TOTAL PATIENT REVENUE: Experiment, or Our Future? March 25, 2013.
68
TOTAL PATIENT REVENUE: Experiment, or Our Future? March 25, 2013
-
Upload
nigel-norton -
Category
Documents
-
view
213 -
download
1
Transcript of TOTAL PATIENT REVENUE: Experiment, or Our Future? March 25, 2013.

TOTAL PATIENT REVENUE:
Experiment, or Our Future?
March 25, 2013

HISTORY & BACKGROUND OF TPR
MHA Statewide Education Program on TPRMarch 25, 2013

TPR Overview• “TPR” = Fixed Total Gross Regulated Patient Revenue
– TPR revenue is 100% fixed regardless of:• Inpatient / Outpatient mix• Increases or decreases in volumes• Changes in case mix
– Since the hospital’s revenue base is fixed, TPR encourages cost effective delivery of care
• Annual Adjustments to TPR Revenue Base– HSCRC-approved Update Factor– Over / Under Charges For Total Cap [One-Time]– Changes in service area population (lesser of: 25% of population growth, or
1%)– Changes in allowable uncompensated care and payor mix
• Minimum agreement for a three-year period
3MHA Statewide Education Program on TPRMarch 25, 2013

TPR Overview• The 10 TPR Hospitals Entered Into A Total Patient Revenue Agreement on
July 1, 2010– The goal of the TPR Agreement was to incentivize hospitals to provide
high quality and reduce utilization– The majority of the TPR hospitals revenue capital was established on
the FY 2010 revenue base• Transition funding based on historical volume and case mix growth• Some hospitals received additional adjustments in July 2011 to
increase the TPR budget related to the opening of new services already planned
4MHA Statewide Education Program on TPRMarch 25, 2013

Comparison with Charge-Per-Case [CPC]
Encourages: Care for the ill and maximizing volumes
Encourages: Wellness and cost effective delivery of care
Adjusts revenue at 85% for increases and decreases in cases and outpatient services
No adjustments for volume changes: 100% fixed--------------------------------------------Limited adjustments for population growth
Adjusts revenue for increases in case-mix (sometimes limited) and decreases at 100%
No adjustment for changes in case-mix
Positive and negative adjustments to revenue (“scaling”) related to Reasonableness of Charges (ROC) ranking
Only positive ROC-related scaling
5
Current CPC System TPR
MHA Statewide Education Program on TPRMarch 25, 2013

Methodology & StructuralConsiderations
METHODOLOGY• Incentive to transition to TPR
– Average volume growth for previous 3 years– Average case mix growth for previous 3 years
• Exemption from negative scaling• Exemption from state-wide readmission policy• Outlier cases are inclusive in TPRSTRATEGIC• Expected volume growth or decline• Program changes and CMI impact• De-regulation of services and/or addition of new services• One-day stays converting to observation• ROC projections• Market Share implications
6MHA Statewide Education Program on TPRMarch 25, 2013

Monitoring ComplianceFINANCIAL• Over / Under recovery of allowed TPR cap is measured at the end of each
fiscal year– Savings – Under; Dissavings – Over– Price Variances are added to/reduce the subsequent year’s revenue base on a
one-time basis• Under the TPR methodology hospitals have the flexibility to charge +/-5%
beyond the approved rates without penalty– Staff may approve extending compliance corridors to +/-10% if it is
demonstrated that this is necessary to do so for a hospital to meet its budget.– The hospital may also request further changes if necessary
• Unit Rate Price Variances are not applied, and are only used to compute potential penalties
7MHA Statewide Education Program on TPRMarch 25, 2013

Monitoring Compliance [cont’d]
STRATEGIC/QUALITY• Maintain market share• Disclosure of financial interest [ownership] in non-
hospital services within primary and secondary service area
• Disclosure of future acquisitions or divestures of non-hospital health services
• Maintain relative performance ranking on HSCRC quality based reimbursement and Maryland hospital acquired conditions ranking
8MHA Statewide Education Program on TPRMarch 25, 2013

9
Calvert Health System 5-Year Capital Plan

FORMATION OF THE MARYLAND TPR COLLABORATIVE
• April 2011 – Executive members of the 10 hospitals began to meet to discuss operating under a total patient revenue system
• Goals:– Sharing of Experiences– Learn Best Practices – Education– Data Analytics – Performance Metrics– Single Voice in Negotiating with HSCRC– Use of Consultants In Formation of Policies, Methodologies and Trending
of Financial, Utilization and Quality Data– Advocacy– CMO and Case Management Connectivity and Education
• August 2012 – Formed LLC• October 2012 – Began Negotiating with HSCRC - The Next 3-Year Agreement
10MHA Statewide Education Program on TPRMarch 25, 2013

Creation of the Collaborative and Strategy for Engagement
11MHA Statewide Education Program on TPRMarch 25, 2013

Defining and Achieving Success
Information/Data Gathering Analytics
Collaborative Priorities
1. Definition of Success—HSCRC,
Internal
2. TPR Phase 2 (the Second Three Years)
Critical AssessmentsPhysician Alignment, Care Management, Costs & Utilization,
and Quality *
SupportingAnalysis
- TPR frameworks
- Roadmaps- Assessments-Performance indicators-Supporting analytics
*Status of population health planning and IT resources will be collected as baseline measurements



Measures of Success: Recall frameworkH
SCRC
: TP
R Co
ntra
ct T
erm
s • Live within revenue constraint
• No cost shifting
• No quality erosion
Exte
rnal
Vie
w • Bend the trend
• Improve quality and delivery of care
• Support phys alignment & delivery reform
• The Waiver
Inte
rnal
Vie
w • Sustainable delivery system
• Improve quality and patient experience
• Lower use• Manage cost• Begin
transformation

16MHA Statewide Education Program on TPRMarch 25, 2013

17MHA Statewide Education Program on TPRMarch 25, 2013

18MHA Statewide Education Program on TPRMarch 25, 2013

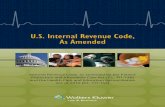
Ambulatory Sensitive Conditions: Admissions & Total Charges
DIABETES UNCONTROLLED
LOWER EXTREMITY AMPUTATION
ASTHMA IN YOUNGER ADULTS
ANGINA
HYPERTENSION
DIABETES SHORT TERM COMPLICATION
DIABETES LONG TERM COMPLICATION
DEHYDRATION
URINARY INFECTION
COPD OR ASTHMA IN OLDER ADULTS
BACTERIAL PNEUMONIA
CONGESTIVE HEART FAILURE
0 500 1000 1500 2000 2500 3000
Admissions and Total Charges for Ambulatory Sensitive Conditions : ALL TPR Hospitals
$9.6M
$20.1M
$7.6M
$3.4M
$2.3M
$8.2M
$916k
$27M
$25.1M
$885k
$885k
$400k

CHF Ambulatory Sensitive Conditions by Hospital
McCready Memorial Hospital
Garrett County Memorial Hospital
Chester River Hospital Center
Dorchester General Hospital
Union Hospital of Cecil County
Calvert Memorial Hospital
Memorial Hospital at Easton
Meritus Medical Center
Carroll Hospital Center
Western Maryland Medical Center
0 100 200 300 400 500 600
Congestive Heart Failure: Admissions and Total Charges
$4.7M
$3.7M
$5.2M
$2.1M
$2.3M
$3.7M
$1.3M
$2.0M
$758k
$406k

One Day Stays: OpportunitiesCa
lver
t
Carr
oll
Ches
ter R
iver
Dor
ches
ter
GCM
H
McC
read
y
East
on
Mer
itus
Uni
on o
f Cec
il
WM
HS
0
500
1,000
1,500
2,000
2,500
3,000
3,500
4,000
4,500
1,731
3,811
469645 765
106
2,035
3,179
1,675
2,550

Days Above the Geometric Mean
Cardiology -
M (2
3899 Days)
Cardiova
scular S
urgica
l - S (
6419 Days)
GI - M
(17862 D
ays)
GI - S (
9488 Days)
Infectious D
isease
- M (1
5372 Days)
Neurology -
M (1
3201 Days)
OB/Neonatal/N
ewborn (3
4129 Days)
Orthopedic/
Muscu
loskeletal -
S (16509.55358615 D
ays)
Psychiatri
c Subtotal -
P (24508 D
ays)
Pulmonology -
M (4
0381 Days)
Pulmonology -
S (3460 D
ays)
Rehabilitation (1
2916 Days)
Urology -
M (1
4784 Days)
0
2,000
4,000
6,000
8,000
10,000
12,000
7,955.7
2,074.1
5,215.3
2,150.9
4,360.7 3,938.6
1,685.12,666.9
5,215.9
10,307.1
431.0
3,223.54,071.0
Day
s A
bove
Geo
met
ric
Mea
n
Potential Cost Savings:
10% Reduction: $3.4 M20% Reduction: $6.7 M

ALL Readmissions, by Payor
63%
5%
3%
6%
1%0%
3%0%
4%9% 2% 1% 2%
01 MEDICARE02 MEDICAID04 BLUE CROSS05 INSURANCE COMPANY06 OTHER GOVERNMENT PAYMENT07 WORKMENS COMP08 SELF PAY09 NO CHARGE12 HMO14 MEDICAID - HMO15 MEDICARE - HMO16 BLUE CROSS - NATIONAL CAPITAL AREA17 BLUE CROSS - OTHER STATE
Medicare & Medicaid = 68%

Initial Discharge Disposition of Readmissions within 1 to 7 Days
61%
13%
10% 2% 2% 2% 1%
To home or self-careTo home under the care of a home health agencyTo a nursing facilityTo another acute care hospitalTo nursing homeTo distinct on-site rehabilitation unit from acute careLeft against medical adviceTo a rehabilitation hospital or rehab. unit of another hospital

Readmission Rates by Initial Product Line, by Hospital
CALVER
T MEM
ORIAL HOSP
ITAL
CARROLL HOSP
ITAL C
ENTE
R
CHESTE
R RIVER HOSP
ITAL C
ENTE
R
DORCHESTE
R GENER
AL HOSP
ITAL O
F CAMBRIDGE
EDW
ARD MCCREA
DY MEM
ORIAL HOSP
ITAL
GARRETT C
OUNTY M
EMORIAL H
OSPITA
L
MEMORIAL H
OSPITA
L AT E
ASTON
UNION HOSP
ITAL O
F CEC
IL COUNTY
WASH
INGTO
N COUNTY HOSP
ITAL
WES
TERN M
D HEALTH
SYST
EM BRADDOCK HOSP
IT
12% 16% 18% 17% 11%15% 16% 18% 14% 18%
12% 15%20%
11% 15% 11% 16% 14% 14% 19%
10% 12%8%
13%6%
10% 13% 16% 12% 16%
GI
Cardiology
Pulmonology
Compares readmission rates across hospitals, only for the the top three product lines of Pulmonology, Cardiology and GI (41% of all readmissions by initial product line)

Care Management and Community Collaboration
26MHA Statewide Education Program on TPRMarch 25, 2013

Care Coordination
• Care Management re-design• ED RN Care Management• Discharge Advocacy Center• Home Health Care pilot• Skilled Nursing Facility Transitionalist• Project Red• Pharmacists in ED doing Medication Reconciliation• Hospice/palliative care expansion • Behavioral Health focus• Diabetic services in the community• PCMH• Credo briefs• Commission on Aging Transitional Care Nurse
27MHA Statewide Education Program on TPRMarch 25, 2013

Safety and Quality
• Medication delivery at bedside• Patient Safety Rounds• New incident reporting system• Installation of infection control surveillance
software• Quality Forum• Patient family centered care• Hospitalist re-design through LEAN
28MHA Statewide Education Program on TPRMarch 25, 2013

IT Infrastructure and Tools
• Implementation of risk adjusted, comparative quality software
• CRISP• Community partners given access to hospital
EMR
29MHA Statewide Education Program on TPRMarch 25, 2013

Protocols/Evidence-Based/Self Care
• Coleman Model• STARR initiative• Care coordination and discharge protocols• Community Health Education• IHI triple aim collaborative• Employee health risk assessment• Health system nutritional initiatives
30MHA Statewide Education Program on TPRMarch 25, 2013

Provider Supply
• Shore Health paying for blocks of specialist time
• Contracting with SNF’s for uninsured patients• Health system employed physicians doing
discharge f/u’s within 3-5 days • Collaboration with FQHCs• Urgent care follow up for uninsured patients• Transitional Care Program
31MHA Statewide Education Program on TPRMarch 25, 2013

Cost Reductions
• Reduction of implant costs• Avoided admissions• LEAN
32MHA Statewide Education Program on TPRMarch 25, 2013

Emergency Department Care Management

ED Care Management and Admission Avoidance

Discharge Lab Follow UpDischarge Advocacy CenterUnresulted Tests at Discharge Follow-Up FY 13
February January December November
Test: # of Patients # of Tests # of Patients # of Tests # of Patients # of Tests # of Patients # of Tests
Positive Blood Culture not on Antibiotics 1 1 1 1 1 1 0 0
Positive Blood Culture not on appropriate Antibiotics 0 0 0 0 1 1 1 1
Other 128 169 37 40 23 25 46 48
Pathology 45 45 5 5 13 13 20 21
Radiology 110 130 3 4 14 18 30 36
Positive Respiratory Culture not on Antibiotics 0 0 0 0 0 0 1 1
Positive Respiratory Culture not on appropriate Antibiotics 0 0 1 1 0 0 0 0
Positive Urine Culture not on Antibiotics 9 9 7 7 4 4 8 8
Positive Urine Culture not on appropriate Antibiotics 2 2 4 4 2 2 0 0
Positive Wound Culture not on Antibiotics 4 4 5 6 1 1 2 3
Positive Wound Culture not on appropriate Antibiotics 1 1 1 1 0 0 0 0
No Status (Screened and no intervention required) 190 394 344 766 442 945 345 705
Total Interventions 300 361 62 69 52 57 108 118

Discharge Phone Calls
Patient Total
Count Count Percent Percent
761 570 72.89% 0.51% 969
Discharge/Encounter Date
119 93 75.61% 0.81% 153
52 35 64.81% 0.00% 73
93 73 75.26% 1.03% 119
60 51 80.95% 0.00% 77
219 158 70.54% 0.45% 274
14 10 71.43% 0.00% 15
70 55 77.46% 0.00% 91
97 70 70.71% 0.00% 118
37 25 67.57% 2.70% 49
Patient CountsPatients
Completed
February Patients Attempted
Patient Contacts
Percent Count
4 187
Patients Removed
Net Patient Total
Patients Do Not Call
782
UnitTotal 97.31%
2East 96.75% 1 30 123
2Eastp 96.30% 0 19 54
3East 95.88% 1 22 97
4East 95.24% 0 14 63
4South 97.77% 1 50 224
4West 100.00% 0 1 14
5East 98.59% 0 20 71
5South 97.98% 0 19 99
5West 100.00% 1 12 37

Discharge Appointments Made
Discharge Appointments by Clerical Assistants FY13 Appointments Made
July 125
August 109
September 74
October 106
November 91
December 76
January 121
February 118
March
April
May
June
Total 820

Medicare Cost per Case for CHF, COPD, and Diabetes**
2011 Q1 2011 Q2 2011 Q3 2011 Q4 2012 Q1 2012 Q2 2012 Q30
1,000
2,000
3,000
4,000
5,000
6,000
7,000
8,000
9,000
170 154 127 123 120 98 104
Total CasesCHF, COPD, Diabetes Arithmetic ObservedCHF, COPD, Diabetes Arithmetic Expected
Cost
** Premier Quality Advisor

Medicare Diabetes Readmission Rate**
2011 Q1 2011 Q2 2011 Q3 2011 Q4 2012 Q1 2012 Q2 2012 Q30.00%
5.00%
10.00%
15.00%
20.00%
25.00%
Total Medicare Readmission Rate
Medicare Expected Readmission Rate
Medicare Diabetes Readmission Rate
Medicare Diabetes Expected Readmission Rate
** Premier Quality Advisor

Medicare COPD Readmission Rate**
**Premier Quality Advisor

CREDO (Emergency Room Care Plan) Case Study
Prior ED utilization:
• March 2011 – February 2012
• # of ED visits – 46
• Total ED Charges– $40,186.78
CREDO implemented March 2012• March 2012 to February
2013• # of ED visits
– 29
• Total ED Charges– $22,796.98

Hospital Readmission Rate

Measures of Success
43MHA Statewide Education Program on TPRMarch 25, 2013

Inpatient Volume Information

Inpatient Case Mix Information

Inpatient Volume Information- Medicare Only

Outpatient Volume- Significant Service Groups

GPSR Adjusted for Transitional Revenue

Outpatient Revenue- Significant Service Groups
Adjusted for Transitional Payments

Revenue Information- MedicareAdjusted for Transitional Payments

Measures of Success
51MHA Statewide Education Program on TPRMarch 25, 2013

Key Findings - Revenue
Gross Patient Service Revenue• Total Population changes have been consistent for TPR
and Non TPR hospitals’ service areas ( 2% vs. 2%)
• Overall TPR Gross Patient Service Revenue (GPSR) has increased less than Non TPR Hospitals GPSR (9.4% vs. 10.2%)
• TPR hospitals’ GPSR per case has increased more than Non TPR Hospitals GPSR per case (17.3% vs. 11.5%)
52MHA Statewide Education Program on TPRMarch 25, 2013

Key FindingsVolume
– 2010-2012 TPR Hospitals’ Total Admissions and Patient Days have decreased significantly more than Non-TPR Hospital’s Admissions and Patient Days (13.2% and 8.3% vs. 6.0% and 2.0%, respectively
– TPR Hospitals’ Medicare Admissions and Patient Days have decreased significantly more than Non TPR Hospitals’ Admissions and Patient Days (10.4% and 7.9% vs. 4.2% and 0.3%, respectively)
– TPR Hospitals’ Outpatient Cases have increased compared to Non TPR Hospitals’ Outpatient Cases (ED: 9/1% vs. 8.5%, SDS, 2.2% vs 0.1%)
Case Mix– TPR Hospitals’ case mix has increased more than Non TPR Hospitals’ case
mix (2.2% vs. 1.6%)
53MHA Statewide Education Program on TPRMarch 25, 2013

Key Findings- QualityMaryland Hospital Acquired Conditions (MHACs)• FY 2011 Performance
– Statewide Scaling Revenue Neutral– TPR Hospitals’ Cumulative Scaling = $643,000– 7 out of 10 hospitals received positive scaling
• FY 2012 Performance (Q1-Q3 final)– Statewide Scaling Revenue Neutral– TPR Hospitals Cumulative Scaling = $2,385,000– 4 out of the top 9 hospitals are TPR hospitals
Quality Based Reimbursement (Clinical Process of Care and HCAHPS)• CY 2010 Performance
– Statewide Scaling Revenue Neutral– TPR Hospitals Cumulative Scaling = $176,000– 7 out of 10 hospitals received positive scaling
54MHA Statewide Education Program on TPRMarch 25, 2013

Same Hospital Readmissions as a % of Total Admissions
% Readmissions Annual Change
FY2010 FY2011 FY2012 FY2011 FY2012 Difference
ARR 9.83% 9.71% 9.40% -0.12% -0.31% -0.19%
TPR 10.50% 10.46% 9.79% -0.04% -0.67% -0.63%
Statewide 10.50% 9.69% 9.37% -0.81% -0.32% 0.49%
Source: HSCRC Nov 7, 2012 Public Meeting

TPR Contract Renewal and Future of the Collaborative
56MHA Statewide Education Program on TPRMarch 25, 2013

Horizon for TPR and the Collaborative • Components of the Next three year contact
– Population adjustment/ the Dynamics of Population growth in Maryland
– Shared savings– In-migration from out of area– Market share– Implications of modification to fixed/ variable factor– Implications of ARR, ODS and Update Factor – Medicaid Expansion and Insurance Exchange potential
for 3% increase in utilization (Hill Top)
57MHA Statewide Education Program on TPRMarch 25, 2013

Horizon for TPR and the Collaborative • Components of the Next three year contact
– Alignment of physician and hospital incentives/ pay for performance
– New services– Quality performance– Waiver modification– Measurement of Success/ Agreement on a target – Time Frame
58MHA Statewide Education Program on TPRMarch 25, 2013


FEE-FOR-SERVICE MOVING TO INTEGRATED CARE, NEW PAYMENT MODELS & RISK
Deliver continuous improvement in clinical cost and quality
Value-based purchasing:HACs, quality, efficiency, cuts
HAC & readmissions penalties
Shared savings
Global paymentBundled payment
Population Management• Population analytics• Care management• Financial modeling and
management• Legal• Physician integration
High Value Episodes• DRG and episode
targeting• Care models and
gainsharing• Data analytics• Cost management
High Performing Hospitals• Most efficient supply chain• Best outcomes in quality, safety• Waste elimination• Satisfied patients

TPR and ACA
• Administrative simplification
• Shared savings ACO’s• Innovation Center• (Preventable) readmissions• Reduce hospital-acquired
conditions• Reduce annual market
basket updates/adjust for productivity
Total Patient Revenue
• Simple program administer• Shared Savings Element to be
included• Innovative Care Concepts • Manage Chronic disease
populations• Improve Quality• Place Patient in the lease
costly venue to return the greatest value
• Targeted populations
61MHA Statewide Education Program on TPRMarch 25, 2013
Accountable Care Act Cost Saving

Garrett County Memorial HospitalKeys to Long Term Success
• 30+ Year History on TPR• Sole Community Provider; Rural Location• Fixed Population Base• Limited in/out migration • Single source for most Technical Facility Services• Non-compete philosophy for Professional Services• Primary Care Service Focus; Limited Specialty Care• Strong Community Collaboration
– Hospital, Physicians, Health Department, Home Health, Social Service Agencies, etc.
• Patient Centered Care Model
62MHA Statewide Education Program on TPRMarch 25, 2013

Garrett County Memorial HospitalKeys to Long Term Success
• Efficient use of hospital resources• Monitoring quality of care and standard clinical practice patterns of all physicians• Friendly, professional care delivery • Tight controls on variable expenses, i.e. pharmaceuticals and the formulary• Close communication/review of ER patients for appropriateness of admission • Patient centered care delivery model which includes family involvement and
coordination of care • Hospital management focus towards care which compliments rather than
competes with physicians, which maintains a separation of technical and professional component reimbursement
• Assisting in physician recruitment to the community• Assuring physician representation on hospital board, strategic planning, etc.
63MHA Statewide Education Program on TPRMarch 25, 2013

Care Coordination and the TPR Initiative
Reducing readmissions
Reducing unnecessary ED visits
More collaboration& standardization of care protocols and processesEmphasis on achieving higher targets&reduced cost per case
Increasing focus on Ambulatory Sensitive Conditions (ASCs)
Emphasis on formal disease management across the care continuum
Electronic Health Records, HIE, Telemedicine, Wireless = Connected stakeholders
Current Focus of TPR hospitals
Requires = Changed Payment Structures
#1
#2
#3
#4
#5Experience
of Care
Population Health
Per Capita Cost
“Triple Aim”
Next Phase for TPR hospitals

Six Dimensions•Physician
employment models and/or effective contract models; incentive systems operating in key areas
•Incentive systems aligned with overall performance goals and quality targets
•Primary care / specialty mix goal is defined, and complement has been achieved
•Physician leadership identifiable
Structure of hospital medical
staff
•Relevant data metrics to support cost/quality/care coordination are established and shared with physicians on a consistent basis
•Feedback from physicians indicates believability in the metrics and the measurement process; indication(s) that physicians are incorporating metrics into their practice patterns
Data
•Caregivers understand their respective roles & willing participants in the care coordination process
•Metrics in place to measure key variables associated with effective coordination
•Connectivity established to support communications across providers
Care Coordination

Six Dimensions (cont’d)
•Quality metrics have been established jointly between physicians and hospital staff
•Progress is shared with physicians and Board on a regular basis
•Feedback loop is established with physicians
•Better performing clinicians are used as mentors
•Consequential remediation program in place for habitual poor performers
Quality
•Best practices developed/adopted/disseminated/monitored
•Focused efforts to reduce variability
•Clinical service redesign and/or rightsizing underway
Cost Optimization
•High degree of mutual trust between hospital and physicians
•Model for shared savings/penalties in place and supported by physicians
•Physician leaders identified and cultivated by hospital for the next generation of physician leadership
Relationships: Hospital-
Physicians

Distinct Opportunities as a Collaborative
• Data Warehouse for quality and efficiency/Information Exchange – Chief Medical Information Officer for the collaborative
• Telehealth– Group purchase/licensing– Demonstration projects / private industry initiatives– Reimbursement models
• Professional fee billing operation: Group purchase/best practices• Midlevels: Models/best practices
– Setting-specific models (e.g. primary care office; ER; etc)• Contracts for employment/incentives• Incentive systems and relevant metrics (e.g. Emergency Room physicians,
Hospitalists)• Medicare ACO
67MHA Statewide Education Program on TPRMarch 25, 2013

Questions?