TOWARDS AN IT ROADMAP FOR BELGIAN HOSPITALS/media/corporate-marketing/our-expertise/... · From...
37
TOWARDS AN IT ROADMAP FOR BELGIAN HOSPITALS
Transcript of TOWARDS AN IT ROADMAP FOR BELGIAN HOSPITALS/media/corporate-marketing/our-expertise/... · From...
TOWARDS AN IT ROADMAP FOR
BELGIAN HOSPITALS

1
Title
Towards an IT Roadmap for Belgian Hospitals
Authors
Prof. Dr. Brecht Cardoen – [email protected]
Prof. Dr. Bjorn Cumps – [email protected]
Mathias Boënne – [email protected]
Table of Contents
Executive summary ............................................................................................... 2
Introduction .......................................................................................................... 4
IT challenges for hospitals ................................................................................................. 4
Focus on digital transformation .......................................................................................... 7
Research question ................................................................................................. 9
A view on a hospital’s capabilities ...........................................................................10
Business architecture ...................................................................................................... 11
IT architecture ................................................................................................................ 14
A closer view on some Belgian hospitals ..................................................................16
Case 1: large non-university hospital ................................................................................ 16
Case 2: large university hospital ....................................................................................... 19
Case 3: large non-university hospital ................................................................................ 22
Case 4: medium-size non-university hospital ...................................................................... 24
From heat map to roadmap ...................................................................................28
Conclusion and next steps .....................................................................................32
Bibliography ........................................................................................................33
Reference
This report is electronically available on www.vlerick.com/healthcare and can be cited as
“Cardoen B., Cumps B. and Boënne M. 2017. Towards an IT Roadmap for Belgian Hospitals.
Vlerick Business School, HMC White Paper”.
Acknowledgement
This report was supported by the Belgian Association of Hospital Directors (ABDH/BVZD)
and made possible by an unconditional grant provided by Xperthis.
Our solution to your specific needs
2
Executive summary
With technology developing at the speed of light, hospitals are embracing the era of digital
transformation and are substantially rethinking how information technology (IT) should
progress within the healthcare setting. The evolution in the domain of healthcare is
increasingly calling for IT proficiency to face the many challenges, including the need for
improved registration, standardisation, integration and exchange of data and information,
the fostering of patient centricity and the push towards a better quality and efficacy of cure
and care. To date, the business requirements of the hospital are not always aligned with
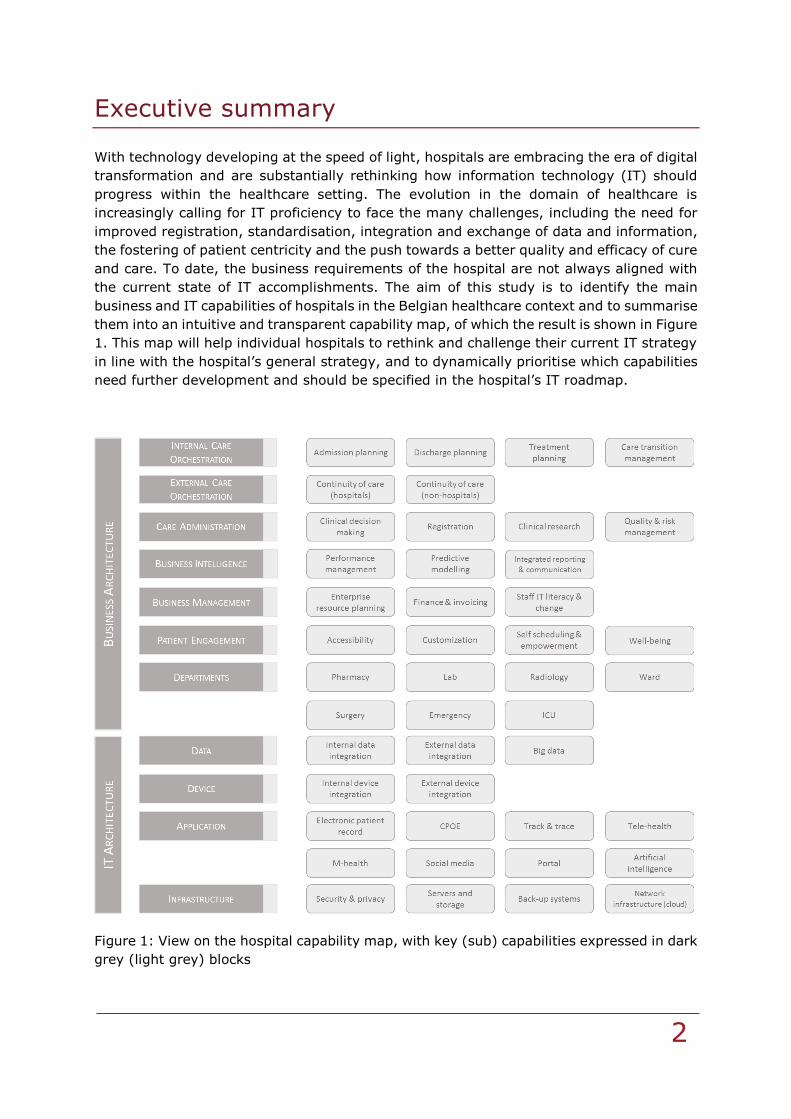
the current state of IT accomplishments. The aim of this study is to identify the main
business and IT capabilities of hospitals in the Belgian healthcare context and to summarise
them into an intuitive and transparent capability map, of which the result is shown in Figure
1. This map will help individual hospitals to rethink and challenge their current IT strategy
in line with the hospital’s general strategy, and to dynamically prioritise which capabilities
need further development and should be specified in the hospital’s IT roadmap.
Figure 1: View on the hospital capability map, with key (sub) capabilities expressed in dark
grey (light grey) blocks
Our solution to your specific needs
3
The research trajectory did comprise two phases. In a first phase, we made ourselves
familiar with the recent context and evolution in the field of hospital information
technology, and interviewed many different stakeholders to learn from their view on recent
IT developments and needs. In a second phase, these insights, together with a view on
recent business literature, led to the creation of a capability map that was iteratively refined
in discussions with hospital executives, mainly on the level of CEO and CIO. We
acknowledge that the choices leading to the capability map of Figure 1 aren’t exact science
and will always leave room for interpretation, adaptation and future changes.
By means of multiple hospital case studies, we illustrate that the capability map can be
used as a heat map to quickly screen the different capabilities and their state of
development within a specific hospital setting. We point out, however, that our model is
not to be confused with a maturity assessment model and therefore does not list specific
scales to measure every (sub) capability. From the case studies, and without aiming to
generalise for the entire Belgian hospital scene, we notice that there is a large variability
by which the capabilities are developed. On the level of the individual hospital, this
variability shows between (i) the key capabilities of a hospital and (ii) the various sub
capabilities that constitute a particular key capability. When comparing the results over the
different cases, we also observe that results substantially differ between the hospitals, thus
indicating that substantial room for improvement exists.
An interesting question is whether all hospitals should develop the same capabilities and if
we therefore should put a joint IT roadmap forward. From the interviews and cases, we
conclude, e.g., that the implementation of the electronic patient record (EPR) is receiving
utmost attention nowadays and constitutes an IT project that many hospitals share. This
seems a sound choice, since the EPR impacts directly or indirectly almost all of the
capabilities that are listed. We do see, though, from the cases that some hospitals are
already actively thinking about the EPR implementation on a network level, while others
are still working hard to get an integrated EPR within their own hospital entity. Apart from
the EPR project, though, it is less clear which capability needs to be prioritised. Given the
differences in the current state of IT among hospitals, and the differences in general
strategy defined by the hospitals, we argue that a one-size-fits-all IT roadmap might
eventually not be desirable. Instead, we recommend hospitals to use the capability map
and pinpoint their own capabilities of interest for the near future. The capability map will
allow them to add relationships between capabilities and reason on the necessary
development of other supporting capabilities given their prioritisation, therefore making it
a dynamic instrument.
Our solution to your specific needs
4
Introduction
Before jumping to the research question (next section), this introduction should provide a
brief overview of the hospital’s information technology (IT) challenges. We also verify
whether these challenges are in line with the general (non-hospital) reality about digital
transformation.
IT challenges for hospitals
Hospitals are facing an overwhelming multitude of challenges. While the amount of
diseases globally continues to grow as a result of the ageing population, health inequality
or people’s lifestyle, the spending of
hospitals keeps rising at unsustainable
rates (Tooke, 2015). Hospitals are
therefore increasingly being pressed by
governments and other stakeholders to
deliver high quality care to patients at the
lowest cost possible. The effective sharing
of relevant information within and
between hospitals has not only proven to
significantly lower hospital costs by
avoiding the duplication of cure and care
practice, it can also substantially lower
the amount of incorrect drug
administrations, the amount of
miscommunications, illnesses and
deceases that could and should be
prevented (Grossman, 2013; Robben,
2015; Vanaudenaerde, 2015). In other
words, information and communication
technologies and processes have the
power to boost the value that hospitals
can deliver to their patients, while
simultaneously lowering the costs to do
so. To reach this double aim, IT should
not only be perceived as a supportive
tool, but as an integral part of the entire
healthcare process.
But even though the healthcare industry
is among one of the most transaction-
intensive industries, Belgian hospitals
have traditionally been lagging in terms
of the implementation and alignment of
their IT, which is one of the reasons why
the Belgian federal government and other
stakeholder institutes are pressing hospitals to put IT as one of the highest priorities on
Methodology
To identify today’s most relevant challenges
about information and communication technology
in hospitals, we did apply a stakeholder
perspective. We interviewed first a series of
relevant non-hospital stakeholders who
frequently and directly interact with hospitals or
are seen as professional specialists in the field of
IT in the healthcare industry. The stakeholders we
interviewed include the NIHDI/RIZIV/INAMI (Ri
de Ridder), the Federal E-health platform (Frank
Robben), the Advisor of the Minister of Social
Affairs and Public Health (Frank Ponsaert), the
Advisor of the Minister of Health of Walloon
Region (Philippe Henry de Generet, written
communication), the Advisor of the Minister for
Welfare, Public Health and Family of Flemish
Region (Caroline Verlinde, Regine Van Ackere,
Wim Vanslambrouck), the Belgian Association for
Doctors' Syndicates (Marc Moens), the CIN-NIC
(Bernard Bolle), the Red Cross (Dominiek
Vanaudenaerde) and the Flemish Patients’
Platform (Roel Heijlen). The authors are very
grateful for these opportunities and would like to
thank all interviewees for their contribution.
Insights derived from the interviews are
complemented by a literature review of recent
business studies (see Bibliography). The insights
derived from the interviews and the literature
were presented and discussed during a workshop
exclusively for hospital directors. The
complementary learnings and discussion of this
workshop are integrated in this section of the
report. Furthermore, the opinion of hospitals is
addressed in detail later in this document by
means of case studies.

Our solution to your specific needs
5
their agenda via policy initiatives such as the action plan1 concerning ehealth listing 20
action points to grow IT in the healthcare sector. One action point that is recently
accelerated because of it’s central role to achieve many other action points concerns the
implementation of the electronic patient record (EPR), for which recently a set of Belgian
Minimum Use Criteria2 (BMUC) and according stages of development have been identified.
Overall, we should be fostering the move towards increased patient centricity in the
decision-making processes of hospitals via transparency and exchangeability of patient
information (Groves et al., 2013; Ponsaert, 2015; Robben, 2015; Verlinde et al., 2015).
The reasoning behind this is that all decisions, including those concerning IT, should
predominantly be based on the benefit for the patient, which is more than often not yet
the case. At this moment, IT and their related processes within and between Belgian
hospitals are unstructured, fragmented, not sufficiently integrated or standardised, and
not supported with sufficient resources. Addressing and overcoming these barriers would
simultaneously boost the quality of care to patients and significantly lower the costs
incurred by Belgian hospitals. The next paragraphs specify the barriers that ought to be
tackled to yield a more efficient hospital environment in Belgium.
FRAGMENTATION: The complexity of the organisational design of hospitals has traditionally
made it very challenging to implement healthcare IT and processes effectively. When
comparing the process of care with a typical manufacturing process, it quickly becomes
apparent that the amount of people, units and technologies involved to ‘process’ one
patient is significantly larger and more variable in comparison with other industries (Wager
et al., 2013). This complexity has resulted into the fragmentation of organisational
structures that now operate as silos within and between hospitals. To enable the sharing
of information between healthcare providers, payers and patients, the development of IT
infrastructures within and between hospitals is a fundamental necessity. The responsibility
to limit and remove fragmentation of IT technologies and processes within hospitals mainly
lies with the hospital management. To overcome fragmentation of IT and processes
between hospitals, the reorganisation into mergers and collaborative networks of hospitals
have been brought forward as solutions (Weil, 2000; Moens, 2015). Recently, Belgian
hospitals are already becoming connected by starting to organise themselves mainly as
networks. Efficient, digital hospitals take the lead in this step by positioning themselves as
extensive metahubs where health information is centralised (PwC, 2013; Verlinde et al.,
2015). However, there is still a long way to go before this barrier is overcome. For instance,
general practitioners in Belgium often still operate independently, rather than being part
of a network.
INTEGRATION AND STANDARDISATION: Multidisciplinary, integrated and interchangeable patient
files with both technological and semantic standards are not yet present within or between
hospitals, even though it would lower hospital costs while improving healthcare quality
(Robben, 2015). Integration links the efforts of organisational units through shared data.
The benefits of integration include increased efficiency, coordination, transparency and
agility (Ross et al., 2006). To a large degree, medical information exchange has been
1 For more information on the ehealth action plan, please visit http://www.plan-egezondheid.be/ or
http://www.plan-esante.be/
2 The BMUC can be retrieved from https://www.health.belgium.be/en/node/28865. We also invite the reader to consult www.ziekenhuisEPD.be for latest details reported by the federal government on the EPR evolution and, e.g., retrieve results of the questionnaire on EPR status and alignment of
hospitals with the BMUC (2016).
Our solution to your specific needs
6
hindered by the lack of standards for data and transactions used by hospitals. Yet, with an
increase in chronic care and multimorbidity, the call for integration will only increase (De
Ridder, 2015). Standardisation would deliver efficiency and transparency across hospitals
while driving down costs (Ross et al., 2006; IBM, 2013). Standardisation has also been
slowed down as the health status and medical condition of a patient is difficult to describe
using comprehensive, coded data (Wager et al., 2013). By no means, though, IT should
be allowed to hinder therapeutic decision making (Robben, 2015; De Ridder, 2015).
Currently, there is no sufficient alignment between standards in primary, secondary and
tertiary care (Verlinde et al., 2015). Standardisation and integration of patient information,
moreover, is not straightforward as many issues arise around data privacy, security and
control (PwC, 2013; Moens, 2015; Robben, 2015). For instance, physicians only require
access to the information needed to support their clinical decisions in the context of the
task being performed, not all the information about a patient should be made available in
all cases. Integration and standardisation also brings up the issue of a potential rise of a
monopoly of a health IT provider in Belgium, which is advised by all stakeholders to be
averted. But the integration and standardisation of IT systems without monopoly can only
be feasible if IT technologies of the software providers are programmed to be able to share
information with each other (Robben, 2015; Verlinde et al., 2015). Interoperability of
health information and communication systems is therefore a necessary condition to
succeed. Another reason that health IT systems are not standardised is because hospitals
often develop and/or customise their health IT to create switching costs for their highly-
knowledgeable workforce. If a physician would switch to another hospital, they would have
to get used to and learn how to work with different software (Robben, 2015). The question
that arises here is whether it is ethical that IT systems and processes are used as switching
barriers to bind the physicians to the hospital while it would be more beneficial to the
patient if they would become more standardised. All interviews pointed out that there is a
clear and urgent need for standardisation concerning the electronic patient record (EPR),
in which the BMUC might be a first step. Denmark is often pointed out as successful
example of adopting an integrated EPR (e.g. Kierkedgaard, 2013). The difference in
political landscape, however, makes an exact imitation of the centralisation of IT for Belgian
hospitals improbable (Ponsaert, 2015). A more reasonable proposed solution for Belgian
hospitals would be to centralise the data in hubs, while the ownership and source of patient
information is kept decentralised. Nevertheless, all interviewees agreed that the
development of the EPR is one of the top priorities for hospitals in Belgium at this time.
RESOURCES: There has historically been an underinvestment of resources, both with respect
to human and capital, in hospital information systems. The resulting restricted/limited
adoption of information and communication technologies still constitutes the source of
many of the issues that hospitals are facing today. This has to do with the inadequate
budgets that have been granted to Belgian hospitals and/or the meager amount of budget
that is distributed towards IT projects within hospitals. When questioning our interviewees,
many indicated to have no view on current IT budgets within hospitals, though.
WORKFORCE: Change management within hospitals is also seen as a substantial barrier that
needs to be overcome. Hospital workforces are often not willing to alter their activities and
behaviour in response to changes in the IT systems (Deloitte, 2015). Autonomy and
transparency of health activities are two main issues that lay at the cause of this reluctance
to adopt new IT systems (Ponsaert, 2015). In addition, physicians nowadays do not receive
any IT training during their education or professional career, so they often do not realise
the strategic value that IT can offer to them (PwC, 2013). Government incentives and

Our solution to your specific needs
7
initiatives stay recommended to stimulate change in hospitals, but are not sufficient on
their own to bring change in the behaviour. The hospital workforces must have a clear
understanding and take the initiative themselves to change their activities and behaviour
in function of the benefit for the patient. Realising success in digital transformation also
requires senior clinical professionals and health IT leaders to define in common an
achievable vision that addresses the relevant challenges (Deloitte, 2014). Thinking about
IT should not only be a task for IT people (De Ridder, 2015). In essence, we really need
to manage change (Robben, 2015; Ponsaert, 2015).
PATIENT ROLE: The expectations of the patients are shifting and the ‘my patient’ view during
treatment needs to fade (De Ridder, 2015; Heijlen, 2015). Patients are becoming
increasingly more informed and therefore will start to make their decisions less and less
based on which hospital is closest, but instead based on the quality of the specific physician
or health service (Verlinde et al.; 2015). In the future, patients might also contribute more
to the care they receive, i.e. they will also provide information to the care institution by
means of mobile technology. Having a more participative patient might also call for working
towards a more responsible patient and being more clear on what can and will be expected
from his/her side.
M-HEALTH: Currently, m-health is often not yet cost-competitive as compared to other
digital health processes since the eco-system around m-health still needs to be developed,
which takes time. In order to capture data from m-health, an eco-system of knowledge
centres, administrators, legislators and big data systems should be set up (Deloitte, 2015;
Robben, 2015). The added value of m-health on the health care process is expected to be
substantial as smartphones offer new ways of engaging with patients (PwC, 2014), but
should not be overrated (Ponsaert, 2015). The healthcare is becoming increasingly more
digitised, as electronic systems are replacing the paper-based systems, opening a gateway
for innovation. More and more sophisticated mechanisms are reaching the market but they
are often hindered as they remain unregulated (PwC, 2013).
It has become clear that Belgian hospitals are facing a multitude of intertwined challenges
in terms of information and communication technologies. In summary, our interviewees
indicate that major challenges lie ahead w.r.t. the EPR, integration, standardisation,
change management, and all of this while putting the patient forward.
Focus on digital transformation
A question that might arise is whether the challenges hospitals have concerning digital
transformation (i.e. the end-to-end integrated business transformation where digital
technology plays a dominant role) are to some extent similar to, or at least in line with,
those of many other industries. In other words, do we also find similar spearheads and
focus points in other industries and settings. To have a view on this, we connect to the
Our solution to your specific needs
8
ExConomy3 framework (Viaene and Danneels, 2015): what are the realities that are
currently driving the digital economy in a broad and general context?
REALITY 1 - Customer Experience is Value: In the digital space, customers will take the lead
and companies need to think more from outside-in instead of inside-out. For healthcare,
this implies that the patient will (finally) take its central position in the healthcare eco-
system, and that services should be built around the patient instead of the healthcare
institution.
REALITY 2 - Customers are moving targets: Companies cannot assume that value
propositions that work today will still be effective tomorrow. Therefore, they need to more
actively and intensely track and follow what the customer is doing and what he/she wants
to achieve (entering the field of big data). For healthcare, it implies that we need to better
monitor the (perhaps even healthy) patient to better answer upcoming and changing
needs. Patient loyalty will disappear in the digital space.
REALITY 3 - Collaboration reshapes strategy and business models: The company on its own
will not have enough strength and offering to fulfill the customer’s needs. Therefore, it
needs to partner with others who excel in complementary capabilities and skills and go
together in targeting the customer. In healthcare, this can be seen as the search for
alliances between hospitals and the formation of care networks to build a strong eco-
system that offers a continuity of care.
REALITY 4 – Eco-system platforms boost value co-creation: The eco-system will only flourish
if there is a performing underlying platform that allows for making the collaboration
happening. This means that your data needs to be combined with data of others, in an
integrated and equally important flexible way. For healthcare, this points to the need for
an easy and safe integration of data with the partners in the healthcare alliance and eco-
system. Enterprise Architecture (EA) helps to build this platform, and especially the use of
APIs (Application Program Interfaces) comes to the forefront for sharing data externally
(with nowadays already many applications in ,e.g., the travel and banking sector).
In essence, it is not so hard to see that these four realities easily transfer to the healthcare
setting, which shows that at least the core of the challenges seem to be universal and
learnings can be taken from general insights on digital transformation too.
3 Listen to what Prof. Dr. Stijn Viaene has to say about the ExConomy framework on
https://www.youtube.com/watch?v=OIx5IDK-WPo

Our solution to your specific needs
9
Research question
The many IT challenges make that it is not straightforward for hospitals to decide upon
focus points in the development of an appropriate IT strategy. The objective of this study
is twofold.
First, we aim to construct a high-level capability map that should help hospitals to identify
strengths and deficiencies in their current IT support of the required set of business
capabilities. It is important to state that we do not aspire to develop an IT maturity
assessment model. A well-known maturity model for the electronic medical record is, e.g.,
provided by the EMRAM4 model of HIMSS. For a general and recent view on the state of
maturity models for hospital information systems, we refer to Carvalho et al. (2015) who
state that maturity models for hospital information systems can be significantly improved.
In their research, they indicate that “the models pertaining to the health field are poorly
detailed, do not provide maturity measuring tools and do not structure the characteristics
of maturity stages according to influencing factors”. More in the interest of this research
study, we want to develop a concise and visual structure that supports professionals who
are looking to quickly overview the digital offering of their hospital from different angles
and in line with the major capabilities that are expected from a hospital setting.
Second, by applying this capability map to some hospitals residing in the Belgian healthcare
landscape and developing small case studies, we hope to identify some patterns that will
hint directions for future digital development. We want to show how the capability map
can be used to move from a static tool, in better understanding the current status, to a
dynamic tool that helps identifying which capabilities to develop given the strategic choice
a hospital is making, leading to the start of designing an IT Roadmap. Since hospitals might
substantially deviate in the current status of their capabilities, as will be shown by the
cases and which was also put forward by the interviews (e.g. Ponsaert, 2015), we do not
intend to generalise one advice for all hospitals. It is in our opinion more useful to show
how choices of capability development impact different capabilities and initiate different
calls for IT development.
4 EMRAM is a maturity model developed by HIMSS with eight stages (0-7) to measure the level of
electronic medical record (EMR) capabilities ranging from limited ancillary department systems to a paperless EMR environment. At Q4 of 2016, about 16 Belgian hospitals took the assessment, and two hospitals reached level 6 (UZ Brussel and CHU Liège). More information to be retrieved from
http://www.himss.eu/healthcare-providers/emram
Our solution to your specific needs
10
A view on a hospital’s capabilities
From the introduction, it shows that in general IT currently does not meet the business
expectations and aspirations of a healthcare organisation or eco-system. Enterprise
Architecture (EA) is often put forward as a methodology to bridge this gap, focusing on the
proper arrangement of elements into a reasoned structure. One could define EA as “the
fundamental organisation of a system embodied in its components, their relationship to
each other, and to the environment, and the principle guiding its design and evolution”
(IEEE Standard 1471-20005). Yet, there is a vaste choice of definitions in the literature,
mainly focused on the outcome of architecting, but equally important one should consider
the process of architecting. We refer to Cumps et al. (2013) for an overview and the
evolution in the field of EA.
Enterprise Architecture is generally considered to comprise both Business Architecture and
IT Architecture. Business Architecture traditionally covers the capabilities of an
organisation (what do we want to do), the organisational structure into different domains,
and the processes that are installed to reach the goals and objectives (how do we want to
realise the capabilities). While processes can more easily change over time, the capabilities
are seen to be more stable. Therefore, decomposing the services and activities of an
organisation in terms of capabilities -
essential basic building blocks - helps to
provide a high-level structure. This
decomposition can be visually summarised
by means of a capability map. The IT
Architecture should consequently be built
to support an organisation in reaching and
developing its capabilities in particular,
and to fit the Business Architecture as a
whole. Therefore, an effective capability
map creates a foundation for execution
and ensures alignment between business
processes and IT (Ross et al., 2006).
Digitisation of hospitals is advised to be
driven by architecture that delivers
capabilities to support services and
processes (Deloitte, 2015).
Figure 1 provides an overview of the
capability map we developed for this
study. It follows the EA structure and
makes a difference between the Business
Architecture and the IT Architecture.
These two main parts show a (non-exhaustive) breakdown in key capabilities (such as
internal care orchestration, external care orchestration, etc.) which on their turn will list
some important sub capabilities (such as admission planning, discharge planning, etc.). In
5 http://standards.ieee.org
Methodology
To build a capability map that fits the Belgian
context and that balances conciseness with
sufficient level of detail, we did use an iterative
process of refinement. In an initial step we did
base ourselves on our own experience of the
operating model of Belgian hospitals, recent
trends, and on frameworks retrieved from
recent business studies, listed in the
bibliography. In a second step, the capability
map was taken to discussion with a number of
practitioners and professionals in the field of
IT/hospital/healthcare. Consequently, we have
been testing and validating the capability map
with four hospitals by means of semi-structured
interviews. After every case we did refine the
map based on feedback or requests for
clarification. Developing a capability map is
difficult as it forces management to frame a
simple vision of a complex organisation. We are
therefore very grateful to the participating
hospitals of the case studies, and in particular to
the interviewees for sharing their insights and
constructive suggestions along the discussions.
Our solution to your specific needs
11
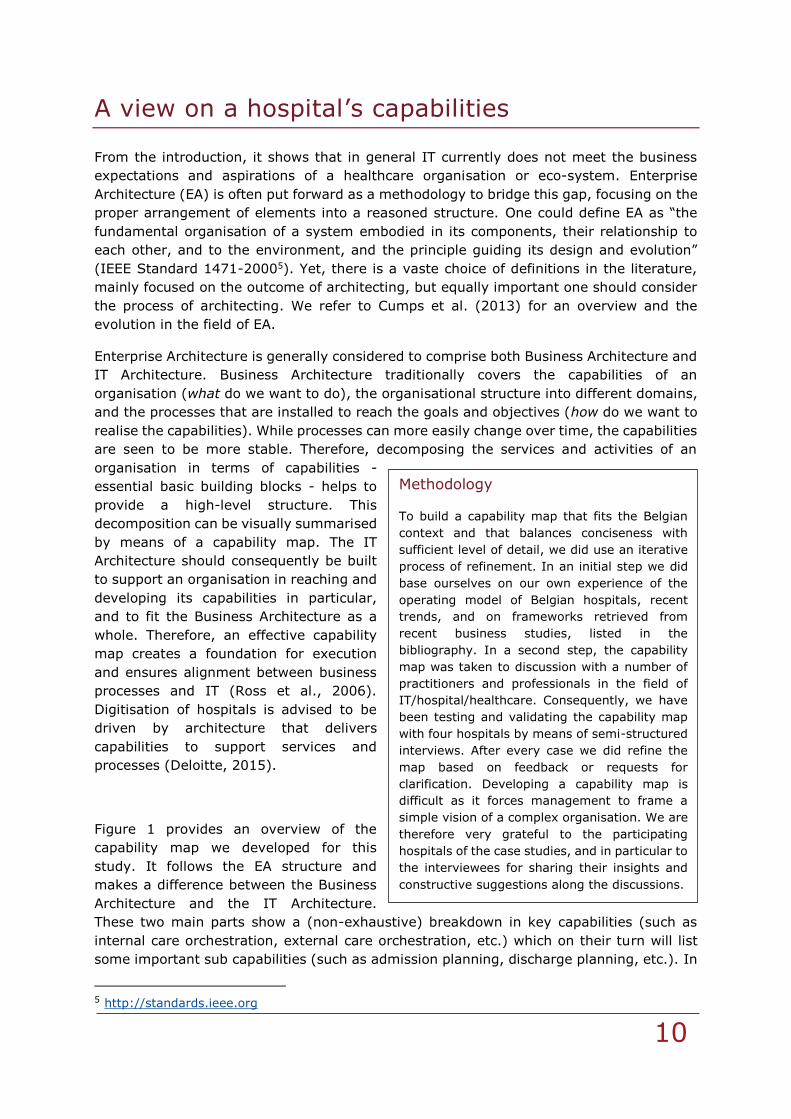
the remainder of this section, we will briefly clarify and situate the different (sub)
capabilities to create a joint understanding and to enhance reasoning with the capability
map.
Figure 1 (bis): View on the hospital capability map, with key (sub) capabilities expressed
in dark grey (light grey) blocks
Business Architecture
INTERNAL CARE ORCHESTRATION: The careful planning, arranging and automation of
composite care services and processes for the patient from the moment he/she enters the
hospital until he/she leaves the premises of the hospital.
ADMISSION PLANNING: The careful planning and managing of the act of admitting
patients or allowing them to enter in the care services of the hospital. This capability
typically involves the inpatient setting and therefore also relates to proper bed
management capabilities.
Our solution to your specific needs
12
DISCHARGE PLANNING: The formulation and planning to release a patient from the care
services of the hospital, here limiting the focus to connecting all information and
stakeholders from inside the hospital entity (<> external care orchestration).
TREATMENT PLANNING: The planning and managing of the actions and methods of
treating patients medically (ambulatory visit/consultation) or surgically.
CARE TRANSITION MANAGEMENT: The planning and managing of transferring a patient
to another (clinical, organisational or nursing) unit within the hospital.
EXTERNAL CARE ORCHESTRATION: The careful planning, arranging and automation of
composite care services and processes for the patient with healthcare institutions and
stakeholders that are not formally part of the hospital entity.
CONTINUITY OF CARE (HOSPITALS): Managing the information exchange and transition
of care for the patient with other hospitals in healthcare eco-system (e.g. those not
being a member of the hospital’s collaborative network, etc.).
CONTINUITY OF CARE (NON-HOSPITALS): Managing the information exchange and
transition of care for the patient with agents other than hospitals in the healthcare
eco-system (e.g. general practitioners, patients, clinical remote ancillary services
(labs), elderly care, etc.).
CARE ADMINISTRATION: Encompassing the activities that relate to the administration of
care (so patient perspective) and the respective registration of input and output (also
outcome-related).
CLINICAL DECISION MAKING: The act of making informed medical decisions that might
be supported or even hinted by automated and predictive IT support.
REGISTRATION: The act of registering information in the hospital information system,
such as active or past diagnoses, patient identification, informed consent,
medication usage, nursing information, etc.
CLINICAL RESEARCH: Supporting the clinical trials by means of technology, e.g. for
aggregating results, sharing datasets or selecting patients.
QUALITY & RISK MANAGEMENT: Capability of preserving and guaranteeing qualitative
and safe healthcare, encompassing hospital accreditation or drug-drug interaction
screening, but also outcome-based analysis turning to the field of value-based
healthcare.
BUSINESS INTELLIGENCE: Technology-driven capabilities for analysing data and presenting
actionable information to help hospital executives, managers and other end users to make
better informed decisions.
PERFORMANCE MANAGEMENT: The assessment of employees, processes, resources or
other factors to gauge progress towards predetermined strategic objectives of the
hospital (e.g. dashboards).
PREDICTIVE MODELLING: The identification, analysis, assessment, control and
avoidance or elimination of unnecessary risks via data-mining technologies that are
used to analyse historical and current data in order to help predict future outcomes
or behaviour. While the emphasis here is on the business perspective, also clinical
Our solution to your specific needs
13
predictive modelling might be an important capability (but resides under care
administration - clinical decision making).
INTEGRATED REPORTING & COMMUNICATION: This is the embedded and detailed reporting
and communication of a clear, concise and integrated overarching picture of a
hospital’s ability to produce value over time for different stakeholders. It
incorporates the reporting and communication of data analysis results of the real-
time data hospitals generate and gather from their day-to-day operational
activities.
BUSINESS MANAGEMENT: Activities associated with effectively and efficiently running,
controlling, leading, monitoring and organising a hospital.
ENTERPRISE RESOURCE PLANNING (ERP): The accounting oriented, relational database
based, multi-module but integrated software activity for identifying and planning
the resource needs of a hospital. ERP provides a user-interface for the entire
organisation to manage product planning, materials and parts purchasing,
inventory control, distribution and logistics, production scheduling, capacity
utilisation, order tracking as well as planning for financial and human resources.
FINANCE & INVOICING: The planning, directing, monitoring, organising and controlling
of the monetary resources of a hospital, including the billing process.
STAFF IT LITERACY AND CHANGE: The level of familiarity and expertise of the hospital’s
workforce with the basic hardware and software concepts and the willingness to
adopt changes in the implementation of the basic hardware and software.
PATIENT ENGAGEMENT: Actions and interactions hospitals make with their patients to obtain
greater benefit from the healthcare services they provide. These actions might take place
on both the administrative and clinical level.
ACCESSIBILITY: The easy to approach, reach, enter and use of services by patients
within and outside of the hospital, e.g. accessibility of the patient towards his/her
own medical record.
CUSTOMISATION: Tailoring of the services to the patient’s particular and individual
needs, e.g. information sharing or handling questions.
SELF SCHEDULING & EMPOWERMENT: The extent to which the hospital enables the patient
to undertake actions and decisions themselves, instead of hospital staff or a
scheduler. By empowering the patient, the hospital often seeks cost reduction while
increasing customer value and experience.
WELL-BEING: Act of following and considering a healthy ‘patient’ instead of focusing
on the curative aspect of care, therefore moving the organisation in the direction of
preventive healthcare.
DEPARTMENTS: Activities and services provided by the hospital’s main medical-technical
departments or units, including the pharmacy, laboratory, radiology, wards and nursing
units, operating theatre and sterilisation unit, emergency department and intensive care
unit.
Our solution to your specific needs
14
IT Architecture
DATA: Information in raw, structured or unstructured form that represents conditions,
ideas or objects relevant to the hospital.
INTERNAL DATA INTEGRATION: The combination of technical and business processes
used to combine data from different sources within the hospital.
EXTERNAL DATA INTEGRATION: The combination of technical and business processes
used to combine data from different sources from the outside the hospital with the
hospital.
BIG DATA HANDLING: Is the analysis, sequencing and monitoring of high-volume, high-
velocity and/or high-variety information that is recorded on a (semi-)continuous
basis. We differentiate big data from big data sets.
DEVICES: We refer to devices as instruments, appliances or equipment, whether used alone
or in combination, including the software intended by its manufacturer to be used for
administrative, diagnostic and/or therapeutic purposes by health professionals to support
patient care.
INTERNAL DEVICE INTEGRATION: The capability of integrating and connecting devices
owned by the hospital to the hospital information system and IT services.
EXTERNAL DEVICE INTEGRATION: The capability of integrating and connecting devices
owned by other stakeholders than the hospital (e.g., bring your own device tablets
or personal computers, smartphones, etc.) to the hospital information system and
IT services, regardless whether the devices are physically present in the hospital or
remote.
APPLICATIONS: Programs that are developed to perform specific functions, either stand-
alone or as input for other programs/applications.
ELECTRONIC PATIENT RECORD: An EPR (or equivalently electronic health record)
contains the standard medical and clinical data gathered by the healthcare provider
(i.e. the electronic medical record), next to ,e.g., nursing data and medication
information so to include a more comprehensive patient history.
COMPUTERISED PHYSICIAN ORDER ENTRY - CPOE: An application to fulfill the e-
prescription of medication, but in the broader sense also for non-medication orders
as those performed by the lab or radiology. The CPOE is often seen as part of the
EPR.
TRACK & TRACE: Applications that foster tracebility and/or localisation of
patients/instruments/equipment/medication/etc. and contribute to health safety
and efficiency.
TELE-HEALTH: Remote communication about and/or surveillance of clinical issues by
means of multi-media technology. Examples include teaching sessions, virtual
physician consultations, tele-ICU, etc.
M-HEALTH: Mobile health applications that often relate to the usage of wearables or
smartphone usage and link to the concept of big data.
Our solution to your specific needs
15
SOCIAL MEDIA: Refers to the usage and exploitation of new media applications such
as facebook, twitter and alike in the healthcare organisation and communication.
PORTAL: Gateway or internet site that provides access or links to other sites, either
for internal use within the healthcare organisation or for external use directed
towards patients and other stakeholders.
ARTIFICIAL INTELLIGENCE: Applications in the field of algorithmic design and machine
learning applied to health data to support clinicial decision making.
INFRASTRUCTURE: IT infrastructure is the underlying base or foundation of all components,
facilities, services and installations that play a role in overall IT and IT-enabled operations
of a hospital. It refers to the composite hardware, software, network resources and services
required for the existence, operation and management of an enterprise IT environment. It
allows a hospital to deliver IT solutions, support and services to its employees, partners
and patients.
SECURITY & PRIVACY: The confidentiality, integrity and availability of data and the
ability of the hospital and patient to determine what data in a computer system can
be shared with third parties.
SERVERS & STORAGE: These are servers that are used to store, access, secure and
manage digital data, files and services. Its purpose is to store and provide access
to data over a shared network or through the internet.
BACK-UP SYSTEMS: The activity of copying, archiving and securing files and databases
in systems so that they will be preserved in case of equipment failure or a
catastrophe and to restore the orginal. It is usually a routine part of the operation
of a hospital.
NETWORK INFRASTRUCTURE (CLOUD): The capability to transfer data, especially huge
size data files, through the network. It also covers the technical features ensuring
the connectivity to the network for all stakeholders.
Our solution to your specific needs
16
A closer view on some Belgian hospitals
The goal of this section is to apply the framework of previous section to several hospital
cases and assess for every item of the capability map its current development status. To
do so, we interviewed the CEO and/or CIO and/or IT department head of the participating
hospitals and jointly discussed every building block of the framework. Since interviews are
a subjective means to acquire information and respondents might be less/more critical in
appraising the items, we tried to align for this during the talks. In the next subsections,
we briefly report on the general findings of every case and visualise the assessment by
colouring each item of the capability map, resulting in a heat map that allows for a quick
glance of the findings. The colour scaling has five stages and considers the following five-
scale range:
( ) - red: We are not actively working or thinking about this item; we are extremely
dissatisfied with our current status;
( ) - orange: The level of development we have is far below the standard and calls for
substantial improvement;
( ) - yellow: We achieve a level of development that fits the goals of today, but this
might not be in line with the challenges of tomorrow so that next steps should be taken;
( ) – light green: We reach a very acceptable and high level of development, which is
however not yet the ideal scenario we would like to realise;
( ) – dark green: This area cannot be further improved and is an area in which we for
sure excel.
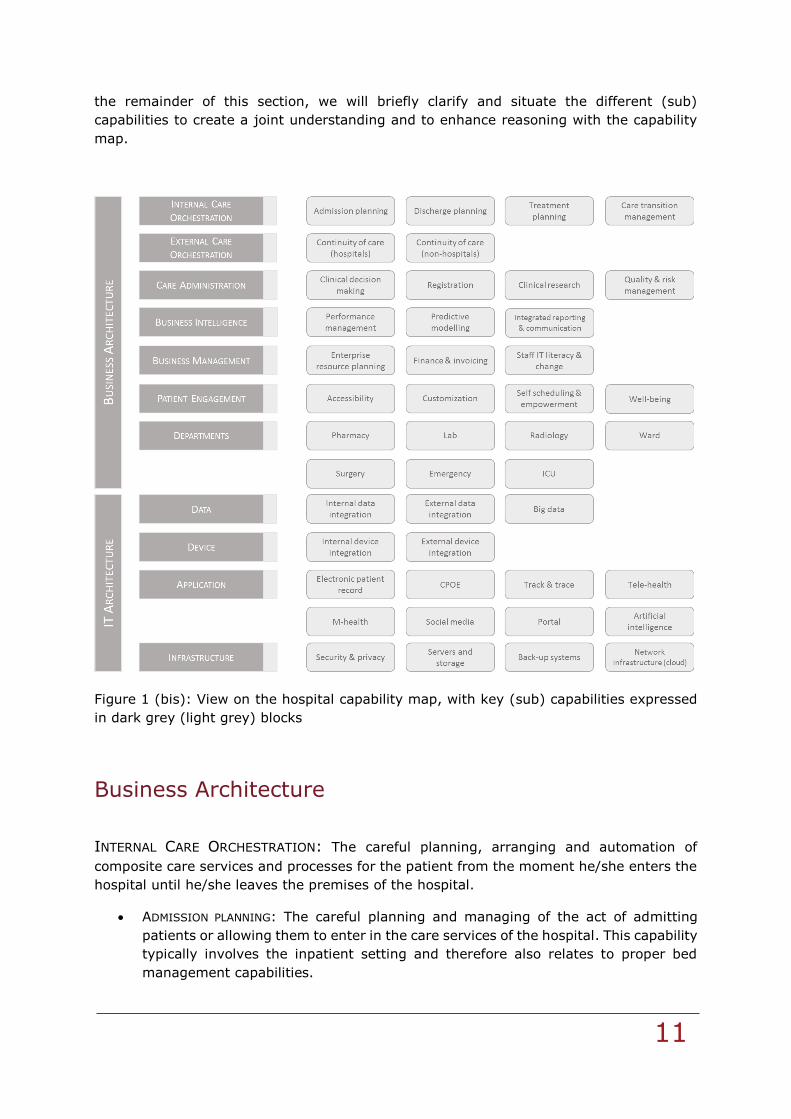
Case 1: large non-university hospital
The first case is about a large (general) non-university hospital with multiple sites, located
in the Flanders region. The hospital has made it’s primary goal to provide the best possible
care for its patients, with the patient as a central focal point around which all activities and
decisions evolve. The hospital currently strives to operationally align its processes and
technologies after the merger in order to become a fully modern and paperless hospital
within a period of 5 years. Yet, at this moment, senior management points out that their
IT is not up for this task. That is why they have committed themselves to fundamentally
change their IT strategy by implementing a number of actions, formulated in an elaborate
IT policy plan.
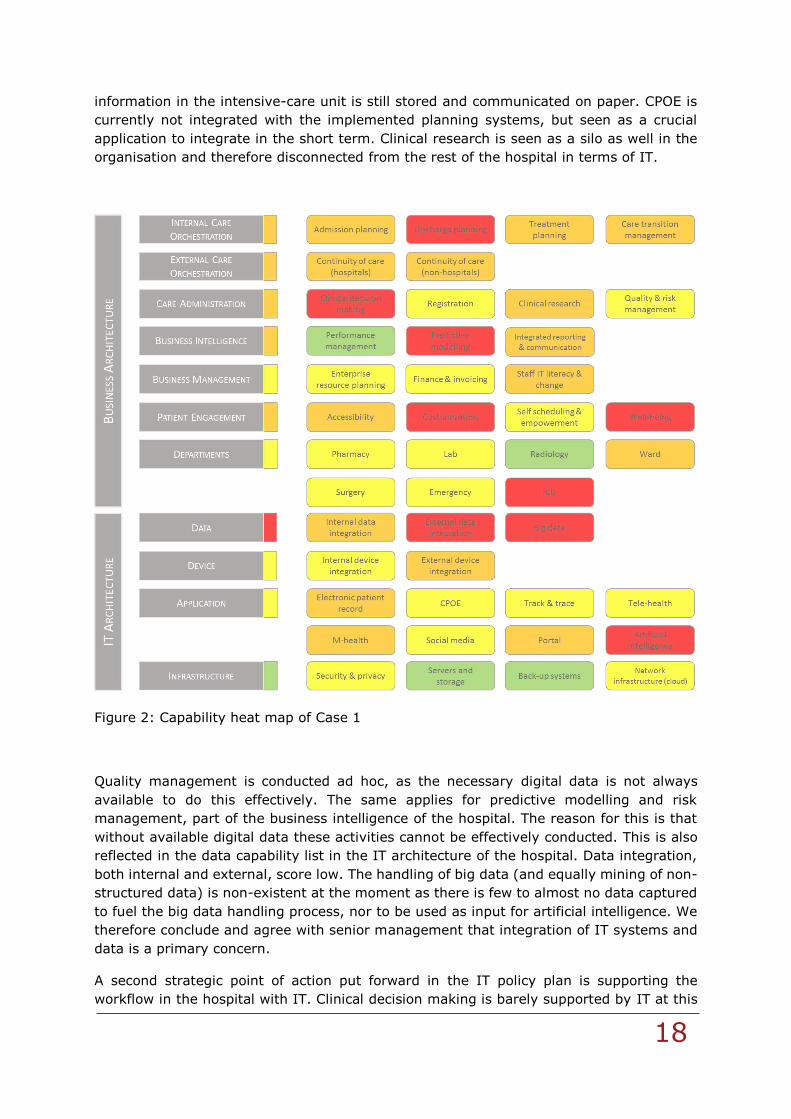
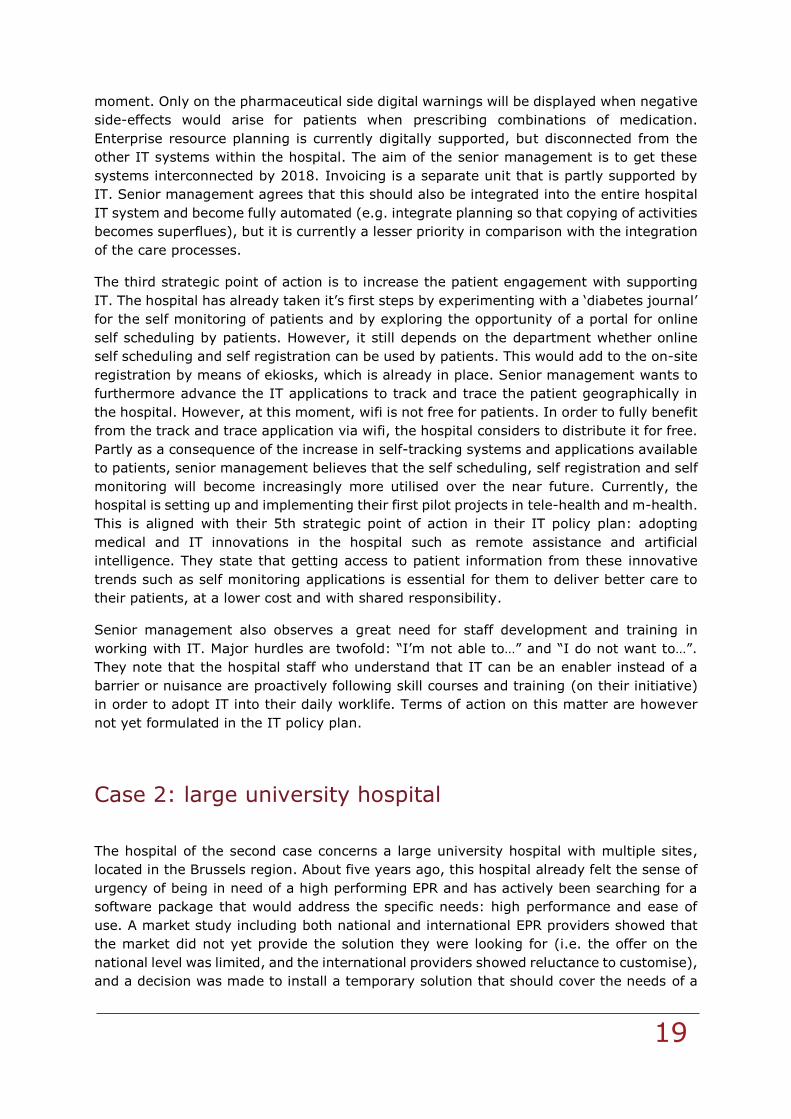
As can be derived from the capability heat map of Figure 2, the overall picture shows
substantial room for improvement in terms of IT. Especially the processes concerning the
orchestration of care of the patients seem poor at first sight. The senior management
indicates that an electronic patient record with standard typology is present, in which at
least patient information from the lab, radiology and pharmacy departments are digitally
stored and made available to external partners, but no more. The goal of senior

Our solution to your specific needs
17
management is to enhance the IT systems substantially in the following 5 years, centred
around the introduction of a new integrated EPR. To do this, 5 strategic action points are
formulated and being implemented as we speak:
1. Supporting care by better integrated IT
2. Supporting workflow with IT
3. Increasing patient engagement through IT
4. Supporting the healthcare network with IT
5. Adopting medical and IT innovations in the hospital
The senior management of the hospital has made the integration of their care processes
and systems their foremost priority in their strategic action plan, as they see this as a
major obstacle that explains the current undesired low state of digitisation. This hurdle
should be overcome first before other issues can be addressed/tackled. The internal care
orchestration is currently digitally underdeveloped. Admission and discharge planning is
mostly manual because there is no sufficiently detailed digital patient information available
as input for these activities. Currently registration of data is focused on what needs to be
provided to the government, not necessarily what’s needed for governance and
management. Moreover, the hospital management wants many of the registrations
(especially quality), instead of following the governmental reporting cycle, to become
continuous. The care transition management is described as rather archaic: e.g. hospital
staff needs to manually screen output to check whether the right patient is in the right
room. The configuration of the IT supporting treatment planning is not adequate enough,
but has at least stepped away from outlook, which made it a very time-consuming process
for the hospital staff. The lack of efficacy is also reflected in the business intelligence
activities of the hospital, for which they indicate that integrated reporting &
communications can be significantly improved, e.g. by moving to ‘self-service reporting’
instead of filing for reports in the respective department. The external continuity of care
for the patient now only happens occasionally with other hospitals. They show that there
isn’t sufficient information sharing between them and general practitioners outside of the
hospital: there is no prior information whatsoever on 95% of incoming patients in the
hospital who are not known to the hospital and do not bring their own letter with medical
information. The only information that is shared so far between hospitals and general
practitioners are the discharge papers and letters specifying medical content. To address
this issue, the hospital is deciding between two strategies in the 4th point of their action
plan: how to connect the network. Either they will opt for sharing patient information by
connecting and interfacing with existing yet scattered IT systems, or they will opt for one,
integrated system to be shared with all external partners. A difficult question remains about
who needs to take the orchestrator-role in the emerging field of networked healthcare:
patients, general practitioners or the hospital? If general practitioners want to take this
responsibility, the hospital states that they should then also get organised accordingly.
Actually, shouldn’t the patient be in the driver seat?
An additional reason for the lack of integration is that the departments inside the hospital
are still organised as silo’s. They should also be integrated in terms of their systems. Senior
management acknowledges that integrating care systems between departments can be
more difficult due to the lack of standards in semantics, typology and so forth, but they
agree that the patient care and administration planning should definitely become
integrated into one system. When comparing departments, they note that all the
Our solution to your specific needs
18
information in the intensive-care unit is still stored and communicated on paper. CPOE is
currently not integrated with the implemented planning systems, but seen as a crucial
application to integrate in the short term. Clinical research is seen as a silo as well in the
organisation and therefore disconnected from the rest of the hospital in terms of IT.
Figure 2: Capability heat map of Case 1
Quality management is conducted ad hoc, as the necessary digital data is not always
available to do this effectively. The same applies for predictive modelling and risk
management, part of the business intelligence of the hospital. The reason for this is that
without available digital data these activities cannot be effectively conducted. This is also
reflected in the data capability list in the IT architecture of the hospital. Data integration,
both internal and external, score low. The handling of big data (and equally mining of non-
structured data) is non-existent at the moment as there is few to almost no data captured
to fuel the big data handling process, nor to be used as input for artificial intelligence. We
therefore conclude and agree with senior management that integration of IT systems and
data is a primary concern.
A second strategic point of action put forward in the IT policy plan is supporting the
workflow in the hospital with IT. Clinical decision making is barely supported by IT at this
Our solution to your specific needs
19
moment. Only on the pharmaceutical side digital warnings will be displayed when negative
side-effects would arise for patients when prescribing combinations of medication.
Enterprise resource planning is currently digitally supported, but disconnected from the
other IT systems within the hospital. The aim of the senior management is to get these
systems interconnected by 2018. Invoicing is a separate unit that is partly supported by
IT. Senior management agrees that this should also be integrated into the entire hospital
IT system and become fully automated (e.g. integrate planning so that copying of activities
becomes superflues), but it is currently a lesser priority in comparison with the integration
of the care processes.
The third strategic point of action is to increase the patient engagement with supporting
IT. The hospital has already taken it’s first steps by experimenting with a ‘diabetes journal’
for the self monitoring of patients and by exploring the opportunity of a portal for online
self scheduling by patients. However, it still depends on the department whether online
self scheduling and self registration can be used by patients. This would add to the on-site
registration by means of ekiosks, which is already in place. Senior management wants to
furthermore advance the IT applications to track and trace the patient geographically in
the hospital. However, at this moment, wifi is not free for patients. In order to fully benefit
from the track and trace application via wifi, the hospital considers to distribute it for free.
Partly as a consequence of the increase in self-tracking systems and applications available
to patients, senior management believes that the self scheduling, self registration and self
monitoring will become increasingly more utilised over the near future. Currently, the
hospital is setting up and implementing their first pilot projects in tele-health and m-health.
This is aligned with their 5th strategic point of action in their IT policy plan: adopting
medical and IT innovations in the hospital such as remote assistance and artificial
intelligence. They state that getting access to patient information from these innovative
trends such as self monitoring applications is essential for them to deliver better care to
their patients, at a lower cost and with shared responsibility.
Senior management also observes a great need for staff development and training in
working with IT. Major hurdles are twofold: “I’m not able to…” and “I do not want to…”.
They note that the hospital staff who understand that IT can be an enabler instead of a
barrier or nuisance are proactively following skill courses and training (on their initiative)
in order to adopt IT into their daily worklife. Terms of action on this matter are however
not yet formulated in the IT policy plan.
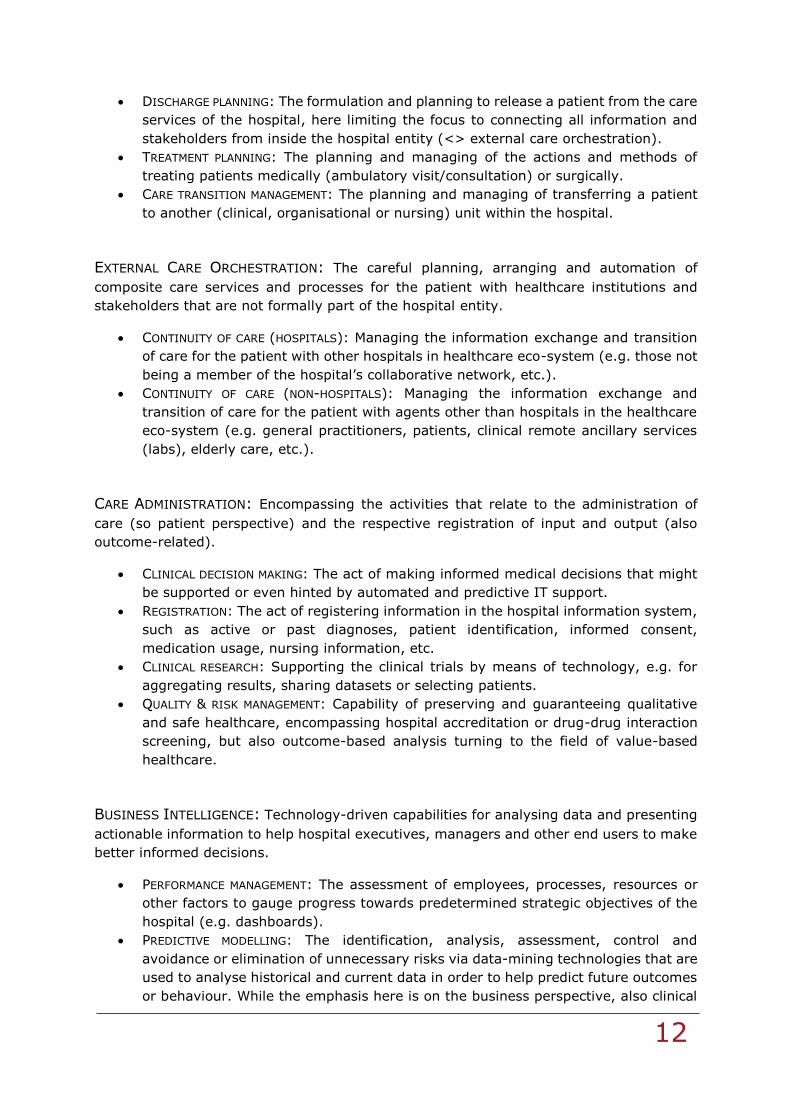
Case 2: large university hospital
The hospital of the second case concerns a large university hospital with multiple sites,
located in the Brussels region. About five years ago, this hospital already felt the sense of
urgency of being in need of a high performing EPR and has actively been searching for a
software package that would address the specific needs: high performance and ease of
use. A market study including both national and international EPR providers showed that
the market did not yet provide the solution they were looking for (i.e. the offer on the
national level was limited, and the international providers showed reluctance to customise),
and a decision was made to install a temporary solution that should cover the needs of a
Our solution to your specific needs
20
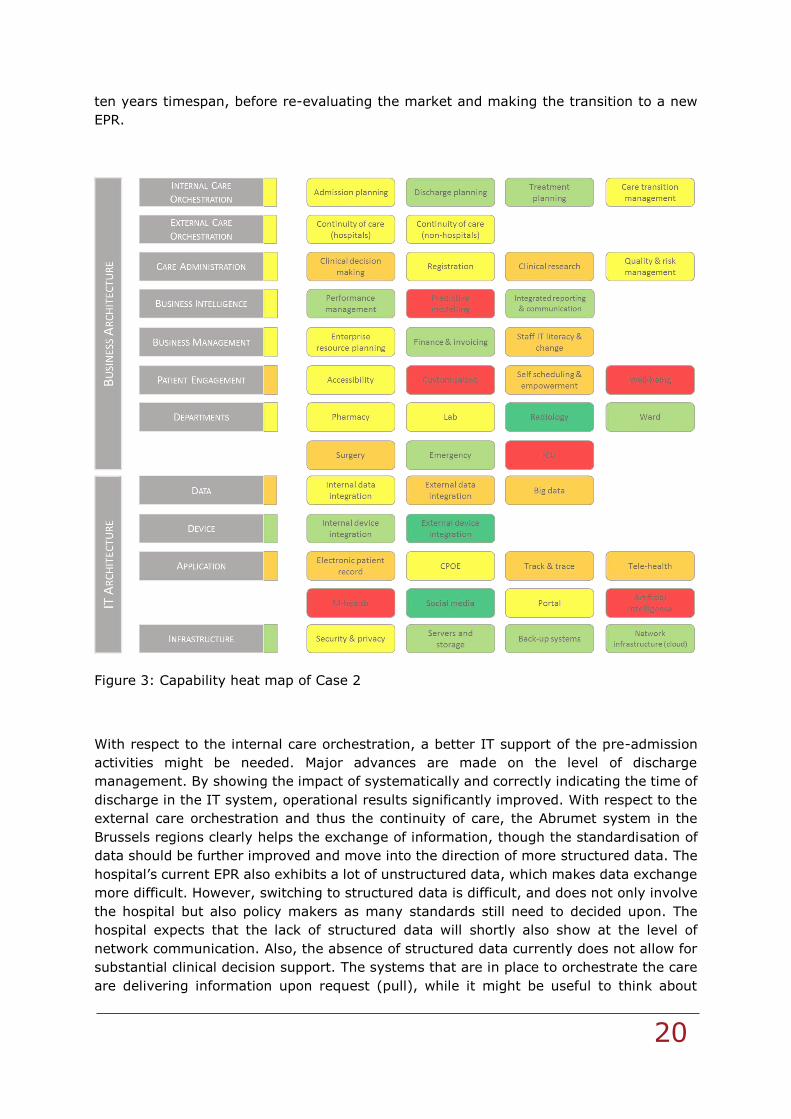
ten years timespan, before re-evaluating the market and making the transition to a new
EPR.
Figure 3: Capability heat map of Case 2
With respect to the internal care orchestration, a better IT support of the pre-admission
activities might be needed. Major advances are made on the level of discharge
management. By showing the impact of systematically and correctly indicating the time of
discharge in the IT system, operational results significantly improved. With respect to the
external care orchestration and thus the continuity of care, the Abrumet system in the
Brussels regions clearly helps the exchange of information, though the standardisation of
data should be further improved and move into the direction of more structured data. The
hospital’s current EPR also exhibits a lot of unstructured data, which makes data exchange
more difficult. However, switching to structured data is difficult, and does not only involve
the hospital but also policy makers as many standards still need to decided upon. The
hospital expects that the lack of structured data will shortly also show at the level of
network communication. Also, the absence of structured data currently does not allow for
substantial clinical decision support. The systems that are in place to orchestrate the care
are delivering information upon request (pull), while it might be useful to think about
Our solution to your specific needs
21
systems that push information without ending with an overload of (not useful) information.
The hospital is furthermore not sure who should be the gatekeeper when dealing with
continuity of care. The most obvious professional here would be the general practitioner.
Quality and risk management is currently focused on tracking and resolving incidents. A
systematic view on the feedback of patients, or medical outcome is yet to be developed.
Next to the IT challenge of producing integrated reports on quality and performance, an
even more important question raises on how outcome and performance should be reported.
With respect to the latter, the hospital points to a multitude of registrations and
opportunities, yet predictive modelling seems to be minimal.
Although the hospital provides an opportunity to request appointments online (which still
need to be confirmed and booked though by staff), the hospital is not yet empowering the
patient to a large extent.
The systems of the departments of the hospital (and those to support clinical research)
substantially differ in the level of digitisation and use of paper. This difference also shows
over the different sites. The management acknowledges that the transition from paper to
IT, or just changes in IT practice, are not always easy to implement and that more attention
should go to change management. In the transition, it is key to show the added value of
the new IT application or system (cf. example on discharge management), though this is
often perceived to be a challenge. The ultimate idea is to have a fully integrated IT system
that connects all currently often fragmented pieces of information in the hospital. The
hospitals points to the subtle but important difference between ‘integrating’ and
‘interfacing’, where interfacing merely points to connecting the bits and pieces, while
integrating is creating added value through the system. For instance, value is created when
medication is automatically added to the invoice of the patient, medication stock levels are
updated, replenishment is triggered and if needed new procurement orders with the
supplier are instantaneously sent out. With respect to some other key applications in the
hospital, mixed results are obtained. Whereas the CPOE is well-developed for the e-
prescription of medication, it needs further attention when assessed in the broader sense
of orders. Tele-health is restricted to remote sessions for medical education. Big data, M-
health and artificial intelligence are not yet the order of the day. The hospital, though,
actively manages its social media.
The IT infrastructure is up-to-date. From a technical point of view, the evolution to having
more data centrally available (e.g. think about PACS and imaging) might push the limits
of the storing and network technology, which actually should allow for easy access
regardless the file size.
Our solution to your specific needs
22
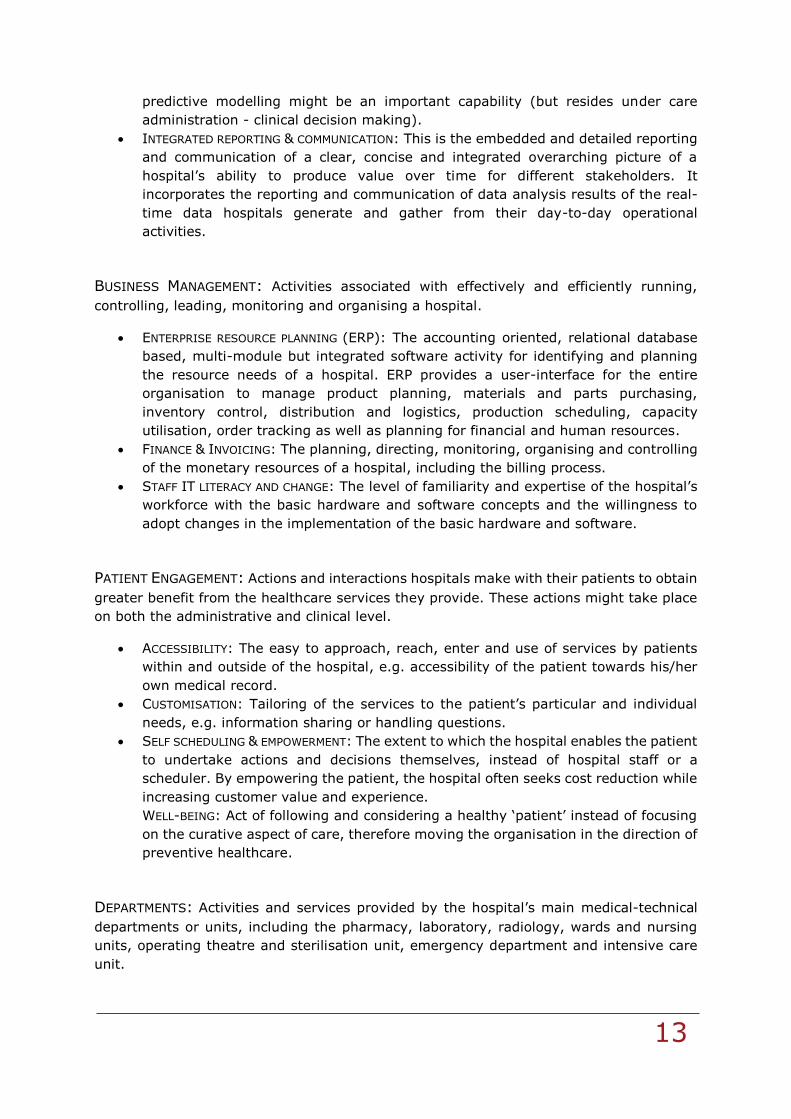
Case 3: large non-university hospital
The third case concerns a large (general) non-university hospital with multiple sites,
located in the Flanders region. Since the hospital resulted from a merger, it has already
set up projects to align the IT systems and work towards standardisation. In the near
future, following the recent changes towards network formations, the hospital aims to
install a shared EPR system with the hospitals participating in their network. The main
focus of this collaborative project is to further integrate patient information over all systems
both within and across hospitals and units. According to the hospital this is best enabled
through the implementation of the same package. A lack of interconnectedness and
standardisation (unequal technical capabilities) between IT systems, are brought forward
as one of the main reasons why the current legacy EPRs are not fit for purpose.
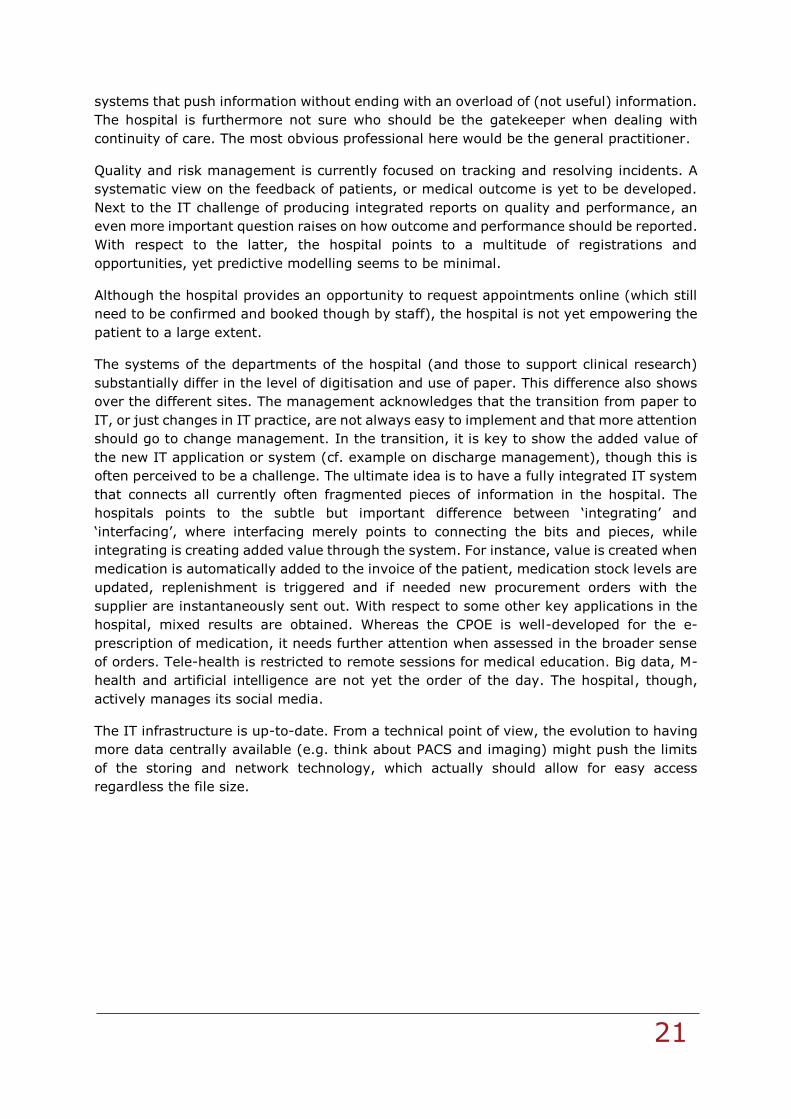
Figure 4: Capability heat map of Case 3
Overall, as indicated in Figure 4, digitisation and automation seem to be well-embedded in
this organisation. The internal care orchestration is digitally well-supported as the
admission, treatment and discharge of patients are planned through standard procedures
Our solution to your specific needs
23
from which is only deviated if the patient situation changes or the doctor in charge decides
to deviate from the standard pathway. Planning in terms of pathways helps to think ahead
and have a proactive policy that eases the transition of care.
One of the main deficiencies brought forward is the connection of the hospital IT and
systems with external stakeholders such as patients, elderly care institutions, general
practitioners or other hospitals. There is barely any communication or sharing of
information outside the boundaries of the hospital, mainly due to a lack of standards for
communicating data. After the discharge, there is no further electronic communication with
the patient, neither is the post-treatment health of patients being tracked. Apart from
being connected to hubs and ehealth, there is little to no automated exchange of
information.
Sufficient sources of information and data are currently present to support cure, care and
management. However, decision support systems exploiting this knowledge to support
clinical decision making are limited, except for the checks for interaction of multiple
medication for a patient. The registration of data is almost entirely paperless, though the
data is not always structured, which might impact the extent to which it can be used in
reports and visuals. The hospital actively uses platforms to support clinical research and is
piloting to see how datasets can be shared among institutions. Over the recent years, there
has been an increase of evaluation capturing systems to actively collect data in order to
control and manage the quality level of the hospital. The outcome-based assessment of
treatments, as prescribed to move towards value-based healthcare, is not yet in place.
Risk and performance management are well-established within the hospital organisation
to ensure patient safety and continuity of business. With respect to track and trace, the
hospital does not yet feature a closed loop medication process. All organisational reporting
is integrated and centralised in one online portal. Predictive modelling, both organisational
and clinical, is very limited to non-existent. Overall, many operations have become fully
automated and supported by IT over the years. The ERP covers the chain from procurement
over stock management to pay.
Clinical experts and physicians within the hospital take the initiative to recommend new IT
and systems to the hospital senior management on a proactive basis. Readiness for change
is therefore deemed present. With respect to the back-office, however, a more traditional
image appears and reluctance to change might be a challenge that calls for a well-
considered approach to increase the adoption of novel IT.
In terms of patient engagement, the hospital has not implemented anything beyond the
basic functionalities such as access to the wifi network. The accessibility of information
towards the patient and business partners is open for improvement, but pilots are running.
Towards the patient, e.g., the hospital is finding a way to install an online platform through
which patients can consult their information and communicate with the hospital. Also
customisation is currently under revision, for instance by means of a pilot examining how
patients can be targeted with precise information regarding their treatment by means of
multi-media. The hospital provides ekiosks for self registration on site, but no applications
are currently in place to foster self scheduling, although also on this topic a project is
running.
Although many departments work digitally and paperless, fragmentedness of IT systems
might still be present as they often have different IT systems (dedicated and some even
Our solution to your specific needs
24
self developed) based on their needs. Different sites might also have different systems,
such as the ICU. When implementing new IT systems, integration into the overall EPR and
hospital information system is set as a paramount criterion. The efforts of the hospital to
build towards a strong EPR result in an enhanced internal data integration. From the
external point of view, integration is directed towards governmental bodies, but can be
significantly improved w.r.t. general practitioners among other. The integration of devices
can be further improved, both internally (e.g. older equipment calls for transferring the
data manually into the IT system) and externally (e.g. integrating apps data of patients -
mobile health or tele-health to be further explored by the hospital but currently no
immediate focus).
The infrastructure is self-managed and considered advanced. Servers & storage are
deemed as state-of-the-art and backup-systems are in place and tested at a regular basis
with black-out exercises.
In sum, the hospital has made significant progress in the automation and digitisation of its
capabilities over the years. Following the strategy of the hospital, efforts will be aimed on
integrating and standardising all distinct applications & systems into a holistic, integrated
EPR, keeping in mind the upcoming transition toward a hospital network. Also, the hospital
aims to boost and empower patient engagement by setting up a “my-hospital” online
platform. Besides communicating and sharing information across the entire ‘care chain’,
enhancing clinical decision support is another key focus area of the hospital.
Case 4: medium-size non-university hospital
The fourth case is about a medium-size (general) non-university hospital operating from a
single site, located in the Flanders region. The hospital was the result from a merger and
a relocation of the facilities to a modern architectural building. Following the upgrade in
facilities, it seems that now the IT systems are generally open for improvement and
therefore will undergo major changes in the near future with the introduction of a new EPR.
While automation of the planning of activities is finding its way into the internal care
orchestration, with a well-developed admission and bed planning tool, it is brought forward
that information of the care process of the patient is still registered on paper moving along
with the patient, which isn’t helpful towards care transition management and internal care
orchestration. The communication of the hospital to external stakeholders remains limited
and unstructured. Since the medical record is connected to a hub, other hospitals can
access upon request information assuming there is a therapeutic relationship with the
patient who also confirmend the informed consent. With respect to nursing information, no
sharing is taking place. It happens that information is provided by exchanging CD-ROM
media or by phone. Communication and information sharing with non-hospital players
occurs via traditional media such as the ehealthbox, e.g. for exchanging secured letters
with the general practicioner. Other stakeholders, like home care agencies or elderly care
institutions apparently are not targeted within the external continuity of care
communication of the hospital.
Our solution to your specific needs
25
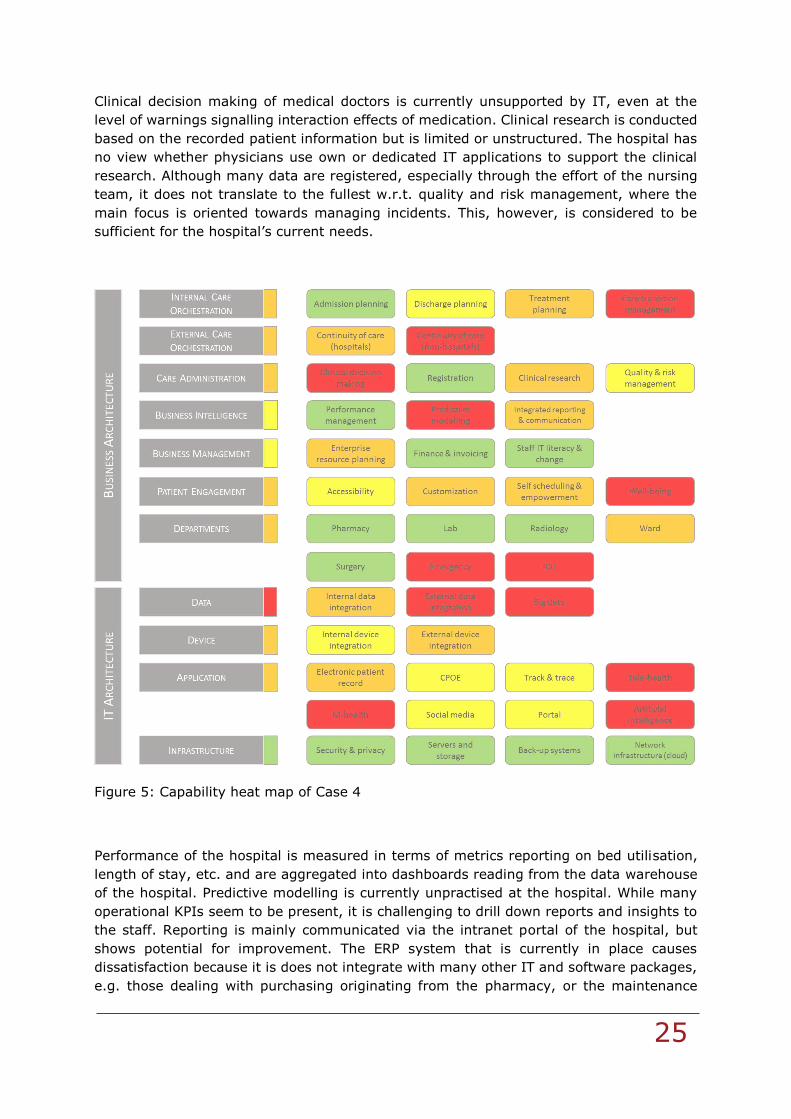
Clinical decision making of medical doctors is currently unsupported by IT, even at the
level of warnings signalling interaction effects of medication. Clinical research is conducted
based on the recorded patient information but is limited or unstructured. The hospital has
no view whether physicians use own or dedicated IT applications to support the clinical
research. Although many data are registered, especially through the effort of the nursing
team, it does not translate to the fullest w.r.t. quality and risk management, where the
main focus is oriented towards managing incidents. This, however, is considered to be
sufficient for the hospital’s current needs.
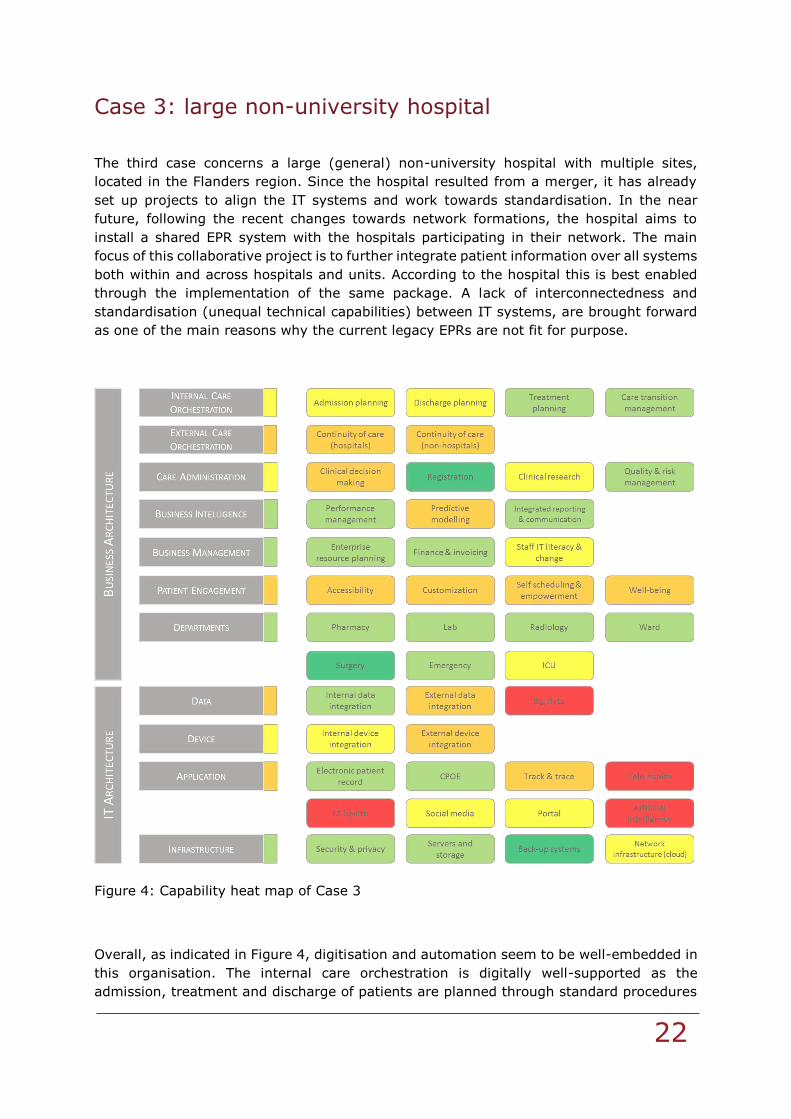
Figure 5: Capability heat map of Case 4
Performance of the hospital is measured in terms of metrics reporting on bed utilisation,
length of stay, etc. and are aggregated into dashboards reading from the data warehouse
of the hospital. Predictive modelling is currently unpractised at the hospital. While many
operational KPIs seem to be present, it is challenging to drill down reports and insights to
the staff. Reporting is mainly communicated via the intranet portal of the hospital, but
shows potential for improvement. The ERP system that is currently in place causes
dissatisfaction because it is does not integrate with many other IT and software packages,
e.g. those dealing with purchasing originating from the pharmacy, or the maintenance
Our solution to your specific needs
26
planning of medical equipment. Also the ERP system has not witnessed sufficient updates.
Financial management and invoicing are brought forward to proceed without any
irregularities. The hospital installs automated checks for irregularities in the invoices based
on listed medical activities. Staff and workforce are constantly being educated to manage
and adapt IT change through e-learning modules, multi-media applications and on-site
training. Also, the hospital strictly follows for every IT project a methodology for managing
the transition phase of IT renewal.
The accessibility of the IT systems by the patients is limited as well in so far that they can
only consult their own information through the hub. Customisation of services towards the
patient via IT applications is minimal, though an enriched website should allow patients
shortly to have a better view on the kind and structure of the invoice they can expect,
taking into account their particular treatment. No applications for self scheduling are
available, though it is mentioned that the hospital provides some kioks in which the
patients can assess by themselves some vital parameters.
Mixed results are seen for the IT support of the departments. For the wards, the medication
prescriptions are digital, though the nursing information is stated on paper. The operating
theatre is identified to be among the better IT supported departments, partly thanks to its
automated link with sterilisation services.
The internal data integration is expected to significantly improve with the introduction of
the new EPR. The hospital’s view on integration entails, e.g. for discharge, that the
immediate and automated update on the medication scheme or ambulatory visits is
mentioned in the discharge letter. In line with the findings on the continuity of care,
external data integration is poor. The hospital is following trends on big data, but currently
does not engage in any application. It is mentioned that apart from the technological side,
also staffing is a prerequisite to achieve results in this field, which is currently not matched
with the IT financing. With respect to device integration, the hospital states to be
theoretically ready for staff to bring their own device, or to connect apps, yet in practice
there seems limited to no request for these services.
The CPOE is part of the EPR and is open for improvement as it only targets medication
orders. Track and trace of patients is currently not in place, except for patients who have
the tendency to leave their designated location without permission and who are
consequently RFID-tagged. Also surgicial instrument sets follow a track and trace protocol.
The hospital does not have a fully closed medication loop, but is piloting within this regard.
Mobile health and tele-health initiatives are currently not on the map within the hospital,
except for participating in remote medical training sessions. The IT department, however,
closely follows these trends by attending information sessions as they believe in the future
impact. As mentioned, the hospital provides a portal which can be seen as a static rather
than collaborative tool. IT infrastructure is considered to be adequate and follows good
practice guidelines, including regular audits on safety and resilience, for which
improvement plans are continuously developed.
The main strategic project defined by the hospital is the adoption of the new electronic
patient record, which is expected to improve a number of problems and barriers that the
hospital wants to overcome such as the limited integration of current IT systems, the need
for consolidation of the ERP system, the empowerment of patients and the introduction of
standardardised information that can be communicated to other hospitals and non-hospital

Our solution to your specific needs
27
players. In essence, the major goals are to not only consolidate and integrate information
throughout the hospital, but also make useful use of the information that is captured to
further improve the care orchestration, both internally and externally. Next to and following
from the EPR renewal, a second aim is to move more toward an engaged and empowered
patient, who might be able to contribute more in the organisation of the healthcare process
and alleviate workload currently performed by hospital staff.

Our solution to your specific needs
28
From heat map to roadmap
From the introduction and case results, we can conclude that IT is often not aligned with,
or even fails to meet, the business expectations of the hospital. Yet, there is agreement
that IT should not be allowed to hinder the medical profession and the provision of care,
resulting in a set of actions impacting the state and usage of IT. In this context, one can
think of an IT roadmap as a plan to match the goals on business capabilities with
technological solutions, therefore describing the steps to be taken for a successful
transition. Often, a differentiation is made between the short term and the long term to
further pinpoint the actions in an appropriate time frame. However, there might be an
evolution over time in how roadmaps should be perceived and used. In the former days, a
roadmap was often seen as a more rigid plan that would connect the “as is” situation with
a “to be” sitation and would deliver a transition of the IT architecture to be followed in the
next, let’s say 10 years. Nowadays, we see that roadmaps are more and more restricted
in the time horizon they span, up to 3 years. Also, the all-encompassing rigid
transformation path has to move for a set of multiple paths based on scenarios so to allow
for flexibility, agility and resilience (cf. the ExConomy framework) and paths which should
be open to change and new opportunities that perhaps are yet to be discovered. In times
of uncertainty6, and for the hospital sector this easily translates to the many political and
legislative decisions that are still to be made in accordance with uncertain technological
evolutions, this makes sense. Furthermore, even though hospitals will act within a joint
and shared political and economical space, it might not be useful to define a generic, all
fitting, IT roadmap that would help them in making a structured transition to a next stage.
While some focal points might be shared among many hospitals, others will not and call
for different actions.
Without any doubt, the IT application project that is top of mind in the Belgian hospital
scene is centred around the EPR7. Either hospitals are dealing with the selection up to the
implementation of a (re)new(ed) EPR for their own institution, or a bit more advanced,
they start thinking about the selection and implementation of an EPR for the hospital
network in which they are about to participate. The huge focus on the EPR does not come
as a surprise, as this application is identified to be the main ‘connector’ or ‘integrator’ that
bridges many applications and capabilities. To have a better understanding, let’s take a
look at Figure 6. In this figure, we highlight the elements of the Business Architecture and
IT Architecture that will be directly impacted by and benefit from an enhanced EPR
functioning in the hospital. If we start from the Belgian Minimum Use Criteria (BMUC) to
scope the base expectations of an EPR towards the near future, we can retrieve and
position the 15 ‘core criteria’ (such as drug drug interaction, e-prescription medication,
automated communication with hubs and eHealth, discharge letters, etc.) under the gray-
scaled building blocks of the capability map. It clearly shows the integrative power of the
6 Cardoen B., Peeters C., Van Dyck W. and Schoonaert L. 2017. Impact of Uncertainty in Times of
Network Formation. Vlerick Business School, HMC White Paper. This white paper can be retrieved from www.vlerick.com/healthcare
7 For some recent examples of hospitals announcing or reporting on the implementation of a new
EPR, see, e.g., UZA (https://www.uza.be/uza-legt-de-fundamenten-voor-een-virtueel-ziekenhuis), AZ Delta (http://www.actualcare.be/nl/nl-management/nl-management-ict/az-delta-kijkt-uit-naar-geintegreerd-epd/), UZ Gent (http://www.zorganderstv.be/nieuws/uz-gent-bouwt-aan-een-nieuw-
toekomstgericht-elektronisch-pati%C3%ABntendossier)
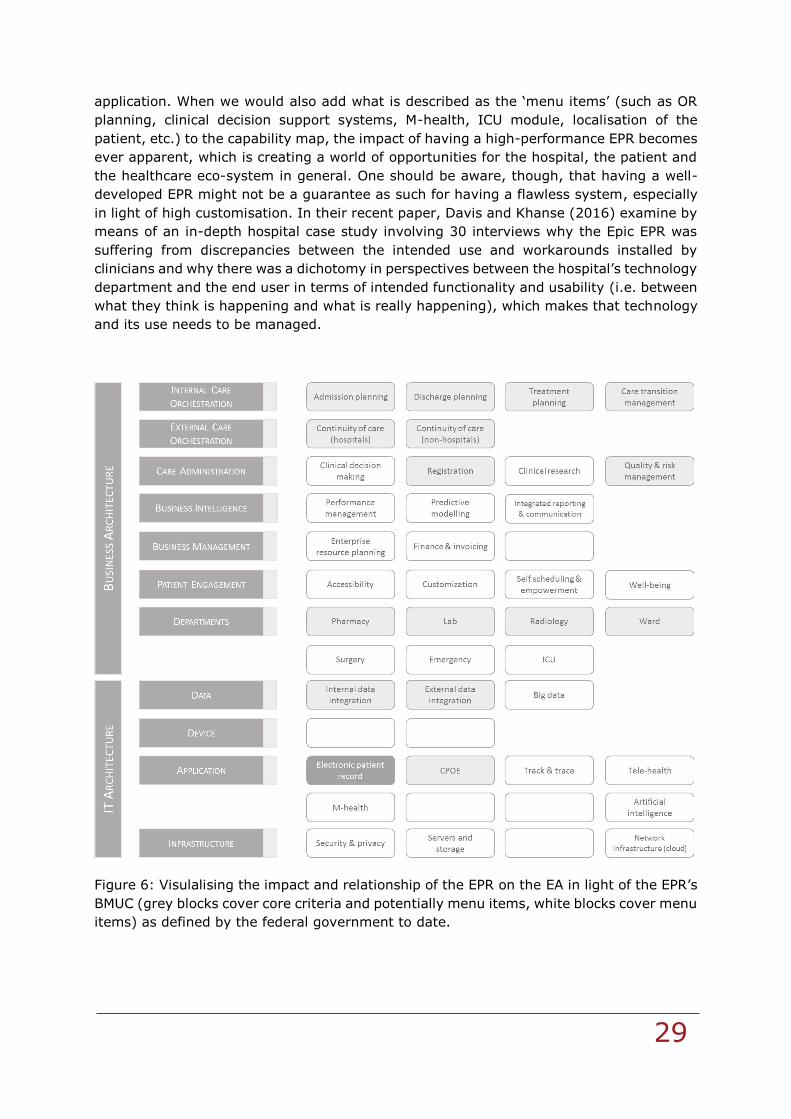
Our solution to your specific needs
29
application. When we would also add what is described as the ‘menu items’ (such as OR
planning, clinical decision support systems, M-health, ICU module, localisation of the
patient, etc.) to the capability map, the impact of having a high-performance EPR becomes
ever apparent, which is creating a world of opportunities for the hospital, the patient and
the healthcare eco-system in general. One should be aware, though, that having a well-
developed EPR might not be a guarantee as such for having a flawless system, especially
in light of high customisation. In their recent paper, Davis and Khanse (2016) examine by
means of an in-depth hospital case study involving 30 interviews why the Epic EPR was
suffering from discrepancies between the intended use and workarounds installed by
clinicians and why there was a dichotomy in perspectives between the hospital’s technology
department and the end user in terms of intended functionality and usability (i.e. between
what they think is happening and what is really happening), which makes that technology
and its use needs to be managed.
Figure 6: Visulalising the impact and relationship of the EPR on the EA in light of the EPR’s
BMUC (grey blocks cover core criteria and potentially menu items, white blocks cover menu
items) as defined by the federal government to date.
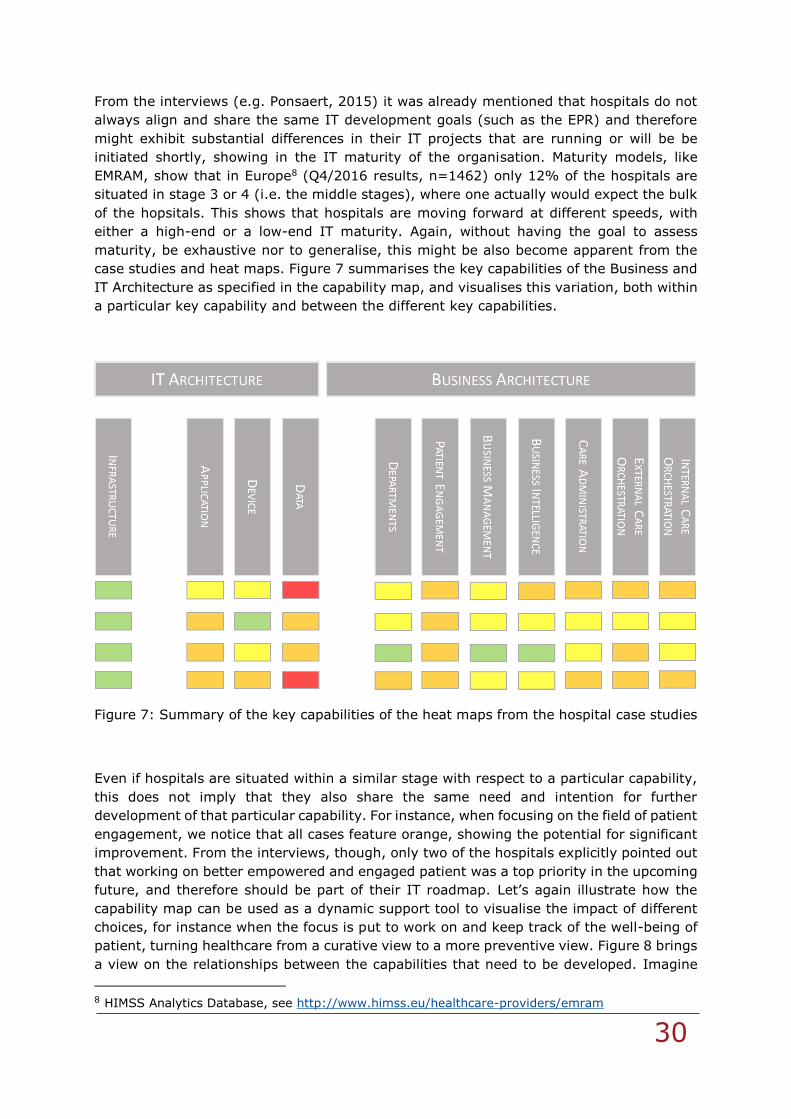
Our solution to your specific needs
30
From the interviews (e.g. Ponsaert, 2015) it was already mentioned that hospitals do not
always align and share the same IT development goals (such as the EPR) and therefore
might exhibit substantial differences in their IT projects that are running or will be be
initiated shortly, showing in the IT maturity of the organisation. Maturity models, like
EMRAM, show that in Europe8 (Q4/2016 results, n=1462) only 12% of the hospitals are
situated in stage 3 or 4 (i.e. the middle stages), where one actually would expect the bulk
of the hopsitals. This shows that hospitals are moving forward at different speeds, with
either a high-end or a low-end IT maturity. Again, without having the goal to assess
maturity, be exhaustive nor to generalise, this might be also become apparent from the
case studies and heat maps. Figure 7 summarises the key capabilities of the Business and
IT Architecture as specified in the capability map, and visualises this variation, both within
a particular key capability and between the different key capabilities.
Figure 7: Summary of the key capabilities of the heat maps from the hospital case studies
Even if hospitals are situated within a similar stage with respect to a particular capability,
this does not imply that they also share the same need and intention for further
development of that particular capability. For instance, when focusing on the field of patient
engagement, we notice that all cases feature orange, showing the potential for significant
improvement. From the interviews, though, only two of the hospitals explicitly pointed out
that working on better empowered and engaged patient was a top priority in the upcoming
future, and therefore should be part of their IT roadmap. Let’s again illustrate how the
capability map can be used as a dynamic support tool to visualise the impact of different
choices, for instance when the focus is put to work on and keep track of the well-being of
patient, turning healthcare from a curative view to a more preventive view. Figure 8 brings
a view on the relationships between the capabilities that need to be developed. Imagine
8 HIMSS Analytics Database, see http://www.himss.eu/healthcare-providers/emram
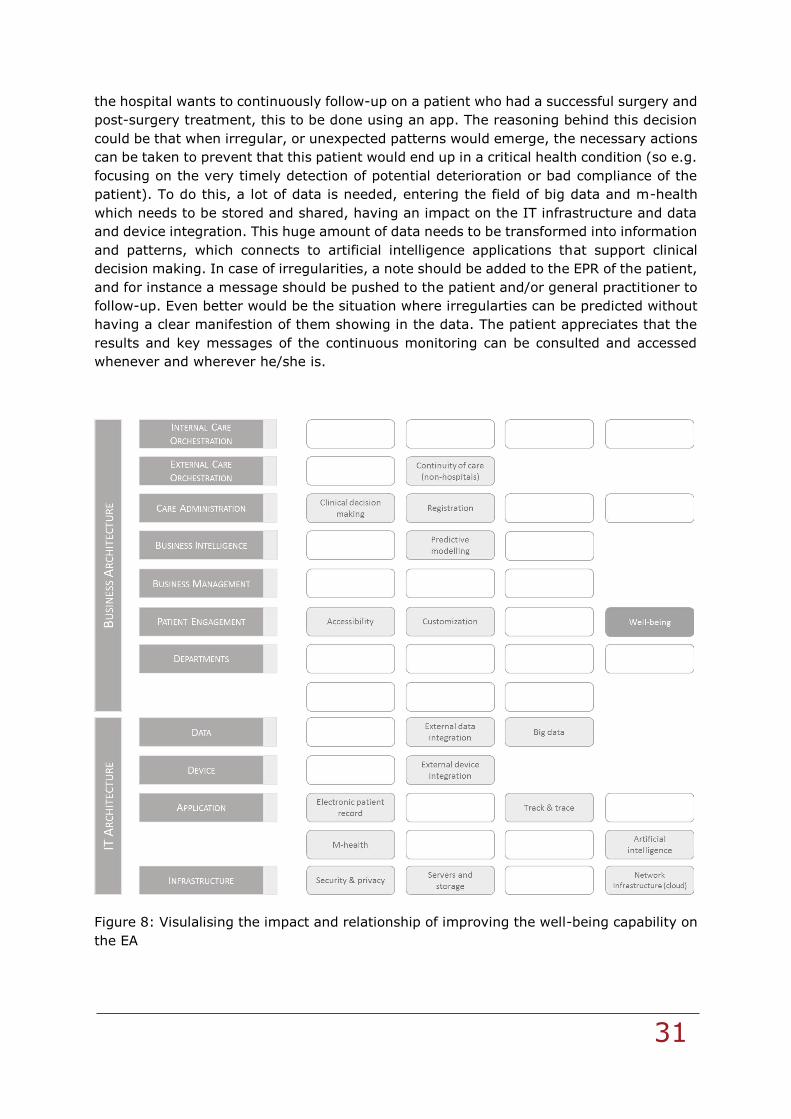
Our solution to your specific needs
31
the hospital wants to continuously follow-up on a patient who had a successful surgery and
post-surgery treatment, this to be done using an app. The reasoning behind this decision
could be that when irregular, or unexpected patterns would emerge, the necessary actions
can be taken to prevent that this patient would end up in a critical health condition (so e.g.
focusing on the very timely detection of potential deterioration or bad compliance of the
patient). To do this, a lot of data is needed, entering the field of big data and m-health
which needs to be stored and shared, having an impact on the IT infrastructure and data
and device integration. This huge amount of data needs to be transformed into information
and patterns, which connects to artificial intelligence applications that support clinical
decision making. In case of irregularities, a note should be added to the EPR of the patient,
and for instance a message should be pushed to the patient and/or general practitioner to
follow-up. Even better would be the situation where irregularties can be predicted without
having a clear manifestion of them showing in the data. The patient appreciates that the
results and key messages of the continuous monitoring can be consulted and accessed
whenever and wherever he/she is.
Figure 8: Visulalising the impact and relationship of improving the well-being capability on
the EA
Our solution to your specific needs
32
Conclusion and next steps
With the development of a pragmatic capability map, we hope to support hospitals in the
development of their IT strategy and the according choices to be made to evolve to a future
digital-proof state. The model should help to dynamically assess how capabilities relate to
one another and how aspired changes to one capability might also require effort on
different dimensions.
We acknowledge that the capability map leaves room for interpretation and is not
exhaustive in listing all capabilities. Also, the capability map is not to be confused with an
IT maturity model, nor with a detailed IT roadmap. Next steps for the hospitals therefore
consist of making a detailed and by definition also technically oriented plan of action to
build the prioritised capabilities, including a well-fitted time horizon and project plan, which
all together will constitute the IT roadmap. In this regard, we want to remind the reader
that the era of a rigid roadmap with long term projections seems to be outdated and
replaced by much more agile, flexible and short-term roadmaps, showing readiness to
adapt to rather unexpected evolutions and change.
Our solution to your specific needs
33
Bibliography
Bolle B. (2015, November 30). Executive manager of CIN-NIC. (M. Boënne & B. Cardoen,
Interviewers)
Bright House Networks. (2014). Meeting the Bandwidth Challenges of a Digital Healthcare
Environment. Syracuse: Bright House Networks.
Cardoen B., Peeters C., Van Dyck W. and Schoonaert L. (2017). Impact of Uncertainty in
Times of Network Formation. Vlerick Business School, HMC White Paper
Chilukuri S. and Van Kuiken S. (2017). Four Keys to Succesful Digital Transformations in
Healthcare. McKinsey & Company, Digital McKinsey (April)
Cumps B., Viaene S., Dussart P. and Vanden Brande J. (2013). Towards Enterprise
Architecture Infused Organisations. Journal of Enterprise Architecture, 9 (2), 8-18
Carvalho J.V., Rocha A. and Vasconcelos J. (2015). Maturity Models for Hospital
Information Systems Management: Are They Mature? DOI: 10.1007/978-3-319-
23024-5_49
CGI. (2014). Healthcare Challenges and Trends: The Patient at the Heart of Care.
Whitepaper. Montreal: CGI Group Inc.
Davis Z. and Khansa L. (2016). Evaluating the Epic Electronic Medical Record System: A
Dichotomy in Perspectives and Solution Recommendations. Health Policy and
Technology, 5, 65-73.
De Ridder R. (2015, December 2). Director General of NIHDI/RIZIV/INAMI. (M. Boënne &
B. Cardoen, Interviewers)
Deloitte Centre for Health Solutions. (2015). 2014 Global Health Care Outlook: Shared
challenges, shared opportunities. London: Deloitte.
Deloitte Centre for Health Solutions. (2015). Connected Health: How digital technology is
transforming health and social care. London: Deloitte.
Deloitte Centre for Health Solutions. (2015). Digital Health in the UK: An industry for the
Office of Life Sciences. London: Deloitte.
Deloitte Centre for Health Solutions. (2015). Healthcare and Life Sciences Predictions
2020: A bold future? London: Deloitte.
DISCIPULUS Project. (2013). Roadmap for the Digital Patient. Brussels: European
Commission.
European Parliament. (1998). Health Care Systems in the EU: A Comparative Study.
Brussels: EU Union.
Grossman J. (2008). Disruptive Innovation in Healthcare: Challenges for Engineering. The
Bridge, 10-16.
Groves P., Kayyali B., Knott D. and Van Kuiken S. (2013). The 'Big Data' Revolution in
Healthcare. McKinsey & Company.
Heijlen R. (2015, December 16). Flemish Patients' Platform. (M. Boënne & B. Cardoen,
Interviewers)
Our solution to your specific needs
34
IBM Global Business Services. (2013). The digital hospital evolution: Creating a framework
for the healthcare system of the future. New York: IBM.
Kierkegaard P. (2011). Electronic Health Record: Wiring Europe's Healthcare. Computer
Law & Security Review, 27 (5), 503-515.
Kierkegaard P. (2013). eHealth in Denmark: A Case Study. New York: Springer Science.
Kierkegaard P. (2013). E-Prescription across Europe. Health and Technology,3 (3), 205-
219.
Leichner D. (2014). Global Health IT Trends and Forecast. Israel: Gartner Inc.
McKinsey & Company. (2014). Applying lean IT to healthcare. New York: Business
Technology Office.
McKinsey & Company. (2015). The road to digital success in pharma. New York: McKinsey.
Mettler T., Fitterer R., Rohner P. and Winter R. (2014). Does a hospital's IT architecture fit
with its strategy? An approach to measure the alignment of health information
technology. Health Systems, 3 (1), 29-42.
Moens, M. (2015, November 17). Belgian Association for Doctors' Syndicate. (M. Boënne,
& B. Cardoen, Interviewers)
OECD & European Commission. (2015). Health at a Glance: Europe 2014. Brussel:
European Commission.
Olsen J. and Baisch M. (2014). An integrative review of information systems and
terminologies used in local health departments. JMIR Medical Informatics, 21, 20-
27.
ONC Office of the Secretary, U.S. Departement of Health and Human Services. (2014).
Report to Congress on Health IT Adoption and HIE. Washington D.C.: ONC.
Ponsaert F. (2015, November 24). Advisor of the Minister of Social Affairs and Public
Health. (M. Boënne & B. Cardoen, Interviewers)
Porter M. and Lee T. (2013). The Strategy That Will Fix Health Care. Harvard Business
Review, 10, 50-70.
PwC Health Research Institute. (2013). Putting data security on the top table: How
healthcare organisations can manage information more safely. London: PwC.
PwC Health Research Institute. (2013). Solving the talent equation for health IT. London:
PwC.
PwC Health Research Institute. (2014). Top health industry issues of 2015: Outlines of a
market emerge. London: PwC.
PwC Health Research Institute. (2015). 21st Century Pharmaceutical Collaboration.
London: PwC.
PwC Health Research Institute. (2015). Healthcare cybersecurity challenges in an
interconnected world: Key findings from the Global State of Information Security
Survey. London: PwC.
Our solution to your specific needs
35
PwC Health Research Institute. (2015). Medical Cost Trend: Behind the Numbers 2016.
London: PwC.
Robben F. (2015, December 1). Administrator General of the e-health program of the
Belgian Federal Government. (M. Boënne & B. Cardoen, Interviewers)
Ross J., Weill P. and Robertson D. (2006). Entreprise Architecture Strategy. Boston,
Massachusettes: Harvard Business School Press.
Tamm T., Seddon P., Shanks G. and Reynolds P. (2011). How does Entreprise Architecture
Add Value to Organisations? Communication of the Association for Information
Systems, 28, Article 10.
Technology, T. O. (2102). Behavioral Health Roundtable: Summary Report of Findings.
Washington DC: ONC.
The Office of the National Coordinator for Health Information Technology (ONC). (2013).
Lessons from the Literature on Electronic Health Record Implementation.
Washington DC: ONC.
The Office of the National Coordinator for Health Information Technology (ONC). (2014).
Demonstrating the Effectiveness of Patient Feedback in Improving the Accuracy of
Medical Records. Washington DC: ONC.
Tooke J. (2015). Future of Healthcare in Europe. London: UCL School of Life & Medical
Sciences.
Vanaudenaerde D. (2015, November 27). Centre Manager Red Cross. (M. Boënne & B.
Cardoen, Interviewers)
Verlinde C., Van Ackere R. and Vanslambrouck, W. (2015, December 1). Ministry for
Welfare, Public Health and Family of Flemish region, Adjunct Deputy Head, Advisor,
Staff Administrator General. (M. Boënne & B. Cardoen, Interviewers)
Viaene S. and Danneels L. (2015). Driving digital: Welcome to the ExConomy. Business
Technology Strategies - Executive Update, Cutter Consortium and Vlerick Business
School, 5p.
Volksvertegenwoordigers, B. K. (2014). Algemene Beleidsnota Gezondheidszorg. Brussel:
Kamer van de 54e Zittingsperiode.
Wager K., Lee F. and Glaser J. (2013). Health Care Information Systems. Jossey-Bass.
Weil T. (2000). Health Networks: Can they be the solution? Tampa, Florida: The University
of the Michigan Press.

Our solution to your specific needs
36