
Touch Receptors and Axons Lecture 13 PSY391S John Yeomans.
44
Touch Receptors and Axons Lecture 13 PSY391S John Yeomans
-
Upload
lora-pearson -
Category
Documents
-
view
215 -
download
0
Transcript of Touch Receptors and Axons Lecture 13 PSY391S John Yeomans.

Touch Receptors and Axons
Lecture 13
PSY391S
John Yeomans

Receptors in Skin
Hairy and glabrous skin are different.

Sensitivity and Acuity
• SS receptors much less sensitive than acoustic or visual receptors.
• More receptors in glabrous skin of fingertips, lips and genitals.
• Fewer receptors in back, proximal limbs.
• Better 2-point discrimination when more receptors, esp. with small receptive fields.
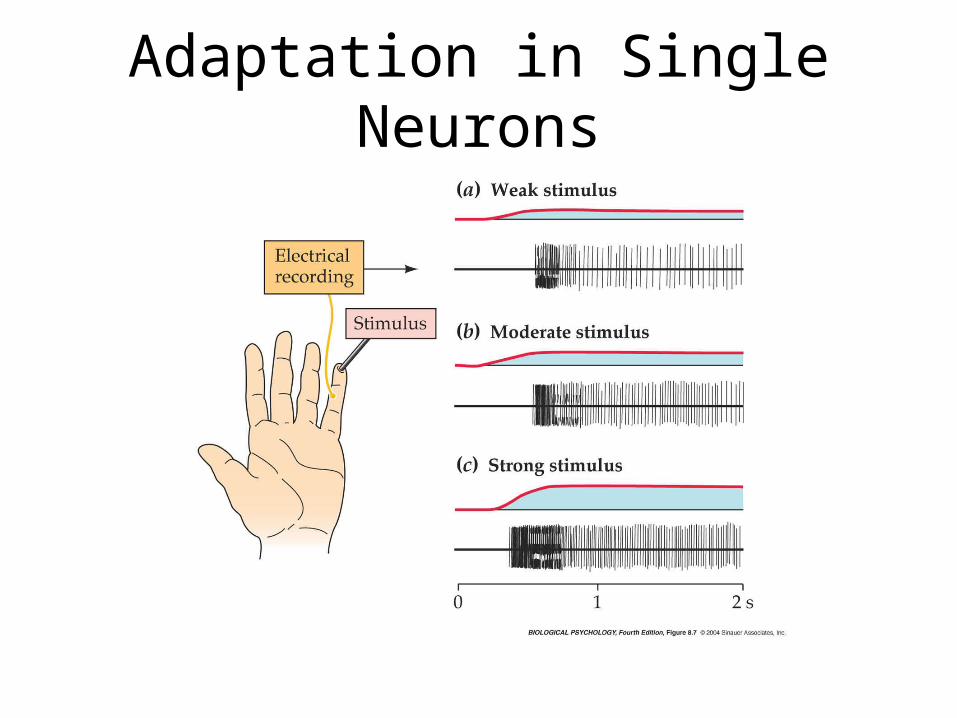
Adaptation in Single Neurons


Pacinian Corpuscles
• Easiest receptor to study due to size and isolation.
• Sensitivity high despite deep location when vibratory stimuli used.
• Fire at onset and removal of 1 s stimulus--Fast adapting.
• Adaptation due to capsule absorbing energy--No adaptation when naked axons are directly stimulated.

Receptive Field
Receptive field is part of the environment to which a neuron responds.

Single Neurons in Human Hand
• Microelectrodes in nerves isolate single neuron action potentials from large axons.
• 4 types of neurons, consistent with 4 receptor types in other animals.
• After studying receptive fields and adaptation, then microstimulate single axons to evoke perceptions!
• Perceptive fields match receptive fields. Valbo and Johansson

Receptive Fields and Adaptation
Glabrous skin of palm and fingertips.Recordings of single axons from median or ulnar nerves.
Valbo and Johansson

4 Different Feelings from Stimulation of Single Axons
• Pacinian: No feeling unless >10 action potentials, then “deep vibration”.
• Meissner’s: 1 AP leads to “tap”. >10 leads to odd “buzzing” or “fluttering” feeling.
• Merkel’s: 4 APs cause “light touch” like leaf. 10 APs cause stronger touch.
• Ruffini: No feeling until at least 2 axons, then “tugging” sensation.
• Labelled lines for touch sensations.

Axon Types
to 100A alpha

Somatosensory Pathways and Cortex
Lecture 14
PSY391S
John Yeomans

Dorsal Column Pathway
Trigeminal Nucleus V
A, Aβ fibers

Dermatomes
Double innervation of each skin area.
Trigeminal V

Spinothalamic Pathway
Trigeminal V
Parietal postcentral gyrus

Skin Temperature Sensation
Cool-Menthol R1Vanilloid R1
Vanilloid-like AδCMR1, VR1 C fibers

Somatosensory Cortex

Cortex Plasticity in Human

Cortical Layers and Columns
Mountcastle

Column Plasticity in Monkey
Cut ulnar nerveLose cortical areas

Lesions of SS Cortex
• Loss of 2-point discrimination.
• Loss of skin temperature discrimination.
• Loss of finest sensitivity and motor control.

Association Areas ofPosterior Parietal Cortex
• 3D Object Recognition
• Body Form (Amorphosynthesis)
• Hand-Eye Coordination
• Movement and Spatial Perception

Pain and Analgesia
Lecture 15
PSY391S
John Yeomans

Pain
• Acute pain signals tissue damage.• Chronic Pain Syndromes:• Causalgia • Neuralgia• Phantom Limb Pain• Usually involve peripheral nerve damage
(neuropathy), but are sustained by CNS.• Hard to treat.

Peripheral Pain Mechanisms

Skin Temperature Sensation
Cool-Menthol R1Vanilloid R1
Vanilloid-like Aδ

Analgesia Pathways


Opiates
• Opium, heroin and morphine.
• Enkephalins
• Endorphins
• Dynorphins
• Receptors: mu, delta, kappa.
• Analgesia, reward, drug abuse.


Muscles and Reflexes
Lecture 16
PSY391S
John Yeomans

Muscle Types
• Smooth muscles in viscera.
• Striated muscles to skeleton and connective tissue.
• Cardiac muscle--visceral striated muscle with rhythmic contractions.
• Fast-twitch and slow-twitch striated muscles.

Muscles

Sliding Filaments

Muscle Fibers and Inputs
• Extrafusal fibers with alpha motor neurons.
• Intrafusal fibers with gamma motor neurons.
• Neuromuscular junction.
• Ach release by Ca++.
• Nicotinic receptorsEPPsAPs
• APsCa++Actin and myosin sliding together.

Neuromuscular Junction

Muscle Receptors

Kinesthetic Receptors
• Movements sensed by receptors in muscles, joints and tendons.
• Joint receptors respond to angle of joint.
• Pacinian corpuscles respond to vibration.
• Spindles respond to muscle stretch.
• Golgi tendon organs respond to stronger stretch.

Spindle Stretch Receptors

Spindle and Tendon Activation

Proprioceptive Pathways
• Spinal reflexes--Monosynaptic stretch. Disynaptic GTO inhibition (clasp-knife).
• Dorsal columns to thalamus and motor cortex.
• Spinocerebellar path.

Motor Units and Rotation
• Motor unit = 1 axon and all the fibres innervated.
• Reciprocal inhibition of competing motor units in ventral horn (flexors vs. extensors).
• Size principle--small motor units first.
• Rotation of motor units, by recurrent inhibition in ventral horn.

Reflexes
• Monosynaptic stretch reflex.
• Disynaptic tendon reflex (clasp-knife).
• Flexion reflex.
• Scratching and walking.

Stretch Reflex


















