Title: MEDICATION ERRORS, MANAGEMENT AND Ref: 1537 …
18
Collated by Clinical Effectiveness Medication Errors, Management and Prevention of Page 1 of 4 Title: MEDICATION ERRORS, MANAGEMENT AND PREVENTION OF Ref: 1537 Version 3 Classification: Protocol Directorate: Trustwide Due for Review: 29/12/20 Responsible Clinical Governance Pharmacist and Medication Safety for review: Officer Document Control Ratified by: Medicines Management Committee Chief Nurse Medical Director Care and Clinical Policies Group Applicability: As indicated Introduction Medication errors have been defined as ‘Unintentional errors in the prescribing, dispensing, or administration of a medicine while under the control of a healthcare professional, patient or consumer which harm the patient or have the potential to harm the patient’ Medication Errors are classified by significance using the following criteria: - No harm This has two sub-categories: No harm (impact prevented) – Any incident that had the potential to cause harm but was prevented, resulting in no harm to anyone. This may be locally termed a ‘near miss’ No harm (impact not prevented) - Any incident that ran to completion but no harm occurred to anyone. Low Any incident causing minor injury requiring first aid treatment but no time lost or, unexpected or unintended patient incident that required extra observation or minor treatment and caused minimal harm to one or more persons receiving NHS-funded care. Moderate Any incident causing injury requiring referral to ED. Any unexpected or unintended patient incident that resulted in a moderate increase in treatment, possible surgical intervention, cancellation of treatment, or transfer to another area, and which caused significant but not permanent harm, to one or more persons receiving NHS-funded care. Severe Any unexpected or unintended patient incident that appears to have resulted in permanent harm to one or more persons. Any RIDDOR incident. Death Any unexpected or unintended incident that directly resulted in the death of one or more persons. Medication errors are one of the leading causes of injury to hospital patients leading to increased morbidity and mortality. The causes of medication errors are multiple including, patient, practitioner and the medicines management systems. Over half of all hospital medication errors occur at the interfaces of care, at admission, discharge and transfer. Interventions that tackle all of these areas are an integral part of this policy and are detailed below. Aim The aim of this policy is to ensure that proactive measures are in place to reduce the incidence and severity of medication errors. The other aim of this policy is to ensure that medication errors are reliably reported and that there is a mechanism in place to ensure that the organisation learns from errors and that appropriate corrective actions are put in place, both organisationally and with individual members of staff. This policy should be read in conjunction with the Trust’s Medicines Policy 0806 & 1927
Transcript of Title: MEDICATION ERRORS, MANAGEMENT AND Ref: 1537 …

Collated by Clinical Effectiveness Medication Errors, Management and Prevention of Page 1 of 4
Title: MEDICATION ERRORS, MANAGEMENT AND PREVENTION OF
Ref: 1537 Version 3
Classification: Protocol Directorate: Trustwide Due for Review:
29/12/20 Responsible Clinical Governance Pharmacist and Medication Safety for review: Officer
Document Control
Ratified by: Medicines Management Committee Chief Nurse Medical Director Care and Clinical Policies Group
Applicability: As indicated
Introduction Medication errors have been defined as ‘Unintentional errors in the prescribing, dispensing, or administration of a medicine while under the control of a healthcare professional, patient or consumer which harm the patient or have the potential to harm the patient’ Medication Errors are classified by significance using the following criteria: -
No harm This has two sub-categories: No harm (impact prevented) – Any incident that had the potential to cause harm but was prevented, resulting in no harm to anyone. This may be locally termed a ‘near miss’ No harm (impact not prevented) - Any incident that ran to completion but no harm occurred to anyone.
Low Any incident causing minor injury requiring first aid treatment but no time lost or, unexpected or unintended patient incident that required extra observation or minor treatment and caused minimal harm to one or more persons receiving NHS-funded care.
Moderate Any incident causing injury requiring referral to ED. Any unexpected or unintended patient incident that resulted in a moderate increase in treatment, possible surgical intervention, cancellation of treatment, or transfer to another area, and which caused significant but not permanent harm, to one or more persons receiving NHS-funded care.
Severe Any unexpected or unintended patient incident that appears to have resulted in permanent harm to one or more persons. Any RIDDOR incident.
Death Any unexpected or unintended incident that directly resulted in the death of one or more persons.
Medication errors are one of the leading causes of injury to hospital patients leading to increased morbidity and mortality. The causes of medication errors are multiple including, patient, practitioner and the medicines management systems. Over half of all hospital medication errors occur at the interfaces of care, at admission, discharge and transfer. Interventions that tackle all of these areas are an integral part of this policy and are detailed below. Aim The aim of this policy is to ensure that proactive measures are in place to reduce the incidence and severity of medication errors. The other aim of this policy is to ensure that medication errors are reliably reported and that there is a mechanism in place to ensure that the organisation learns from errors and that appropriate corrective actions are put in place, both organisationally and with individual members of staff. This policy should be read in conjunction with the Trust’s Medicines Policy 0806 & 1927
Medication Errors, Management and Prevention of Collated by Clinical Effectiveness Page 2 of 4
Prevention of Medication Errors Procurement The Trust through the Commercial Medicines Unit, through Regional Contracts and through the Peninsula Purchasing and Supply Agency comply with the guidance set out in ‘Purchasing for Safety’ 1. This guidance is to ensure that safety considerations are taken into account when procurement decisions are made that relate to medicines. Supply Standard operating procedures should be in place to govern the issue and supply of medicines from the dispensary and from the pharmacy dispatch area to all users of the pharmacy service. Prescribing The Trust promotes and supports competent prescribing and all prescribers – both medical and non-medical prescribers are expected to have the necessary prescribing competencies as described by the National Prescribing Centre’s ‘Single Competency Framework’2
https://icon.torbayandsouthdevon.nhs.uk/areas/non-medical-prescribing/Pages/default.aspx
The design of both the Trust’s drug prescription & administration record and the planned electronic prescribing system are designed to promote and support the safe prescribing and administration of medicines. Details of how to prescribe are described within the Medicines Policy. 0806 & 1927 Prescription Verification The Trust provides a clinical pharmacy service comprising pharmacists and appropriately trained pharmacy technicians. Prescriptions are reviewed according to the Ward Pharmacy Prescription Screening Guidelines and the Dispensary Screening Guidelines. All prescriptions for inpatients on admission should be reconciled as per the ‘Medicines Reconciliation’ policy 1341. Medicines reconciliation is undertaken by doctors, nurses, pharmacists and pharmacy technicians. This is to ensure that medicines prescribed on admission are correct and validated through a recognised process. Medicines are reconciled on weekdays with the aim that 95% of those patients have had their medicines reconciled within 24 hours of admission. Medicines Information Medicines information support is available to provide guidance relating to the prescribing and administration of medicines to any clinical staff within the Trust. Medicines Information support is available Monday to Friday 9am-5pm from the pharmacy department or from the on call pharmacist outside normal working hours. Proactive information is also supported by Medicines Information to ensure that the relevant information support is available within all clinical areas. This information includes; IV monographs / Prescribing and treatment guidelines / Safety Alerts / Joint Formulary. The Trust Medicines Information service is required to comply with the standards set by the UK Medicines Information Group. Administration of Medicines The Trust promotes and supports the competent administration of medicines in line with the Trust’s Medicines Policy, the Medicines Competency Assessment for drug rounds3 and the Medicines Administration Course. The design of the Trust’s drug prescription and administration record promotes and supports the safe prescribing and administration of medicines. Administration of medicines should be within the competencies of the healthcare professional involved and the administration of medicines by nurses should be compliant with the Nurse and Midwifery Council ‘Standards for Medicines Management’4.

Collated by Clinical Effectiveness Medication Errors, Management and Prevention of Page 3 of 4
Staff Training Mandatory and voluntary medicine management training for medical, nursing and pharmacy staff is available. It is the responsibility of individual clinical staff and their line managers, through the appraisal process, to ensure that all mandatory training is undertaken and those personnel are always practicing within their competencies. Actions to Manage Medication Errors Reporting Medication Errors
1. The Trust promotes a positive approach to reporting and staff are encouraged and supported
to be open and honest about incidents that have or may have caused harm. 2. Medication errors should be reported in line with the Trust’s Adverse Event Management
Policy and reported on the incident reporting system within 24 hours.
3. Medication errors made by nursing, medical, pharmacy or other professional groups are
covered by this policy and should be managed in a consistent manner. 4. All medication errors MUST be reported (See appendix 1) especially those involving high risk
medicines, see the following: -
5. Medication errors should be reported to the Governance lead for the Division. The Pharmacy
Governance lead will ensure that serious events or recurrent errors are referred to the Trust’s Medicines Management Committee via the Director of Pharmacy or his deputy.
6. All medication errors classified as moderate, severe or death on the incident reporting system
need to be referred to the Director of Pharmacy.
Management of Reported Errors Any error classified as ‘moderate, severe or death’ should be reviewed by the service lead/Matron, the Divisional Governance Lead and the Pharmacy Governance Lead. To help determine the appropriate course of action the Incident Decision Tree (appendix 2) should be considered. Process for managing and supporting staff
The manager and member of staff will develop an action plan depending on the needs identified.
If the medication error is of no harm or low severity the manager in conjunction with the member of staff must follow the algorithm in Appendix 1. If the medication error severity is classed as moderate, severe or death, or a no harm- impact prevented (near miss) with the potential for a moderate, severe or death outcome, the manager / educational supervisor must follow the algorithm in Appendix 1, it is the manager / educational
Amiodarone Insulin Oral anticancer medicines
Amphoteracin Intrathecal medicines Parkinsons medicines
Anticoagulants (oral) Ketamine Potassium (IV)
Chemotherapy (IV) Methotrexate Sodium Chloride/Glucose 0.18/4% Epidural medicines Midazolam
Gentamicin (NICU) Monoclonal antibodies Desmopressin
Heparin Opioids Clozapine

Medication Errors, Management and Prevention of Collated by Clinical Effectiveness Page 4 of 4
supervisor’s responsibility to either carry out an investigation or allocate the investigation to another competent trained member of staff. The manager / educational supervisor is responsible for checking the severity of the incident and ensuring the incident reporting system is updated in a timely manner. Any areas of concern identified as a result of the investigation must be addressed by the manager / educational supervisor. If this is an error classified as ‘moderate, severe or death’ OR if a repeat or second error made by the member of staff within the last two months, then the manager / educational supervisor should consider using the incident decision tree to determine what type of action is required.
Working in line with the algorithm in Appendix 1, the manager / educational supervisor may need to make the decision to temporarily suspend the member of staff from undertaking certain duties e.g. medication administration. In all cases, it is important that the member of staff is supported by their manager / educational supervisor during this process and kept informed of any actions that may have to be taken. Learning from Errors After a medication error, it is important that there should be an opportunity for the staff member to discuss the incident with their manager as soon as possible after the incident. The purpose of the discussion is to:
Discuss the incident to enable the member of staff to reflect on the circumstances.
Allow the member of staff to discuss how they feel and discuss any concerns they may have.
Examine the details of the incident and identify if there are any gaps in policy and protocols that could prevent another incident/near miss occurring again.
Identify if there are any training or performance issues with the member of staff
Action plans to be put in place
Determine if the member of staff has made a recent or previous medication errors The line manager / educational supervisors are responsible for identifying staff who continue to make medication errors and support them in line with this policy specified in the algorithm listed in Appendix 1. Medicines Management Committee A key role of this committee is to ensure that the organisation learns from the medication errors that are reported. The committee is responsible for ensuring that corrective actions are implemented by appropriate groups or individuals to prevent similar errors in the future. The monitoring of these action plans is achieved through the Medicines Management Risk Register; this is maintained by the Medicines Management Committee and reviewed at each meeting. Medication errors will be reported to the Medicines Management Committee every three months. Appendix 1 – Algorithm for the Management of Medication Errors
Appendix 2 – Incident Decision Tree
Appendix 3 – Supporting Documents
Appendix 4 – Pharmacy Process for Handling Reported Medication Incidents

Collated by Clinical Effectiveness Algorithm for the Management of Medication Errors Page 1 of 1
Appendix 1
Algorithm for the Management of Medication Errors
No Harm / Low Harm Moderate / Severe Harm or Death
Carry out a local review Inform Senior Manager and Director of Pharmacy Carry out formal RCA
Ask clinical staff involved to reflect on incident and include comments on the Incident Reporting System.
Member of staff involved complete reflective account to be attached to the Incident Reporting System.
Consider using NPSA Incident Decision Tree to identify any systems errors as part of the local review
Use NPSA Incident Decision Tree to identify any systems errors as part of the RCA
Confirm whether this is a repeat error or near miss
Supportive discussion to include reflection by member of staff
If a no harm- impact prevented (near miss) with the potential for a moderate, severe or death outcome then manage as a moderate, severe or death severity incident
If this is a 2nd medication error within a 2 month period suspend from medicine administration while RCA in progress
Arrange further training as appropriate e.g. medicines administration, safe prescribing or medicines reconciliation ASAP
Supportive discussion with member of staff and line manager / educational supervisor to include review of the reflective account by the member of staff
Discussion between the member of staff and line manager / senior nurse / educational supervisor dependant on the outcome of the RCA
Action plan in place
Consider:
Arranging medicines administration or prescribing training if clinician has made a repeat error/near miss
Temporary suspension from medicine administration
For other members of staff consider a review of duties and further training
Action plan
Ensure training has been delivered before lifting suspension from medicines administration
Initiate a period of supervision when suspension has been lifted
Consider:
Suspension from duty and following formal investigation consider:
Initiating Disciplinary Procedure
This is the responsibility of the line manager with support from the service lead/Matron, the Divisional Governance Lead and Pharmacy.

Incident Decision Tree Collated by Clinical Effectiveness Page 1 of 1
Appendix 2
Incident Decision Tree Deliberate Harm
TestPhysical/Mental Health Test Foresight Test Substitution Test
Were the actions
as intended?
Were adverse
consequences
intended?
Need to consider acts of
omission as well as
commission. Examples
could be failing to administer
medication or calling cardiac
arrest team. Consider
whether the individual forgot
to take it or was prevented
from taking action or did they
decide themselves not to
take action or refuse to carry
out on an instruction. **
Does there appear to be evidence of ill
health or substance abuse? Does the
individual have a known medical
condition?
You need to assess the situation at
the time of the incident. For
example, if a member of staff had
an asthmatic attack, which they
say caused the error, was there
actual evidence of the attack
happening at the time of the
incident? You need to consider the
impact of the illness on the
individual. Also need to consider
things like was the individual
suffering stress which may not
necessarily relate to work, was it
out of character for the individual to
behave in the way that they did?
If Yes then consider referral to
Occupational health or the Disciplinary
Process
Did the individual depart
from agreed protocols or
Safe procedures?
Were the protocols and
safe procedures
available, workable,
intelligible, correct and in
routine use?
Is there evidence that
the individual took and
unacceptable risk?
You need to decide whether the
individual took an unacceptable risk,
exposing patients to a medical
condition which they have
themselves and which they have not
reported, e.g. nurse who fails to
report that she is a TB carrier. **
Would another individual coming
from the same professional group,
possessing comparable
qualification and experience,
behave in the same way in similar
circumstances?
Were there any deficiencies in
training, experience or
supervision?
Were there significant mitigating
circumstances?
Disciplinary process
** If Yes to any of the
questions indentified,
consider disciplinary
process.
Yes
Possibly
Possibly
No No
Yes
Yes
Possibly
No
No
No
No
No
System
Failure
Review
System
No
No
Yes
Yes
Yes

Collated by Clinical Effectiveness Supporting Documents Page 1 of 1
Appendix 3 Supporting Documents 1. Purchasing for safety https://www.gov.uk/government/collections/commercial-medicines-unit-cmu
2. NPC Competency Framework for Prescribers https://www.rpharms.com/Portals/0/RPS%20document%20library/Open%20access/Professional%20standards/Prescribing%20competency%20framework/prescribing-competency-framework.pdf 3. Medicines competency assessment. (Pages 8 – 12)
4. NMC Standards for Medicines Management http://www.nmc-uk.org/Documents/NMC-Publications/NMC-Standards-for-medicines-management.pdf

Medicines Competency Assessment Collated by Clinical Effectiveness Page 1 of 5
Appendix 3 (point 3)
Medicines Round Competency Assessment for Torbay and South Devon Healthcare Staff in Acute & Community Hospitals (Refer to Medicines Policy for supporting information-see Clinical Guidelines, Trustwide, Drugs) Name of nurse being assessed: Date
Competency Competent Not Competent
Comments/Action Plan
Sign:
1 Discuss accountability in relation to medicines administration
2 Locate, access and demonstrate a working knowledge of TSDFT Medicines Policy
3 For commonly used medicines within their area of practice (to be identified by ward manager), discuss:
Normal dose range
Indication
Common side effects
Common interactions
Important contra-indications (Enter details on the reverse of this page)
4 Discuss the actions and procedure to be followed should a drug error be made or identified
5 Demonstrate the correct procedure for administration of medicines (observe at least 5 patients) including:
5a Check medicine is prescribed correctly
5b Check patient identity (name band)

Collated by Clinical Effectiveness Medicines Competency Assessment Page 2 of 5
Competency Competent Not Competent
Action Plan and timescale to achieve competency
Signature
5c Select correct medicine
5d Check allergy status
5e Check name of medicine, dosage, expiry date, route
5f Observe patient taking medicine
6 Demonstrate correct procedure for administration of the following specific high risk medicines:
6a Controlled drugs
6b Insulin
6c Oral anticoagulants
7 Administer medicines by the following routes (ward manager to highlight those relevant to clinical area):
7a Subcutaneous, including infusion by syringe driver
7b Nebulised
7c Topical including patches
7d Via enteral tube

Medicines Competency Assessment Collated by Clinical Effectiveness Page 3 of 5
Competency Competent Not Competent
Action Plan and timescale to achieve competency
Signature
7e Other routes:
8 Correctly record the administration of medicines
9 Discuss patient and/or carer education related to medicines (observe at least one patient interaction)
10 Discuss and demonstrate the correct processes for dealing with an actual or potential missed dose
11 Discuss and demonstrate the correct process for dealing with self medication
12 Discuss and demonstrate the correct processes around discharge medicines (including discharge planning)
13 Discuss and demonstrate correct procedures for ordering medicines, including controlled drugs
14 Discuss and demonstrate correct procedures related to safe and appropriate storage of medicines, including disposal and security
15 Discuss and demonstrate correct process for transfer of medicines between wards

Collated by Clinical Effectiveness Supporting Documents Page 4 of 5
Competency Competent Not Competent
Action Plan and timescale to achieve competency
Signature
16 Identify and access appropriate and available resources for medicines information:
BNF
Intranet
Colleagues including pharmacy, medical, nursing staff
Locally relevant sources as identified by ward manager
17 Discuss the correct processes for obtaining medicines or information related to medicines out of hours
Candidate has/ has not achieved competency in all sections of the assessment tool. (delete as appropriate)
Signature of assessor: Designation: Date: I (Signature or candidate)………………………………………….acknowledge my own competency in the administration of medicines Date: Signature of ward manager (if different from assessor)…………………………………………………………..

Medicines Competency Assessment Collated by Clinical Effectiveness Page 5 of 5
Summary Of Assessment
Summary of Action Points Action Taken Signature and date

Collated by Clinical Effectiveness Pharmacy Process for Handling Reported Medication In Page 1 of 2
Appendix 4
Pharmacy Process for Handling Reported Medication Incidents
Medication Incident
Reported to Pharmacy
Governance Lead
via Datix
Inform ward/specialty
pharmacist
Medication Incident grades
as per Trust Guidelines by
Pharmacy Governance Lead
Did the error involve a Controlled
Drug?
Did the error involve the security or
theft of medicines?
Did the incident cause or have
potential to cause severe harm or
death
Ensure that any remedial actions
are completed and all relevant
parties informed (table 1).
Inform the Trust Accountable
Officer for Controlled Drugs and the
Director of Pharmacy
Report to the Director of
Pharmacy
Ensure disussed at the next
Medicines Management Committee
Yes
Yes
Yes
Yes
Log and determine
with the ward
pharmacist or
department lead what
further action is
required (table 2)
NoReport to the Director of
Pharmacy
Pharmacy Process for Handling Reported Medication Incidents Collated by Clinical Effectiveness Page 2 of 2
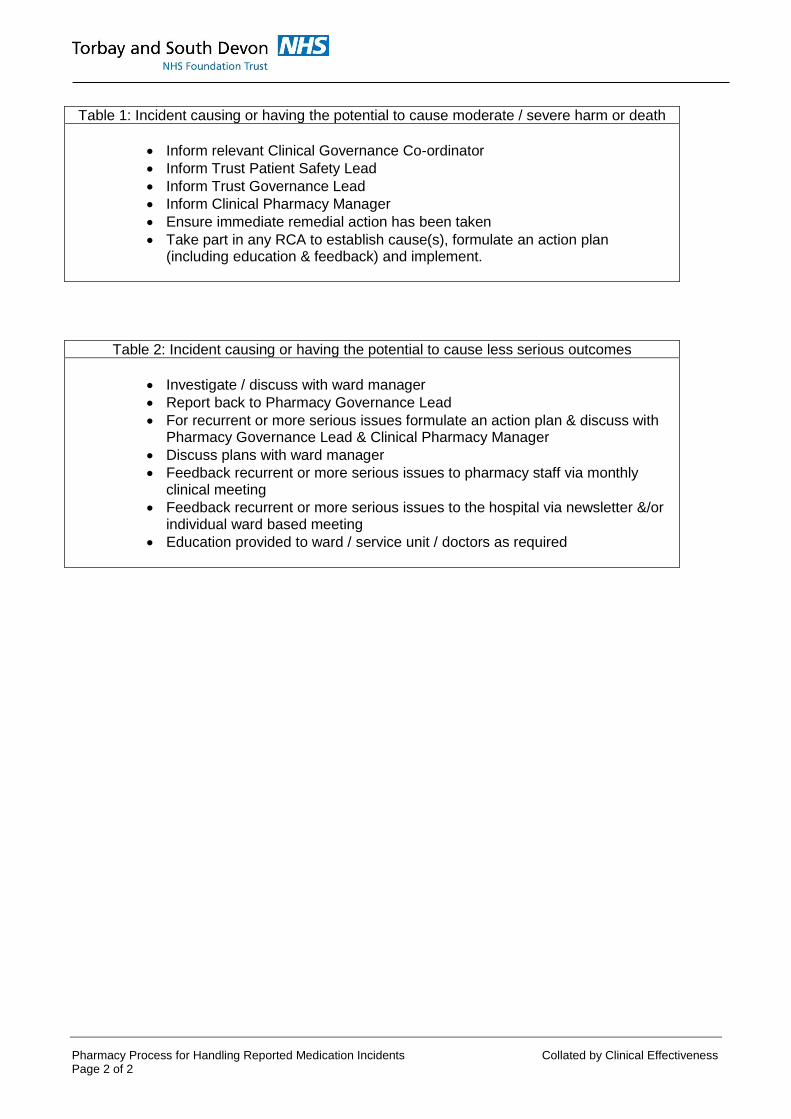
Table 2: Incident causing or having the potential to cause less serious outcomes
Investigate / discuss with ward manager
Report back to Pharmacy Governance Lead
For recurrent or more serious issues formulate an action plan & discuss with Pharmacy Governance Lead & Clinical Pharmacy Manager
Discuss plans with ward manager
Feedback recurrent or more serious issues to pharmacy staff via monthly clinical meeting
Feedback recurrent or more serious issues to the hospital via newsletter &/or individual ward based meeting
Education provided to ward / service unit / doctors as required
Table 1: Incident causing or having the potential to cause moderate / severe harm or death
Inform relevant Clinical Governance Co-ordinator
Inform Trust Patient Safety Lead
Inform Trust Governance Lead
Inform Clinical Pharmacy Manager
Ensure immediate remedial action has been taken
Take part in any RCA to establish cause(s), formulate an action plan (including education & feedback) and implement.

Collated by Clinical Effectiveness Medication Errors, Management and Prevention of Document Control Information Page 1 of 1
Protocols & Guidelines – Document Control This is a controlled document. It should not be altered in any way without the express permission of the author or their representative. On receipt of a new version, please destroy all previous versions.
Ref: 1537 Title: Medication Errors, Management and Prevention of
Date of Issue: 29 December 2017 Next Review Date: 29 December 2020
Version: 3
Author: Clinical Governance Pharmacist and Medication Safety Lead
Index: Pharmacy
Classification: Guideline
Applicability: As indicated
Equality Impact:
The guidance contained in this document is intended to be inclusive for all patients within the clinical group specified, regardless of age, disability, gender, gender identity, sexual orientation, race and ethnicity & religion or belief.
Evidence based: Yes
References: Purchasing for Safety NPC Competency Framework for Prescribers NMC Standards for Medicines Management
Produced following audit:
No
Audited: No
Approval Route: See ratification Date Approved: 18 December 2017
Approved By:
Medicines Management Committee Chief Nurse Medical Director Care and Clinical Policies Group
Links or overlaps with other policies: 0806 Medicines Policy; 1341 Medicines Reconciliation
All TSDFT Trust strategies, policies and procedure documents.
PUBLICATION HISTORY:
Issue Date Status Authorised
1 8 November 2012 New Clinical Director of Pharmacy Director of Nursing and Quality Medical Director
2 3 October 2014 Revised Clinical Director of Pharmacy Director of Nursing, Patient Experience and People’s Experience Interim Medical Director
3 29 December 2017 Revised Chief Nurse Medical Director Medicines Management Committee Care and Clinical Policies Group
3 20 February 2018 Review Date Extended 2 Years to 3 Years

Medication Errors, Management and Prevention of Collated by Clinical Effectiveness The Mental Capacity Act Page 1 of 1
The Mental Capacity Act 2005 The Mental Capacity Act provides a statutory framework for people who lack capacity to make decisions for themselves, or who have capacity and want to make preparations for a time when they lack capacity in the future. It sets out who can take decisions, in which situations, and how they should go about this. It covers a wide range of decision making from health and welfare decisions to finance and property decisions Enshrined in the Mental Capacity Act is the principle that people must be assumed to have capacity unless it is established that they do not. This is an important aspect of law that all health and social care practitioners must implement when proposing to undertake any act in connection with care and treatment that requires consent. In circumstances where there is an element of doubt about a person’s ability to make a decision due to ‘an impairment of or disturbance in the functioning of the mind or brain’ the practitioner must implement the Mental Capacity Act. The legal framework provided by the Mental Capacity Act 2005 is supported by a Code of Practice, which provides guidance and information about how the Act works in practice. The Code of Practice has statutory force which means that health and social care practitioners have a legal duty to have regard to it when working with or caring for adults who may lack capacity to make decisions for themselves. All Trust workers can access the Code of Practice, Mental Capacity Act 2005 Policy, Mental Capacity Act 2005 Practice Guidance, information booklets and all assessment, checklists and Independent Mental Capacity Advocate referral forms on iCare http://icare/Operations/mental_capacity_act/Pages/default.aspx
Infection Control
All staff will have access to Infection Control Policies and comply with the standards within them in the work place. All staff will attend Infection Control Training annually as part of their mandatory training programme.
“The Act is intended to assist and support people who may lack capacity and to discourage anyone who is involved in caring for someone who lacks capacity from being overly restrictive or controlling. It aims to balance an individual’s right to make decisions for themselves with their right to be protected from harm if they lack the capacity to make decisions to protect themselves”. (3)

Collated by Clinical Effectiveness Medication Errors, Management and Prevention of Rapid Equality Impact Assessment Page 1 of 1
Rapid (E)quality Impact Assessment (EqIA) (for use when writing policies)
Please contact the Equalities team for guidance:
For South Devon & Torbay CCG, please call 01803 652476 or email [email protected] For Torbay and South Devon NHS Trusts, please call 01803 656676 or email [email protected]
This form should be published with the policy and a signed copy sent to your relevant organisation.
Policy Title (and number) Medication Errors, Management and Prevention
of 1537
Version and Date Version 3
Policy Author Clinical Governance Pharmacist and Medication Safety Lead
An (e)quality impact assessment is a process designed to ensure that policies do not discriminate or disadvantage
people whilst advancing equality. Consider the nature and extent of the impact, not the number of people affected.
Who may be affected by this document?
Patients/ Service Users ☐ Staff ☐ Other, please state… ☐
Could the policy treat people from protected groups less favorably than the general population? PLEASE NOTE: Any ‘Yes’ answers may trigger a full EIA and must be referred to the equality leads below
Age Yes ☐ No☒ Gender Reassignment Yes ☐ No☒ Sexual Orientation Yes ☐ No☒
Race Yes ☐ No☒ Disability Yes ☐ No☒ Religion/Belief (non) Yes ☐ No☒
Gender Yes ☐ No☒ Pregnancy/Maternity Yes ☐ No☒ Marriage/ Civil Partnership Yes ☐ No☒
Is it likely that the policy could affect particular ‘Inclusion Health’ groups less favorably than the general population? (substance misuse; teenage mums; carers
1; travellers
2; homeless
3;
convictions; social isolation4; refugees)
Yes ☐ No☐
Please provide details for each protected group where you have indicated ‘Yes’.
VISION AND VALUES: Policies must aim to remove unintentional barriers and promote inclusion
Is inclusive language5 used throughout? Yes ☒ No☐ NA ☐
Are the services outlined in the policy fully accessible6? Yes ☒ No☐ NA ☐
Does the policy encourage individualised and person-centred care? Yes ☒ No☐ NA ☐
Could there be an adverse impact on an individual’s independence or autonomy7? Yes ☐ No☒ NA ☐
EXTERNAL FACTORS
Is the policy a result of national legislation which cannot be modified in any way? Yes ☐ No☒
What is the reason for writing this policy? (Is it a result in a change of legislation/ national research?)
Who was consulted when drafting this policy?
Patients/ Service Users ☐ Trade Unions ☐ Protected Groups (including Trust Equality Groups) ☐
Staff ☒ General Public ☐ Other, please state… ☐
What were the recommendations/suggestions?
Does this document require a service redesign or substantial amendments to an existing process? PLEASE NOTE: ‘Yes’ may trigger a full EIA, please refer to the equality leads below
Yes ☐ No☒
ACTION PLAN: Please list all actions identified to address any impacts
Action Person responsible Completion date
AUTHORISATION: By signing below, I confirm that the named person responsible above is aware of the actions assigned to them
Name of person completing the form Medication Safety Officer & Governance Pharmacist
Signature
Validated by (line manager) Signature

Collated by Clinical Effectiveness Medication Errors, Management and Prevention of New Data Protection Regulation Page 1 of 1
Clinical and Non-Clinical Policies – New Data Protection Regulation (NDPR) Torbay and South Devon NHS Foundation Trust (TSDFT) has a commitment to ensure that all policies and procedures developed act in accordance with all relevant data protection regulations and guidance. This policy has been designed with the EU New Data Protection Regulation (NDPR) in mind and therefore provides the reader with assurance of effective information governance practice. NDPR intends to strengthen and unify data protection for all persons; consequently, the rights of individuals have changed. It is assured that these rights have been considered throughout the development of this policy. Furthermore, NDPR requires that the Trust is open and transparent with its personal identifiable processing activities and this has a considerable effect on the way TSDFT holds, uses, and shares personal identifiable data. The most effective way of being open is through data mapping. Data mapping for NDPR was initially undertaken in November 2017 and must be completed on a triannual (every 3 years) basis to maintain compliance. This policy supports the data mapping requirement of the NDPR. For more information:
Contact the Data Access and Disclosure Office on [email protected],
See TSDFT’s Data Protection & Access Policy,
Visit our GDPR page on ICON.