Towards a National eHealth/Telehealth Strategy for Pakistan › lead › Publications › DP 29-...
30
Towards a National eHealth/Telehealth Strategy for Pakistan: Experiences, Challenges and Opportunities Abdul Muqeet, Hammad Durrani
Transcript of Towards a National eHealth/Telehealth Strategy for Pakistan › lead › Publications › DP 29-...
Towards a National eHealth/Telehealth Strategy for Pakistan:Experiences, Challenges and Opportunities
Abdul Muqeet, Hammad Durrani

About the AuthorsMr. Abdul Muqeet works as Assistant Manager eHealth Technologies for Aga Khan Development Network eHealth Resource Centre at the Aga Khan University (AKU). He is a Biomedical Engineer with extensive background and interest in use of eHealth technologies to facilitate healthcare services and education. His research interest focuses on application of different technologies in healthcare settings and the evidence based implementation of eHealth programs in developing countries. Mr. Muqeet has contributed extensively to eHealth research, especially in medical image compression, PACS, Electronic Health Records, mobile health and telehealth for healthcare institutions globally.
Dr. Hammad Durrani is a medical doctor with a Masters in Health Policy and Health Management. Being a strong advocate of integrating eHealth with routine health care, he is currently working as a Manager Research in PANACeA (PAN Asian Collaboration for Evidence-based eHealth Adoption and Application) at the Aga Khan University in Karachi, Pakistan. In this capacity, he is mentoring two eHealth Projects, which are being carried out in the Philippines, Indonesia, Bangladesh, India and Pakistan. He is also involved in conducting systematic reviews on different eHealth modalities, currently working on Health Informatics evidence available in Asia.
Dr. Durrani is also a member of the eHealth Taskforce for the Aga Khan Development Network, with responsibilities of planning and strategizing eHealth applications and its concepts in over 20 countries in Asia and Africa. He is also one of the founding members of the eHealth Association of Pakistan.
Table of ContentsD
ecem
ber 2
012
Executive Summary 02Delineation of Terms and Structure of the Document 03Chapter 1 05Understanding eHealth and its Benefits 05Experiences of Telehealth/eHealth in Pakistan 05Chapter 2 08eHealth Policy Development Needs 09Chapter 3 11Challenges in eHealth/Telehealth Planning and Implementation for Pakistan 11Chapter 4 17The Way Forward 17Annexure 19Bibliography 22

LEAD PakistanDiscussion Paper Series
Towards a National eHealth/Telehealth Strategy for Pakistan:Experiences, Challenges and Opportunities
Foreword
LEAD Pakistan, in collaboration with the Lucile & David Packard Foundation, has launched “Our World – Women
Leadership in Reproductive Health& Development”, a project that aims to sensitize a cross-sectoral network of
leaders and motivate them to raise the profile of reproductive health in the social development sector through
public policy engagement and media. As part of the project process background papers have been produced.
This paper describes a need to develop a strategic approach to Telehealth in particular and eHealth in general in
Pakistan, given its potential role and importance in the provision of quality services that equitably improve health
outcomes, respond to peoples' legitimate demands, throughout the Pakistan.
The role of Information and Communication Technology (ICT) can no longer be ignored in any development sector,
including healthcare settings. Introduction of ICT in healthcare, referred to as eHealth, has offered several new
dimensions to improve access and quality of care. eHealth has been an increasingly successful strategy in filling
the gap of access and quality in healthcare system. Through outreach in remote areas, eHealth can play a major
role in solving maternal child health issues in the rural population.
Though the health indicators of Pakistan have improved in the last two decades, this rate of improvement is
relatively slower than the neighboring countries. The use of technology in the health sector of Pakistan, like other
developing countries, is in its early phase. Within this national context, eHealth is project-based, featuring a few
small initiatives that are seldom connected to each other. As a result, they do not achieve sustainability being
donor funded for a limited time period.
Where eHealth is a new technology, there is an inevitable resistance in accepting it in normal practice and
integrating it within the current Pakistani health system. Through this paper LEAD attempts to highlight a number
of challenges for incorporating eHealth in Pakistan's health system. As a way forward, the need for a national
eHealth policy and strategy has been identified. Establishing the main directions, as well as planning the detailed
steps in eHealth strategy formation, is key to achieving longer-term goals such as health sector efficiency, reform
or more fundamental transformation.
Ali. T. Sheikh
CEO, LEAD Pakistan
01

Executive SummaryeHealth (use of information technology in healthcare) has been an increasingly successful strategy in filling the
gap of access and quality in healthcare system. Through outreach in remote areas, eHealth can play a major role
in solving maternal child health issues in the rural population.
Though the health indicators of Pakistan's have improved in the last two decades, but this rate of improvement is
relatively slower than the neighboring countries. Pakistan's mortality for under-five remains the highest among
the South Asian (SA) countries. High maternal mortality (deaths) combined with high fertility (birth) results in
ratio of 1:89 women dying from pregnancy related causes. In addition, increasing burden of non-communicable
diseases now compounds persisting burden of infectious diseases.
The use of technology in the health sector of Pakistan, like other developing countries, is in its early phase. Most of
the eHealth services so far, have been tested as pilot projects. As a result, they did not achieve sustainability
being donor funded for a limited time period. However, some successful examples of eHealth implementation
have been seen in Pakistan coming from the Holy Family Hospital, the Mayo Hospital and the Aga Khan University
Hospital. More research-based evidence is needed to convince the academics, managers or policy-makers to
make eHealth an integral part of the health system.
To make eHealth a part and parcel of Pakistan's health system, multiple policy issues need to be addressed.
Learning examples on successful eHealth policy formation are available from sources such as the European
Union, Commonwealth eHealth priorities and some country level policies from Malaysia, India and Kenya. The
common points in all successful policies have been identifying regional priorities and challenges, adaptive
strategic partnerships, reaching consensus on local projects and promote information and expertise exchange.
Where eHealth is a new technology, there is an inevitable resistance in accepting it in normal practice and
integrating it within the current Pakistani health system. For incorporating eHealth in Pakistan's health system,
nine challenges have been discussed in this paper such as social & cultural issues, technology, ethical issues,
change management, sustainability, monitoring & evaluation, devolution and integration.
As a way forward, the need for a national eHealth policy and strategy has been identified. Establishing the main
directions, as well as planning the detailed steps in eHealth strategy formation, is key to achieving longer-term
goals such as health sector efficiency, reform or more fundamental transformation.
In this document eHealth follows the WHO definition of eHealth as the cost-effective and secure use of
information and communications technologies (ICT) in support of health and health-related fields, including
health-care services, health surveillance, health literature, and health education, knowledge and research [1, 2,
3]. eHealth is at the intersection of medical informatics, public health and business, and in a broader sense, the
term characterizes not only a technical development, but also a state-of-mind, a way of thinking, an attitude, and
a commitment for networked, global thinking, to improve health care locally, regionally, and worldwide by using
information and communication technology [4]. The applications of eHealth are grouped under the following
02
Dec
embe
r 201
2

03
categories:
Telehealth: Telehealth (or Telemedicine) refers to the use of ICT in provision of health services at a distance. This
includes teleconsultations in live or store-and-forward mode [5].
Health Informatics: Health Informatics refers to management of clinical and administrative information through
ICT. Some examples include Electronic Health Record (EHRs), Picture Archival and Communication Systems
(PACS), Health Management Information Systems (HMIS), and e-Surveillance [6].
eLearning: eLearning refers to education of healthcare providers and communities facilitated through the use of
ICT [7].
mHealth: Mobile eHealth (or mHealth) has emerged as an important segment of eHealth, and involves using
wireless technologies to transmit and enable various eHealth data contents and services. It broadly
encompasses the use of mobile telecommunication and multimedia technologies (such as Bluetooth,
GSM/GPRS/3G, WiFi, WiMAX, and so on) as they are integrated within increasingly mobile and wireless health
care delivery systems and is part of a movement towards citizen-centered health service delivery. Mobile
technologies by nature lend themselves to more decentralized health service delivery. Usually these are accessed
by the health worker through devices such as mobile phones, smart phones, PDAs, and laptops [8].
NOTE: The term mHealth is sometimes incorrectly applied to the use of vehicles (equipped with telehealth
capability) which are 'mobile' in the sense of being physically driven from one location to another.
Purpose of the document: This current document describes a need to develop a strategic approach to Telehealth
(in particular and eHealth in general in Pakistan), given its potential role and importance in the provision of
quality services that equitably improve health outcomes, respond to peoples' legitimate demands, throughout
the Pakistan. The document provides a direction for the many actions being undertaken throughout the Pakistan
and, it is hoped, will unify such efforts into a cohesive whole that meets the individual and collective aspirations of
the provinces, agencies and institutions working on Telehealth/eHealth in Pakistan. It is also important to have
an eye on the broader eHealth development that does not diminish the effort by narrowly focusing on Telehealth or
Telemedicine.
Outline of the document: This document outlines the current status of Telehealth/eHealth development in
Pakistan, how it provides an alternative approach for healthcare delivery, opportunities and challenges for
Telehealth/eHealth development in Pakistan, concluded by an implementation plan (the way forward).
The role of Information and Communication Technology (ICT) can no longer be ignored in any development sector,
including healthcare settings. Introduction of ICT in healthcare (hereby referred to as eHealth) has offered several
new dimensions to improve access and quality of care. eHealth with its different dimensions (telehealth, mobile-
Health and health informatics), [9] offers ways to improve access and quality of care, with direct benefits not only
Understanding eHealth and its Benefits
Delineation of Terms and Structure of the Document
LEAD PakistanDiscussion Paper Series
Towards a National eHealth/Telehealth Strategy for Pakistan:Experiences, Challenges and Opportunities

to the communities and patients in need, but also to the healthcare providers working in different levels of the
health system [10]. These benefits could be in the form of supporting remote providers in provision of healthcare
to the patients, improving knowledge of healthcare providers, and management of information for accelerated
decision-making.
eHealth interventions represent a strategy for potentially addressing problems with access to and quality of
Dec
embe
r 201
2
04

health care through telehealth. eHealth can play a been noticeable improvement in some health
major role and an alternate model in provision of indicators over the years, on the whole, considerable
essential services to remote areas, such as improvement is needed. Overall, life expectancy in
specialized maternal and child health (MNCH) to Pakistan remains lower than many in its peer group,
support basic services in the communities, while infant as well as maternal mortality rates are
availability of clinical and administrative data to amongst the highest in the region (63 per 1000 births
enable the planners to take timely and appropriate and 260 out of 100,000 mothers).
decisions, access to the specialists for emergency (MDGs) has been
and difficult cases [11]. eHealth (through m-Health) slow, particularly against MDG 2 on primary
can also play a crucial role in Behavioral Change education, MDG 4 on child mortality, and MDG 5 on
Intervention (BCI) through implementation of an maternal health. Poor access for disadvantaged
i n t e g r a t e d I n f o r m a t i o n , E d u c a t i o n a n d groups and poor quality of care are issues
Communications (IEC) strategy in promoting MNCH undermining the delivery of effective health services
services like safe motherhood and family planning [16].
programs. BCI and advocacy aims to promote Pakistan health system follows the pattern of a knowledge, attitude, and behavior to its typical health system of a developing country. beneficiaries to increase demand for and use of Suffering a huge burden of diseases, inadequate MNCH services [12]. It also aims to increase popular health infrastructure and equipment, and silos of understanding of the barriers and risks to safe care resulting in duplication of efforts (vertical and motherhood and communicate desired behavior, horizontal healthcare system augmented by post and to reduce stigma and exclusion of disadvantage 18th amendment scenario; improving the health and risk groups [13]. system requires a fundamental change in approach
to the way health care is delivered in this country.
Role of eHealth in improving the quality of
information and its management has also been The Pakistan health system is also straining to deal proven globally. Lack of timely and reliable data is with increasing cost and demand pressures and a often cited as a serious impediment to successful shortage of skilled health care workers. Given this delivery of health services [14]. eHealth provides a reality, there is a need to move to a system where platform for electronic management of health every interaction between consumers and care management information systems (HMIS) to providers achieves maximum impact on health improve efficiency and effectiveness of health outcomes and where scarce financial and human system. An effective HMIS system at the district level resources are deployed as effectively as possible. will carry both epidemiological information This change will require a fundamental shift in the (prevalence, incidence, mortality, and morbidity way information is accessed and shared across the statistics) and administrative information (resource health system. eHealth offers a process of closing inputs and service utilization) [6]. the above gaps by harnessing Inforamtion and
Communication Technology for improved healthcare
delivery in addition to other ongoing efforts.
The technology use in the health sector of Pakistan,
like other developing countries is in its infancy. Pakistan is the world's sixth most-populous country, Pakistan started with eHealth pilot projects and behind Brazil and ahead of Bangladesh with a programs, much like the eHealth development and population of 173,593,00.[15]. While there has
Progress against
the Millenium Development Goals
Comparison of Experiences of Telehealth/eHealth in
Pakistan
Chapter 1
05
1. In 2000, 189 nations made a promise to free people from extreme poverty and multiple deprivations including Health. This pledge turned into the eight Millennium Development Goals.(http://www.undp.org/content/undp/en/home/mdgoverview.html)
1
LEAD PakistanDiscussion Paper Series
Towards a National eHealth/Telehealth Strategy for Pakistan:Experiences, Challenges and Opportunities

progress in other countries; supported mostly by the this activity has performed 7980 + clinics. The
international donors. Although the projects were program has reached rural population in Attock,
successful in demonstrating relevance and Pindigheb, Khushab, DG Khan, R Y Khan, Mithan
application of the technology and proved success of Kot, Jhang, Rajanpur and Gujrat [18].
eHealth solutions in the local environment, these æ Telemedicine project by Electronic Government were not designed to produce research evidence to Directorate (E.G.D) Pakistan: The project of convince the academics, managers or policy-makers Telemedicine was launched in Pakistan by to support eHealth. Moreover, no serious efforts have Electronic Government Directorate (E.G.D) the been made, from the government side to harness the Ministr y of Information and Technology, use of technology in healthcare. The main Islamabad, Pakistan in 2007. The project was developments in eHealth came from the private started in 3 hospitals, i.e. Mayo Hospital, Holy sector and autonomous organizations working in Family Hospital Rawalpindi and Jinnah Post public sector. Organizations like COMSATS institute Graduate Medical Center. It is now operational in Islamabad, Gambat Institute of Medical Sciences, 2 out of 3 hubs, i.e. Mayo Hospital and the Holy Aga Khan University Hospital Karachi, Holy Family Family Hospital. The JPMC Hub is not functional Hospital Rawalpindi, Jinnah Post Graduate Medical due to funds exhaustion. The EGD project at Mayo Center Karachi and Mayo Hospital Lahore came Hospital, Lahore is providing Tele-consultations forward with successful pilot projects, particularly in to the District Headquarter Hospitals of Gujrat, telehealth and telemedicine [17]. Rajanpur, Jhang and Dera Ghazi Khan [19].
æ eHealth activities at Aga Khan University: In 2009
In terms of health informatics, no serious or Aga Khan Health Ser vices Pakistan in
concerted efforts from the public sector have been coordination with Aga Khan Development
seen. The reasons for this rest on the gaps on how Network (AKDN) eHealth Resource Center, Aga
health information is generated, processed, saved Khan University started Teleconsultation link
and used. In Pakistan information is being generated between different levels of health centers for
at two levels, i.e. at vertical and horizontal levels, with patient management, triage and referral of cases.
minimum connections between the two. After Programs were implemented in Gilgit Baltistan
devolution and 18th amendment the fragmentation connecting Gilgit Medical Center to three
has only increased. Currently, some provinces are secondary care and primary health care facilities
working on District Health Information Systems of Hunza and Ghizer districts [20].
(DHIS) implementation, while at the tertiary care æ Aman Telehealth Call Centre: Aman Health has level, there are only a few hospitals whch are using 24/7 health call center providing high quality electronic medical records or have automated their health information, health guidance, and referral hospital information systems. There are few for the urgent, acute or chronic health problems to examples where hospitals have developed in-house unreached population [21].EMR softwares like Pakistan institute of Medical
Sciences, Aga Khan University Hospital, Shaukat
Khanum Memorial hospital and the Indus Hospital
Karachi. Despite the growing attention, investments and
potential for using eHealth, limited understanding
exists in Pakistan of how Telehealth/eHealth-based æ
applications, services and systems are designed, Hospital initiated telehealth program from 2008
implemented and used. The process of planning and till date under the National Rural Support
implementing Telehealth/eHealth requires an in-program (NRSP) and with support of the
depth understanding of the needs of the health Electronic Government Directorate (E.G.D)
system and all its stakeholders, and their role in the Pakistan. Under NRSP, specialist medical clinics
changing healthcare environment. Experience from such as cardiology, surgery, gynecology, peads,
the developed world has shown several impediments neurology and urology were initiated and till now
Telehealth at Holy Family Hospital: Holy family
eHealth Policy Development Needs:
Dec
embe
r 201
2
06
for eHealth policy development, including lack of WHA58.28 urging member states to consider
information about the role of Telehealth/eHealth developing long-term strategic plans for
in provision of health care, well-defined developing and implementing eHealth services.
operational and support policies, demonstration The World Health Organization (WHO) and its
of cost and benefit, and identification of clinical Global Observatory for eHealth (GOe) support
proponents [22]. This kind of insight suggests the these goals by providing member states with
n e e d f o r d e v e l o p m e n t o f a s o u n d strategic information and guidance on effective
Telehealth/eHealth strategy to guide the planning eHealth practices, policies, and standards [25].
process for Telehealth/eHealth initiatives [23, In the passage below, the authors have attempted 24]. Technologically appropriate and culturally to determine how many countries have eHealth sensitive Telehealth/eHealth solutions need to be policies, strategy or roadmaps. Data from the WHO identified, aligned, and prioritized in a manner that Global Observatory for eHealth Report (WHO GOe maximizes the efficiency and effectiveness of Report) provides the starting point. The report services in any given setting. presents data on several aspects of national
policy, including information policy, ePolicy, and
eHealth policy. The report emphasizes the premise Recent years have seen global and regional that “the most favorable approach to the entities stepping into the eHealth policy arena. Timplementation of eHealth at the national level is adopted Resolution
he
World Health Assembly (WHA)
07
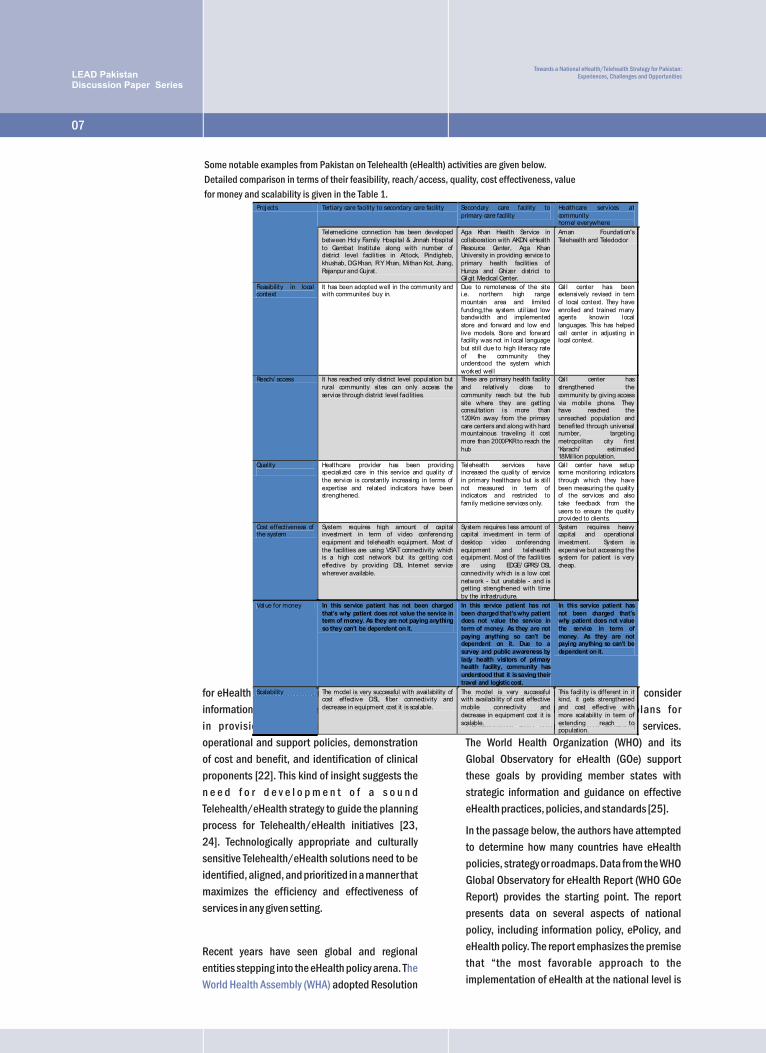
Some notable examples from Pakistan on Telehealth (eHealth) activities are given below.
Detailed comparison in terms of their feasibility, reach/access, quality, cost effectiveness, value
for money and scalability is given in the Table 1. Projects Tertiary care facility to secondary care facility Secondary care facility to
primary care facility Healthcare services at community home/ everywhere
Telemedicine connection has been developed between Holy Family Hospi tal & Jinnah Hospi tal to Gambat Institute along with number of district level facili ties in Attock, Pindigheb, khushab, DG Khan, R Y Khan, Mi than Kot, Jhang, Rajanpur and Gujrat.
Aga Khan Health Service in col laboration with AKDN eHealth Resource Center, Aga Khan University in providing service to primary health facilities of Hunza and Ghizer district to Gilgit Medical Center.
Aman Foundation's Telehealth and Teledoctor
Feasibility in local context
It has been adopted well in the community and with communites’ buy in.
Due to remoteness of the site i.e. northern high range mountain area and limi ted funding,the system util ized low bandwidth and implemented store and forward and low end live models. Store and forward facility was not in local language but still due to high literacy rate of the community they understood the system which worked wel l
Cal l center has been extensively revised in tern of local context. They have enrolled and trained many agents knowin local languages. This has helped call center in adjusting in local context.
Reach/ access It has reached only district level population but rural community si tes can only access the service through district level faci lities.
These are primary health facility and relatively close to community reach but the hub site where they are getting consul tation is more than 120Km away from the primary care centers and along with hard mountainous traveling it cost more than 2000PKR to reach the hub
Cal l center has strengthened the community by giving access via mobile phone. They have reached the unreached population and benefi ted through universal number, targetingmetropolitan city first 'Karachi' estimated18Mil lion population.
Quality
Healthcare provider has been providing specialized care in this service and qual ity of the service is constantly increasing in terms of expertise and related indicators have been strengthened.
Telehealth services have increased the quali ty of service in primary healthcare but is stil l not measured in term of indicators and restricted to family medicine services only.
Cal l center have setup some monitoring indicators through which they have been measuring the quality of the services and also take feedback from the users to ensure the quality provided to clients.
Cost effectiveness of the system
System requires high amount of capi tal investment in term of video conferencing equipment and telehealth equipment. Most of the facilities are using VSAT connectivity which is a high cost network but its getting cost effective by providing DSL Internet service wherever available.
System requires less amount of capital investment in term of desktop video conferencing equipment and telehealth equipment. Most of the facili ties are using EDGE/ GPRS/ DSL connectivity which is a low cost network - but unstable - and is getting strengthened with time by the infrastructure.
System requires heavy capital and operational investment. System is expensive but accessing the system for patient is very cheap.
Value for money In this service patient has not been charged that’s why patient does not value the service in term of money. As they are not paying anything so they can’t be dependent on it.
In this service patient has not been charged that’s why patient does not value the service in term of money. As they are not paying anything so can’t be dependent on it. Due to a survey and public awareness by lady health visitors of primary health facility, community has understood that it is saving their travel and logistic cost.
In this service patient has not been charged that’s why patient does not value the service in term of money. As they are not paying anything so can’t be dependent on it.
Scalability The model is very successful with avai lability of cost effective DSL fiber connectivity and decrease in equipment cost it is scalable.
The model is very successful with availabi lity of cost effective mobile connectivity and decrease in equipment cost it is scalable.
This facil ity is different in it kind, it gets strengthened and cost effective with more scalability in term of extending reach to population.
LEAD PakistanDiscussion Paper Series
Towards a National eHealth/Telehealth Strategy for Pakistan:Experiences, Challenges and Opportunities

to have a framework of strategic plans and policies were recognized:
that lay the foundation for development.”[26]. A
2002 study on eHealth policies, identified 20 æ Identify regional priorities and challenges
countries with a defined eHealth policy or activity
æ Foster strategic partnershipsin policy development. Policy and policy
development were not necessarily at a national æ Reach consensus on projectslevel and several, including the U.S., were at state,
æ Promote information and expertise exchange.provincial or territory levels. These early adopters
were Australia, Canada, China, Croatia, Denmark,
Finland, Iran, Malaysia, Malta, New Zealand, Nineteen members joined dialogues in East and Russia, Singapore, South Korea, Sweden, Taiwan, West Africa and South Asia. Kenya, The Maldives Tanzania, Thailand, United Kingdom, U.S. and and Uganda received direct support. Seven Vietnam [27]. The WHO GOe Report found that members joined the Southern African Workshop. 25% of responding countries had a national Partners included East, Central and Southern telemedicine policy or strategy. The African, Africa Health Community (ECSAHC), West African Eastern Mediterranean, and South-East Asian Health Organization (WAHO) and the African Union Regions currently show the lowest rates of national Commission (AUC). Eleven additional issues telemedicine policy implementation, but the identified include affordability, human and ICT highest projected growth. The European Region capacity and risk mitigation.was the most advanced in this area, with
approximately 40% of responding countries iii. Act 564, the having a national telemedicine policy. By Telemedicine Act of 1997, aims “to provide for the comparison, only 10% to 15% of responding regulation and control of the practice of countries in the Eastern Mediterranean, South-telemedicine; and for all matters connected East Asian, and African Regions reported having a therewith”. The Law drafters have sought to national policy [25].protect their citizens from doctors or others who
might not be clinically competent. Section 3 of the The following is a brief description of some Act describes persons who may practice national and regional eHealth Policies: telemedicine in Malaysia and requires that they be
“…a fully registered medical practitioner holding a
valid practicing certificate.” If the consultation is i. In
with a doctor outside of Malaysia, then that doctor 2004, the European Commission (EC) presented
must hold, “a certificate to practice telemedicine an eHealth Action Plan, calling on Member States
issued by the Council (Malaysian Medical to develop their eHealth Roadmaps to 2010 [28-
C o u n c i l ) ” a n d t h e d o c t o r m u s t 29]. This plan is part of achieving the Lisbon
practice“telemedicine from outside Malaysia Strategy and looks to the creation of a European
through a fully registered medical practitioner eHealth area [28], free patient mobility and
holding a valid practicing certificate.”empowerment of the citizen through eHealth
Services and interoperability [30].
iv. The policies for eHealth laws in India
offer the following guidelines for international ii.
practice of telemedicine across borders: [33]In 2008, at the Commonwealth Health Ministers
Meeting (CHMM), the following eHealth priorities
Malaysian Telemedicine Act [32]:
eHealth Policy for the European Union:
India:
Commonwealth Priorities and Guidelines [31]:
Dec
embe
r 201
2
08
Chapter 2
2. The World Health Assembly is the decision-making body of WHO. It is attended by delegations from all WHO Member States and focuses on a specific health agenda prepared by the Executive Board. http://www.who.int/mediacentre/events/governance/wha/en/index.html
2

(i) Mutual recognition between countries to æ Harmonizing health and technology expertise,
recognize the license granted by the home country æ Phased implementation of prioritized eHealth to allow doctors to practice in other countries. initiatives, and
(ii) Reciprocity between countries where licensed æ Business continuity plans (redundancy) in doctors can practice in both countries. critical aspects of eHealth system, such as
(iii) Registration, “where the doctor submits to the security and disaster planning.
legal regime governing medical negligence and
malpractice in the country where the patient vi. Key Themes and Contents for the eHealth
resides or communicates from, but not the Policies: The literature review conducted by Khoja
licensing requirements for doctors in that and Durrani et al [35], identified ninety nine policy
country.” issues related to eHealth. These were grouped
(iv) Limited licensure where a doctor obtains under nine themes on the basis of similarities in limited licensure through a licensed referring their application:doctor in the country from where the patient
communicates or resides in.
1. Networked care.
2. Inter-jurisdictional practicev. The recent
3. Diffusion of eHealth / Digital Dividestrategy document lays down the vision, mission,
objectives and the five strategic areas of 4. eHealth integration with existing systemsintervention. The new strategy focuses on
5. Response to new initiativesimproving the management of information in five
6. Goal-setting for eHealth policysectors: telemedicine, health information
systems, information for citizens, mHealth and 7. Evaluation and research eLearning. To aid implementation, the strategy
8. Investment subdivides the Health Information Systems pillars
9. Ethics in eHealth.into various functional domains:
The list of policy issues and their categorization æ Patient centric information under each theme is given in Annexure 1.
æ Pharmacy and medical supply chain
information system
æ Financial Information, including insurance
and payments
æ Health workforce management and training
æ Regulation.
The strategy also identifies the key factors and
principles of success, which include:
æ S t r o n g l e a d e r s h i p a n d g o v e r n a n c e
mechanism,
æ Collaboration and partnership,
æ Leveraging available resources,
æ Safeguarding privacy and security,
eHealth Strategy of Kenya : [34]
09
LEAD PakistanDiscussion Paper Series
Towards a National eHealth/Telehealth Strategy for Pakistan:Experiences, Challenges and Opportunities

Challenges in eHealth/Telehealth Planning and
Implementation for Pakistan
have to be carefully observed especially when we
are dealing with teleconsultation across provinces
and consultations with rural respondents in
discussing reproductive health issues. Rural areas
have increased barriers to culturally appropriate
healthcare through eHealth because of increased
rates of poverty, increasingly large ethnic minority
populations, and various degrees of geographical
isolation and cultural factors specific to rural
communities. Although culture and language are
major barriers to receiving appropriate eHealth
services, they cannot be separated from other
related influential variables, such as poverty and
geography. Each of these critical issues must be
taken into account when planning technologically
enabled rural health care services.
b) Social Factors: In Pakistan, just like other
developing countries, equivalent services are
expected in both urban and remote locations.
Citizens are increasingly expecting the same
consistent and equitable health care access
across remote regions as in densely populated The rapid expansion of the use ICT in other non- urban centers; significantly differences between health sectors in Pakistan already provides the health outcomes for advantaged and opportunities for collaboration and partnerships, disadvantaged populations (urban/rural, which can be used as building blocks for eHealth economic status and literacy disparities). The use policies, applications and strategies. However of eHealth within or between institutions involves eHealth poses many challenges related to the number of factors that require proper planning, technology and health information among others, supported by well-defined policies, rules, and therefore the right policies, strategies, standards or guidelines at the institutional, organization, resources and institutions need to jurisdictional and global levels. Absence of these be in place in order to realize maximally its policies may lead to several problems during the benefits. Some of the challenges which eHealth cycle of eHealth planning, that may lead either to development faces in Pakistan are as follows: failures in achieving the intended goals, or
inadvertent widening of gaps in health status and
knowledge levels between different sectors of the a) Cultural Factors: In Pakistan, there always population and increasing rather than decreasing have been strong cultural influences, with people health inequity, also termed as 'Digital Divide' coming from different background and tribes. The [37]. cultural policy document of Pakistan outlines
protection for groups and individuals with a
distinct language, script or culture (Article 28) and c) Change Management: eHealth and Telehealth the discouragement of parochial, racial, tribal, in Pakistan is in a unique situation where the need sectarian and provincial prejudices (Article 33) for awareness, capacity and innovation has where every second province and districts are occurred simultaneously. A huge majority of distinct from each other [36]. In eHealth during healthcare providers and other staff working in teleconsultation the cultural norms and values both public and private sector hospitals and other
Dec
embe
r 201
2
10

healthcare settings are used to the orthodox way of functions are scaled back and it is made
handling information (mainly through paper compatible with devolution. However, since
records) and are unaware of the advancements in ministerial abolition has become symbolic of
eHealth. There is thus a huge need for introducing provincial autonomy, there is need to explore the
these technologies to healthcare providers and next best alternative, which can enable retaining
policy-makers at the institutional or government national functions in health at the federal level.
levels, so that they can take informed decisions This should now be the objective of planning in the
about the use of technology with its benefits and health stream, post 18th Amendment”. [41]
risks.
The draft of National Health Policy of Pakistan of
Resistance to change has become rooted in 2009 (was published as draft form, but after the
certain professional roles – the introduction of ICT 18th amendment is not officially recognized now
in healthcare disrupts traditional structures and as National Health Policy 2009) seeks to improve
hierarchies. Frequently, professionals are the health indicators of the country. It aimed to do
unwilling to collaborate in recording and so by delivering a set of basic health services for all
exchanging patient data, with concomitant by improving health manpower, gathering and
distrust for on-site data storage and access using reliable health information to guide program
control [38]. effectiveness and design, and strategic use of
emerging technology.
The effectiveness of the telehealth relies on the
adaptation of professional practices, the setting In this new scenario the Provincial Ministries of
up of adequate coordination mechanisms Health will play a pivotal role, not only in meeting
between participating institutions as well as the people's needs for care and protecting public
adaptation of organizational practices within the health, but in preserving health systems through
institutions. Besides the technology aspects, uncertain times. Promotion and adoption of
change management must also take into account eHealth and Telehealth also stands on the
work relations between involved professionals and Provincial Ministries of Health shoulder. The
the organizational procedures that support them Provincial Ministries of information Technology
[39]. and Telecommunications are also essential to
development in all spheres and can make a vital
contribution to the health sector. d) G o v e r n a n c e : 18 t h A m e n d m e n t a n d
Positioning eHealth Within Provincial Health
Systems: After the 18th Amendment, it was The Role of Federal Government for broader
perceived that now health would fall exclusively in eHealth development also remains critical. To
the domain of the provinces. The provinces have promote the national eHealth agenda, it is
shown willingness to finance and manage new necessary that a national eHealth governance
responsibilities, however, various issues mechanism is established at the federal level. This
pertaining to human resource, distribution of will lead to follow common goals and a predictable
f inances and resources needs a careful ICT environment enable coordinated action:
examination by the Federal Government [40]. building consensus on policy, facilitating better
use of shared resources and regulation of the
private sector, and investment in ICT skills and Some health policy experts also propose that “the
infrastructure to improve health outcomes. Ministry of Health should not be abolished; it
should be recast so that its service delivery
11
Chapter 3
LEAD PakistanDiscussion Paper Series
Towards a National eHealth/Telehealth Strategy for Pakistan:Experiences, Challenges and Opportunities

12
There is a clear danger that by failing to adopt ICT have different methods of recording and storing
solutions in health sector by the provincial data. The context of each site, the perspectives of
government the public sector may become the individuals working within them and the
incapable of competing with the private operators, patterns by which they work, are also likely to
create further silos of care and cause delays and differ. These factors will influence the effective use
needless duplication, leading to underdeveloped of, and clinical benefit resulting from, a
health information systems and capacities. telemedicine application and the extent to which
similar results can be expected in other
organizations [43]. The technical features and An important part of the eHealth policy will be the
performance of a telemedicine application will governance structure for eHealth in Pakistan;
also influence the clinical results, for example if an noting the fact that for the progress of the national
application does not allow clinicians to follow their eHealth agenda, a national eHealth governance
normal work routines, it may not be used and thus mechanism needs to be established and
will not produce clinical benefits [44].maintained. This structure will start with a National
eHealth Secretariat. The proposed Secretariat will
have representatives of provincial ministries of eHealth evaluation must examine not only to what
h e a l t h , m i n i s t r i e s o f i n f o r m a t i o n a n d extent an application was effective, but also why it
communication technology and also ministries of was or was not ef fective. An evaluation
education. To avoid bureaucratic hurdles, it would methodology must utilize health information data
have been better to give the the Secretariat an not only from traditionally utilized, mainly
autonomous status. quantitative health information sources (e.g.
medical records data), but also from qualitative
sources (e.g. interview data with doctors and e) Monitoring & Evaluation: There are many
nurses). Due to the infancy of telemedicine challenges to producing reliable evidence about
projects, reliable evaluation methodologies, the ef fects of telemedicine applications.
which consider both if and why an application was Evaluation is rarely seen as an integral part of
effective, have not been tested. Monitoring of an implementation, thus resources are not usually
eHealth program and making it knowledge is still a dedicated to evaluation. Sometimes resources are
missing component in eHealth programs.dedicated after implementation, so prospective
collection of baseline data is not possible.
Retrospective collection of health information f) Technology: Use of ICT in Pakistan and other
presents many challenges in terms of identifying similar developing countries has grown at a
appropriate sources and collection techniques. tremendous pace. Most of this use is driven by
These issues complicate the evaluation of many reduction in Internet charges, high use of mobile
interventions, while the specific nature of phones and PDAs, and lowering of hardware cost.
telemedicine evaluation presents fur ther These enablers have lead to high teledensity and a
complications [42]. Most telemedicine tremendous increase in connectivity [45].
interventions have been pilot projects, limited to a
single site and influencing the care of a small This growth calls for opportunities to explore ICT
number of patients. This limits the extent to which use in healthcare. With current growth in ICT, it is
traditionally employed methods of enquiry and possible to expand the use of eHealth to more
statistical analysis can produce meaningful institutions and areas, but this would require
results about the clinical and economic impact of proper facilities to test current technologies, and
an application (e.g. randomized controlled trials introduce them to the healthcare providers to
are designed to evaluate large, not small, improve their awareness and skills. At the same
populations). Telemedicine applications depend time, huge demand for capacity building for the
on communication between two sites that may
Dec
embe
r 201
2

new and existing technology has also grown in the g) Sustainability: Sustainability defines an
healthcare institutions. There is a need for well- eHealth system which has passed the pilot phase
organized hands-on training programs for health and is fully operational to provide data for
professionals and the support staff. These assessing its overall performance in line with a set
programs can provide better learning if conducted of predefined benchmarks and indicators [48].
in laboratory settings, using simulators or models,
rather than a real-life situation. Finally, it is In Europe there are three different approaches of
important to keep the door of innovation open healthcare financing. First system is centered on
because of the novel and unique nature of e-health public taxation [49]. Second is on utilizing
products. There is a need for spaces where compulsory social insurance [50]. Third is based
products and ideas from industry can be shared on private finance through voluntary insurance
with the healthcare providers during the that operates via links with standard social
development phase, and take feedback on how to insurance. Along with these approaches, there are
amend these products based on the needs of its several costs sharing ways through which patients
users. This can best be achieved if users can get contribute to healthcare financing.
hands-on experience on these technologies and
also use it in simulated situations that are close to
their real-life settings. Thus a combination of Telehealth history in Pakistan shows that in funded awareness building, skills-development and projects whenever funding is exhausted, the innovation research can provide best path to move project also finishes. In this regard the biggest forward with eHealth technologies. challenge is to build remuneration/incentives on
each teleconsultation to doctors of both sides.
Insurance and reimbursement should insulate Any policies and guidelines designed for an
providers and patients from the immediate eHealth policy should allow greater penetration of
financial consequences of the use of expensive telecommunication companies, such as mobile
technologies [38]. Similarly mechanism of companies, Internet service providers, integrated
charging for consultation through a call center is services digital network providers, and satellite
still a challenge. vendors, to reach the poorest communities,
reduce the cost of telecommunication, provide
universal and unlimited access to the Internet, and Joint investment and development involving users, allow for appropriate use of eHealth for governments, academic and financing institutions commercial and humanitarian purposes. Both and agencies, technical co-operation agencies government and private sector can play their part and industry interests is seen as necessary to in achieving these objectives. create sustainable eHealth solutions.
In Pakistan's national IT Policy [46], one of the Speeding up eHealth adoption depends on the goals is to promote extensive use of IT applications presence of factors such as incentives, in education, health, and other sectors with competition, return on investment, and regulation. widespread use of the Internet. Governments must establish mechanisms to
create or secure markets for new eHealth By March 2013 Pakistan will have 3G connections
technologies, which will propose cheaper eHealth and this will eventually decrease the cost of
solutions, thus reducing the risks involved in connectivity with increase in the speed of internet
Research and Development and improving the across the country, which will add positively to the
chances of a satisfactory return on investment in eHealth and m-Health development in Pakistan
eHealth for the private health subsector.[47].
13
LEAD PakistanDiscussion Paper Series
Towards a National eHealth/Telehealth Strategy for Pakistan:Experiences, Challenges and Opportunities

14
h) Ethical Issues: In 1999, the 51st World makers to take initiative and introduce changes for
Medical Association (WMA) General Assembly in further collaboration among various vertical
Tel Aviv adopted a policy statement on health program information systems and integrate
“Accountability, Responsibilities and Ethical them into one system. In the current system the
Guidelines in the Practice of Telemedicine.” It flow of information in the vertical and horizontal
included the following: “Because of the risks of information system are not yet integrated with
information leakage inherent to some types of each other. The integrated approach will not only
electronic communication, the physician has an save the resources but will also improve the
active obligation to ensure that all established efficiency of the information system as a whole. It
standards of security measures have been is also required to encourage utilization of
followed to protect the patient's confidentiality.” information at the facility level by providing up-to-
This is an unachievable goal in the developing date and quick access to information.
world and indeed in the developed world, where
telephony is a form of telemedicine. The WMA For achieving optimal degree of integration, all
General Assembly rescinded the Statement in healthcare professionals, particularly physicians
2006 [51]. It adopted a revised Statement on the and nurses have to play a key role in establishing
Ethics of Telemedicine at the 2007 WMA General the strategy of integration at all levels of
Assembly [52]. The section on data security now healthcare. Planning and developing a national
reads, “The physician must aim to ensure that strategy can be the guiding principle in
patient confidentiality and data integrity are not approaching the proverbial finish line, where tools
compromised. Data obtained during a telemedical such as information technology (IT) should be
consultation must be secured through encryption indispensable to support us on this long and
and other security precautions must be taken to arduous path [53]. In spite of the proven
prevent access by unauthorized persons.” The importance of telehealth service, it is still not
problem now is with the definition of “data.” Do being integrated as a component in the
digital telephones transfer or transmit data, and mainstream healthcare system.
what of videoconference teleconsultations?
Similarly, countries looking at the Malaysian
Telemedicine law as a model, may find themselves
actually blocking the use of inter-jurisdictional
practice of eHealth. In Pakistan, as no policy or
s t r a t e g y e x i s t s o n h o w t o c a r r y o u t
teleconsultation, no ethical guidelines have been
formulated. Patient confidentiality and data
integrity remains a concern.The case for adopting eHealth technologies has
been evident for over a decade. However, it has i) Integration with Health Service: The Integrated taken a crisis in the health sector in many countries Health System will build a complete record of the to move eHealth from the periphery to the centre of medical history of individuals that includes any strategic health planning. In an increasingly digital diseases they suffered from, treatment methods world, spurred by technological advances, and medications received, and concentrates on economic investment, and social and cultural the medical phenomena that affect patients' changes, there is growing recognition that future. Specialists and service providers will inevitably the health sector must integrate ICT into record such information. The system will consist of its way of doing business. an information system enabling retrieval of all
data, health indicators, consultations and Developing a national eHealth programme is a medical opinions concerning the individual. The goal of many countries. A national eHealth scenario in Pakistan demands the decision
The Way Forward:
Dec
embe
r 201
2

programme can contribute to reaching health and context. The ICT applications used may themselves
development goals, and for some countries, will be innovative, but the projects are rarely
constitute a major step towards implementing sustainable. They fail because of a lack of
recommendations such as those of the United infrastructure and skills, a narrow focus on one
Nations Millennium Development Goals: Target 18 particular aspect of eHealth that disregards other
(in co-operation with the private sector, make concerns and impacts, and a lack of ownership by
available the benefits of new technologies, the health entities involved. The use of ICT in the
especially information and communications) and general population in Pakistan is limited to not
Recommendation Three of the Commission on much more than mobile phones. The commercial
Information and Accountability for Women's and ICT market is fragmented, with little local expertise
Children's Health (integrate the use of Information available. The government has no role in funding
and Communication Technologies in countries' and technical support for eHealth. This comes
national health information systems and health i n s t e a d f r o m a i d a g e n c i e s , d o n o r s ,
infrastructure). Experience has shown that nongovernmental organizations (NGOs) and
harnessing information and communication consultants. In this constrained environment,
technologies (ICT) for health requires planning at Pakistan lacks in its international obligations for
the national level, to make the best use of existing public health reporting.
capacity while providing a solid foundation for
investment and innovation. Establishing the main The driving factors for eHealth in case of Pakistan
directions, as well as planning the detailed steps are improving access to health care for the
needed, is the key to achieving longer-term goals citizens, and improving the quality of that care.
such as health sector efficiency, reform or more Classic examples of eHealth include provision of
fundamental transformation. telemedicine services to remote areas, and
asynchronous consultations such as via e-mail for
A country's eHealth strategy should be based on access to medical advice.
national health priorities, the available and
potential resources, and the current eHealth For a national plan, Pakistan should focus on
environment. A national vision for eHealth also making the case for eHealth, creating awareness
takes shape within a national context that can be and establishing a foundation for investment,
considered in terms of two dimensions. The ICT workforce education and adoption of eHealth in
environment represents the national ICT market priority systems and services. There is a common
and overall penetration of computing and misconception that countries can “leapfrog” to
networking infrastructure. The enabling more advanced eHealth systems. But without a
environment for eHealth is fundamental to scaling parallel focus on creating the enabling
up and sustaining ICT adoption in the health environment, innovations in ICT will stay isolated
sector. It includes aspects such as governance, and have only a limited impact on health.
policy, legislation, standards and human
resources.
The benefits of eHealth have not been fully
harnessed by Pakistan due to lack of an enabling Pakistan is a country where the ICT environment
eHealth policy framework. eHealth policy maps and enabling environment for eHealth are both in
out national vision, goal and strategy for rational their early stages. Within this national context,
introduction and application of ICTs for health and eHealth is project-based, featuring a few small
healthcare for maximum benefit.initiatives that are seldom connected to each
other. Projects tend to be time-limited, proof-of-
concept pilots, where ICT is introduced (or The policy should guide all national and imported) to demonstrate a technology in a limited international development ef for ts toward
15
LEAD PakistanDiscussion Paper Series
Towards a National eHealth/Telehealth Strategy for Pakistan:Experiences, Challenges and Opportunities

achieving the national goal of health for all. should also provide a vision and clear guidance to
eHealth policy must form an integral part of the all stakeholders such as the public, patients,
overall national health policy, ICT policy and other health professionals and others. The presence of a
development policies. The policy should provide a clear national eHealth policy facilitates
framework for enhancing ICT effectiveness for mainstreaming and coordination of eHealth
equitable health care delivery in line with the applications by all planners and implementers (eg
national health policy and strategies, and other government and donors) thus ensuring synergy
relevant policies, taking into account the country's and minimizing resource wastage
priorities, resources and capabilities. The policy
16
Dec
embe
r 201
2

Last Word:
Countries like Pakistan can focus on a range of
structured activities that lead to the progressive
development of a national eHealth strategy. These
include:
a. Involving the key health and non-health
stakeholders in creating a national eHealth vision
and plan and its subsequent implementation.
b. Forming an understanding of the current
eHealth environment in terms of the programmes,
projects and eHealth components that already
exist.
c. Establishing the strategic context for eHealth
to provide the foundation for the eHealth vision
and plan, and to enable the government to make
informed decisions on whether to pursue
opportunities that present themselves from the ICT
industry and other stakeholders.
d. Establishing governance mechanisms to
provide improved visibility, coordination and
control of eHealth activities that are occurring
across the country's health sector.
e. The country should also identify the short-,
medium- and long-term goals for eHealth
development, recognizing the importance of
demonstrating outcomes and benefits throughout
the process of national eHealth strategy
implementation, and
f. To build and maintain momentum and support
for eHealth.
17
Chapter 4
LEAD PakistanDiscussion Paper Series
Towards a National eHealth/Telehealth Strategy for Pakistan:Experiences, Challenges and Opportunities

18
Dec
embe
r 201
2

19
AnnexureThemes Policy Categories Issues
Networked Care A. Global eHealth policies
a) Functional and Semantic interoperability
b) Standardization of Electronic Health Record (EHR)
c) Intellectual property rights
B. Jurisdictional (National and
Provincial/ Sub-National)
policies
a) Regulation of appropriate technologies
b) Commitment of funds
c) Standardization of EHR
d) Sharing of services
e) Proper connectivity
f) Controlling malpractice
g) Cultural issues in communication
C. Institutional/ Individual
policies
a) Proper distribution of human resources
b) Readiness building and effective change management
c) Deployment of appropriate technologies
d) Meeting the needs of insurance companies
e) Reimbursement and Remuneration
f) Sharing of patient information
g) Sharing of knowledge
h) Sharing of services
i) Standardization measures for EHR
j) Ensuring Integrity and quality of data / information
k) Proper connectivity
l) Risk management
m) Cultural issues in communication
Inter-jurisdictional Practice
A. Global eHealth policies
a) Policies on managing health information on the Internet
b) Intellectual property rights
c) Complimenting policies and healthcare regulations in different
regions
d) Sharing of knowledge
A. Jurisdictional (National and
Provincial/ Sub-National)
policies
a) Accountabil ity/ liabil ity of care
b) Licensing
c) Accreditation of services
d) Local, National and international policies
B. Institutional/ Individual
policies
a) Accountabil ity/ liabil ity of care
LEAD PakistanDiscussion Paper Series
Towards a National eHealth/Telehealth Strategy for Pakistan:Experiences, Challenges and Opportunities

Diffusion of eHealth/ Digital Divide
A. Global eHealth policies
a) Telecommunication policies allowing increased access
a) Controlling cost of technology
b) Providing Universal and unlimited access to Internet
c) Humanitarian vs. Commercial policies
d) Sharing of knowledge and services
b) Jurisdictional (National and
Provincial/ Sub-National) policies
a) Increasing focus on open-source technologies
b) Telecommunication policies allowing increased access
c) Controlling cost of technology
d) Capacity building
c) Institutional/ Individual
policies
a) Capacity building
eHealth integration with existingsystems
A. Jurisdictional (National and
Provincial/ Sub-National) policies
a) Improving clinical effectiveness
b) Improving quality of care
c) Change in business rules in organizations
B. Institutional/ Individual
policies
a) Redefining the roles and responsibil ities of different players
b) Wider ethical acceptability
Response to new initiatives
A. Jurisdictional (National and
Provincial/ Sub-National) policies
a) Defining the stakeholders at different levels
B. Institutional/ Individual
policies
a) Defining the roles and responsibil ities of different players, such as local providers and specialist
b) Change management
c) End-user support
d) Regulating IT use
e) Maintaining doctor-patient relationship
f) Wireless networks and securit y issues
g) Evaluation of new technologies in local environments
Goal-Setting for eHealth Policy
A. Global eHealth policies
a) Making eHealth part of the overall development effort
b) Funding of eHealth programs
B. Jurisdictional (National and
Provincial/ Sub-National) policies
a) Providing suitable telecommunication infrastructure to promote eHealth
b) Aligning policies with IT innovations
c) Innovative and forward looking policies
d) Covering for the opportunity cost of health providers’ time
e) Timing of government action
f) Developing leadership structures for eHealth programs
g) Developing strategies for eHealth adoption
h) Information governance
A. Institutional/ Individual
policies
a) Standards of care
b) Guidelines for human resources
Evaluation &Research
A. Jurisdictional (National and
Provincial/ Sub-National) policies
a) Justification of Health providers’ time
b) Cost-effectiveness
c) Impact of eHealth on healthcare management
d) Demonstrate health outcomes
e) Evidence on clinical effectiveness
f) Progress in learning
B. Institutional/ Individual
policies
a) Providing simulation environment
b) Encouraging coordinated research
c) Dissemination for policy-making and benefit of others
Investment A. Jurisdictional (National and
Provincial/ Sub-National) policies
i. Use of eHealth for commercial purposes
ii. Public-Private Partnership
iii. Cross-border advertisement and sale of drugs
Dec
embe
r 201
2
20
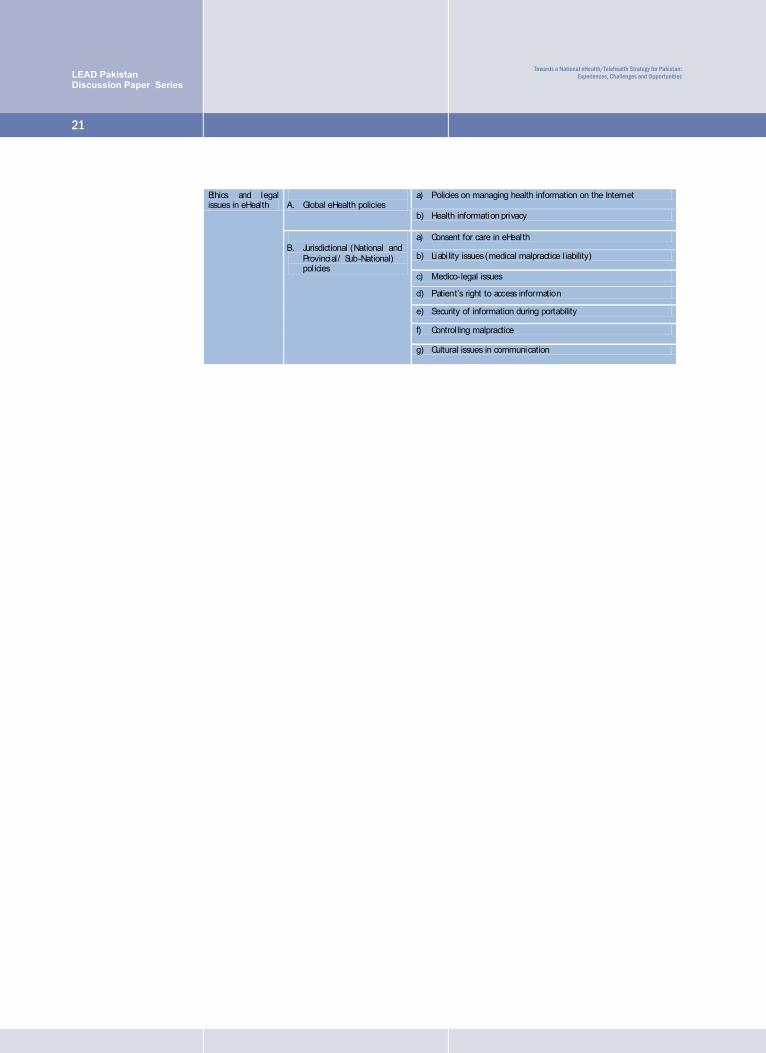
Ethics and legal issues in eHealth
A. Global eHealth policies
a) Policies on managing health information on the Internet
b) Health information privacy
B. Jurisdictional (National and
Provincial/ Sub-National) policies
a) Consent for care in eHealth
b) Liability issues (medical malpractice liability)
c) Medico-legal issues
d) Patient’s right to access information
e) Security of information during portability
f) Controlling malpractice
g) Cultural issues in communication
21
LEAD PakistanDiscussion Paper Series
Towards a National eHealth/Telehealth Strategy for Pakistan:Experiences, Challenges and Opportunities

1. World Health Organization. (2005), Global Observatory for eHealth. Retrieved November 7, 2007 Last
accessed 10.10.2012 URL [http://www.who.int/kms/initiatives/ehealth/en/]
2. World Health Organization, Resolution and Decision, Fifty-Eighth World Health Assembly, Geneva, 16-25
May, 2005 Last Accessed on 10.10, 2012 URL http://apps.who.int/gb/ebwha/pdf_files/WHA58-
REC1/english/A58_2005_REC1-en.pdf
3. Al-Shorbaji N, e-health in the Eastern, Mediterranean Region: a decade of challenges and achievements,
Eastern Mediterranean Health Journal, Vol. 14, Special Issue
4. G Eysenbach, What is eHealth? J Med Internet Res 2001;3(2):e20) last accessed on 12.10.2012 from
http://www.jmir.org/2001/2/e20/
5. Wotton R, Craig J, & Patterson V (2006). Introduction to Telemedicine. (2nd ed.) London, UK: Royal
Society of Medicine Press Ltd.
6. Bath P. Health Informatics: Current Issues and Challenges. Journal of Information Science.
2008;34 (4):501-518.
7. Tavangarian D, Leypold ME , Nölting K, Röser M, Voigt D, Is e-Learning the Solution for Individual
Learning? Electronic Journal of e-Learning Volume 2 Issue 2 2004 (273-280)
8. Istepanian, R., Laxminarayan, S., & Pattichis, C. (2006). M-Health: Emerging Mobile Health Systems. NY:
Springer.
9. Clark, T., Adopting health care informatics and technologies. Am J Health-Syst Pharm, Jan 2007. 64.
10. Heinzelman, P., Williams,CM.,Lugn NE.,Kvedar JC., Clinical outcomes associated with
telemedicine/telehealth. Telemed J E Health, 2005. 11: p. 329-347.
11. Ouma, S., Herselman, ME., E-health in Rural Areas: Case of Developing Countries. Int J Biolog Med Sci,
2008. 4: p. 194-200).
12. Walraven G, Manaseki-Holland S, Hussain A, Tomaro JB, Improving Maternal and Child Health in Difficult
Environments: The Case For “Cross-Border” Health Care, PloS Medicine, Jan 2009, 6 (1): p. 17-21
13. Health Metrics Network. (2005). Health Metrics Network: What it is, what it will do and how countries can
benefit. Geneva: World Health Organisation. Available from: www.who.int/)
14. Ali M, Hoikoshi Y, Situation Analysis of health management information systems in Pakistan; Pakistan J.
Med. Res. Vol.41 No.2, 2002.
15. World Health Organization, Country Profile: Pakistan, Last accessed on 6.10.2012, URL
http://www.who.int/countries/pak/en/).
16. Health and Nutrition, Economic Survey of Pakistan 2011-2012, Last accessed on 6.10.2012, URL
http://www.finance.gov.pk/survey/chapter_12/highlights.pdf
17. Stakehodler Telehealth workshop Report, by Lead Pakistan dated 23th September, 2012
18. Telemedicine and eHealth Training Centre, Holy Family Hospital, Rawalpindi, last accessed on 18.10.2012
from http://www.telemedicine.pk/
19. Progress Report of Telemedicine Mayo Hospital, 2009-2011 last accessed on 4.10.2012 from
http://www.telemedmayo.com/Telemed%20report%20mayo%20Hospital.pdf
20. eHealth response to flood Disasters in Gilgit Baltistan and Chitral, last accessed on 4.10.2012 from
http://www.ehap.net.pk/index.php?option=com_content&view=article&id=106&Itemid=105
21. Aman Telehealth, last accessed on 4.10.2012 from http://amanfoundation.org/health/aman-tele-
BibliographyD
ecem
ber 2
012
22

23
heath/telehealth/
22. Latifi R. The Do's and Don't's when You Establish Telemedicine and e-Health (Not Only) in Developing
Countries. Current Principles and Practices of Telemedicine and e-Health. 2008;131:139-43.
23. Bashshur R, Shannon G. National Telemedicine Initiatives: Essential to Healthcare Reform.
Telemedicine and e-health. 2009;15(6):1-11.
24. Scott RE. Future proofing telehealth in developing Countries. J Telemed Telecare. 2007;13(Suppl 3):70-
72.
25. WHO Global Observatory for eHealth Report on Telemedicine-Opportunities and developments in Member
States URL http://whqlibdoc.who.int/publications/2010/9789241564144_eng.pdf [last Accessed: 17-10-
2012]
26. Kay,M., van Andel, M O-G, Klint, K, Tristram, C. Building Foundations for eHealth. Progress of Member
States. Report of the WHO Global Observatory for eHealth. 2006:1-326. Switzerland, WHO Press.
27. Scott,R.E., Chowdhury,M.F.U., Varghese,S. Telehealth policy: looking for global complimentarity. Journal
ofTelemedicine and Telecare 2002;8 (Suppl 3 ):55-57.
28. European Council European Council (2006): Council Conclusions on Common Values and Principles in the
European Union Health Systems. Document (2006/C146/01). Official Journal of the European Union
2006:3.
29. Commission of the European Communities. Commission of the European Communities - COM (2004)
356: Communication from the Commission to the Council, the European Parliament, the European Economic
and Social Committee and the Committee of the Regions: making health care better for European citizens: An
action plan for a European eHealth Area. 2004.
30. Wilson,P., Leitner, C H, Moussalli, A. Mapping the Potential of eHealth, Empowering the citizen through
eHealth tools and services. 2004
31. Commonwealth Secretariat e-Health Initiatives Progress Report to Commonwealth Health Ministers,
Commonwealth eHealth Secretariat last accessed on 8.10.2012, from
http://www.thecommonwealth.org/files/189921/FileName/HealthProgressReports-E-Health.pdf
32. Telemedicine Act 1997 (Malaysia). URL:
http://unpan1.un.org/intradoc/groups/public/documents/APCITY/UNPAN025631.pdf [Accessed: 17-10-
2012].
33. Health information and telemedicine: legal framework. A preliminary report. 2003: [Accessed: 17-10-
2012].] URL: http://www.mit.gov.in/telemedicine/annexure8a.pdf 1-26.10
34. Kenya eHealth Strategy 2011-2017, Ministry of Medical Services and Ministry of Public Health and
Sanitation, 2011. [Accessed: 17-10-2012]. URL.
http://svn.whomahler.net/hcicontent/ethiopia/lib/exe/fetch.php?media=workshops:ethiopia:kenya_final_
national_ehealth_strategy_2011-2017_.pdf.
35. Khoja S, Durrani H, . 'Scope of eHealth policy issues”, - J Med Internet Res- 2012. - 1 : Vol. 14. - p. e34.
36. Ministry of Culture, Pakistan Cultural Policy (draft), . [Accessed: 17-10-2012]. URL.
http://tinyurl.com/avv6u9u
37. Scholman B F. The digital divide: How wide and how deep? Online Journal of Issues in Nursing; 2004
[updated 2004; cited 2008 May 15th]; Available from:
http://www.nursingworld.org/ojin/infocol/info_14.htm.
38. Rodrigues, Roberto J. "Compelling issues for adoption of eHealth." The Commonwealth Health Ministers
Reference Book 2008
LEAD PakistanDiscussion Paper Series
Towards a National eHealth/Telehealth Strategy for Pakistan:Experiences, Challenges and Opportunities

39. Lamothe, L., Fortin, JP, Case Study: Managing Change in the Implementation of Telehealth Technology In
the Magdalene Islands, Quebec, The Telehealth Change Management Steering Committee, October 2006
40. National Management College, Strategic Appraisal Of 18th Amendment Federal/ Provincial Roles And
Impact On Service Delivery, National School Of Public Policy , Feb 2012
41. Nishtar S, Health and the 18th Amendment: Retaining National Functions in Devolution, last accessed on
12.10.2012 from http://www.heartfile.org/pdf/HEALTH_18AM_FINAL.pdf
42. Brear, Michelle. "Evaluating telemedicine: lessons and challenges." Health Information Management
Journal 35.2 (2006): 23-31.
43. Lorenzi, N. M. (2004). Beyond the gadgets. British Medical Journal 328(7449): 1146-7.
44. Kaplan, B. (2001). Evaluating informatics applications-some alternative approaches: theory, social
interactionism, and call for methodological pluralism. International Journal of Medical Informatics 64(1): 39-
56
45. Ministry of Information Technology, Government of Pakistan last accessed 10.10.2012 from
http://www.moitt.gov.pk/
46. IT& Telecommunication Division, Ministry of Information Technology, National IT Policy and Action Plan,
Link www.pakboi.gov.pk/pdf/National_IT_Policy.pdf, 2000, Last accessed 15.10.2012
47. Mehwish Khan, Prime Minister Approves 3G Policy in Pakistan, Pro Pakistani Blog, last accessed on
12.10.2012 from http://propakistani.pk/2011/11/23/prime-minister-approves-3g-policy
48. K. K. Lorenzo Valeri, Daan Giesen, Patrick Jansen, Business Models for eHealth Final Report. February.
2010,
49. Doron, Abraham. "The effectiveness of the Beveridge model at different stages of socio-economic
development: The Israeli experience." Beveridge and social security (1994): 189-202.
50. Hörl, W. H., F. De Alvaro, and P. F. Williams. "Healthcare systems and end-stage renal disease (ESRD)
therapies—an international review: access to ESRD treatments." Nephrology Dialysis Transplantation
14.suppl 6 (1999): 10-15.
51. World Medical Association. World Medical Association statement on accountability, responsibilities and
ethical guidelines in the practice of telemedicine 1999, Last accessed 02.10.2012 from URL:
http://www.wma.net/e/policy/a7.htm
52. World Medical Association. World Medical Association statement on the ethics of telemedicine, October
2007. Last accessed 02.10.2012 from URL: http://www.wma.net/e/policy/t3.htm
53. Prijatelj, Vesna, and U. Rajkovic. "From ehealth to integrated health care: theory and practice.
Dec
embe
r 201
2
24


LEAD Pakistan Occasional PapersNO. QTY.
25 Carbon Market Development in Pakistan: Issues and Opportunities by Malik Amin Aslam Khan
24 Corporate Response to Climate Change in Pakistan by Dr. Harish Kumar Jeswani
23 Breaking Moulds or Reinforcing Stereotypes? A Gendered Analysis of the Skills Development
System in Pakistan by Frida Khan
22 Pakistan’s Options for Climate Change Mitigation & Adaptation by Dina Khan
21 Alternative Dispute Resolution: The Informal Justice Sector in Pakistan by Dr. Iffat Idris
20 GDP Growth Semblance and Substance by Saeed Ahmad Qureshi
19 Water and Conflict in the Indus Basin: Sub-national Dimensions by Dr. Daanish Mustafa
18 Socio-economic Profile and Prospects for Diffusion of Renewable Energy in Cholistani Villages by
Dr. Asif Qayyum Qureshi
17 Energy Pricing Policy in Pakistan: Existing Prices and a Proposed Framework by Syed Waqar Haider
16 Governance of Fragile Ecosystems: Conserving Wild Natural Resources in Pakistan.
(Governance Series) by Dr. Amin U. Khan
15 Coping with the agreement on Textile and Clothing: A case of the Textile Sector of Pakistan by
Dr. Aqdas Kazmi
14 Globalization of Ecological Risk: Environmental News Agencies @ Internet (Governance Series) by
Zafarullah Khan
13 Who Makes Economic Policies? The Players Behind the Scene. (Governance Series) by Dr. A. R.
Kemal
12 Getting Out of the Debt Trap: Simulating Debt Retirement Strategies for Pakistan. (Governance
Series) by Dr. Eatzaz Ahmed
11 The Four Cs of NGO-Government Relations: Complementarity, Confrontation, Cooperation and
Co-optation by Adil Najam
10 The Management of Foreign Aid and External Aid: The Tricks of Getting More Aid.
(Governance Series) by Dr. Pervez Tahir
09 Governance of Foreign Aid and the Impact on Poverty in Pakistan: A Critical Review.
(Governance Series) by Dr. Abid A. Burki
08 Climate Change: Global Solutions and Opportunities for Pakistan by Malik Amin Aslam
07 Urban Corridors: The Ecology of Roadside Vegetation in Pakistan by Dr. Khalid Farooq Akbar
06 Environment and Development in Pakistan: From Planning Investment to Implementing Policies by
Dr. Pervez Tahir
05 Leadership and Institutions in Water Resource Management by Abdul Qadir Rafiq
04 Who Governs Water? The Politics of Water Resource Management by Hans Frey.
03 Policy Advocacy: A Framework for NGOs by Ali Qadir
02 Nala Lai: Ecology and Pollution in Human Settlements by LEAD Pakistan Cohort 6
01 Child Labor in Pakistan: Globalization, Interdependence and International Trade Regimes by
Save the Children (UK) and LEAD Pakistan

ORDER FORM
Manager CommunicationsLEAD PakistanLEAD HouseF 7 Markaz, Islamabad-44000Tel: 92-51-2651511Fax: 92-51-2651512
I would like to purchase the as mentioned on the back of this Order
Form. Please find a bank draft of _______________________________________
in favour of LEAD-Pakistan drawn on the Islamabad branch of:
________________________________________________________________________
Please despatch the requested number of copies of the Occasional Papers as mentioned on
the back of this Order Form on the following address:
___________________________________________________________________
_______________________________________________________________
______________________________________________________________
__________________________________________________________________
________________________________________________________________________
________________________________ _________________________________
_____________________________
Occasional Paper (s)
Rs/US$
Name:
Designation:
Organization:
Address:
Tel: Fax:
E-mail:
The prices of all Occasional Papers are as follows:
o each for individuals o each for institutions
o each
Local: Rs 250 Rs 500
International: US$ 20
For Credit Card Users only
American Express Master Card Visa Card Other
Card # Name:
Address:
Date of expiry: Country:_
Tel: Email:
Signature:
Please charge my credit card
o o o o
______________________________ ______________________________________
________________________________________________________________________
________________________ ___________________________________
_________________________________ ______________________________________
______________________