
Title of the panel - IPPA · Title of the panel Going Universal? Universal Health Coverage on Paper...
39
1 3 rd International Conference on Public Policy (ICPP3) June 28-30, 2017 – Singapore Panel T17a P07 Session 1 Title of the panel Going Universal? Universal Health Coverage on Paper and in Practice Title of the paper Implementing Policy Under A Decentralized And Democratic Polity: Lesson Learned From Indonesian Policy Transition Towards Universal Health Coverage Author Wahyudi Kumorotomo Gadjah Mada University, Indonesia [email protected] Date of presentation June 28th, 2017
Transcript of Title of the panel - IPPA · Title of the panel Going Universal? Universal Health Coverage on Paper...

1
3rd International Conference
on Public Policy (ICPP3) June 28-30, 2017 – Singapore
Panel T17a P07 Session 1
Title of the panel
Going Universal?
Universal Health Coverage on Paper and in Practice
Title of the paper
Implementing Policy Under A Decentralized And Democratic Polity:
Lesson Learned From Indonesian Policy Transition Towards Universal Health Coverage
Author
Wahyudi Kumorotomo Gadjah Mada University, Indonesia
Date of presentation June 28th, 2017

2
Implementing Policy Under A Decentralized and Democratic Polity: Lesson Learned from Indonesian Policy Towards UHC (Universal Health Coverage)
ABSTRACT This study is aimed at explaining the implementation process of a public policy using an Indonesian case, especially the health policy towards a UHC (Universal Health Coverage), an area of policy that is being planned and implemented in many developing countries. Since 2014, the Indonesian government launched a comprehensive policy for more effective social welfare system. Under a grand design of the National Social Security System, two agencies called BPJS (Badan Pelaksana Jaminan Sosial, Social Security Administering Bodies) are set up. The BPJS program on health is targeted to cover at least 121.6 million Indonesian in the first year and would cover all the population in 2019. The government is trying to deal with a far-reaching health-care reform to create a Universal Health Coverage (UHC) that has been in practice in many developed countries. In order to finance the program, the government has worked out two systems. First, individuals living below the poverty line will get financial assistance under the Premium Payment Assistance (PPA). Second, individuals who are employed and able to finance the premium are included in the non-PPA group consisting civil servants, private sector employees, entrepreneurs, military and police officers. However, it is still unclear whether the government is ready to deal with financial provision according to the initiated coverage. The financial shortage might also be expected in providing premium for wage-earners and non-salaried workers. The BPJS finance has run a deficit in the last three years at about 4 percent. Under a decentralized system, there have been issues about coordination of policy and expenditures between the central and regional governments, in the interests of both equity and also efficiency. Deteriorated quality of services in health care have forced well-paid workers to seek higher-quality care elsewhere under a financial scheme of insurance providers. Keywords: democratic governance, health finance, Universal Health Coverage, policy implementation, Indonesia.

3
I. INTRODUCTION
Having been stalled for years, the Indonesian government launched a
comprehensive policy for more effective social welfare system. Under a grand
design of the SJSN (Sistem Jaminan Sosial Nasional, National Social Security
System), two agencies called BPJS (Badan Pelaksana Jaminan Sosial, Social
Security Administering Bodies) have been set up. The first BPJS on health is
initiated under the universal health-‐‑care program, known as Jaminan Kesehatan
Nasional (JKN) or National Health Insurance. This BPJS on health has been
operational since January 2014 by merging four state-‐‑owned companies that
traditionally focusing their businesses on health insurance. The second BPJS will
be launched in July 2015 to offer accident and life insurance as well as pension
programs.
The BPJS program on health is targeted to cover all the population by the
end of 2019. In effect, the coverage target is planned from a process of a
conversion and a registration procedure. The conversion includes 24.5 million
individuals formerly registered under Askes and Jamsostek, the state insurance
provider for public officials and formal private companies' employees, 86.4
million individuals under the community health insurance scheme (Jamkesmas),
and 1.6 million individuals from the military and the police registered under the
scheme of Asabri. The registration is expected to come from individuals who
would see the benefit of having a health insurance under the government-‐‑
administered system.
It appeared that the Indonesian government is trying to deal with a far-‐‑
reaching health-‐‑care reform to create a Universal Health Coverage (UHC) that
has been in practice in many developed countries. The JKN covers
comprehensive benefits from infectious diseases such as influenza to expensive
medical treatment such as heart surgery, dialysis and cancer therapies. In order
to finance the JKN, the government has worked out two systems. First,
individuals living below the poverty line will get financial assistance under the
PBI (Penerima Bantuan Iuran, Premium Payment Assistance). Second,
individuals who are employed and able to finance the premium are included in

4
the non-‐‑PBI group consisting civil servants, private sector employees,
entrepreneurs, military and police officers.
However, it is still unclear whether the government is ready to deal with
financial provision according to the initiated coverage. In 2014, while the
government has increased budget allocation for Jamkesmas from Rp 8.29 trillion
to Rp 19.3 trilion, the minimum premium remained at Rp 19,225 ($ 1.57) per
person. The financial shortage might also be expected as the premium collected
from wage-‐‑earners and non-‐‑salaried workers would not be enough to finance
health services. Dr. Fahmi Idris, the director of BPJS, was quoted as saying that
until December 2014, the government could only collect Rp 41 trillion from the
premium while the claims liability has amounted to Rp 42.6 trillion, a mismatch
of 103.88 percent (Kontan, 17 Feb 2015). Nevertheless, according to the
government plan, the proposal to raise the premium from Rp 19,225 to Rp
27,500 would only be materialized in 2016.
In order to avoid insolvency in the JKN system, the Ministry of Health has
set low reimbursement levels for hospitals. Although most of the hospitals have
signed up for JKN, the low reimbursement might eventually dampen the interest
of private clinics and hospitals, which lead to overcrowding in state hospitals.
Another possibility is that the deteriorated quality of services in health care
would force well-‐‑paid workers to seek higher-‐‑quality care elsewhere under a
financial scheme of insurance providers.
This study is aimed at explaining the implementation process of the
Indonesian new health-‐‑care system administered by the BPJS with the focus on
financial aspect. As a national policy involving millions of citizens, it is important
to understand how the JKN will affect the government budget, whether the policy
is financially solvent, and whether the targeted coverage is realistically
sustainable. Aside from describing the national picture of the JKN policy, the
study will be explaining its implementation at the regional level.
The analysis is conducted based on the available online data on the
national government budget, especially from the master plan of the SJSN and the
JKN schemes that are published by the Indonesian Ministry of Health. In order to
get the international perspectives, comparative analysis will be exercised using
the experience of countries adopted or those that are in transition towards the

5
UHC. Policy notes, journals, and references that are available in the WHO
headquarter and UNRISD were referred to conduct the analysis. Aside from the
available online resources and WHO library, interviews and discussions with
experts in Graduate Institute of International and Development Studies,
University of Geneva, are also carried out.
In Indonesia, statistics on local hospitals, clinics, diagnostic centers, and
the available human resources such as doctors, nurses and paramedic officers
are collected from the local Dinas Kesehatan (Local Agency of Health) and public
hospitals. Interviews with the director of regional BPJS and the Jamkesda were
undertaken to understand what has been happening on the ground. Some
additional interviews with stake-‐‑holders and medical doctors and patients who
registered into the BPJS system have also been undertaken.
The master plan for implementing JKN has been laid out by the Ministry
of Health in the Road-‐‑Map for National Health Insurance 2012-‐‑2019, a
complicated and ambitious policy for a country that is targeting universal
coverage for 252.8 million people. Table 1 describes the main elements of JKN.
Table 1. Financial Plan for Indonesian Universal Health Coverage
Resource Collection Pooling Purchasing / Provision Government budget to public facilities.
Existing funds to be pooled and managed by BPJS.
Payments to public and private health facilities.
Government contribution for poor and near-‐‑poor: Rp 22,000 -‐‑ 27,000 ($ 2.2 -‐‑ 2.7) per month.
Jamkesmas Jamkesda (some) Askes Asabri Jamsostek. 2014 target: Rp 121.6 million covered.
Public Health Clinics and private providers: capitation. Hospitals: Diagnosis Related Groups (INA-‐‑CBG) based payments to be negotiated and varied according to region.
Self funded contributions. Laborers: 5-‐‑6% of monthly wages. Non-‐‑wage laborers / informal sector: 5-‐‑6% of monthly wages. To be covered partly by the government.
2019 target: Entire population, including the remaining Jamkesda scheme. Total predicted coverage in 2019: 256.5 million people.
Benefit packages: Comprehensive. Initially third-‐‑class hospital for government funded and second-‐‑class hospital for self funded. Target: second-‐‑class for all by 2019.
Source: Road-‐‑map of JKN; Mboi,2014

6
According to the plan, the transformation of five existing schemes
(Jamkesmas, Askes, Asabri, Jamsostek, and parts of Jamkesda) into a single
scheme under BPJS should be completed in 2014. Then, the BPJS will manage the
health insurance scheme for all people who have paid the premium and all for
whom it has been paid. As explained earlier, the BPJS system will cover both the
premium payers as well as poor individuals whose premium is paid by the
government under the Premium Payment Assistance (PBI). Monthly premium
and membership fee (4.5% of salary) are made compulsory for all the workers,
and the registration is to be completed in mid 2015. By 2017, all big and medium
enterprises are expected to have the scheme. By 2018, the small enterprises are
targeted to join. And by 2019 all Indonesian citizens and foreigners who work
permanently in the country should be covered by the BPJS scheme.
At the international level, studies on the transition of health financing
towards universal coverage are still lacking or fragmented at best. According to
Savedoff (2012), there are typically four areas of study on health financing; First,
studies that address the growth in health spending and are mostly concerned
with efforts to reduce costs and improve cost-‐‑effectiveness. Second, studies on
the rising share of pooled funding that are usually focus on institutional issues
such us the merits of public and private provision, insurance, and services.
Thirds, studies on the effects of public policies like user fees and community
health insurance, the impact of out-‐‑of-‐‑pocket (OOP) expenditures on people's
risks of impoverishment, and generally focus on how to reduce OOP spending on
health. Fourth, studies that try to disentangle causality, asking whether rising
incomes are responsible for improved health or if improvements in health have
driven economic growth.
Under such research mapping, this study relates to the second category
and seeks to provide a better picture on how to raise pooled public fund that is
critical for extending health services to attain universal coverage. How should
decisions are made when there is an issue of government contribution? Given the
coverage that would imply a large number of individuals in diverse regional
health facilities, is the national standard applicable for all the regions? What
should be done if there is a problem of insolvency and financial sustainability?

7
These are the questions during the implementation stage that would determine
the success of health policy in Indonesia.
II. PATHWAYS TOWARD UNIVERSAL HEALTH COVERAGE (UHC)
a. The Social Nature of Universal Coverage
The main issue of health services for the poor is the burden of payments
that have to be born by individuals, that is the so-‐‑called out-‐‑of-‐‑pocket payments.
Around the globe, out-‐‑of-‐‑pocket payments create financial barriers that prevent
millions of people from receiving needed health services. And many of those who
pay for health services are confronted with financial catastrophe and
impoverishment (Carrin et al, 2008). Even some people who have enough
income might eventually confront financial problem when they are getting old or
experiencing health problem and cannot get sufficient insurance to cover health
services.
Therefore, the idea of universal coverage is to protect people, at all
income levels, from financial risks associated with ill health. In all countries, the
question is how to create health financing systems that are able to achieve and
maintain universal coverage. By definition, universal coverage certainly implies
basic social security as it meant to secure access for all individuals to appropriate
promotive, preventive, curative and rehabilitative services at an affordable cost.
One should note, however, that the concept of universal coverage is not based on
subjective judgment of the policy makers. Many politicians say that they have
launched a social health protection and are committed to implement health
finance for all. Yet political statements and program launching is not enough. The
conceptual fault here is that universal coverage sometimes can be used to justify
practically any health financing reform (Kutzin, 2013) while the objective
coverage is not entirely attained. The objective of universal coverage is efficiency
and equity in health resource distribution so that objectivity, transparency and
accountability have to be assured.
Before a country can set up a full-‐‑fledged universal coverage, it usually
takes a route of gradually implementing Social Health Insurance (SHI). The WHO

8
recognizes SHI as a social mechanism for raising and pooling funds to
finance health services, along with tax-‐‑financing, private health insurance,
community insurance, and others (Carrin & James, 2004). In many European
countries, working people and their employers, as well as the self-‐‑employed, pay
contributions that cover a package of health services available to other people,
who then become their dependents or the insurees.
The governments sometimes also pay subsidies into these systems in
order to ensure the financial sustainability. This is something that might be
problematic in most developing countries for two reasons; First, the
governments are not able to collect taxes and enough revenues to support the
subsidy. Second, the contribution should be made compulsory and therefore it
has to be explicitly stated in the law and the government has to enforce the
provision. Therefore, it is important that the government should give attention to
the issues of financial adequacy while expanding coverage can only be attained
through a strong policy determination towards better health services for the
whole society.
One of the most formidable challenges for policy makers is how to make
public contribution compulsory for certain elements of the society so that a large
pool of funding would be enough for universal coverage. It should be noted that
no country has attained universal coverage by relying on voluntary
contributions. There are many possible schemes for health insurance that are
offered by commercial companies, state-‐‑owned enterprises, non-‐‑government
organizations, or community raised funding, but at the end the government
should regulate that the contribution for universal coverage is compulsory.
Once the government makes it compulsory for all the citizens to register
and to contribute to a nationally-‐‑pooled insurance, a necessary condition for
universality is attained. Some middle-‐‑income countries may opt to explore
voluntary prepayment mechanisms as an alternative to out-‐‑of-‐‑pocket payments,
but experts say that this would rarely become a long-‐‑term solution toward a
universal coverage (Kutzin, 2012). For that reason, it is important that the
government understand the ultimate goal of universal health coverage as parts
of social program that needs long-‐‑term vision of national development.
Although the idea of risk pooling is appealing for policy makers in many

9
countries, however, there fact is rather disappointing. The World Health
Organization reported in 2010 that more than half of the world population is
lacking any type of social and healthcare protection. In many cases, lack of health
care services is caused by low level of income in developing countries. Individual
and household health care programs cannot be sufficiently financed as the
governments cannot get enough revenues from taxes and service charges.
Surprisingly, universal coverage is also an issue in developed countries.
The United States of America, for example, is an economic giant and spends more
than 17.9 percent of its GDP (among the highest proportion in the world), yet
15.4 percent of its population remains uncovered by health insurance (US
Census Bureau, 2012; World Bank, 2014). The ineffective free-‐‑market
mechanism to provide health services for the poor is the main reason for many
countries to embrace universal coverage. Therefore, it is encouraging that the
USA and China, the two major economic powers that previously relied on private
insurance for health care, are currently moving back to universal coverage
policy.
Low-‐‑income and middle-‐‑income countries are recently making steps
towards developing health systems that would cover all of its population, a
policy that has been adopted in most European countries since World War II. The
BRIC (Brazil, Russia, India, China) are among the most populated countries
implementing policies toward universal coverage. Countries in Africa, such as
Ghana, Moldova and Rwanda are adopting the new health systems to cover all
the citizens. In Asia, similar policies have been implemented in Kyrgystan,
Malaysia, Thailand and Indonesia.
In Europe, universal coverage emerged from a belief in solidarity, a fear of
revolution, and a changing view of the role of the state. Substantial benefits
accruing from universal health care have been acknowledged from the
experience of European countries, especially Germany, France, England,
Netherlands and Switzerland, which have implemented the policy since the end
of World War II. However, even when the policy has been in practice for decades,
the universal benefits cannot be taken for granted. Recently, due to economic
slow down in some parts of Europe, universal health care is under a threat
(McKee, 2013). Even in well developed European countries, radical austerity
10
policies posed a threat for universal health coverage, particularly in countries
where the governments perceived serious moral hazards in their social security
programs.
That is why strong national leadership and long-‐‑term commitment are
essential to achieve and sustain universal coverage policy. Experience from
middle-‐‑income countries tells how national leadership in can be critical in the
overall goal achievement. For example, the national government in Turkey
clearly stated that it is illegal for a hospital to retain patients who are unable to
pay for a healthcare service (Atun et al, 2013). Such a measure was taken under a
comprehensive health plan started in 2003. Although Turkey is still in progress
towards an appropriate scale of equitable coverage, its clear policy on access and
affordability would help a long the way.
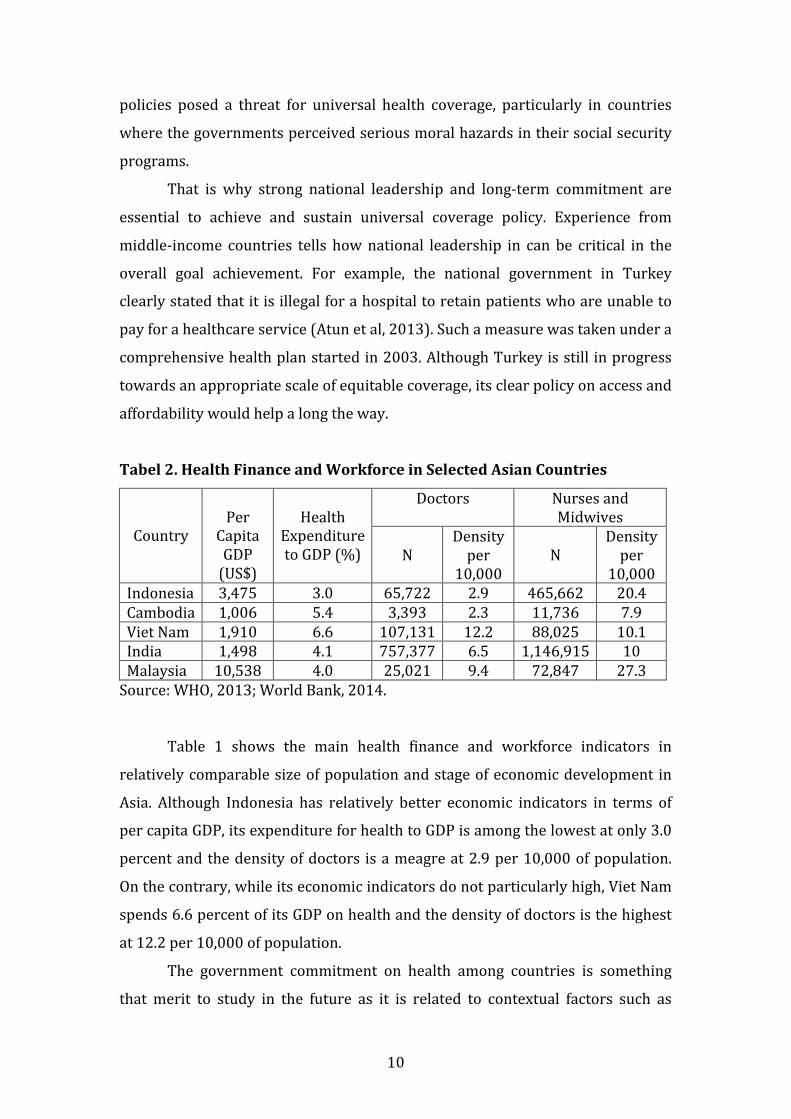
Tabel 2. Health Finance and Workforce in Selected Asian Countries
Country
Per Capita GDP (US$)
Health
Expenditure to GDP (%)
Doctors Nurses and Midwives
N
Density per
10,000
N
Density per
10,000 Indonesia 3,475 3.0 65,722 2.9 465,662 20.4 Cambodia 1,006 5.4 3,393 2.3 11,736 7.9 Viet Nam 1,910 6.6 107,131 12.2 88,025 10.1 India 1,498 4.1 757,377 6.5 1,146,915 10 Malaysia 10,538 4.0 25,021 9.4 72,847 27.3 Source: WHO, 2013; World Bank, 2014.
Table 1 shows the main health finance and workforce indicators in
relatively comparable size of population and stage of economic development in
Asia. Although Indonesia has relatively better economic indicators in terms of
per capita GDP, its expenditure for health to GDP is among the lowest at only 3.0
percent and the density of doctors is a meagre at 2.9 per 10,000 of population.
On the contrary, while its economic indicators do not particularly high, Viet Nam
spends 6.6 percent of its GDP on health and the density of doctors is the highest
at 12.2 per 10,000 of population.
The government commitment on health among countries is something
that merit to study in the future as it is related to contextual factors such as

11
political history, education, and culture. The similar notion also applies when one
should analyze the transition towards universal coverage for health services.
b. Indonesian MoH Road Map
The Ministry of Health has set up an action plan for BPJS Kesehatan
consisting six task forces that are responsible for the following implementation
areas:
a. Health facilities, referral system and infrastructures;
In total, the country provides 2,302 hospitals with 264,303 beds. There
are 40 medical doctors, 11 dentists, 75 midwives and 158 nurses for
every 100,000 population.
b. Finance, transformation of programs and institutions;
Setting premiums and tariffs are among the crucial task for the BPJS. The
transformation of existing insurance and health schemes (Jamkesmas,
Askes, Jamsostek) into a universal health insurance is in progress.
c. Regulatory supports for implementation;
Government Regulation No.101/2012 on the beneficiaries of government
subsidy and Presidential Decree No.12/2013 on social health insurance
have been operational. However there are more technical regulations,
MoH decrees, and procedures for health insurance scheme to be
formulated and implemented.
d. Human resource and capacity building;
It is to develop human resource mapping, distribution, and assignment. As
the universal health insurance requires new approach in managing
hospitals, doctors, nurses and other human resources, new mind-‐‑set is to
be disseminated among them.
e. Pharmaceutical and medical devices;
The tasks include developing e-‐‑catalogue for national medical system,
setting formularies for drugs and medical devices, and establishing a
Health Technology Assessment that is responsible for supervising
pharmaceutical industries.
f. Socialization and advocacy;

12
This task-‐‑force is responsible for preparing materials, strategies, and
media for national campaigns or socialization. It remains to be seen
whether the 2019 target of creating a single healthcare system is realistic
enough to be completed.
In accordance to the MoH Decree No.69/2013, the BPJS adopts the latest
version of Indonesia Case Based Groups (INA-‐‑CBG) tariff as its pattern for
processing and paying medical claims. The INA-‐‑CBG is a diagnostic
reimbursement system that replaced the previous fee-‐‑for-‐‑service
reimbursement system. After being launched on January 2014, the BPJS has
collected Rp 5.4 trillion ($ 475.2 million) in premiums and paid out Rp 1.04
trillion in claims to hospitals. Most of high-‐‑rank officials in the MoH believe that
BPJS will be financially strong in the long run.
However, many hospital managements and doctors do not share those
beliefs. Increased numbers of BPJS members seeking hospital services under the
JKN program have led public hospitals struggling with expenses. Indicative
observations also noted that many poor patients have been rejected by public
hospitals. The patients have been desperately seek appropriate beds for medical
treatments in the Community Health Service and Type C hospitals as the
management declares that all beds are fully occupied. The hospital managements
worry that they would face financial insolvency if they accept all the poor patient
applications (Tijan, 2014).
The financial consequence of universal health insurance for the national
budget is something that has not been made public, including the plan of
president Joko Widodo who keen on making Kartu Sehat (Health Cards) in line
with the BPJS system. Already in April 2014, Minister of Health Nafsiah Mboi
stated the need to revise healthcare tariff for JKN by arguing that the health
facilities and medical workers paid less than what procedures cost (National
News, Jakarta, 01/04/2014). The contribution rate will ultimately have to be
increased if the benefit is higher, or else the benefits will ultimately have to be
reduced in order to keep the cost the same (World Bank, 2012). Again, this
indicates that continuous assessment on the INA-‐‑CBG tariffs is one of the
prerequisite to ensure BPJS financial viability, a big task for Mrs. Nila Moelok, the
newly appointed Minister of Health.

13
As a single entity allowed to collect medical funds for all Indonesian
citizens, the BPJS will have an enormous power to ensure that all the services
provider (hospitals, clinics, doctors, diagnostic centers) to follow the standards
for quality, efficiency, timeliness and service effectiveness. This will in effect
abolish fee-‐‑for-‐‑service system that is proven to be costly. However, the JKN
system is still unclear about how to make the BPJS held accountable to the public.
A supervisory body at the national level is yet to be established. Another
uncertainty is how the government will impose sanctions on employers and
employees who fail to participate in the BPJS programs. The BPJS registration is
currently conducted on voluntary basis and ultimately there are risks that the
universal health coverage cannot be completed according to the plan.
III. CONNECTING FINANCE WITH GOALS: THE BPJS PERFORMANCE
a. Coverage
In order to assess the effectiveness of Indonesian health finance policy to
cover health services for the population, it is important to consider how has been
the performance of the BPJS in integrating various health schemes in the country.
As a health scheme specifically targeted for the poor and near-‐‑poor, the
Jamkesnas is now managed by the BPJS. Jamkesnas program was started in 2005
as Askeskin, literary means health insurance for the poor. In 2007, the Askeskin
that was originally based on households was renamed Jamkesmas to be based on
individuals and expanded to also cover the near-‐‑poor. With the official estimates
indicate that there are 76.4 million poor and near-‐‑poor beneficiaries of the 252.8
million total population in 2014, the BPJS is managing formerly Jamkesmas to
cover almost one third of the population.
With the funding of about a quarter of the central government budget on
health, the BPJS handling on Jamkesmas target is likely determine the Indonesian
government intention to attain a universal coverage. It is therefore important to
analyze the whole institutional arrangement for health policy in Indonesia as
administrative efficiency is also a key factor determining the quality and the
coverage of health services in the country.

14
Indonesia spent 3.0 percent of its GDP on health with the total health
expenditure per capita of US$ 104.25 in 2014. The public spending accounted for
41.1 percent of the total health expenditure and almost half of the public
spending was at the district level. As described earlier, this level of spending is
relatively low among countries with comparable levels of income. And, due to
decentralization policy started in 2001, the effectiveness of health spending
might even lower as it depends on how the district governments spend their
budget on health. Under Indonesia's decentralized system, provincial and district
governments are responsible for health service delivery and that is why they
account for nearly half of the government spending on health.
Since 2014, the BPJS is aimed at integrating Jamkesmas, Jamsostek, Askes,
and Jamkesda (which actually means insurance schemes managed by provincial
and district governments). However, it turned out that most of Jamkesda
schemes are currently managed by the provincial and district governments.
There have been resistance from some of the provincial governors and district
heads to fully integrate to the BPJS systems on the grounds that most
beneficiaries at the local levels are in favor of the Jamkesda and they have been
registered by the Jamkesda. As a compromise, the BPJS is applying the so-‐‑called
"bridging" program for registration and for reimbursement of health services
provided by public as well as private hospitals. Therefore, in many provinces and
districts the Jamkesmas is complemented and even substituted by the Jamkesda
Based on the SHA (System of Health Accounts) for Indonesia (Soewondo
et al, 2011), it is also indicated that 51.6% financial resources for healthcare
provision is carried out by public and private hospitals. Nevertheless, the
institutional picture is actually more complicated. At the community level,
healthcare services are undertaken by voluntary workers in the Poskesdes
(Village Health Posts) and Posyandu (Integrated Service Posts). Voluntary
midwives and nurses work at the Poskesdes to provides curative services.
During a monthly gatherings, voluntary workers run the Posyandus that are
assisted by a doctor and nurses from the Puskesmas (Sub-‐‑district Health Clinics)
and the Pustu (smaller scale Puskesmas). In 77,465 villages throughout the
country, there are 53,152 Poskesdes' and 268,439 Posyandus.

15
Puskesmas and Pustu at the sub-‐‑district level are managed by a medical
doctor and assisted by nurses and midwives to carry out basic health services.
Six basic services for the Puskesmas and Pustu include: 1) health promotion, 2)
environmental health, 3) maternal and child health services (including family
planning), 4) community nutrition program, 5) prevention and eradication of
communicable diseases, and 6) basic medical treatments. The number of
Puskesmas and Pustu has increased from 7,699 in 2005 to 9,321 in 2011, which
means an average growth of 3.5 percent per annum (Suryahadi et al, 2014). Due
to geographical and financial diversity across the districts, however, there is
diversity in Puskesmas and Pustu services. In some urbanized districts,
Puskesmas may have inpatient facilities and more comprehensive medical
treatments. But in remote districts of Maluku or Papua islands, the Puskesmas
may not have a professional medical doctor while medicines and treatments are
severely lacking.
The total number of hospital in Indonesia has increased from 1,145 in
2000 to 2,302 in 2014. The inpatient facilities are also improved as the total bed
number increased from 107,537 to 264,303 in the same period. Nevertheless, as
also indicated earlier, the bed to population ratio in Indonesia is still among the
lowest among East Asian and Pacific countries. The Ministry of Health
categorizes general hospitals into classes: Class A with more than 400 beds,
certain number of specialized medical doctors, and advanced equipment; Class B
with 200-‐‑400 beds, some specialized doctors and standard equipment; Class C
with 100-‐‑200 beds, general medical doctors and basic equipment; and Class D
with 50-‐‑100 beds with mostly general medical doctors. As explained, Class A and
B hospitals tend to be available in more urban areas while Class C and Class D
hospitals and Puskesmas are those mostly available in rural and remote areas.
There are also three classes of Special Hospitals with health services focusing on
medical specialties (obstetric and gynecology, ophthalmology, oncology,
dentistry, internist, surgery, urology, cardiology, psychiatry, neurology, etc).
As a middle-‐‑income country with GDP per capita of US$ 3,475 in 2014 and
enjoyed good economic growth rates in the last few decades, Indonesia has made
impressive health gains. Life expectancy at birth has increased from 45 years in
1960 to almost 70 years in 2010. Infant mortality rate has dropped from 128 per

16
1,000 live births to 27 per 1,000 live births in the same period. However, poverty
and poor health services continue to be a fundamental issue in the country.
About 18 percent of its population continues to live below US$ 1 a day.
Malnutrition rates are particularly high as reflected in the fact that 35.6 percent
of Indonesian children under 5 are stunted. The government envisioned that
issues on poverty and health services could be addressed by Jamkesmas
program.
Figure 2. Out-‐‑of-‐‑Pocket (OOP) Shares of Total Health Expenditure (%)
Source : WHO, SUSENAS.
Figure 3. Insurance Coverage Among Three Population Groups
Source: Adapted from Thangcharoensathien, 2011; MoH, 2014
46.6 48.2
41.844.7
49.1 47.2 45.442.5
14.418.1
27.2 28.1 26
36.2
46.3 47.2
0
10
20
30
40
50
60
1995 1998 2001 2004 2007 2010 2013 2015
OOP shares
Insurance Coverage
16% 20%
64%
100%
15%20%
13%
48%
0%
20%
40%
60%
80%
100%
120%
Formal sector
The poor Informal sector
Total
Population
Insurance Coverage

17
The access and the quality of health care facilities remain a problem in
Indonesian remote districts. Starting from 2010s, the health insurance coverage
has surpassed the percentage of out-‐‑of-‐‑pocket spending. Yet even after the
establishment of BPJS and further implementation of Jamkesmas, the out-‐‑of-‐‑
pocket spending in the country in 2015 is predicted to remains high at 42.5
percent (Figure 2), far above the WHO recommended rates of 15 to 20 percent.
One should note that the WHO recommended rates of 15-‐‑20 percent are based
on the assumption that only at those levels is risk of impoverishment due to
catastrophic health spending generally found to be low (WHO, 2010).
Although the BPJS program may help Indonesia to catch up international
standard of coverage, the challenge is formidable given its sheer size of
population and its diverse targets. Figure 3 shows that while the formal sector
workers have been mostly covered by insurance schemes and the poor may be
covered under the PBI scheme, only 13% of informal sector workers are covered
by health insurance. These are the people belong to the precarious group who
can be impoverished once a family member is severely sick and the family have
to bear the out-‐‑of-‐‑pocket burden of health services.
The existence of prepayment system does not guarantee financial
protection. The international experience has proven this caveat. For example, in
India, 15% of individuals enrolled in the Self-‐‑Employed Women Association are
faced financially catastrophic level of payment even after reimbursement for
hospital admission; in China, Chinese Rural Cooperative Medical System covers
only 30% of inpatient expenditure, yet there is relatively a rare case of financial
catastrophes (Thangcharoensathien et al, 2011). Therefore, the Indonesian
authorities should really be careful in assessing the Jamkesnas scheme,
particularly in evaluating whether the scheme is effective in reducing out-‐‑of-‐‑
pocket spending among the poor and near-‐‑poor.
BPJS scheme on healthcare system is designed to cover both the premium
payers as well as poor individuals whose premium is paid by the government
under the Premium Payment Assistance (PBI). All the standards for services,
eligibility for members, and premium rates, are set by the Ministry of Health. To
expand healthcare coverage, the BPJS is responsible for registering health

18
beneficiaries, administering membership, supervising health-‐‑care providers, and
managing claims and complaints. For registering beneficiaries, BPJS and MoH
refers to national statistics that is compiled by the BPS (Badan Pusat Statistik,
National Bureu of Statistics). The providers -‐‑-‐‑ public and private hospitals, health
clinics, and community health centers -‐‑-‐‑ would then claim fees and medical
services provided by the Ministry of Health via the BPJS offices.
For the formal sector workers, the monthly premium and membership
fee (4.5% of salary) are made compulsory, and the registration is to be
completed in mid 2015. For the informal workers, the nearly-‐‑poor and the poor,
the minimum monthly premium under the PBI scheme has been adjusted from
Rp 5,000 (0.6 US$) in 2007 to Rp 19,225 (1.57 US$) in 2014. According to MoH
Decree No.69/2013, the BPJS must adopt the latest version of Indonesia Case
Based Groups (INA-‐‑CBG) tariff as its pattern for processing and paying medical
claims. The INA-‐‑CBG is a diagnostic reimbursement system that replaced the
previous fee-‐‑for-‐‑service reimbursement system.
Based on the estimate that the government finance is targeted to cover
86.4 million with the PBI premium of Rp 19,225 per person per month, the
central government's contribution to BPJS would equal to Rp 19.9 trillion. Since
the government budget in 2014 was only Rp 44.9 trillion, it implies that almost
half of the overall government health budget would be used to finance the BPJS.
Then, the consequence is straightforward: the share for financing other areas of
spending such as salaries and operating costs for centrally-‐‑financed hospitals,
investments in improving supply and much-‐‑needed preventive and promotive
interventions would have to be shrunk. The 2015 budget is allocating Rp 47.8
trillion. With this incremental increase in the government budget, there would
only two possibilities: pending the reimbursement of BPJS claims, or reducing
other expenditure components in health. Without additional funds to cover the
elderly, orphanage children, street children, homeless people and informal sector
workers, the envisaged universal coverage is still a long way to go.

19
b. Composition of Risk Pools
In theory, the fundamental principle of universal coverage affirms that
contributions are not risk-‐‑based but are instead based on ability-‐‑to-‐‑pay. This
principle reflects a desire for equal access to healthcare and a certain degree of
equity in contribution setting. However, the principle implies a problem of the
so-‐‑called adverse selection, where high risks chase low risks out of the insurance
market. Adverse selection is a particular tendency when the health scheme
registration is voluntary and the same benefit package is offered to all those in
the pool (Carrin & James, 2004).
The phenomena of adverse selection can be explained as a moral hazard
in health service. A certain degree of prepayment combined with risk pooling
may result in some individuals being entitled to more health care than they have
paid for. This suggests that individuals may have an excess demand for health
care or aspire for "free" health care as they are confronted with a subsidized
price of health care. Some may argue that moral hazard would not happen in
health as one should expect people to prefer being healthy to demanding care.
However, the reality is that as one get sick, he or she may want to obtain as much
care as possible. Moreover, when there are no financial barriers to demand
health care at various levels of the health care system, people may want to
bypass the lower echelons and demand care from more specialized and
expensive facilities.
The reality of adverse selection and moral hazard in health care seem
occurred when the BPJS started registration and pay for claims from the general
hospitals in the country. Insofar, the MoH rules that while registration is
voluntary, a similar benefit package of health care is offered to those who have
registered. After nation-‐‑wide voluntary registration was started in January 2014,
many people who perceived themselves as having a serious illness rushed to
register in the BPJS offices. Some of the new members are in fact relatively
healthy, but some others had been indicated with acute diseases that needed
urgent medical treatments. Therefore, during the first months of
implementation, the BPJS has to pay a large amount of claims from the
catastrophic disease in many general hospitals.

20
Table 3. Costs of Catastrophic Medical Treatments in General Hospitals (%) Components General Hospital Class
A (N=6) General Hospital Class B
(N=2) Special Hospital
(N=3) CD C S CD C S CD C S
Accommodation 9.86 12.84 13.47 11.74 7.61 13.89 26.69 9.71 11.23 Ward treatment 15.7 9.87 14.79 26.17 9.75 25.15 28.36 8.38 32.12 Laboratory 19.1
9 11.17 23.01 14.94 6.63 11.87 10.85 11.25 12.35
Radiology 2.55 3.05 12.17 5.33 1.55 12.91 3.45 2.98 8.33 Surgery 2.44 21.74 5.29 1.46 12.53 2.61 0.00 32.77 0.00 Non-‐‑surgery 10.4
5 0.05 0.13 0.00 0.00 0.00 0.00 0.00 0.00
Medical rehab 3.12 0.09 1.27 0.00 0.00 0.00 0.00 0.00 2.21 Other treatment 4.74 3.47 2.12 4.69 1.04 5.34 8.78 14.83 2.23 Medicine 28.0
9 37.53 26.46 26.61 11.78 19.96 21.87 20.07 31.42
Medical consumables
3.86 0.18 1.30 9.06 49.12 8.27 0.00 0.00 0.00
Total 100 100 100 100 100 100 100 100 100 Average Costs (Million Rp)
410.0
236.24
228.68
396.13 136.48
305.97
38.22 86.71 62.13
Note: CD: Cardiac Disease C : Cancer S : Stroke Source: Budiarto, 2012; MoH, 2014.
Table 4. Comparison Between Actuarial Costs and Claims from INA-‐‑CBG (Rp) Hospital
Actuarial Costs Claims (INA-‐‑CBG) CD C S CD C S
General (Class A)
83,590,111 90,018,978 69,295,894 93,227,404 71,828,561 16,212,746
General (Class B)
4,079,878 6,867,048 3,271,237 6,936,283 4,495,967 2,977,179
Special 8,190,252 13,692,311 3,657,221 16,647,900 11,999,754 3,217,077 Average 45,568.486 72,554,004 36,255,390 52,127,993 57,818,963 8,240,261 Source: Budiarto, 2012; MoH, 2014.
Table 3 shows the proportion of costs for medical treatment for
catastrophic diseases (cardiac disease with open surgery, cancer, and stroke) in
selected general hospitals. It turns out that the major costs in all hospitals are for
medicine (11.78-‐‑31.42%) and inpatient accommodation (7.61-‐‑26.69%). The
pattern of costs for medicine, accommodation, and ward treatment has
similarities among the three hospital categories. However, surgeries and medical
rehabilitation are only carried out in higher class hospitals, either Class A or
Class B. For non-‐‑surgery treatment, higher class hospitals tend to charge more

21
while for other treatment there is no pattern, but the tendency is that special
hospitals would charge more. An exception for higher cost in Class B for stroke
inpatients is because these patients tend to stay longer in the hospital for ward
treatment, physiotherapy, and other health services.
The data evidently shows that higher class hospitals would charge more
(Table 4). The expense for cardiac inpatient treatment in Class A hospitals is
twenty times higher than that in Class B and ten times higher than that in Special
Hospital. For cancer inpatients, the expense for medical treatment in Class A
hospital is also much higher in comparison to that in Class B hospital and Special
Hospital. For stroke inpatients, between Class B hospitals and Special Hospital
the expense is about the same, but it would be twenty times higher if they go to
Class A hospitals.
Therefore, to ensure financial sustainability with pooled funding it is
important that the so-‐‑called "clinical pathways" or medical referential system
among different hospital classes have to be applied consistently. Within a pooled
funding of general insurance system, a patient with relatively less severe illness
who can be treated in the Puskesmas or Class C hospital should not be allowed to
go to Class A hospital for similar treatment because it would create an excess
demand for health care, which would incur unnecessary costs.
The comparison in Table 4 also suggests that, with an exception for
cancer treatment, the average amount of health care claims under the INA-‐‑CBG
index are higher than the actuarial. Overall, the nominal gap of between actuarial
costs and claims is Rp 2,925,540. This notion is important because most of those
who have registered to the BPJS believed that the nominal claims from INA-‐‑CBG
scheme are lower than what they should pay to the hospitals.
From a macro perspective, this confirms that there has been adverse
selection during the early stages of BPJS registration. Cardiac failures, cancer and
stroke are categorized as catastrophic diseases that imply high costs in the
hospitals. And if the costs cannot be recovered by the pooled fund and the
government subsidy that are being administered by the BPJS, the whole system
would financially fail. Therefore, there are strategic principles that has to be
considered by the decision makers: 1) the sustainability of finance and services,
2) people's ability-‐‑to-‐‑pay for insurance, 3) equity and fairness in health services,

22
and 4) fair competition among hospital managements. Many aspects have to be
taken account to attain expand insurance coverage, and the clinical pathway is
just one of them.
IV. DECENTRALIZED HEALTH SERVICES: THE JAMKESDA
a. Local Budget and Health Financing
It is envisaged in the Road-‐‑Map for National Health Insurance 2012-‐‑2019
that all the financial resources managed by different agencies should be
integrated into a single system under the BPJS. However, in the Indonesian
decentralized political context, it is a tough challenge for the Ministry of Health
to integrate health, let alone the newly established BPJS. The fundamental
fragmentation is between the ex-‐‑Jamkesmas schemes that are presently
managed by the BPJS and the Jamkesda schemes managed by provincial and
district governments. Of the total 34 provinces in the country, only Papua and
West Papua that do not have Jamkesda schemes. Jamkesda funds currently cover
an estimated 31.6 million people in almost all provinces and 352 districts/cities.
Law No.36/2009 national health policy stipulates that 10 percent of the
government budget must be allocated on health. However, most of the provincial
and local governments have not reach this percentage as the average is only 9.56
percent. At the provincial level, the lowest allocation is Riau at 6.57 percent and
the highest is Bali at 12.7 percent. As explained earlier, the Indonesian
government financial commitment on health is relatively weak in comparison to
other countries in the region.
After the political transition into a relatively more democratic
government in late 1990s, there was so much hope that decentralization would
bring the local government closer to the people's need. It was an illusive hope as
most decision makers at the sub-‐‑national government do not give appropriate
attention on health, education, social security, and all elements of public services
that have been badly needed by the local people. Many of the politicians have in
fact spend local budgets more on public official salaries, building monuments,
sport stadiums, and more grandiose projects for their own political populism.

23
As most of the sub-‐‑national governments allocate too little for financing
health programs, the per capita budget for health is also very low from the
international standard. Among the provinces, the national average of health
budget per capita is only Rp 286,665 (US$ 22.05) per person/year in 2014. One
should note that different levels of political commitment among the governors,
fiscal capacity and total population in the provinces are among the critical factors
influencing their budget priority on health. The provincial government of Riau is
among the highest in terms of fiscal capacity, yet they only allocate 6 percent of
the budget on health. On the contrary, Aceh provincial government is among the
lowest on fiscal capacity, but they allocate 10 percent of the budget on health.
While the BPJS encounter difficulties in integrating the local Jamkesda
into a universal scheme, there is also a large variety on how Jamkesda perform in
the provinces and districts. As described in Table 6, the percentage of Jamkesda
member to the total population is highly diverse from 1.89 percent (East Java) to
65.35 percent (South Sumatra). It is somewhat ironical that East Java province,
one of the most populated provinces with more than 37.4 million people, only
registered the least percentage of its people to Jamkesda scheme. It appears that
there is a legal vacuum on how the sub-‐‑national governments should formulate
policies on health. The central government has to acknowledge and support
decentralization policy as it is written in the constitution. However, there should
be some policy instruments to ensure that the sub-‐‑national governments really
undertake health care programs more seriously since it is fundamental for the
whole nation.
Table 6. Jamkesda Membership
No. Province Population Jamkesda Member
% Population
1 Aceh 4,842,238 2,226,352 45.98 2 North Sumatra 12,982,204 1,208,893 9.31 3 West Sumatra 4,846,909 1,141,149 23.54 4 Riau 5,538,367 1,341,395 24.22 5 Jambi 3,092,265 254,167 8.22 6 South Sumatra 7,450,394 4,868,723 65.35 7 Bengkulu 1,715,518 73,560 4.29 8 Lampung 7,608,405 4,513,155 59.32 9 Bangka Belitung 1,223,296 739,027 60.41 10 Riau Islands 1,679,163 174,730 10.41 11 Jakarta Capital
Region 9,607,787 4,300,000 44.76

24
12 West Java 43,053,732 5,082,200 11.80 13 Central Java 32,382,657 2,926,402 9.04 14 Jogja 3,457,491 1,007,153 29.13 15 East Java 37,476,757 706,982 1.89 16 Banten 10,632,166 479,170 4.51 17 Bali 3,890,757 2,440,964 62.74 18 West
Nusatenggara 4,500,212 572,976 12.73
19 East Nusatenggara 4,683,827 725,824 15.50 20 West Kalimantan 4,395,983 585,157 13.31 21 Central
Kalimantan 2,212,089 840,339 37.99
22 South Kalimantan 3,626,616 1,077,575 29.71 23 East Kalimantan 3,553,143 1,868,741 52.59 24 North Sulawesi 2,270,596 490,981 21.62 25 Central Sulawesi 2,635,009 483,968 18.37 26 South Sulawesi 8,034,776 4,892,070 60.89 27 South-‐‑East
Sulawesi 2,232,586 89,643 4.02
28 Gorontalo 1,040,164 495,869 47.67 29 West Sulawesi 1,158,651 48,447 4.18 30 Maluku 1,533,506 657,470 42.87 31 North Maluku 1,038,087 319,196 30.75 32 West Papua 760,422 n.a. n.a. 33 Papua 2,833,381 n.a. n.a. 34 North Kalimantan 723.005 n.a. n.a. National 237,989,154 46,632,278 19,59
Note : North Kalimantan is newly established province in 2012, data on Jamkesda is unavailable Source : MoH, 2014.
In order to assess the performance of Jamkesda, whether or not the
scheme would result in equitable health services that cover all of Indonesian
citizens, there are at least three aspects of health care management to be
evaluated, namely: membership or registration, financial management, and
benefit package distribution. Again, decision makers in Indonesia should learn
from experience of other countries that universal coverage cannot be
materialized within a short time. It needs strong political commitment,
perseverance, and appropriate adjustment during the implementation.
First, the membership to the JKN system depends on how the sub-‐‑
national governments accept the poor families or individuals who come to the
Jamkesda or BPJS regional offices. Some local government authorities admit and
include all the citizens who had not registered in any of the public insurance
system. The only difference is that those who come with enough money would

25
have to pay the premium and those who cannot afford to pay would be
registered under the PBI assistance. There are also other local governments that
essentially register all the citizens with the minimum benefit as a benchmark. It
means that all the citizens are entitled to at least a minimum benefit from the
local government. Those who cannot pay the premium, or presumably the poor
and near-‐‑poor, would be entitled to Level III health care services at the public
hospitals. And those who can afford to pay the premium may aspire for higher
level of health care services. Still, there are two provinces that use rather
procedural approach by registering poor individuals into the Jamkesda scheme
only if they bring the SKTM (Surat Keterangan Tidak Mampu, Poor Family
Identities), a letter of recommendation issued by the Dinas Sosial (Local Agency
for Social Affairs). All these government approaches are likely determine why in
certain provinces the level of membership to Jamkesda is very low while in other
provinces it is surprisingly high as shown in Table 6.
Second, the way provincial governments collect and manage health
insurance funds is critical in the national effort to attain universal coverage.
There are varieties of methods applied by the provincial governments in
determining their member contributions. In general, three methods are applied:
1) Free or no payment, 2) Contribution with the rate below the BPJS standard,
and 3) Contribution with the rate above the BPJS standard. Majority of the
Jamkesda (in 25 provinces) impose contribution with the rate below the BPJS
standard (Rp 19,255 basic premium), while three provinces impose contribution
with the rate above the BPJS standard, and four provinces do not impose any
payment. It means that, although many complained that the basic premium was
too low, the BPJS standard rate has in fact higher than those being applied in
regional Jamkesda.
It would be interesting to check whether the Jamkesda that do not impose
payment can really maintain a good quality for health services and those that
charge more are delivering better benefit packages for the consumers.
Maintaining appropriateness or a fair balance between the premium rate and
health service quality is important though majority of the Jamkesda has seen the
BPJS standard rate as a good reference. Given the diversity in health care
facilities across the provinces, the Ministry of Health should also encourage

26
governors and district heads to develop and maintain hospitals, clinics and other
health facilities and upgrade medical human resources accordingly.
In managing the pooled fund of Jamkesda, some of the provincial
governments are engaged in collaborative contracts with PT Askes (that is
transformed into regional BPJS) and the Dinas Kesehatan (Local Agency for
Health), which together form a Badan Pelaksana (Executing Body) of local health
insurance. There are also certain provincial governments that consider Jamkesda
as a part of the government agencies and its managerial decisions has to be
reported to the governor. The costs of delivering health services for the citizens
under its jurisdiction are to be shared between the provincial and the district
governments. There are 14 provinces in which the costs are fully financed by the
district government. In several provinces that are using traditional approach in
in health care financing, functions are simply separated into two: administrative
function and service function, in which the Jamkesda is to carry out
administrative function such as registration, determining the contribution, and
allocating government budget while hospitals (mostly treated as the BUMD, the
local government public enterprise) and clinics are to carry out health services,
determining tariff for services, and reporting capitation funds.
Third, the benefit package for medical treatment undertaken by the
Jamkesda is also the key indicator on how the government proceeds to universal
coverage. Out of the total 34 provinces in Indonesia, 18 provinces set the benefit
according to the JKN or previously Jamkesmas standard of services. This would
include preventive and curative personal health care, rehabilitative services and
ward accommodation. But in the other 16 provinces, the governments set the
benefit according to their local regulation (Peraturan Daerah). There are two
different reasons why these provinces do not follow the central government
regulation; First, the provincial authorities consider that they are able to provide
better health services than that being offered by the central government, and
therefore they wanted to regulate the benefit under local regulation. Relatively
rich provinces like Jakarta Special Region or East Kalimantan should have been
able to offer more comprehensive services for their citizens. A study in six
provinces, however, found that although provinces use local regulations, the
benefits are similar to those regulated by the central government (Supriyantoro,

27
2014). Second, some provincial authorities do not follow the central government
regulation on the benefit due to financial constraint. These are the provincial
governments that can offer only class-‐‑three services and many elements of the
services are scrapped.
b. The Premium Payment Assistance (PBI) For the first time, Law No.40/2004 on National Social Security System
rules that individuals living below the poverty line will get financial assistance
for their health care under the PBI (Penerima Bantuan Iuran, Premium Payment
Assistance), with the basic amount of Rp 19,225 (1.57 US$). After started the
nation-‐‑wide registration in 2014, the BPJS reported that 86.4 million PBI
recipients have been recorded. The BPJS also stated that the recorded numbers
are still increasing along with the Jamkesda integration into the JKN system.
However, after verifications were carried out in the regions, it also turned
out that many of the PBI registrations were incorrect and presumably the
benefits were miss-‐‑targeted. The Center of Health Finance and Insurance (P2JK)
of the MoH stated that 2,558,490 (2.96 percent) of the total 86.4 million PBI
records were incorrect. These are the number of those who cannot actually be
considered as the poor or near-‐‑poor. In South Sumatra, only 704 PBI recipients
were wrongly recorded and in North Sulawesi the number was only 1,271.
However, in Banten 290,438 (9.01%) PBI recipients of its 3,221,969 population
were wrongly recorded.
At this point, it seems that the notion on incorrect number was a result of
misperceptions between authorities in the MoH, the BPJS and the sub-‐‑national
governments. According to Law No.40/2004, the universal health coverage is
defined as a condition when all the Indonesian citizens are entitled to health
insurances by either paying premiums or being admitted to the public insurance
schemes under the government assistance of the PBI. Meanwhile, many of the
sub-‐‑national government authorities consider that universal health coverage is
to ensure that every citizen in their administrative jurisdictions must be entitled
to a minimum of class-‐‑three health care services. Regardless of their income, all
have the rights to get a medical treatment in class-‐‑three services. Due to this
different understanding about the universal coverage, many of the PBI

28
registrations may have double-‐‑counted or in fact under-‐‑represented in certain
regions.
Admittedly, the issue of data validity on poverty in Indonesia is something
that hindered the effectiveness of various programs in the country. Policies on
Bantuan Langsung Mandiri (BLT), a cash-‐‑transfer to help the poor after the
economic crisis in early 2000s, the labor-‐‑capital program for rural development
under PNPM Mandiri, have been among the miss-‐‑targeted programs due to data
accuracy. Regarding the data on the poor and near-‐‑poor referred by central
government and BPJS, there are possible inconsistencies with regional data
recorded by the Jamkesda. One should note that data on individuals who are
considered as the poor is not static. A poor family may succeed to climb up the
ladder to higher income status when one of its members can get a formal job,
which then help the entire family. On the contrary, a family with decent income
may be suddenly thrown back into poverty if one of its member severely sick and
has to pay out-‐‑of-‐‑the-‐‑pocket health services without additional income. Many of
this so-‐‑called "transient poor" is simply unrecorded by the central government
agency.
While integration is fundamental to pursue universal coverage and to
avoid inefficient funding for health services, there have been good intentions on
the part of sub-‐‑national governments. Many of the governors and district heads
do not want to see near-‐‑poor people are impoverished because they are not
registered in the BPJS system. Therefore, the policies are just to cover all to class-‐‑
three services, though sometimes it is politically labeled as "free health services".
The provincial government of Gorontalo, for example, affirmed that they want to
retain Jamkesda insurance because many of poor people in this province were
not covered by the Jamkesmas and were not registered as PBI recipients by the
central BPJS. Established as a province only in 2002 with a million population,
Gorontalo is governed by authorities who have a better commitment to improve
health services through Jamkesda. Policy coordination among the provincial and
district authorities has been relatively effective in monitoring the PBI assistance.
Gorontalo province is relatively successful not only in helping the poor with PBI
but also in improving local human resources for public health.

29
The Gorontalo approach is different from what has been taken in West
Sumatra. The governor of West Sumatra from the beginning of BPJS registration
has stated that Jamkesda should be integrated to JKN in order to ease the fiscal
burden on the provincial budget. For those who have enough income to buy the
premium, the provincial government urged them to join a program called Jamkes
Mandiri (self reliant health insurance). Therefore, the result is a combination of
locally managed health insurance system and the subsidized PBI system that is
managed under the national JKN.
A rather unsuccessful story is in East Nusatenggara province. The
provincial government has been committed to provide PBI assistance to all of its
poor citizens. They provided a special allocated dana talangan
(floating/reserved funds) from the provincial budget for whoever registered as
PBI members. Unfortunately, the beneficiary data was not accurately verified
while repayment of claims from the local hospitals was not adequately
controlled. For several months, the provincial government budget was
overburdened with health claims from the local hospitals to the extent that other
local development priorities are set aside. As the provincial government was
finally stop the repayment, many of the local hospitals were financially insolvent
to carry out their health services.
There have been various issues on how to allocate financial resources to
assist the poor via PBI scheme, which apparently centered on the integration
between central and sub-‐‑national governments, data accuracy and consistency,
and close monitoring during the implementation so as to ensure accountability
for further progress on health equity and quality. Another shortcoming of
financial health assistance for the poor is the fact that in nearly all regions the
focus of health program has been only on the curative aspect (Gani, 2010). In the
future, the PBI assistance would be more efficient when the authorities manage
to shift the focus onto the promotive and preventive aspects so that curative
treatments can be reduced while the coverage is expanded.

30
c. Jamkesda and Health Services in Jogja Province: A Case In order to understand the implementation of universal coverage policy at
the sub-‐‑national level, a case of the Jamkesda in Jogja Province is presented. The
province of Jogja is relatively small compared to the other provinces as it only
covers 3,185 kilometer square area with a population of 3,340,438 in 2012. It
consists of one city and four rural districts. There are 69 hospitals in the
province, of which 3 are Class A, 11 are Class B, and the rest are Class C, Class D
and non-‐‑classified local hospitals.
Sultan Hamengku Buwono X, the governor of Jogja province, says that the
provincial government prepares 121 Puskesmas, 141 main clinics and dental
service providers, 48 public and private hospitals, three clinical labs, and 11
pharmacies. It is expected that these health facilities would accommodate
2,062,488 individuals who already registered as Jamkesda members. Especially
for the PBI recipients, the provincial government has provided 138 beds of third-‐‑
class facilities, and 60 beds of second and first-‐‑class facilities. In addition, three
units of ambulatory service are also made available for PBI recipients.
According to Governor Regulation No.19/2011, Jamkesda membership is
categorized into three, namely: the PBI recipients whose basic premium are paid
by the provincial government, members or insurees under the COB
(Coordination of Benefits) whose premium are partially funded from cost-‐‑
sharing schemes made available by the provincial and district governments, and
the independent members who are mostly public servants and private company
employees.
Government authorities, BPJS regional officials, and Jamkesda officials are
trying hard to ensure that clinical pathways and medical referential systems are
well functioning in health services. Until November 2014, they had the
experience that many of the applicants to regional BPJS and the newly registered
members rushed to Class A hospitals to get health services, particularly to
Sardjito Hospital, the biggest general hospital in the city. Although Sardjito
Hospital has around 750 beds, it was really hard to reserve a ward
accommodation as everybody wanted to go to this hospital. Therefore, the
government is currently emphasizing the importance of collaborative networks

31
among the Puskesmas, midwives, nurses and paramedics who work in private
clinics and the medical doctors who work in public as well as private hospitals.
According to Dr. Elvy Effendi, the director of Jamkesda, it has been a tough
job to convince all the stake-‐‑holders about the importance of following clinical
pathways and medical referential systems. He has to tirelessly communicate
with medical professionals, officials, and Jamkesda members that the hospitals
can refuse to admit less severe patients who have no reference from the
Puskesmas and lower level hospitals. But moral hazard can take various modus
operandi. A patient may ask for class-‐‑three accommodation when he admitted to
a hospital. Then, while being treated in the ward he would ask to move to first-‐‑
class accommodation as he knew that it would only cost him an extra 40 percent
for accommodation while the medical treatment would follow first-‐‑class
standard.
Things have been more manageable currently as people begin to
understand that they can get standardized services in all Puskesmas, private
clinics, hospitals and pharmacies under Jamkesda jurisdiction. An official at the
Jamkesda claimed that about 70 percent of the medical reference system is
followed. But reducing moral hazard and adverse selection is a hard challenge
for Jamkesda as it closely linked to issue on finance.
Figure 4. Code Entry Accuracy in Panti Rapih Hospital (%)
Source: Nuryanti, 2014.
44.56
3.418.95
18.7624.3
57.12
9.39 9.55 10.3 13.64
0102030405060
Diagnosis
Treatment

32
The other pressing issue is the data accuracy on Jamkesda membership
and the mismatch of health service finance between the hospitals and the claims
to be paid by Jamkesda, both of which would create deteriorating effect on
sustainability. First, it is suspected that there have been double-‐‑counting in
Jamkesda membership. Mr. Effendi said that until end of 2014 there are
1,336,042 individuals registered in Jamkesda (including those insured under
former Jamkesos), leaving 889,198 individuals in the province uninsured.
However, he believes that because many have actually acquired double
insurance under the Jamkesos and Jamkesda, the government should have been
able to expand the coverage to those who are uninsured.
Second, as INA-‐‑CBG system is relatively new for many of the doctors and
computer operators in the hospitals, the overwhelming claims to the regional
BPJS may also due to inaccuracies. Figure 4 shows that in Panti Rapih hospital,
the biggest Class A private hospital in the province, only 44.56 percent of the
diagnosis input to INA-‐‑CBG complies according to correct specification. The fact
that 18.76 percent is mismatched and 24.3 percent is unrecognized confirms the
importance of human resource development in the implementation of INA-‐‑CBG
system in the region. The level of compliance of data entry for treatments is
higher at 57.12 percent but it is still below the WHO standard.
Most of the health services delivered in the region are dealing with
curative and rehabilitative treatments ranging from infectious and
communicable diseases such as influenza, pneumonia, bronchitis and typhus;
injuries from work and social activities; degenerative diseases such as diabetics,
hypertension, and dialysis; to catastrophic diseases such us cardiac failures,
stroke and cancer. The provincial government is urging Jamkesda and local
hospitals to move towards preventive and promotive health services. Preventive
services would deal with clinical pathology, Pap-‐‑smear test, mammography,
echocardiography, thalassemia, total protection for prenatal and antenatal and
children immunology. And promotive services would deal with nutrition
campaign for various groups including pregnants, under-‐‑five children, geriatrics,
and high-‐‑risk individuals. Yet it would take time for all the stake-‐‑holders and the
populace to acknowledge that a focus on preventive and promotive aspects
would eventually reduce financial burden for curative services.

33
The Jogja province authorities find it easier to convince the public
hospital managements compared to those of the private hospitals regarding the
importance of universal coverage. For public hospitals that get most of their
budgets from the government, a mandatory scheme for financing the poor and
informal sector workers would be readily accepted. However, for private
hospitals that have long been investing on assets (lands, buildings) and on staffs
without external help, the idea of servicing the poor has always been linked with
financial break-‐‑even and profit. As explained, this relates to the reason why INA-‐‑
CBG bridging system has been going slow in the private hospitals.
V. CONCLUSIONS
Based on the Indonesian's JKN road map, the government has identified
and followed some general paths for instituting universal health coverage.
Applying prospective payments, mandating a compulsory scheme, expanding
coverage on the poor, and instituting capitation with a case base mix have been
implemented. The government has also been trying to address the issue on
financial fragmentation by defining the collection and pooling the funds under
the BPJS management. Nevertheless, the bold move in Indonesian health
financing has to face with realities in the implementation that may not guarantee
the success toward universal coverage. There are many challenges ahead that
have to be met with strong commitment, perseverance and adequate knowledge
on the core problems of coverage and efficiency while dealing with the raising
demand for health services in the country.
Although the government policy on health has been reinvigorated with
the establishment of BPJS, one should note that the Indonesian financial
commitment remains very low at 3.0 percent or US$ 104.25 per capita
expenditure of GDP. This is a fundamental issue given the fact that the challenge
for insurance coverage is astonishingly high with the greatest proportion coming
from the informal sector workers. The policy makers should understand that
informal sector workers belong to precarious group who would be easily
impoverished from catastrophic illness if out-‐‑of-‐‑pocket health service is the only
available option for them.

34
As a country with large size of population and recently committed to
decentralization, integration and pooled funding as the prerequisites for
universal coverage are problematic. Not only that there is different
understanding between the national and sub-‐‑national authorities on the
meaning and the pathways to be taken for attaining universal coverage,
decentralization also tends to entail different political commitment, perpetuate
fragmentation, and disrupt efforts to vertically integrate the system. This adds
up to the problem of integration already faced at the regional level as evidenced
in the slow process of bridging the INA-‐‑CBG system.
Meanwhile, the immediate impacts of implementing universal coverage
commonly learned from international experience are also dealt by Indonesian
health officials. Adverse selection or moral hazards, double-‐‑counting on
beneficiaries, inconsistent medical database, financial leakages due to mismatch
between actuarial and claims, unclear clinical pathways, and lack of human
resources to administer prospective payments are among the problems that
need to be solved in the incoming years. While aiming for the national target on
coverage, many of health professionals in the country have to deal with technical
difficulties in adjusting to the new system.
Building a strong pooled-‐‑fund for universal health coverage requires
institutional arrangements that are responsive to financial efficiency, benefit
equity, and continuous commitment to the poor. Within a decentralized
environment in Indonesia, this would need mutual trust and understanding
among different levels of government, in which professional attitude, knowledge
and willingness to learn from mistakes are essential. Intensive consultation
among the decision makers, economic and financial experts, medical
professionals, technical staffs, and the public at large will determine whether this
bold step result in equitable health.
Reference
1. Adisasmito, W. (2007). Sistem Kesehatan. (Jakarta: Rajagrafindo Persada).

35
2. Anonymous. (2012). "Jamkesmas Health Service Fee Waiver: Social
Assistance Program and Public Expenditure Review No.4". (World Bank,
Jakarta Office).
3. Anonymous. (2008). Closing the Gap In A Generation. (Geneva: WHO,
Commission on Social Determinants of Health).
4. Anonymous. (2009). Financing Strategy for the Asia Pacific Region 2010-‐‑
2015. (Geneva: WHO Regional Office for the Western Pacific).
5. Anonymous. (2015). Fiscal Space, Public Finance Management and Health
Financing Policy. (Montreoux: WHO).
6. Anonymous. (2014). Making Fair Choices On The Path to Universal Health
Coverage. (Geneva: WHO).
7. Anonymous. (2012). Policy Note on SJSN: Designing and Financing of SJSN
Employment Benefits. (Jakarta: World Bank, July 2012).
8. Anonymous. (2012). Child Poverty and Disparities in Indonesia: Challenges
for Inclusive Growth. (New York: SMERU, Bappenas, UNICEF).
9. Anonymous. (2008). Framework and Standards of Country Health
Information Systems. (Geneva: WHO, Health Metric Network).
10. Arifianto, A. (2004). Reformasi Sistem Jaminan Sosial di Indonesia: Sebuah
Analisis atas Undang-‐‑undang Jaminan Sosial Nasional. (Jakarta: Lembaga
Penelitian Semeru).
11. Atun R. et al. (2013). Universal Health Coverage in Turkey. (Geneva: WHO
Lancet Papers Vol. 382 July 6, 2013). Available at:
http://dx.doi.org/10.1016/S0140-‐‑6736(13)61051-‐‑X
12. Boychuk G.W. (2008). National Health Insurance in the United States and
Canada: Race, Territory and the Roots of Difference. (Washington:
Georgetown University Press).
13. Budiarto W. & Sugiharto M. (2012). Biaya Klaim INA-‐‑CBG dan Biaya Riil
Penyakit Katastrofik. (Jakarta: Pusat Humaniora, Litbang Kesehatan,
Kementerian kesehatan).
14. Carrin G. (2003). Community Based Health Insurance Schemes in
Developing Countries: Facts, Problems and Perspectives. (Geneva: World
Health Organization Discussion Paper, No.1).

36
15. Carrin G., James C. (2004). Reaching Universal Coverage Via Social Health
Insurance: Key Design Features in the Transition Period. (Geneva: World
Health Organization Discussion Paper, No.2).
16. Carrin G., Mathauer I., Xu K., Evans D. (2008). Universal Coverage of
Health Services: Tailoring Its Implementation. Bulletin of World Health
Organization, No.11, November 2008. Available at: bit.ly/Carrin2UHC.
DOI: 10.2471/ BLT.07.049387.
17. Deacon, B. (2005). "From 'Safety Nets' Back to 'Universal Social
Provision': Is the Global Tide Turning?", Global Social Policy, No.5(1),
2005.
18. Gani A. et al (2008). Laporan Kajian Sistem Pembiayaan Kesehatan di
Beberapa Kabupaten dan Kota. (Jakarta: Fakultas Kesehatan Masyarakat,
UI).
19. Gauld R. (2005). Comparative Health Policy in The Asia-‐‑Pacific. (New York:
Open University Press).
20. Harimurti P., Pambudi E., Pigazzini A., Tandon A. (2013). The Nuts and
Bolds of Jamkesmas: Indonesia's Government-‐‑Financed Health Coverage
Program for the Poor and Near Poor. (Washington DC: The World Bank
UNICO Series No.8).
21. Hart J.T. (2006). The Political Economy of Health Care: A Clinical
Perspective. (Bristol: The Policy Press).
22. Indriani D., Kusnanto H., Mukti A.G., Kuntoro. (2013). Dampak Biaya
Laboratorium Terhadap Tarif INA-‐‑CBG dan Biaya Riil Diagnosis
Leukemia. (Jurnal Kesehatan Masyarakat Nasional, Vol.7, No.10, May
2013).
23. Joedadibrata, D. (2012). A Study of the Shift Towards Universal Social
Policy in Indonesia. (The Hague, Master Thesis, ISS, The Netherlands).
24. Jonas S., Goldsteen R.L., Goldsteen K. (2007). An Introduction to the U.S.
Health Care System. (New York: Springer Publishing Company).
25. Joumard I., Hoeller P., Andre C., Nicq C. (2005). Health Care Systems:
Efficiency and Policy Settings. (Paris, OECD).
26. Keita M. (2007). The Political Economy of Health Care in Senegal. (Leiden:
Koninklijke Brill).

37
27. Kutzin, J. (2013). Health Financing for Universal Coverage and Health
System Performance: Concepts and Implications for Policy. Bulletin of the
World Health Organization. No. 8, 2013. Available at: bit.ly/KutzinUHC.
DOI: 10.2471/BLT. 12.113985
28. Longest B.B. (2005). Contemporary Health Policy. (Washington DC:
AUPHA-‐‑HAP).
29. Mathauer I., Cavagnero E., Vivas G., Carrin G. (2010). Health Financing
Challenges and Institutional Options to Move Towards Universal Coverage
in Nicaragua. (Geneva: WHO, Discussion Paper No.2, 2010).
30. Mboi, N. (2014). Moving Towards Universal Health Access in Indonesia.
(Jakarta: The Minister international presentation. Acessed on August
27th, 2014).
31. McKee M. (2013). Universal Health Coverage: A Quest for All Countries
But under Threat in Some. Value in Health. No. 1 (January-‐‑February
2013). Available at: bit.ly/McKeeUHC. DOI: 10.1016/j.jval.2012.10.001
32. Milton B., Moonan M., Taylor-‐‑Robinson D., Whitehead M. (2011). How Can
the Health Equity Impact of Universal Policies Be Evaluated? Insights Into
Approaches and Next Steps. (Copenhagen: WHO Regional Office for
Europe).
33. Mohamad, K. (2011). "Setelah UU BPJS Disahkan". Kompas. (Jakarta, 23
December 2011).
34. Mossialos E., Dixon A., Figueras J., Kutzin J. (2002). Funding Health Care:
Options for Europe. (Buckingham: Open University Press).
35. Nuryanti. (2014). Evaluasi Ketepatan Diagnosis dan Tindakan di Rumah
Sakit Panti Rapih Yogyakarta. Jurnal Manajemen Informasi Kesehatan
Indonesia, Vol.3 No.1, Oktober 2014).
36. Paolucci F. (2011). Health Care Financing and Insurance: Options for
Design. (Heidelberg: Springer).
37. Pauly M.V., Herring B. (2002). Cutting Taxes for Insuring: Options and
Effects of Tax Credits for Health Insurance. (Washington DC: The American
Enterprise Insitute)
38. Preker A.S. & Carrin G. (2004). Health Financing for Poor People: Resource
Mobilization and Risk Sharing. (Washington DC: The World Bank).

38
39. Saltman R.B., Busse R., Figueras J. (2004). Social Health Insurance Systems
in Western Europe. (New York: WHO, European Observatory on Health
Systems and Policies, Open University Press).
40. Savedoff W. (2012). Transitions in Health Financing and Policies for
Universal Health Coverage: Final Report of the Transitions in Health
Financing Project, Results for Development. Washington, August 24, 2012.
Available at: bit.ly/Savedoff2UHC
41. Simmods A., Hort K. (2013). Institutional Analysis of Indonesia's Proposed
Road Map to Universal Health Coverage. (Melbourne: The Nossal Institute
of Global Health).
42. Smith P.C., Ginnely L., Sculphers M. (2005). Health Policy and Economics:
Opportunities and Challenges. (New York: Open University Press).
43. Soewondo P., Najib M., Sari K. (2011). SHA-‐‑Based Health Accounts in the
Asia-‐‑Pacific Region: Indonesia 2005-‐‑2009. SHA Technical Paper No.15.
(Seoul: OECD-‐‑Korea Policy Center)
44. Supriyantoro (2014). Formulasi Kebijakan Integrasi Jaminan Kesehatan
Daerah ke Sistem Jaminan Kesehatan Nasional Menuju Universal Health
Coverage. (Yogyakarta: Gadjah Mada University, Unpublished Doctoral
Dissertation).
45. Thabrany H. (2008). The Politics of National Health Insurance of Indonesia:
A New Era for Universal Coverage. (Rome: The Seventh European
Conference on Health Economics).
46. Thabrany H. (2014). Jaminan Kesehatan Nasional. (Jakarta: Rajagrafindo
Persada).
47. Thaha, A. (2007). Laporan Teknis di Balik Tabir Penyusunan UU No.40
tahun 2004: Sebuah Analisis. (Jakarta: GTZ).
48. Thomson S., Foubister T., Mossialos E. (2009). Financing Health Care in
the European Union: Challenges and Policy Responses. (Copenhagen: WHO
& The European Observatory on Health Systems and Policies, Observatory
Studies Series No.17).
49. Tijan A. (2014). "Analisa Kebijakan Undang-‐‑undang Implementasi BPJS",
Opini, Kompasiana. (Jakarta, 25 May 2014).

39
50. Tribowo A. (2014). Sistem Pembiayaan Kesehatan Di Era BPJS-‐‑JKN.
(Jakarta: Pusat Case Mix Nasional, Kementerian Kesehatan, mimeo).
51. Wall A. (1996). Health Care System in Liberal Democracies. (London:
Routledge).
52. Weissert C.S. & Weissert W.G. (2006). Governing Health: The Politics of
Health Policy. (Baltimore: John Hopkins University Press).
53. WHO. (2010). Health System Financing: The Path to Universal Coverage.
(Geneva: WHO).
54. Windrawan, P. & Purwaningrum F. (2014). Sistem Pengetahuan dan
Desentralisasi Kesehatan di Indonesia: Kajian Multidisiplin. (Yogyakarta:
Total Media).
55. Xiaolu B. (2014). Fiscal Space for Universal Health Coverage in Indonesia:
Lessons form Jamkesmas Financing. (East Asia Pacific HNP Policy Brief
Series, March, 2014).
56. Zweifel P. (2007). The Theory of Social Health Insurance. (Hanover: Now
Publishers Inc.)
*****


















