Tom Ball FRCS (Tr & Orth) Phil Vaughan FRCS (Tr & Orth...
76
Consensus of the 4 th Round Table Budapest June 2014 Tom Ball FRCS (Tr & Orth) Phil Vaughan FRCS (Tr & Orth) Dishan Singh FRCS (Orth) Complications in Foot and Ankle Surgery
Transcript of Tom Ball FRCS (Tr & Orth) Phil Vaughan FRCS (Tr & Orth...

Consensus of the 4th Round TableBudapest June 2014
Tom Ball FRCS (Tr & Orth)
Phil Vaughan FRCS (Tr & Orth)
Dishan Singh FRCS (Orth)
Complications in Foot and Ankle Surgery

Preface
The 1st Round Table meeting was held in Padua in June 2011, followed by the 2nd meeting in Paris inJune 2012 and the 3rd meeting in Barcelona in June 2013. This year’s meeting in Budapest has onceagain not followed the usual orthopaedic meeting format where faculty members lecture todelegates. As always, the meeting is unique in that all participants have an equal input to review theliterature and present their individual experience on a topic - with ample time for an informaldiscussion of the subject in a relaxed setting.
In 2014, we have chosen to discuss the topic of dealing with complications we may encounter in ourclinical practice. Discussion of complications is rarely addressed in the foot and ankle literature or atmeetings where more time is spent on discussion of success. To quote Mercer Rang, the surgeongrieves for the patient who has suffered a complication under his or her care and the surgeon’s wholeoutlook on a particular problem may be altered. Yet, a surgeon has to formulate a logical plan forinvestigating and treating the encountered complication.
Phil Vaughan and Tom Ball were responsible for recording opinions and capturing the essence of thedebates, many of which resulted in consensus being reached on areas of foot and ankle practice. Thisbooklet collates the literature review and the views of all those who participated.
This booklet does not represent Level I evidence derived from prospective randomized controlled trialsbut represents the compilation of the combined experience of 35 British orthopaedic surgeons as wellas a much valued input from Chris Coetzee from the United States of America and Michael Stephensfrom Ireland.
I hope that you will find something of use and relevant to your own practice.
Dishan Singh, MBChB, FRCS, FRCS (Orth)
Consultant Orthopaedic Surgeon
Royal National Orthopaedic Hospital
Stanmore, United Kingdom
October 2014

Consensus of the 4th Round Table
Budapest 2014
Complications in Foot & Ankle Surgery
Tom Ball
Phil Vaughan
Dishan Singh
Convenors:
Mr Dishan Singh
Mr Paul Cooke
Mr Nick Geary
Mr Fred Robinson
Hosts:
Ortho Solutions
_______________________________
Distilled in this document are the thoughts and opinions with consensus where possible of 35 Orthopaedic Foot and Ankle ConsultantSurgeons who gathered from across the United Kingdom, Ireland and USA. Though eminence rather than true evidenced based medicinethis represents the concepts of over 200 years of combined experience. A basis of invited lectures introduced open and frank discussionfrom which consensus was sought. The statements herein only represent those of individuals and no claim is made that they areirrefutable. All the percentage figures quoted represent the proportion of the surgeons present who voted on the subject in discussion.

Deep vein thrombosis Dishan Singh
Infection/ wound healing Simon Platt
Delayed union/ non-union Chris Coetzee
Malunion Paul Cooke
Nerve injury Michael Stephens
Chronic Pain including RSD Andy Molloy
Hallux varus David Williamson
Recurrence Mark Herron
Avascular necrosis metatarsal head Mark Davies
Transfer metatarsalgia Anand Pillai
Failed cheilectomy Stephen Bendall
First MTP joint malunion/non-union Ben Rudge
Failed first MTP joint Keller’s or arthroplasty Tim Williams
Floating toe/stiff MTPJ Amit Amin
Short or floppy lesser toes after surgery Rick Brown
Non-union, malunion, AVN after Weil or DMMO Fred Robinson
Session 3 HALLUX RIGIDUS SURGERY
Session 1 GENERAL POST-SURGICAL COMPLICATIONS
Session 4 LESSER TOE SURGERY
Session 2 HALLUX VALGUS SURGERY

Achilles tendon rerupture Matthew Henderson
Wound healing after Achilles surgery Callum Clark
Achilles too long or too short Sam Singh
Persistent flat foot after tib post reconstruction Chris Coetzee
Problems after peroneal tendon surgery Michael Stephens
Failed lateral ligament stabilisation Rhys Thomas
Failed talar dome OCD debridement Andy Goldberg
Failed syndesmosis repair Senthil Kumar
Malunion ankle fracture incl short fibula Hiro Tanaka
Failed deltoid ligament repair Sunil Dhar
TAR malleollar fracture Tim Clough
TAR malalignment/ loosening Bob Sharp
TAR wound & neurovascular complications Mike Karski
Malunion triple/midfoot arthrodesis Nick Cullen
Non-union hindfoot/midfoot arthrodesis Ioan Tudur Jones
Malunion calcaneal fracture Ian Sharpe
Malunion/ Non-union talar neck fracture Kurt Haendlmayer
AVN talar neck fracture Steve Parsons
Navicular stress fracture Nick Talbot
Session 5 TENDON, LIGAMENT & OCD SURGERY
Session 6 ANKLE FRACTURE
Session 7 ANKLE REPLACEMENT
Session 8 HINDFOOT & MIDFOOT SURGERY

Deep Vein Thrombosis
Debate continues on the perceived incidence of deep vein thrombosis (DVT) after foot and anklesurgery and the role of prophylaxis. This is partly because there is a discrepancy in the literature in thedefinition of what constitutes a deep vein thrombosis: symptomatic/ asymptomatic and particularly thedistinction between distal (below knee or calf) or proximal (above knee or thigh) DVTs.
Calf DVTs are only detected if a whole leg ultrasound scan is performed. On the other hand manyradiology departments follow the NICE Clinical Guideline 144 of 2012 to only scan and report onproximal DVTs, because whole leg ultrasound is time consuming and technically demanding. CalfDVTs only very rarely cause pulmonary emboli and are therefore not usually treated byanticoagulation. However about 30% of calf DVTs can propagate to become proximal DVTs in abouta week and the NICE guidelines 144 state that proximal leg ultrasound should be repeated in 6-8 daysin high risk patients (all orthopaedic patients). An audit at the Royal National Orthopaedic Hospitalhas shown that junior doctors are unaware of this guideline and requests for a repeat ultrasound scanare rarely made. DVTs after orthopaedic surgery may therefore be under-diagnosed and under-reported.
Patel et al. retrospectively reviewed a large U.S healthcare management database and identified 1172patients with Achilles tendon ruptures and found a reported incidence of 0.43% of symptomaticDVTs. Scandinavian studies where a detailed sonographic study of the whole leg patients with anAchilles tendon rupture has been performed have stated that the incidence of symptomatic andasymptomatic DVT to be about 32%. Some clinicians thus perceive the incidence of DVT afterAchilles tendon rupture to be high. A detailed study of the paper of Nilson-Helander et al, forexample, however identifies that of the 32 reported DVTs in 100 patients with symptomatic andasymptomatic DVTs, 27 were calf DVTs and 5 were thigh DVTs (the reported rate in the UK wouldthus be 5% and not the reported 32% rate in the study). It is thus suggested that all studies andguidelines on prophylaxis should clearly state whether calf DVTs are being considered.
Prophylaxis
The NICE guidelines 2010 (section 2.2.6) on lower limb casts that highlights that patients in a castshould be risk assessed and LMWH discussed and offered. In 2012 we reached an unusual butsatisfying 100% consensus that every patient should undergo risk assessment for DVT during electivesurgery. Immobilisation and NWB status were highlighted as a significant risk factor.
Current practice 2014: The use of LMWH prophylaxis when in a NWB cast:
70% use prophylaxis after a triple fusion
80% use prophylaxis with Achilles tendon ruptures
100% use prophylaxis after ankle fracture if there is an additional risk factor
When in a WB cast...
15% would use prophylaxis in ankle fractures with no additional risk factors

Investigation
Whilst the symptoms and signs of a DVT are often non-specific, it is the presence of symptoms/ signsor a high level of suspicion that alerts the clinician to investigate. Whilst venography may remain thegold standard, USS remains the most practical and widely available. D-dimer is of questionable use inthe post-operative period as it will usually be raised.
Current practice 2014: How to investigate if clinically suspicious for DVT
15% would measure the D-dimer
75% would refer for an USS (50% via hospital protocol)
65% would ask for USS whole leg
80% of those who refer for USS would repeat USS if negative but suspicion remained
However 0% used the Wells 2 level score as per the NICE guidelines
The NICE guidelines (figure) highlight that the Wells two level test probability score (figure) shouldbe used to determine the probability of DVT and guide treatment.
Treatment of DVT
Current practice 2014: symptomatic proximal DVT
3 months anticoagulation if time limited risk factor i.e. cast/ immobilisation
6 months anticoagulation if risk factor isn’t time limited
>12 months or lifetime anticoagulation if recurrent DVT or patient has a malignancy
Current practice 2014: on distal DVT
30% would anticoagulate
10% would not anticoagulate
60% did not know and would consult DVT service/ haematologists
Consensus on DVT prevention 2014
All patients should be risk assessed for DVT Immobilisation in a NWB cast remains a significant risk factor and progressing patient to WB
status, decreases this risk. Patients who are NWB in cast should have LMWH prophylaxis
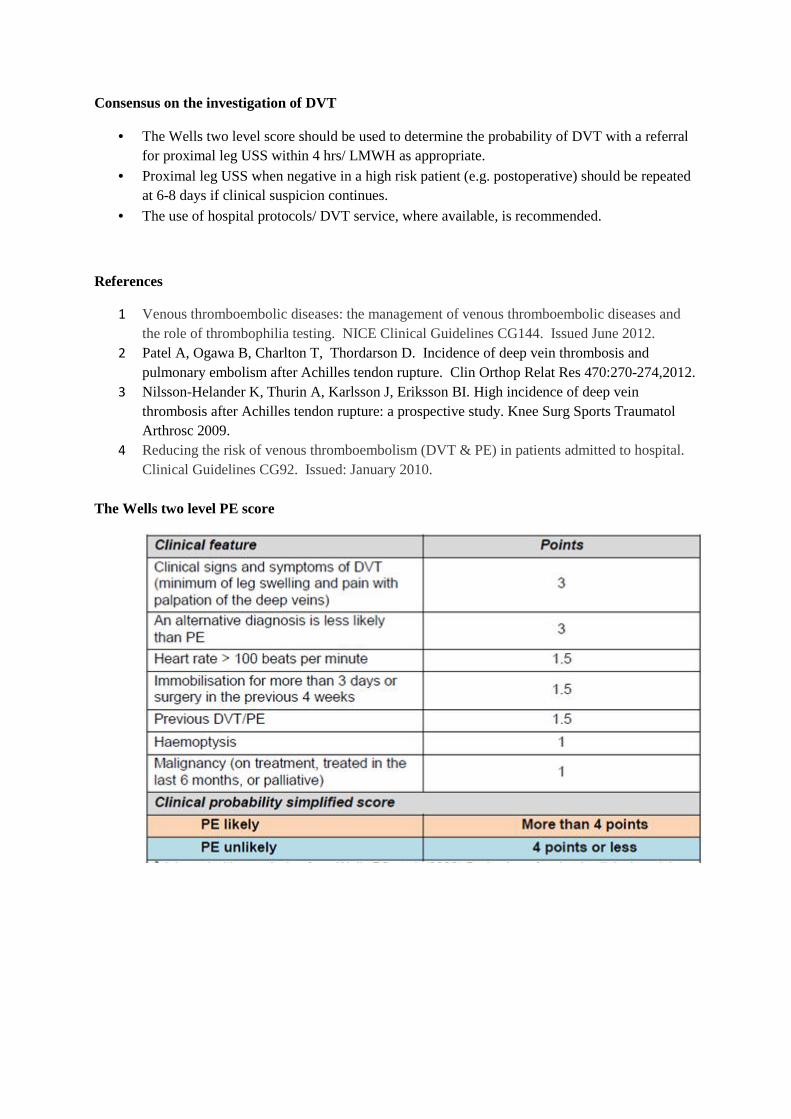
Consensus on the investigation of DVT
The Wells two level score should be used to determine the probability of DVT with a referralfor proximal leg USS within 4 hrs/ LMWH as appropriate.
Proximal leg USS when negative in a high risk patient (e.g. postoperative) should be repeatedat 6-8 days if clinical suspicion continues.
The use of hospital protocols/ DVT service, where available, is recommended.
References
1 Venous thromboembolic diseases: the management of venous thromboembolic diseases andthe role of thrombophilia testing. NICE Clinical Guidelines CG144. Issued June 2012.
2 Patel A, Ogawa B, Charlton T, Thordarson D. Incidence of deep vein thrombosis andpulmonary embolism after Achilles tendon rupture. Clin Orthop Relat Res 470:270-274,2012.
3 Nilsson-Helander K, Thurin A, Karlsson J, Eriksson BI. High incidence of deep veinthrombosis after Achilles tendon rupture: a prospective study. Knee Surg Sports TraumatolArthrosc 2009.
4 Reducing the risk of venous thromboembolism (DVT & PE) in patients admitted to hospital.Clinical Guidelines CG92. Issued: January 2010.
The Wells two level PE score

DVT diagnosis guidelines as suggested by NICE

Wound healing
There are times in all our practice when wound healing by primary intention is either not possible orunsuitable. The wound, whether surgical or traumatic, is then required to heal by secondary intentionor via the transfer of tissue from elsewhere. The latter of these is almost exclusively under the controlof the plastic surgeon which leaves us to deal with the slow to heal, often infected, granulating wound.It is in the management of such wounds that negative pressure wound therapy (NPWT) has gainedpopularity. The sceptics amongst us may say that this is due to slick marketing and “pseudoscience”,however in trying to reach consensus it was clear that in the management of a “difficult” wound theiruse is generally recommended.
Current practice 2014: Do you use Vac therapy for difficult to heal wounds?
100% yes
With such popularity it is useful to remind ourselves of what negative pressure dressing can add towound management. They should not be used as a replacement for adequate wound irrigation anddebridement or instead of a graft or flap by your local plastic surgeon. NPWT provides:
Maintains a moist environment✓
Reduces oedema✗
Increases local blood flow✓
Stimulates angiogenesis and granulation tissue✓
Reduces wound size✓
Removes wound healing inhibitors✗
Reduces bacterial load✗
Consensus on the use of vac dressings.
Their use is generally recommended as an adjunct when primary wound closure or soft tissue
transfer techniques are not appropriate.
Non-union – Diagnosis and management
Diagnosis of Non-union
Whilst we all accept that this diagnosis is based on a combination of symptoms, signs and imagingresults, we often look towards the latter for an objective assessment of what can vary widelyclinically.
Current Practice 2014: The use of CT to diagnose non-union
75% use CT for the diagnosis of a non-union
85% require ≥50% bony continuity for union on CT
However the percentage of bony continuity on CT does not have any clinical correlation and thereforewhether the joint is fused or not fused ultimately depends on the clinical picture. Some groups wouldaccept that given a lack of clinical symptoms bony continuity of 20-25% is sufficient to diagnose bonyunion.
How to address Non-union
Is it infected? Is there mechanical failure? Is the patient suitable for further surgery? Are there patient factors that can be managed better?
There are undoubtedly situations when there is infection and/ or mechanical failure of a fusion orfixation that will require early surgical intervention. However in the absence of either of these factorsthe use of adjuvant therapy is advocated. This may take the following forms:
Bone stimulation: Implanted or external Concentrated growth factors BMP and alternatives
Bone stimulation
A fracture site produces a negative electropotential. Through manipulation of this further celluarstimulation can be provided to promote bone healing. This can be provided internally or externally.There is a lot of evidence for long bones and its use is supported by NICE guideline MTG12.However, there is only early evidence to support its use in the ankle but not in the foot (1,2).
Current practice 2014: Use of Exogen stimulation
50% routinely use Exogen in non-unions
25% would like to use it but have funding issues

Growth Factor concentrate
Bone marrow aspirate can be used independently or in combination with platelet rich plasma (PRP),injected into the site of concern and produce a small but measurable improvement in bone healing (3).Within this it is felt that BMA may play a greater role but there is to date insufficient evidence tosupport this.
BMPThese are all members of the TGF-β superfamily (except BMP-1). They are modulators ofosteoprogenitor and mesenchymal cells during osseous healing. The genetically engineered rhBMP2/7have limited approval and have to be used “off label” for foot and ankle cases. Despite this there issome limited evidence for their successful use in high risk ankle and hindfoot fusions such asdiabetics, the immunosuppressed or following high energy injury(4).
Current practice 2014: Use of BMP for non-unions
US surgeons use it for every case
20% of British surgeons use it routinely and have good access to it.
40% of British surgeons have to apply specially via commissioners
Hindfoot non-union experience from Guys Hospital
Revision surgery for a hindfoot non-union should be performed in conjunction with your
microbiologist. The experience from Guys Hospital follows the following steps:
1. Assume it is infected
2. No antibiotics until samples taken.
3. Give broad spec such as vancomycin and gent (dw micro)
4. Samples to take are 3xmicro and 3x histology
5. Send micro for PCR
6. If cultures are negative then antibiotics are discretionary and are only given if thought to be
high risk
7. If cultures are positive then antibiotics are given as per sensitivities until union is achieved.
Infected non-unions are effectively therefore treated with a single stage revision and suppressive
antibiotics until union. The pathogens noted from the experience at Guys are either
staphylococcus aureus, enterobacter or pseudomonas.
Consensus
A non-union can be defined as a painful arthrodesis with <50% bony continuity
Exogen stimulator use is recommended
Bone stimulation with BMP/ growth factors for high risk patients
Assume it is infected
Non-union – Risk factors
Whilst the definition of a non-union remains variable, it is generally accepted that approximately 1 in20 patients undergoing an elective ankle or hindfoot fusion will develop one. In the treatment orindeed the prevention of a non-union it is vital to identify the risk factors for poor bone healing. Theserisks can be broadly divided into host factors and surgical site factors.
The commonest host factors are infection, smoking, nutritional (vitamin D deficiency), diabetes,vascular compromise and systemic factors. The surgical site, the soft tissues and the mechanicalenvironment the bone is placed under until it unites, is under our control.
Infection:
Staph Aureus has been shown to inhibit osteoblast activity and stimulates osteoclast activity (1).However infection can be sub-clinical with normal inflammatory markers and therefore difficult todetect. Culture results from problematic wounds can be misleadingly negative, in part due to biofilmformation and previous bacteriostatic antibiotic effects. Molecular diagnostics (DNA & RNA PCR)are more sensitive and thus play an important role in detecting infection as a cause of non-union.
Smoking:
The relative risk of developing a non-union as a smoker is up to 5X when compared to non-smokers.Also their time to union is 25% longer.
Current practice 2014: Would you perform an elective primary fusion on a smoker
40% would not
60% would advise to stop but operate anyway
NSAIDs:
There is some evidence in animal models that COX-2 inhibition inhibits early bone healing. Howeverthis hasn’t been reproduced in humans (2).
Poor evidence in humans
Current practice 2014: Use of NSAIDs in a patient undergoing a fusion
50% advise against the use in the first 2 weeks
Diabetics
Whilst we all council a diabetic patient on the increased risks of surgery and also the time to union,there are three main factors that significantly increase bone healing complications (3):
1. Peripheral neuropathy2. Duration of surgery3. HbA1c >7%
To a great extent these risk factors can be controlled.
Nutritional status
Vitamin D is essential for bone mineralisation and the subsequent maintenance of bone quality andfracture healing. Despite this the true benefits of supplementation even in vitamin D deficient patientsremain unclear (4).
Current practice 2014: Do we investigate for vitamin d deficiency?
10% would test for it before primary surgery
25% would test for it in a patient with non-union
Currently in the USA the use of vitamin D supplementation, to promote bone healing/ union, in thoseundergoing major foot and ankle surgery is becoming widespread. Vit D level is not tested. This isbased on a health-economics argument as the cost of vitamin D 5000 IU/day or 50,000 IU weekly for3 weeks pre-operatively and 12 weeks post-operatively is significantly less (10%) than the laboratorytest for deficiency.
Consensus on non-union
All patients with a non-union should undergo investigation for vitamin D deficiency. This canbe performed and managed by the treating surgeon or a local metabolic bone specialist.
Smokers should be advised of the increased risk of non-union and advised to stop andNSAIDs avoided in the 1st 2/52 post-op.
Diabetic control needs to be optimum in the period leading up to their surgery and theirHbA1c normalised in conjunction with a diabetologist. The surgical procedure on a diabeticneed to be appropriately planned to minimise its duration.
References
1. BMC musculoskeletal disorders. 2013Jun14;14:1872. Kurmis. J Bone Joint Surg Am, 2012 May 02;94(9):815-8233. J Foot Ankle Surg. 2013 Mar-Apr;52(2):207-114. Bone. 2014 Jul;64C:288-2975 Midis N, Conti SF. Revision ankle arthrodesis. FAI 20026 Saltzman et al: PEMF as treatment for delayed healing of foot and ankle arthrodesis. FAI
20047 Clin Orthop Rel Res. DOI: 10.1007/11999-014-3548-38 Bibbo. Tech Orthop 2011;26: 28–31

Malunion
A working definition of a malunion is when there is bony unity without proper restoration of the
normal anatomical and weight-bearing axis of the limb. It can occur in multiple planes, which all need
to be addressed.
Angulation
Translation/ displacement
Shortening
Rotation
Complex
A malunion can occur due to a lack of adequate reduction at the time of surgery or due to insufficient
construct stability. Stability needs to be maintained until the bone unites and requires the full
compliance of the patient. The time taken for a bone to unite varies widely and risk factors such as
smoking, nutritional deficiency, diabetes, vasculopathy and systemic disease such as rheumatoid
should be taken into consideration.
Vitamin D deficiency was raised again as an area of renewed interest in such patients, especially from
the USA.
Current practice 2014: Regarding the investigation for vitamin D deficiency
7% would test for in the presence of a symptomatic malunion
When there is a malunion it can have wide-ranging effects:
Pain
Dysfunction
Instability
Arthritis
When addressing a malunion deformity the principles of deformity adhered to. Deformity correction
requires the identification of the mechanical and anatomical axis, the CORA (Centre of rotation and
angulation) and the bisector line. The CORA is where the anatomical axis meet and the bisector line,
a line that bisects the obtuse angle of that deformity at the CORA.

Consensus on malunion
Investigate for vitamin D deficiency
Manage risk factors
Follow Deformity correction rules
o When osteotomy and hinge at level of CORA, only angulation is required to correct
deformity
o When osteotomy is done at a different level than the CORA, but hinge at level of
CORA then angulation and translation are both required to correct deformity. The
mechanical axis becomes parallel but anatomical axis becomes zigzag.
o When osteotomy and hinge are both not at level of CORA then translation deformity
occurs.
o In complex deformities consider each CORA separately, or consider performing
osteotomy at the resolved CORA to avoid multiple osteotomies.
Obey the law of rhomboidal osteotomy. The apex of the wedge should be at the skin or
beyond it. We are correcting boney and soft tissue deformity.

Nerve injury
Neurological compromise can present with sensory, motor or mixed symptoms and signs, either aspart of the primary pathology or as a complication of surgical management.
In the management of post-operative neurological compromise it is important to be able to rely onclinical symptoms and signs as investigation with MRI or even EMG is inconclusive and userdependant. Despite this both investigations should be used to exclude proximal lesions, accessorymuscles, tumours and to highlight muscle function.
The common lesions around the foot and ankle are:
Saphenous nerve Superficial peroneal nerve Deep peroneal nerve Tibial nerve Sural nerve
Damage to the deep peroneal or the tibial nerve would have major motor and sensory implications forthe foot. Such lesions should generally be noticed within the acute phase and therefore be explored,repaired and/or decompressed.
The superficial sensory nerves or one of their aberrant branches may easily be damaged leaving asmall area of insensate skin that is managed conservatively, but may subsequently develop aproblematic superficial chronic neuroma.
Symptomatic chronic superficial nerve lesions should undergo exploration and decompression. In thepresence of a neuroma, resection and burial in either bone, soft tissue or a nerve wrap should beperformed.
Consensus on treating nerve injury
Rely on clinical symptoms and signs Acute lesions should be decompressed/repaired Chronic lesion can be decompressed Neuromata:
Resect proximally Resect deep to facia Burial in bone better than muscle Keep away from the joint to avoid tension Peri-operative use of local anaesthetic infiltration

Chronic Regional Pain Syndrome (CRPS)
Patients in chronic pain often feel misunderstood and may exaggerate symptoms or signs in order to
get clinicians to understand and acknowledge their problem. This makes this a difficult area of our
practice to manage.
CRPS can be seen in up to 25% (1, 2, 3) of post-operative/ post trauma patients but in some
CRPS patients there is no obvious preceding cause (4). It is usually confined to a single limb but
can “spread” to additional limbs in 7% (5-7).
It is often divided into 2 subtypes
Type 1 – Absence of major nerve lesion
Type 2 – Presence of major nerve lesion (more common)
There are many reasons why a patient may have ongoing pain post-operatively including malunion,
non-union, loose prosthesis, infection, nerve injury, metal allergy and psychosocial. It is therefore
wise to take a broad approach to the investigation and management of such patients and only come to
a conclusion of complex regional pain syndrome (CRPS) when other causes have been excluded.
In addition to excluding other causes of pain, CRPS has typical symptoms and signs that need to be
observed before the diagnosis can be made. These are highlighted by the Budapest criteria (8).
Budapest criteria
To make a clinical diagnosis the following criteria must be met:
1. Continued pain, disproportionate to the inciting event
2. Must report at least one symptom in three of the following four categories
i. Sensory-Hyperaesthesia and/or allodynia
ii. Vasomotor- temperature asymmetry and skin colour changes
iii. Pseudomotor/ oedema-sweating changes
iv. Motor/ trophic- stiffness, weakness, hair loss, nails, skin
3. Must display at least one sign in two or more of the following categories
i. Sensory-Evidence of hyperaesthesia and/or allodynia
ii. Vasomotor- Skin temperature asymetry >1°C and skin colour changes
iii. Pseudomotor/ Oedema-Evidence of sweating changes
iv. Motor/ trophic- Evidence of stiffness, weakness or trophic changes hair
loss, nails, skin
4. No other clinical diagnosis that explains symptoms/ signs
The chronicity of symptoms may be predicted by the presence of psychosocial risk factors or
“yellow flags”.
Previous negative experiences with health professionals
Poor coping strategies
Litigation
Overuse of appliances
Passivity
Negative family influences
Distress
Anxiety/ Depression
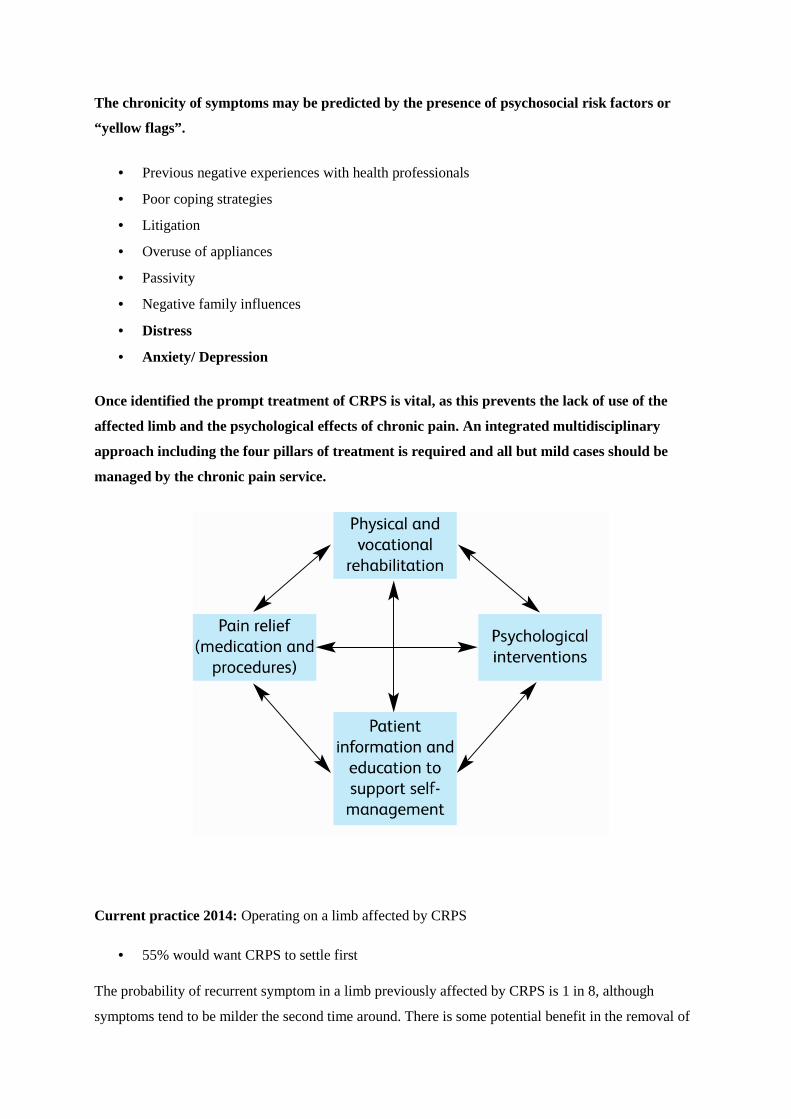
Once identified the prompt treatment of CRPS is vital, as this prevents the lack of use of the
affected limb and the psychological effects of chronic pain. An integrated multidisciplinary
approach including the four pillars of treatment is required and all but mild cases should be
managed by the chronic pain service.
Current practice 2014: Operating on a limb affected by CRPS
55% would want CRPS to settle first
The probability of recurrent symptom in a limb previously affected by CRPS is 1 in 8, although
symptoms tend to be milder the second time around. There is some potential benefit in the removal of

metalwork in someone with CRPS as there may occasionally be an undiagnosed metal allergy
contributing to the pain.
Consensus on re-operating on those with CRPS
Deal with ongoing underlying orthopaedic pathology
Remove metalwork
Pain team management of CRPS symptoms before and afterwards
Consider vitamin C and pregabalin prophylaxis
Amputation as an extremely last resort as only 25% successful
1) Atkins et al JBJS BR 1990
2) Dijkstra et al Eur J Pain 2003
3) Schasfoort et al Arch Phys Med Rehabil 2004
4) Baran et al. Anesth Anal 2002
5) Veldman et al. Lancet 1993
6) Van Rijn et al J Neural Trans 2011
7) Maleki et al. Pain 2000
8) Beerthuizen et al Eur J Pain 2009

Recurrent Hallux Valgus
“Despite correct selection and application of surgical techniques, it is a fact that recurrence stilloccurs.”
Recurrent hallux valgus is a problematic topic, first because it is not always clearly defined in theliterature. It is often surgeon defined and therefore prone to bias. One could use the hallux valgusangle (HVA), the inter-metatarsal angle (IMA) or the position of the sesamoids.
Faber1, comparing Hohmann distal closing wedge osteotomy with the Lapidus procedure, definedrecurrence as an AOFAS score of 0 for alignment and/or those who were dissatisfied.
Austin and Leventen2 using the Chevron osteotomy quoted a recurrence rate of 10%. Okuda3 hadaround 10% recurrence after basal osteotomies. The initial pathology, severity of valgus, the ability toapply general principles and finally the execution of the surgery are probably more important than theparticular osteotomy used.
Minimally invasive surgery has a wide range of quoted recurrence rates, from 2.6% to 40%, whichmakes interpretation of this literature difficult without further work.
Patients may have recurrence of painless deformity, but remain satisfied, or vice versa. Faber foundthat 50% of those with recurrence were satisfied, would have the surgery again and did not wantrevision surgery. Equally, not all patients with a good correction will have a good outcome score.
Sammarco4 found that risk factors for recurrence include:
rheumatoid arthritis
generalised or localised hypermobility
a neurological aetiology
osteoarthritis
Poor compliance with post-operative instructions.
Okuda found the pre-operative HVA was predictive.
Management of recurrence
Conservative measures, including adapted shoes, should not be dismissed. The technical andpsychological challenge of revision surgery for patient and surgeon should point both towards thisoption.
If the initial correction was inadequate, a reliable, powerful osteotomy may be a reasonable anduncomplicated option – such as the Scarf5 – combined as always with balanced soft tissuereconstruction. Kitaoka and Patzer6 used a crescentic basal osteotomy on 16 feet, giving moderateresults (10 satisfied, 2 dissatisfied).
Hypermobility of the first ray (often defined as 1cm of dorso-plantar movement relative to the secondray) may be relevant to recurrence, but is controversial. There is debate as to whether it is causative orsecondary in hallux valgus, and whether it stabilises after correction. Nevertheless the concept, that

hypermobility allows an osteotomised metatarsal to escape into varus again, seems plausible. Thisleads naturally to the proposal of the Lapidus procedure (corrective 1st TMT arthrodesis). Coetzeeet al7 used it as salvage for failed hallux valgus surgery in 26 feet, with good improvement in anglesand no recurrence, but with three non-unions and only 77% unreserved satisfaction (one patientdissatisfied). Bednarz and Manoli’s series8 of primary Lapidus procedures for hypermobile feetshowed almost a 20% recurrence rate, but with 96% satisfaction, and a Okuda et al's randomisedcontrolled trial3 of Lapidus procedure vs Hohmann osteotomy for unselected feet with hallux valgus,found a 9% recurrence rate and a 20% dissatisfaction rate with the Lapidus procedure at 10 years. Thetrial also showed no difference between the recurrence rates for the two contrasting procedures, evenin a subgroup of patients with pre-operative first ray hypermobility. The procedure also has a longrecovery with most surgeons advising several weeks spent non weight bearing in a cast, and, beingproximal, it is both powerful and technically demanding, and so is unappealing to many surgeons.
First metatarso-phalangeal arthrodesis may seem an attractive option, offering as it does the chanceto virtually rule out a second recurrence, but it does remove a significant function in eliminating 1st
MTP movement. Grimes and Coughlin9 published a series of 33 patients, 55% of whom were treatedfor recurrent deformity, and delivered 88% patient satisfaction with correction, but an overallsatisfaction rate of 72% “good or excellent”. First MTP fusion may risk later inter-phalangeal jointarthritis. It does however offer early weight bearing and is surely the procedure of choice in anarthritic, valgus joint.
In summary, no procedure has universal success after failed hallux valgus surgery and conservativemanagement should be discussed and offered. Osteotomies, 1st TMT fusion or 1st MTP fusion can allbe justified, but more importantly, the factors leading to failure should be analysed and then addressedduring the revision. The surgeon should counsel patients that around 20% may still be dissatisfiedafter revision surgery and that fusions have a significant non-union rate.
Discussion
In response to questions on technique for the Lapidus procedure, Dr Coetzee clarified thatwhen the first ray is hypermobile, he believes the first and second metatarsals should be prepared forfusion and joined proximally with a screw to achieve true stability. He finds this technique provides asolid fusion and satisfaction, without screw breakage or complaints about a non-mobile first ray.
References
1. Faber FW, van Kampen PM, Bloembergen MW. Long-term results of the Hohmann andLapidus procedure for the correction of hallux valgus: a prospective, randomised trial witheight- to 11-year follow-up involving 101 feet. Bone Joint J. 2013;95-B:1222-1226.
2. Austin DW, Leventen EO. A new osteotomy for hallux valgus: a horizontally directed “V”displacement osteotomy of the metatarsal head for hallux valgus and primus varus. Clin OrthopRelat Res. 198125-30.
3. Okuda R, Kinoshita M, Yasuda T, Jotoku T, Shima H. Proximal metatarsal osteotomy for halluxvalgus: comparison of outcome for moderate and severe deformities. Foot Ankle Int.2008;29:664-670.
4. Sammarco GJ, Idusuyi OB. Complications after surgery of the hallux. Clin Orthop Relat Res.200159-71.
5. Bock P, Lanz U, Kroner A, Grabmeier G, Engel A. The Scarf osteotomy: a salvage procedurefor recurrent hallux valgus in selected cases. Clin Orthop Relat Res. 2010;468:2177-2187.
6. Kitaoka HB, Patzer GL. Salvage treatment of failed hallux valgus operations with proximal firstmetatarsal osteotomy and distal soft-tissue reconstruction. Foot Ankle Int. 1998;19:127-131.
7. Coetzee JC, Resig SG, Kuskowski M, Saleh KJ. The Lapidus procedure as salvage after failedsurgical treatment of hallux valgus: a prospective cohort study. J Bone Joint Surg Am. 2003;85-A:60-65.
8. Bednarz PA, Manoli A. Modified Lapidus procedure for the treatment of hypermobile halluxvalgus. Foot Ankle Int. 2000;21:816-821.
9. Grimes JS, Coughlin MJ. First metatarso-phalangeal joint arthrodesis as a treatment for failedhallux valgus surgery. Foot Ankle Int. 2006;27:887-893.

Hallux Varus
The most common cause of hallux varus is iatrogenic, after hallux valgus surgery. Less commoncauses include congenital, traumatic, burns contracture, inflammatory arthritis and neuromuscular.
Rates of post-operative hallux varus in the literature range from 4% (Choi, Brodsky et al1) to 17%(Trnka et al2). Part of the disparity is explained by the inclusion of asymptomatic cases in Trnka’sseries, whereas Choi only counted those who returned spontaneously and were dissatisfied. Trnkaused a powerful basal metatarsal osteotomy, which may also have contributed.
Causes of iatrogenic hallux varus
Any of the steps of hallux valgus surgery can cause varus if exaggerated.
Excessive resection of the medial eminence removes the bony support for the medial side of theproximal phalanx and was felt to be the leading cause of varus in Trnka’s series.
Over-correction of the intermetatarsal angle (IMA) or of the valgus interphalangeus are alsoobvious causes and predominated in Choi’s series.
Excessive lateral release (dividing the lateral collateral ligament, for instance), over-tightening of themedial capsulorraphy (common in the McBride procedure) and aggressive post-operative bandagingmay result in varus through soft tissue imbalance.
Excision of the fibular sesamoid is another known iatrogenic cause of varus.
As varus progresses it may be accompanied by clawing of the hallux (especially if FHB was released),an in-growing toenail and adduction of the lesser toes.
Trnka found that two thirds of patients tolerated varus well with “excellent” subjective outcomes. Itwas poorly tolerated if the angle was over 15 degrees, if there was transfer metatarsalgia orosteoarthritis of the MTP joint.
Management
Conservative management of hallux varus ranges from leaving it alone, splinting in the early phase toencourage lateral soft tissues to contract, to adapting shoes with a wide, deep toe box later on.
Operative management in the presence of arthritis should be with first MTP fusion.
If there is a fixed claw hallux, interphalangeal fusion should be combined with MTP realignmentprocedures.
Osseous corrections essentially reverse the steps in hallux valgus correction, and include bone graftingthe medial eminence as required; first metatarsal osteotomy; and “reverse Akin” osteotomy of theproximal phalanx.

Rochwerger3 reviewed 7 out of 8 patients who had undergone bone grafting of the medial eminencewith iliac crest graft and showed good corrections into 16-22 degrees of valgus. Only the patient with22 degrees was dissatisfied.
Scarf or Chevron osteotomies can be used to reverse hallux varus by medialising the head andcorrecting the distal metatarsal articular angle as necessary. Brodsky1 treated thirteen patients withscarf/Akin and six with Chevron/Akin osteotomies. One patient was dissatisfied and two had recurrentvarus. He noted that a pre-operative limited range of motion often improved after the correction.
Many soft tissue corrections have been devised which involve tendon transfers. Essentially they aimto reconstruct a deficient lateral collateral ligament and adductor tendon. Johnson’s dynamic extensorhallucix longus (EHL) transfer4 takes the tendon from the distal phalanx, threads it under theintermetatarsal ligament and transfers it into the lateral side of the proximal phalanx, fusing theinterphalangeal joint to prevent clawing.
Myerson’s modification5 splits EHL, leaving both halves attached distally, and threads the proximalend under the intermetatarsal ligament and into the first metatarsal as a static stabiliser. Anothervariant uses EHB6.
Valtin described a transfer of the first dorsal interosseous muscle from the second toe into the first7.Hawkins takes the distal attachment of abductor hallucis, passes it under the metatarsal and into thelateral aspect of the proximal phalanx7. A “reverse Hawkins” procedure divides the abductorproximally and transfers this end under the phalanx and into the lateral aspect of the first metatarsal.An analogous procedure has been described in one case using a mini-tightrope implant.
Plovanich et al7 reviewed eight studies reporting a total of 68 feet. With a mean follow up of 30months, there were 80-85% “good” results and 16% complication rate. These included four cases ofosteoarthritis, three of recurrent varus, and two of hallux valgus.
In conclusion, iatrogenic hallux varus is best avoided by judicious hallux valgus surgery, but mildvarus is well tolerated. Appropriate bony correction gives reliable results. There are several possibletendon transfers but little evidence to choose between them.
Discussion and Consensus
Of the 34 surgeons present, 30/34 (88%) had had at least one post-operative hallux varus. Themajority had been treated with bony procedures. Thirteen surgeons had treated one or more patientswith a soft tissue only procedure alone. The consensus was that surgeons would do this if no bonycorrection was required.
It was suggested that recurrence and varus are two sides of the same coin, that is under and overcorrection. Incorrect selection of technique may contribute, e.g. using a proximal osteotomy to correcta mild hallux valgus is quite likely to over-correct.
The issue of whether to use intra-operative fluoroscopy was raised. Fourteen of 34 (41%) never use it,eight (24%) always use it and eight sometimes use it e.g. for difficult cases. Mr Molloy presented 31cases performed without fluoroscopy, compared with 31 cases done with fluoroscopic guidance after achange in practice8. Although not randomised, this study showed a statistical difference in the amountof correction (bigger correction achieved when using fluoroscopy) and better positioning of thesesamoids on post-operative radiographs, and for this reason he recommends it. Others urged

colleagues to adopt intra-operative fluoroscopy both to protect themselves medicolegally and toencourage best practice throughout the profession, but there was considerable opposition to this, notleast because fluoroscopy availability is limited.
Fourteen (41%) surgeons requested post-operative check radiographs within a day of surgery (if nottaken intra-operatively), whereas eleven (32%) did not request radiographs until six weeks post-operatively.
References
1. Choi JH, Zide JR, Coleman SC, Brodsky JW. Prospective study of the treatment of adultprimary hallux valgus with scarf osteotomy and soft tissue realignment. Foot Ankle Int.2013;34:684-690.
2. Trnka HJ, Zettl R, Hungerford M, Muhlbauer M, Ritschl P. Acquired hallux varus and clinicaltolerability. Foot Ankle Int. 1997;18:593-597.
3. Rochwerger A, Curvale G, Groulier P. Application of bone graft to the medial side of the firstmetatarsal head in the treatment of hallux varus. J Bone Joint Surg Am. 1999;81:1730-1735.
4. Johnson KA, Spiegl PV. Extensor hallucis longus transfer for hallux varus deformity. J BoneJoint Surg Am. 1984;66:681-686.
5. Skalley TC, Myerson MS. The operative treatment of acquired hallux varus. Clin Orthop RelatRes. 1994183-191.
6. Myerson MS, Komenda GA. Results of hallux varus correction using an extensor hallucis brevistenodesis. Foot Ankle Int. 1996;17:21-27.
7. Plovanich EJ, Donnenwerth MP, Abicht BP, Borkosky SL, Jacobs PM, Roukis TS. Failure aftersoft-tissue release with tendon transfer for flexible iatrogenic hallux varus: a systematic review.J Foot Ankle Surg. 2012;51:195-197.
8. Holland P, Molloy AP. Intra-operative radiography for scarf osteotomies of the first metatarsal.Bone Joint J. 2013;95-B:21.

Transfer Metatarsalgia after Hallux Valgus Surgery
Transfer metatarsalgia can be defined as forefoot pain caused by dysfunction in another forefoot area1.It occurred not uncommonly after older first metatarsal osteotomies like the Wilson and the Mitchellosteotomies, with rates quoted at 11-20% 2-4. It is commoner in the Greek foot type. Incidence withmodern surgery is unknown.
Virtually all first metatarsal osteotomies cause some shortening and may also inadvertently elevate thefirst metatarsal head. This prevents normal loading of the first ray during the second and third rockersof gait, transferring more load to the lesser metatarsal heads. “Too much” shortening has beendefined5 as 4mm or a ratio6 of lengths of first and second metatarsal of less than 0.825.
When the load transfer is minimal the patient can adapt her gait and activities, but when severe, ittends to progress, with callus formation and plantar plate rupture, and may co-exist with recurrenthallux valgus or first MTP arthrosis. In this situation the normal forefoot mechanics need to berestored.
Careful examination can detect these signs as well as an elevated or short first metatarsal, and candistinguish between second rocker metatarsalgia, with callus directly under the metatarsal heads, andthird, where the callus is more distal. These indicate that the problem is elevation or shortening of thefirst metatarsal, respectively. More patients experience pain in the third than in the second rocker –perhaps because, in third rocker, the load is not shared with any other part of the foot. The position ofthe sesamoids may also have a role in proper loading of the first metatarsal.
Gastrocnemius tightness has been implicated by many researchers in metatarsalgia7,8 and should beincluded in the assessment.
Radiological assessment starts with weight bearing DP and lateral radiographs and an oblique. Thestate of the joints is assessed, previous surgery noted and particular attention paid to the degree ofshortening and elevation of the first metatarsal. Computed tomography, particularly weight bearing ifavailable, shows the relative height of different metatarsals very precisely. If this is not available askyline view of the forefoot is occasionally a very useful tool [scribe's addition].
Within the umbrella of non-operative management, padding around the prominent metatarsals hasgood evidence, and adding a rocker to the shoe can offload the forefoot9. Stretching thegastrocnemius-soleus complex to reduce the relative pressure through the forefoot also has goodevidence10.
Although load transfer to the forefoot is very complex when looked at with finite element analysis,surgical treatment aims to restore particularly the first metatarsal’s role in taking more than one thirdof the body weight during stance phase. Maestro proposed his metatarsal parabola11, a description ofthe ideal relative lengths of the metatarsals, which, although not a perfect model, is as good a guide asany in terms of length, as long as relative elevation or depression of the metatarsal heads is alsoconsidered.
Lengthening of the first ray can be achieved with an osteotomy if for recurrent hallux valgus, or withbone block arthrodesis for first MTP arthrosis. For pure elevation, Caminear12 described an openingwedge plantar flexion osteotomy of the first ray. First MTP Replacement is a controversial way toachieve lengthening and probably not to be recommended in a complex revision situation.Alternatively the ideal metatarsal parabola can be achieved by shortening one or more lesser rays withosteotomies as described by Weil, Helal, Maceira or percutaneous distal metatarsal minimally
invasive osteotomy (DMMO) but each have their problems with stiff or floating toes, transfer pain toother rays, and delayed union (see later section on lesser metatarsals).
While post-operative metatarsalgia is usually a biomechanical problem requiring surgical correction,other causes of post-operative metatarsalgia should always be considered including non-union,infection, nerve injury, CRPS, hallux varus, and avascular necrosis of the first metatarsal head. Beforeembarking on complex surgery to correct the biomechanics, non-surgical exacerbating factors shouldbe considered - over-training in the athlete, excessive weight, poor shoe choice and forefoot fatatrophy – and caution should be taken in counselling these patients for surgery.
References
1. Illustrated Dictionary of Podiatry and Foot Science. Elsevier Limited; 2009
2. Mitchell CL, Fleming JL, Allen R, Glenney C, Sanford GA. Osteotomy-bunionectomy forhallux valgus. J Bone Joint Surg Am. 1958;40-A:41-58; discussion 59.
3. Wilson JN. Oblique Displacement Osteotomy For Hallux Valgus. J Bone Joint Surg Br.1963;45:552-556.
4. Merkel KD, Katoh Y, Johnson EWJ, Chao EY. Mitchell osteotomy for hallux valgus: long-termfollow-up and gait analysis. Foot Ankle. 1983;3:189-196.
5. Carr CR, Boyd BM. Correctional osteotomy for metatarsus primus varus and hallux valgus. JBone Joint Surg Am. 1968;50:1353-1367.
6. Schemitsch E, Horne G. Wilson’s osteotomy for the treatment of hallux valgus. Clin OrthopRelat Res. 1989221-225.
7. Barouk P. Recurrent metatarsalgia. Foot Ankle Clin. 2014;19:407-424.
8. Aronow MS, Diaz-Doran V, Sullivan RJ, Adams DJ. The effect of triceps surae contractureforce on plantar foot pressure distribution. Foot Ankle Int. 2006;27:43-52.
9. Chang AH, Abu-Faraj ZU, Harris GF, Nery J, Shereff MJ. Multistep measurement of plantarpressure alterations using metatarsal pads. Foot Ankle Int. 1994;15:654-660.
10. Gajdosik RL, Vander Linden DW, McNair PJ et al. Viscoelastic properties of short calf muscle-tendon units of older women: effects of slow and fast passive dorsiflexion stretches in vivo. EurJ Appl Physiol. 2005;95:131-139.
11. Maestro M, Besse JL, Ragusa M, Berthonnaud E. Forefoot morphotype study and planningmethod for forefoot osteotomy. Foot Ankle Clin. 2003;8:695-710.
12. Caminear DS. Role of metatarsus primus elevatus in the pathogenesis of hallux rigidus.[letter].Foot Ankle Int 2000;21(11):967.

Avascular Necrosis of the First Metatarsal Head
Avascular necrosis (AVN) of the first metatarsal is almost always iatrogenic, caused through adisruption of the blood supply.
Sarrafian1 in 1993 described seven variations in the way the dorsalis pedis artery gives rise to theartery of the first web space. It may pass dorsal to the intrinsic muscles, plantar to them or throughthem, for instance. Other authors (including Sherreff2, Resch3, Barouk4, Edwards5) have contributedsince and the consensus in the literature is that the head is supplied mainly by plantar metaphysealbranches from the medial plantar artery and also by somewhat less important dorsal branches, as wellas the nutrient artery of the first metatarsal, which is derived from the dorsalis pedis. The nutrientartery is inevitably separated from the head in any osteotomy, leaving the plantar vessels as the mainblood supply to be respected during the surgical approach. Kumar6 found that specifically the plantar-lateral corner of the metatarsal neck is the predominant site for vascular ingress. Barouk hasemphasised the importance of the plantar metaphyseal artery.
AVN has occasionally been associated with steroid injections and open cheilectomies, but mostnotably with distal metatarsal osteotomies. It has been noted in Silver’s, Mitchell’s, Wilson’s and theChevron osteotomy7-12, with rates of around 20% common historically. Some of these authors raisedthe possibility that it was the combination of a lateral release (damaging the plantar-lateral vessels)with an osteotomy that caused AVN. Kuhn et al13 used a laser Doppler probe intra-operatively, andshowed that either lateral release or Chevron osteotomy alone reduced the flow only minimally, buttogether they reduced it by over 70%. These authors and several others since, however, reported anabsence of AVN during follow up, including Resch3, who randomised patients to a Chevron with orwithout a lateral release. Edwards5 recommended that the osteotomy should exit extra-capsularly andshould have a longer plantar limb, in order to preserve the afore-mentioned plantar metaphysealvessels.
The radiographic diagnosis of AVN can be challenging, given the presence of the sesamoids, post-surgical changes and sometimes incidental degenerative cysts. It also requires serial post-operativeradiographs – a practice which incurs cost and which is therefore implicitly discouraged in somemodern healthcare systems. Initial porosity gives way to sclerosis, then fragmentation and a crescentsign (subchondral fracture), and finally signs of osteoarthritis.
Meier and Kenzora8 classified AVN radiographically as:
Stage 1 : pre collapse
Stage 2 : collapse
Stage 3 : arthritis
Further imaging may include bone scintigraphy, which has high sensitivity but can be difficult tointerpret soon after surgery and so has low specificity; computed tomography to tell of the extent ofbone death; and MRI, which again is sensitive but cannot necessarily differentiate AVN from oedema,fracture, infection, CRPS or even a Charcot process.
If non-operative management with off-loading and so on fails, the surgical options are arthrodesis,replacement or a Keller excision arthroplasty. Arthrodesis effectively treats joint pain and arthrosis,and has good results reported7,14. It is biologically plausible that it also enables re-vascularisation via

the fused phalanx. By contrast, there is no strong case in the literature for replacement after AVN,while a Keller's may be an option for a low demand patient.
Thankfully, in modern UK practice where long limb Chevron and scarf osteotomies predominate,AVN is rare, but surgeons should keep the diagnosis in mind when reviewing a dissatisfied post-operative patient.
References
1. Sarrafian SK. Anatomy of the Foot and Ankle: descriptive, topographic, functional. Lippincott Williams& Wilkins, 1993, pp.375-425.
2. Shereff MJ, Yang QM, Kummer FJ. Extraosseous and intraosseous arterial supply to the first metatarsaland metatarsophalangeal joint. Foot & Ankle Int. 1987;8(2):81-93.
3. Resch S, Stenstrom A, Gustafson T. Circulatory disturbance of the first metatarsal head after Chevronosteotomy as shown by bone scintigraphy. Foot Ankle. 1992;13:137-142.
4. Barouk LS. Scarf osteotomy for hallux valgus correction. Local anatomy, surgical technique, andcombination with other forefoot procedures. Foot Ankle Clin. 2000;5:525-558.
5. Edwards WH. Avascular necrosis of the first metatarsal head. Foot Ankle Clin. 2005;10:117-127.
6. Malal JJG, Shaw-Dunn J, Kumar CS. Blood supply to the first metatarsal head and vessels at risk with achevron osteotomy. JBJS (Am). 2007;89:2018-2022.
7. Brodsky JW, Ptaszek AJ, Morris SG. Salvage first MTP arthrodesis utilizing ICBG: clinical evaluationand outcome. Foot Ankle Int. 2000;21:290-296.
8. Meier PJ, Kenzora JE. The risks and benefits of distal first metatarsal osteotomies. Foot Ankle. 1985;6:7-17.
9. Courtman NH, Weighill FJ. Distal first metatarsal osteotomy and adductor release as a treatment of halluxvalgus. J R Coll Surg Edinb. 1995;40:133-135.
10. Peterson DA, Zilberfarb JL, Greene MA, Colgrove RC. Avascular necrosis of the first metatarsal head:incidence in distal osteotomy combined with lateral soft tissue release. Foot Ankle Int. 1994;15:59-63.
11. Thomas RL, Espinosa FJ, Richardson EG. Radiographic changes in the first metatarsal head after distalchevron osteotomy combined with lateral release through a plantar approach. Foot Ankle Int.1994;15:285-292.
12. Johnston K, Cracchiolo A. The effect of chevron osteotomy with lateral capsular release on the bloodsupply to the first metatarsal head. JBJS (Am) 1995;77-A,2:197
13. Kuhn MA, Lippert FG, Phipps MJ, Williams C. Blood flow to the metatarsal head after chevronbunionectomy. Foot Ankle Int. 2005;26:526-529.
14. Brosky TA, Menke CR, Xenos D. Reconstruction of the first metatarsophalangeal joint following post-cheilectomy avascular necrosis of the first metatarsal head: a case report. J Foot Ankle Surg. 2009;48:61-69.
Failed Cheilectomy
Cheilectomy for hallux rigidus can be said to have failed if pain persists and/or dorsiflexion remainslimited. In the speaker's experience most failures are avoidable by careful patient selection. In asystematic review, failure occurred in just under 10% of cheilectomies1, and most of these wererevised to first MTP fusion. However, before automatically offering fusion, surgeons should considercauses of failure other than painful arthrosis.
In selecting patients for cheilectomy, surgeons should perform the “grind test” (axial compressioncombined with a twisting motion) and an impingement test, with the foot loaded, the first metatarsalheld down and the toe dorsiflexed up to end range. These tests are equally usefully in a patient with afailed cheilectomy. Clinical examination may indeed point to painful arthrosis as the cause, but mayalso detect ongoing impingement, suggesting inadequate cheilectomy; or signs of infection, nerveinjury or complex regional pain syndrome.
Depending on the cause, the surgeon may suggest footwear modification (a more roomy toebox, aforefoot rocker in the sole) and the patient may or may not accept it. A steroid injection may sootheresidual synovitis, which may be indicated by a soft block to dorsiflexion on impingement testing.Revision cheilectomy may be warranted if pain returns after injection, the grind test is negative, andmost of the joint is preserved on radiographs. The speaker performs minimally invasive revisioncheilectomy with a low speed burr, accompanied by an arthroscopy of the joint which allowsinspection and treatment of the joint surfaces. Some would advocate adding a dorsiflexion osteotomy(e.g. BonneyMcNab also called Moberg osteotomy) of the proximal phalanx, particularly if intra-operative dorsiflexion is still less than 70 degrees after the cheilectomy2,3.
For continuing painful arthrosis, fusion would probably be regarded as the “gold standard”, butalternatives are a Keller arthroplasty, joint replacement or interposition arthroplasty. Jointreplacements are attractive to patients and surgeons alike but, when they fail they leave a large bonedefect which is a considerable reconstructive challenge. Nevertheless one may considerhemiarthoplasty with a metal component which appears to be robust for several years4. In the olderpatient (eg over 60) the more familiar silastic replacement gives good results in most5. The Kellerprocedure (partial excision of the proximal phalanx) was ubiquitous a generation ago but is rarelydone now. It may still be performed for hallux rigidus, with good results reported6. It has theadvantage that there is no metalwork that can fail, loosen or get infected, and no bony union orosseous integration is expected, so it may be suited to a low demand patient who cannot tolerate therecovery period after arthrodesis or joint replacement. Interpositional arthroplasty is a variant of theKeller procedure and also has been reported7..
In summary, where cheilectomy is deemed to have failed, the surgeon should take a few minutes toconsider the possible reasons and to address them in treatment, although in practice, a fusion willusually be the revision procedure of choice.
Discussion
The discussion centred on patient selection for cheilectomy, which many felt was the primaryinfluence on the success rate of the procedure. Mr Bendall reiterated that the decision to do a

cheilectomy is best made on clinical grounds rather than on radiographs. He would guide a patientwith no joint space towards a fusion, but would leave the choice of cheilectomy open to them ifimpingement were the dominant problem. On the other hand, Mr Robinson pointed out that patientchoice does not guarantee patient satisfaction.
While a minority of those present would add a dorsiflexion osteotomy, Mr Stephens pointed out thatthe patient most likely to benefit is the sportsperson who relies on the third rocker. Mr Williamsondecompresses the first MTP joint with a shortening Chevron first metatarsal osteotomy, and finds thishelps restore a useful range of movement.
Consensus66% of those present offer a simple, open cheilectomy on a suitable patient.18% offer minimally invasive cheilectomy.9% sometimes add a Moberg or Akin osteotomy.3% sometimes add a first metatarsal osteotomy.3% do not offer cheilectomy.None of those present routinely add an osteotomy to a cheilectomy.
References
1. Roukis TS. The need for surgical revision after isolated cheilectomy for hallux rigidus: asystematic review. The Journal of Foot and Ankle Surgery. 2010;49:465-470.
2. Citron N, Neil M. Dorsal wedge osteotomy of the proximal phalanx for hallux rigidus. Long-term results. Journal of Bone & Joint Surgery, British Volume. 1987;69:835-837.
3. Waizy H, Czardybon MA, Stukenborg-Colsman C et al. Mid-and long-term results of the jointpreserving therapy of hallux rigidus. Archives of orthopaedic and trauma surgery.2010;130:165-170.
4. Townley CO, Taranow WS. A metallic hemiarthroplasty resurfacing prosthesis for the halluxmetatarsophalangeal joint. Foot & Ankle International. 1994;15:575-580.
5. Laird L. Silastic joint arthroplasty of the great toe: a review of 228 implants using the double-stemmed implant. Clinical orthopaedics and related research. 1990;255:268-272.
6. Schneider W, Kadnar G, Kranzl A, Knahr K. Long-term results following Keller resectionarthroplasty for hallux rigidus. Foot & Ankle International. 2011;32:933-939.
7. Lau JTC, Daniels TR. Outcomes following cheilectomy and interpositional arthroplasty inhallux rigidus. Foot & Ankle International. 2001;22:462-470.

Non-union / Malunion in first MTP Fusion
Defining non-union has its pitfalls but for present purposes could be defined as definite lack of bonybridging on radiographs or computed tomography, with no radiological progression over a threemonth interval. It may not necessarily be symptomatic. Mal-union again is elusive to define given thatpatients' acceptance of different positions can vary widely and there is no absolute range. However itis generally accepted that the toe is ideally positioned around 25 degrees dorsiflexed compared to themetatarsal (although this depends on the height of the arch) or 10 degrees dorsiflexed compared to thefloor, giving it clearance in second rocker but ensuring contact in third rocker. If dorsiflexedexcessively the toe will rub on shoes and there may be more sesamoid pain. The hallux lies naturallyin 10-15 degrees valgus, parallel with the second toe, although in a fusion it may be desirable to leavea slight gap as the newly stiff hallux will not allow for any accommodation if the lesser toes arecrowded. On the other hand, too straight an angle may lead to interphalangeal joint arthrosis. Finsenshowed “only a weak correlation between position and clinical outcome”1 – probably because thereare so many other factors that affect outcome.
In a systematic review2 of 37 studies and 2818 arthrodeses, there was a 5.4% non-union rate; only athird of them were symptomatic. Mal-union was judged to be present in 6.1%. There are patientrelated factors and surgeon related factors3,4.
Patient factors
Patient factors Pathology RheumatoidRevisionsUse of bone block
Smoking Three times risk of non-union infoot and ankle arthrodeses5
Diabetes Increases time to union and ratesof non-union6,7
Medication NSAIDs – conflicting evidence butprudent to avoidCorticosteroids – slow union inrats
Surgical factors Technique Joint preparationFixation
Post-op protocol Weight-bearingSplintage
Fixation can be with:
A single screw (including intramedullary)
Crossed screws
Parallel screws
Staples
Dorsal Plate: Locked or Non-locking
Dorsal plate and oblique compression screw

Of these, a dorsal plate and lag screw has been shown to be the strongest construct8. However in thesystematic review2, non-union rates were only higher for a single screw:
Single screw: 8.7%
Crossed screws: 4.9%
Parallel screws: 0% (only 22 patients)
Dorsal plate +/- lag screw: 5%
Staples: 5%
Conservative treatment of non-union and mal-union involves altering shoes, adding stiffness or arocker to the sole. As surgical treatment, Saxby showed that removal of metal was a worthwhile andsimple measure, with 66% of patients satisfied after that procedure alone9.
If this fails or is predicted to fail, the non-union should be taken down, the joint re-prepared and fixed,with or without bone graft. If there is bone loss then an iliac crest bone block is the commonestmethod of restoring first ray length and may have an 80% rate of union10.
“Drilling and grafting” is a technique first described by Dennis in 1895 in Philadelphia andpopularized by Böhler in the 1930s11. Mr Rudge presented two cases he has treated with this technique,revising the fixation only if necessary. Fluoroscopically guided drilling across the non-union siteallows insertion of a core of bone harvested from the heel into the drill hole. In both cases thisappeared to foster solid union by three to four months. The technique avoids fully opening andrevising the joint, and so may be useful in selected cases where there is non-union but the position andfixation are acceptable.
Discussion
All surgeons present performed first MTP fusions routinely.
There was unanimous consensus that intra-operative simulated weight bearing is mandatory whenpositioning the hallux for a fusion.
0% use a solitary screw for fixation
17 (50%) use two screws, crossed or parallel
1 (3%) use a compression screw with a non-locked plate
12 (35%) use a compression screw with a locked plate
0% would use a dorsal plate alone as it was felt that this leads to a plantar gap and higher non-union.
There was lively debate as to whether two screws or a screw and plate provided better fixation, withno consensus.

References
1. Aas M, Johnsen TM, Finsen V. Arthrodesis of the first metatarsophalangeal joint for halluxrigidus—optimal position of fusion. The Foot. 2008;18:131-135.
2. Roukis TS. Nonunion after arthrodesis of the first metatarsal-phalangeal joint: a systematicreview. The Journal of Foot and Ankle Surgery. 2011;50:710-713.
3. Thevendran G, Younger A, Pinney S. Current Concepts Review: Risk Factors for Nonunions inFoot and Ankle Arthrodeses. Foot & Ankle International. 2012;33:1031-1040.2.
4. Gaston MS, Simpson AHRW. Inhibition of fracture healing. Journal of Bone & Joint Surgery,British Volume. 2007;89:1553-1560.
5. Cobb TK, Gabrielsen TA, Campbell DC, Wallrichs SL, Ilstrup DM. Cigarette smoking andnonunion after ankle arthrodesis. Foot & Ankle International. 1994;15:64-68.
6. Perlman MH, Thordarson DB. Ankle fusion in a high risk population: an assessment ofnonunion risk factors. Foot & ankle international. 1999;20:491-496.
7. Loder RT. The influence of diabetes mellitus on the healing of closed fractures. Clinicalorthopaedics and related research. 1988;232:210-216.
8. Politi J, Hayes J, Njus G, Bennett GL, Kay DB. First metatarsal-phalangeal joint arthrodesis: abiomechanical assessment of stability. Foot & ankle international. 2003;24:332-337.
9. Hope M, Savva N, Whitehouse S, Elliot R, Saxby TS. Is it necessary to re-fuse a non-union of ahallux metatarsophalangeal joint arthrodesis? Foot & Ankle International. 2010;31:662-669.
10. Myerson MS, Schon LC, McGuigan FX, Oznur A. Result of arthrodesis of the halluxmetatarsophalangeal joint using bone graft for restoration of length. Foot & Ankle International.2000;21:297-306.
11. Bohler, Lorenz : Pseudoarthrosen bekandlung mit der Beck'schen Bohrung.Zentralbl. f. Chir., 57, I654, 1930.

Revision of the failed MTP implant and failed Keller's
MTP arthoplasty may fail due to pain, infection, wear, loosening, fracture and transfer pain and otherbiomechanical disturbances. As well as history, examination, radiographs and CRP, computedtomography, magnetic resonance imaging or bone scan can all give useful information. In approachingthis challenge, the principal aims of treatment are to:
Improve pain
Improve mobility
Stop bone destruction
Stop soft tissue destruction
Clear infection
Restore foot mechanics
Preserve motion if possible
Implant removal and resection arthroplasty was investigated by Kitaoka1. Ten failed Silastics wereremoved at an average of 3.1yrs. The results were excellent in seven patients, good in one, fair in oneand poor in one. The main problems in the latter were Hallux Elevatus and Transfer Metatarsalgia. Soa Keller's procedure is a very reasonable salvage operation.
With interposition arthroplasty, the implant is removed, synovectomy performed and soft tissueinserted in the joint as “anchovy interposition”. Suitable grafts include EHB tendon, plantaris,hamstring or joint capsule. A similar idea using the “Graft Jacket” as a spacer yielded a good result inone case, where the whole proximal phalanx had been eroded2. However, it is difficult to see how any

of these procedures re-function the first ray, given that they take away length and de-tension theextrinsic tendons.
Re-Implantation was investigated by Hariharan3 in 2004. Silastics were removed and the MOJEimplanted in seven feet. At 18 months' follow up their AOFAS scores were acceptable and theprocedure was deemed safe. Koenig4 similarly removed silastic implants and implanted the BiometTotal Toe replacement with good results at 12 months in nine out of ten patients. Both these studieshave short follow up times.
Iliac Crest Bone Graft Arthrodesis was investigated as a technique by Brodsky5 in 2000. Twelvepatients underwent the surgery, eight for a failed MTPJ Implant. Eleven of twelve achieved union atan average of fifteen weeks, and were not pain-free but were said to have minimal pain. Patients wereliving independently but not able to indulge in sport. Transfer pain was relieved. There were threemajor complications: two with skin necrosis (presumably due to tension) and one with non-union anda broken plate.
For the salvage of the painful Keller's arthroplasty, Coughlin and Mann6 performed 16 arthrodeses ofthe 1st MTP joint, four with intercalary bone graft. They report a 100% union rate, good relief oftransfer pain, and all patients satisfied. In another study7, this approach was contrasted with repeatKeller's arthroplasty, Z lengthening of EHL, capsular reefing and excision of the sesamoids: thefusions did relatively well with 13/29 excellent and 5/29 poor results, compared to 11/21 poor and noexcellent results in the repeat Keller's group.
Therefore a pragmatic approach is suggested for failed first MTP arthroplasty. Any implant is removedand if infection is suspected or confirmed, reconstruction is delayed, with the option of insertingtemporary antibiotic-loaded beads. In order to re-function the first ray for comfortable load bearing, itmust be made longer and more plantar, for which intercalary bone graft fusion is ideal, using iliaccrest tricortical graft. This is technically challenging, in achieving good toe alignment, matching thegraft to the bony cuts, filling defects, balancing the need for length with the tension that soft tissuescan tolerate, and balancing the lesser rays. If the patient's demands are low then simple removal,synovectomy and Keller's procedure is a reasonable option.
Discussion
Two surgeons had used allograft iliac crest with similar results to autograft. On fixation of the iliaccrest graft, many surgeons do not fix it at all, since it is difficult and there is naturally compression.Some surgeons fashion the graft into a dowel which fits inside the phalanx and the metatarsal. Othersuse a single compression screw across the whole construct because there is frequently delayed or non-union of the distal bone-graft interface, the literature notwithstanding.
It was pointed out that the interphalangeal joint may be stiff and painful in some of these patientswhich complicates their treatment. The rotation of the toe must be such that this joint is well aligned inthe sagittal plane, and the distal phalanx must clear the ground in stance but allow contact during thethird rocker. If painful enough it can be fused with the obvious disadvantage of a totally stiff hallux.
Of the 34 surgeons present, 20 (59%) do not perform any kind of first MTP replacement. Of the 14who do, nine insert Silastic implants, six perform hemi-arthroplasties (with some overlap betweengroups) and two perform total MTP replacement. No-one present would use a ceramic implant.

References
1. Kitaoka HB, Holiday AD, Chao EYS, Cahalan TD. Salvage of Failed First MetatarsophalangealJoint Implant Arthroplasty by Implant Removal and Synovectomy: Clinical and BiomechanicalEvaluation*. Foot & Ankle International. 1992;13:243-250.
2. Khoury WE, Fahim R, Sciulli JM, Ehredt Jr DJ. Management of Failed and Infected FirstMetatarsophalangeal Joint Implant Arthroplasty by Reconstruction with an Acellular DermalMatrix: A Case Report. The Journal of Foot and Ankle Surgery. 2012;51:669-674.
3. Sloan A, Ramaswamy R, Hariharan K. Revision arthroplasty for failed first metatarsophalangealjoint arthroplasties with ceramic arthroplasty and impaction bone grafting. Foot and anklesurgery. 2004;10:23-27.
4. Koenig RD. Revision arthroplasty utilizing the Biomet Total Toe System for failed siliconeelastomer implants. The Journal of foot and ankle surgery: official publication of the AmericanCollege of Foot and Ankle Surgeons. 1993;33:222-227.
5. Brodsky JW, Ptaszek AJ, Morris SG. Salvage first MTP arthrodesis utilizing ICBG: clinicalevaluation and outcome. Foot & Ankle International. 2000;21:290-296.
6. Coughlin MJ, Mann RA. Arthrodesis of the first metatarsophalangeal joint as salvage for thefailed Keller procedure. J Bone Joint Surg Am. 1987;69:68-75.
7. Machacek FJ, Easley ME, Gruber F, Ritschl P, Trnka HJ. Salvage of a failed Keller resectionarthroplasty. J Bone Joint Surg Am. 2004;86-A:1131-1138.

Floating Toe
A floating toe is a lesser toe that sits off the ground after a metatarsal shortening osteotomy (MSO)such as Weil's, Helal's, Maceira or distal minimally-invasive metatarsal osteotomy (DMMO). It is adifficult problem to manage.
There are various hypotheses explaining floating toes. Trnka et al1 proposed that shortening changesthe action of the lumbricals and interossei from flexors to extensors. Dampening of the windlassmechanism was proposed by Perez et al2. Additional factors in floating toe are thought to be thepresence of a plantar plate tear, the type of osteotomy that was performed, whether a PIPJ arthrodesiswas required as well (makes floating toe more likely) and how the toe was splinted post-operatively.
To combat excessive shortening one could aim for less than 3mm shortening of Weil's osteotomies,double-cutting to focus on elevation rather than shortening; or one could use a Maceira cut, which hasalso been called a triple cut Weil osteotomy.
Floating toes are common, with Highlander et al.3 reporting a 36% rate in 1131 cases. Hofstaetter etal.4 reported a 68% rate in 25 cases with seven year follow up.
To prevent a floating toe after a MSO, something must hold the toe down at the MTP joint. A K-wireacross the flexed joint will provide reliable splintage for a few weeks. Plantar plate repair oradvancement may be tried, or flexor to extensor transfer (effectively converting FDB tendon into aflexor of the MTPJ, like the intrinsic muscles)5. A similar concept is FDB transfer to the proximalphalanx6. Chalayan et al5 performed a biomechanical study on cadavers, testing resistance todorsiflexion and dorsal subluxation of the toe. They found that flexor to extensor transfer added toMTPJ stability following Weil osteotomy. If the plantar plate was disrupted, Weil osteotomy left thejoint very unstable.
There is debate about whether the plantar plate should be repaired if torn, should be advanced in allcases or never repaired at all. It is recognised that there is an increased incidence of floating with PIPJarthrodesis, which may relate to K-wires over-straightening; a good reason to consider a PIP fusionimplant. On the other hand, if a K-wire is used and driven across the MTP joint as well, the joint maybe protected from subluxation long term. Alternatively a blocking K wire can be used dorsal to the toewithout transfixing it.
Intuitively, post-operative splinting (or lack of it) would also affect outcome. A recent study of 30patients demonstrated that a special splint (made by Darco) resulted in 0 cases of floating toe, butwithout the length of follow up of the older studies7.
There is little in the literature about treating floating toes. A flexor to extensor transfer or plantar plateadvancement may be tried but at the expense of stiffness, which is inevitable8. Ideally floating toes areprevented, as above, by avoiding excessive shortening, considering flexor to extensor transfer ifshortening more than 3mm, considering plantar plate advancement if that pathology is suspected, andaggressive post-operative splinting and manipulation.
Discussion and consensus
All present sometimes use Weil osteotomies except one surgeon who uses Maceira osteotomies. 23out of 34 surgeons (68%) sometimes perform double cut Weil osteotomies to avoid plantarising thelesser metatarsal head, while one surgeon performs a double cut to prevent floating toe.
There was agreement that post-operative dressing or taping is important to prevent the toe from rising.The dorsal scar may otherwise contract and contribute to floating.
Thirteen out of 34 surgeons (38%) were performing plantar plate repairs, but of these thirteen, elevenexpressed dissatisfaction with the procedure, illustrating that this is not a settled question. Tighteningand stiffening of the MTP joint were concerns for several surgeons as they felt that patients preferfloppy to stiff toes. There was also disagreement about the reliability of translational pain or the “miniLachmann test” of the toe as a diagnostic test for plantar plate pathology.
It was proposed that a floating toe may arise when only one ray is shortened and the others left behind,de-tensioning the soft tissues of the operated toe alone as the tendons of FDL are bound to each otheras well as to FHL at the knot of Henry. A solitary Weil osteotomy may also risk transfer pain on to theadjacent ray; three surgeons (9%) as a rule therefore tended not to do solitary Weil osteotomies,whereas the rest would sometimes do them. Some surgeons found that soft tissue releases around theMTPJ were usually enough to bring down a hyperextended toe, without having to shorten themetatarsal as well. Others favoured a Stainsby procedure with generous resection of most of theproximal phalanx to treat both PIP and MTP deformity at once.
It was generally acknowledged that distal metatarsal osteotomies are difficult technically, particularlywhen judging how much to take off in a double cut, and care must be taken not to plantar flex thehead. An intra-operative skyline view of the forefoot may help judge the relative height of themetatarsal heads, as well as a dorso-plantar view to judge the metatarsal cascade in the transverseplane.
References1. Trnka HJ, Nyska M, Parks BG, Myerson MS. Dorsiflexion contracture after the Weil
osteotomy: results of cadaver study and three-dimensional analysis. Foot Ankle Int. 2001;22:47-50.
2. Perez HR, Reber LK, Christensen JC. The role of passive plantar flexion in floating toesfollowing Weil osteotomy. J Foot Ankle Surg. 2008;47:520-526.
3. Highlander P, VonHerbulis E, Gonzalez A, Britt J, Buchman J. Complications of the Weilosteotomy. Foot Ankle Spec. 2011;4:165-170.
4. Hofstaetter SG, Hofstaetter JG, Petroutsas JA, Gruber F, Ritschl P, Trnka HJ. The Weilosteotomy: a seven-year follow-up. J Bone Joint Surg Br. 2005;87:1507-1511.
5. Chalayon O, Chertman C, Guss AD, Saltzman CL, Nickisch F, Bachus KN. Role of plantarplate and surgical reconstruction techniques on static stability of lesser metatarsophalangealjoints: a biomechanical study. Foot Ankle Int. 2013;34:1436-1442.
6. Lee LC, Charlton TP, Thordarson DB. Flexor digitorum brevis transfer for floating toeprevention after Weil osteotomy: a cadaveric study. Foot Ankle Int. 2013;34:1724-1728.
7. Godoy-Santos AL, Diniz Fernandes T, Luzo C, Ortiz RT, Sakaki M, Weil LJ. Effectiveness ofthe Dorsal Thermoplastic Locking Orthosis to Prevent Floating Toes in Postoperative Follow-upof Weil Osteotomies: Pilot Study. Foot Ankle Spec. 2014;7:356-362.
8. Myerson MS, Jung HG. The role of toe flexor-to-extensor transfer in correctingmetatarsophalangeal joint instability of the second toe. Foot Ankle Int. 2005;26:675-679.

Floppy or Short Toes After Surgery
Coughlin wrote that a floppy or flail toe is “one of the most difficult complications”. It is an iatrogeniccondition in which the digit lacks structural stability. It is usually a result of excessive resection of thedistal aspect of the proximal phalanx during correction of a claw or hammer toe deformity. It is not thesame as a floating toe where the toe fails to purchase the ground1,
The patient may complain of poor cosmesis, toes that press on the toe box of the shoe, weakness oflesser toe push off in 3rd rocker, and awkwardness putting on socks. Clinically the toe is hypermobileand in particular hyper-extensible.
Floppy toes could be classified according to whether too much bone was taken (hard) or tendonsreleased too keenly (soft), as follows:
Hard – Type 1, after hammer toe correction with aggressive resection of the distal end of theproximal phalanx
Hard – Type 2, excessive resection of the metatarsal head
Soft – overzealous release of EDB and EDL.
Like all iatrogenic problems, the best treatment Is prevention. Conservative measures would includeshoes with a wide, high toe box. Surgical repair options include;
Revision PIP fusion with structural bone graft
Revision fusion with an implant.
Syndactylization.
V-Y Plasty.
Amputation.
Revision PIP fusion with an implant may be suitable for “Hard Type 1” floppy toes but the patientmay well need new bone stock. A retrospective review of 22 flail toes in 13 patients reported an 82 %success rate, performing one-stage digital lengthening with autologous bone from the ipsilateralcalcaneus2.
An over shortened metatarsal (“Hard Type 2” toe) requires re-balancing of the metatarsal cascade,with shortening osteotomies to the other metatarsals.
Syndactylization is an established treatment for congenital crossed toes3 but not for flail toe. It is, intheory, a reasonable, if drastic, solution for any of the types of floppy toe.
Soft Tissue V-Y plasty involves soft tissue release and a skin procedure, with or without resection ofpart of the metatarsal head. There are case series but it does not address the shortening or instability ofthe toe4,5.
If there is lack of EDB and EDL (“Soft” type floppy toe), adhesiolysis, Z shortening or free EDB graftcould be considered, but there are no published case series of these technique.
Amputation of the toe is a salvage technique for both hard & soft types with which every surgeon willbe familiar, and yet case series for this procedure have not been published. Cosmesis is obviouslyaffected and there is a risk of hallux valgus after second toe amputation, so this option tends to bereserved for the elderly, or for those who do not want complicated surgery with a prolonged recovery.
In summary, flail toes should be avoided by resecting bone judiciously and taking care whenlengthening the extensor tendons. For surgical revision of “Hard Type 1” flail toe, what little literatureexists supports PIP fusion with block bone graft; for “Hard Type 2” we should restore the metatarsalcascade, and for “Soft” flail toe there is no established solution, but soft tissue correction mayreasonably be attempted. Salvage options are syndactylization or amputation of the toe.

References
1. McGlamry ED. Floating toe syndrome. J Am Podiatry Assoc. 1982;72:561-568.
2. Mahan KT, Downey MS, Weinfeld GD. Autogenous bone graft interpositional arthrodesis forthe correction of flail toe. A retrospective analysis of 22 procedures. J Am Podiatr Med Assoc.2003;93:167-173.
3. Rao GS, James JH. Artificial syndactylisation for congenital crossed toes. Br J Plast Surg.1987;40:502-504.
4. Friend G. Correction of iatrogenic floating toe following resection of the base of the proximalphalanx. Clin Podiatr Med Surg. 1986;3:57-64.
5. Pichney GA, Derner R, Lauf E. Digital “V” arthrodesis. J Foot Ankle Surg. 1993;32:473-479.

Non-union, malunion and avascular necrosis after Weil or Distal Minimally invasiveMetatarsal Osteotomies
Non-union and AVN after Weil osteotomy are extremely rare – the author having only ever seen twonon-unions. Only four delegates had encountered AVN and there are only a few cases in the literature1.Non-union used to be common with the more proximal Helal osteotomies, which frequently requiredplaster immobilisation and sometimes plating. The problems with Weil osteotomies are in planningwhich “normal” rays to operate on as demanded by some of the philosophies in forefootreconstruction; how to correct varus and valgus toes (moving the head into the concavity of thedeformity does not always work); avoiding stiff or floating toes; and avoiding causing malunion andtransfer pain by inadvertently moving the metatarsal head plantar-wards.
Consensus:
DMMO's are not yet mainstream (only four of 34 delegates perform them).
Avoiding malunion is about good technique (keeping the saw blade parallel to the sole), doing adouble cut, particularly on the lateral rays, checking fluoroscopic images on the table, and feeling thefoot for prominence of the metatarsals on the table. The last is a cost-free form of pedobarography.
Consensus:
Seventeen surgeons (50%) always X ray Weil osteotomies intra-operatively; seven (21%) sometimesdo and eight (24%) never do.
To avoid stiffness, a more extensive decompression and patient led toe exercises both help. For mostpatients, physiotherapy may not be any better than the surgeon teaching the exercises, but it can beuseful in reluctant patients. Patients should be warned that If stiffness does settle, it is oftenworthwhile removing the screws and adding a synovectomy and adhesiolysis at 6 to 12 months.
Accepting then that Weil osteotomies are not without potential problems, one alternative is theaforementioned Helal osteotomy. Trnka in 19962f reported 61% excellent or good results, but 22%had transfer lesions, 5% non-unions and 10% delayed unions. Winson et al3 studied 124 feet in 93patients who had undergone a sliding Helal metatarsal osteotomy at an average of 3.4 years. 19% hadpoor results and 14% had required a revision procedure. 40% had symptomatic plantar callosities.Poor results were associated with age >65, the addition of first and fifth metatarsal osteotomies, andthe use of plaster immobilization. A fixed claw toe was a common sequela of the surgery. By contrastDavies et al4 reviewed their series of what were essentially Weil's in 47 feet and found 77% pain freeat around a year, with only one union delayed beyond 6 weeks. They felt stiffness was not a problemwith aggressive physiotherapy.
Trnka in 19995 directly compared Helal and Weil osteotomies and found the latter had higher patientsatisfaction; less recurrent metatarsalgia (0 vs 27%), fewer transfer lesions (0 vs 41%), fewer nonunions (0 vs 5) and fewer pseudarthroses (0 vs 3). At 7 years follow up after Weil's, Hofstaetter andTrnka6 found 88% excellent or good results, but 12% had redislocated and were “floating”. Theyassociated failure with inadequate shortening.
A DMMO is essentially a percutaneous, quick osteotomy, generally performed with a burr and notfixed with metalwork, and is distal to where Helal's were performed. Being in metaphyseal bone theygenerally unite. In a comparison of 39 DMMO and 33 Weil7, there was little difference except that theDMMO group recovered slightly slower and had more oedema, and possibly more delayed union.There was no significant difference in rates of stiffness, union, radiological “recoil”, and transferlesions. So there may be little to choose between the two methods.
In summary, at the moment Weil's osteotomies appear to be as good a solution as any for lesser MTPJproblems. The speaker advocates being aggressive with the degree of shortening and number of raysshortened, using a double cut often, and always with the 4th and 5th rays, and being ready to removemetalwork and release the dorsal scarring for cases of stiffness.
References
1. Bayliss NC, Klenerman L. Avascular necrosis of lesser metatarsal heads following forefootsurgery. Foot Ankle. 1989;10:124-128.
2. Trnka HJ, Kabon B, Zettl R, Kaider A, Salzer M, Ritschl P. Helal metatarsal osteotomy for thetreatment of metatarsalgia: a critical analysis of results. Orthopedics. 1996;19:457-461.
3. Winson IG, Rawlinson J, Broughton NS. Treatment of metatarsalgia by sliding distal metatarsalosteotomy. Foot Ankle. 1988;9:2-6.
4. Davies MS, Saxby TS. Metatarsal neck osteotomy with rigid internal fixation for the treatmentof lesser toe metatarsophalangeal joint pathology. Foot Ankle Int. 1999;20:630-635.
5. Trnka HJ, Muhlbauer M, Zettl R, Myerson MS, Ritschl P. Comparison of the results of the Weiland Helal osteotomies for the treatment of metatarsalgia secondary to dislocation of the lessermetatarsophalangeal joints. Foot Ankle Int. 1999;20:72-79.
6. Hofstaetter SG, Hofstaetter JG, Petroutsas JA, Gruber F, Ritschl P, Trnka HJ. The Weilosteotomy: a seven-year follow-up. J Bone Joint Surg Br. 2005;87:1507-1511.
7. Henry J, Besse JL, Fessy MH. Distal osteotomy of the lateral metatarsals: a series of 72 casescomparing the Weil osteotomy and the DMMO percutaneous osteotomy. Orthop TraumatolSurg Res. 2011;97:S57-S65.

Achilles Tendon Rupture
Surgical and conservative management of an Achilles tendon rupture can give equivalent re-rupturerates (1). However there are multiple other endpoints to consider including gastro-soleus function andwound breakdown which can have a considerable impact the final outcome of our treatment.
Consensus on Current practice 2014: Choice of treatment
In the average patient, 50% would obtain an ultrasound to assess if the torn ends appose on plantarflexion. Failure for ends to oppose would be seen as an indication for surgical intervention
Consensus on Current practice 2014: Conservative management
10% Cast only
10% Boot/ splint only
65% cast for 2 weeks then boot/ splint
15% attendees did not vote
Nearly all attendees allow full weightbearing in boot/splint
Consensus on Current practice 2014: How would you treat an active sporty fit and well 40 yr oldpatient who presents day 1?
25% Conservative management
25% No strong feelings
50% Surgical treatment
Current practice 2014: How would you treat an elite athlete presenting on day 1.
95% Surgical treatment
5% Conservative
Current practice 2014: Suture type for repair
65% Absorbable
35% Non-absorbable
Whilst the general consensus was to use an absorbable suture, it was highlighted there are other suturefactors that are important such as whether it is braided or not; not all absorbable sutures are equal. Anabsorbable suture induces an inflammatory reaction but an inert suture material forms a foreign bodythat was felt to be the cause of post-operative complications seen after Achilles surgery. A braidedsuture used in a locking pattern such as the Krackow suture, may get better “grip” of the tendon endswhen compared to a non-locked or monofilament suture.

Current practice 2014: Method of repair
35% Mini-invasive
65% Open
Re-rupture
This can broadly be defined as a recurrent Achilles tendon rupture within 6 months of an adequatelytreated primary rupture. It is thought to occur in between 5-10% of patients and depends on manyfactors including the function/ compliance of the patient and the primary rupture treatment.
There is little evidence in how best to treat these patients although the general consensus was to offera different method treatment and rehabilitation.
Achilles length
Ruptured tendons treated either surgically or conservatively can heal elongated or tight with residualequinus. Usually this is either due to improper tensioning during surgery or over stretching duringrehabilitation.
Other than tibio-talar impingement the Achilles tendon is the main restrictor to ankle dorsiflexion andthus the range of dorsiflexion is a reliable test for Achilles length, when compared to a normal side. Adifference of 10 degrees is thought to be significant.
Lengthened tendon
This often correlates to a poor clinical outcome and patients may complain of gait disturbance withweakness in end-range plantar flexion, during the third rocker. Care should be taken in themanagement of Achilles ruptures to avoid a lengthened tendon. USS may highlight a gap, predictingincreased length once healed, although the effect of this on final function has not been clinicallyquantified. Equally during surgical repair the tendon grasping suture needs to be locked to avoidslipping or stretching during rehabilitation.
The long tendon can be shortened surgically by procedures such as a Z shortening, however whilstsuch may help with the gait disturbance they do not offer a significant improvement in isokineticgastro-soleus strength (2,3).
Shortened tendon
When there is symptomatic shortening surgical lengthening with either a Z lengthening and side toside repair or other technique is a possible solution.
A stiff ankle or lack of dorsiflexion beyond 10 degrees of fixed plantar flexion will overload theforefoot and will affect the second rocker of gait. This may be prevented during surgical treatment bythorough division of adhesions, tying knots away from the rupture side and meticulous epitendonousrepair. Also regular progression from equinus to neutral during functional rehabilitation is essential.

Wound healing
There is little in the literature to highlight how best to manage this difficult complication of surgicalmanagement. Wounds can be a problem after various forms of Achilles surgery, but are commonest(5-10%) after traumatic rupture repair or reconstruction.
Scars around the achilles can be painful and tender or hypertrophic especially in the insertional area.The wound edges can necrose or there can be necrosis of the whole soft tissue covering the Achilles.Infection, when it occurs, can be superficial or deep.
Some of these problems can be avoided by meticulous surgical technique. Thick soft tissue flaps withan incision placed away from the midline can avoid interference with footwear. Others have changedto use percutaneous techniques.
Current practice 2014: Use of percutaneous Achilles repair
60% regularly use an open repair
40% regularly use a percutaneous technique
50% of these use transverse skin incisions
50% of these use longitudinal incisions
However there will be a time that despite good technique a wound infection occurs. Clearly there aremany host factors that are important with diabetics, smokers and those on steroids up to 8X morelikely to get an infection.
Current practice 2014: experience of wound healing problems
50% had experienced wound healing problems in Achilles surgery patients
Infection can be divided into superficial or deep wound problems and may be fungal as well asbacterial. All problematic wounds should undergo microbiological swab for MC+S and fungalscrapings/culture.
Deep infection needs to be treated in conjunction with a plastic surgeon. It may be a case of debridingthe wound and then undergoing a period of “dress & suppress” whilst it granulates. In the case ofrequiring deep and extensive soft tissue debridement any tendon defect should be assessed. This defectmay then require reconstruction with a V-Y plasty, tendon grafting or transfer of peroneus brevis orFHL, as well as a skin graft or fasciocutaneous flap.
Consensus on management of achilles tendon ruptures
Length of treatment >6 weeks Conservative management: Cast for 2 weeks covered by LMWH prophylaxis. Progress into
splint or boot weight bearing immediately. No need for prolonged LMWH Surgical management: Non-midline incision or percutaneous, longitudinal incisions and
debridement of adhesions. Meticulous soft tissue handling. Use of the thickest, braided, bio-absorbable suture available. Kessler or Krackow grasping suture technique, knots away fromrupture, tensioned properly to correct length. Epitendonous repair. Same rehabilitation asconservative.
If too long or too short, then whilst length can be corrected the strength will usually not return.

Patients should be counselled fully for the risks of re-rupture and wound problems
References
1. J Bone Joint Surg Am. 2012;;94(23):2136-43
2. Bohnsack et al Z Orthop Ihre Grenzgeb. 2000 Nov-Dec;138(6):501-5
3. Maffulli et al Int Orthop. 2012 Oct;36(10):2087-93
Persistent Flat Foot after Tibialis Posterior Tendon Surgery
As a flat foot deformity progresses the position of the forefoot in relation to the hindfoot changes. In
the correction of the flat foot it is important to assess and correct each deformity. Failure to achieve
this at the time of surgery may lead to a persistent flat foot deformity, which may or may not be
symptomatic.
Repair of the tibialis posterior tendon is seldom sufficient in isolation and an FDL tendon transfer
needs to be augmented with a boney procedure. At the same time any subtalar deformity needs to be
reduced with a spring ligament reconstruction +/- a further boney procedure. It is this subtalar
reduction that restores the shape of the foot.
Current practice 2014: Surgery in stage II deficiency – spring ligament
95% routinely reconstruct the spring ligament
This then should be augmented by either a medial displacement calcaneal osteotomy or by a lateral
column lengthening and can also be protected with an arthroereisis screw and/ or a gastrocnemius
recession. The choice between these procedures will depend on the surgeon, the extent of midfoot
abduction and the pitch of the calcaneus.
Current practice 2014: Surgery in stage II deficiency – Lateral column lengthening
45% do very rarely
55% have done on occasion
For a calcaneal osteotomy to work it requires a normal pitch of the calcaneus and it has no effect on
the talo-navicular joint, thus the TN joint needs to be normal. When the calcaneal pitch is low a lateral
column lengthening restores foot shape and reduces the TN joint subluxation. In adults there is a 10-

20% risk of non-union with a lateral column lengthening and therefore it is best selected for the
younger adult and the non-smoker. In the older patient or a smoker a subtalar fusion may be more
appropriate. When performed care should be taken to first reduce the ST joint and not just fuse in situ,
as it is the reduction of the subtalar joint that reduces the TN joint.
Current practice 2014: Surgery in stage II deficiency – Arthroereisis screw
10% use to protect reconstruction
Although seldom used amongst those present it was generally felt that this screw holds the reduction
of the subtalar joint, but that it only works in conjunction with other procedures. When used the screw
is often symptomatic and thus routine removal at 6 months following reconstruction is advised.
Current practice 2014: Surgery in stage II deficiency – Gastrocnemius recession
65% perform a recession in the majority of cases
This can be performed in the body of the muscle/ facia or by medial head release. It may be best to
perform this at the start of reconstruction to allow full correction of hindfoot deformity.
Once the hindfoot position has been corrected any midfoot and forefoot correction should be
performed. This is performed where the midfoot break is, whether this is the TN or NC joints.
Consensus on stage II flat foot correction
1. Gastrocnemius recession
2. FDL tendon transfer
3. Spring ligament reconstruction
4. Calcaneal osteotomy or lateral column lengthening
5. Arthroereisis screw by some present

Peroneal Tendon Surgery
In the management of ongoing symptomatic peroneal tendon pathology it is vital to highlight whatyou are trying to treat. There are five main problems that we see:-
Pain Instability Split tears Single complete tear Double tears/ revision
In the presence of painful tendonopathy, injection of LA +/- steroid can both be diagnostic andtherapeutic, although this is not risk free.
Current practice 2014: Injection of peroneal tendon/ sheath
65% are happy to use injections
90% of these are USS guided
20% have seen iatrogenic tendon rupture after injection
10% of those who use injections advise a brace afterwards
An unstable tendon(s) need to be stabilised and this can be achieved by either soft tissuereconstruction or by deepening the peroneal groove. When recurrent, a tendo-achilles graft has beenshown to be beneficial (1).
When the tendon is torn it is vital to highlight whether this is complete or incomplete and whichtendon(s) is/are affected. Incomplete or spit tears tend to be longitudinal and thus can be treated bydecompression/ synovectomy, peroneal tubercle excision and low lying muscle belly resection, even ifrecurrent.
Isolated ruptures of peroneus longus are unusual, but when they do occur the distal stump retractsdeep into the plantar aspect of the foot. In the absence of PL there may be little functional deficit otherthan metatarsus elevatus. In a complete rupture of peroneus brevis the tendon stump is easy to retrieveand should undergo tenodesis to the adjacent PL tendon as long as it is intact.
When both tendons are torn it is more difficult to treat. This can either occur as the primary pathologyor in a single tendon which has undergone a tenodesis in the past. In this situation reconstruction withFHL along with distal stump tenodesis is advised. This then balances the pull of tibialis posterior anddoesn’t tend to require the addition of a split tibialis anterior transfer.
Consensus on persistent problematic peroneal tendons
Pain –USS guided injection Instability – Re-stabilise +/- augment with graft Split tears – Tubularise +/- tenodesis Single complete tear- Tenodesis Double tears/ revision – FHL transfer
Reference
1. FAS:1999 267-270

Failed Lateral Ligament Reconstruction
Consensus was previously reached on surgery for lateral ligament reconstruction in Barcelona 2013.
70% would re-do a modified Brostrom
There are multiple reasons for failure of a stabilisation procedure but they can broadly be grouped into
Genuine repeat injury Missed pathology
Technical failure
A primary modified Brostrom repair has a 80-90% success rate. If after surgery and full rehabilitationthere is symptomatic instability or ongoing pain there may be alternative pathology that is contributingthat also needs to be addressed. Some are very common such as peroneal tendon pathology seen inapproximately 1 in 3 patients with ankle instability and others like lateral process fractures andsubtalar instability are rarer but have similar symptoms and signs to those of ankle instability.Thorough examination and investigation is therefore paramount with XR including stress views, MRIand CT +/- arthrogram where appropriate.
Incidence of other pathology in chronic lateral ankle ligament instability (1):
• Peroneal tendon injury 28%
• Os trigonum 13%
• Lateral gutter ossicles 10%
• Varus 8%
• Anterior osteophytes 3%
• Tarsal coalition 2%
When there is true persistent or recurrent ankle instability after a modified Brostrom procedure andfailed instability rehabilitation then the surgical approach should be:-
Ankle arthroscopy Redo modified Brostrom/ direct repair
+ Anatomical augmentation+/- Extra-anatomical tenodesis with hamstring or synthetic ligament
The choice of material for augmentation varies from autograft or allograft semitendonosis, peroneusbrevis, palmaris longus tendon to synthetic ligaments
Current Practice 2014: Use of autograft for augmentation of redo lateral ligament reconstruction
35% use peroneus brevis attached distally
15% use peroneus brevis not attached
20% use hamstrings
10% use allograft (Mostly USA)

Use of the posterior half of peroneus brevis allows the intact anterior portion to hypertrophy over thefollowing years, reducing the deficit from its harvest.
References
1. Chronic lateral ankle instability & associated conditions: a rationale for treatment. Strauss,Forsberg, Lippert. FAI 2007 Oct;28(10):1041-4.
Failed Treatment of Osteochondral Defects of The Ankle
Management of osteochondral defect of the ankle is dependent on chronicity, size and position on thetalar and tibial surfaces. In contained defects where the fragment cannot be fixed, microfracture orabrasion arthroplasty is seen as the gold standard treatment. This is usually performed arthroscopicallyand when performed adequately can have good initial results in 80% of cases.
Current practice 2014: Ankle microfracture
35% would use abrasion arthoplasty
65% would perform microfracture
60% would perform microfracture with a pick
40% would perform microfracture with a k wire
Current practice 2014: unstable but intact cartilage
10% would debride and microfracture
90% would leave intact
However not everyone will have a good outcome and the majority of patients who have ongoingsymptoms following primary microfracture treatment will have repeat surgery although this is of noproven benefit if the primary surgery has been done adequately. Even in those who do have a goodoutcome, 50% need further surgery in the next 10-15 years (Bristol Group). In those who haveongoing pain the presence of other pathology such as OA, inflammatory arthritis or other intra/ extra-articular causes need to be discussed.
At RNOH Stanmore from 2005-2013 there were 30 patients referred for failed treatment of theirOCD. Within this group there was a male to female ratio of 2:1 and most had undergone 2 previousmicrofracture procedures (range 1-5). They performed ACI/ MACI in 13/30, Hemicap 8/30, Chondron7/30, and CICR in 2/40. At a mean of three years 48% still have pain.
Consensus
Microfracture is gold standard primary treatment with pick or wire In the investigation of these lesions a CT/ CT arthogram in plantar flexion should be
performed. There is no role for MRI or SPECT CT.

Malunion Ankle Fracture and Failed Syndesmosis Repair
Ramsey and Hamilton have described that a 1mm talar shift can lead to a 42% decrease in congruentarea but no proof exists that a 1mm shift leads to post-traumatic arthritis per se. It should also beremembered that talar shift is dynamic not static.
Yablon JBJA 77 – 53 demonstrated that in perfectly fixed bimalleolar fractures, osteoarthritis wasrarely seen at 6 months to 9 years. It was proposed that fibular fixation was the key factor but recentauthors have suggested that the deltoid is akey determinant (Barrie).
Ankle fracture malunion is a preventable disease, with attention to the posterior malleolus, Weber C’s,deltoid instability etc. The most common malunion is a short and externally rotated fibula with talarshift.
In avoiding the problems of ankle malunion and inadequate fixation of the syndesmosis, specialistfoot and ankle surgeons will need to make sure the initial management of these injuries is dealt withwell by their colleagues.
The simple principles, taking no short cuts, are to:
Fix the fibula fracture
Fix the medial side if fractured
Be prepared to hook out the deltoid ligament from the joint if blocking reduction
Fix the syndesmosis if necessary
To clarify this last point, Boden et al1 studied syndesmosis stability in cadavers 25yrs ago, modellingpronation external rotation injuries by dividing the appropriate bones and ligaments. They concludedthat if the deltoid ligament was intact and the medial and lateral fractures repaired, the syndesmosiswill be stable regardless of where the fibular fracture is. If the deltoid ligament was injured and thefibular fracture was under 4.5cm from the ankle joint, fixing the fibula was enough to stabilise thesyndesmosis. Van den Bekerom et al2 tested this hypothesis intra-operatively in 62 patients using the“hook test” and found Boden's criteria had high specificity but low sensitivity and that a hook testsometimes showed syndesmotic instability even in fixed fibular fractures within 4.5cm of the anklejoint.
The concept of fixing the syndesmosis without fixing the fibula has crept in but this can allow non-anatomic healing and a poor clinical outcome. Obeid et al advocate3 leaving “high” fibular fractures inMaisonneuve injuries, fixing the syndesmosis with a percutaneous screw, based on five cases.
Consensus question: how high would you fix?
If a fibular fracture is up to 8cm above the plafond, all delegates wound fix the fracture.
10cm above, 23/34 (68%) would fix the fibula.
With a mid-shaft fracture, 9 (26%) would fix it.
With a fracture two thirds of the way up, none of the delegates would fix it.

Ho et al4 in another cadaveric study show that plating a mid-shaft fibular fracture and fixing thesyndesmosis has a mechanical advantage over syndesmotic fixation alone. The former gave additionalrotational stability to the ankle on cyclical loading.
In a non-randomised clinical study of twelve patients5, Pelton et al compared the approaches taken bytwo different teams. The group that were treated with ORIF of the fibula and two syndesmotic screwshad anatomic or near anatomic reductions; the group that underwent the percutaneous technique hadan unacceptable rate of malunion and diastasis and this technique was abandoned.
In treating failed syndesmotic injury, van den Bekerom, de Leeuw and van Dijk6 advocate fixing if theinjury is under 6 weeks old, reconstructing if under 6 months and fusing the syndesmosis if over 6months. If there is fibular malunion, an osteotomy may be necessary to allow reconstruction or fusionof the syndesmosis.
Discussion
It was pointed out that comminuted fibular fractures may be inadvertently mal-reduced and plated,making subsequent reduction of the syndesmosis impossible. So the two steps should perhaps becombined or perhaps even the order of fixation reversed. Similarly in late reconstruction, the fibularfracture is often malunited, so it should be osteotomised to allow reduction of the joint.
It was again emphasised that the deltoid ligament can be trapped in the joint blocking reduction, inwhich case this must be recognised and the medial side opened and cleared. Repairing the deltoid mayeven add welcome stability.
Discussion about ankle fractures
Should you CT after fixing a Weber C fracture?
Of those who regularly treat fractures, 5/23 (22%) surgeons routinely CT their ownsyndesmosis repairs post operatively.
6/23 (26%) sometimes do a post-operative scan.
12/23 (52%) do not.
Of those who scan, nine out of 11 request both ankles, while two are happy to look at one side only.
Mr Molloy pointed out that while 70% are mal-reduced on CT with a syndesmosis screw in, 80% ofthose self-correct once the screw is removed.
On late syndesmotic reconstruction, there was a question on approaching the 6 week to 6 monthdelayed pt. Van Dijk makes a point of repairing the tibiofibular ligaments as well as using asyndesmotic screw, whereas Mr Kumar finds that clearing out the syndesmosis to enable reductionleaves very little ligament left, so he relies on the screw and, in time, fibrosis.
Mr Clark presented 7 synostoses that he had done with mean 3.5 year follow up. None had anklearthritis but all had some pain; function was acceptable but not normal.
There is a technique attributed to Chris Walker of a distal fibular osteotomy below the syndesmosis –restoring the anatomy of the tibiotalar joint without the difficulties of reducing the chronic diastasis –and the early results of six cases are promising.

Consensus on reconstruction of the syndesmosis
With a splayed, symptomatic syndesmosis, how many surgeons would fuse the syndesmosis at 12months?
1/32 would fuse
15 /32 would always do a soft tissue repair
9 would explore and obtain consent to do either procedure, fusing if unable to clear out thesoft tissue adequately to obtain a reduction.
References
1. Boden SD, Labropoulos PA, McCowin P, Lestini WF, Hurwitz SR. Mechanical considerationsfor the syndesmosis screw. A cadaver study. J Bone Joint Surg Am. 1989;71:1548-1555.
2. van den Bekerom MP, Haverkamp D, Kerkhoffs GM, van Dijk CN. Syndesmotic stabilizationin pronation external rotation ankle fractures. Clin Orthop Relat Res. 2010;468:991-995.
3. Obeid EM, Amr M, Hirst P, Paul AS. Percutaneous fixation of Maisonneuve and Maisonneuve-type fractures: a minimally invasive approach. Injury. 1998;29:619-622.
4. Ho JY, Ren Y, Kelikian A, Aminian A, Charnley I, Zhang LQ. Mid-diaphyseal fibular fractureswith syndesmotic disruption: should we plate the fibula? Foot Ankle Int. 2008;29:587-592.
5. Pelton K, Thordarson DB, Barnwell J. Open versus closed treatment of the fibula inMaissoneuve injuries. Foot Ankle Int. 2010;31:604-608.
6. van den Bekerom MP, de Leeuw PA, van Dijk CN. Delayed operative treatment of syndesmoticinstability. Current concepts review. Injury. 2009;40:1137-1142.
Deltoid Ligament Reconstruction
Experience of the delegates
Not all those present dealt with trauma. Four questions were put to the delegates.
Have you repaired a deltoid ligament acutely following trauma?
25 said yes, 1 no.
Do you do open repair?
All said yes
Have you repaired the deltoid for chronic instability following trauma?
19 yes, 5 no.
Have you dealt with non-traumatic deltoid insufficiency?
10 yes, 9 no.
Anatomy and function
All studies agree that the deltoid is a broad, thick sheet with multiple bands. Most studies agree thatthere is a superficial and deep component. Cadaveric studies disagree on the different bands, showingit is difficult to separate them1-3. Parts include the deep tibiotalar ligaments, the tibionavicularligament and the tibiocalcaneal ligament. It also attaches to the spring ligament. The strongest partsare the anterior and posterior deep tibiotalar ligaments. The (superficial) tibiocalcaneal part is alsoimportant and strong.
The functions are to limit abduction tilt of the talus and to stabilise the ankle in plantarflexion andduring pronation/supination of the rest of the foot. Translation of the talus is limited by bony anatomy,not the deltoid. The deltoid also prevents malrotation of subtalar joint4.
These ligaments necessarily degenerate in Truro stage 4 acquired planovalgus foot. We may soon seethis disease more with an ageing population.
Patterns of injury
Historically deltoid injuries have been treated with neglect as it was felt that the intrinsic stability ofthe ankle would allow full recovery and return of stability. However, Renstrom et al5 found thatbetween 20-40% of ankle injuries presenting for medical care lead to chronic instability and disability.Deltoid injury is seen with syndesmotic injuries and up to 18% of ankle sprains6. Isolated deltoidinjuries are rare and most are associated with fractures.
Chronic insufficiency is seen with posterior tibial tendon dysfunction, triple arthrodesis, and totalankle replacement.
Hintermann7 wrote on the diagnosis and treatment of deltoid insufficiency and classified the tearsanatomically.
Type 1 were avulsed proximally and were the commonest, 72% in his series.
Type 2 are torn within the substance and are the least common, 9%.
Type 3 are distal and made up 19%.
The repair differs depending on the type.
Is this repair necessary acutely? Several studies8-11 in the 1980s and 1990s concluded that it was notimportant to repair the deltoid acutely as long as the mortise is reduced anatomically, the fibula isfixed and the syndesmosis stabilised. Jelinek and Porter, on the other hand, stated that the advantagesof open repair were that the joint was inspected for osteochondral injury, range of motion was saferearlier, and there is more chance of avoiding chronic instability12.
Chronic reconstruction is more challenging. It needs to be combined with realignment of the hindfootif it is to last. Nelson and Younger describe repair of the superficial deltoid combined with naviculo-cuneiform fusion and lateral column lengthening to reconstruct a flat foot13. Deland used PeroneusLongus tendon as a graft to reconstruct deltoid14. However the procedure was difficult and one of thefive cases remained in valgus tilt.
Myerson's group described a minimally invasive deltoid reconstruction for flat foot, combined with atriple fusion, with 3 failures in 8 patients15. Haddad et al16 reconstructed the superficial and deep partsof deltoid using a free tibialis anterior tendon graft in six fresh frozen cadavers. The repair was testedon an Instrom jig and it was found to be strong and effective in vitro. However in the UK tendonallografts are not widely available.
Mr Dhar presented a patient with stage 4 flat foot in whom he had done a medial calcanealdisplacement osteotomy (MCDO), lateral column lengthening, deltoid and spring ligament syntheticrepair and FDL transfer to reconstruct tibialis posterior. After practising it in the cadaveric lab, heobtained a durable and comfortable reconstruction.
In conclusion this is a difficult problem, and the problem of reconstructing deltoid is not yet solved.
References
1. Milner CE, Soames RW. The medial collateral ligaments of the human ankle joint: anatomicalvariations. Foot Ankle Int. 1998;19:289-292.
2. Pankovich AM, Shivaram MS. Anatomical basis of variability in injuries of the medialmalleolus and the deltoid ligament. I. Anatomical studies. Acta Orthop Scand. 1979;50:217-223.
3. Boss AP, Hintermann B. Anatomical study of the medial ankle ligament complex. Foot AnkleInt. 2002;23:547-553.
4. Michelson J, Hamel A, Buczek F, Sharkey N. The effect of ankle injury on subtalar motion.Foot Ankle Int. 2004;25:639-646.
5. Renstrom PA. Persistently Painful Sprained Ankle. J Am Acad Orthop Surg. 1994;2:270-280.
6. Lin CF, Gross ML, Weinhold P. Ankle syndesmosis injuries: anatomy, biomechanics,mechanism of injury, and clinical guidelines for diagnosis and intervention. J Orthop SportsPhys Ther. 2006;36:372-384.
7. Hintermann B. Medial ankle instability. Foot Ankle Clin. 2003;8:723-738.
8. Tourne Y, Charbel A, Picard F, Montbarbon E, Saragaglia D. Surgical treatment of bi- andtrimalleolar ankle fractures: should the medial collateral ligament be sutured or not? J FootAnkle Surg. 1999;38:24-29.
9. Stromsoe K, Hoqevold HE, Skjeldal S, Alho A. The repair of a ruptured deltoid ligament is notnecessary in ankle fractures. J Bone Joint Surg Br. 1995;77:920-921.
10. Harper MC. The deltoid ligament. An evaluation of need for surgical repair. Clin Orthop RelatRes. 1988156-168.
11. Baird RA, Jackson ST. Fractures of the distal part of the fibula with associated disruption of thedeltoid ligament. Treatment without repair of the deltoid ligament. J Bone Joint Surg Am.1987;69:1346-1352.
12. Jelinek JA, Porter DA. Management of unstable ankle fractures and syndesmosis injuries inathletes. Foot Ankle Clin. 2009;14:277-298.
13. Nelson DR, Younger A. Acute posttraumatic planovalgus foot deformity involving hindfootligamentous pathology. Foot Ankle Clin. 2003;8:521-537.
14. Deland JT, de Asla RJ, Segal A. Reconstruction of the chronically failed deltoid ligament: anew technique. Foot Ankle Int. 2004;25:795-799.
15. Jeng CL, Bluman EM, Myerson MS. Minimally invasive deltoid ligament reconstruction forstage IV flatfoot deformity. Foot Ankle Int. 2011;32:21-30.
16. Haddad SL, Dedhia S, Ren Y, Rotstein J, Zhang LQ. Deltoid ligament reconstruction: a noveltechnique with biomechanical analysis. Foot Ankle Int. 2010;31:639-651.
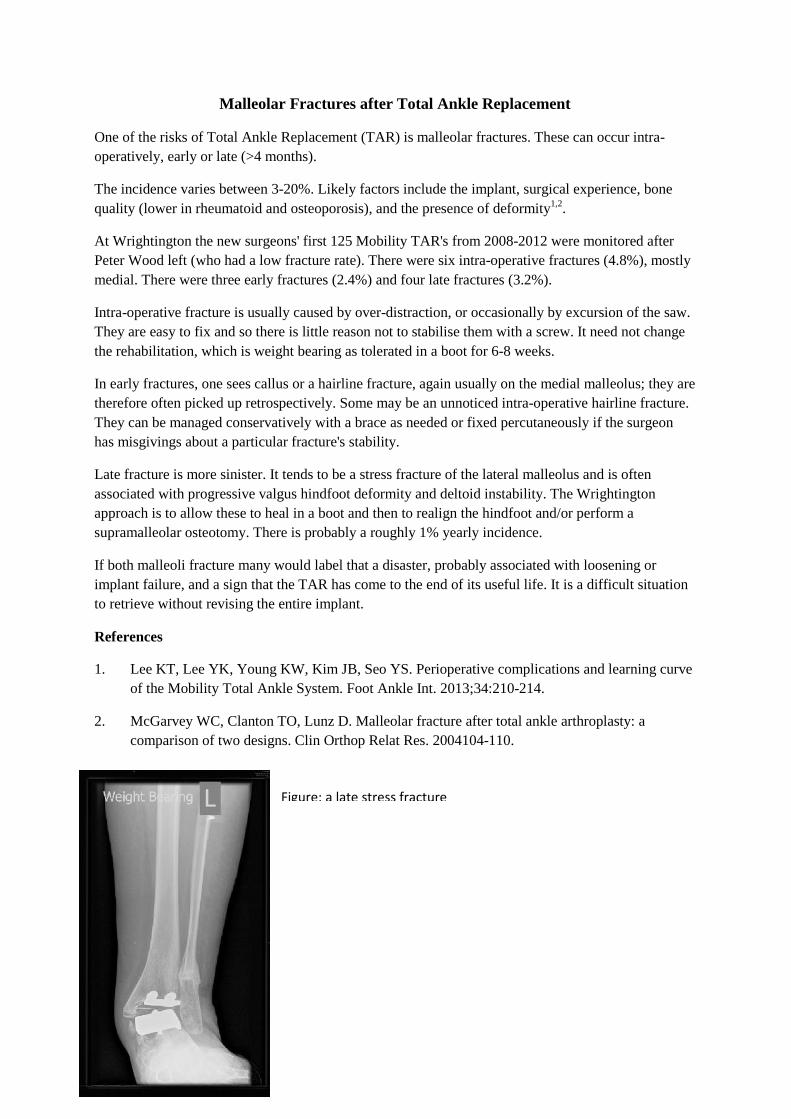
Malleolar Fractures after Total Ankle Replacement
One of the risks of Total Ankle Replacement (TAR) is malleolar fractures. These can occur intra-operatively, early or late (>4 months).
The incidence varies between 3-20%. Likely factors include the implant, surgical experience, bonequality (lower in rheumatoid and osteoporosis), and the presence of deformity1,2.
At Wrightington the new surgeons' first 125 Mobility TAR's from 2008-2012 were monitored afterPeter Wood left (who had a low fracture rate). There were six intra-operative fractures (4.8%), mostlymedial. There were three early fractures (2.4%) and four late fractures (3.2%).
Intra-operative fracture is usually caused by over-distraction, or occasionally by excursion of the saw.They are easy to fix and so there is little reason not to stabilise them with a screw. It need not changethe rehabilitation, which is weight bearing as tolerated in a boot for 6-8 weeks.
In early fractures, one sees callus or a hairline fracture, again usually on the medial malleolus; they aretherefore often picked up retrospectively. Some may be an unnoticed intra-operative hairline fracture.They can be managed conservatively with a brace as needed or fixed percutaneously if the surgeonhas misgivings about a particular fracture's stability.
Late fracture is more sinister. It tends to be a stress fracture of the lateral malleolus and is oftenassociated with progressive valgus hindfoot deformity and deltoid instability. The Wrightingtonapproach is to allow these to heal in a boot and then to realign the hindfoot and/or perform asupramalleolar osteotomy. There is probably a roughly 1% yearly incidence.
If both malleoli fracture many would label that a disaster, probably associated with loosening orimplant failure, and a sign that the TAR has come to the end of its useful life. It is a difficult situationto retrieve without revising the entire implant.
References
1. Lee KT, Lee YK, Young KW, Kim JB, Seo YS. Perioperative complications and learning curveof the Mobility Total Ankle System. Foot Ankle Int. 2013;34:210-214.
2. McGarvey WC, Clanton TO, Lunz D. Malleolar fracture after total ankle arthroplasty: acomparison of two designs. Clin Orthop Relat Res. 2004104-110.
Figure: a late stress fracture

Malalignment in Total Ankle Replacement
It is accepted wisdom that malalignment and TAR do not mix. Both the meniscus and the bone aremore likely to fail if loaded asymmetrically. Early TAR series bear this concept out, but recentliterature appears to show that perfect alignment is not so important.
In fact the apparent difference may relate to a change of language over the decades. Definingmalalignment is not simple. There are three planes and six degrees of freedom. Osteophytes can givethe false impression of malalignment; some cases are correctible with the bony cuts, others due to softtissue laxity require a soft tissue procedure; in some patients it is the ankle itself that is malaligned, inothers it is the foot beneath it. Also we tend to judge alignment from the distal tibia and assume anormal knee, but should we be measuring from the hip?
Authors should, but do not always, distinguish between pre-operative malalignment and post-operative, and state how it was measured. A common error is to call some asymmetrical medial tibialwear (which will be automatically corrected with the first tibial cut) severe varus.
We need to find out and then teach the limits on pre-operative malaignment and how it can becorrected; and improve rates of post-operative malalignment whether it be due to technique,instrument design or patient anatomy.
Early series showed that varus of over 10-15 degrees increased the failure rate1-3 if not corrected.Others state that if reduced to within 10 degrees of neutral, deformity does not preclude successfulTAR4-8. Corrective procedures can be staged or simultaneous and include ligament release or repair,supramalleolar osteotomy, calcaneal osteotomy and corrective triple fusion. These are demandingprocedures. Correction through the tibial or talar cuts should not be dismissed as a relatively simplesolution to some alignment problems.
Having said this, experienced surgeons will have seen satisfied patients with persistent deformity andTAR's lasting for many years. The clinical outcome rarely correlates with the X ray! Some recentseries appear to confirm that there is not a strong correlation between deformity and failure6,9. Pre-operative deformity merely means that more corrective procedures are needed.
Other problems include coronal translation, with the talus slipping out from beneath the tibia, whichwill load the meniscus unevenly and impinge on one of the malleolus, but again there are examples ofthese patients doing well clinically. In the sagittal plane, anterior subluxation is a feature of somepatients' ankle arthritis and seems worthy of correction; Lee et al10 attempted to correct this, but in aquarter the subluxation recurred after 12 months, but with no difference to function. They felt this wasmore of a problem with the Hintegra prosthesis than with the Mobility. One factor in anteriorsubluxation is how much sagittal tilt is put on the tibial component; the standard aimed for is 4-6degrees from perpendicular to the tibial axis, but it is hard to be this accurate, and the image intensifiercan easily give a false impression.
Minor mal-rotation of the components should not matter in mobile bearing prostheses because thetibia is usually flat and unconstrained; but if excessive, it in some prostheses it causes impingement ofthe meniscus and implant failure.
Even when corrected, 25% of those with pre-operative coronal deformity will recur. The literaturebrands these failures but in clinical practice some do well despite apparent problems on radiographs.Paul Cooke's concept of “safe failure” is when the talar component progressively subsides (possiblythrough AVN) until the malleoli support the weight. This is seen not infrequently in TAR's over 10

years old. Some malleoli are seen to hypertrophy as a result of their new function. Many patientscomplain of impingement symptoms but many are painless, and if so, there is no reason to revisethem.
References
1. Doets HC, Brand R, Nelissen RG. Total ankle arthroplasty in inflammatory joint disease withuse of two mobile-bearing designs. J Bone Joint Surg Am. 2006;88:1272-1284.
2. Haskell A, Mann RA. Ankle arthroplasty with preoperative coronal plane deformity: short-termresults. Clin Orthop Relat Res. 200498-103.
3. Wood PL, Deakin S. Total ankle replacement. The results in 200 ankles. J Bone Joint Surg Br.2003;85:334-341.
4. Cornelis Doets H, van der Plaat LW, Klein JP. Medial malleolar osteotomy for the correction ofvarus deformity during total ankle arthroplasty: results in 15 ankles. Foot Ankle Int.2008;29:171-177.
5. Hintermann B, Valderrabano V, Dereymaeker G, Dick W. The HINTEGRA ankle: rationale andshort-term results of 122 consecutive ankles. Clin Orthop Relat Res. 200457-68.
6. Hobson SA, Karantana A, Dhar S. Total ankle replacement in patients with significant pre-operative deformity of the hindfoot. J Bone Joint Surg Br. 2009;91:481-486.
7. Kim BS, Choi WJ, Kim YS, Lee JW. Total ankle replacement in moderate to severe varusdeformity of the ankle. J Bone Joint Surg Br. 2009;91:1183-1190.
8. Ryssman D, Myerson MS. Surgical strategies: the management of varus ankle deformity withjoint replacement. Foot Ankle Int. 2011;32:217-224.
9. Mann JA, Mann RA, Horton E. STAR ankle: long-term results. Foot Ankle Int. 2011;32:S473-S484.
10. Lee KT, Jegal H, Park YU et al. Comparison of sagittal subluxation in two different three-component total ankle replacement systems. Foot Ankle Int. 2013;34:1661-1668.

Wound and Neurovascular Complications of TAR
National Joint Registries pick up some major complications like revision for infection, but are notdesigned to pick up minor wound complications or nerve injuries. We are left then with case series ormeta-analyses based on case series – which are often reported by a single surgeon operator. Seriousvascular complications are very rare and are not further considered.
Definitions of various wound complications can be problematic and are often not spelled out. Mostwould consider a deep infection to be one requiring further operative intervention. Other terms likesuperficial infection, delayed healing, minor central skin necrosis and dehiscence are used with theassumption that their meanings are universal.
Goldberg's team reviewed the literature on 7942 TAR's1. They found an overall rate of 2.4% forsuperficial infection; 1.1% for deep infection; 1.3% for major intra-operative nerve injuries.
Saltzman et al2 studied 593 STAR ankles in a prospective multi-centre trial of TAR versus fusion, anddocumented post-operative status meticulously. They found a 22% rate of loss of sensation after TAR,most commonly around the medial side of the navicular, presumably from injury to the medial branchof the superficial peroneal nerve. Most surgeons will gloss over this and treat it almost as part of theprocedure. They also reported a 4.5% superficial infection rate, major infection 1.2%, and majorwound complications 2%, one of which required a revision.
Lee et al3 couched their first 50 cases in terms of a learning curve by arbitrarily dividing them into thefirst 25 and second 25 cases. There was a 12% nerve injury rate in the first group, none in the second.One deep infection was treated by revision to fusion. There were three “minor wound complications”but here the problems with nomenclature are illustrated as some of these required split skin grafts,which most surgeons would regard as an appreciable complication.
Wood4 had 2.5% minor wound problems, including one patient who was revised to a fusion as aresult.
Treatment for superficial infection is generally regular dressing changes and oral antibiotics. Deepinfections are most wisely managed according to the Oxford protocol5 (see below) with a two stageprocedure leading to fusion.
In order to reduce deep infections, IV antibiotics must be given. The low rate of infection makes itvirtually impossible to properly test interventions designed to reduce it further. Clean air theatres withlaminar flow are often used. Different methods of skin preparation have been studied in the foot andankle6, with post-preparation bacterial culture number as the outcome measure. The best preparationwas alcoholic chlorhexidine used twice, but it is unknown whether this translates into fewer clinicalinfections.
There may or may not be a benefit to the surgeons wearing a ventilated “space suit” that covers thehead. The New Zealand joint registry appeared to show that laminar flow and “space suits”, bothindependently and together, were associated with increased revision for infection in THR and TKR7.The modern suit has no exhaust, unlike the Charnley system that historically was associated with alower infection rate. Positive pressure at the head end of modern suits expels air from the lowestextremity, whereas the Charnley suit sucks air from the bottom to the top, and this may well affect thespread of microbes from the surgeon's body.

Surgical technique is of course relevant to wound complications. In the anterior approach the skin isthin and retraction must be careful, preferably avoiding self-retainers as they increase the tension onthe skin.
Summary
Superficial peroneal nerve injury is common but rarely significant.
2-5% of TARs develop a superficial infection which by definition will not have a significanteffect on outcome if treated appropriately.
Deep infection rate is just above 1% and is a serious complication often necessitating revisionto fusion.
References
1. Zaidi R, Cro S, Gurusamy K et al. The outcome of total ankle replacement: a systematic reviewand meta-analysis. Bone Joint J. 2013;95-B:1500-1507.
2. Saltzman CL, Mann RA, Ahrens JE et al. Prospective controlled trial of STAR total anklereplacement versus ankle fusion: initial results. Foot Ankle Int. 2009;30:579-596.
3. Lee KB, Cho SG, Hur CI, Yoon TR. Perioperative complications of HINTEGRA total anklereplacement: our initial 50 cases. Foot Ankle Int. 2008;29:978-984.
Protocol for managing failed TAR (Oxfordgroup – JBJS Br 2006)
Failed ankle replacement
Standing x rays and bloods
Signs of infect ion No sign of infect ion(biopsy in equivocal cases)
2 stage revision 1 stage revision(Frozen sect ion issuspicious of infect ion
Revision anklereplacement
Fusion (Oxfordrecommend TTC fusion)
Fusion with Ilizarovframe
(Amputat ion)

4. Wood PL, Prem H, Sutton C. Total ankle replacement: medium-term results in 200Scandinavian total ankle replacements. J Bone Joint Surg Br. 2008;90:605-609.
5. Kotnis R, Pasapula C, Anwar F, Cooke PH, Sharp RJ. The management of failed anklereplacement. J Bone Joint Surg Br. 2006;88:1039-1047.
6. Yammine K, Harvey A. Efficacy of preparation solutions and cleansing techniques oncontamination of the skin in foot and ankle surgery: A systematic review and meta-analysis.Bone Joint J. 2013;95-B:498-503.
7. Hooper GJ, Rothwell AG, Frampton C, Wyatt MC. Does the use of laminar flow and space suitsreduce early deep infection after total hip and knee replacement?: the ten-year results of theNew Zealand Joint Registry. J Bone Joint Surg Br. 2011;93:85-90.
TAR complications: Discussion
It was felt by many that STARs caused more lateral fractures, the Mobility more medial. Mostimplants do well in the first 5-10 years but, as with hips, it may be later in their life that they start tobe differentiated.
Mr Cooke clarified that “safe failure” or subsidence is safe only if the foot is square to the floor; assoon as there is tilt, the TAR fails catastrophically and clinically and requires revision.
There was a discussion about altering the approach to go lateral to EHL, more direct on to the talusand needing less retraction on the skin, but the consensus was clearly against this.
More than one surgeon uses prophalactic wire up one or both malleoli. This stops the saw going toofar out and also makes ORIF easier if needed. In the USA several surgeons put a screw in the medialmalleolus for every case!
Heterotopic ossification is another method by which a TAR may fail clinically, causing posteriorimpingement for instance. One way of dealing with it is to remove the insert, use rongeurs to get itout, and replace the liner; or use a posteromedial or posterolateral approach. Two surgeons had used aposterior incision to get at heterotopic bone.
Late malleolar fractures can almost be seen as a separate disease caused by malalignment.Osteoporosis and osteomalacia may also be factors.

Malunion of Triple Arthrodesis
Open reduction and triple arthrodesis for the planovalgus foot is a technically difficult procedure.Because of this, malunion or mal-alignment is a well-recognised complication and can be seen in up to15% of patients (1).
Current practice 2014: Triple fusion for planovalgus foot
90% have had a suboptimal result in terms of alignment in their own practice
Indeed S. Haddad can be quoted as saying:
“The precarious balance required to create a plantigrade foot via triple arthrodesis with pre-existing deformity leaves even the most skilled surgeon challenged”
So if you experience malunion in such patients you are in good company. However is it somethingthat we actively look for or consent patients for?
Current practice 2014: Triple fusion for planovalgus foot
25% check and document malalignment at 3/12 post-op
60% consent patient for malalignment
Thus full appreciation of the plano-valgus deformity is vital to understand how to correct it fullyduring triple arthrodesis and prevent mal-alignment. Assessment of the patient pre-operativelyrequires full clinical examination and should include assessment of the mid/forefoot in relation to acorrected hindfoot.
Radiographs should include weight bearing views of both ankle and foot, cobey views and a CT. Aweight baring PED CT can be although of as the gold standard although this is not currently availablein many centres.
The apex or CORA of a planovalgus deformity is at the subtalar joint and there is often additionalforefoot supination. Both a calcaneal osteotomy and a lateral column lengthening address thedeformity away from this point and therefore may cause translation and mal-alignment. This has led tothe introduction of sinus tarsi correction of the planovalgus deformity, particularly in the adolescent(2,3). Deformity is best corrected at the CORA and thus each correction tailored to the individualdeformity.
Current practice 2014: Medial approach for severe flat foot
20% routinely use this approach
Medial approach should be used especially if tethered or poor lateral skin or a dislocated TN joint
Current practice 2014: Gastrocnemius/ Achilles lengthening

20% always do this when doing a triple for a flat foot
60% do this according to findings on table
Patients should always be assessed for gastrocnemius/Achilles tightness and corrected when needed.
This allows deformity correction.
Current Practice 2014: Lateral column lengthening as well as triple arthrodesis
10% of people routinely do this
Current practice 2014: Bone graft for triple arthrodesis
5% currently do this
Consensus
We propose that there is individual assessment of the severe stiff flat foot deformity. All patients
should be consented for malalignment and have their pre and post-operative alignment documented. A
triple fusion should be combined with the procedures in an “a la carte” manner rather than a “carte
blanche” to ensure full correction of the deformity at the CORA.
Gastrocnemius/ Achilles lengthening to allow reduction
Tricortical or “sugarcube” graft in sinus tarsi
Lateral column lengthening
Fusion of 1st TMTJ
1. J Bone Joint Surg Am. 1999 Oct;81(10):1391-402. Saltzman CL1, Fehrle MJ, Cooper RR15% residual deformity. Triple arthrodesis: twenty-five and forty-four-year averagefollow-up of the same patients.
2. Vedantam R, Capelli AM, Schoenecker PL: subtalar arthroereisis for the correction ofplanovalgus foot in children with neuromuscular disorders. J Paed Orthop 1998:18
3. Giannini BS, Ceccarelli F, Surgical treatment of flexible flat foot in children, 4 year followup study JBJS Am 2001: 83

Calcaneal Fracture Malunion
Current practice 2014: Calcaneal fractures
80% would operate on calcaneal fractures
Of those who would operate 100% would fix a 2 part fracture
The indications to operate are to decrease the likelihood of poor outcome. However, which fracturesdo better and which do not benefit from surgical intervention is not fully understood and what isrequired is publication of recent research to highlight this.
The main aim in treating calcaneal fracture is to avoid malunion as its sequel such as:
Subtalar arthritis Calcaneo-cuboid arthritis Sub-fibular impingement Peroneal tendon pathology Loss calcaneal height Hindfoot varus Widened heel Tibial/ sural nerve irritation
This will usually be identified from the clinical history and clinical examination focusing on pain,gait, heel alignment and motion of the ankle and subtalar joints. Radiographically these sequela canoften be identified by measuring the talocalcaneal height (TCH) the Talocalcaneal angle (TCA) or the
Talar-declination angle (TDA).
In 1996 Stephen and Sanders (1) identified three subgroups of calcaneal malunion that were thenmodified by Rammelt and Zwipp (2) into six subgroups, in 2013. This latest classification can be usedto direct future surgical intervention.

The aim of revision surgery is maintain or correct any mal-alignment in particular varus and restorethe TCH, TCA and the TDA. This may require a bone block arthrodesis of the subtalar joint,particularly if there is >8mm of height loss.
Current practice 2014: Subtalar arthrodesis for calcaneal malunion.
80% use a bone block selectively to restore height
Coronal plane deformity should be addressed with a calcaenal osteotomy such as the closing wedge(Dwyer), the vertical slide (Huang) or through the primary fracture line (Romash). However these arerarely performed especially inconjunction with a subtalar fusion.
Consensus
Calcaneal malunion involves an incongruent subtalar joint, varus malalignment and tuberositydisplacement.
Degenerate joints and malalignment need to be addressed if revised
References
1. Stephens HM, Sanders R. Foot Ankle Int. 1996 Jul;17(7):395-401.2. Rammelt S, Zwipp H. Int Orthop. 2013 Sep;37(9):1707-17.
Sequale of Talar Neck Fractures
In the management of acute talar neck fractures it is vital to “get it right first time” as the possiblesequale include:
Maliunion/ malalignment Avascular necrosis +/- collapse Ankle arthritis Subtalar arthritis

Uncoupling of ankle, hindfoot and midfoot mechanics
To do this a CT scan in the acute setting enables the surgeon both to measure alignment displacement,to look for subluxation of ankle or subtalar joint and classify the Hawkins type. Hawkins divided talarneck fractures into 4 types :
I. UndisplacedII. Subtalar dislocation
III. Subtalar & Ankle dislocationIV. Subtalar, ankle and talonavicular dislocation
Current practice 2014: Talar neck fractures
90% would treat type I fracture conservatively
Type I fractures are essentially undislaced and can therefore be treated conservatively. All otherfractures are best treated surgically. This is best performed by either a double approach or thedorsomedial approach alone. Timing of sugery doesn’t have a clear effect however promptintervention is usually advocated due to the risks of AVN especially with higher grade injuries. TypeIII and IV injuries should be treted as an emergency to convert them to a type II and temporarystablisation with external fixtation
Current practice 2014: Post operative treatment talar neck fractures
40% would NWB for 6/52
50% would NWB for 12/52
Malunion
Current practice 2014: Talar malunions
35% present had dealt with a malunion within the past year
Malunion deformity tends to be medial shortening, varus and extension.
This is addressed through the dorsomedial incision at the main area of comminution in thedorsomedial cortex. Restoration of length to prevent varus is paramount. In the acute phase this isachieved with a medial plate and or screws however in the presence of an established malunion then amedial osteotomy to correct length, varus and extension with interposition tricortical grafting shouldbe perfromed in addition. When there is an established malunion then the presence of concomitantarthritis in either the ankle and/or subtalar then salvage treatment with fusion procedures should beconsidered.

Avascuar necrosis
Avascular necrosis (AVN) is a pathological process characterised by:
Loss of blood supply Cellular death Collapse of bony structure Joint derangement
In Hawkins’ classification we are reminded of the somewhat precarious blood supply of the talus.Disruption in blood supply can occur from traumatic injury and render the talus avascular; the risk ofwhich increases as displacement increases. However there are other causes that should be consideredparticularly in the absence of a history of significant trauma.
AVN can be detected on plain radiograph or on MRI when subtle and staged according to the Ficatstaging. T2 weighted images allow differentiation between necrotic and hyperaemic areas,highlighting that AVN doesn’t have to involve the whole bone perhaps allowing targeted therapy.
In 2004 Horst et al (1) suggested the way of addressing AVN of the talus illustrated in the figure 1.Patients with early AVN need to undergo joint preserving surgery. This consists of decompression,grafting or re-fixation of a non-union. Treatment of late AVN depends on the proportion of the bone/joint involved but usually requires joint fusion or excision of the talus and bone grafting to restoreheight. Any such surgery is a big undertaking and requires long, slow rehabilitation with 3/12 in aplaster (6/52 NWB) and 3/12 in a protective boot.
References
1. Horst et al Foot Ankle Clin N Am 9 (2004) 757–773
Consensus
All but type I fractures should undergo ORIF Type III & IV should undergo emergency surgery to convert to type II and then wait
definitive surgery as the soft tissues allow Medial length, varus and extension deformity are what we are trying to avoid Patients should be NWB for 6 weeks and protected for 3/12 AVN should be addressed as suggested by Horst
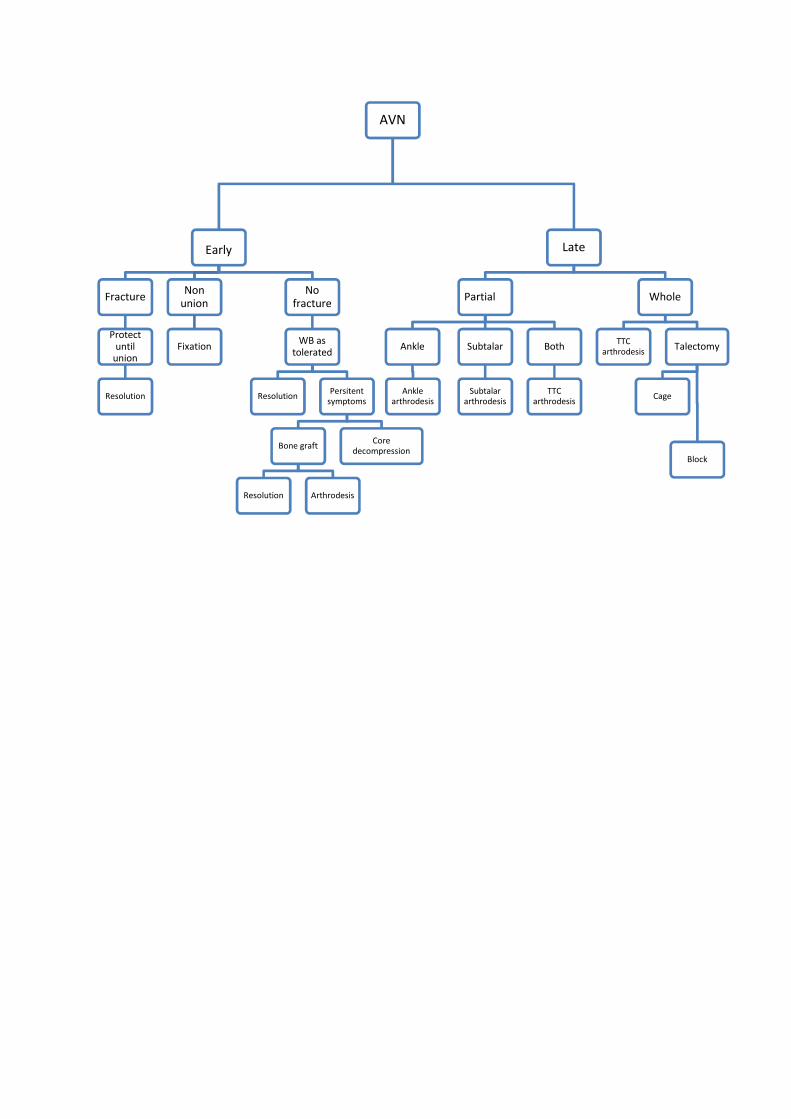
AVN
Early
Fracture
Protectuntil
union
Resolution
Nonunion
Fixation
Nofracture
WB astolerated
Resolution Persitentsymptoms
Bone graft
Resolution Arthrodesis
Coredecompression
Late
Partial
Ankle
Anklearthrodesis
Subtalar
Subtalararthrodesis
Both
TTCarthrodesis
Whole
TTCarthrodesis Talectomy
Cage
Block

Navicular Stress Fractures
Navicular fractures are rare in isolation. Acute fractures are either avulsion of the tuberosity or a body
fracture. Stress fractures of the navicular occur due to repetitive stress in a region of poor blood
supply. They originate at the proximal dorsal articular surface and propagate distally and
perpendicular to the longitudinal axis in central third. They usually present insidiously and plain
radiographs are often normal. An MRI scan can be difficult to differentiate between a stress reaction
and a fracture, whilst a bone scan is sensitive but non-specific. The most widely used classification
system depends on CT findings (1):
I. Dorsal cortical break
II. Involves fracture propagation into body
III. Complete fracture exists plantar aspect
Current Practice 2014: Treatment of un-displaced Type III navicular fracture
65% would treat surgically
35% would treat conservatively
All would keep them NWB for 6-8/ 52
Current practice 2014: Type III navicular fracture no sclerosis
90% would operate percutaneously
10% would perform ORIF
The primary reason for non-union is the weight bearing status, with those treated WB 3 times as likely
to get a non-union as those treated NWB (2,3). A systematic review in 2010 concluded that fracture
type did not correlate with outcome, regardless of treatment. The literature is supportive of the
conservative management of undisplaced fractures as long as they are kept NWB for 6-8/ 52.
The indications to operate are displacement, failure of conservative management or delayed
presentation and sclerotic fracture margins. This is usually performed percutaneously for acute
fractures and open for sclerotic fractures or non-unions, although a sclerotic fracture can be freshened
up percutaneously with a k wire to avoid opening the fracture. After reduction of the fracture with
debridement of the fracture margins as required, compression screws should be placed from lateral to
medial. Bone grafting and locking plates can be reserved for the rare case of non-union after ORIF,
which occurs in <5% of cases (4). Such cases also require that any co-existing foot deformity is taken
into consideration.

Consensus
Type III fractures should undergo surgical fixation
Patients should be kept NWB for 6 weeks
ORIF if there are sclerotic edges
References
1. Saxena A, Fullem B, Hannaford D. Results of treatment of 22 navicular stress fractures and a
new proposed radiographic classification system. J Foot Ankle Surg. Mar-Apr 2000;39(2):96-
103.
2. Stress fractures of the tarsal navicular: a retrospective review of 21 cases. JBJS
1982;64A:700-12
3. Outcome of conservative and surgical management of navicular stress fractures in athletes.
Am J Sports Med 1992;20:657-66
4. Torg et al. Management of tarsal navicular stress fractures: conservative versus surgical
treatment: a meta-analysis. Am J Sports Med 2010; 38:1048-53
5. Fitch KD, Blackwell JB, Gilmour WN. Operation for non-union for stress fracture of the
tarsal navicular. J Bone Joint Surg Br 1989;71:105–10.

Convened participants of the 2014 Round Table Meeting were:
Amit AminTom Ball
Stephen BendallRick Brown
Callum ClarkTim Clough
Chris CoetzeePaul CookeNick CullenMark DaviesSunil DharNick Geary
Andy GoldbergKurt Haendlmayer
Matthew HendersonMark HerronMike Karski
Senthil KumarAndy MolloySteve ParsonsAnand PillaiSimon Platt
James RitchieFred Robinson
Ben RudgeRobert Sharp
Ian SharpeDishan Singh
Sam SinghMichael Stephens
Nick TalbotHiro TanakaRhys Thomas
Ioan Tudur JonesPhilip VaughanTim Williams
David Williamson

Ortho Solutions LimitedWest Station Business ParkSpital RoadMaldonEssex CM9 6FFUnited Kingdom
T: +44 (0) 1621 843599F: +44 (0) 1621 858953E: [email protected]