TKCC/Garvan Cancer Biology Seminars Melanoma & Cancer Immunotherapy · 2016. 2. 23. · Clinical...
47
TKCC/ Garvan Cancer Biology Seminars Melanoma & Cancer Immunotherapy 19/02/2016 A/Prof Anthony Joshua Head, Dept of Medical Oncology St Vincent’s Hospital, Sydney
Transcript of TKCC/Garvan Cancer Biology Seminars Melanoma & Cancer Immunotherapy · 2016. 2. 23. · Clinical...
-
TKCC/Garvan Cancer Biology Seminars Melanoma & Cancer Immunotherapy
19/02/2016
A/Prof Anthony Joshua Head, Dept of Medical Oncology
St Vincent’s Hospital, Sydney
-
ImmunotherapyProgress:ALongTimeComing
Joost W et al. Nature Reviews Drug Discovery;10:591-600, 2011.
-
ThreeRequirementsforSpontaneousorTherapeu;cImmuneResponse
Immunization T-cell response
Overcome Immune
Suppression
Mellman, Coukos, Dranoff. Nature 2011;480:480-489
-
ImmunotherapyBalance
• Anti-Cancer – Lymphocytes (CD8
T cells) – Cytokines: IFN-γ,
IL2 – Dendritic cells (DC) – CD40, OX40, TLR
• Tumor Promoting – Lymphocytes (T reg) – Cytokines: TGF-beta,
IL-10, IDO – Suppressive
macrophage – CTLA-4, PD1, LAG3,
TIM3
-
TumorAn;gens Tissue associated antigens
• MART1, gp100, tyrosinase; PSA, her2/neu, mesothelin, CEA, folate receptor-α
Oncofetal/cancer-testis • MAGE family • BAGE family • GAGE family • NY-ESO-1
Universal Antigens • Survivin, hTERT
Neo-antigens • CDK4, β-catenin, mutated introns • New sequences resulting from mutations
-
MSLawrenceetal.Nature000,1-5(2013)doi:10.1038/nature12213
Soma>cmuta>onfrequenciesobservedinexomesfrom3,083tumor-normalpairs.
TumorswithaHighMuta;onalLoad
-
[TITLE]
Presented By Padmanee Sharma, MD, PhD at 2013 ASCO Annual Meeting
-
ImmuneCheckpointPathways
CentralLoca;onAn;gen-Presen;ngCell
CTLA-4Blockade(ipilimumab) PD-1Blockade(nivolumab)CTLA-4Blockade(ipilimumab) PD-1Blockade(pembrolizumab,nivolumab)
Presented By Jedd D. Wolchok, MD, PhD at 2013 ASCO Annual Meeting
-
1stGenerationAgents
-
ImprovedSurvivalwithIpilimumab(An;-CTLA-4)
• Stage IV or unresectable Stage III Melanoma
• Now Health Canada approved 1st line
-
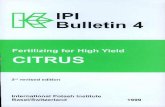
Long-termSurvivalin4846Metasta;cMelanomaPa;entsTreatedwithIpilimumab
Pa;entsatRiskIpilimumab 4846 1786 612 392 200 170 120 26 15 5 0
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
0 12 24 36 48 60 72 84 96 108 120
Ipilimumab
CENSORED
Median OS, months (95% CI): 9.5 (9.0–10.0) Pooled Data: Phase II, III, EAP
3-year OS rate, % (95% CI): 21 (20–22)
Prop
or;o
nAlive
Months
Schadendorf, Hodi FS, Robert et al. ESMO 2013
-
Gattinoni et al. Nature Reviews Immunology 6: 383–393, 2006.
Adop;veCellTherapy(ACT)withTIL
NCI Strategy !• Highly selected TIL!• Rapid expansion protocol!
Lymphodepletion: Cytoxan/Fludarabine!
- Increase IL2, IL7, IL15 availability!- Reduce regulatory T cells!
Administration of high dose IL-2!- Toxic, but fewer doses given!
-
Rosenberg,AACRAnnualMee>ng,2014
-
TILTherapyAcrosstheWorld
1) Dudley/Rosenberg - 50-70% response rates, 22% complete responses (years)
2) Besser/Schacter – 40-50% response rates (57, 5 CR 18, PR) 10% CR
3) Radyvani/Hwu – 48% response rates (15/31, 2 CR) 4) Ellebaek/Svane – 30% response rates (2/6, 2 CR)
5) Pilon-Thomas/Sarnaik – 38% response rates (13 patients; 2 CR, 3 PR
6) Princess Margaret – Canadian trials initiated
-
2ndGenerationAgents
-
Robert C et al. N Engl J Med 2015;372:320-330
Original Article Nivolumab in Previously Untreated Melanoma without BRAF Mutation
UPDATE-the2-yearOSratewithfrontlinenivolumabwas57.7%comparedwith26.7%fordacarbazine.
-
Characteristics of Response.
Robert C et al. N Engl J Med 2015;372:320-330
-
Case
-
Presentation
• 41yearoldpreviouslywell
• Irregularlesiononrightthighforapproximately12months
• Shavebiopsy3.2mm,ulcerated,mitoticrate3/mm2,followedbyWLEandSNB(0/2)
• DeterminedtobeBRAFNeg,NRAS+ve
-
MetastaticPresentation
• InitialCTsclear
• 1yearpostdiagnosisnotedtohavenewmetastaticinfrahilarnode(1.4cm),6mmRLL
nodule
• ReferredforPETscan/EBUS-+veformelanoma
-
Movingtowardstherapy
• ShortintervalCTdemonstratedrighthilarnode(15mm),rightfissuralnodule,RLL
noduleallincreasinginsize
• Alsonewrightinguinalnode(16mm)
-
Pretreatment 2 Months
PartialResponse(78%decreaseinindexlesion@2months):
TILpa;ent1:Clinicalresponse
Otherlesions@2months:Pulmonarynodules-stableRighthilarnodes–absentSubcutlesionRtupperthigh-absent
AfterTILinfusion:[email protected](progression).Pembrolizumab(response).
-
Clinical Experience With NIVO Plus IPI Combination
• Phase I study of NIVO plus IPI in advanced melanoma:1,2 – ORR up to 53% (CR rate of 18%) – 2-year OS rate up to 88%
• Phase II study of NIVO plus IPI in untreated melanoma:3 – ORR of 61% with the combination vs. 11% for IPI alone; CR rate of 22% with
the combination – Treatment-related grade 3–4 adverse events (AEs): 54% for the combination
vs. 24% for IPI
• In the above studies, response rates were similar regardless of PD-L1 expression1-3
1. Wolchok et al. N Engl J Med 2013;369:122-33; 2. Oral presentation by Dr. Mario Sznol at the ASCO 2014 Annual Meeting; 3. Postow et al. N Engl J Med 2015;372:2006-17.
28
-
CA209-067: Study Design
29
Randomized, double-blind, phase III study to compare NIVO + IPI or NIVO alone to IPI alone
Unresectable or Metatastic Melanoma
• Previously untreated
• 945 patients
Treat until progression**
or unacceptable
toxicity
NIVO 3 mg/kg Q2W + IPI-matched placebo
NIVO 1 mg/kg + IPI 3 mg/kg Q3W for 4 doses then
NIVO 3 mg/kg Q2W
IPI 3 mg/kg Q3W for 4 doses +
NIVO-matched placebo
Randomize 1:1:1
Stratify by:
• PD-L1 expression*
• BRAF status
• AJCC M stage
*Verified PD-L1 assay with 5% expression level was used for the stratification of patients; validated PD-L1 assay was used for efficacy analyses.
**Patients could have been treated beyond progression under protocol-defined circumstances.
N=314
N=316
N=315
-
PFS (Intent-to-Treat)
NIVO + IPI (N=314)
NIVO (N=316)
IPI (N=315
)
Median PFS, months (95% CI)
11.5 (8.9–16.7)
6.9 (4.3–9.5)
2.9 (2.8–3.4)
HR (99.5% CI) vs. IPI
0.42 (0.31–0.57)*
0.57 (0.43–0.76)*
--
HR (95% CI) vs. NIVO
0.74 (0.60–0.92)**
-- --
*Stratified log-rank P
-
Response to Treatment
NIVO + IPI (N=314)
NIVO (N=316)
IPI (N=315)
ORR, % (95% CI)* 57.6 (52.0–63.2)43.7 (38.1–
49.3)19.0 (14.9–
23.8) Two-sided P value vs IPI
-
Tumor Burden Change From Baseline
NIVO + IPI Median change: -51.9%
NIVO Median change: -34.5%
IPI Median change: +5.9%
Confirmed responder 30% reduction in tumor burden by RECIST v1.1
32
Bas
elin
e re
duct
ion
from
b
asel
ine
in ta
rget
lesi
ons
(%)
Bas
elin
e re
duct
ion
from
b
asel
ine
in ta
rget
lesi
ons
(%)
Bas
elin
e re
duct
ion
from
b
asel
ine
in ta
rget
lesi
ons
(%)
-
155 171 164
91 97 47
32 34 16
113 115 83
78 83 36
1 1
4 7 3
No. at Risk NIVO + IPI
NIVO IPI
0
0 3 6 9 12 15 18 21 Months
Prop
ortio
n al
ive
and
prog
ress
ion-
free
1.0
0.8
0.6
0.4
0.2
0.0 NIVO + IPI NIVO IPI
0 3 6 9 12 15 18
0.2
0.4
0.6
0.8
1.0
0.0
PFS by PD-L1 Expression Level (1%)
Prop
ortio
n al
ive
and
prog
ress
ion-
free
NIVO + IPI NIVO IPI
123 117 113
65 42 19
26 13 5
82 50 39
57 34 12
0 0
6 2 0
No. at Risk NIVO + IPI
NIVO IPI
Months
mPFS HR
NIVO + IPI 12.4
0.44
NIVO 12.4 0.46
IPI 3.9 --
mPFS HR
NIVO + IPI 11.2
0.38
NIVO 2.8 0.67
IPI 2.8 --
PD-L1 ≥1%* PD-L1
-
Safety Summary
Patients Reporting Event, %
NIVO + IPI (N=313) NIVO (N=313) IPI (N=311)
Any Grade
Grade 3–4
Any Grade
Grade 3–4
Any Grade
Grade 3–4
Treatment-related adverse event (AE) 95.5 55.0 82.1 16.3 86.2 27.3
Treatment-related AE leading to discontinuation 36.4 29.4 7.7 5.1 14.8 13.2
Treatment-related death* 0 0.3 0.3
*One reported in the NIVO group (neutropenia) and one in the IPI group (cardiac arrest).
34
• 67.5% of patients (81/120) who discontinued the NIVO + IPI combination due to treatment-related AEs developed a response
-
AdoptiveTcelltherapy
• UnderwentResectionofinguinalnode
• UnderwentApharesis
• AdmittedforTreatment6weekslaterforTILtherapy
• Fludarabine/CyclophosphamidethereaftersubcutaneousIL2
-
Recovery
• Recoveredwell,playinghockey
• Remainsonpneumocystisprophylaxis
• CTscansshowsignificantimprovement3
monthsposttreatment
-
Relpase
• RestagingMRIalsodemonstratesa1.1cmprecentralbrainlesion
• TreatedwithSRS9monthsfromTILStherapy
-
Relapse2
• Restagingdemonstrateda4.9X1.8cmrightdiaphragmaticmassalongwithgrowthinthe
RLLnodule
-
RESPONSE
-
Vb13.1CD8TCellPopula;onIncreasedwithClinicalResponses
Vb5
.3V
b9V
b18
Vb1
3.1
Vb5
.2V
b23
Vb1
1V
b13.
2V
b7.1
Vb1
7V
b5.1
Vb1
3.6
Vb2
Vb1
Vb2
2V
b4V
b3V
b16
Vb2
0V
b8V
b12
Vb2
1.3
Vb1
4V
b7.2
Unk
now
n0
20
40
60
% o
f CD
8
Vb5
.3V
b9V
b18
Vb1
3.1
Vb5
.2V
b23
Vb1
1V
b13.
2V
b7.1
Vb1
7V
b5.1
Vb1
3.6
Vb2
Vb1
Vb2
2V
b4V
b3V
b16
Vb2
0V
b8V
b12
Vb2
1.3
Vb1
4V
b7.2
Unk
now
n0
20
40
60
% o
f CD
8
Vb5
.3V
b9V
b18
Vb1
3.1
Vb5
.2V
b23
Vb1
1V
b13.
2V
b7.1
Vb1
7V
b5.1
Vb1
3.6
Vb2
Vb1
Vb2
2V
b4V
b3V
b16
Vb2
0V
b8V
b12
Vb2
1.3
Vb1
4V
b7.2
Unk
now
n0
20
40
60
% o
f CD
8
Vb5
.3V
b9V
b18
Vb1
3.1
Vb5
.2V
b23
Vb1
1V
b13.
2V
b7.1
Vb1
7V
b5.1
Vb1
3.6
Vb2
Vb1
Vb2
2V
b4V
b3V
b16
Vb2
0V
b8V
b12
Vb2
1.3
Vb1
4V
b7.2
Unk
now
n0
20
40
60
% o
f CD
8
Vb5
.3V
b9V
b18
Vb1
3.1
Vb5
.2V
b23
Vb1
1V
b13.
2V
b7.1
Vb1
7V
b5.1
Vb1
3.6
Vb2
Vb1
Vb2
2V
b4V
b3V
b16
Vb2
0V
b8V
b12
Vb2
1.3
Vb1
4V
b7.2
Unk
now
n0
20
40
60
% o
f CD
8
PeripheralBlood1W 4W
InfusionProduct
16W 28W
40W 50W 59W 65W
Vb13.1
ResponsetoTILs
ResponsetoPembrolizumab
Baseline
-
Otherpoints
-
43
-
ProgressionversusPseudo-progression
Ribas A et al. Clin Cancer Res 2009;15:7116-7118©2009 by American Association for Cancer Research
-
45
-
irAEsObservedwithNovelImmuno-oncologyTherapy
Ifnotvigilant,mayresultinmoreseriousimmune-relatedadverseevents
Endocrine • Headache• Visualchanges• Fever• Fatigue/weakness• Confusion
Neurologic • Sensoryormotorneuropathy
• Muscleweakness• Fatigue• Difficultywakingup
Hepatic • AbnormalLFTs(eg,AST,ALT,totalbilirubin)
Skin • Skinrashorpruritus
Gastrointestinal (GI) • Diarrhea• Stomachpain• Nausea/vomiting/pain• Bloodinstool• Constipation
ALT:alanineaminotransferaseAST:aspartateaminotransferaseirAE:immune-relatedadverseevent
-
Perc
ent a
live
Immunotherapy Targeted therapy
1 2 Years
3 0 1 3 0 2 Years
Combination
1 3 0 2 Years
Combining immunotherapy and targeted therapy for melanoma?
Perc
ent a
live
Perc
ent a
live