TM Current Political and Social Issues in the Prevention and Treatment of HIV/AIDS in Africa Cissy...
37
TM Current Political and Social Issues in the Prevention and Treatment of HIV/AIDS in Africa Cissy Kityo Mutuluuza MD, MSc Deputy Director Research & Clinical Joint Clinical Research Center
-
Upload
magdalene-knight -
Category
Documents
-
view
212 -
download
1
Transcript of TM Current Political and Social Issues in the Prevention and Treatment of HIV/AIDS in Africa Cissy...

TM
Current Political and Social Issues in the
Prevention and Treatment of HIV/AIDS in Africa
Cissy Kityo Mutuluuza MD, MSc
Deputy Director Research & Clinical
Joint Clinical Research Center

The HIV/AIDS burdenThe grim picture of Africa
The World Sub-Saharan Africa
Adults and children living with HIV/AIDS 36.1 million 25.3 million
Adults and childrennewly infected 2000 5.3 million 3.8 million
Death so far dueto AIDS 22 million 15 million
Orphans due to AIDS 14 million 11 million



Main pillars of prevention
• Abstinence
• Be Faithful
• Condom use
• Voluntary Counselling and Testing
• STD Treatment
• PMTCT

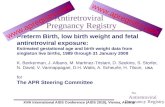
Trends in the Ugandan HIV epidemic
0
5
10
15
20
25
30
35
1989 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000
Years
Rates
(%)
Nsambya Rubaga Mbarara Jinja Tororo Mbale
Rat
es %

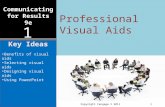
HIV infection trends among pregnant women: Dakar
²for trend: HIV1: p=0.6 HIV2: p=0.6 Prevalence in 1998: HIV1 0.5 (95% CI [0 – 3.0])
HIV2 0.2 (95% CI [0 – 0.7])
0
1
2
3
4
5
1989 1990 1991 1992 1993 1994 1995 1996 1997 1998
Pre
vale
nce
(%
)
HIV1HIV2

Lessons
• Possibility to prevent spread of the epidemic (Senegal)
• Possibility to contain and reduce (Uganda)

What is needed for success?
• Strong and committed political leadership
• Visible ownership by National leaders

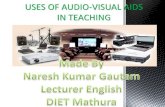
Lag between the first reported AIDS case and initiation of a National AIDS Control Program
0
0.5
1
1.5
2
2.5
3
3.5
4
Uganda(1982)
Rwanda(1983)
Burundi(1983)
Kenya(1984)
Sudan(1986)
Yea
rs

Political commitmentWhat is needed for success?
• Multi-sectoral approach and community mobilization
• Broad awareness of HIV/AIDS in general population
• Efforts to reduce AIDS stigma
• Promote policy/legal changes to prevent discrimination
• National commitment to sex education of youth
• Availability of external assistance in financing and implementation

Prevention vs. Treatment
• Prevention - better than cure
• 25 million Africans already infected and need care
Both treatment and prevention are priorities

Treatment as a preventive tool
• Mother to child transmission prevention
• General transmission
• Promotion of VCT
• Creation of better surveillance
• Stops some children from becoming orphans

Examples of treatment Examples of treatment advantages for Africa - 1advantages for Africa - 1
WITH HAARTWITH HAART WITHOUT HAARTWITHOUT HAART
HealthHealthWell, strong happy Sickly, weak
less/no opportunistic infection Expensive to treat opportunistic
infections
Social economicSocial economicProductive Too ill to work effectively
Self sufficient Dependent and diminishing assets
Family catered for Family suffering e.g no school fees
Able to pay taxes etc Dependent on public services and
Contribution to country soon to leave orphans

Prevention
WITH HAART WITHOUT HAART
Incentive for VCT Testing - so what?
Less likely to transmit virus More likely to transmit virus
Positive living more likely Positive living less likely and stake in the future future looks bleak
Examples of treatment Examples of treatment advantages for Africa - 2advantages for Africa - 2

AIDS patients and availability of ARVs



Response to the AIDS epidemic
• Prevention and Care programs reach fewer than 1 in 5 people who need them
• Proportion of women covered by PMTCT 5%
• Proportion who needed VCT and received it 7%
• Condom use in sex with a non co-habiting partner19%– Over 200 myths, misperceptions and fears that hinder access
to use of condoms
• 60% of primary school students receive basic AIDS education
• Only 1 million people in low and middle income countries were receiving ART by June 2005

The Epidemic in Africa will continue to expand unless HIV Treatment and Prevention are
scaled up dramatically

Scaling up towards universal access by 2010
• Access to HIV prevention, care, treatment and support interventions
• Access is a function of availability, affordability and acceptability
• Coverage indicates the optimal availability and utilization– acceptability, equity and sustainability


Scaling up prevention and care
• Reducing HIV incidence will decrease demand for treatment
• Expanded access to treatment offers an opportunity for prevention efforts– Client initiated VCT– Provider initiated routine offer of HIV testing (STD,
TB & MCH clinics, high prevalence settings)
• Visible treatment success should encourage more open dialogue about HIV
• Care and compassion messages will help reduce stigma

Challenges for achieving universal access - 1
• Insufficient political will in many African countries for sustained evidence based programs
• Multi-sectoral responses are still not a reality in some countries
• Sustainable financing mechanisms (both national and international) are still not in place to meet costs of programs for those in need

Challenges for achieving universal access - 2
• Under resourced and over stretched health systems
• Maintaining a reliable, affordable and adequate supply of quality medicines, condoms and diagnostics
• Financial, cultural and social barriers to access for populations most at risk, affected and in need

Vulnerable groups
• Girls and women
• Women are 30% more likely to be infected than men
• Prevention strategy of ABC not easy – Cultural norms, lack of social and economic power
– Female condoms
• Costs involved in care prevent women and girls from accessing treatment and related diagnostics


Sex workers
• HIV prevalence is generally higher in sex workers than general population
• Prevention programs for sex workers highly cost-effective


Reducing vulnerability
• Initiatives that enhance economic and social development and empower women and girls contribute to effective AIDS responses
• e.g. Universal free education (Uganda, Kenya)– VCT for couples
– Mining companies in S. Africa changing from single sex hostels to family housing for migrant workers

Stigma
• More willingness to seek VCT and avoid transmission
• Acceptance of AIDS victims and involvement in their care

Social economic status
• Cost of ART and related care is a major obstacle to accessing treatment
– Decrease uptake
– Decrease adherence
– Treatment failure

Way forward
• Prevention, treatment and care for:– General population
– High risk populations
– High risk settings
– Special groups

Recommendations
• Generate, improve and sustain national and international political commitment
• Countries in Africa need to scale up HIV prevention and treatment programs based on lessons learnt
• Build on existing structures and strengthen capacity for scaling up interventions

Recommendations
• Foster integration of HIV prevention and treatment
• Greater involvement of PLWAs especially those most marginalized
• Promotion and fulfillment of human rights including gender equality at the highest political level

Recommendations
• Health sector reform is required to ensure that the most efficient and effective models for health delivery are implemented (Primary Health Care)
• Provide treatment and care free of charge at point of service delivery

Conclusion
To have an impact on the future course of the epidemic, successful treatment and prevention
programmes must rapidly become comprehensive programs that reach all those at risk and obstacles to prevention must be swiftly
addressed and overcome