensed data included in the model were day
LST, precipitation and NDVI. The area specific and all areas daily, LST,
precipitation and NDVI values were then aggregated to weekly temporal
resolution for the study period 2003-2012. For LST and NDVI we computed
weekly mean values while for precipitation we computed weekly totals.
Figure 9. Map showing the mean LST and NDVI for the three study areas in Western Kenya
aggregated for the years 2003-2012 [60].
The delayed effect of day LST, precipitation and NDVI on the weekly malaria
mortality was modelled using Distributed Lag Non-Linear Models (DLNM)
package in R[190]. The DLNM framework allows modelling of non-linear
relationships in dimensions of the predictor as well as its lag. DLNM for each
of the environmental variables was created using a natural cubic spline basis
with 3 degrees of freedom to capture the non-linear effects as well as their lag
dimensions. We modelled lags 0 to 12 weeks for each of the explanatory
variables. Weekly malaria deaths were assumed to follow a quasi-Poisson
process allowing for over-dispersion. In each model, a natural cubic spline
function of time trend allowing one degree of freedom per year of data was
included to capture long-term time trends of malaria mortality based on

36
previous estimation. The model equations used for estimating the effect of
each environmental variable on malaria mortality were:
1 . 𝑙𝑛 (𝐸(𝑌𝑡)) = 𝛽𝑜 + 𝑠(𝑇, 𝑡𝑖𝑚𝑒𝑑𝑓) + 𝑓(𝑋𝑡 , 𝑙𝑎𝑔𝑑𝑓, 𝑣𝑎𝑟𝑑𝑓)+𝛽𝑖𝑋𝑖
2 . 𝑙𝑛 (𝐸(𝑌𝑡)) = 𝛽𝑜 + 𝑠(𝑇, 𝑡𝑖𝑚𝑒𝑑𝑓) + 𝑓(𝑋𝑡 , 𝑙𝑎𝑔𝑑𝑓, 𝑣𝑎𝑟𝑑𝑓)+𝛽𝑖𝑋𝑖 +
𝑠(𝑚𝑜𝑛𝑡ℎ, 𝑣𝑎𝑟𝑑𝑓)
𝐸(𝑌𝑡)~ 𝑃𝑜𝑖𝑠𝑠𝑜𝑛
where 𝐸(𝑌𝑡) is the expected number of malaria deaths in week t. 𝛽𝑜 is the
intercept, 𝑠(𝑇, 𝑡𝑖𝑚𝑒𝑑𝑓) is the smooth function of time with degree of freedom
𝑡𝑖𝑚𝑒𝑑𝑓 , 𝑓(𝑋𝑡 , 𝑙𝑎𝑔𝑑𝑓, 𝑣𝑎𝑟𝑑𝑓) is the crossbasis function of variable t and its lag
dimension with vardf and lagdf degrees of freedom respectively controlling for
the the ith covariate 𝑋𝑖 . For example, the model for precipitation included
LST day and NDVI as linear predictors. We also ran similar models adjusting
explicitly for within year seasonality by including a smooth function of month
with 3 degrees of freedom shown in equation 2 with the additional s (month,
vardf) component. The cross-basis functions of day LST, precipitation and
NDVI were centered at 28 °C, 20 mm and 0.4 respectively for each of the
areas. Centering values were determined by visual examination of the
exposure mortality relationships. For NDVI we chose a centering value of 0.4
based on a study in coastal town of Kilifi in Kenya[199], which showed an
NDVI threshold of 0.3 to 0.4 for increase in malaria incidence. It should be
noted that the choice of centering value does not change the relationship
between outcome and exposure. Relative risks presented are in reference to
these centering points. We also modelled the delayed effect of precipitation on
NDVI and computed cross-correlation coefficients.
We plotted the overall effects of each of the remote sensing variables over the
whole lag period up to 12 weeks, and plotted contour graphs showing both the
lag effect at the whole range of predictor variable. The lag effects were
estimated as 1 °C increase in day LST, 0.1 decrease in NDVI below the
centering value and 10 mm increase in rainfall above the reference value.
Paper III
In paper III, we used remote sensing data and longitudinal malaria morbidity
data from a district hospital in Western Kenya to develop and compare
statistical models to forecast malaria admissions and assess the accuracy of
these models at lead times from one to three months. Specifically, we
compared the performance of boosted general additive model with that of
without boosting.

37
In this study, we used malaria admissions data collected at the Siaya district
hospital for the period 2003-2013. The hospital surveillance data were
complete for this period and collected routinely by the health care workers
employed by the KEMRI/CDC. We extracted the admissions data for children
under five years of age with confirmed P. falciparum malaria. The data were
then aggregated to monthly time scale for each year to create a time series
dataset.
Satellite derived day and night LSTs, NDVI and precipitation data for the
period 2003-2013 were extracted and used as predictors. We averaged day
and night LSTs to get mean LST. In addition to these variables,
Evapotranspiration data from the MODIS product MOD16 available at 8 days
temporal and 1-kilometer spatial resolution was included. These datasets were
aggregated to monthly temporal resolution. We computed monthly totals for
rainfall and monthly averages for the other environmental factors.
A General Additive Modelling framework was employed to build forecast
models for malaria admissions, with smooth functions of environmental
factors at different lead times. Two different general additive models were
developed, one using a boosting algorithm to optimize model fit and the other
with no boosting. The malaria admissions data used in this study exhibited
over-dispersion. In a Poisson distribution, the mean and variance are equal.
Over-dispersion occurs when variance is greater than the mean. To account
for over-dispersion, we assumed negative binomial distribution in both
models.
The general additive model (GAM) without boosting was developed using the
mgcv package in R[194]. The model included a cubic regression spline of time
to adjust for the overall trend in malaria admissions during the study period.
To address the observed within-year seasonality of malaria, we used a cyclic
cubic regression function of month to capture the peaks in malaria
admissions. Mean LST, evapotranspiration (ET) and precipitation were
included as cubic regression splines in the model.
Malaria cases in any given month are likely to be correlated with malaria cases
in preceding months. The number of previously infected individuals
determines the reservoir of infectious mosquitoes, which in turn affects the
current population of infected individuals. To control for this autocorrelation,
we included previous malaria cases as autoregressive terms (AR) in the
models for each lead time. Previous studies in this HDSS area [21] and in
Burundi [200] included a 1-month AR term to adjust for autocorrelation. We
also included a simple random effect spline function of month. Smoothing
degrees of freedom were optimally determined using general cross validation.

38
To assess different prediction lead times, three separate models were
developed with 1-month, 2-month and 3-month lead times. To attain a 1-
month lead time we took a lag of one month of environmental factors and
malaria cases and for the 2-month and 3-month lead times we took a lag of
two and three months, respectively.
The model equations were:
𝐿𝑜𝑔(𝑌𝑡) = 𝑠(𝑡𝑖𝑚𝑒) + 𝑠(𝑚𝑜𝑛𝑡ℎ, 𝑏𝑠 = "cc") + 𝑠(𝑙𝑆𝑇𝑡−1 ) + 𝑠(𝑃𝑟𝑒𝑐𝑖𝑝𝑖𝑡𝑎𝑡𝑖𝑜𝑛𝑡−1 )
+ 𝑠(𝐸𝑇𝑡−1 ) + 𝑠(𝑚𝑜𝑛𝑡ℎ, 𝑏𝑠 = "re") + 𝑠(𝑀𝐴𝐿𝑡−1 )
𝐿𝑜𝑔(𝑌𝑡) = 𝑠(𝑡𝑖𝑚𝑒) + 𝑠(𝑚𝑜𝑛𝑡ℎ, 𝑏𝑠 = "cc") + 𝑠(𝑙𝑆𝑇𝑡−2 ) + 𝑠(𝑃𝑟𝑒𝑐𝑖𝑝𝑖𝑡𝑎𝑡𝑖𝑜𝑛𝑡−2)
+ 𝑠(𝐸𝑇𝑡−2) + 𝑠(𝑚𝑜𝑛𝑡ℎ, 𝑏𝑠 = "re") + 𝑠(𝑀𝐴𝐿𝑡−2 )
𝐿𝑜𝑔(𝑌𝑡) = 𝑠(𝑡𝑖𝑚𝑒) + 𝑠(𝑚𝑜𝑛𝑡ℎ, 𝑏𝑠 = "cc") + 𝑠(𝑙𝑆𝑇𝑡−3 ) + 𝑠(𝑃𝑟𝑒𝑐𝑖𝑝𝑖𝑡𝑎𝑡𝑖𝑜𝑛𝑡−3 )
+ 𝑠(𝐸𝑇𝑡−3 ) + 𝑠(𝑚𝑜𝑛𝑡ℎ, 𝑏𝑠 = "re") + 𝑠(𝑀𝐴𝐿𝑡−3 )
𝑌𝑡~Negative Binomial
where s is a smoothing spline; bs=”cc” is the cyclic cubic regression spline
basis function of month to control for seasonality; bs=”re” is the random effect
spline basis; and MAL represents the autoregressive malaria cases. The other
spline functions are cubic regression splines. Models 1, 2, and 3 correspond to
1-month, 2-month and 3-month prediction lead times, respectively.
General Additive Model with boosting (GAMBOOST)
The general additive model with boosting was developed using gamBoostlss
[195, 196] package in R. Similar to the GAM model, we used smooth base
learners of time, Mean LST, ET, precipitation and previous malaria cases as
AR terms for each lead time. We also include a random base learner for month
and a cyclic base learner for month. The equations for each model are as
follows:
𝐿𝑜𝑔(𝑌𝑡) = 𝑏𝑏𝑠(𝑡𝑖𝑚𝑒) + 𝑏𝑏𝑠(𝑚𝑜𝑛𝑡ℎ, 𝑐𝑦𝑐𝑙𝑖𝑐 = 𝑇) + 𝑏𝑏𝑠(𝑙𝑆𝑇𝑡−1 )
+ 𝑏𝑏𝑠(𝑃𝑟𝑒𝑐𝑖𝑝𝑖𝑡𝑎𝑡𝑖𝑜𝑛𝑡−1 ) + 𝑏𝑠𝑠(𝐸𝑇𝑡−1 ) + 𝑏𝑟𝑎𝑛𝑑𝑜𝑚(𝑚𝑜𝑛𝑡ℎ)
+ 𝑏𝑏𝑠(𝑀𝐴𝐿𝑡−1 )
𝐿𝑜𝑔(𝑌𝑡) = 𝑏𝑏𝑠(𝑡𝑖𝑚𝑒) + 𝑏𝑏𝑠(𝑚𝑜𝑛𝑡ℎ, 𝑐𝑦𝑐𝑙𝑖𝑐 = 𝑇) + 𝑏𝑏𝑠(𝑙𝑆𝑇𝑡−2)
+ 𝑏𝑏𝑠(𝑃𝑟𝑒𝑐𝑖𝑝𝑖𝑡𝑎𝑡𝑖𝑜𝑛𝑡−2 ) + 𝑏𝑠𝑠(𝐸𝑇𝑡−2 ) + 𝑏𝑟𝑎𝑛𝑑𝑜𝑚(𝑚𝑜𝑛𝑡ℎ)
+ 𝑏𝑏𝑠(𝑀𝐴𝐿𝑡−2 )

39
𝐿𝑜𝑔(𝑌𝑡) = 𝑏𝑏𝑠(𝑡𝑖𝑚𝑒) + 𝑏𝑏𝑠(𝑚𝑜𝑛𝑡ℎ, 𝑐𝑦𝑐𝑙𝑖𝑐 = 𝑇) + 𝑏𝑏𝑠(𝑙𝑆𝑇𝑡−3 )
+ 𝑏𝑏𝑠(𝑃𝑟𝑒𝑐𝑖𝑝𝑖𝑡𝑎𝑡𝑖𝑜𝑛𝑡−3) + 𝑏𝑠𝑠(𝐸𝑇𝑡−3 ) + 𝑏𝑟𝑎𝑛𝑑𝑜𝑚(𝑚𝑜𝑛𝑡ℎ)
+ 𝑏𝑏𝑠(𝑀𝐴𝐿𝑡−3 )
𝑌𝑡~Negative Binomial
Where bbs is the smooth base learner. The smooth base learner for month is
set to be cyclic to control for seasonality. Random is the random base learner
for month. MAL represents the autoregressive malaria cases. Models 1, 2, and
3 correspond to 1-month, 2-month and 3-month prediction lead times,
respectively.
Model validation
To get an optimal number of boosting iterations we performed k-fold cross
validation on the training dataset. K-fold cross validation involves partitioning
the training data into k subsets. In each run, one subset is held for validation
while the remaining k-1 subsets are used for model fitting. The number of
iterations giving the lowest prediction in the k out of sample set is chosen.
We performed 5- fold validation with 1,000 initial iterations with 0·01 step to
get the number of boosting iterations for the gamboostlss model. To assess
the predictive ability of the models, we split the data into training and testing
datasets. The time series for the period 2003-2012 was used for model
training while the 2013-time series for model testing. R-squared statistic, root
mean squared error (RMSE), normalized mean squared error (NMSE), mean
absolute error (MAE) and normalized mean absolute error (NMAE) were used
for model comparison. The equations for these measures are given below:
𝑀𝐴𝐸 =1
𝑛∑ |𝑒𝑖|
𝑛
𝑖=1
𝑅𝑀𝑆𝐸 = √1
𝑛∑ 𝑒𝑖
2
𝑛
𝑖=1
𝑁𝑀𝑆𝐸 =1
�̅�√
1
𝑛∑ 𝑒𝑖
2,𝑛𝑖=1 where y̅ is the scaling factor
Where 𝑒𝑖 = 𝑓𝑖 − 𝑦𝑖 , where 𝑓𝑖 𝑖s the prediction and 𝑦𝑖 the observed value.

40
The NMAE is scaled using the lowest and the highest values in the series. The
different measures are relevant when there are different scales [201]; in this
case mean malaria admissions differ between test and training periods. These
measures have been explained in more detail in Shcherbakov et al [201]. We
included the normalized measures to be able to assess prediction accuracy
between training and test periods [201].All analysis was done using R
statistical software [202]. The DMwR [203] package was used to produce the
forecast accuracy statistics.
Paper IV
In this paper, we developed a framework to assess the economic value of an
operational early warning system to aid decision making within the public
health sector. The framework can be used to estimate the costs and benefits
associated with the use of early warning information generated by an EWS.
We proposed two different approaches on how forecasting can be integrated
into health systems for disease planning and response. The first method
assumes an early warning system that can issue alerts on high transmission
events based on disease thresholds while the other assumes a system that
churns out absolute disease forecasts.
Decision-analytical modelling framework [204, 205] was the quantitative
approach proposed for assessing costs and benefits incorporating the accuracy
of disease forecasts. We defined economic value as net benefit, which is total
benefits minus total costs. A positive net benefit is a general signal to policy
makers that response measures are economically feasible. In principle, the
probability of a false warning in the case where threshold is used or prediction
errors decreases as the lead time decreases. However, shorter lead times may
mean reduced cost savings due to reduced amount of averted disease burden.
The proposed framework makes it explicit the trade-offs between forecast
accuracy, cost of response, and potential cost savings as a function of lead
time.

41
Results
Distribution of malaria health outcomes
Mortality
Between 2003 and 2008, 1768 malaria deaths occurred among children under
the age of five in Asembo and Gem areas of the KEMRI/CDC HDSS. Physician
coding was employed to derive cause of death from VA questionnaires. There
was an average of 5.6 malaria child deaths in a week. Between 2003 and 2006,
there was a steady decline in the number of child deaths due to malaria, but
the trend reversed in 2008. The highest number of deaths (386) was observed
in 2004 with 2008 following closely at 368 deaths. A general seasonal pattern
was observed and is captured in Figure 11. The highest average monthly
number of admissions occurred in May while October registered the least
number of admissions. The number of malaria mortality events derived using
probabilistic INTERVA method for VA between 2003 and 2012 in all the three
HDSS areas was 3,809. The highest number total malaria deaths in a year was
696 observed in 2008. The least number of deaths was observed in 2007 with
210 malaria deaths. The average weekly malaria deaths were 2 and weekly
average deaths ranged from 0 to 20 deaths.
Malaria admissions
There were 8,476 confirmed P. falciparum malaria admissions for children
under the age of five at Siaya district hospital between 2003 and 2013 with a
mean of 64 admissions due to malaria per month. The years 2003, 2004 and
2008 saw the highest number of admissions with 1258, 1468 and 1249
respectively. There have been huge declines in admissions over the years with
the recent years registering very low number at 197 and 166 admissions for the
years 2012 and 2013.
Distribution of weather variables
Temperature
From the Kisumu airport data, the mean temperature for the entire period
2003-2008 was 23.6C and ranging from a minimum of 20.7C to a maximum
of 27.6C. The hottest years recorded was 2005 with a mean temperature of
24.1C. The maximum temperature ranged from 25.4 to 35.5C with a mean
of 29.5C in the same period while the minimum temperature varied between
14.4 and 20.8C. For the period 2003 to 2012, the day land surface

42
temperature from MODIS for the entire KEMRI/HDSS area ranged from
19.9C to 39.1C with a mean of 29.7C. In terms of regional differences in day
LST, the mean day LST for Asembo, Gem and Karemo for the entire study
period 2003-2012 was 30.5C, 29.1C and 29.4C respectively. The time series
of the distribution of temperature in Kisumu is captured in Figure 10.
Precipitation
The rainfall data summaries for Kisumu show that the average total weekly
rainfall amounts are 23 mm and range between 0-232 mm. The total rainfall
observed between 2003 and 2008 in Kisumu was 7,446 mm. The wettest year
was 2006 with a total rainfall of 1,548 mm and the driest year was 2005 with
total rainfall of 969 mm with a mean of 18.3 mm per week (refer to Figure 10).
The average total precipitation registered in the three KEMRI/CDC HDSS
areas for the whole period 2003 to 2012 was 15,609 mm with a mean weekly
precipitation of 29.5 mm with a maximum of 196 mm. Similar to Kisumu the
wettest year in the HDSS areas was 2006 with a total rainfall of 2,172 mm and
2005 as the driest year with total rainfall of 1,343 mm. Comparing the three
HDSS areas, Gem received the highest amount of rainfall in the period 2003
to 2012 with total rainfall of 16,541 mm followed by Karemo at 15,683 mm and
finally Asembo with 14,602 mm of rainfall. The average weekly total rainfall
in Asembo was 27.6 mm, 31.2 mm in Gem and 29.6 mm in Karemo.
Normalized difference vegetation index (NDVI)
For all the three HDSS areas, the weekly mean NDVI was 0.61 and ranged
from 0.3 to 0.77 in the period 2003 to 2012. The highest mean NDVI was in
2007 at 0.65 while the least mean NDVI was in 2009 with a value of 0.58. Gem
region is the greenest with a mean NDVI of 0.64 followed by Karemo with an
NDVI of 0.62 and the least green being Asembo with mean NDVI of 0.58. In
2007, the greenest year, all the three areas registered mean NDVI values above
0.6. The distribution is displayed in Figure 10.

43
Figure 10. Time of series plot of weather data (mean temperature, min temperature,
maximum temperature and precipitation(KIS)) from Kisumu airport 2003-2008 and remote
sensing 2003-2012. Day LST, precipitation (TRMM) and NDVI are satellite derived and the rest
from the airport. The plot also describes malaria deaths by INTERVA and physician coding
cause of death derivation.

44
Figure 11. Weekly seasonal distribution of malaria deaths and remote sensing derived day LST,
NDVI and precipitation in three endemic areas Asembo, Gem and Karemo, Western Kenya
aggregated for the period 2003-2012.
Seasonality of malaria deaths and environmental variables
Figure 11. Shows weekly mean malaria mortality plotted against weekly
summaries of remote sensing variables. We can see clearly that peaks in
malaria mortality follows peaks of environmental factors with different lag
phase shifts. Figure 12 shows the within year weekly distribution of malaria
mortality, day LST, precipitation and NDVI contrasted by area while Figure
13 shows monthly distribution of malaria admissions. We observe two peaks
in malaria transmission corresponding to the bimodal peaks also observed for
the environmental variables. Malaria mortality increases gradually from
about week 12 and peaks at week 22 and another less peak occurs towards the
end of the year starting from week 42 and peaking at week 48. The peak in day
LST occurs during the weeks of February. The increase in precipitation starts
from week 9 and peaks at week 19 and again start at week 39. The two peaks
for NDVI are at 19 and 46 weeks respectively.

45
Figure 12. Weekly seasonal distribution of malaria deaths and remote sensing derived day LST,
NDVI and precipitation by KEMRI/CDC HDSS area 2003-2012.
Figure 13. Average monthly admissions of under 5 P falciparum malaria cases at Siaya district
hospital 2003 -2013.

46
Relationship between environmental factors and malaria mortality
Mean temperature
Figure 14 shows association between weekly malaria mortality in Asembo and
Gem and mean weekly temperature from Kisumu airport at different lag
strata. There is no significant relationship for lag strata derived from week 1
to week 8. The exposure lag response relationship changes for longer lags from
9 weeks. At lag strata of 9-12 weeks, the relative risk is significant at
temperatures of above 25 and increases almost linearly. The lag effect is
stronger for mean temperatures above 25C at lag 13-16 weeks.
Figure 14. Relative risks of Malaria/Anemia mortality in children under five years with weekly
mean temperature (Tmp) at different lag strata [59].

47
Day land surface temperature
Figure 16A shows the overall effect of day LST on weekly malaria mortality in
Asembo, Gem and Karemo areas combined over the whole lag period. The
effect of day LST is significant for temperatures above 34C compared to the
reference of 29C. For example, at day LST of 36.9C the relative risk of
malaria mortality is 2.19 [1.29-3.74]. When we compare the overall effect by
study area we observe some differences as displayed in Figure 17. In Asembo
Figure 17A, there is no significant LST value across the range of LST. However,
in Gem, Figure 17D; there is a significant risk association for day LST below
27C and above 34C. For example, at 24.9C the RR is 1.66 [1.02-2.73] and
for LST of 36.9C the RR is 3.23 [1.59-6.56] resulting in a U-shape typical of
temperature mortality relationships. In karemo Figure 17G the effect is
significant for lower temperature e.g. at LST of 25.7 the RR is 2.06 [1.26-3.37].
Delayed effect of day LST
Figure 16D shows the exposure lag response relationship between day LST
and malaria mortality in all the three areas combined in a contour plot. We
observe shorter lag positive significant effect at lower day LST values below
29C and longer lag effect for LST values in the upper percentiles. Figure 18
displays this lag pattern for specific weekly day LST values. In Figure 18, we
see that for weekly LST value of 27.3C, the lag effect is significant from lag
week 0 to lag week 4. At lag week 4, the RR is 1.0086 [1.003-1.014]. At higher
weekly day LST of 36.9C the lags are significant from lag week 7 up to lag
week 12 with highest relative risk at week 12 amounting to 1.23 [1.09-1.4].
Precipitation
Figure 15 shows the exposure-response relationship as lag strata between
weekly cumulative precipitation from Kisumu airport and under five malaria
mortality in Asembo and Gem for the period 2003 to 2008. There is no
significant effect at combined lags 1 to 4 weeks. There is relatively increased
risk for weekly total rainfall between 120 mm and 180 mm in lag strata 5 to 8
weeks. However, the relationship is stronger for lags 9 to 12 weeks with linear
increase in risk with increasing weekly total rainfall. With higher lag 13-16
weeks the risk increase from 80 mm and then starts to drop at 200 mm
resulting in an inverted U-shaped relationship.
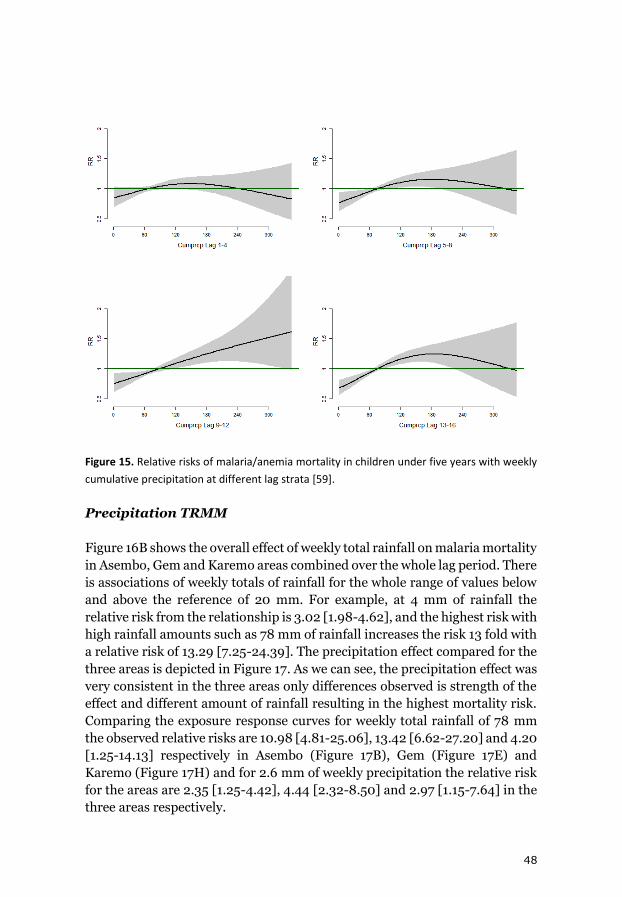
48
Figure 15. Relative risks of malaria/anemia mortality in children under five years with weekly
cumulative precipitation at different lag strata [59].
Precipitation TRMM
Figure 16B shows the overall effect of weekly total rainfall on malaria mortality
in Asembo, Gem and Karemo areas combined over the whole lag period. There
is associations of weekly totals of rainfall for the whole range of values below
and above the reference of 20 mm. For example, at 4 mm of rainfall the
relative risk from the relationship is 3.02 [1.98-4.62], and the highest risk with
high rainfall amounts such as 78 mm of rainfall increases the risk 13 fold with
a relative risk of 13.29 [7.25-24.39]. The precipitation effect compared for the
three areas is depicted in Figure 17. As we can see, the precipitation effect was
very consistent in the three areas only differences observed is strength of the
effect and different amount of rainfall resulting in the highest mortality risk.
Comparing the exposure response curves for weekly total rainfall of 78 mm
the observed relative risks are 10.98 [4.81-25.06], 13.42 [6.62-27.20] and 4.20
[1.25-14.13] respectively in Asembo (Figure 17B), Gem (Figure 17E) and
Karemo (Figure 17H) and for 2.6 mm of weekly precipitation the relative risk
for the areas are 2.35 [1.25-4.42], 4.44 [2.32-8.50] and 2.97 [1.15-7.64] in the
three areas respectively.

49
Delayed effect of precipitation
The contour plot in Figure 16E shows the lag patterns at different values across
the range of weekly total rainfall. For weeks with total precipitation below 20
mm, the lag effect is delayed significant increased risk from week 5 and for
weeks with higher cumulative rainfall, the lag effects are immediate starting
at week 0. At lag week 1 and 8, the relative risk for mortality are 1.18 [1.08-
1.28] and 1.30 [1.21-1.39] for 78 mm of rainfall. At 9 mm of weekly rainfall the
first significant lag is week 6 with an RR of 1.06 [1.001-1.11] and the risk
increase for each subsequent lag with highest risk at lag 12 with RR of 1.11
[1.06-1.15]. This lag relationship for precipitation is captured in Figure 18.
Normalized difference vegetation index (NDVI)
Figure 16C shows the overall effect of average weekly vegetation index on
malaria mortality in Asembo, Gem and Karemo areas combined over the
whole lag period. The risk is higher for weeks with vegetation indices below
0.4, which is the reference value. For example, at NDVI values 0.3 and 0.2 the
relative risks for mortality increases by 3.10 [1.73-5.56] and 9.62 [2.99-30.94]
respectively. The risk for malaria death is significantly lowered with higher
NDVI values, e.g. for weeks with average NDVI of 0.62 the relative risk is 0.28
[0.16-0.48]. Exploring the association considering area offers some
differences between the study areas. At weekly average of NDVI of 0.3 the RR
risks in Asembo (Figure 17C), Gem (Figure 17F), are 2.18 [1.06-4.51] and 3.40
[1.64-7.05], but not significant in Karemo (Figure 17I) with a relative risk of
1.45 [0.44-4.83].
Delayed effect of NDVI
The temporal relationship between NDVI and malaria mortality is displayed
as a contour plot in Figure 16F.From the contour plot, we see that with NDVI
below 0.4, the lag effect has a strong effect at short lags, while at high indices
the effect is more delayed and protective. Figure 18 shows risk of malaria
deaths at different lag weeks for specific values of NDVI. For weeks with
average NDVI of 0.3, the lag effect is stronger at lag 0 and significant up to
week 5 with a decreasing trend. For example, at lag week 1 the RR is 1.16 [1.05-
1.28] and 1.07 [1.004-1.15] at lag week 5. Very vegetation green weeks with
NDVI of 0.7 reduces the risk of malaria death at longer lags, e.g. a RR of 0.89
[0.82-0.97] for a lag of 10 weeks.

50
Figure 16. The overall risk of day Land Surface Temperature (LST oC) (A), precipitation (mm)
(B), and Normalized Difference Vegetation Index (NDVI) (C) on malaria mortality for all areas
for the whole lag period. The bold lines indicate relative risks while the shaded regions display
the 95% Confidence intervals. D, E and F are the lag patterns for day LST, precipitation and
NDVI respectively at the whole range of predictors [60].
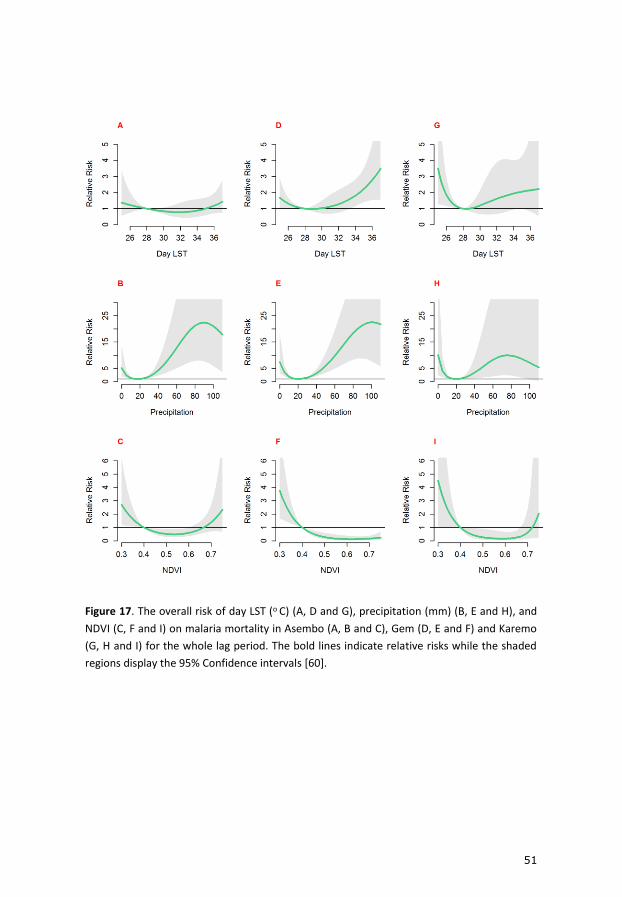
51
Figure 17. The overall risk of day LST (o C) (A, D and G), precipitation (mm) (B, E and H), and
NDVI (C, F and I) on malaria mortality in Asembo (A, B and C), Gem (D, E and F) and Karemo
(G, H and I) for the whole lag period. The bold lines indicate relative risks while the shaded
regions display the 95% Confidence intervals [60].
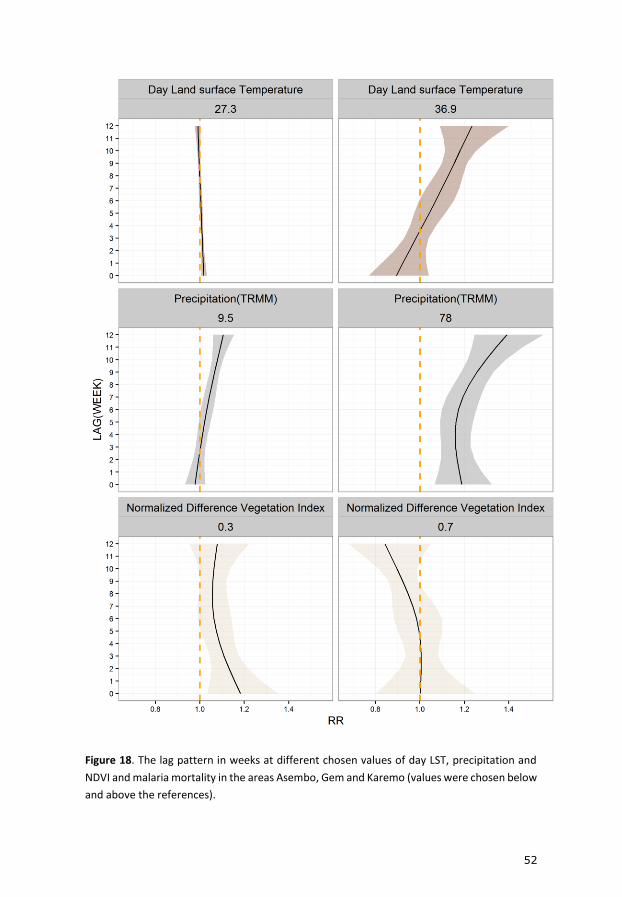
52
Figure 18. The lag pattern in weeks at different chosen values of day LST, precipitation and
NDVI and malaria mortality in the areas Asembo, Gem and Karemo (values were chosen below
and above the references).

53
Prediction of monthly malaria admissions
Table 1 shows various model prediction metrics comparing GAM modelling
approach and the GAMBOOST approach at different prediction lead times
ranging from 1 to 3 months in forecasting malaria admissions among children
at the Siaya district hospital. The GAM model with boosting performed better
at all the prediction lead times. The most accurate lead time was one month
in all the models. For the 1-month lead time, the GAMBOOST model explained
80% of the variation in the data during training period 2003-2012 and 71% of
the variation in the forecasting of 2013 malaria admissions. The GAM model
at 1-month lead time captures 77% of the variation during training, but was
not able to replicate this during forecasting of the 2013 cases. With increasing
lead times, the predictive capability of both models decreased. For example,
the GAMBOOST model only accounted for 50% of the variation at the 3-
month lag internal prediction.
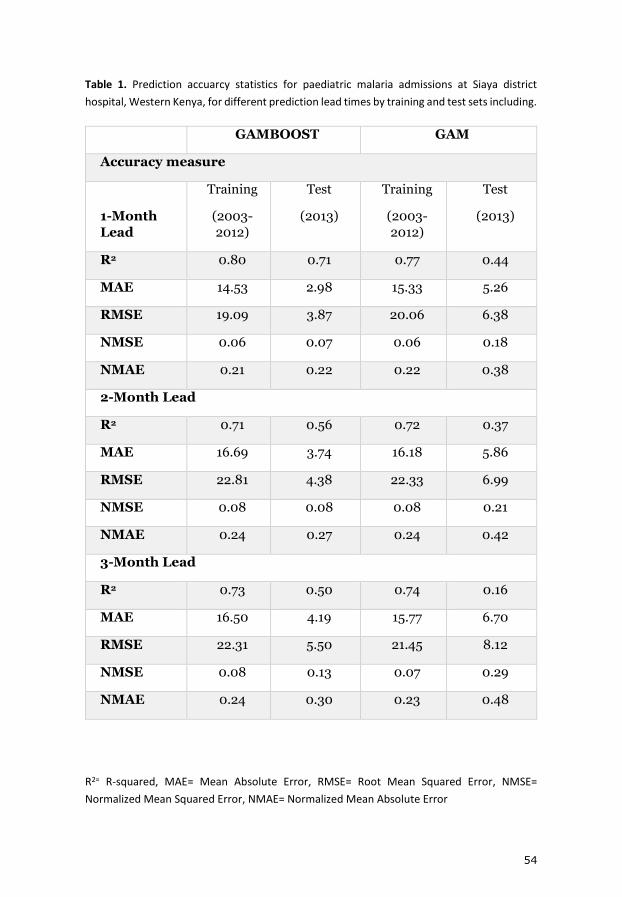
54
Table 1. Prediction accuarcy statistics for paediatric malaria admissions at Siaya district
hospital, Western Kenya, for different prediction lead times by training and test sets including.
GAMBOOST GAM
Accuracy measure
1-Month
Lead
Training
(2003-
2012)
Test
(2013)
Training
(2003-
2012)
Test
(2013)
R2 0.80 0.71 0.77 0.44
MAE 14.53 2.98 15.33 5.26
RMSE 19.09 3.87 20.06 6.38
NMSE 0.06 0.07 0.06 0.18
NMAE 0.21 0.22 0.22 0.38
2-Month Lead
R2 0.71 0.56 0.72 0.37
MAE 16.69 3.74 16.18 5.86
RMSE 22.81 4.38 22.33 6.99
NMSE 0.08 0.08 0.08 0.21
NMAE 0.24 0.27 0.24 0.42
3-Month Lead
R2 0.73 0.50 0.74 0.16
MAE 16.50 4.19 15.77 6.70
RMSE 22.31 5.50 21.45 8.12
NMSE 0.08 0.13 0.07 0.29
NMAE 0.24 0.30 0.23 0.48
R2= R-squared, MAE= Mean Absolute Error, RMSE= Root Mean Squared Error, NMSE=
Normalized Mean Squared Error, NMAE= Normalized Mean Absolute Error

55
Figure 19. Observed and predicted paediatric malaria admissions at Siaya district hospital,
Western Kenya by prediction lead time for the period 2003-2013 from the GAMBOOST model.
The black line displays observed malaria admissions, the grey line predicted values during the
training period 2003-2012, and the red line the 2013 forecasted values. The red vertical dotted
line marks the beginning of the test period.
The normalized mean squared error (NMSE) is very comparable in
GAMBOOST 1-month lead time with 0.06 and 0.07 during model training and
testing periods respectively. Thus, the model validation reinforce the
GAMBOOST algorithm to provide better predictive power comparing to the
GAM model. Figure 19 shows a graphical, comparison between observed
malaria admissions data and the model predictions. The GAMBOOST model
capture closely the yearly seasonal pattern and the peak closely for the 1-
month lead time model.

56
A framework for economic evaluation of early warning and response system benefits
Options to health system integration
This framework outlines two different approaches on how forecasting can be
integrated into the health systems: 1. We assume an existing operational early
warning system capable of issuing forecast of high/epidemic events several
months ahead at discrete intervals. In this situation we predict the probability
of exceeding the pre-defined threshold, e.g. P(�̂�𝑡>threshold) where �̂�is the
number of cases or incidence (approach 1); or, 2 we assume integration of
forecasting within existing surveillance systems as a routine activity and
predict the number of cases, or incidence, �̂�𝑡 (approach 2). In the situation the
health outcome, �̂�𝑡, is a number of disease counts, we can estimate the number
of cases that require hospitalization, the number of cases that progress to
severe disease and the number of deaths. On the cost side, both methods
include the actual costs of response strategies at different lead times, but the
first approach also includes the costs of false (positive or negative) warnings
given the forecast accuracy. On the benefits side, we include the valuation of
averted health outcomes (averted disease burden in terms of uncomplicated
and severe cases) in monetary units given the level of uncertainty associated
with disease forecasts and the effectiveness of response strategies at different
lead times.
Uncertainty of forecasts
There are a few key characteristics of a disease forecast. An important one is
that with increasing forecasting lead time, i.e. the time for issuing of forecast
to the realization of forecast, the accuracy of detecting epidemic intensity, is
expected to diminish. For the forecasted entity �̂�𝑡 (approach 2), we estimate
the validity of the forecast by measuring the mean square error (MSE) of the
prediction to the true occurrence of the disease. In approach 2, where the
predicted entity is P(�̂�𝑡>threshold), we estimate the accuracy of detecting this
anomalies beyond the threshold by the forecast as a probability.
Response interventions
For forecast of disease frequencies, or epidemics, becoming useful within the
health system, they need to be aligned to a set of response strategies. The
longer lead time is considered an attractive feature in preparing and
responding to future disease events, where possibilities are given to extend the
routine surveillance activities and to make them more rigorous. The lead time
can also open up for new possibilities of intervening and preventing, or

57
limiting the impact, of outbreaks, and potentially make the effect of response
activities stronger. In this research, we assume decision makers have already
a set of interventions known to be effective in preventing disease, of which
they also know how much time they need in the implementation to reach this
effect, so that they can synchronize this with a response at a specific lead time.
We symbolize the relationship between intervention effectiveness and lead
time using, 𝑒𝑖 where e denotes the effectiveness of the specific intervention, or
for a combination set of interventions (e.g. a response program), and where i
denotes the lead time.
Costs of disease management, information management, and
response programs
The cost components include the cost of response programs for each
intervention, or combinations of interventions, e.g. the cost of running a
response program at a specific lead time and the cost of running the
information management system, which we assume constant. We denote CRi
as the cost of the response at lead time i, the while the cost of information
management is denoted CI. We assume that the costs of interventions in the
response program is known, and ultimately, for each lead time decision
makers have identified a set of response action to take given their operational
capacity and estimated how much the cost is for running the program to
achieve the desired effect. We also assume the cost of running the forecasts
and dissemination information, CI, is known.
We further consider the direct medical costs of outpatient and inpatient
treatment of cases in the formal health sector, and denote this with CT. Thus,
we consider the economic burden of disease will be measured using the cost
of treatment, but the cost of hospitalizations and management of severe
disease can be used. CT can be used as an entity providing an economic
valuation of each specific averted disease case from the response activities. We
assume that models estimating the probability of epidemics still can provide
estimates of disease cases and hospitalizations associated with the predicted
event. In the latter case, the disease frequency estimates are considered the
excess numbers beyond the specified acceptance threshold.
Net benefit of response programs
To assess the economic value of a response program, we formulate an
equation for estimating the net benefit of responding to the forecasted disease
frequency or epidemic. We define the net benefit as 𝑁𝐵𝑡,𝑖, where t denoted
time and i denotes lead time. We set up two different ways to quantify the net
benefits, one for the situation where the threshold is pre-defined and we

58
estimate the outbreak probability and excess morbidity/mortality (approach
1), the other where we forecast the morbidity and evaluate the net benefit of
responding (approach 2). In situations where the threshold for epidemics is
defined and �̂�𝑡 predicts excess beyond this threshold, we defined 𝑁𝐵𝑡,𝑖 as
function of:
𝑁𝐵𝑡,𝑖 = (�̂�𝑡,𝑖 ∗ 𝑒𝑖 ∗ 𝐶𝑇) − (𝐶𝐼 + 𝐶𝑅𝑖 + (𝑃𝑓𝑎,𝑖 ∗ 𝐶𝑅𝑖)) (1)
Here �̂�𝑡,𝑖 ∗ 𝑒𝑖 represents cases averted due to the response at lead time i, and
𝑃𝑓𝑎,𝑖 ∗ 𝐶𝑅𝑖 is the cost of false alarm at lead time i. Thus, the cost of intervening
is weighted using the probability of false alarm. To this, we add the running
costs, CI, and the value of each averted case, CT.
In situations where the threshold for epidemics is not defined and �̂�𝑡 predicts
total cases, we define 𝑁𝐵𝑡,𝑖 as:
𝑁𝐵𝑡,𝑖 = (�̂�𝑡,𝑖 ∗ 𝑒𝑖 ∗ 𝐶𝑇) − (𝐶𝐼 + 𝐶𝑅𝑖) (2)
Here, there is no false-alarm penalization, but the �̂�𝑡,𝑖 will instead be including
the MSE of forecasted to observed differences, which is going to be larger if
the forecasts are “missing” epidemics. The other parameters are similar to
those described in formula (1).
Simulation of uncertainty
The parameters used in the formula for computing net benefits have
uncertainty around them. Sensitivity analysis can be used to show the changes
in net benefit as the parameters are varied. Due many parameters with
uncertainty, we propose to use probability sensitivity analysis (PSA) to model
the uncertainty around the parameters. The uncertainties are assumed to
follow probability distribution functions. The uncertainty around forecast
prediction, intervention effectiveness, and probability of false alarms can be
assumed to follow a Poisson/binomial, Asymptomatic normal and binomial
distributions, respectively, while the uncertainty around costs may be
assumed to follow lognormal or uniform distributions. Markov Chain Monte
Carlo (MCMC) simulation can then be used to draw several samples
randomly, for example 10,000 samples, based on the probability distribution
of the model parameters in the formulas (1) and (2) resulting in a simulated
estimated of the distribution of 𝑁𝐵𝑡,𝑖. The estimated probability distribution
function of 𝑁𝐵𝑡,𝑖 can be computed at each time t and for each lead time i. We
illustrate a hypothetical distribution of 𝑁𝐵𝑡,𝑖 in Figure 20.
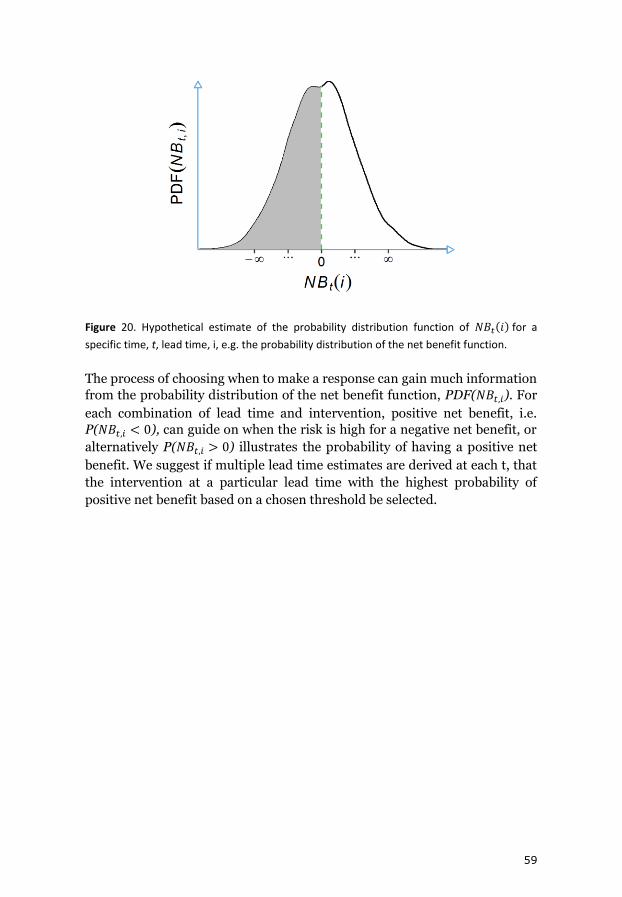
59
Figure 20. Hypothetical estimate of the probability distribution function of 𝑁𝐵𝑡(𝑖) for a
specific time, t, lead time, i, e.g. the probability distribution of the net benefit function.
The process of choosing when to make a response can gain much information
from the probability distribution of the net benefit function, PDF(𝑁𝐵𝑡,𝑖). For
each combination of lead time and intervention, positive net benefit, i.e.
P(𝑁𝐵𝑡,𝑖 < 0), can guide on when the risk is high for a negative net benefit, or
alternatively P(𝑁𝐵𝑡,𝑖 > 0) illustrates the probability of having a positive net
benefit. We suggest if multiple lead time estimates are derived at each t, that
the intervention at a particular lead time with the highest probability of
positive net benefit based on a chosen threshold be selected.

60
Discussion
In order to develop effective malaria early warning programs, the need to
quantify the relationship between environmental factors such as rainfall and
temperature with malaria burden becomes apparent. The relationship
between these factors in the environment and malaria is expected to follow
biological progression with varying temporal delay between exposure and the
event. This temporal dimension provides useful information that can guide
the timing of interventions to curb the devastating effects such in epidemic
situations. In this thesis, we have made effort to answer specific questions
regarding the presence of interacting weather factors, remote sensing proxies
for changes in environmental conditions and malaria mortality in rural
western Kenya using state of the art modelling techniques and used the
information to develop predictive models that can be used in early warning
situations.
In the first objective, we explored the lagged relationship between weekly total
rainfall, weekly mean temperature and malaria mortality for Asembo and Gem
areas of the KEMRI/CDC HDSS combined using general additive modelling
framework that allowed us to model the weather covariates as smooth
functions. For example, we have shown that the effect of mean temperature
on malaria mortality is much delayed starting to manifest from week 9 with
linear increase with average temperatures above 25oC, and a J-shaped
relationship with lags greater than 13 weeks. These results echo with lag
patterns identified by Chirebvu et al in Botswana where they found a positive
correlation between malaria transmission and maximum temperature with a
lag of 2 months and a lag of one month for mean temperature [206]. However,
in this study they assume, linear relationship between temperature and
malaria transmission. A recent study that employed general additive mixed
model to tease out the relationship between air temperature and malaria
incidence in Uganda and Rwanda using spline functions, reported positive
relationship between air temperature with malaria incidence with a lag
ranging from zero to 2 months in Rwanda and quadratic relationship between
temperature and malaria incidence in Uganda with protective effect for
temperatures below 30oC in Uganda [207]. Some studies have looked at the
effect of temperature and malaria without considering the lag dimension. For
example, in Nepal, an increase by 1 degree in mean temperature resulted in a
25% increase in risk of malaria [208]. In Papua New Guinea [209] a positive
association was observed for min temperature between 0-2 months, which
resonates with our findings for Asembo, and Gem. However is some regions,
like Chennai in India, shorter lag of 1 month was observed between malaria
and temperature [210]. Using a mathematical model to simulate the effect of
61
temperature on malaria incidence, an optimal temperature of between 21-25
oC was needed for maximum malaria transmission in Kwazulu Natal region in
south Africa [211], in our study region the effect of temperature is seen for
weeks with mean temperatures above 24oC.
Land surface temperature
In the second objective, we assessed the relationship between variables
derived by satellites and their relationship with malaria mortality in all the
three areas of the KEMRI/CDC HDSS. For temperature we used the MODIS
derived day land surface temperature as a proxy for surface temperature. At a
spatial resolution of 1km, we could assess the spatial differences in
relationship between the regions. In the second objective, we use distributed
lag non-linear models, which permitted simultaneous modelling of both the
lag and exposure space. For Asembo, Gem and Karemo areas combined, there
was an increase in risk for day LST above 34oC and a decrease in risk for day
LST from minimum to 28oC. We observed negative relationship shown by
decreasing risk with day LST below 29oC from week 0 to week 4 which is
similar study in the HDSS that showed negative relationship between day LST
and malaria transmission with a lag of 1 month [21] and in as study by Hay
Kilifi [57]. In the study by Hay [57]on the effect of day LST on malaria
admissions, they did not find any correlation In Siaya district but we show
positive relationship with day LST below 29oC. Day LST has been shown to
associate with mosquito density for period of between current and previous
month in Nouna HDSS in Burkina Farso [212].
Several other studies have used the flexible DLNM approach as we did to study
the effect of weather factors and malaria incidence [213-218]. Others have
used polynomial distributed lag model [219, 220], which is similar to DLNM
framework as it imposes constraints on the coefficients which reduces the
model degree of freedom. For example, using DLNM [213] in China, it was
shown that 1-degree increase in min temperature was significant for lags 4 to
9 weeks with highest risk at 7 weeks. This close to what we find of delayed lag
effect for day LST above 29oC which was the reference from week 7. Again, in
China, Guo [214] showed that high temperatures were associated with
increased risk of malaria with effect lasting 4 weeks for temperatures above
30oC, which is similar to our reference temperature of 29oC when constructing
the cross basis function in the DLNM. In Ethiopia[81], a positive association
was found between 1 month lag of LST and malaria incidence. In endemic
regions of Zambia a quadratic relationship between day LST was identified,
the risk increased with day LST above 30oC, which quite similar with what we
find with our analysis [221]. In areas stratified as hot in Ethiopia, max
temperature was found negatively associated with malaria incidence with

62
shorter lags of 3, 4 and 5 weeks [219]. In the Kenyan coast [220], max
temperature was shown to associate negatively with malaria incidence
between 5-35 days and positively associate with max temperature from 29-48
days which echoes our finding of longer lag effects for higher day LST.
Precipitation
For both the first and second paper, the effect of precipitation showed
nonlinear relationship, where the risk for malaria mortality increased linearly,
then decreased after reaching various thresholds. In the first objective, the
effect of total rainfall started manifesting after lag of 5 weeks, with effect
showing more strongly after lag of 9 weeks with linear relationship and at
longer lags, 13 to 16 weeks the effect showed the regular inverted U-shaped
relationship. At 13-16 weeks’ lag, the threshold is about, 140 mm/week of
rainfall after which the mortality relationship declines. This nonlinear
relationship between precipitation has been shown in other studies, for
example in Botswana [69] a quadratic relationship was found, with the
relationship forming the basis of a predictive model for early warning. When
they included 0 to 2 months lag of rainfall in a spatio-temporal model, Amek
et al. did not any relationship between rainfall and malaria transmission [21].
This could be due to several reasons, the inclusion of NDVI, which is a proxy
for water content, and probably the assumption of linearity between rainfall
and malaria transmission. In another study in the HDSS [24]areas, previous
total annual rainfall also did not any effect on malaria mortality and may due
consideration of longer lag ranges and assumption of linearity masking the
true relationship. A study in Nepal that did not take into account lags of
monthly total rainfall and included relative humidity also did not find any
relationship between rainfall and malaria risk [208].
In the second paper, we showed the relationship between TRMM satellite
precipitation and malaria mortality in the three areas in the KEMRI/CDC
using DLNM to capture both the lag and exposure space. The relationship
again was well captured by smooth cubic splines where the mortality risk
increased from a weekly total precipitation of 20 mm, then peaked at about a
weekly total of 80 mm of rainfall, and then declined. The threshold, the point
of maximum mortality in this analysis at 80 mm of weekly rainfall was
different for the first paper. This may be due to differences in source of rainfall
data. The TRMM rainfall data was extracted for the HDSS study area while in
paper 1 we used rainfall data collected at Kisumu airport, which is about 60
km away and may not have represented the precipitation patterns in the study
area. This underscores the importance of remote sensing data in improving
risk assessment in geographic areas where routine collection of weather data
may be lacking. Using DLNM, it has been shown that 10 mm increase in

63
rainfall increased the risk of malaria at lags of 2-4 weeks and 9-10 weeks with
highest risk at week 3 in china [213]. In our analysis a similar observation is
noted, where higher total weekly rainfall having short lag effect with effect
starting from week 0. The study in Rwanda and Uganda [207], where they
modelled rainfall and malaria incidence using DLNM, with mathematical
simulation in kwazulu Natal [211] and semiparametric Poisson regression in
endemic areas in Zambia [221], showed a similar relationship, where there is
increase and then decrease, resulting in an inverted U-shaped relationship as
we have similarly shown. In kwazulu Natal, precipitation effect peaked at 107
mm of rainfall and then declined [211] while in Zambia [221] it peaked at 100
mm of total rainfall. However, in Guangdong in China [214], a J-shaped
relationship was found between rainfall and malaria incidence with a
threshold of 150 mm of weekly total rainfall and effect precipitation
manifesting after 4 weeks and persisting for 15 weeks. They identified a high
risk at week 8 with 225 mm of total weekly rainfall. In some studies in Kenya,
along the coastal region and western Kenya at Siaya [199] , a longer lag of 2
months was identified for cold cloud duration and malaria admissions in
Kenya, which is a proxy for rainfall and in Sudan[222] a 2 month lag of rainfall
was associated with density of An arabiensis. In Guinea, the lag relationship
between rainfall and malaria differed in the region studied with a range of 1-
2 months [209]. In Niger using the DLNM approach [215], the delayed effect
of 1 mm increase in rainfall resulted in 7.2% increase in risk with highest risk
observed between 32 and 33 days. In Ghana, the delayed effect was evident
between 1 – 2 weeks and 9 weeks in endemic regions [223]. A study in
highlands of Ethiopia showed that TRMM precipitation products performed
better as explanatory variable to malaria occurrence than other products and
had positive relationship with malaria disease with a lag of 1-3 months [81].
In Ethiopia [219], using polynomial distributed lag method, the effect of
rainfall was positive at lags of 10-12 weeks with maximum lag at 12 weeks in
areas that were classified as cold. In this study, regions that were classified as
hot had shorter lag effects for rainfall from 6 weeks persisting to week 10.
Using the same method as above, it was shown that rainfall was associated
with mosquito density between 4-47 days in coastal regions of Kenya [220].
Normalized difference vegetation index
In the second paper, in addition to day LST and precipitation, we also
modelled the relationship between mean weekly NDVI values and malaria
mortality. We observe an L-shaped relationship. Mortality risk is higher for
NDVI of below 0.4 and protective for NDVI above 0.4. This threshold of
between 0.3 and 0.4 has been shown between NDVI and malaria admissions
in Kilifi in the coast and Siaya district in Western Kenya. For example in Siaya,
the correlation was 0.6 with a 1-month lag [57]. The L-shape relationship is

64
consistent in the three areas, Asembo, Gem and Karemo. The lag pattern is
similar to what we show and with NDVI below 0.4; the lag association is
significant from week 0 to week 5. Amek, [21] showed that NDVI was
positively related with mosquito density in Asembo and Gem; however they
did not show the NDVI ranges that are significant. Midekisa also showed the
NDVI had a lag of 1-3 month with malaria incidence in Ethiopian highlands
[81]. The interaction between NDVI and rainfall could explain the difference
in expected increase in risk with increasing NDVI. However, we observe that
for lower NDVI, below 0.4 the risk increased. One explanation for this could
be that, when NDVI is low, it means the conditions are drier and any pools of
water may provide suitable breeding sites for mosquitoes thus increase in risk
while when the NDVI is above, 0.4 there could be presence of more water
related to high rainfall amounts which could result in the flushing away of
mosquito breeding sites resulting in the protective effect observed in our
study.
Prediction of malaria admissions
After the lag and risk assessment in objective 1 and objective 2, we used the
information to develop predictive models for P. falciparum malaria
admissions for children using lagged remote sensing data to provide lead
times for potential action. The use of satellite imagery has been particular
encouraged in malaria forecasting [78]. From our results, the best performing
model used a novel variable selection by employing boosting regression [195].
Similar to other studies, the prediction errors increased with forecast
horizons. The 1-month lead time model provided the least predictions errors
in which the previous month’s values of malaria cases and remote sensing data
are modeled. Many studies have shown better predictions at one-month lag
[80, 224-227].
In Ethiopia [140], seasonal adjustment using last three month’s malaria
incidence data provided lower forecast errors, the first month having the least
prediction error as in our models. However, the seasonal adjustment method
provided robust predictions lasting up to 9 months. Another study in Ethiopia
confirmed that predictive model providing a lead time one month was
comparable to early detection methods in epidemic warning [219].
In Sri Lanka, exponential weighted moving average models have been used to
forecast malaria 1 month to four months ahead [225]. In this study, the best
models varied by district and forecasting horizon. A study in India [226] used
support vector machine firefly algorithm in optimal variable selection to
forecast malaria transmission using lags of temperature and rainfall. The best
lag was 1 month with a coefficient of determination of 0.83, which is in line

65
with our findings where we found coefficient of 0.8. In Burundi [80], 1 month
lag of temperature, NDVI and rainfall provided a forecasting accuracy of 93%,
with an R2 of 82% which close to our finding. In Kilifi district [228], at the
Kenya coast, using a combination of sea surface temperature (SST) and
rainfall, data for the previous 2 months, provided better prediction accuracies.
In this, we postulate that the use of SST provided longer lead time compared
to our models as has been shown in other studies [69].
We have shown that forecast models for malaria incidence have better
predictive skill at 1-month lead time. This information can useful in the early
detection in epidemic regions to marshal prevention strategies. If used for
early detection especially in epidemic environments, its two more weeks
gained in addition to the two weeks proposed in the rollback malaria initiative.
In malaria endemic regions, this information can be used to bolster
prevention and treatment strategies to avert excess cases. The models could
be improved to provide longer lead times by using seasonal forecasts. Seasonal
forecasts have been shown to provide longer lead times ranging from 1 to 6
months e.g. [151].
Economic evaluation framework of early warning systems
In paper IV of this study we developed a framework to make it easier to choose
among policy options in the control of vector borne diseases, which can be
extrapolated to control of malaria with an existing early warning system. The
framework makes it easier to include uncertainty that arise in the use of
predictive information and in effectiveness of interventions by including
errors in predictions and uncertainty and its variation with lead time. In the
framework, we proposed two methods, which holistically covers situations for
endemic and epidemic transmission setting. The method proposed for
endemic situation is the absolute diseases forecasts without reference to any
set thresholds. The other one, more commonly discussed, is the use of early
warning that predicts the occurrence of events based on pre-defined epidemic
thresholds. In situations where thresholds are used, sensitivity and specificity
can be aligned to the economic evaluation. We connect this to decision
analytic techniques to choose best intervention and time taking into account
arising uncertainties. We calculated the net benefit of each intervention or
combinations of intervention at each lead time to choose the best one given
the lead time prediction accuracy. The health outcome of the economic
evaluation of the early warning is the intervention effect in reducing disease
burdens within the health system. The evaluation can further be extended to
compute life years saved due to interventions by considering the deaths
avoided if the economic analysis is made from a larger not health system
specific perspective. The net benefits are computed by taking the differences
66
between the projected costs saved due to effect of response strategy and the
sum of costs of response and cost of running the information management
system. In epidemic conditions, the net benefit also includes the cost of false
alarm. For each lead time and intervention, the net benefits are computed.
The uncertainty around the parameters used to compute the net benefits are
included in the model as probability distribution functions and simulations
made by drawing from multiple parameters distributions. The drawn samples
are then used to compute the probability of positive net benefit, which forms
the basis of the intervention choice. The intervention with the highest
probability of net positive net benefit may be chosen as the optimal one.
The ranges for intervention effectiveness and the costs of treatments of the
diseases can be extracted from published research through sensitivity
analysis, unless it can be locally derived from local data and assessments. At
first, it may be challenging to get intervention effectiveness per lead time as
required by this model. However, we present the framework also to identify
what type of key information to be collected in setting up sustainable and cost-
effective early warning systems. This framework can be developed into a
computer program and used to make intervention choices. Given that it is
impossible to evaluate early warning system retrospectively, we suggest that
this framework can be validated for a period of time say five years with an
existing early warning system. In paper III of this thesis, we developed three
models to forecast malaria admissions at Siaya district hospital at 1, 2 and 3-
month prediction lead time. One of the measure of prediction accuracy
estimated was the mean squared error (MSE). We can, for example, use
method 2 of this framework to compare interventions such use of ITN where
the effectiveness is known since we make forecasts of actual admissions
numbers if the cost parameters are estimated.
Methodological considerations
The weekly malaria mortality data used in paper I and paper II were from
same VA questionnaires. The difference was in the way the cause of death was
derived. In the first, physician coding was used to get probable cause of death
while in the second paper, INTERVA method was used. In paper I, we
included anemia deaths. The inclusion of anemia deaths did not change the
results. We compared the numbers by both methods for period 2003 to 2008.
The INTERVA method resulted in more malaria deaths in all the years save
for 2003. The INTERVA methods has been shown to be in concordance with
physician coding in deriving cause of death [172]. We did not compare the way
the associations with environmental factors would vary depending on which
method was used. In the third paper, we used confirmed P. falciparum
malaria admissions data to develop the prediction models; we should assess

67
how the models predictive skills would perform if we used mortality data
derived through VA. The deaths collected through the regular surveillance in
the HDSS may not be timely for implementation in an early warning system.
As mentioned, the community interviewers usually visit each household every
four months, meaning there is a lag of 4 months before mortality events that
occurred in between are collected and processed through the VA system.
However, the parallel system that utilizes the village reporters to notify
immediately mortality events may provide mortality indicators to use in an
early warning system. Recent efforts have resulted in parsimonious VA
questionnaire that can be used together with the INTERVA algorithm in a
mobile device for real time determination of cause of death.
In the paper II, we used remote sensing data that provided opportunity to
perform regional risk assessment that was not possible in paper I where we
assumed the environmental factors are homogenous. The weather data in
paper I was from Kisumu airport, which is 60km away. In both papers, we
used ecological modelling which usually biases estimates towards the null.
However, the results did not vary so much with using highly resoluted data as
Amek et al [21] used in assessing malaria transmission risk at location level
for the study area.
In paper I we used GAM modelling framework, while in the paper II we used
distributed lag nonlinear models. Both methods allowed us to include model
the nonlinear effects of the environmental factors by controlling for
seasonality and trends. In paper I, the lag strata were created, but in paper II
the constrained modelling in DLNM allowed looking effect of each lag that
would not have been possible with the GAM given the many lags considered
ranging from 0 to 16 weeks. With the DLNM method, we could predict the lag
pattern at specific value of the environmental, which is not possible yet using
GAM. In most studies using remote sensing data and malaria, some form of
filtering implemented on the data before correlations are made. For example
Fourier temporal processing was been used to filter NDVI in the study by Hay
[57]. Filtering may help weed out variations in satellite data that could be
caused by cloud contamination. We did not filter the vegetation and LST
MODIS data in this study. For each of the study areas in paper II we used the
same model formulations, e.g. same degree of freedom for trend function but
may be the parameters would have been different for different regions. We did
not perform sensitivity analysis to find the best combination of degrees of
freedom for the cross basis functions to find the best suitable for the three
areas.
In the prediction paper III, we evaluated the GAMBOOSTLSS model in
improving forecast precision. The GAM model performed well during

68
training, but could not be replicate same accuracy in the forecast stage.
However, the GAMBOOST model showed robustness in forecast. Given the
changing patterns of malaria admissions, the boosted regression appeared the
better method in choosing smoothing regression parameters. In the
prediction, we could have compared different lags in the same model to get
combination of lags that had more skill in forecasting future cases.
In the framework in paper IV, we assume an existing and well-functioning
disease early warning system, which is not true for many countries. The
framework also assumes existence of high quality costs data both for
intervention and management of disease, which could be far from reality. The
model we propose is general covering even regions with endemic
transmission, but decision makers may be unwilling to invest in early warning
systems in endemic conditions where warning may be interpreted as just
season increase in disease cases. The model also does not incorporate possible
changes in costs and effectiveness that can occur over a period of time, say five
years. A warning message may result in certain activities such as the use of
nets, stocking of drugs at health facilities and general protective actions taken
by the populations, this can be difficult to include explicitly in the evaluation
especially for intervention effectiveness. Intervention effectiveness for vector
borne diseases can be affected by several factors such as insecticidal
resistance, drug resistance, weak health systems that could result in drug stock
outs and not include explicitly be included in this economic evaluation
framework
Policy recommendations
In this research, we have shown that climate information can be used to
develop forecasting systems with health outcomes such as morbidity and
mortality. The KEMRI/CDC health and demographic surveillance platform
provided a time series of malaria mortality data derived using VA and the
hospital based surveillance data from the Siaya district hospital. This
underscores the importance of HDSS for the improvement of community
health by providing information that can be challenging to find in poor
resource setting. We have also shown time lag between exposures, in this case,
climatic factors such as rainfall and temperature and malaria mortality in the
Western Kenya. The information is useful for developing early warning
forecast model as we have shown in the forecast of malaria admissions at Siaya
district hospital. In addition, the use of remote sensing data can be an
inexpensive way to get spatially accurate climate data to use in disease
modelling though it requires expertise in processing; this has been made
easier through efforts made by institutions such as International Research
Institute for Climate and Society.

69
Improvement in the collection of surveillance data and its use in malaria
control has been recommended in order to eliminate malaria by 2030. In this
study, we have utilized malaria surveillance data, for example from the Siaya
district hospital together with remote sensing data to predict future malaria
admission with some level of accuracy given the lead times. In our prediction
model, the 1-month lag was the most accurate. With this information on the
number of cases for the next month, malaria control managers can ensure
health facilities are well stocked with antimalarial, the health community
workers can advise the households to take preventive measures such as ITNs.
The framework we have developed for policy choice of intervention in
epidemic and endemic situations can encourage the use of surveillance
information in disease management. As much as disease forecasts may not be
accurate, integrating the uncertainty in policy choice in terms of net benefit in
reducing disease occurrence can encourage risk averse policy makers to
initiate response actions using probabilities of net benefits from each
intervention given the time window to act. The economic framework requires
that disease control managers have robust surveillance systems with risk
monitoring components such as rainfall and temperature. One inexpensive
way to collect temperature using simple temperature data loggers while for
rainfall, rain gauges can be installed. Remote sensing data can also be
retrieved from internet portals for regions where climate data is non-existent
or insufficient. With the surveillance in place, disease forecast can be made
into the future and interventions chosen based on projected probability of
positive net benefit. The model we have developed was for endemic region of
Western Kenya but can be used in epidemic regions such as highlands of East
Africa. This becomes more crucial with the projected global warming through
climate change that may increase transmission in highland regions
characterized by low temperatures. The next steps would be to deploy the early
warning forecast model together with the economic framework model to
choose the best intervention and to evaluate this in the study for its impact on
reducing malaria burden to the health system.
For policy makers, we suggest the strengthening of disease surveillance
systems. Improving diagnostics and continuous recording of disease events in
easy to retrieve format in a database. We recommend the collection of
environmental data through installation of weather stations that continuously
monitor climate variables such as rainfall and temperature or increase
capacity of technical staff to process data from remote sensing. We also
recommend the collection of vulnerability indicators such malnutrition,
economic levels, migrations of people to endemic regions to improve on model
fit. Together, this information from the surveillance can be used to create
informative predictive models, which can serve as a basis and improve timely
decision-making.

70
In addition, data and parameters of costs and effectiveness for the economic
evaluation should be collected within the health systems, to compute the net
benefits of response strategy to enable evaluation of the local early warning
system. We recommend that economic evaluation of forecasts to response
strategies should be embedded as a standard component of early warning
system to enable evidence based decision-making and optimal utilization of
available health system resources.

71
Conclusions
In this thesis, we have shown that climatic and environmental factors were
associated with malaria mortality in endemic region in Western Kenya. We
used the latency in the relationships of the remote sensing variables to malaria
surveillance data to develop a forecast model of malaria admissions among
children at the Siaya district hospital. The forecasts showed high accuracy at
a one-month lead time. We found boosting regression techniques showed
higher accuracy compared to standard regression models. We further
proposed an economic framework for integrating forecasts into evidence
based decision-making of response measures. The proposed framework can
accommodate two types of forecast information emanating from prediction
models, either alerts based on set thresholds or prediction of actual disease
occurrence. A method to estimate the net benefit probability distribution
function is described, which can inform decision makers on the probability a
net benefit beyond a specific threshold.
This thesis has contributed towards developing, and integrating early
warnings, into evidence based public health with application to controlling
malaria in an endemic region in Western Kenya. The contributions are
towards risk knowledge, development of prediction models, and the
integration of early warning systems into public health systems. We
recommend that economic evaluation be implemented as a standard
component of early warning systems to guide decision-makers to the long-
term optimal utilization of available health system resources.

72
Acknowledgements
I would like to appreciate several people who made this PhD possible and
made the journey palatable. First, I would like to thank the INDEPTH network
that initiated the CLIMIMO workshop that piqued my interest in climate
modelling of disease and made it possible to meet Dr. Joacim Rocklöv who
supported and guided me through the PhD period as my main supervisor,
providing technical as well as moral support. I would like to appreciate the
financial support through the years to undertake the studies at Umea
University. This PhD work has been collaborative process between my main
supervisor and other supervisors, Prof Clas Ahlm and Yesim Tozan. I have
benefited greatly by standing on the shoulders of my supervisors and learning
from their different expertise to make me a better researcher. From Prof Clas,
I gained great insight on infectious diseases while from Yesim Tozan; my
knowledge on health economics was enhanced. Many thanks to you Yesim for
hosting me at New York University as a research scholar during the spring
semester 2016. The exchange visit to New York would not have been possible
without the support from the graduate school of population dynamics at Umeå
University, I appreciate this support.
The PhD would not have been possible without support from the KEMRI/CDC
HDSS management that allowed me to use the health data and gave me time
off to study. In this regard, I would like to appreciate Dr. Frank Odhiambo,
Dr. Amek Nyaguara and Dr. Daniel Kwaro for their support and
encouragement during this process. I also pay gratitude to the HDSS staff who
processed the data and the residents that provided the data used in the study.
The journey back and forth from Umeå to Kenya would have not been possible
without the great logistical expertise of indefatigable Birgitta Åström and the
team around her including Ulrika Harju, whom I would like to thank for
making my journey and stay at Umeå a painless and rewarding process. I
would also like to appreciate the editorial suggestions made by Lena
Mustonen.
My stay in Umeå would not have been enjoyable without my PhD colleagues
and friends. In this regard, I would like to thank Vijendra Ingole, Mikkel
Quam, Jing Helmersson, Thadeus Egondi, Kanyiva Muindi, Joseph Zulu,
Moses Tetui, Osama Ahmed, Nathaniel Sirili, Regis Hitimana, Fredinah
Nematovu, Masoud Vaezghasemi, Julia Schröders, and Kateryna Karhina
among others for the great time we had in Umeå and the encouragements
during this journey. Through the lengthy discussions and arguments over
dinner, I felt home away from home.

73
Finally yet importantly, I would like to thank my family who have been the
source of inspiration and strength throughout this journey. I would like to
thank my wife, Catrine Anyango and my son Larry Morgan for the support and
allowing me to be away from them as I undertook my studies. I would also like
to thank my mother Evalin Auma Sewe who has inspired me the whole of my
life and instilled in me the need to advance academically.

74
References 1. Carter, R. and K.N. Mendis, Evolutionary and historical aspects of
the burden of malaria. Clin Microbiol Rev, 2002. 15(4): p. 564-94. 2. Miller, L.H., et al., Malaria biology and disease pathogenesis:
insights for new treatments. Nat Med, 2013. 19(2): p. 156-67. 3. Loy, D.E., et al., Out of Africa: origins and evolution of the human
malaria parasites Plasmodium falciparum and Plasmodium vivax. Int J Parasitol, 2016.
4. White, N., Plasmodium knowlesi: the fifth human malaria parasite. Clinical infectious diseases, 2008. 46(2): p. 172-173.
5. Greenwood, B.M., et al., Malaria. Lancet, 2005. 365(9469): p. 1487-98.
6. Snow, R.W., et al., Relation between severe malaria morbidity in children and level of Plasmodium falciparum transmission in Africa. Lancet, 1997. 349(9066): p. 1650-4.
7. Good, M.F., Vaccine-induced immunity to malaria parasites and the need for novel strategies. Trends Parasitol, 2005. 21(1): p. 29-34.
8. Aly, A.S., A.M. Vaughan, and S.H. Kappe, Malaria parasite development in the mosquito and infection of the mammalian host. Annu Rev Microbiol, 2009. 63: p. 195-221.
9. WHO. World Malaria Report 2015. Geneva: World Health Organization. 2015.
10. Gething, P.W., et al., A new world malaria map: Plasmodium falciparum endemicity in 2010. Malar J, 2011. 10: p. 378.
11. Kenya malaria indicator survey 2015. 12. Noor, A.M., et al., The risks of malaria infection in Kenya in 2009.
BMC Infect Dis, 2009. 9: p. 180. 13. Obonyo, C.O., et al., In-hospital morbidity and mortality due to
severe malarial anemia in western Kenya. Am J Trop Med Hyg, 2007. 77(6 Suppl): p. 23-8.
14. Githeko, A.K., et al., The reservoir of Plasmodium falciparum malaria in a holoendemic area of western Kenya. Trans R Soc Trop Med Hyg, 1992. 86(4): p. 355-8.
15. Phillips-Howard, P.A., et al., The efficacy of permethrin-treated bed nets on child mortality and morbidity in western Kenya I. Development of infrastructure and description of study site. Am J Trop Med Hyg, 2003. 68(4 Suppl): p. 3-9.
16. Phillips-Howard, P.A., et al., Efficacy of permethrin-treated bed nets in the prevention of mortality in young children in an area of high perennial malaria transmission in western Kenya. Am J Trop Med Hyg, 2003. 68(4 Suppl): p. 23-9.
17. Lindblade, K.A., et al., Sustainability of reductions in malaria transmission and infant mortality in western Kenya with use of insecticide-treated bednets: 4 to 6 years of follow-up. Jama, 2004. 291(21): p. 2571-80.
18. Eisele, T.P., et al., Effect of sustained insecticide-treated bed net use on all-cause child mortality in an area of intense perennial malaria

75
transmission in western Kenya. Am J Trop Med Hyg, 2005. 73(1): p. 149-56.
19. Hawley, W.A., et al., Community-wide effects of permethrin-treated bed nets on child mortality and malaria morbidity in western Kenya. Am J Trop Med Hyg, 2003. 68(4 Suppl): p. 121-7.
20. Adazu, K., et al., Health and demographic surveillance in rural western Kenya: a platform for evaluating interventions to reduce morbidity and mortality from infectious diseases. Am J Trop Med Hyg, 2005. 73(6): p. 1151-8.
21. Amek, N., et al., Spatial and temporal dynamics of malaria transmission in rural Western Kenya. Parasit Vectors, 2012. 5: p. 86.
22. Bayoh, M.N., et al., Anopheles gambiae: historical population decline associated with regional distribution of insecticide-treated bed nets in western Nyanza Province, Kenya. Malar J, 2010. 9: p. 62.
23. Amek, N.O., et al., Childhood cause-specific mortality in rural Western Kenya: application of the InterVA-4 model. Glob Health Action, 2014. 7: p. 25581.
24. Hamel, M.J., et al., A reversal in reductions of child mortality in western Kenya, 2003-2009. Am J Trop Med Hyg, 2011. 85(4): p. 597-605.
25. O'Meara, W.P., et al., Changes in the burden of malaria in sub-Saharan Africa. Lancet Infect Dis, 2010. 10(8): p. 545-55.
26. Desai, M., et al., Age-specific malaria mortality rates in the KEMRI/CDC health and demographic surveillance system in western Kenya, 2003-2010. PLoS One, 2014. 9(9): p. e106197.
27. Feikin, D.R., et al., Mortality and health among internally displaced persons in western Kenya following post-election violence, 2008: novel use of demographic surveillance. Bull World Health Organ, 2010. 88(8): p. 601-8.
28. Streatfield, P.K., et al., Malaria mortality in Africa and Asia: evidence from INDEPTH health and demographic surveillance system sites. Glob Health Action, 2014. 7: p. 25369.
29. Odhiambo, F.O., et al., Profile: the KEMRI/CDC Health and Demographic Surveillance System--Western Kenya. Int J Epidemiol, 2012. 41(4): p. 977-87.
30. Beguy, D., et al., Health & Demographic Surveillance System Profile: The Nairobi Urban Health and Demographic Surveillance System (NUHDSS). Int J Epidemiol, 2015. 44(2): p. 462-71.
31. Scott, J.A., et al., Profile: The Kilifi Health and Demographic Surveillance System (KHDSS). Int J Epidemiol, 2012. 41(3): p. 650-7.
32. Gething, P.W., et al., Modelling the global constraints of temperature on transmission of Plasmodium falciparum and P. vivax. Parasit Vectors, 2011. 4: p. 92.
33. Kiszewski, A., et al., A global index representing the stability of malaria transmission. Am J Trop Med Hyg, 2004. 70(5): p. 486-98.
34. Guerra, C.A., et al., The limits and intensity of Plasmodium falciparum transmission: implications for malaria control and elimination worldwide. PLoS Med, 2008. 5(2): p. e38.

76
35. Caminade, C., et al., Impact of climate change on global malaria distribution. Proc Natl Acad Sci U S A, 2014. 111(9): p. 3286-91.
36. Craig, M.H., R.W. Snow, and D. le Sueur, A climate-based distribution model of malaria transmission in sub-Saharan Africa. Parasitol Today, 1999. 15(3): p. 105-11.
37. Hay, S.I., et al., A world malaria map: Plasmodium falciparum endemicity in 2007. PLoS Med, 2009. 6(3): p. e1000048.
38. Stern, D.I., et al., Temperature and malaria trends in highland East Africa. PLoS One, 2011. 6(9): p. e24524.
39. Tonnang, H.E., et al., Zoom in at African country level: potential climate induced changes in areas of suitability for survival of malaria vectors. Int J Health Geogr, 2014. 13: p. 12.
40. Omumbo, J.A., et al., Raised temperatures over the Kericho tea estates: revisiting the climate in the East African highlands malaria debate. Malar J, 2011. 10: p. 12.
41. Bayoh, M.N. and S.W. Lindsay, Effect of temperature on the development of the aquatic stages of Anopheles gambiae sensu stricto (Diptera: Culicidae). Bull Entomol Res, 2003. 93(5): p. 375-81.
42. Bayoh, M.N., Studies on the development and survival of anopheles gambiae sensu stricto at various temperatures and relative humidities. 2001, Durham
43. Bayoh, M.N. and S.W. Lindsay, Temperature-related duration of aquatic stages of the Afrotropical malaria vector mosquito Anopheles gambiae in the laboratory. Med Vet Entomol, 2004. 18(2): p. 174-9.
44. Kelly-Hope, L.A., J. Hemingway, and F.E. McKenzie, Environmental factors associated with the malaria vectors Anopheles gambiae and Anopheles funestus in Kenya. Malar J, 2009. 8: p. 268.
45. Kirby, M.J. and S.W. Lindsay, Effect of temperature and inter-specific competition on the development and survival of Anopheles gambiae sensu stricto and An. arabiensis larvae. Acta Trop, 2009. 109(2): p. 118-23.
46. Paaijmans, K.P., et al., Relevant microclimate for determining the development rate of malaria mosquitoes and possible implications of climate change. Malar J, 2010. 9: p. 196.
47. Blanford, J.I., et al., Implications of temperature variation for malaria parasite development across Africa. Sci Rep, 2013. 3: p. 1300.
48. Paaijmans, K.P., A.F. Read, and M.B. Thomas, Understanding the link between malaria risk and climate. Proc Natl Acad Sci U S A, 2009. 106(33): p. 13844-9.
49. Paaijmans, K.P., et al., Influence of climate on malaria transmission depends on daily temperature variation. Proc Natl Acad Sci U S A, 2010. 107(34): p. 15135-9.
50. Patz, J.A., et al., Predicting key malaria transmission factors, biting and entomological inoculation rates, using modelled soil moisture in Kenya. Trop Med Int Health, 1998. 3(10): p. 818-27.

77
51. Asare, E.O., A.M. Tompkins, and A. Bomblies, A Regional Model for Malaria Vector Developmental Habitats Evaluated Using Explicit, Pond-Resolving Surface Hydrology Simulations. PLoS One, 2016. 11(3): p. e0150626.
52. Yamana, T.K. and E.A. Eltahir, Incorporating the effects of humidity in a mechanistic model of Anopheles gambiae mosquito population dynamics in the Sahel region of Africa. Parasit Vectors, 2013. 6: p. 235.
53. B, M., A Study of the Influence of relative Humidity on the Life and Infectibility of the Mosquito. Indian Journal of medical research, 1930. 17(4): p. 1119-1137.
54. Bomblies, A., Modeling the role of rainfall patterns in seasonal malaria transmission. Climatic Change, 2012. 112(3): p. 673-685.
55. Bisanzio, D., et al., Use of prospective hospital surveillance data to define spatiotemporal heterogeneity of malaria risk in coastal Kenya. Malar J, 2015. 14: p. 482.
56. Cohen, J.M., et al., Topography-derived wetness indices are associated with household-level malaria risk in two communities in the western Kenyan highlands. Malar J, 2008. 7: p. 40.
57. Hay, S.I., R.W. Snow, and D.J. Rogers, Predicting malaria seasons in Kenya using multitemporal meteorological satellite sensor data. Trans R Soc Trop Med Hyg, 1998. 92(1): p. 12-20.
58. Imbahale, S.S., et al., Variation in malaria transmission dynamics in three different sites in Western kenya. J Trop Med, 2012. 2012: p. 912408.
59. Sewe, M., et al., The association of weather variability and under five malaria mortality in KEMRI/CDC HDSS in Western Kenya 2003 to 2008: a time series analysis. Int J Environ Res Public Health, 2015. 12(2): p. 1983-97.
60. Sewe, M.O., C. Ahlm, and J. Rocklov, Remotely Sensed Environmental Conditions and Malaria Mortality in Three Malaria Endemic Regions in Western Kenya. PLoS One, 2016. 11(4): p. e0154204.
61. Thomson, M.C., et al., Use of rainfall and sea surface temperature monitoring for malaria early warning in Botswana. Am J Trop Med Hyg, 2005. 73(1): p. 214-21.
62. Boussari, O., et al., Modeling the seasonality of Anopheles gambiae s.s. biting rates in a South Benin sanitary zone. Transactions of The Royal Society of Tropical Medicine and Hygiene, 2014. 108(4): p. 237-243.
63. Coetzee, M., M. Craig, and D. le Sueur, Distribution of African malaria mosquitoes belonging to the Anopheles gambiae complex. Parasitol Today, 2000. 16(2): p. 74-7.
64. Koenraadt, C.J., A.K. Githeko, and W. Takken, The effects of rainfall and evapotranspiration on the temporal dynamics of Anopheles gambiae s.s. and Anopheles arabiensis in a Kenyan village. Acta Trop, 2004. 90(2): p. 141-53.
65. Lindsay, S.W., L. Parson, and C.J. Thomas, Mapping the ranges and relative abundance of the two principal African malaria vectors,

78
Anopheles gambiae sensu stricto and An. arabiensis, using climate data. Proc Biol Sci, 1998. 265(1399): p. 847-54.
66. Kristan, M., et al., Variations in entomological indices in relation to weather patterns and malaria incidence in East African highlands: implications for epidemic prevention and control. Malar J, 2008. 7: p. 231.
67. Minakawa, N., et al., The effects of climatic factors on the distribution and abundance of malaria vectors in Kenya. J Med Entomol, 2002. 39(6): p. 833-41.
68. Ebhuoma, O. and M. Gebreslasie, Remote Sensing-Driven Climatic/Environmental Variables for Modelling Malaria Transmission in Sub-Saharan Africa. Int J Environ Res Public Health, 2016. 13(6).
69. Ceccato, P., et al., Application of Geographical Information Systems and Remote Sensing technologies for assessing and monitoring malaria risk. Parassitologia, 2005. 47(1): p. 81-96.
70. Xie, Y., Z. Sha, and M. Yu, Remote sensing imagery in vegetation mapping: a review. Journal of Plant Ecology, 2008. 1(1): p. 9-23.
71. Connor, S.J., et al., Environmental information systems in malaria risk mapping and epidemic forecasting. Disasters, 1998. 22(1): p. 39-56.
72. Connor, S.J., et al., Using climate information for improved health in Africa: relevance, constraints and opportunities. Geospat Health, 2006. 1(1): p. 17-31.
73. Adigun, A.B., et al., Malaria risk in Nigeria: Bayesian geostatistical modelling of 2010 malaria indicator survey data. Malar J, 2015. 14: p. 156.
74. Dantur Juri, M.J., et al., Satellite-derived NDVI, LST, and climatic factors driving the distribution and abundance of Anopheles mosquitoes in a former malarious area in northwest Argentina. J Vector Ecol, 2015. 40(1): p. 36-45.
75. Omumbo, J.A., et al., Updating Historical Maps of Malaria Transmission Intensity in East Africa Using Remote Sensing. Photogramm Eng Remote Sensing, 2002. 68(2): p. 161-166.
76. Sogoba, N., et al., The spatial distribution of Anopheles gambiae sensu stricto and An. arabiensis (Diptera: Culicidae) in Mali. Geospat Health, 2007. 1(2): p. 213-22.
77. Dambach, P., et al., Utilization of combined remote sensing techniques to detect environmental variables influencing malaria vector densities in rural West Africa. Int J Health Geogr, 2012. 11: p. 8.
78. Rogers, D.J., et al., Satellite imagery in the study and forecast of malaria. Nature, 2002. 415(6872): p. 710-5.
79. Fastring, D.R. and J.A. Griffith, Malaria incidence in Nairobi, Kenya and dekadal trends in NDVI and climatic variables. Geocarto International, 2009. 24(3): p. 207-221.
80. Gomez-Elipe, A., et al., Forecasting malaria incidence based on monthly case reports and environmental factors in Karuzi, Burundi, 1997-2003. Malar J, 2007. 6: p. 129.

79
81. Midekisa, A., et al., Remote sensing-based time series models for malaria early warning in the highlands of Ethiopia. Malar J, 2012. 11: p. 165.
82. Haque, U., et al., The role of climate variability in the spread of malaria in Bangladeshi highlands. PLoS One, 2010. 5(12): p. e14341.
83. Samadoulougou, S., et al., Multilevel and geo-statistical modeling of malaria risk in children of Burkina Faso. Parasit Vectors, 2014. 7: p. 350.
84. Machault, V., et al., Spatial heterogeneity and temporal evolution of malaria transmission risk in Dakar, Senegal, according to remotely sensed environmental data. Malar J, 2010. 9: p. 252.
85. Mendez, F., G. Carrasquilla, and A. Munoz, Risk factors associated with malaria infection in an urban setting. Trans R Soc Trop Med Hyg, 2000. 94(4): p. 367-71.
86. Rulisa, S., et al., Malaria prevalence, spatial clustering and risk factors in a low endemic area of Eastern Rwanda: a cross sectional study. PLoS One, 2013. 8(7): p. e69443.
87. Chirebvu, E., M.J. Chimbari, and B.N. Ngwenya, Assessment of risk factors associated with malaria transmission in tubu village, northern botswana. Malar Res Treat, 2014. 2014: p. 403069.
88. Baragatti, M., et al., Social and environmental malaria risk factors in urban areas of Ouagadougou, Burkina Faso. Malar J, 2009. 8: p. 13.
89. Homan, T., et al., Spatially variable risk factors for malaria in a geographically heterogeneous landscape, western Kenya: an explorative study. Malar J, 2016. 15: p. 1.
90. Chirombo, J., R. Lowe, and L. Kazembe, Using structured additive regression models to estimate risk factors of malaria: analysis of 2010 Malawi malaria indicator survey data. PLoS One, 2014. 9(7): p. e101116.
91. Graves, P.M., et al., Individual, household and environmental risk factors for malaria infection in Amhara, Oromia and SNNP regions of Ethiopia. Trans R Soc Trop Med Hyg, 2009. 103(12): p. 1211-20.
92. West, P.A., et al., Malaria risk factors in North West Tanzania: the effect of spraying, nets and wealth. PLoS One, 2013. 8(6): p. e65787.
93. Roberts, D. and G. Matthews, Risk factors of malaria in children under the age of five years old in Uganda. Malar J, 2016. 15: p. 246.
94. Safeukui-Noubissi, I., et al., Risk factors for severe malaria in Bamako, Mali: a matched case-control study. Microbes Infect, 2004. 6(6): p. 572-8.
95. Keating, J., et al., Self-reported malaria and mosquito avoidance in relation to household risk factors in a Kenyan coastal city. J Biosoc Sci, 2005. 37(6): p. 761-71.
96. Munga, S., et al., Land use and land cover changes and spatiotemporal dynamics of anopheline larval habitats during a four-year period in a highland community of Africa. Am J Trop Med Hyg, 2009. 81(6): p. 1079-84.
97. Mutuku, F.M., et al., A supervised land cover classification of a western Kenya lowland endemic for human malaria: associations of

80
land cover with larval Anopheles habitats. Int J Health Geogr, 2009. 8: p. 19.
98. Raso, G., et al., Spatial risk profiling of Plasmodium falciparum parasitaemia in a high endemicity area in Cote d'Ivoire. Malar J, 2009. 8: p. 252.
99. Wayant, N.M., et al., Correlation between normalized difference vegetation index and malaria in a subtropical rain forest undergoing rapid anthropogenic alteration. Geospat Health, 2010. 4(2): p. 179-90.
100. Stresman, G.H., Beyond temperature and precipitation: ecological risk factors that modify malaria transmission. Acta Trop, 2010. 116(3): p. 167-72.
101. Alemu, A., et al., Urban malaria and associated risk factors in Jimma town, south-west Ethiopia. Malar J, 2011. 10: p. 173.
102. Matthys, B., et al., Urban farming and malaria risk factors in a medium-sized town in Cote d'Ivoire. Am J Trop Med Hyg, 2006. 75(6): p. 1223-31.
103. Protopopoff, N., et al., Ranking malaria risk factors to guide malaria control efforts in African highlands. PLoS One, 2009. 4(11): p. e8022.
104. Sutcliffe, C.G., et al., Changing individual-level risk factors for malaria with declining transmission in southern Zambia: a cross-sectional study. Malar J, 2011. 10: p. 324.
105. Ghebreyesus, T.A., et al., Household risk factors for malaria among children in the Ethiopian highlands. Trans R Soc Trop Med Hyg, 2000. 94(1): p. 17-21.
106. Sintasath, D.M., et al., Malaria prevalence and associated risk factors in Eritrea. Am J Trop Med Hyg, 2005. 72(6): p. 682-7.
107. Ayele, D.G., T.T. Zewotir, and H.G. Mwambi, Prevalence and risk factors of malaria in Ethiopia. Malar J, 2012. 11: p. 195.
108. Yamamoto, S., et al., Household risk factors for clinical malaria in a semi-urban area of Burkina Faso: a case-control study. Trans R Soc Trop Med Hyg, 2010. 104(1): p. 61-5.
109. Haque, U., et al., Risk factors associated with clinical malaria episodes in Bangladesh: a longitudinal study. Am J Trop Med Hyg, 2013. 88(4): p. 727-32.
110. Woyessa, A., et al., Malaria risk factors in Butajira area, south-central Ethiopia: a multilevel analysis. Malar J, 2013. 12: p. 273.
111. Ndiath, M.M., et al., Application of geographically-weighted regression analysis to assess risk factors for malaria hotspots in Keur Soce health and demographic surveillance site. Malar J, 2015. 14: p. 463.
112. Okumu, F.O., et al., Mathematical evaluation of community level impact of combining bed nets and indoor residual spraying upon malaria transmission in areas where the main vectors are Anopheles arabiensis mosquitoes. Parasit Vectors, 2013. 6: p. 17.
113. WHO, Malaria epidemics: forecasting, prevention, early detection and control: from policy to practice: report of an informal consultation: Leysin, Switzerland, 8-10 December 2003. 2004.

81
114. Barnes, K.I., P. Chanda, and G. Ab Barnabas, Impact of the large-scale deployment of artemether/lumefantrine on the malaria disease burden in Africa: case studies of South Africa, Zambia and Ethiopia. Malar J, 2009. 8 Suppl 1: p. S8.
115. Crowell, V., et al., Modelling the cost-effectiveness of mass screening and treatment for reducing Plasmodium falciparum malaria burden. Malar J, 2013. 12: p. 4.
116. Kern, S.E., et al., Community screening and treatment of asymptomatic carriers of Plasmodium falciparum with artemether-lumefantrine to reduce malaria disease burden: a modelling and simulation analysis. Malar J, 2011. 10: p. 210.
117. Gahutu, J.B., et al., Prevalence and risk factors of malaria among children in southern highland Rwanda. Malar J, 2011. 10: p. 134.
118. Winskill, P., et al., Malaria risk factors in north-east Tanzania. Malar J, 2011. 10: p. 98.
119. Zhou, G., et al., Community-wide benefits of targeted indoor residual spray for malaria control in the western Kenya highland. Malar J, 2010. 9: p. 67.
120. Fullman, N., et al., Nets, spray or both? The effectiveness of insecticide-treated nets and indoor residual spraying in reducing malaria morbidity and child mortality in sub-Saharan Africa. Malar J, 2013. 12: p. 62.
121. Giardina, F., et al., Effects of vector-control interventions on changes in risk of malaria parasitaemia in sub-Saharan Africa: a spatial and temporal analysis. Lancet Glob Health, 2014. 2(10): p. e601-15.
122. Gimnig, J.E., et al., The Effect of Indoor Residual Spraying on the Prevalence of Malaria Parasite Infection, Clinical Malaria and Anemia in an Area of Perennial Transmission and Moderate Coverage of Insecticide Treated Nets in Western Kenya. PLoS One, 2016. 11(1): p. e0145282.
123. Hamel, M.J., et al., The combination of indoor residual spraying and insecticide-treated nets provides added protection against malaria compared with insecticide-treated nets alone. Am J Trop Med Hyg, 2011. 85(6): p. 1080-6.
124. Protopopoff, N., et al., Combination of Insecticide Treated Nets and Indoor Residual Spraying in Northern Tanzania Provides Additional Reduction in Vector Population Density and Malaria Transmission Rates Compared to Insecticide Treated Nets Alone: A Randomised Control Trial. PLoS One, 2015. 10(11): p. e0142671.
125. Steketee, R.W. and C.C. Campbell, Impact of national malaria control scale-up programmes in Africa: magnitude and attribution of effects. Malar J, 2010. 9: p. 299.
126. West, P.A., et al., Enhanced protection against malaria by indoor residual spraying in addition to insecticide treated nets: is it dependent on transmission intensity or net usage? PLoS One, 2015. 10(3): p. e0115661.
127. Griffin, J.T., et al., Reducing Plasmodium falciparum malaria transmission in Africa: a model-based evaluation of intervention strategies. PLoS Med, 2010. 7(8).
82
128. McNabb, S.J.N., et al., Conceptual framework of public health surveillance and action and its application in health sector reform. BMC Public Health, 2002. 2: p. 2.
129. Anker, M., Evaluating the costs and benefits of national surveillance and response systems. Methodologies and options. 2005.
130. Abeku, T.A., Response to malaria epidemics in Africa. Emerg Infect Dis, 2007. 13(5): p. 681-6.
131. UNEP, Early Warning Systems: A State of the Art Analysis and Future Directions. Division of Early Warning and Assessment (DEWA),United Nations Environment Programme (UNEP), Nairobi. 2012.
132. WHO, Malaria Early Warning Systems—A Framework for Field Research in Africa. 2001. 1-84.
133. Cox, J. and T.A. Abeku, Early warning systems for malaria in Africa: from blueprint to practice. Trends Parasitol, 2007. 23(6): p. 243-6.
134. DaSilva, J., et al., Improving epidemic malaria planning, preparedness and response in Southern Africa. Report on the 1st Southern African Regional Epidemic Outlook Forum, Harare, Zimbabwe, 26-29 September, 2004. Malar J, 2004. 3: p. 37.
135. Thomson, M.C. and S.J. Connor, The development of Malaria Early Warning Systems for Africa. Trends Parasitol, 2001. 17(9): p. 438-45.
136. Lindblade, K.A., E.D. Walker, and M.L. Wilson, Early warning of malaria epidemics in African highlands using Anopheles (Diptera: Culicidae) indoor resting density. J Med Entomol, 2000. 37(5): p. 664-74.
137. Cullen, J.R., et al., An epidemiological early warning system for malaria control in northern Thailand. Bull World Health Organ, 1984. 62(1): p. 107-14.
138. Davis, R.G., et al., Early detection of malaria foci for targeted interventions in endemic southern Zambia. Malar J, 2011. 10: p. 260.
139. Abeku, T.A., et al., Malaria epidemic early warning and detection in African highlands. Trends Parasitol, 2004. 20(9): p. 400-5.
140. Abeku, T.A., et al., Forecasting malaria incidence from historical morbidity patterns in epidemic-prone areas of Ethiopia: a simple seasonal adjustment method performs best. Trop Med Int Health, 2002. 7(10): p. 851-7.
141. Mabaso, M.L. and N.C. Ndlovu, Critical review of research literature on climate-driven malaria epidemics in sub-Saharan Africa. Public Health, 2012. 126(11): p. 909-19.
142. Mateus, J.C. and G. Carrasquilla, Predictors of local malaria outbreaks: an approach to the development of an early warning system in Colombia. Mem Inst Oswaldo Cruz, 2011. 106 Suppl 1: p. 107-13.
143. Ceccato, P., et al., Malaria stratification, climate, and epidemic early warning in Eritrea. Am J Trop Med Hyg, 2007. 77(6 Suppl): p. 61-8.
144. Grover-Kopec, E., et al., An online operational rainfall-monitoring resource for epidemic malaria early warning systems in Africa. Malar J, 2005. 4: p. 6.
83
145. Hay, S.I., et al., Malaria early warning in Kenya. Trends Parasitol, 2001. 17(2): p. 95-9.
146. Hay, S.I., et al., Forecasting, warning, and detection of malaria epidemics: a case study. Lancet, 2003. 361(9370): p. 1705-6.
147. Teklehaimanot, H.D., et al., Weather-based prediction of Plasmodium falciparum malaria in epidemic-prone regions of Ethiopia II. Weather-based prediction systems perform comparably to early detection systems in identifying times for interventions. Malar J, 2004. 3: p. 44.
148. Chatterjee, C. and R.R. Sarkar, Multi-step polynomial regression method to model and forecast malaria incidence. PLoS One, 2009. 4(3): p. e4726.
149. Lauderdale, J.M., et al., Towards seasonal forecasting of malaria in India. Malar J, 2014. 13: p. 310.
150. Thomson, M., et al., Malaria early warning in Kenya and seasonal climate forecasts. Lancet, 2003. 362(9383): p. 580.
151. Thomson, M.C., et al., Malaria early warnings based on seasonal climate forecasts from multi-model ensembles. Nature, 2006. 439(7076): p. 576-9.
152. Klafft, M. and U. Meissen. Assessing the economic value of early warning systems. in Proceedings of the 8th International Conference on Information Systems for Crisis Response and Management. 2011.
153. Schröter, K., et al., Effectiveness and Efficiency of Early Warning Systems for Flash-Floods (EWASE). 2008.
154. Rogers, D. and V. Tsirkunov, Costs and benefits of early warning systems. Global Assessment Report on Disaster Risk Reduction, 2011.
155. Worrall, E., An economic evaluation of malaria early warning systems in Africa: a population dynamic modelling approach. 2001, University of Liverpool.
156. Worrall, E., S.J. Connor, and M.C. Thomson, A model to simulate the impact of timing, coverage and transmission intensity on the effectiveness of indoor residual spraying (IRS) for malaria control. Trop Med Int Health, 2007. 12(1): p. 75-88.
157. McConnell, K.J., Evaluating Health Policy Under Uncertainty: An Application to Early Warning Systems. 2001, Stanford University.
158. Schröter, K., et al., EWASE—Early Warning Systems Efficiency: Evaluation of flood forecast reliability. Flood risk management research and practice. London: Taylor & Francis Group, 2009: p. 755-765.
159. Ye, Y., et al., Health and demographic surveillance systems: a step towards full civil registration and vital statistics system in sub-Sahara Africa? BMC Public Health, 2012. 12: p. 741.
160. Sankoh, O. and P. Byass, The INDEPTH Network: filling vital gaps in global epidemiology. Int J Epidemiol, 2012. 41(3): p. 579-88.
161. Ekstrom, A.M., et al., INDEPTH Network: contributing to the data revolution. Lancet Diabetes Endocrinol, 2016. 4(2): p. 97.
162. Sankoh, O., et al., INDEPTH launches a data repository and INDEPTHStats. Lancet Glob Health, 2013. 1(2): p. e69.

84
163. Amek, N., et al., Using health and demographic surveillance system (HDSS) data to analyze geographical distribution of socio-economic status; an experience from KEMRI/CDC HDSS. Acta Trop, 2015. 144: p. 24-30.
164. AbouZahr, C., et al., Towards universal civil registration and vital statistics systems: the time is now. Lancet, 2015. 386(10001): p. 1407-18.
165. AbouZahr, C., et al., Civil registration and vital statistics: progress in the data revolution for counting and accountability. Lancet, 2015. 386(10001): p. 1373-85.
166. Byass, P., Uncounted causes of death. Lancet, 2016. 387(10013): p. 26-7.
167. Byass, P., The UN needs joined-up thinking on vital registration. Lancet, 2012. 380(9854): p. 1643.
168. Serina, P., et al., A shortened verbal autopsy instrument for use in routine mortality surveillance systems. BMC Med, 2015. 13: p. 302.
169. Leitao, J., et al., Revising the WHO verbal autopsy instrument to facilitate routine cause-of-death monitoring. Glob Health Action, 2013. 6: p. 21518.
170. Byass, P., et al., Strengthening standardised interpretation of verbal autopsy data: the new InterVA-4 tool. Glob Health Action, 2012. 5: p. 1-8.
171. Byass, P., et al., Refining a probabilistic model for interpreting verbal autopsy data. Scand J Public Health, 2006. 34(1): p. 26-31.
172. Byass, P., et al., Comparing verbal autopsy cause of death findings as determined by physician coding and probabilistic modelling: a public health analysis of 54 000 deaths in Africa and Asia. J Glob Health, 2015. 5(1): p. 010402.
173. Wan, Z., et al., Quality assessment and validation of the MODIS global land surface temperature. International Journal of Remote Sensing, 2004. 25(1): p. 261-274.
174. Wan, Z. and J. Dozier, A generalized split-window algorithm for retrieving land-surface temperature from space. IEEE Transactions on geoscience and remote sensing, 1996. 34(4): p. 892-905.
175. Li, Z.-L., et al., Satellite-derived land surface temperature: Current status and perspectives. Remote Sensing of Environment, 2013. 131: p. 14-37.
176. Wan, Z., et al., Validation of the land-surface temperature products retrieved from Terra Moderate Resolution Imaging Spectroradiometer data. Remote sensing of Environment, 2002. 83(1): p. 163-180.
177. Wan, Z., MODIS land surface temperature products users’ guide. Institute for Computational Earth System Science, University of California, Santa Barbara, CA, 2006.
178. Huete, A., et al., Overview of the radiometric and biophysical performance of the MODIS vegetation indices. Remote sensing of environment, 2002. 83(1): p. 195-213.
85
179. Huete, A., C. Justice, and H. Liu, Development of vegetation and soil indices for MODIS-EOS. Remote Sensing of Environment, 1994. 49(3): p. 224-234.
180. Huete, A., C. Justice, and W. Van Leeuwen, MODIS vegetation index (MOD13). Algorithm theoretical basis document, 1999. 3: p. 213.
181. Ramon , S., et al., MODIS Vegetation Index User’s Guide. 2010. 182. van Leeuwen, W.J., A.R. Huete, and T.W. Laing, MODIS vegetation
index compositing approach: A prototype with AVHRR data. Remote Sensing of Environment, 1999. 69(3): p. 264-280.
183. USGS. https://lpdaac.usgs.gov/. 184. Rowlingson, R.B.a.T.K.a.B., rgdal: Bindings for the Geospatial Data
Abstraction Library. 2014. 185. Hallman, J. tis: Time Indexes and Time Indexed Series. 2013;
Available from: http://CRAN.R-project.org/package=tis. 186. Center, E.O., TRMM Data Users Handbook. National Space
Development Agency of Japan, 2001. 187. Gasparrini, A., Modeling exposure-lag-response associations with
distributed lag non-linear models. Stat Med, 2014. 33(5): p. 881-99. 188. Gasparrini, A., B. Armstrong, and M.G. Kenward, Distributed lag
non-linear models. Stat Med, 2010. 29(21): p. 2224-34. 189. Gasparrini, A., Modelling lagged associations in environmental time
series data: a simulation study. Epidemiology, 2016. 190. Gasparrini, A., Distributed Lag Linear and Non-Linear Models in R:
The Package dlnm. J Stat Softw, 2011. 43(8): p. 1-20. 191. Gasparrini, A. and M. Leone, Attributable risk from distributed lag
models. BMC Med Res Methodol, 2014. 14: p. 55. 192. Hastie, T. and R. Tibshirani, Generalized additive models. Statistical
science, 1986: p. 297-310. 193. Wood, S.N., Generalized additive models: an introduction with R.
2006. 194. Wood, S. and M.S. Wood, Package ‘mgcv’. R package version, 2016:
p. 1.7-29. 195. Hofner, B., A. Mayr, and M. Schmid, gamboostLSS: An R package for
model building and variable selection in the GAMLSS framework. arXiv preprint arXiv:1407.1774, 2014.
196. Hofner, B., Boosting in structured additive models. 2011, lmu. 197. Fox-Rushby, J. and J. Cairns, Economic evaluation. 198. Peng, R.D., F. Dominici, and T.A. Louis, Model choice in time series
studies of air pollution and mortality. Journal of the Royal Statistical Society: Series A (Statistics in Society), 2006. 169(2): p. 179-203.
199. Hay, S., R. Snow, and D. Rogers, From predicting mosquito habitat to malaria seasons using remotely sensed data: practice, problems and perspectives. Parasitology Today, 1998. 14(8): p. 306-313.
200. Nkurunziza, H., A. Gebhardt, and J. Pilz, Forecasting Malaria Cases in Bujumbura. World Academy of Science, Engineering and Technology, International Journal of Mathematical, Computational, Physical, Electrical and Computer Engineering, 2010. 4(1): p. 14-19.
201. Shcherbakov, M.V., et al., A survey of forecast error measures. World Appl Sci J, 2013. 24: p. 171-176.

86
202. Team, R.C., R: A language and environment for statistical computing. 2013.
203. Torgo, L. and M.L. Torgo, Package ‘DMwR’. Comprehensive R Archive Network, 2013.
204. Brown, Z., et al., Stakeholder development of the malaria decision analysis support tool (MDAST). Malaria Journal, 2012. 11(1): p. 1.
205. Kramer, R.A., et al., Using decision analysis to improve malaria control policy making. Health policy, 2009. 92(2): p. 133-140.
206. Chirebvu, E., et al., Clinical Malaria Transmission Trends and Its Association with Climatic Variables in Tubu Village, Botswana: A Retrospective Analysis. PLoS One, 2016. 11(3): p. e0139843.
207. Colon-Gonzalez, F.J., et al., Assessing the effects of air temperature and rainfall on malaria incidence: an epidemiological study across Rwanda and Uganda. Geospat Health, 2016. 11(1 Suppl): p. 379.
208. Dhimal, M., et al., Spatio-temporal distribution of malaria and its association with climatic factors and vector-control interventions in two high-risk districts of Nepal. Malar J, 2014. 13: p. 457.
209. Imai, C., et al., Associations between malaria and local and global climate variability in five regions in Papua New Guinea. Trop Med Health, 2016. 44: p. 23.
210. Kumar, D.S., et al., Spatial trend, environmental and socioeconomic factors associated with malaria prevalence in Chennai. Malar J, 2014. 13: p. 14.
211. Okuneye, K. and A.B. Gumel, Analysis of a temperature- and rainfall-dependent model for malaria transmission dynamics. Math Biosci, 2016.
212. Diboulo, E., et al., Bayesian variable selection in modelling geographical heterogeneity in malaria transmission from sparse data: an application to Nouna Health and Demographic Surveillance System (HDSS) data, Burkina Faso. Parasit Vectors, 2015. 8: p. 118.
213. Bi, Y., et al., Impact of climate variability on Plasmodium vivax and Plasmodium falciparum malaria in Yunnan Province, China. Parasit Vectors, 2013. 6: p. 357.
214. Guo, C., et al., Malaria incidence from 2005-2013 and its associations with meteorological factors in Guangdong, China. Malar J, 2015. 14: p. 116.
215. Jusot, J.F. and O. Alto, Short term effect of rainfall on suspected malaria episodes at Magaria, Niger: a time series study. Trans R Soc Trop Med Hyg, 2011. 105(11): p. 637-43.
216. Wardrop, N.A., et al., Plasmodium vivax malaria incidence over time and its association with temperature and rainfall in four counties of Yunnan Province, China. Malar J, 2013. 12: p. 452.
217. Zhao, X., et al., Characterizing the effect of temperature fluctuation on the incidence of malaria: an epidemiological study in south-west China using the varying coefficient distributed lag non-linear model. Malar J, 2014. 13: p. 192.
218. Zhao, X., et al., The temporal lagged association between meteorological factors and malaria in 30 counties in south-west

87
China: a multilevel distributed lag non-linear analysis. Malar J, 2014. 13: p. 57.
219. Teklehaimanot, H.D., et al., Weather-based prediction of Plasmodium falciparum malaria in epidemic-prone regions of Ethiopia I. Patterns of lagged weather effects reflect biological mechanisms. Malar J, 2004. 3: p. 41.
220. Walker, M., et al., Temporal and micro-spatial heterogeneity in the distribution of Anopheles vectors of malaria along the Kenyan coast. Parasit Vectors, 2013. 6: p. 311.
221. Shimaponda-Mataa, N.M., et al., Modelling the influence of temperature and rainfall on malaria incidence in four endemic provinces of Zambia using semiparametric Poisson regression. Acta Trop, 2016.
222. Himeidan, Y.E., et al., Pattern of malaria transmission along the Rahad River basin, Eastern Sudan. Parasit Vectors, 2011. 4: p. 109.
223. Krefis, A.C., et al., Modeling the relationship between precipitation and malaria incidence in children from a holoendemic area in Ghana. Am J Trop Med Hyg, 2011. 84(2): p. 285-91.
224. Wangdi, K., et al., Development of temporal modelling for forecasting and prediction of malaria infections using time-series and ARIMAX analyses: a case study in endemic districts of Bhutan. Malar J, 2010. 9: p. 251.
225. Briet, O.J., et al., Models for short term malaria prediction in Sri Lanka. Malar J, 2008. 7: p. 76.
226. Ch, S., et al., A Support Vector Machine-Firefly Algorithm based forecasting model to determine malaria transmission. Neurocomputing, 2014. 129: p. 279-288.
227. Zinszer, K., et al., Forecasting malaria in a highly endemic country using environmental and clinical predictors. Malar J, 2015. 14: p. 245.
228. Karuri, S.W. and R.W. Snow, Forecasting paediatric malaria admissions on the Kenya Coast using rainfall. Glob Health Action, 2016. 9: p. 29876.


















