Title – xxx Speaker Implementing paediatric procedural sedation in emergency departments: 2013...
28
Title – xxx Speaker Implementing paediatric procedural sedation in emergency departments: 2013 Ketamine Dr David Krieser FRACP Paediatric Emergency Physician, Sunshine Hospital – Western Health
-
Upload
nathan-clemens -
Category
Documents
-
view
217 -
download
0
Transcript of Title – xxx Speaker Implementing paediatric procedural sedation in emergency departments: 2013...

Title – xxx
Speaker
Implementing paediatric procedural sedation in emergency departments: 2013
Ketamine
Dr David Krieser FRACPPaediatric Emergency Physician, Sunshine Hospital – Western Health

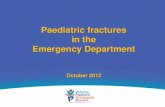
Case
• An 8 year old boy– Monkey bars + Gravity
• FALL– Obvious left upper limb deformity
– Note• Past History• Last intake of solids / liquids• Assessment of injury – neurovascular observations• Pain score and management

Imaging

Why parenteral sedation?
• Some procedures too painful for nitrous oxide
• Alternative to GA in theatre

Why ketamine?
• Predictable response compared with other agents
• IM and IV options
• Maintenance of upper airway tone and reflexes
• Established safety profile

Ketamine in your ED• Ketamine and/or other parenteral agents will not be
appropriate in all EDs.
• Each health services is responsible to determine what procedures & level of sedation in your ED
• If yes
• Policies and procedures are in place
• Staff trained in paediatric life support
• Staff trained and credentialed in use of Ketamine

General principles• Appropriate location• Sedation team:
– Proceduralist + sedation doctor + sedation nurse
– Senior doctor support
• Authorisation• Fasting • Consent• IV agents administered by doctor only• Close monitoring

What is ketamine?
• Dissociative anaesthetic
– Thalamo-cortical input separated from limbic system– Profound amnesia and analgesia – “sensory isolation”– Not a dose dependent effect – a threshold is crossed
• Maintains upper airway tone and protective reflexes
• Cardio respiratory stimulant • There is no reversal agent• Demonstrated as safe in children in EDs

Indications
• Short very painful ED procedures or if immobilisation needed– Fracture reduction– Laceration repair (esp. facial)– Incision and drainage

Contraindications• History of airway problems, delayed gastric emptying• Very unwell• URTI, acute respiratory disease
– Laryngospasm
• Children < 1 year – Airway malposition, respiratory depression
• Children >12 years• History of psychosis / ADHD
– Emergence reaction
• Porphyria, thyrotoxicosis– Sympathomimetic effects increased

Ketamine: Dosing• IV Ketamine
– 1 mg/kg slow IV over 1 minute– Onset 1 minute– Additional doses 0.25-0.5 mg/kg slow IV– Fast push INCREASED RISK of respiratory depression
• IM Ketamine– 4 mg/kg– Onset 3-5 minutes– Additional doses IV 0.25 mg/kg

Comparing IV and IMRoute of administration
Intravenous (IV)
Intramuscular (IM)
Advantages Ease of repeat dosingFaster recovery
No IV needed
Clinical onset 1 minute 3-5 minutes
Duration of effective sedation (approx.)
15 minutes 15-30 minutes
Recovery (approx.) 60 minutes 90-150 minutes
Initial dose 1 mg/kg 4 mg/kg
Subsequent dose 0.25-0.5 mg/kg Insert IV and give further doses 0.25-0.5 mg/kg
Maximum dose 5 mg/kg 5 mg/kg (combined IM and IV)

Ketamine: Parent preparation
• Need to warn parents about ketamine effects:– For IV - tell them it usually works VERY fast
• “like a switch”– Eyes open: may appear awake
• “lights are on, nobody is home”– May move and need restraint – May adopt strange limb positions– May drool– May experience unusual sensations on
recovery / agitation / nightmares– Requires observation period before discharge

Ketamine: Adverse effects• Airway malposition
• Hyper-salivation
• Laryngospasm
• Respiratory depression
• Cardiovascular stimulation
• May elevate intracranial / intraocular pressure
• Ataxia
• Emergence reaction
• Vomiting (recovery)

Ketamine: Emergence reaction
• Hallucinations, dreaming during recovery– More frequent in adults/adolescents
– Risk factors:• female, rapid IV, excessive noise and stimulation,
prior personality disorder
– Reduce risk:• suggest topics for dreaming – Ask before
sedation what the child likes to do and get them to think about it
• dim and quiet environment

Let’s use ketamine
Return to the Case

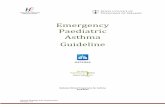
Case
• An 8 year old boy– Monkey bars + Gravity
• FALL– Obvious left upper limb deformity
– Note• Past History• Last intake of solids / liquids• Assessment of injury – neurovascular
observations• Pain score and management

Imaging

StaffKetamine
A doctor, credentialed for the agent used, to administer the sedation and monitor the patient AND a nurse credentialed for paediatric sedation to assist the sedation doctor.
Another doctor to perform the procedure.
Appropriate senior clinician available on site with the ability to immediately respond if required.

Ketamine: The procedure
• Perform only in designated area with full resuscitation equipment available
• IV administration only by a doctor• Give slowly (over ~ 1 minute) to reduce
adverse effects
• Continuous ECG and O2 sat monitoring
• Record observations (including BP) 5 minutely

Ketamine: The procedure• 8 year old boy with forearm fracture
– Weight – 25 kg • Remember topical anaesthetic for IV insertion• Guided imagery; music• Must prepare all equipment for reduction and
plaster as per local guidelines– May include: Image Intensifier (+ radiographer), plaster of
Paris, padding, sling etc
• Consent for sedation AND for procedure– Explain risks

Ketamine: The procedureSuggested prescription
IV administration
1. Calculate the initial dose
2. Draw up into a 1 ml syringe
3. Transfer this (using the drawing up needle) into an appropriate size syringe and dilute with normal saline to a final concentration of 10 mg/ml
4. Administer slowly over 1 minutee.g. 20 kg Child, add 0.2 ml of ketamine to
1.8 ml normal saline = 20 mg/2 ml (10 mg/ml)


Ketamine: The procedureAtropine
• Have atropine available– Calculate the dose = 0.02 mg/kg (20 mcg/kg)
• Write down this calculated dose in case it is needed
– Do NOT draw up – Use only if symptomatic

If you don’t label it… you don’t know what it is• Australian Commission on Safety and Quality
in Health Care• National Recommendations for labeling
– All injectable medicines drawn up should be labeled immediately• Includes flushes, normal saline
– Multiple syringes should be prepared and labeled if required
– Care not to cover volume graduations with label

Other agents
• Include: – propofol– ketamine/propofol (Ketofol) – midazolam (unreliable)– chloral hydrate (non-painful procedures)
• Same principles of safe practice apply

Summary: Key elements• Procedure can occur in your ED• Child is suitable to have ketamine• Child and parent preparation• Standardised processes including
– Consent– Drug management– Documentation – Monitoring– Discharge
• Credentialing of staff• Recognition and management of adverse events

Questions