TOLERANCE VACCINE- WHERE ARE WE? UNITED NATIONS-GENEVE H L Trivedi, F.R.C.P. (C) Director,...
25
TOLERANCE VACCINE- WHERE ARE WE? UNITED NATIONS-GENEVE H L Trivedi, F.R.C.P. (C) Director, Professor, G. R. Doshi & K.M. Mehta Institute of Kidney Diseases & Research Centre, Dr H L Trivedi Institute of Transplantation Sciences,
-
Upload
sheila-johnson -
Category
Documents
-
view
215 -
download
0
Transcript of TOLERANCE VACCINE- WHERE ARE WE? UNITED NATIONS-GENEVE H L Trivedi, F.R.C.P. (C) Director,...

TOLERANCE VACCINE- WHERE ARE WE?
UNITED NATIONS-GENEVE
H L Trivedi, F.R.C.P. (C)
Director, Professor,
G. R. Doshi & K.M. Mehta
Institute of Kidney Diseases & Research Centre,
Dr H L Trivedi
Institute of Transplantation Sciences,
Civil Hospital Campus, Ahmedabad, INDIA

What is a Vaccine ?
A vaccine is a biological preparation that
improves immunity to a particular disease. A
vaccine typically contains a small amount of
an agent that resembles a microorganism. ...

Tolerance Vaccine In Transplantation
• Tx pts –stable grafts-↓pCTL frequencies at 3 mths post-Tx
• May be permanent
• Tubular cells can induce specific anergy
• Chimerism can lead to graft acceptance
Ophir E, Reisner Y. Induction of tolerance in organ recipients by hematopoietic stem
cell transplantation. Int Immunopharmacol.2009 Jun;9(6):694-700.Epub 2009 Jan 16

• Veto - An authoritative prohibition or rejection of a proposed or
intended act
• What is a Veto Cell ?
• The term “VETO” relates to the ability of cells to neutralize
cytotoxic T-lymphocyte precursors directed against their antigen
• Veto Activity: capacity to specifically suppress cytotoxic T cell
precursors directed against antigens of themselves, not against third
party antigens (Miller,1980)
Tolerance vaccine of Veto Cells
Muraoka S, Miller RG. Cells in bone marrow and in T cell colonies grown from
bone marrow can suppress generation of cytotoxic T lymphocytes directed against
their self antigens. J Exp Med. 1980;152: 54-71.

• Cells within the human CD34+ population as well as their
immediate early myeloid progeny, are endowed with potent veto
activity
• Thus it is possible to harvest more veto cells on culturing of CD34+
cells for short term and make a vaccine from these cells with other
cells
• These cells should survive, multiply, block/ delete/ functionally
inactivate effector cells
How Can We Make a Vaccine of Veto Cells ?
Gur H, Krauthgamer R,Berrebi A, Nagler A, Klein T, Martelli M, Tabililo A and
Reisner Y. Tolerance induction by megadose hematopoietic progenitor cells:
expansion of veto cells by short-term culture of purified human CD34+ cells. Blood.
2002; 99: 4174-4181

Types And Sources Of Veto Cells
BM CELLS
CD34+ CD 33-
LYMPHOCYTE
SUBPOPULATION
CD34+ CD 33+
CD 34- CD 33+
Activated NK cells
Activated CD4+ T-cells
Activated CD8+ T-cells
Activated B-cells
SOURCES :
BM, Thymus, spleen, LN, Fetal Liver
In-vitro expansion

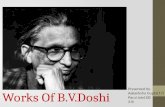
Mechanism Of Action Of Veto Cells
Effector cell Veto cell
Fas L
MHC
CD 8+
TCR
α-3
Fas
MHC 1
Apoptosis
Reduction of FADD like Il-1-converting enzyme-inhibitory protein
O hr 24 hr 48 hr 72 hr
FLIP

Our Experience With Veto Cells

Study Design - Oct ’08- ‘09

Salient Features
• Clonal stimulation with stem cell cocktail
• Clonal deletion with Bortezomib (Proteasome inhibitor)
with adjuvant MP, ATG, Rituximab
• Chimerism and veto cell associated tolerance
• Kidney transplantation without conventional
immunosuppression
Donor-Healthy relative with compatible blood groupInformed consent and study forms approved by IRB

• N=22, M: F: 20 : 2, • Mean Age (years): 28.3 (16-53)• Donor profile: HLA mis-match A/B/DR: 2.08 ± 1.02.
Parents: 17, Sibs: 4, Son: 1
Cross gender donors: 16• Mean CD34+ infused: 2 X 106/kgBW (range: 0.14-9.3)• Basic DS:
CGN : 17
Lupus Nephritis : 01
FSGS : 01
Vasculitis : 01
Primary IgAN : 01
MPGN : 01
Patient and Donor Profile

Generation and expansion of veto cells from CD34+ cells
• 100 ml BM aspirated from donor PSIC under LA after cytokine stimulation
(G-CSF, 600 g s.c.x 2 days)
• BM collected in T.C. flask with specific media for BM containing an early
acting cytokine mixture including SCF,TPO and Flt3 ligand
• In vitro expansion- CO2 incubator for 7-8 days at 37ºC under humidified
condition with 5% CO2 95% O2 , media changed every other day
• On 7/ 8th day cells were harvested and checked for sterility, viability and counts
under FACScan for yield
• Portal infusion of recipient on 8th day
• Second deletion cycle with Bortezomib to abrogate all antibodies
• Transplantation without immunosuppression with favorable immune response

• Follow-up (mths): 14.9 (10.4-19.6)
• Mean S. Cr. (mg%): 1.7 ± 0.6(0.9-3.2)
• Rejections -3 (13.6 %) (T/B/Suspicious)
Immunosuppression: Mean SCr (mg%)
Nil: 3 - 1.22 ± 0.16
Pred only: 10 1.6 ± 0.64
Tac./MMF : 8 1.97 ± 0.67
Clinical Results

n=22
CD34+/33- CD34+/33+ CD34-/33+
BM
Beginning
0.38%
(0.03-1.08%)
0.17%
(0.01-0.88%)
0.67%
(0.05-2.19%)
CBM
End
0.70 %
(0.08-2.85)
0.53%
(0.05-2.61%)
0.82%
(0.08-2.21%)
Rise in Veto
Cells
2 fold
p= 0.006
3.1 fold
p= 0.001
1.2 fold
p= NS
Lab ResultsVeto Cell Expansion In Cultured BM

n=22
CD34+/33- CD34+/33+ CD34-/33+
before 0.04 ± 0.03 0.02 ± 0.01 2.47 ± 1.84
9 months later
0.09 ± 0.08 0.29 ± 0.42 6.62 ± 3.09
Statistical
Significance
P =0.009 P =0.07 P= 0.09
Post Tx Status of Veto Cells In Renal Allograft Recipients

Lab Results
CD34+/33-: 0.13 CD34+/33+:0.14CD34-/33+: 0.20
BM: Before in-vitro expansion CBM: Post in-vitro expansion
CD34+/33-: 0.22 CD34+/33+:3.69CD34-/33+: 7.13
Pt.: Before infusion Pt.: Post-Tx- in vivo expansion
CD 4+: 36.98 %CD8+: 60.75 %
CD 4+: 43.17 %CD 8+: 54 %
CD34+/33-: 0.15 CD34+/33+:0.13CD34-/33+: 0.03
CD34+/33-: 0.36 CD34+/33+:0.38CD34-/33+: 8.56

H & E, X 100 PAS, X 100
S. P., 38, F, Basic Ds: DPLN, Donor: father, HLA match:4/6, Tx dt: 20th Apr,09, Surveil. Bx- 6 mths posttx., SCr: 0.8 mg%, No drugs

A., 23,M, Basic Ds: CGN, Donor: Mother, HLA match:3/6, Tx dt: 7th Apr,’09, Surveil. Bx- Normal, SCr: 1.48 mg%
Peripheral blood LH. chimerism: 6.8 % at 6 mths posttx, IS- 5 mg Pred/day
PBC BY FISH

CDB36: RN, 19/M (father) Tx: 12 June ‘09 3 June 2010
A B C DRB1 DQ DRB345 Bw
PT 1132(1
9) 18 51(5) 7 14 2 3 6(1) 2 51 52 4 6
DN 1 11 5 40 - 1415 (2) - 6(1) - 51 - 4 6
19
POD: 356
5/<5/75/<5/7
7/5/10FCM -/-7/5/10FCM -/-
MP (x4)
Prednisone
MP (x4)MP (x1)
MP (x4) +IVIg (x6)
DSA
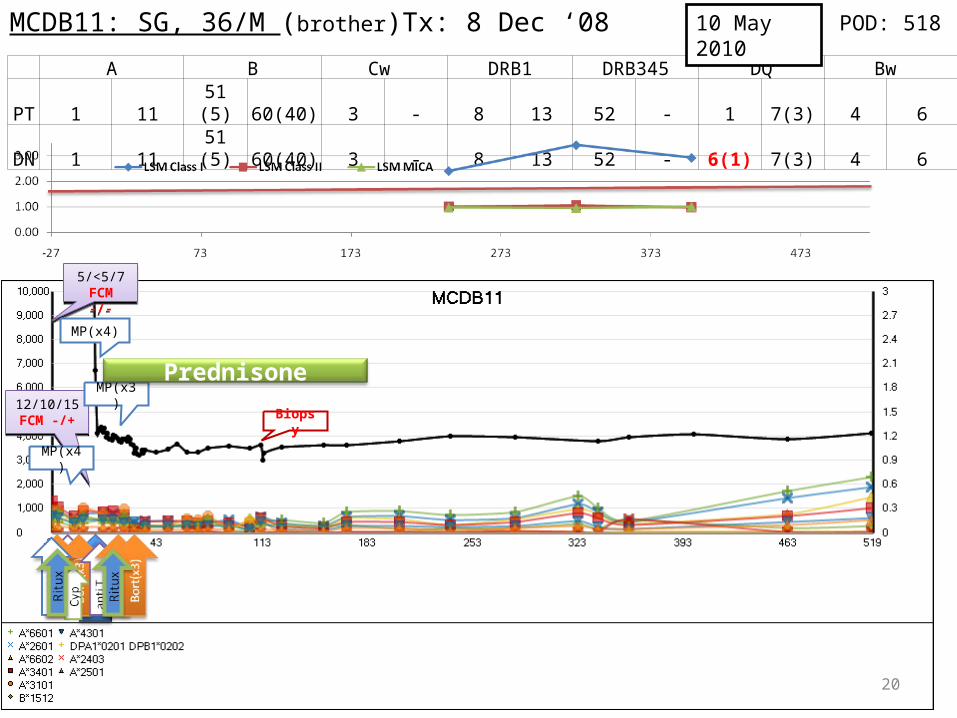
MCDB11: SG, 36/M (brother)Tx: 8 Dec ‘08
A B Cw DRB1 DRB345 DQ Bw
PT 1 11 51 (5) 60(40) 3 - 8 13 52 - 1 7(3) 4 6DN 1 11 51 (5) 60(40) 3 - 8 13 52 - 6(1) 7(3) 4 6
POD: 51810 May 2010
20
12/10/15FCM -/+
12/10/15FCM -/+
5/<5/7FCM -/-5/<5/7FCM -/-
MP(x3)
MP(x4)
Biopsy
Prednisone
MP(x4)

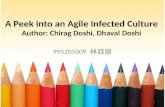
Veto Cell Activity Noted As Absence of MLR
Positive MLRG0 / G1=2.48 %
AfterNegative MLR
G0 / G1=96.18%
73.68%2.48%
1.08%

Discussion
• Stem cell dose escalation is one way to overcome immune
rejection of incompatible transplant
• Studies suggest that veto cells within CD34+ progenitors
mediate facilitating effect to overcome major genetic barriers
and enable rapid and durable engraftment of mismatched
transplants without GVHD
• FACScan study revealed that the predominant phenotype of
CD34+/33- cells used at initiation of the culture was replaced
at the end of a culture by cells expressing phenotype of early
myeloid phenotypes such as CD34+/33+ and CD34-/33+ Cont…

Discussion
• What are the benefits due to ?
• Bortezomib with other deletional agents ?
• Stem cells and Veto cells ?
• It is the combination of both
• Stable graft function
• Normal surveillance Bx of graft
• Existence of long lasting peripheral blood chimerism
• Persistence of Veto cell counts
• Persistence of Veto activity (Negative MLR)

Conclusion• Transplantation without conventional immunosuppression is now
a reality at Ahmedabad using veto cells and clonal deletion
• Human CD34+ cells in short term cultures are usually associated
with a significant loss of self-renewal capacity, our cells have still
retained this self-renewal capacity and also achieved
differentiation into myeloid phenotype
• More veto cells can be harvested by culturing of human CD34+
cells for short term with an early-acting cytokine mixture
including SCF,TPO and Flt-3 ligand
• This vaccine will open up new doors to treat other autoimmune
disorders if treated on time

Sufferings have no age, gender, religion, race or color. Let this research give the gift of good healthy life to all
allograft recipients across the globe!