Topics in Palliative Care Medical Oncology Residents December 8, 2008 Jeff Myers MD, CCFP, MSEd...
76
Topics in Palliative Care Medical Oncology Residents December 8, 2008 Jeff Myers MD, CCFP, MSEd Program Head – Supportive Care, Palliative Care and Psychosocial Oncology Odette Cancer Centre Asst Professor, Faculty of Medicine, University of Toronto
-
Upload
griffin-simmons -
Category
Documents
-
view
215 -
download
0
Transcript of Topics in Palliative Care Medical Oncology Residents December 8, 2008 Jeff Myers MD, CCFP, MSEd...
Topics in Palliative CareMedical Oncology Residents
December 8, 2008Jeff Myers MD, CCFP, MSEdProgram Head – Supportive Care, Palliative Care and Psychosocial Oncology
Odette Cancer CentreAsst Professor, Faculty of Medicine, University of Toronto

HospiceHospicePalliative carePalliative care
Curative / remissive therapyCurative / remissive therapy
PresentationPresentation Death

Palliative Care Consult Team at Sunnybrook
Inpatient consult service Outpatient Palliative Care Clinic (OCC) Bone Mets Clinic CHF clinic Kidney Care Clinic ALS Clinic *PCU MDs – Wynnychuk, Chakraborty, Sirianni, Selby, Kim,
Tamber

Ed
63 yo male – HR prostate CA, several areas of bony mets (including L2, 3, 4 but not ischium, ilium, sacrum or right hip area)
C/o increasing right buttock pain, 8/10, deep, dull, achy in character, radiates down back of right leg, 10/10 (“more of a shooting feeling”)

Ed
Current analgesic regimen:– Fentanyl 50 mcg/hr patch – change q72h– Tyl #3 – 1-2 po q6h prn (uses on average
5/day when pain “severe”, unsure of benefit)
– Colace 100mg BID– wife reluctant to support increasing patch
as her nephew is a heroin addict

Objectives
Improve management of nociceptive pain
Address neuropathic pain
Address fears about opioids
Objectives
Improve management of nociceptive pain
Address neuropathic pain
Address fears about opioids
Fentanyl Patch
Oral BT form not available Onset of action, time to reach steady state
and absorption highly variable Does not allow for rapid titration In setting of malignant pain, fentanyl only
appropriate when:– pain is well controlled and unlikely to vary
considerably– oral route not available**

Ed – Opioid Options
Opioid Rotation – Correct for Cross Tolerance?- If yes, decrease by 30%- If no, leave dose the same
Calculation of Breakthrough Dose:– 10% of total 24 hour dose OR– 50% of q4h dose How frequent?
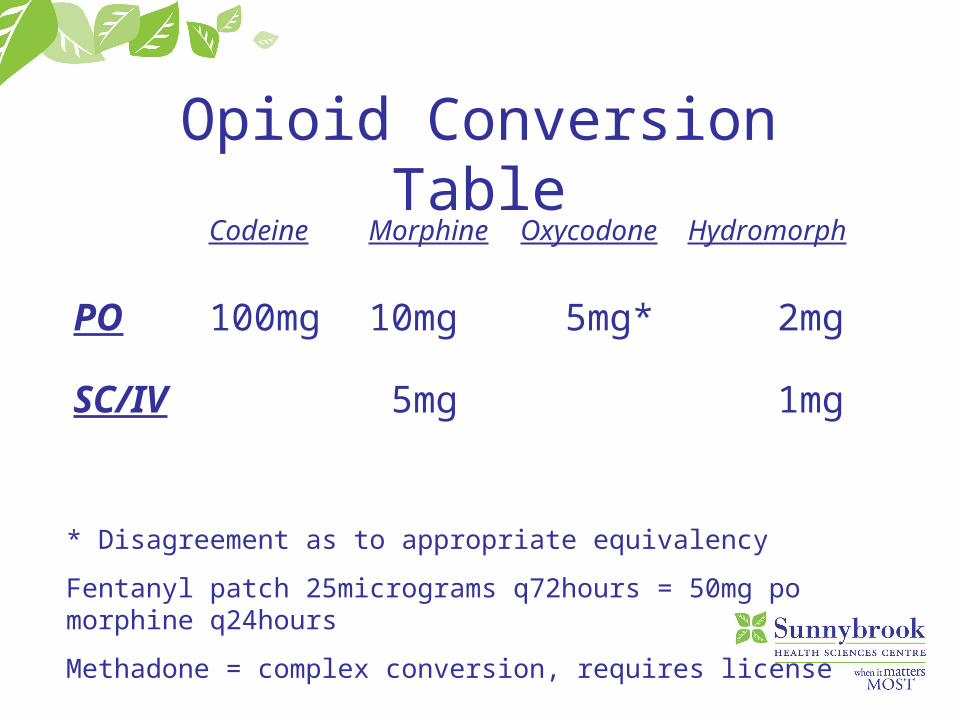
Opioid Conversion TableCodeine Morphine Oxycodone Hydromorph
PO 100mg 10mg 5mg* 2mg
SC/IV 5mg 1mg
* Disagreement as to appropriate equivalency
Fentanyl patch 25micrograms q72hours = 50mg po morphine q24hours
Methadone = complex conversion, requires license
1 Percocet (5mg PO oxycodone) =
10mg PO morphine = 2 mg PO hydromorphone

Cost Comparison
Ed
Fentanyl 50mcg/hr = Morphine 100mg q24h = Hydromorphone 20mg q24h

Ed
Fentanyl 50mcg/hr = Morphine 100mg q24h = Hydromorphone 20mg q24h
Hydromorph Contin 9mg BID

Ed
Fentanyl 50mcg/hr = Morphine 100mg q24h = Hydromorphone 20mg q24h
Hydromorph Contin 9mg BID
Hydromorphone 2mg q1h prn

What was wrong with original breakthrough?
Tylenol #3 – 1-2 po q6h prn 5/day

Opioid Conversion TableCodeine Morphine Oxycodone Hydromorph
PO 100mg 10mg 5mg* 2mg
SC/IV 5mg 1mg
* Disagreement as to appropriate equivalency
Fentanyl patch 25micrograms q72hours = 50mg po morphine q24hours
Methadone = complex conversion, requires license

What was wrong with original breakthrough?
Tylenol #3 – 1-2 po q6h prn 5/day
Tyl #3 = Codeine 30mg = Morphine 3mg =
Hydromorphone 0.6 mg (1/4 of reqd)
What was wrong with original plan for constipation?
Recent evidence suggesting no efficacy with stool softeners (docusate)
Must have laxative – maximize Senna and, if necessary, add Lactulose

Objectives
Improve management of nociceptive pain
Address neuropathic pain
Address fears about opioids
Neuropathic Pain Disordered function of the nervous system
anywhere from the periphery to the cerebral cortex; VERY common component of “malignant pain”, poorly managed
Pain may be described as sharp, burning, “pins and needles”, shooting
Treat with opioids, TCAs, anticonvulsants Specifically – gabapentin, nortriptyline,
desipramine

Ed
If neuropathic component of pain syndrome not fully relieved with opiate then add adjuvant
If ODB, begin with nortriptyline (25mg – 100mg) fewer anticholinergic SE than amitriptyline
Apply through Section 16 for gabapentin PCFA = only Palliative Care MDs

Ed
Titrate gabapentin dose: 300mg HS for two days, 300mg BID for two days, 300mg TID, continue to titrate dose (up to 3600mg/day well tolerated; renally cleared; correct for creat clearance)
Lyrica (pregabalin) – only indications are diabetic neuropathy and post-herpetic neuralgia (dosage up to 300mg/day in 2 or 3 divided doses)

Pregabalin “Lyrica” Developed specifically to maintain biologic
activity of gabapentin while improving pharmacokinetic properties
Approved in 2004 for:– Adjunct AED– Diabetic peripheral neuropathy, postherpetic neuralgia– GAD– Neuropathic pain
Pregabalin-pharmacodynamics
Lipophilic analogue of gabapentin Designed to improve diffusion across
BBB lipophylic antagonist at voltage gated
Ca channels (6× more potent than gabapentin)

Pregabalin - Dosing
Initiate 150 mg/day (divided BID or TID) Titrate to 300 mg/day (divided TID) over 1
week Maximum 600 mg/day Reduce if CrCl<60 mL/min Taper over 1 week to discontinue Abrupt discontinuation associated with
withdrawal (nausea, H/A, diarrhea)
Proposed Benefits of Pregabalin
Onset of action as early as 1 week Rapid dose titration Similar efficacy observed with BID and
TID dosing At dose > 75mg BID, more cost
effective than gaba No head to head efficacy data
Ed
Phone follow up in 3 days, deep buttock pain somewhat improved (using 8 BTs per day), radiating pain unchanged
Ed
Phone follow up in 3 days, deep buttock pain somewhat improved (using 8 BTs per day), radiating pain unchanged
Titrate Hydromorph Contin based on BT use and add neuropathic adjuvant
CIPN
Taxanes – 50-70% pts experience mild to moderate numbness, tingling, burning/stabbing in hands and feet
Vinca Alkaloids – 25%; high doses associated with absent Achilles reflex, weak distal muscles, foot drop
Platinum (Oxaliplatin) – Sx can occur after prolonged therapy and may develop 3-8 weeks after last dose

CIPN - Tx
Cancer, 2007: One placebo controlled RCT – gabapentin (max dose 2700mg) for six weeks – no benefit
JCO, 2004: Case series, gabapentin used as secondary prophylaxis with 90% reduction in taxane-induced arthralgias/myalgias (300mg TID; 2 days prior to start to 5 days following completion of chemo)

Opioid Resistant Pain
Neuropathic Pain
Bony metastases
Incident Pain
Visceral Pain

Other options for management of complex pain
Steroids Methadone Bisphosphonates Radiotherapy Interventions

Interventional Pain Management Techniques
Nerve blocks Vertebroplasty/cementoplasty Intraspinal analgesia
epidural intrathecal

Objectives
Improve management of nociceptive pain
Address neuropathic pain
Address fears about opioids
Which of the following is the strongest opioid?
A) fentanyl
B) hydromorphone
C) morphine
D) oxycodone
E) none of the above
Opioid “Strength”
Patients/caregivers ask “Is this too strong?” How do we respond?

Opioid “Strength”
Patients/caregivers ask “Is this too strong?” How do we respond? Potency (opiate receptor affinity; accounts for
“difference” in # of mg) Equianalgesic dosing Titrate to effectiveness “All opioids are in the same category in terms of
strength. Its about figuring out which one and what dose works the best for you and your pain.”
Ed’s Wife: Fears About Opioids
Often education and dispelling myths is all that is required to address adherence

Opioid Myths
MYTH 1 – opioids cause addiction Physical dependence is an expected result of long-term
opioid treatment but SHOULD NOT BE CONFUSED WITH ADDICTION
Physical dependence = withdrawal syndrome Addiction is a chronic neurobiologic disease with
genetic, psychosocial and environmental factors Helpful to patients to differentiate reason for use ie
relieving physical pain versus escaping psychological “pain”
Opioid Myths
MYTH 2 – opioids cause euphoria In terminally ill patients +/- those with pain,
opioids do NOT cause euphoria Mood may improve because their pain is
relieved

Opioid Myths
MYTH 3 – opioids = rapid tolerance Tolerance = state of adaptation,
diminished effect of drug over time Clinically significant tolerance is
unusual however in patients with progressive disease, increased levels of opioids are needed to control increased levels of pain
Opioid Myths MYTH 4 opioids = respiratory depression Respiratory depression is extremely rare Downregulation of mu2 receptor within 48 hours of
routine dosing Opioids are a crucial part of the treatment plan for
patients with end stage COPD, end stage CHF, advanced lung cancer
Naloxone (Narcan) is rarely indicated Differentiate between opioid side effects and
normal dying process
Nausea

Jack
58 yo male; advanced colorectal; colectomy followed by FOLFOX
Further abdominal progression; current on FOLFIRI
In ER with 6 days prog increasing abdo distension and generalized abdo pain; 2 days n/v; no BM x 2 days
prn Percocet worsened nausea

Jack
Proximal partial SBO diagnosed, NG inserted, IV fluids started, Gravol 25-50mg IV q4h prn for nausea and morphine 5mg sc q4h prn for pain
24 hour f/u - pt still c/o severe nausea, abdo pain somewhat improved (morphine BT x 4 given), pt has used Gravol routinely

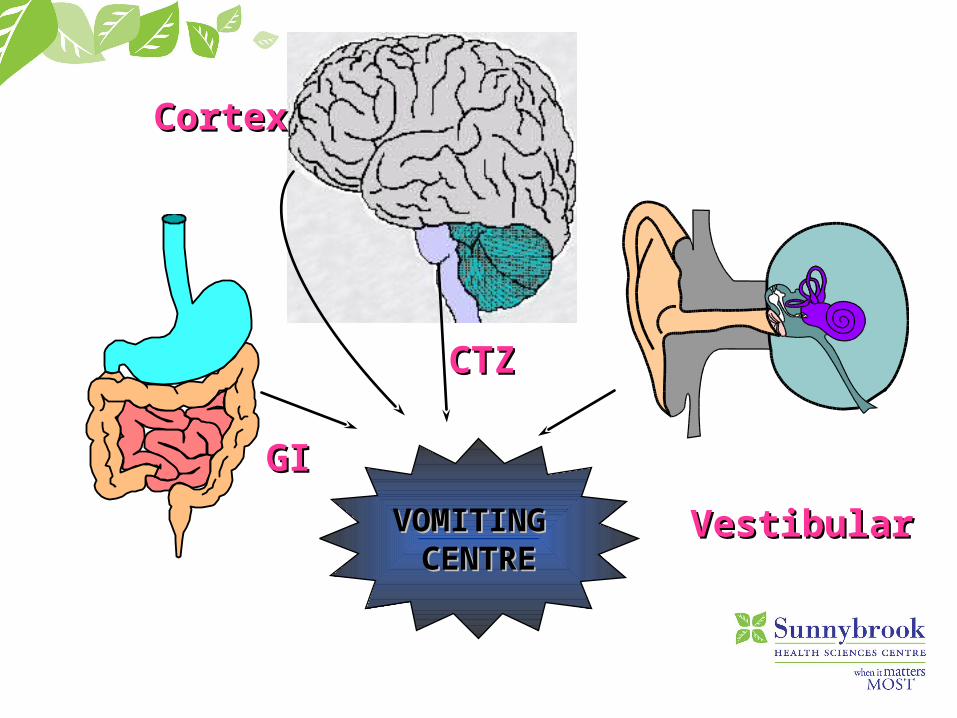
Nausea/Vomiting
Vomiting centre in reticular formation of medulla
Activated by stimuli from:– Chemoreceptor Trigger Zone (CTZ)– Upper GI tract & pharynx– Vestibular apparatus– Higher cortical centres
CortexCortex
CTZCTZ
VestibularVestibular
GIGI
VOMITING VOMITING CENTRECENTRE
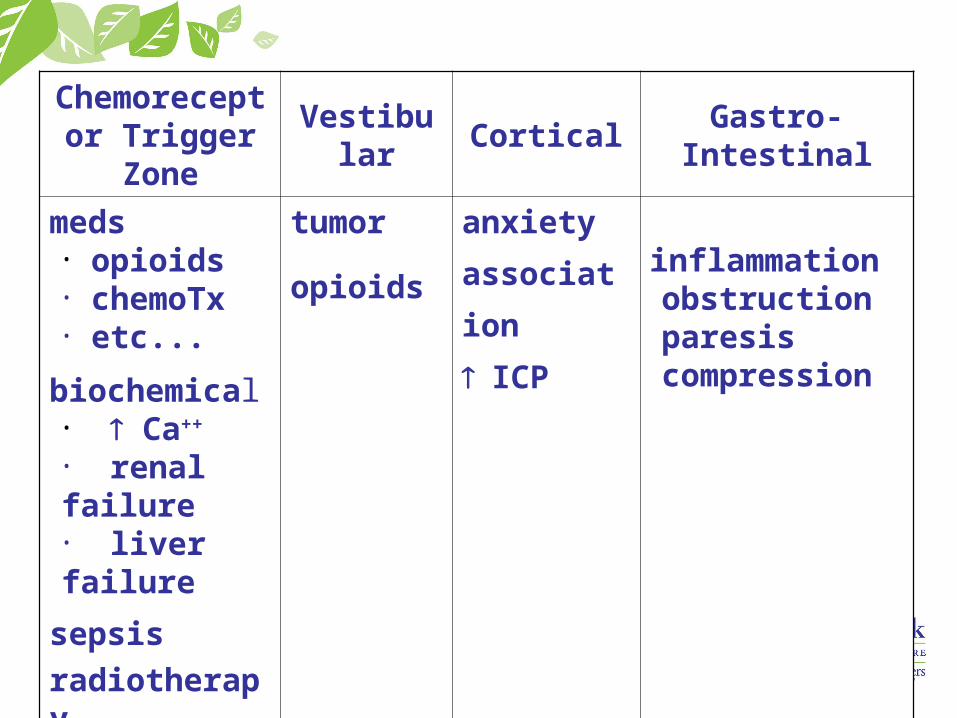
Chemoreceptor Trigger Zone
Vestibular Cortical Gastro-Intestinal
meds• opioids• chemoTx• etc...
biochemical• Ca++
• renal failure• liver failure
sepsis
radiotherapy
tumor
opioids
anxiety
association
ICP
inflammationobstructionparesiscompression
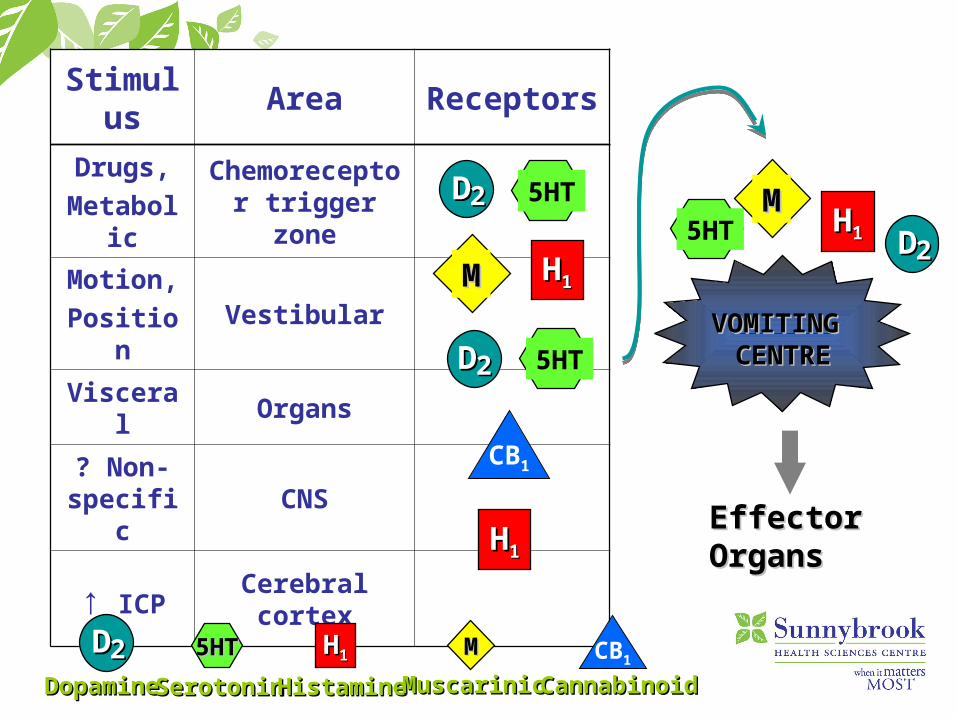
Stimulus Area Receptors
Drugs,
MetabolicChemoreceptor
trigger zone
Motion,
PositionVestibular
Visceral Organs
? Non-specific
CNS
↑ ICP Cerebral cortex
DD22 5HT
MM HH11
DD22 5HT
HH11
VOMITING VOMITING CENTRECENTRE
5HTMM
HH11
5HT5HT MMHH1122
EffectorEffectorOrgansOrgans
DopamineDopamineSerotoninSerotoninHistamineHistamineMuscarinicMuscarinicCB1
CannabinoidCannabinoid
CB1
DD22
DD22

1250
Relative Anti-Emetic Receptor Affinities
Summary of Anti-Emetics
Dopamine Antagonists – haloperidol > prochlorperazine > CPZ > metoclopramide
Muscarinic Antagonists – scopolamine Histamine Antagonists – dimenhydrinate
> promethazine > meclizine Serotonin Antagonists – ondansetron Misc – cannabinoids, steroids, benzos

Jack
Proximal partial SBO diagnosed, NG inserted, IV fluids started, Gravol 25-50mg IV q4h prn for nausea and morphine 5mg sc q4h prn for pain
24 hour f/u - pt still c/o severe nausea, abdo pain somewhat improved (morphine BT x 4 given), pt has used Gravol routinely
Jack
Optimal medical management of both nausea and the MBO would include:– Octreotide 500 micrograms sc tid– Dexamethasone 4mg sc/iv q8h – Opioids for pain– Consider Buscopan– Consider motility agents
Haloperidol 0.5 mg anti-emetic of choice for opioid induced nausea
Nausea
Think about underlying mechanism, associated receptor and use appropriate category of medication
Haldol – safe

Dyspnea
Epidemiology 70% of patients experience dyspnea in the
final six weeks of life1
55% of patients with advanced cancer experience at least moderate dyspnea2
Of those with symptom, 60-80% rate it as clinically important3
1National Hospice Study2Bruera et.al.3Donnelly and Walsh. The symptoms of advanced cancer. Sem Oncol 22(2):67-72

Pathophysiology
Initiation of breathing and its ongoing control is one of the main functions of the medulla (and to a lesser extent the pons)
Medulla receives afferent neural input from:– chemoreceptors in carotid and aortic bodies
– receptors in the muscles/tendons that participate in breathing
– receptors in the upper and lower airways
– receptors in the medulla itself that respond to changes in pH (which is largely regulated by pCO2)

Pathophysiology
Efferent instructions to the muscles involved in breathing comes through two spinal cord pathways:– from the medulla through the ventral portion– from the cortex through the dorsal
corticospinal tract
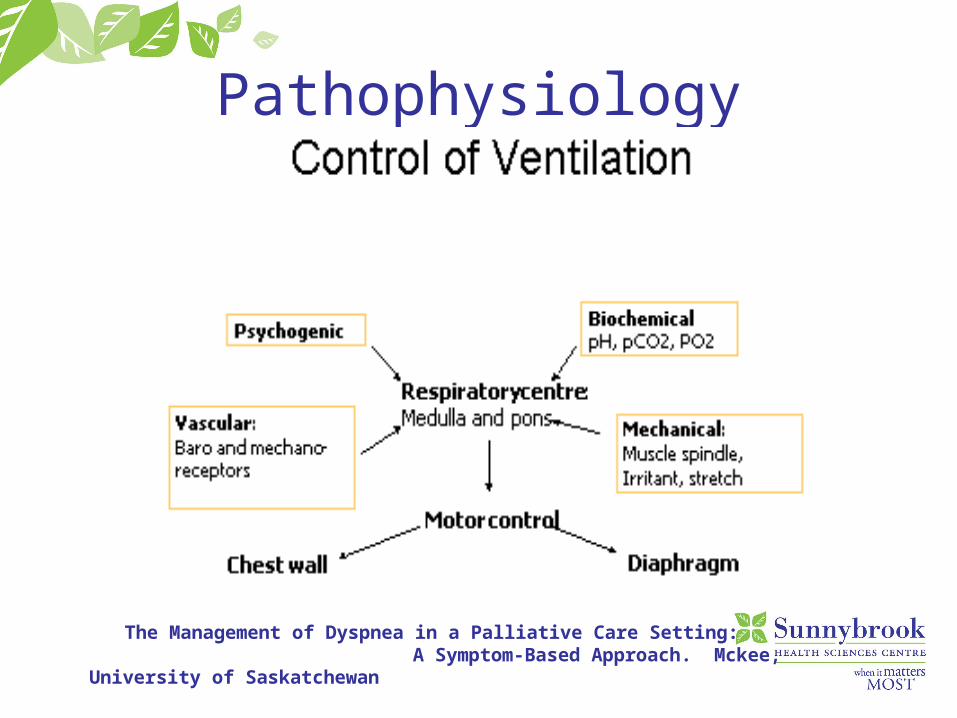
Pathophysiology
The Management of Dyspnea in a Palliative Care Setting: A Symptom-Based Approach. Mckee, University of Saskatchewan

Symptom Management
Non-pharmacologic Pharmacologic:
– opioids– benzodiazepines– phenothiazines– systemic corticosteroids

Opioids
Exact mechanism is not well understood
Benefit does not result from inhibition of respiratory drive– significant relief has been demonstrated
with no change in ventilation or pCO2
Opioids Few opioids have been studied and data is
surprisingly sparse Majority of evidence – morphine Conclusions of a systematic review:
significant overall benefit of systemic opioids on breathlessness and exercise tolerance1
Nebulized morphine compared to placebo is not beneficial for relieving dyspnea or exercise tolerance
1Jennings et. al. A systematic review of the use of opioids in the management of dyspnea. Thorax. 57:939-944
Benzodiazepines
Only one trial published involving cancer patients1
– compared morphine alone, midazolam alone and the combination
– when combined, dyspnea significantly improved
No trials examining benzos alone have demonstrated significant improvement in dyspnea or exercise tolerance
1Navigante et. al. Midazolam as adjunct therapy to morphine in the alleviation of severe dyspnea perception in patients with advanced cancer. J Pain Symptom Manage 31:38-47
Phenothiazines No studies in cancer patients One placebo controlled trial detected a
significant benefit with promethazine on dyspnea and exercise tolerance1
1Woodcock et. al. Drug treatment of breathlessness. Br Med J 283:343-346
Corticosteroids
No comparative trials have been published
Dyspnea - Conclusions
Existing evidence supports the use of systemic opioids for treating dyspnea
Oral promethazine could be used as an alternative if opioids not an option
No evidence to support the use of benzodiazepines to treat dyspnea (although known to significantly improve anxiety)
Future research: hydromorphone, oxycodone, fentanyl corticosteroids

End of Life Discussion
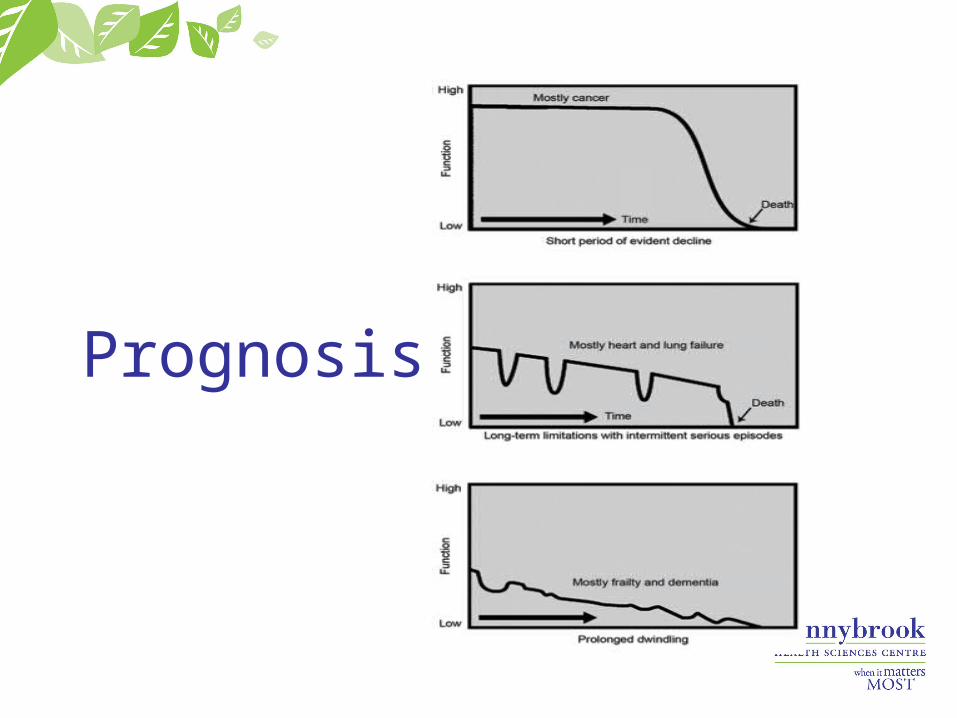
Prognosis

End of Life Discussion
JAMA. 2008 Oct 8;300(14):1665-73
Wright AA, Zhang B, Ray A, Mack JW, Trice E, Balboni T, Mitchell SL, Jackson VA, Block SD, Maciejewski PK, Prigerson HG.
Associations between end-of-life discussions, patient mental health, medical care near death, and caregiver bereavement adjustment.
End of Life Discussion To determine whether end-of-life discussions with
physicians are associated with fewer aggressive interventions
Multisite, prospective, longitudinal cohort study of patients with advanced cancer and their informal caregivers (n = 332 dyads)
Median f/u (enrollment to death) = 4.4 months Bereaved caregivers' psychiatric illness and quality
of life was assessed a median of 6.5 months later

End of Life Discussion
Primary outcome measures: aggressive medical care (eg, ventilation, resuscitation) and hospice in the final week of life
Secondary outcomes included patients' mental health and caregivers' bereavement adjustment
123 of 332 (37.0%) patients reported having end-of-life discussions before baseline
End of Life Discussion
Discussions were not associated with higher rates of major depressive disorder or worry
After propensity-score weighted adjustment, end-of-life discussions were associated with lower rates of ventilation, resuscitation and ICU admissions
More aggressive medical care was associated with worse patient QoL and higher risk of major depressive disorder in bereaved caregivers

Advance Care Planning
Advocate for ACP and Goals of Care Discussions to be an iterative routine element of cancer care for patients with incurable disease
“The role of chemotherapy at the End of Life: When is Enough, Enough?”
JAMA June 11, 2008 – Vol 299(22): 2667-2678.