To Use Them Together or Not Understanding Drug Interactions With HCV Medications
42
1 To Use Them Together or Not Understanding Drug Interactions With HCV Medications Rajwant Minhas, FH Resident HIV/AIDS Rotation May 2012
description
To Use Them Together or Not Understanding Drug Interactions With HCV Medications. Rajwant Minhas, FH Resident HIV/AIDS Rotation May 2012. Objectives. Understand principles of drug interactions Become aware of drug interactions of HCV medications with: Antiretrovirals Antidepressants - PowerPoint PPT Presentation
Transcript of To Use Them Together or Not Understanding Drug Interactions With HCV Medications

1
To Use Them Together or NotUnderstanding Drug Interactions With HCV Medications
Rajwant Minhas, FH Resident
HIV/AIDS Rotation
May 2012

2
Objectives
• Understand principles of drug interactions• Become aware of drug interactions of HCV medications
with:– Antiretrovirals– Antidepressants– Statins– Antihypertensives– Contraceptives and hormonal replacement– Methadone– Steroids

3
Drug-Time Concentration Curve
Source: http://www.skepticnorth.com/2012/01/generic-drugs-should-we-be-skeptical/

4
How Are Drugs Eliminated From Body?
• Renal: Excreted unchanged in the urine.
• Clearance directly proportional to renal function
• Probenecid: Drug that blocks renal excretion of other drugs
Patrick D. Drug Metabolism. University of Texas Pharm 143M Class Notes. Fall 2008

5
Drug Metabolism
• Liver: Primary site for drug metabolism
• Mediated by Cytochrome P-450 system present in liver and enterocytes of small intestine
Image Source: http://www.nature.com/nrd/journal/v1/n1/fig_tab/nrd705_F1.html
Patrick D. Drug Metabolism. University of Texas Pharm 143M Class Notes. Fall 2008

6
Drug Metabolism• Drug metabolism: Chemical transformation of drug by enzymatic
systems
• Goal:– To de-toxify drugs, and
– Make them either more water soluble (for excretion in urine) or more fat soluble (for excretion in the bile, and then into the feces).
– Hydrosoluble molecules: Low toxicity risk ↑ renal excretion
– Lipophilic drugs Hydrophilic Metabolites
Patrick D. Drug Metabolism. University of Texas Pharm 143M Class Notes. Fall 2008

7
CYP450• The P450 cytochromes chemically
oxidize or reduce drugs
• > than 25 human cytochrome P450’s
• They are named by number and letter: – 4 major families indicated by
number– 6 major sub-families indicated
by letter– Individual enzymes within a
subfamily indicated by number
• For example 3A4, 2D6, 2C19
Badea G. Drug Metabolism. Feb 2007

8
CYP450 System
Badea G. Drug Metabolism. Feb 2007

9
P-glycoprotein
• Transports drugs out of the cell
• Tissue expression is varied
• Found in the major absorption, distribution and elimination organs
• P-gp inducers and inhibitors\
Source: http://www.nature.com/nrc/journal/v2/n6/images/nrc823-f3.gif

10
Drug Interactions
• Pharmacokinetic Interactions:– Inhibition of metabolism – Induction of metabolism – Altered drug absorption – Inhibition of renal excretion – Displacement from plasma
protein binding sites
• Pharmacodynamic Interactions: – Synergism or antagonism of
drug effects, without alterations in concentrations of either drug
Badea G. Drug Metabolism. Feb 2007

11
Examples of Drug Interactions• Drug interactions involving oral medications can take place in at least 2 sites: the liver and
the intestine.
• Drug Inhibition:– Saquinavir + ritonavir: Inhibition of CYP 3A4
• 20 fold ↑ in plasma concentration
• Drug Induction:– Phenytoin + Lopinavir/Ritonavir: Multi-agent interaction, mechanism unclear. Both
phenytoin and ritonavir are drug inducers, ritonavir is a drug inhibitor too• 30% lower lopinavir AUC• 35% lower ritonavir AUC• 23% lower phenytoin AUC
• Pharmacodynamic Interaction: – Enhanced bone marrow suppression in patients given concurrent zidovudine and
ganciclovir
Lexicomp. Kiser JJ et al. Hepatology 2012;55:1620-1628.

12
But How Do I Find All This Information?

13

14

15

16
hep-druginteractions.org/

17

18

19

20

21
BOC and TVR Pharmacokinetics
• BOC: Metabolized by CYP3A4, CYP3A5 and aldoketoreductases– Strong reversible inhibitor of CYP3A4 and p-
glycoprotein– Protein binding 75%
• TPV: Substrate and strong inhibitor of CYP3A4 and p-glycoprotein– Protein binding 59-76%
Kiser JJ et al. Hepatology 2012;55:1620-1628.

22
Drug Interactions With BOC & TPV
• Rifampin: Potent CYP3A4 inducer
– Reduced the single dose TPV AUC and Cmax by 92% and 86%
• Ketoconazole: A potent CYP3A inhibitor
– Increased single dose TPV AUC and Cmax by 62% and 24% after a single dose of ketoconazole
• TPV increased digoxin Cmax and AUC by 1.5 and 1.85 fold
– Lower doses may be required, monitor digoxin levels
Kiser JJ et al. Hepatology 2012;55:1620-1628.

23
Drugs to Avoid or Use With Caution in Patients on BOC or TPV
• Anxiolytics and Sleep Aids• Antidepressants• Antihypertensive Agents• Antipsychotics• Drug addiction support medications• Immunosuppressants• Opioid Replacements• Oral Contraceptives• Statins
Kiser JJ et al. Hepatology 2012;55:1620-1628.

24
Protease Inhibitors With Statins
• : Contraindicated, potential for myopathy including rhabdomyolysis• : A lower maintenance dose may be warranted, with additional clinical monitoring
Statin Boceprevir Telaprevir
Atorvastatin
Lovastatin
Simvastatin
Rosuvastatin
Pravastatin
Hep-druginteractions.org Tseng A. Toronto General Hospital April 24, 2012

25
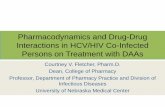
TPV + Atorvastatin
Mean plasma concentration-time profile of atorvastatin following oral administration with and without telaprevir. Error bars represent the standard error of the mean.
Lee JE et al. Antimicrob Agents Chemother. 2011 October; 55(10): 4569–4574.
Combination contraindicated

26

27
Opioid Replacements
Methadone Buprenorphine
•85% plasma protein bound
•Metabolized by CYP3A, 2C8 and glucuronidation
•TPV displaces methadone from its plasma protein binding sites
But free concentrations were unchanged
A methadone dose adjustment likely unnecessary with the addition of TPV
•BOC: ↑ or ↓ methadone•Limited data have been reported showing that BOC is safely tolerated with methadone, with no dose reductions required
96% plasma protein bound
Metabolized by CYP3A, 2C8 and glucuronidation
TPV: No effect on buprenorphine pharmacokinetics
BOC Monograph: ↑ or ↓ buprenorphine
Clinical monitoring recommended
Methadone and buprenorphine: Do not inhibit or induce CYP enzymes
Kiser JJ et al. Hepatology 2012;55:1620-1628.

28
TPV + Methadone
No dose adjustment required
Levin J. 46th Annual Meeting of the European Association for the Study of the Liver (The International Liver Congress 2011), Berlin, Germany, 30 March-3 April 2011

29

30
Antidepressants
hep-druginteractions.org/

31
AntidepressantsBOC TPV
Escitalopram
CYP2C19 with a minor contribution by CYP3A4 and CYP2D6
↔ BOC
? ↓ vs ↔ Escitalopram
Conflicting reports
↔ TPV
↓ Escitalopram
Wide therapeutic index but dose may need to be adjusted
Desipramine
Trazodone
↑ Desipramine
↑ Trazodone
May lead to SEs: nausea, dizziness, hypotension, syncope
Use with caution and consider a lower dose
Be aware of potential for reductions in SSRI exposures with TPV and BOC, increase the antidepressant doses as needed
Kiser JJ et al. Hepatology 2012;55:1620-1628.
Levin J. 46th Annual Meeting of the European Association for the Study of the Liver (The International Liver Congress 2011), Berlin, Germany, 30 March-3 April 2011

32

33
Anxiolytics and Sleep Aids• Flurazepam, triazolam highly dependent on CYP3A for metabolism
– Avoid use with BOC and TPV – Consider dose reduction with diazepam
• Zopiclone: Co administration has not been studied but may increase zopiclone concentrations through CYP3A inhibition.
– A clinically significant effect on BOC exposure is unlikely
• Zolpidem: AUC ↓ 42% by TPV and t1/2 ↓ from 4.32 to 3.37 hrs. Higher dose may be required with TPV
Alprazolam (IV)
Midazolam (IV)
Triazolam (IV)
↑ alprazolam
↑ midazolam
↑ triazolam
• No interaction studies with IV benzodiazepines
• Closely monitor for respiratory depression and/or prolonged sedation
• Avoid use and if necessary consider dose adjustment of benzodiazepines
Victrelis Triple monograph. 2011 Merck Canada.Kiser JJ et al. Hepatology 2012;55:1620-1628.

34
Antipsychotics
• No formal drug interaction studies• Predictions must be made based on knowledge of clinical pharmacology
of each agent
• Quetiapine metabolized solely by CYP3A4– Avoid with BOC and TPV when possible
• Aripiprazole – Reduce by half when TPV or BOC are initiated and titrate
antipsychotic dose to effect
• Risperidone Co administration has not been studied but may ↑ risperidone concentrations.
Kiser JJ et al. Hepatology 2012;55:1620-1628.

35
PIs and Steroids
BOC + inhaled budesonide and fluticasone: ↑ budesonide ↑ fluticasone resulting in significantly reduced serum cortisol concentrations
Dexamethasone + BOC: ↓ BOC, dexamethasone = CYP3A4/5 inducerMay result in loss of therapeutic effect, avoid this combination if
possible and use with caution if necessary
Victrelis Triple monograph. 2011 Merck Canada. hep-druginteractions.org/
BOC TPV

36
Antimigraine Agents
hep-druginteractions.org
Ergots: Potential for acute ergot toxicity characterized by peripheral vasospasm and ischemia of the extremities and other tissues.
Rizatriptan: Co administration has not been studied but, based on metabolism and clearance, a clinically significant interaction is unlikely.
Eletriptan: CONTRAINDICATED with TPV due to potential for coronary artery vasospasm, transient MI, MI, ventricular tachycardia, and ventricular fibrillation
Victrelis Prescribing Information, Merck & Co Inc, May 2011.

37
Oral ContraceptivesBOC TPV
Ethinyl estradiol
↓ AUC by ~25 ↓ AUC by ~25%
TPV: ↓ ethinyl estradiol levels ↑ FSH, LH ↓ endogenous progesterone levels loss of contraception efficacy
Progesterone component
↑ drosperinone AUC and Cmax by 99% and 57% resp.
Progestin only contraception is effective, but it is difficult to know with certainty whether BOC would increase the levels of all progestins or if it is unique to drosperinone
May lead to ↑ adverse effects with increased progestin concs. E.g. hyperkalemia
↓ norethindrone slightly (~11%)
Kiser JJ et al. Hepatology 2012;55:1620-1628.
Do not rely on the use of ethinyl estradiol and progestin-based hormonal contraception during triple therapy for HCV and for 2 weeks after the discontinuation of BOC or TPV
BOC + Drospirenone = contraindicated
BOC: Alternative methods of non-hormonal contraception are recommended.
TPV: Alternative methods of contraception should be used when estrogen-based contraceptives are coadministered with TPV.
Tseng A. Toronto General Hospital April 24, 2012

38
Antihypertensive Agents
• ACEI or Diuretics: CYP enzymes are not involved in the metabolism– Drug interactions unlikely
• B-Blockers: Only carvedilol metabolized to some extent by CYP3A4
• ARBS: Irbesartan and losartan metabolized by CYP3A4– Dose reductions could be considered
• Calcium Channel Blockers: Highly reliant on CYP3A – Susceptible to increases in exposure from BOC and TPV– Consider reducing the dose
Kiser JJ et al. Hepatology 2012;55:1620-1628.

39
TPV + Amlodipine
Lee JF et al. Antimicrob Agents Chemother. 2011 October; 55(10): 4569–4574
Mean plasma concentration-time profile of amlodipine following oral administration with and without telaprevir. Error bars represent the standard error of the mean.
Options:
Decrease amlodipine dose
Use ACE-inhibitor
Diuretics

40Source: Toronto General Hospital. http://www.hivclinic.ca/main/drugs_interact_files/DAA-ARV%20int%20table_summary.pdf

41
Contraindications to BOC and TPV
Antifungals: Use ketoconazole, itraconazole, posaconazole and voriconazole with caution

42
Thank You!