TM Prepared for your next patient. Management of ... · Management of Bronchiolitis: A Clinical...
33
Management of Bronchiolitis: A Clinical Update Todd A. Florin, MD, MSCE, FAAP Assistant Professor, Department of Pediatrics University of Cincinnati College of Medicine Division of Pediatric Emergency Medicine Cincinnati Children’s Hospital Medical Center TM Prepared for your next patient.
Transcript of TM Prepared for your next patient. Management of ... · Management of Bronchiolitis: A Clinical...

TM
Management of Bronchiolitis:
A Clinical Update Todd A. Florin, MD, MSCE, FAAP Assistant Professor, Department of Pediatrics University of Cincinnati College of Medicine Division of Pediatric Emergency Medicine Cincinnati Children’s Hospital Medical Center
TM
Prepared for your next patient.

TM
Disclaimers Statements and opinions expressed are those of the authors and not
necessarily those of the American Academy of Pediatrics. Mead Johnson sponsors programs such as this to give healthcare
professionals access to scientific and educational information provided by experts. The presenter has complete and independent control over the planning and content of the presentation, and is not receiving any compensation from Mead Johnson for this presentation. The presenter’s comments and opinions are not necessarily those of Mead Johnson. In the event that the presentation contains statements about uses of drugs that are not within the drugs' approved indications, Mead Johnson does not promote the use of any drug for indications outside the FDA-approved product label.

TM
Objectives Briefly discuss the epidemiology and clinical features
of acute bronchiolitis.
Review the evidence behind currently recommended diagnostic tests and therapies for acute bronchiolitis.
Describe emerging therapies in acute bronchiolitis, including hypertonic saline and high-flow nasal cannula.

TM
Introduction and Definitions A disorder most commonly caused in infants by viral
lower respiratory tract infection. “A constellation of clinical symptoms and signs including
an upper respiratory prodrome followed by increased respiratory effort and wheezing in children less than 2 years of age.” (AAP Guideline 2006)
It is the most common lower respiratory infection in this age group and is characterized by acute inflammation, edema, and necrosis of epithelial cells lining small airways, increased mucus production, and bronchospasm.

TM
Pathophysiology Viral Infection in Upper Respiratory Tract
Spread to Lower Respiratory Tract
Inflamed Bronchiole Epithelium
White Blood Cells Infiltrate Bronchiolar Epithelium
Submucosal and Adventitial Edema
Sloughed, necrotic epithelium and fibrin
plugs airways
Airway Obstruction
- Air Trapping - Atelectasis - Bronchospasm - Ventilation/Perfusi
on Mismatch
Hypoxemia
Presenter
Presentation Notes
Smooth muscle constriction plays little role, thus limited role of bronchodilators

TM
Challenges to Management
Phenotypic heterogeneity
o Isolated episode of viral-induced wheezing
o Episodic wheezing without atopy
o Multiple exacerbations of wheezing associated with asthma
Phenotypes respond differently to treatment
Etiologic heterogeneity

TM
Epidemiology
Bronchiolitis
RSV Isolates
Year Hall CB. Respiratory syncytial virus and parainfluenza virus. N Engl J Med. 2001;344(25)1917–1928

TM
Virology Respiratory syncytial virus
o 50-80% Human metapneumovirus
o 10-20% Adenovirus Rhinovirus Parainfluenza Influenza
Co-Infection Common: 10-30%

TM
Clinical Presentation Rare in 1st month, peaks at 2-5 months Upper Respiratory Infection
o Rhinitis Lower Respiratory Disease
o Tachypnea o Wheezing o Cough o Crackles o Use of accessory muscles o Nasal flaring
Fever in approximately 30%

TM
Diagnostic Testing Large variation in diagnostic testing obtained by clinicians1
Evidence-based reviews do not support any diagnostic tests, including chest radiographs and viral testing, for routine bronchiolitis2,3
Standardization in care has resulted in substantial reduction in diagnostic testing with cost and outcome benefits4,5
Diagnostic testing should be reserved for specific cases 1Florin TA, Byczkowski T, Ruddy RM. Variation in the management of infants hospitalized for bronchiolitis persists after the 2006 American Academy of Pediatrics bronchiolitis guidelines. J Pediatr. 2014; In Press 2Zorc JJ, Hall CB. Bronchiolitis: recent evidence on diagnosis and management. Pediatrics. 2010;125(2):342–349 3American Academy of Pediatrics Subcommittee on Diagnosis and Management of Bronchiolitis. Diagnosis and management of bronchiolitis. Pediatrics. 2006;118(4):1774–1793 4Perlstein PH, Kotagal UR, Bolling C, et al. Evaluation of an evidence-based guideline for bronchiolitis. Pediatrics. 1999;104(6):1334–1341 5Todd J, Bertoch D, Dolan S. Use of a large national database for comparative evaluation of the effect of a bronchiolitis/viral pneumonia clinical care guideline on patient outcome resource utilization. Arch Pediatr Adolesc Med. 2002;156(11):1086–1090

TM
Outline Theoretical Mechanism Evidence Recommendation(s)
TM
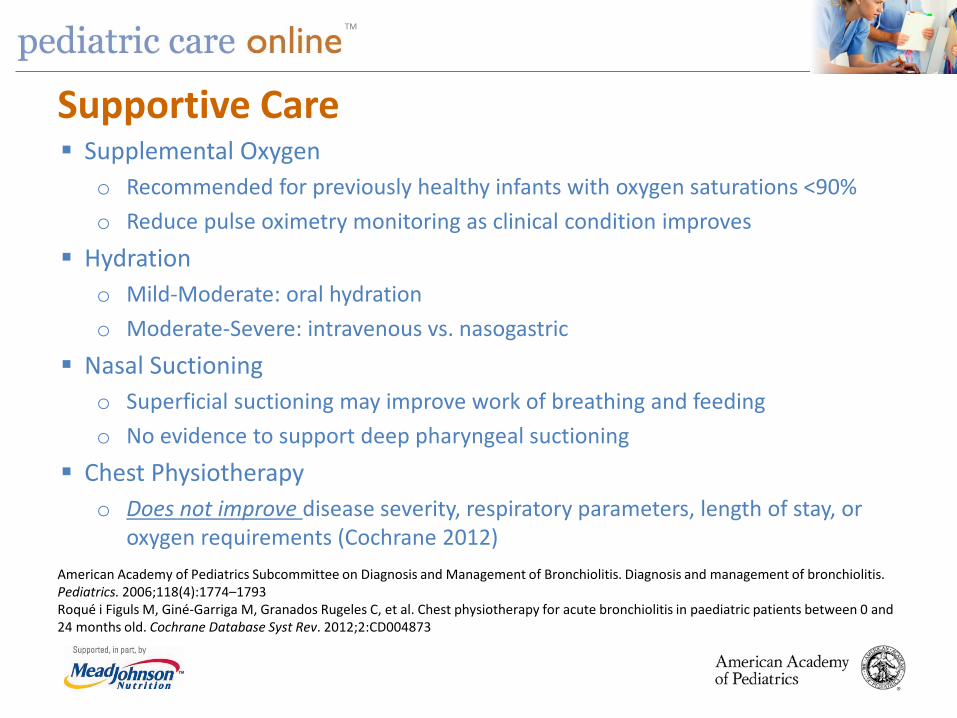
Supportive Care Supplemental Oxygen
o Recommended for previously healthy infants with oxygen saturations <90% o Reduce pulse oximetry monitoring as clinical condition improves
Hydration o Mild-Moderate: oral hydration o Moderate-Severe: intravenous vs. nasogastric
Nasal Suctioning o Superficial suctioning may improve work of breathing and feeding o No evidence to support deep pharyngeal suctioning
Chest Physiotherapy o Does not improve disease severity, respiratory parameters, length of stay, or
oxygen requirements (Cochrane 2012) American Academy of Pediatrics Subcommittee on Diagnosis and Management of Bronchiolitis. Diagnosis and management of bronchiolitis. Pediatrics. 2006;118(4):1774–1793 Roqué i Figuls M, Giné-Garriga M, Granados Rugeles C, et al. Chest physiotherapy for acute bronchiolitis in paediatric patients between 0 and 24 months old. Cochrane Database Syst Rev. 2012;2:CD004873

TM
Bronchodilators: Short-Acting Beta-Agonists Theoretical Mechanism:
o Beta-agonist effects reverse bronchoconstriction
Evidence: o No difference:
• Hospital admission • Length of stay • Oxygen saturation • Length of illness
o Favoring SABA: • Clinical score after treatment • ~25% with transient improvement
o Potential adverse effects
Recommendation: o Not for routine use o Anecdotal experience suggests benefit in a subset of children trial may be appropriate but
should not be continued unless objective evidence of improvement recent evidence recommends against a trial
Gadomski A, Scribani MB. Bronchodilators for bronchiolitis. Cochrane Database Syst Rev. 2014;6:CD001266 American Academy of Pediatrics Subcommittee on Diagnosis and Management of Bronchiolitis. Diagnosis and management of bronchiolitis. Pediatrics. 2006;118(4):1774–1793
Presenter
Presentation Notes
Plot = Hospitalization

TM
Bronchodilators: Racemic Epinephrine Theoretical Mechanism:
o Beta-agonist properties reverse bronchoconstriction, while alpha-agonist properties cause vasoconstriction and reduce edema
Evidence: o Superior to placebo for short-term outcomes
• Hospitalization within 24 hours • Outpatient clinical score
o No difference: • Inpatient clinical course • Vital signs • Length of stay • Readmissions
Recommendation: o No evidence for repeated dosing or prolonged use in inpatients
Hartling L, Bialy LM, Vandermeer B, et al. Epinephrine for bronchiolitis. Cochrane Database Syst Rev. 2011;6:CD003123 American Academy of Pediatrics Subcommittee on Diagnosis and Management of Bronchiolitis. Diagnosis and management of bronchiolitis. Pediatrics. 2006;118(4):1774–1793
Presenter
Presentation Notes
Plot = Hospitalization
TM
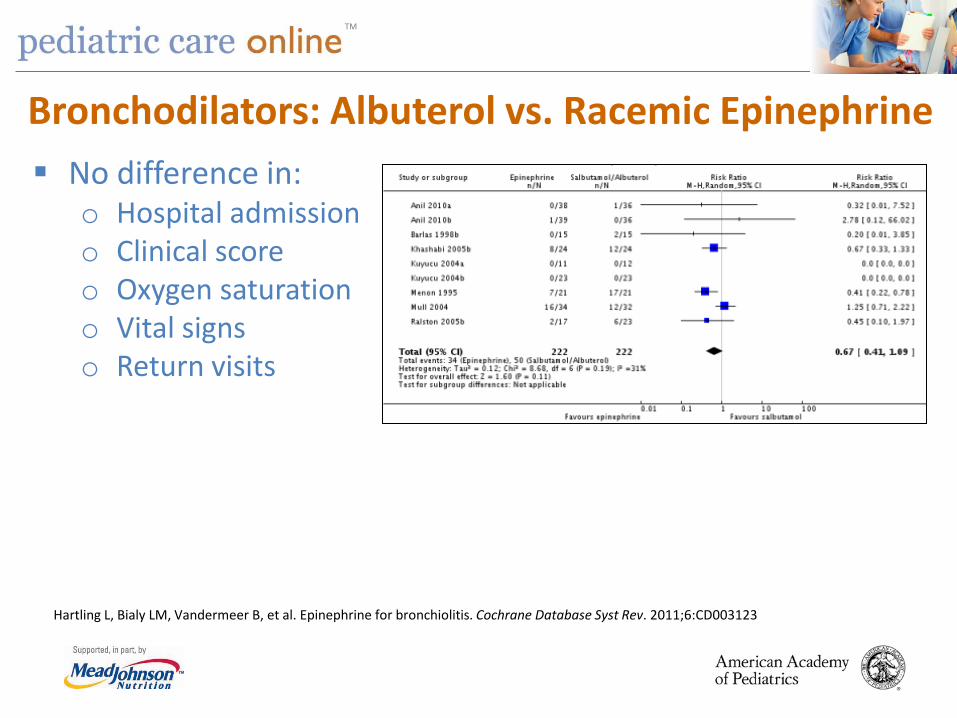
Bronchodilators: Albuterol vs. Racemic Epinephrine No difference in:
o Hospital admission o Clinical score o Oxygen saturation o Vital signs o Return visits
Hartling L, Bialy LM, Vandermeer B, et al. Epinephrine for bronchiolitis. Cochrane Database Syst Rev. 2011;6:CD003123

TM
Corticosteroids Theoretical Mechanism:
o Anti-inflammatory effect
Evidence: o No difference compared to placebo:
• Admissions at day 1 and 7 • Length of stay • Clinical score
Recommendation: o Not recommended for routine use Fernandes R, Bialy LM, Vandermeer B, et al. Glucocorticoids for acute viral bronchiolitis in infants and young children. Cochrane Database Syst
Rev. 2013;6:CD004878 American Academy of Pediatrics Subcommittee on Diagnosis and Management of Bronchiolitis. Diagnosis and management of bronchiolitis. Pediatrics. 2006;118(4):1774–1793
Presenter
Presentation Notes
Dexamethasone fails to produce anti-inflammatory effects in acute RSV bronchiolitis because it lacks sufficient impact on production of inflammatory cytokines that play a major role in the disease (Somers CC. Pediatr Allergy Immunol 2009) Plot = Hospitalization
TM
Racemic Epinephrine PLUS Dexamethasone Theoretical Mechanism:
o Possible synergistic effect between adrenergic agents and corticosteroids
Evidence: o Single, multicenter RCT of 800 infants o 4 groups: Epi alone, Dex alone, Epi+Dex, Placebo
• Epinephrine: 3 mL of 1:1000 x 2 • Dexamethasone: 1 mg/kg (max 10 mg), then 0.6 mg/kg daily x 5d
o Infants in the epinephrine-dexamethasone group were significantly less likely than those in the placebo group to be admitted by day 7 (RR 0.65, 95%CI 0.45-0.95, p=0.02).
o After adjustment, this result was rendered insignificant (p=0.07). Recommendation:
o Insufficient evidence to recommend epinephrine and dexamethasone in combination
Plint A, Johnson DW, Patel H, et al. Epinephrine and dexamethasone in children with bronchiolitis. N Engl J Med. 2009;360(20):2079–2089

TM
Leukotriene Receptor Antagonists Theoretical Mechanism:
o High levels of pro-inflammatory leukotrienes in airways of infants with bronchiolitis
Evidence: o No benefit compared with placebo in randomized trials in acute
symptoms • Does not shorten duration of illness
o May reduce frequency of post-bronchiolitis wheezing o Small, heterogeneous trials
Recommendation: o Not currently recommended
Amirav I, Luder AS, Kruger N, et al. A double-blind, placebo-controlled randomized trial of montelukast for acute bronchiolitis. Pediatrics. 2008;122(6):e1249–e1255 Bisgaard H, Flores-Nunez A, Goh A, et al. Study of montelukast for the treatment of respiratory symptoms of post-respiratory syncytial virus bronchiolitis in children. Am J Respir Crit Care Med. 2008;178(8):854–860

TM
Theoretical Mechanism: o Enhances mucociliary clearance by decreasing mucus viscosity
Evidence: o May decrease hospital length of stay (with longer lengths of stay)
o 7 studies show no short-term improvement in respiratory distress in emergency department; 1 shows decreased admission with 3% saline
o Likely safe without bronchodilators (retrospective) Recommendation:
o May be useful in inpatient setting, likely not useful in emergency department
Hypertonic Saline
Zhang L, Mendoza-Sassi RA, Wainwright C, et al. Nebulised hypertonic saline for acute bronchiolitis in infants. Cochrane Database Syst Rev. 2013;7:CD006458 Florin TA, Shaw KN, Kittick M, et al. Nebulized hypertonic saline for bronchiolitis in the emergency department: a randomized clinical trial. JAMA Pediatr. 2014;168(7):664–670 Ralston S, Hill V, Martinez M. Nebulized hypertonic saline without adjunctive bronchodilators for children with bronchiolitis. Pediatrics. 2010; 126(3):e520–e525

TM
Antibiotics Theoretical Mechanism:
o Concerns for bacterial infection: fever, young age, secondary infections
Evidence: o Low rates of serious bacterial infection (1-12%)
• Urinary tract infection most common o Chest radiograph findings may be misinterpreted o Acute otitis media is frequent (~50%) o RCTs: No benefit of antibiotics in bronchiolitis
Recommendation: o Use antibiotics only in those with specific indications for
bacterial infection (e.g., UTI, AOM) American Academy of Pediatrics Subcommittee on Diagnosis and Management of Bronchiolitis. Diagnosis and management of bronchiolitis. Pediatrics. 2006;118(4):1774–1793

TM
High-Flow Nasal Cannula Theoretical Mechanism:
o Washout nasopharyngeal dead space o Overcome nasopharyngeal resistance with flow o Positive distending pressure o Improved conductance and compliance
Evidence: o Retrospective reviews in PICU1,2
• Decrease need for intubation • Decrease respiratory rate • Decrease PICU length of stay
o Prospective cohort in PICU3 • 13 infants • Increased end-expiratory lung volumes • Improved RR, FiO2, and SaO2
o Only one low-quality RCT—five trials ongoing
Recommendation: o May be useful in severe illness, but insufficient evidence to make a recommendation for
routine use
1McKiernan C, Chua LC, Visintainer PF, et al. High flow nasal cannulae therapy in infants with bronchiolitis. J Pediatr. 2010;156(4):634–638 2Schibler A, Pham TM, Dunster KR, et al. Reduced intubation rates for infants after introduction of high-flow nasal prong oxygen delivery. Intensive Care Med. 2011;37(5):847–852 3Hough JL, Pham TM, Schibler A. Physiologic effect of high-flow nasal cannula in infants with bronchiolitis. Ped Crit Care Med. 2014;15(5)e214–e219
Presenter
Presentation Notes
A heated humidified circuit with a blended oxygen source used to deliver flows that exceed the patient’s inspiratory flow rate with or without an increased oxygen concentration; this eliminates the entrainment of room air and purges the nasopharyngeal space of end expiratory gases

TM
Continuous Positive Airway Pressure (CPAP) Theoretical Mechanism:
o Positive end-expiratory pressure dilates flow-limited airways airway and alveolar recruitment reduces mean airway resistance decreased work of breathing
Evidence: o Small, low-quality studies with mixed results o Some reduction in pCO2, respiratory rate, modified Wood asthma
score
Recommendation: o Insufficient evidence to recommend CPAP o May be useful in severe patients to avoid intubation
Donlan M, Fontela PS, Puligandla PS. Use of continuous positive airway pressure (CPAP) in acute viral bronchiolitis: a systemic review. Pediatr Pulmonol. 2011;46(8):736–746 Thia LP, McKenzie SA, Blyth TP, et al. Randomised controlled trial of nasal continuous positive airways pressure (CPAP) in children. Arch Dis Child. 2008;93(1):45–47

TM
Helium-Oxygen (Heliox) Theoretical Mechanism:
o Helium has lower density than air improve gas flow through high-resistance airways
o Effects rapid (minutes) o Labor intensive
Evidence: o Lower respiratory score immediately after initiation o No reduction in rate of intubation, need for mechanical ventilation,
PICU length of stay o Small studies, heterogeneous methods
Recommendation: o Insufficient evidence for a recommendation—need for larger trials
with homogenous administration Liet JM, Ducruet T, Gupta V, et al. Heliox inhalation therapy for bronchiolitis in infants. Cochrane Database Syst Rev. 2010;4:CD006915
TM
Surfactant Theoretical Mechanism:
o Abnormalities of surfactant quality and/or quantity seen in severe cases of bronchiolitis
Evidence: o 3 small randomized trials (n=79)
• No difference in duration of mechanical ventilation • Duration of ICU stay less in surfactant group • Favorable effects on oxygenation and CO2 elimination • No adverse events or complications
Recommendation: o Insufficient evidence for a recommendation—need for larger
trials Jat KR, Chawla D. Surfactant therapy for bronchiolitis in critically ill infants. Cochrane Database Syst Rev. 2012;9:CD009194

TM
Ribavirin Theoretical Mechanism:
o Broad-spectrum antiviral inhibits RNA and DNA virus replication
Evidence: o PRO: May reduce duration of mechanical ventilation and days of
hospitalization; possible decrease in subsequent wheezing episodes o CON: Small samples sizes, heterogeneous trials, controversial efficacy,
expensive, cumbersome, possible teratogenic and other health effects on caregivers
Recommendation: o Not routinely recommended; may consider for severe disease or those
at high risk for severe disease
Ventre K, Randolph AG. Ribavirin for respiratory syncytial virus infection of the lower respiratory tract in infants and young children. Cochrane Database Syst Rev. 2007;1:CD000181 American Academy of Pediatrics Subcommittee on Diagnosis and Management of Bronchiolitis. Diagnosis and management of bronchiolitis. Pediatrics. 2006;118(4):1774–1793

TM
Home Oxygen Therapy Theoretical Mechanism:
o Mild hypoxia a major reason for hospitalization o Treatment at home for those with hypoxia without other
indications for admission may decrease need for hospitalization Evidence:
o 1 retrospective cohort study and 1 RCT (Denver [high altitude]) o Well tolerated and supported by parents and pediatricians o Median oxygen use = 6 days o <10% ultimately required admission
Recommendation: o Insufficient evidence to recommend o Need more evidence for benefit at sea level
Bajaj L, Turner CG, Bothner J. A randomized trial of home oxygen therapy from the emergency department for acute bronchiolitis. Pediatrics. 2006;117(3):633–640 Flett KB, Breslin K, Bruan PA, et al. Outpatient course and complications associated with home oxygen therapy for mild bronchiolitis. Pediatrics. 2014;133(5):769–775

TM
Palivizumab Theoretical Mechanism:
o Humanized mouse monoclonal antibody Evidence:
o Reduction in RSV-associated hospitalization in high-risk groups: • Chronic lung disease • Congenital heart disease • Premature (<35 weeks gestation)
o No decrease in mortality, rate of recurrent wheeze o Costly—optimal cost benefit with use during peak RSV months
Recommendation: o Administer to high-risk infants in appropriate manner during RSV
season o Not cost-effective or beneficial for routine use in all infants
American Academy of Pediatrics Subcommittee on Diagnosis and Management of Bronchiolitis. Diagnosis and management of bronchiolitis. Pediatrics. 2006;118(4):1774–1793 American Academy of Pediatrics. In Pickering LK, Baker CJ, Kimberlin DW, Long SS, eds. Red Book: 2012 Report of the Committee on Infectious Diseases. Elk Grove Village, IL: American Academy of Pediatrics; 2012
TM
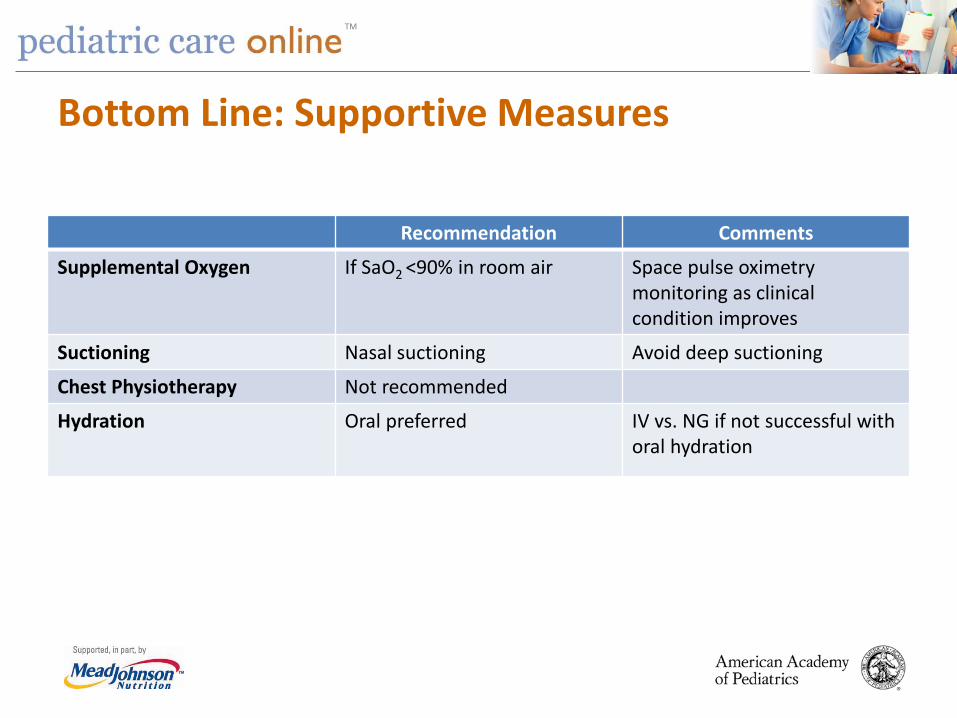
Bottom Line: Supportive Measures
Recommendation Comments
Supplemental Oxygen If SaO2 <90% in room air Space pulse oximetry monitoring as clinical condition improves
Suctioning Nasal suctioning Avoid deep suctioning
Chest Physiotherapy Not recommended
Hydration Oral preferred IV vs. NG if not successful with oral hydration
TM
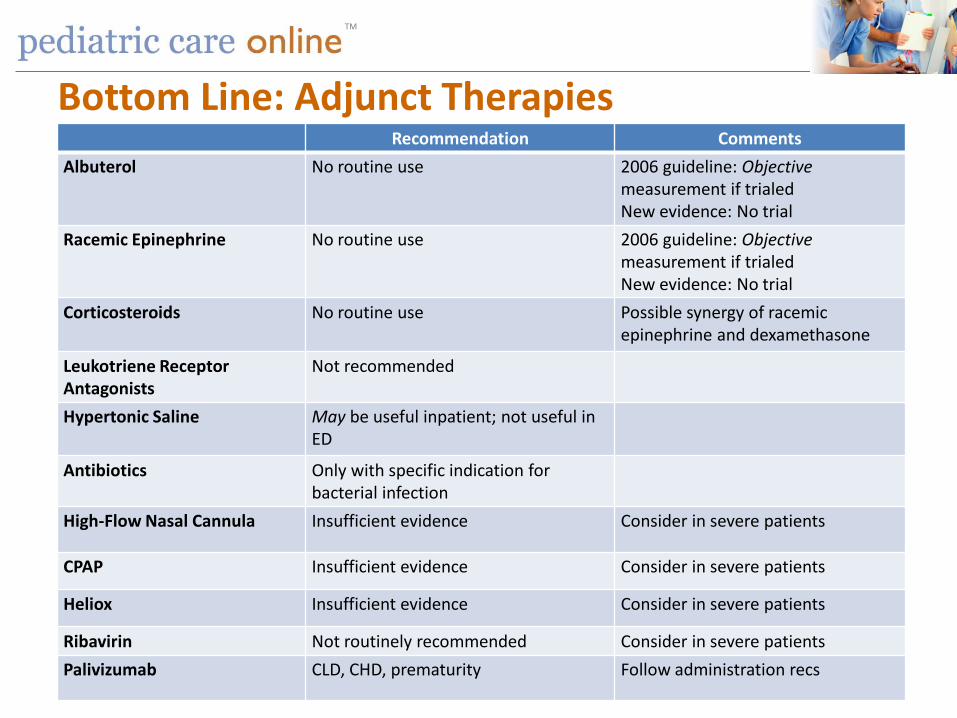
Bottom Line: Adjunct Therapies Recommendation Comments
Albuterol No routine use 2006 guideline: Objective measurement if trialed New evidence: No trial
Racemic Epinephrine No routine use 2006 guideline: Objective measurement if trialed New evidence: No trial
Corticosteroids No routine use Possible synergy of racemic epinephrine and dexamethasone
Leukotriene Receptor Antagonists
Not recommended
Hypertonic Saline May be useful inpatient; not useful in ED
Antibiotics Only with specific indication for bacterial infection
High-Flow Nasal Cannula Insufficient evidence Consider in severe patients
CPAP Insufficient evidence Consider in severe patients
Heliox Insufficient evidence Consider in severe patients
Ribavirin Not routinely recommended Consider in severe patients Palivizumab CLD, CHD, prematurity Follow administration recs
TM
THANK YOU!
TM
Value in Inpatient Pediatrics (VIP) Network (www.aap.org/quiin/vip)
The VIP Network is a healthcare stewardship organization which improves the value of care delivered to any pediatric patient in a hospital bed by helping providers implement clinical practice guidelines and other best practices, with a special focus on eliminating harm and waste caused by overutilization. Visit A Quality Collaborative for Improving Hospitalist Compliance with the AAP Bronchiolitis Guideline (B-QIP) (www.aap.org/quiin/vipbqip) to view recent improvement strategies for bronchiolitis care

Hospitalists are fast becoming the “go to” leaders for inpatient education… It’s a great time to be a pediatric hospitalist! Ricardo Quinonez, MD, FAAP
Section Chairperson
AAP SECTION ON Hospital Medicine
Celebrating 15 years of Accomplishments: 1999-2014 •Founded the first journal dedicated to Pediatric Hospital Medicine (PHM), Hospital Pediatrics. •Edited and published the popular point-of-care manual, “Caring for the Hospitalized Child: A Handbook of Inpatient Pediatrics.” • Drafted the policy statement “Guiding Principles for Pediatric Hospital Medicine Programs,” outlining basic principles for starting and maintaining PHM programs. •Assisted in developing the innovative Advancing Pediatric Educator Excellence Teaching Program. •Established working groups to tackle topics such as certification, neonatal hospital medicine, surgical patient care, and quality. •Created the PHM Abstract Research Award as well as funded numerous grant opportunities and a visiting professorship series. •Supported the early efforts of community hospitalists and PHM fellowship directors. •Expanded educational offerings for residents interested in PHM and founded the first annual Fellows Conference in Park City Utah

TM
Free PCO Trial Visit Pediatric Care Online today for additional information on this and other topics.
www.pediatriccareonline.org
Pediatric Care Online is a convenient electronic resource for immediate expert help with virtually every pediatric clinical information need with must-have resources that are
included in a comprehensive reference library and time-saving clinical tools.
Don’t have a subscription to PCO? Then take advantage of a free trial today!
Call Mead Johnson Nutrition at 888/363-2362 or, for more information, go to
https://www.pediatriccareonline.org/prepared/freetrial.html