Towards a confidential system of researching for the common good
31
Towards a confidential system of researching for the common good Professor Joe Barry Dept. of Public Health & Primary Care, TCD Health Intelligence, Population Health, HSE Promoting Health Research & Protecting Patient Rights Portarlington, November 29, 2006
description
Towards a confidential system of researching for the common good. Professor Joe Barry Dept. of Public Health & Primary Care, TCD Health Intelligence, Population Health, HSE Promoting Health Research & Protecting Patient Rights Portarlington, November 29, 2006. Outline of Presentation. - PowerPoint PPT Presentation
Transcript of Towards a confidential system of researching for the common good

Towards a confidential system of researching
for the common good
Professor Joe BarryDept. of Public Health & Primary Care, TCDHealth Intelligence, Population Health, HSE
Promoting Health Research & Protecting Patient Rights Portarlington, November 29, 2006

Outline of Presentation
• Define Epidemiology and Public Health
• Examples
• Our ethical and legal framework
• Challenges
• A way forward

Epidemiology & Public Health
Epidemiology Public Health Practice
The measurement of the distribution and determinants of disease in time, place and person.
The science and art of prolonging life, promoting
health and preventing death through organised
efforts of society.

Do poor people die at an earlier age than rich people?

Irish Data on Health Inequalities
Source: “Inequalities in Mortality 1989-1998”, IPHI 2001

Has alcohol caused more, or fewer deaths in Ireland
recently?


Do we have a big underage drinking problem?

Percentages of boys and girls who have been ‘really drunk’
0
10
20
30
40
50
60
70
Boys 12-14 Boys 15-17 Girls 12-14 Girls 15-17
SC 1-2
SC 3-4
SC 5-6

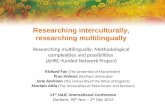
Is our suicide rate really increasing?

Irish Male Suicide Rates, 1980 -2001
0
5
10
15
20
25
30
35
1980 1982 1984 1986 1988 1990 1992 1994 1996 1998 2000
Rat
e p
er 1
00,0
00
15-24yrs 25-44yrs45-64yrs Over 65yrs
National Suicide Research Foundation
3-year moving averages

Ethical and Legal Framework
• Medical Council
• Data Protection Acts
• Research Ethics Committees
• Various guidelines
• Our job descriptions

Medical Council
• Confidentiality - 4 exceptions
• Data protection compliant• Consent if patients
involved• Anonymity• Research Ethics
Committees

Data Protection Acts
• Fair access and processing• Special, explicit and lawful
purpose(s)• Use and disclosure
appropriate• Safe and secure• Accurate and up-to-date• Relevant and not excessive• Retain only as long as
necessary• Available to individual

Q. Can I as a doctor, consultant or hospital doctor use patient data for research or statistical purposes?
A. Ideally you should make patients aware in advance if you intend to use their data for your own research purposes. However, the Act provides that such uses of personal data are permitted, even where the patient was not informed in advance, provided that no damage or distress is likely to be caused to the individual.
Source: Data Protection Commissioner, UCC Summer School, September 2004

Paragraphs 3 and 4 provide for other exceptions:
“(….) where processing of the data is required for the purposes of preventative medicine, medical diagnosis, the provision of care or treatment, or the management of healthcare services, and where those data are processed by a health professional subject under national law or rules established by national competent bodies to the obligation of professional secrecy or by another person also subject to an equivalent obligation of secrecy.”
Source: European Guidance for Healthcare Professionals on Confidentiality and Privacy in Healthcare, EuroSOCAP, 2006. www.eurosocap.org
Legal boundaries to privacy and confidentiality

“Information from hospital records is to be analysed anonymously (unlinked) to identify risk factors predicting poor outcomes from surgery. As the hospital staff cannot be redeployed to extract and anonymise the information, a trained nurse or clerical officer from the research team is assigned to copy and anonymise the information.
Here too, although the justification for the study would still need to be considered by an Ethics Committee, the infringement of confidentiality is minimal and there are unlikely to be significant ethical or legal objections to this aspect of the study.”
Source: Medical Research Council Ethics Series, Personal Information in Medical Research, 2003

National patient/client identifier and data protection
“A number of factors have been identified as hindering research in the health services. One of these is the absence of a national patient/client identifier that would allow much better assessment of health outcomes and the quality of care patients and clients receive in the health services. This issue is being addressed in the context of the proposal of the Minister for Social, Community and Family Affairs that every citizen is assigned an RSI number from birth. The Minister proposes that the same system be used in relation to the health services, with due regard to the need to protect the confidentiality of the professional/client relationship.”

Will the closure of small A/E units put lives at risk?


The percentage of cases of RTA within 60 minutes of a public acute hospital
HB Episodes % Cases within 60 minutes of a hospital
Current Intermediate Extreme
ECAHB 933 95.8 98.3 95.4MHB 681 85.0 82.7 71.7MWHB 927 87.2 91.0 83.5NAHB 1496 100.0 100.0 100.0NEHB 881 99.5 97.8 79.6NWHB 987 85.3 44.5 43.7SEHB 2336 67.3 78.2 66.2SHB 2247 88.0 88.7 67.2SWAHB 1427 98.7 98.6 99.2WHB 2872 57.1 78.4 47.5Ireland 14787 81.8 85.2 71.8

The percentage of cases of AMI within 60 minutes of a public acute hospital
HB Episodes % Cases within 60 minutes of a hospital
Current Intermediate Extreme
ECAHB 380 93.9 96.1 92.1MHB 253 81.8 74.3 67.6MWHB 264 90.2 85.6 78.4NAHB 366 100.0 100.0 100.0NEHB 495 99.8 97.2 74.5NWHB 339 86.7 47.5 42.2SEHB 598 65.6 75.3 60.7SHB 674 86.4 86.9 66.5SWAHB 369 99.2 97.6 98.6WHB 505 66.3 65.1 37.2Ireland 4243 85.6 82.8 70.0

How many heroin takers are there in Dublin?

Prevalence estimates and corresponding rates per thousand population by age and sex, Dublin 1996 and 2001
Dublin 1996 Dublin 2001
Estimate Rate/
1000 pop.
Estimate Rate/
1000 pop.
M 15-24 5405 56 2735 24.3
M 25-34 3512 42 3740 36.3
M 35-54 1427 11 1793 13.0
F 15-24 1778 18 1766 18.7
F 25-34 1039 11 1784 16.2
F 35-54 300 2 626 4.2
Total 13461 21 12444 18.2
Source: Prevalence of Opiate use in Ireland 2000-2001. A 3-source Capture Recapture Study. NACD


Actions - Quality and Fairness …
Action 111 - An independent Health Information and Quality Authority will be established
Action 115 - The National Health Information Strategy will be published and implemented
Action 116 - There will be a sustained programme of investment in the development of national health information systems as set out in the National Health Information Strategy

Actions - Quality and Fairness …
Action 117 - Information and communications technology will be fully exploited in service delivery
Action 118 - Information-sharing systems and the use of electronic patient records will be introduced on a phased basis
Action 121 - Health information legislation will be introduced

Actions - Health Information …
Action 13 - Health information will be geo-coded by small area
Action 17 - A legislative framework to support the National Health Information Strategy will be developed
Action 18 - A framework for information governance will be developed
Action 19 - A national health information standards framework will be developed

Actions - Health Information …
Action 24 - A system to evaluate and monitor the implementation of the National Health Information Strategy will be established
Action 27 - The Health Information and Quality Authority will review and update the National Health Information Strategy every year and submit it to the Minister of Health and Children for approval

Challenges
• Costs
• Culture
• Consent - routine datasets
• Getting the balance right
• Individual v common good
• Differing values
• Who decides?

A Way Forward
• Extension of today
• Revisit DoHC documents
• Health Information Bill
• Training
• Governance Structures