
Tissue Renewal, Regeneration, and Repair · PDF fileT1 3 Tissue Renewal, Regeneration, and...
20
3 Tissue Renewal, Regeneration, and Repair Control of Normal Cell Proliferation and Tissue Growth Tissue Proliferative Activity Stem Cells Embryonic Stem Cells Reprogramming of Differentiated Cells: Induced Pluripotent Stem Cells Adult (Somatic) Stem Cells Stem Cells in Tissue Homeostasis Cell Cycle and the Regulation of Cell Replication Growth Factors Signaling Mechanisms in Cell Growth Receptors and Signal Transduction Pathways Transcription Factors Mechanisms of Tissue and Organ Regeneration Liver Regeneration Extracellular Matrix and Cell-Matrix Interactions Collagen Elastin, Fibrillin, and Elastic Fibers Cell Adhesion Proteins Glycosaminoglycans (GAGs) and Proteoglycans Healing by Repair, Scar Formation, and Fibrosis Mechanisms of Angiogenesis Growth Factors and Receptors Involved in Angiogenesis ECM Proteins as Regulators of Angiogenesis Cutaneous Wound Healing Local and Systemic Factors That Influence Wound Healing Pathologic Aspects of Repair Fibrosis 79 Injury to cells and tissues sets in motion a series of events that contain the damage and initiate the healing process. This process can be broadly separated into regeneration and repair (Fig. 3–1). Regeneration results in the complete restitution of lost or damaged tissue; repair may restore some original structures but involves collagen deposition and scar formation. In healthy tissues, healing, in the form of regeneration or repair, occurs after practically any insult that causes tissue destruction, and is essential for the survival of the organism. 1 Regeneration refers to the proliferation of cells and tissues to replace lost structures, such as the growth of an amputated limb in amphibians. In mammals, whole organs and com- plex tissues rarely regenerate after injury, and the term is usually applied to processes such as liver growth after partial resection or necrosis, but these processes consist of compensa- tory growth rather than true regeneration. 2 Regardless, the term regeneration is well established and is used throughout this book. Tissues with high proliferative capacity, such as the hematopoietic system and the epithelia of the skin and gastrointestinal (GI) tract, renew themselves continuously and can regenerate after injury, as long as the stem cells of these tissues are not destroyed. 3 Repair most often consists of a combination of regeneration and scar formation by the deposition of collagen. The relative
Transcript of Tissue Renewal, Regeneration, and Repair · PDF fileT1 3 Tissue Renewal, Regeneration, and...

T1
3
Tissue Renewal, Regeneration, and Repair
Control of Normal Cell Proliferation and Tissue Growth
Tissue Proliferative ActivityStem Cells
Embryonic Stem CellsReprogramming of Differentiated Cells:
Induced Pluripotent Stem Cells Adult (Somatic) Stem CellsStem Cells in Tissue Homeostasis
Cell Cycle and the Regulation of Cell Replication
Growth FactorsSignaling Mechanisms in Cell Growth
Receptors and Signal Transduction Pathways
Transcription Factors
Mechanisms of Tissue and Organ Regeneration
Liver Regeneration
Extracellular Matrix and Cell-Matrix Interactions
CollagenElastin, Fibrillin, and Elastic FibersCell Adhesion ProteinsGlycosaminoglycans (GAGs) and
Proteoglycans
Healing by Repair, Scar Formation, and Fibrosis
Mechanisms of AngiogenesisGrowth Factors and Receptors
Involved in AngiogenesisECM Proteins as Regulators of
AngiogenesisCutaneous Wound HealingLocal and Systemic Factors That Influence
Wound HealingPathologic Aspects of Repair
Fibrosis
79
Injury to cells and tissues sets in motion a series of events that contain the damage and initiate the healing process. This process can be broadly separated into regeneration and repair (Fig. 3–1). Regeneration results in the complete restitution of lost or damaged tissue; repair may restore some original structures but involves collagen deposition and scar formation. In healthy tissues, healing, in the form of regeneration or repair, occurs after practically any insult that causes tissue destruction, and is essential for the survival of the organism.1
Regeneration refers to the proliferation of cells and tissues to replace lost structures, such as the growth of an amputated limb in amphibians. In mammals, whole organs and com-
plex tissues rarely regenerate after injury, and the term is usually applied to processes such as liver growth after partial resection or necrosis, but these processes consist of compensa-tory growth rather than true regeneration.2 Regardless, the term regeneration is well established and is used throughout this book. Tissues with high proliferative capacity, such as the hematopoietic system and the epithelia of the skin and gastrointestinal (GI) tract, renew themselves continuously and can regenerate after injury, as long as the stem cells of these tissues are not destroyed.3
Repair most often consists of a combination of regeneration and scar formation by the deposition of collagen. The relative
Ch003-X3121.indd 79 12/1/2008 3:44:21 PM
Administrator
Typewriter
Dr. Upik A. Miskad, PhD, SpPA
Administrator
Typewriter
2008
Administrator
Typewriter
http://media.axon.es/pdf/72856.pdf
userr
Textbox
1. Miskad2008 (truncated)

T1
CHAPTER 3 Tissue Renewal, Regeneration, and Repair 93
LIVER REGENERATION
The human liver has a remarkable capacity to regenerate, as demonstrated by its growth after partial hepatectomy, which may be performed for tumor resection or for living-donor hepatic transplantation (Fig. 3–11). The popular image of liver regen-eration is the daily regrowth of the liver of Prometheus, which was eaten every day by an eagle sent by Zeus (Zeus was angry at Prometheus for stealing the secret of fire, but did he know that Prometheus’s liver would regenerate?). The reality, although less dramatic, is still quite impressive. In humans, resection of approximately 60% of the liver in living donors results in the doubling of the liver remnant in about one month. The portions of the liver that remain after partial hepatectomy constitute an intact “mini-liver” that rapidly expands and reaches the mass of the original liver (see Fig. 3–11). Restoration of liver mass is achieved without the regrowth of the lobes that were resected at the operation. Instead, growth
occurs by enlargement of the lobes that remain after the oper-ation, a process known as compensatory growth or compensa-tory hyperplasia. In both humans and rodents, the end point of liver regeneration after partial hepatectomy is the restitu-tion of functional mass rather than the reconstitution of the original form.69
Almost all hepatocytes replicate during liver regeneration after partial hepatectomy. Because hepatocytes are quiescent cells, it takes them several hours to enter the cell cycle, progress through G1, and reach the S phase of DNA replication. The wave of hepatocyte replication is synchronized and is followed by synchronous replication of nonparenchymal cells (Kupffer cells, endothelial cells, and stellate cells).
There is substantial evidence that hepatocyte proliferation in the regenerating liver is triggered by the combined actions of cytokines and polypeptide growth factors. With the exception of the autocrine activity of TGF-a, hepatocyte replication is
Regeneration
C
LL
M
RL
A
B
RL
G2G1
Priming
Cytokines
Growthfactors
Quiescence
G0
M
S
Progression
C
FIGURE 3–11 Liver regeneration after partial hepatectomy. A, The lobes of the liver of a rat (M, median; RL and LL, right and left lateral lobes; C, caudate lobe). Partial hepatectomy removes two thirds of the liver (median and left lateral lobes). After 3 weeks the right lateral and caudate lobes enlarge to reach a mass equivalent to that of the original liver without regrowth of the median and left lateral lobes. B, Entry and progression of hepatocytes in the cell cycle (see text for details). C, Regeneration of the human liver in living-donor transplantation. Computed tomography scans of the donor liver in living-donor hepatic transplantation. Upper panel is a scan of the liver of the donor before the operation. The right lobe, to be used as a transplant, is outlined. Lower panel is a scan of the liver 1 week after performance of partial hepatectomy. Note the great enlargement of the left lobe (outlined in the panel) without regrowth of the right lobe. (A, From Goss RJ: Regeneration versus repair. In Cohen IK et al [eds]: Wound Healing. Biochemical and Clinical Aspects. Philadelphia, WB Saunders, 1992, pp 20–39; C, courtesy of R. Troisi, MD, Ghent University, Ghent, Belgium; reproduced in part from Fausto N: Liver regeneration. In Arias I, et al: The Liver: Biology and Pathobiology, 4th ed. Philadelphia, Lippincott Williams & Wilkins, 2001.)
Ch003-X3121.indd 93 12/1/2008 3:44:38 PM
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight

T1
94 CHAPTER 3 Tissue Renewal, Regeneration, and Repair
strictly dependent on paracrine effects of growth factors and cytokines such as HGF and IL-6 produced by hepatic non-parenchymal cells. There are two major restriction points for hepatocyte replication: the G0/G1 transition that bring quies-cent hepatocytes into the cell cycle, and the G1/S transition needed for passage through the late G1 restriction point. Gene expression in the regenerating liver proceeds in phases, start-ing with the immediate early gene response, which is a tran-sient response that corresponds to the G0/G1 transition. More than 70 genes are activated during this response, including the proto-oncogenes c-FOS and c-JUN, whose products dimerize to form the transcription factor AP-1; c-MYC, which encodes a transcription factor that activates many different genes; and other transcription factors, such as NF-kB, STAT-3, and C/EBP.70 The immediate early gene response sets the stage for the sequential activation of multiple genes, as hepatocytes prog-ress into the G1 phase. The G1 to S transition occurs as previ-ously described (see Fig. 3–7).
Quiescent hepatocytes become competent to enter the cell cycle through a priming phase that is mostly mediated by the cytokines TNF and IL-6, and components of the complement system. Priming signals activate several signal transduction pathways as a necessary prelude to cell prolifera-tion. Under the stimulation of HGF, TGFa, and HB-EGF, primed hepatocytes enter the cell cycle and undergo DNA replication (Fig. 3–11). Norepinephrine, serotonin, insulin, thyroid and growth hormone, act as adjuvants for liver regen-eration, facilitating the entry of hepatocytes into the cell cycle.
Individual hepatocytes replicate once or twice during regeneration and then return to quiescence in a strictly regu-lated sequence of events, but the mechanisms of growth ces-sation have not been established. Growth inhibitors, such as TGF-b and activins, may be involved in terminating hepato-cyte replication, but there is no clear understanding of their mode of action. Intrahepatic stem or progenitor cells do not play a role in the compensatory growth that occurs after partial hepa-tectomy, and there is no evidence for hepatocyte generation from bone marrow–derived cells during this process.28,37 However, endothelial cells and other nonparenchymal cells in the regenerating liver may originate from bone marrow precursors.
Extracellular Matrix and Cell-Matrix InteractionsTissue repair and regeneration depend not only on the activity of soluble factors, but also on interactions between cells and the components of the extracellular matrix (ECM). The ECM regulates the growth, proliferation, movement, and differen-tiation of the cells living within it. It is constantly remodeling, and its synthesis and degradation accompanies morphogene-sis, regeneration, wound healing, chronic fibrotic processes, tumor invasion, and metastasis. The ECM sequesters water, providing turgor to soft tissues, and minerals that give rigidity to bone, but it does much more than just fill the spaces around cells to maintain tissue structure. Its various functions include:
Mechanical support for cell anchorage and cell migration, and maintenance of cell polarity
Control of cell growth. ECM components can regulate cell proliferation by signaling through cellular receptors of the integrin family.
Maintenance of cell differentiation. The type of ECM pro-teins can affect the degree of differentiation of the cells in the tissue, also acting largely via cell surface integrins.
Scaffolding for tissue renewal. The maintenance of normal tissue structure requires a basement membrane or stromal scaffold. The integrity of the basement membrane or the stroma of the parenchymal cells is critical for the organized regeneration of tissues. It is particularly noteworthy that although labile and stable cells are capable of regeneration, injury to these tissues results in restitution of the normal structure only if the ECM is not damaged. Disruption of these structures leads to collagen deposition and scar formation (see Fig. 3–2).
Establishment of tissue microenvironments. Basement membrane acts as a boundary between epithelium and underlying connective tissue and also forms part of the filtration apparatus in the kidney.
Storage and presentation of regulatory molecules. For example, growth factors like FGF and HGF are secreted and stored in the ECM in some tissues. This allows the rapid deployment of growth factors after local injury, or during regeneration.
The ECM is composed of three groups of macromolecules: fibrous structural proteins, such as collagens and elastins that provide tensile strength and recoil; adhesive glycoproteins that connect the matrix elements to one another and to cells; and proteoglycans and hyaluronan that provide resilience and lubrication. These molecules assemble to form two basic forms of ECM: interstitial matrix and basement membranes. The interstitial matrix is found in spaces between epithelial, endo-thelial, and smooth muscle cells, as well as in connective tissue. It consists mostly of fibrillar and nonfibrillar collagen, elastin, fibronectin, proteoglycans, and hyaluronan. Basement mem-branes are closely associated with cell surfaces, and consist of nonfibrillar collagen (mostly type IV), laminin, heparin sulfate, and proteoglycans.71
We will now consider the main components of the ECM.
COLLAGEN
Collagen is the most common protein in the animal world, pro-viding the extracellular framework for all multicellular organ-isms. Without collagen, a human being would be reduced to a clump of cells, like the “Blob” (the “gelatinous horror from outer space” of 1950s movie fame), interconnected by a few neurons. Currently, 27 different types of collagens encoded by 41 genes dispersed on at least 14 chromosomes are known72 (Table 3–2). Each collagen is composed of three chains that form a trimer in the shape of a triple helix. The polypeptide is characterized by a repeating sequence in which glycine is in every third position (Gly-X-Y, in which X and Y can be any amino acid other than cysteine or tryptophan), and it contains
Ch003-X3121.indd 94 12/1/2008 3:44:38 PM
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight

A Model of Liver Regeneration
Leon A. Furchtgott,† Carson C. Chow,‡ and Vipul Periwal‡*†Department of Physics, Princeton University, Princeton, New Jersey; and ‡Laboratory of Biological Modeling, National Institute of Diabetes andDigestive and Kidney Diseases, National Institutes of Health, Bethesda, Maryland
ABSTRACT The network of interactions underlying liver regeneration is robust and precise with liver resections resulting incontrolled hyperplasia (cell proliferation) that terminates when the liver regains its lost mass. The interplay of cytokines andgrowth factors responsible for the inception and termination of this hyperplasia is not well understood. A model is developedfor this network of interactions based on the known data of liver resections. This model reproduces the relevant publisheddata on liver regeneration and provides geometric insights into the experimental observations. The predictions of this modelare used to suggest two novel strategies for speeding up liver mass recovery and a strategy for enabling liver mass recoveryin cases where a resection leaves <20% of the liver that would otherwise result in complete loss of liver mass.
INTRODUCTION
The liver’s ability to regenerate has been known since
ancient times and has been the subject of scientific study
since the early 20th century (1). After a partial hepatectomy
(removal of a section of the liver), liver cells reenter the cell
cycle and replicate until the liver recovers its lost mass,
within a precision of 10% (2). Although numerous studies
have investigated the molecular mechanisms of liver regen-
eration, including the roles of cytokines, growth factors,
matrix remodeling, and metabolic signals (3,4), several basic
questions remain. How does the liver integrate signals from
different signaling pathways and from metabolic stresses,
including detoxification functions, in order to control cell
replication? How does liver regeneration stop once the liver
reaches its original mass, and how does the liver avoid an
oscillatory cycle of overgrowth and apoptosis? This article
proposes a simple mathematical model for liver regeneration
to answer these questions.
In a healthy adult liver, only ~1 hepatocyte in 20,000
(0.005%) is in the cell cycle (5). The rest are quiescent, in
the G0 state. After partial hepatectomy, hepatocytes reenter
the cell cycle by going from the G0 state to the G1 phase.
Cells in the early G1 phase progress, driven by growth
factors, through the G1/S restriction point, after which cells
are committed to progress to mitosis, even in the absence of
the G1 growth factors. However, cells in early G1 phase that
have not reached the restriction point can return to quies-
cence in the absence of growth factors (6). Following Fausto
and Riehle (3), we consider three subpopulations of hepato-
cytes in our model: quiescent cells (Q), primed cells (P), and
replicating cells (R).
In the priming phase of liver regeneration, multiple imme-
diate-early genes such as c-fos and c-jun are induced (7).
These immediate-early genes (IE) take liver cells from the
G0 phase to the G1 phase of the cell cycle. The level of
expression of immediate-early genes, in turn, is controlled
in large part by a network of cytokines (8,9). Levels of tumor
necrosis factor (TNF) increase after partial hepatectomy (10).
TNF binds to its receptor on Kupffer cells, which activates
the transcription factor nuclear factor-kB, which leads to
increased interleukin-6 (IL-6) transcription and production.
IL-6 binds to its receptor on hepatocytes. The receptor inter-
acts with gp130 and activates two Janus kinase (JAK)
proteins. JAK phosphorylates monomeric signal transducer
and activator of transcription 3 (STAT3), which then imme-
diately homodimerizes to the active form (11). JAK also acti-
vates the mitogen-activated protein kinase pathway. STAT3
promotes transcription of many immediate-early genes,
including suppressor of cytokine signaling 3 (SOCS3),
which binds to JAK proteins and blocks further signaling
through competitive inhibition with inactive STAT3 (12).
Thus, the negative feedback mechanism of SOCS3 ensures
an initial spike in transcription, after which quiescent cells
can no longer enter the cell cycle.
Once cells have entered the G1 phase, their progression
through the cell cycle to the proliferating phase is driven
by growth factors (GF). The most important growth factor
for liver regeneration is hepatocyte growth factor (HGF),
which binds to the c-met receptor (13,14). Pro-HGF, an inac-
tive form of HGF, is depleted from the extracellular matrix
during the first three hours after partial hepatectomy, after
which it is produced by nonparenchymal cells (15). Uroki-
nase-type plasminogen activator activates pro-HGF and is
detected within the first 5 min after partial hepatectomy
(16). Other growth factors include epidermal growth factor
(EGF) (17), transforming growth factor a (18), and heparin-
binding EGF-like growth factor (HB-EGF) (19). In the
absence of growth factors, cells return to quiescence. Once
cells are in the replicating phase, the length of the cell cycle
is fairly fixed.
The extracellular matrix (ECM) plays an important role in
the regulation of liver regeneration (20). After partial hepa-
tectomy, the ECM is degraded by matrix metalloproteinases
Submitted October 2, 2008, and accepted for publication January 8, 2009.
*Correspondence: [email protected]
Editor: Alexander Mogilner.
� 2009 by the Biophysical Society
0006-3495/09/05/3926/10 $2.00 doi: 10.1016/j.bpj.2009.01.061
3926 Biophysical Journal Volume 96 May 2009 3926–3935
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Textbox
2. Furchtgott2009 (truncated)

In these latter two contexts, it is crucial to experimentally
determine specifically which of the myriad metabolic
demands on the liver are most important as factors in the over-
all quantity we have characterized as the metabolic load M.
DISCUSSION
Our model relies on distinguishing between three cell phases,
as suggested by Fausto et al. (9): quiescent cells, primed cells
and replicating cells. The addition of a primed phase, in addi-
tion to the traditional quiescent and replicating phases, allows
for much greater control of cell proliferation. The initial cyto-
kine burst, the size of which depends on the metabolic load,
takes cells from the quiescent state to the primed state. One
important control mechanism is that after the initial burst,
cells can no longer be primed: once cells return to quiescence,
they cannot enter the cell cycle again. Another control mech-
anism is that primed cells can make a decision between
proceeding to the replicating phase and returning to the quies-
cent phase. Under elevated levels of growth factors, primed
cells continue to the replicating phase; under low levels of
growth factors, they return to quiescence. The level of growth
factor depends on the size of the liver both in terms of growth
factor production, which is proportional to the metabolic load,
and in terms of growth factor inactivation, which is propor-
tional to the size of the ECM. Finally, the number of cells in
the proliferating state depends on the balance between the
body’s metabolic needs and the size of the ECM, which grows
back as the metabolic load decreases.
DNA synthesis occurs at different times in liver paren-
chymal and nonparenchymal cells (8). Since the ECM is
produced by nonparenchymal cells, whereas the metabolic
load is relieved by the growth of parenchymal cells, it is
possible to envisage a model in which the control of liver
growth depends on a coordination between the parenchymal
and nonparenchymal cell cycles. Our model does not distin-
guish between different types of liver cells, suggesting that
the difference in cell cycle parameters is not necessary for
liver regeneration to occur.
Our model shows a steady and smooth regrowth of the
liver. However, early studies of liver regeneration (1,38)
report several waves of liver growth, presumably correspond-
ing to different rounds of cell division (after a 2/3 resection,
each cell reproduces on average 1.6 times). This aspect of
liver regeneration, though not included in our model of regen-
eration, could easily be captured in a stochastic version of our
model.
While liver regeneration is a complex process (4,8) at the
molecular level, the simplicity of our mathematical model
suggests that liver regeneration is not a complex process in
the mathematical sense: it involves (excluding degeneracies)
a small number of pathways that relate liver growth to the
body’s metabolic needs and elegantly succeed in tightly
controlling the regenerative process. The framework that
we have developed here may help guide the development
of future experiments and therapies.
This research was supported by the Intramural Research Program of the U.S.
National Institutes of Health, National Institute of Diabetes and Digestive
and Kidney Diseases.
REFERENCES
1. Higgins, G., and R. Anderson. 1931. Restoration of the liver of thewhite rat following partial surgical removal. Arch. Pathol. (Chic).12:186–202.
2. Fausto, N. 1997. Hepatocytes break the rules of senescence in serialtransplantation studies—is there a limit to their replicative capacity?Am. J. Pathol. 151:1187–1189.
3. Fausto, N., and K. J. Riehle. 2005. Mechanisms of liver regenerationand their clinical implications. J. Hepatobiliary Pancreat. Surg.12:181–189.
4. Michalopoulos, G. K. 2007. Liver regeneration. J. Cell. Physiol.213:286–300.
5. Mangnall, D., N. C. Bird, and A. W. Majeed. 2003. The molecularphysiology of liver regeneration following partial hepatectomy. LiverInt. 23:124–138.
6. Heath, J. K. 2000. Principles of Cell Proliferation. Blackwell Science,Oxford, UK.
7. Su, A. I., L. G. Guidotti, J. P. Pezacki, F. V. Chisari, and P. G. Schultz.2002. Gene expression during the priming phase of liver regenerationafter partial hepatectomy in mice. Proc. Natl. Acad. Sci. USA.99:11181–11186.
8. Taub, R. 2004. Liver regeneration: from myth to mechanism. Nat. Rev.Mol. Cell Biol. 5:836–847.
9. Fausto, N., J. S. Campbell, and K. J. Riehle. 2006. Liver regeneration.Hepatology. 43:S45–S53.
10. Iwai, M., T.-X. Cui, H. Kitamura, M. Saito, and T. Shimazu. 2001.Increased secretion of tumor necrosis factor and interleukin 6 fromisolated, perfused liver of rats after partial hepatectomy. Cytokine.13:60–64.
11. Levy, D. E., and J. D. Jr. 2002. STATs: transcriptional control and bio-logical impact. Natl. Rev. 3:651–662.
12. Campbell, J. S., L. Prichard, F. Schaper, J. Schmitz, A. Stephenson-Famy, et al. 2001. Expression of suppressors of cytokine signalingduring liver regeneration. J. Clin. Invest. 107:1285–1292.
FIGURE 8 Liver regeneration under decreased metabolic load. After an
85% partial hepatectomy, the metabolic load was halved for 48 h before
being raised to normal at time 48 h (dashed line). The diagonal, cross-
hatched, and solid areas represent quiescent, primed, and replicating cells,
respectively.
Biophysical Journal 96(10) 3926–3935
3934 Furchtgott et al.
userr
Highlight

The identification of stem cells in human liver diseases and hepatocellular carcinoma
Joan Oliva, Barbara A. French, X. Qing, Samuel W. French ⁎Department of Pathology, Harbor-UCLA Medical Center, Torrance, CA 90509, USA
a b s t r a c ta r t i c l e i n f o
Article history:Received 23 December 2009Available online 18 January 2010
Keywords:Epidermal growth factor (EGF)Hepatocyte growth factor (HGF)Glutathione S-transferase placental (GST-P)O. volvulus 6 (OV-6)AIR (antisense Igf2r)
Liver stem cells are thought to preside in bile ducts and the canals of Hering. They extend into the liverparenchyma at a time when normal liver cell proliferation is suppressed and liver regeneration isstimulated. In the present study 69 liver biopsies and surgically excised liver tumors were studied for thepresence of liver stem cells. It was found that human cirrhotic livers and hepatocellular carcinomas (HCC)frequently exhibited isolated single scattered hepatocyte stem cells within the liver parenchyma ratherthan in the portal tract, bile duct or the canal of Hering. These cells expressed liver stem cell markers. HCCsalso contained isolated tumor cell which expressed the same stem cell markers. The markers used wereGST-P, OV-6, CK-19, Oct-3/4 and FAT10. They were identified by immunofluorescent antibody staining.HGF, EGF, CK19, AIR, H19, Nanog, Oct-3/4 and FAT10 were identified by RNA-FISH. H19 is a non-codingRNA, which is expressed in most HCCs. Results: Immunohistochemistry and RNA-FISH performed on humanlivers identified isolated stem cells in liver parenchyma as follows: Stem cells identified byimmunohistochemical markers (OV-6 and GST-P) and RNA-FISH markers (HGF, EGF, CK19 and H19) werefound scattered in the liver parenchyma of cirrhotic livers and within hepatocellular carcinomas (HCCs).Precirrhotic ASH or NASH all stained negative for these stem cells. In HCCs, 13 out of 15 had stem cellslocated within the tumor (78%). In cirrhotic livers, 12 out of 28 (37%) had liver parenchymal stem cellspresent. In one case of stage 3 precirrhosis, stem cells were also found. Double staining for the markersshowed colocalization of the markers in stem cells. Stem cells were found in 33% of HBV, 47% of HCV, 25% ofalcoholic steatohepatitis (ASH) and 17% of non-alcoholic steatohepatitis (NASH). The frequency of stemcells found in the different disease categories correlates with the frequency of HCC occurring in thesedifferent diseases.
© 2010 Elsevier Inc. All rights reserved.
Introduction
The liver plays a central role in metabolic homeostasis, as it isresponsible for the metabolism, synthesis, storage and redistributionof nutrients, carbohydrates, fats and vitamins (Saxema et al., 2003).Importantly, it is the main detoxifying organ of the body, whichremoves wastes and xenobiotics by metabolic conversion and biliaryexcretion. The main cell type of the liver that carries out most ofthese functions is the parenchymal cell, or hepatocyte, which makesup ∼80% of cells, in the liver. Although adult hepatocytes are longlived and normally have a low rate of cell division, they maintain theability to proliferate in response to toxic injury and infection (Cantzet al., 2008). The amazing regenerative capacity of the liver is mostclearly shown by the two-thirds partial-hepatectomy model in
rodents, which was pioneered by Higgins and Anderson in 1931(Higgins and Anderson, 1931). Cell division is rarely seen inhepatocytes in the normal adult liver, as these cells are in the G0phase of the cell cycle (Michalopoulos and DeFrances, 1997; Taubet al., 1999). The degree of replication of these cells correlates withthe degree of inflammation and fibrosis in diseases such as chronichepatitis, hemochromatosis, alcoholic and non-alcoholic steatohe-patitis (Libbrecht et al., 2000; Lowes et al., 1999). However, afterpartial hepatectomy approximately 95% of hepatic cells, which arenormally quiescent, rapidly re-enter the cell cycle. The onset ofDNA synthesis is well synchronized in hepatocytes, beginning incells that surround the portal vein of the liver lobule and proceedingtowards the central vein (Minuk, 2003). Many growth factors areinvolved in the regeneration of the liver: hepatocyte growth factor(HGF) (Nishino et al., 2008), epidermal growth factor (EGF)(Natarajan et al., 2007), transforming growth factors (TGFs)(Weymann et al., 2009), insulin (Stefano et al., 2006), glucagon(Kothary et al., 1995) and insulin like growth factor (Sanz et al.,2005).
In animal models, in which hepatocytes are directly damaged andthereby induced to undergo necrosis. His resembles simulates
Experimental and Molecular Pathology 88 (2010) 331–340
⁎ Corresponding author. Department of Pathology, LA Biomedical Institute, 1124West Carson Street, Torrance, CA 90502, USA.
E-mail address: [email protected] (S.W. French).
0014-4800/$ – see front matter © 2010 Elsevier Inc. All rights reserved.doi:10.1016/j.yexmp.2010.01.003
Contents lists available at ScienceDirect
Experimental and Molecular Pathology
j ourna l homepage: www.e lsev ie r.com/ locate /yexmp
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Textbox
3. Oliva2010 (truncated)

Liver RegenerationGEORGE K. MICHALOPOULOS*
Department of Pathology, University of Pittsburgh School of Medicine, Pittsburgh, Pennsylvania
Liver regeneration after partial hepatectomy is a very complex andwell-orchestrated phenomenon. It is carried out by the participation ofall mature liver cell types. The process is associated with signaling cascades involving growth factors, cytokines, matrix remodeling, andseveral feedbacks of stimulation and inhibition of growth related signals. Livermanages to restore any lostmass and adjust its size to that ofthe organism, while at the same time providing full support for body homeostasis during the entire regenerative process. In situationswhen hepatocytes or biliary cells are blocked from regeneration, these cell types can function as facultative stem cells for each other.J. Cell. Physiol. 213: 286–300, 2007. � 2007 Wiley-Liss, Inc.
Liver is an interesting organ with high regenerative capacity andcomplex functions (Michalopoulos and DeFrances, 1997; Taub,2004;Michalopoulos andKhan, 2005c; Fausto et al., 2006). Liverreceives all exiting circulation from the small and most of thelarge intestine, as well as spleen and pancreas, through theportal vein. Its ‘‘strategic’’ location in relation to the food supplyvia the portal vein, and the unique gene- and protein-expressionpatterns of hepatocytes (the main functional cells of the liver)allow it to function as a biochemical defense against toxicchemicals entering through the food and as a re-processor ofabsorbed food ingredients. Nutrients entering the liver aretransformed into secreted proteins (albumin, most coagulationfactors, several plasma carrier proteins etc. in the peripheralblood), lipids sent as lipoproteins into the other tissues,carbohydrates stored in the liver as glycogen (the main glucosereserve used for stabilization of glucose levels in the blood).Synthesis of bile is essential for absorption of fat and lipophilicnutrients. As a major regulator of plasma glucose and ammonialevels, liver is essential for optimal function of the brain. Loss ofliver function leads to chronic ‘‘hepatic encephalopathy’’ andeventually coma. Thewide array of functions performed by livertowards the rest of the body has been safeguarded byevolutionary events which imparted to liver a phenomenalcapacity to regenerate. This process allows liver to recover lostmass without jeopardizing viability of the entire organism. Thephenomenon of liver regeneration following loss of livermass isseen in all vertebrate organisms, from humans to fish. It is alsotriggered when livers from small animals (e.g., dogs) aretransplanted to large recipients of the same species. It has beenrecorded and mythologized in ancient times from the myth ofPrometheus and libraries of clay tables picturing scarred liversof sacrificial animals, used to foretell the future in ancientBabylon and Rome (Michalopoulos and DeFrances, 1997).
Loss of liver mass can be induced by administeringhepatotoxic chemicals (e.g., carbon tetrachloride). This isfollowed by an inflammatory response which removes tissuedebris, followed by the regenerative response. Mostcommonly, however, regeneration of the liver is studied byperforming a surgical procedure which removes 2/3 of the livermass in rodents (rats and mice), a technique known as 2/3partial hepatectomy (PHx) (Higgins, 1931). Due to the multi-lobe structure of the rodent liver, three of the five liver lobes(representing 2/3 of the liver mass) can be removed by an easysurgical procedure, without causing any tissue damage to theresidual two lobes. The latter grow in size to restore anaggregate equivalent to the mass of the original five lobes. Theprocess, in rats and mice, is complete within 5–7 days aftersurgery. The reproducibility of PHx in terms of mass removedand precision of timing of the sequence of ensuing events hasmade PHx the preferred approach for experimental study ofliver regeneration. In a clinical setting, this procedure is also
done in humans, in order to resect solitary liver metastases orrepair trauma, etc.
PHx triggers a sequence of events that proceed in an orderlyfashion and can be observed from the first 5 min to 5–7 days.Hepatocytes are the first cells to enter into DNA synthesis.A 2/3 PHx leaves a residual 1/3 of hepatocytes. They undergoone round of DNA synthesis (leading to 60% of hepatocytes)which peaks at 24 h for the rat and at approximately 36 h for themouse (Unless otherwise specified, times after PHx referred inthis review will follow the time table of regeneration in the rat,which is more reproducible). A second smaller percent of cellsenter into a second round of DNA synthesis and establish theoriginal number of hepatocytes. A small wave of apoptosis ofhepatocytes seen at the end ofDNA synthesis suggests that thisis a mechanism to correct an over-shooting of the regenerativeresponse (Sakamoto et al., 1999). The proliferation ofhepatocytes advances from periportal to pericentral areas ofthe lobule, as a wave of mitoses (Rabes, 1977). Hepatocytessurrounding the central veins (positive for glutamine synthetase(Gebhardt et al., 2007) are the last ones to undergo cellreplication. Proliferation of biliary epithelial cells occurs a littlelater than hepatocytes. Proliferation of endothelial cells starts at2–3 days and ends around 4–5 days after PHx. The kinetics ofproliferation of stellate cells has not been fully explored. Stellatecells are cells of myofibroblastic origin, surroundinghepatocytes, located under the sinusoidal cells, producingextracellular matrix and several cytokines including HGF, andhaving a gene expression pattern substantially similar to theastrocytes of the brain (Neubauer et al., 1996; Cassiman et al.,2001). It should be emphasized that replacement of the losthepatic mass is mediated through proliferation of mature adulthepatocytes and the other hepatic cell types. It is not mediatedby proliferation of a selective subpopulation of stem cells (as inskin and small intestine). Normal liver weight is reestablishedwithin 5–7 days (8–15 days in humans). At the end ofregeneration, the size of the liver lobules is remarkably largerand the thickness of the hepatocyte plates is almost twice the
Contract grant sponsor: NIH;Contract grant numbers: CA035373, CA103958.Contract grant sponsor: Rangos Fund.
*Correspondence to: George K. Michalopoulos, Department ofPathology, University of Pittsburgh School of Medicine, Pittsburgh,PA 15261. E-mail: [email protected]
Received 7 May 2007; Accepted 9 May 2007
DOI: 10.1002/jcp.21172
MINI-REVIEW 286J o u r n a l o fJ o u r n a l o f
CellularPhysiologyCellularPhysiology
� 2 0 0 7 W I L E Y - L I S S , I N C .
userr
Textbox
4. Michalopoulos2007 (truncated)

size of the normal one cell thickness (Michalopoulos andDeFrances, 1997). Previous studies suggest that there is slowlobular reorganization taking place for several weeks, andeventually liver histology becomes indistinguishable from theoriginal (Wagenaar et al., 1993).
Broadly defined, partial hepatectomy is a type of liver injury,though no immediate histological damage results from it. Thus,it is not surprising that the signaling pathways triggered duringliver regeneration strongly resemble those of wound healing,seen in other tissues. The difference with the classic woundhealing process is that the changes observed in liver occur overthe entire organ (largest single organ in the body!) and thatsome of the signals may be derived in part from the peripheralcirculation.
Hemodynamic Changes Following 2/3Partial Hepatectomy
In a typical wound healing scenario, the injury to the tissueresults in disruption of capillary vascular networks andextravasation of blood, accompanied by local release ofcoagulation factors, platelets, growth factors, etc. (Schafer andWerner, 2007). This is clearly not the case following 2/3 PHx.Three liver lobes are surgically removedwithout damage to theresidual two lobes. Even though there is no damage to theresidual tissue, there are big changes in hepatic blood flowpatterns. There is considerable literature suggesting that theearly hemodynamic changes after PHx are important, and, eventhough there is no extravasation of whole blood, thehemodynamic alterations after PHx induce a global spectrum ofevents across the entire liver that resembles a wound healingresponse. The arterial component of the blood supply per unitof liver tissue does not change after 2/3 PHx; the portalcontribution per unit tissue, however, triples. Portal veincontinues to carry the entire outflow from intestine, spleenand pancreas. The entire flow now needs to traverse througha capillary bed whose cross-section is mathematically down to1/3 of the original. The hepatic capillaries have fenestratedendothelial cellswhich bring direct access of plasma through theendothelial cells to the hepatocytes. A recent studydemonstrated that if these changes are prevented by keepingpressure of the portal vein constant, there is deficient activationof HGF and increased hepatocyte apoptosis, even though thekinetics of PCNA nuclear labeling do not seem to be affected(Marubashi et al., 2004). Another point that needs to be betterunderstood is the potential impact of the change of oxygenpartial pressure in the hepatic blood after PHx. Portal veinblood has amuch lower oxygen concentration compared to thearterial blood. The relative increase in portal blood per unitliver tissue after PHx should result in decreased oxygenpressure in the circulating blood, perhaps triggering a hypoxicresponse. Recent studies however have shown that hypoxia inthe liver may be regulated through pathways different than theclassic ones, since HIF1a is not identified in hepatocyte nuclei,but it is instead seen in peroxisomes and mitochondria (Khanet al., 2006). The tripling of the portal vein contribution shouldalso cause a mathematical tripling in the availability perhepatocyte of growth factors and cytokines derived fromintestine and pancreas. Such factors include insulin andepidermal growth factor (EGF), endotoxin, as well as nutrientsderived from the food supply (amino acids, lipids, andcarbohydrates). Overall, of all aspects of liver regeneration, theimportance of the hemodynamic events and the change ofrelative proportion of portal to arterial blood are the leaststudied and least understood. There is an almost universalagreement however that the aggregate changes describedabove trigger the better understood and better studied changesof signaling pathways in liver tissue, described below.
Early Events Occurring in Liver After PHx
PHx induces rapid induction of more than 100 genes notexpressed in normal liver (Taub, 1996, 2004). These genesrelate directly or indirectly to preparative events for the entryof hepatocytes into the cell cycle. The functions served areseveral andmany of these genes (e.g., IGFBP1) appear to play anessential role. Mice deficient in IGFBP1, for example, havedeficient regenerative response (Leu et al., 2003). The preciserole of the many genes expressed early in liver regeneration isnot always clear and the early changes in gene expressionshould be viewed as serving both the entry of hepatocytes intothe cell cycle as well the orchestration of specific adjustmentsthat hepatocytes have to make, so that they can deliver allessential hepatic functions while going through cellproliferation. Given the fact that more than 95% of hepatocytesgo through cell proliferation during 48 h, it is truly amazing thatthe support provided by liver to the whole body is notperceptibly diminished during regeneration. One of the earliestobserved biochemical changes is increase in activity of urokinaseplasminogen activator (uPA) (Fig. 1). This occurs over theentire tissue of the remnant lobes. As seen in early stages ofwound healing (Kortlever and Bernards, 2006), there isincrease in uPA activity throughout the entire liver starting asearly as 5 min after PHx (Mars et al., 1995). The relationshipbetween increase in uPA and the hemodynamic changesdiscussed above is not clear, but there is literature documentingincrease of uPA in several cell types including endothelial cellsfollowingmechanical stress associatedwith increased turbulentflow (Sokabe et al., 2004). Thus, alterations of vascular flowpatterns alone can trigger some of the early events. Increase inuPA activity is accompanied by activation of plasminogen toplasmin (within 10 min) and appearance of fibrinogendegradation products (Kim et al., 1997). Urokinase is known toactivate matrix remodeling, seen in most tissues during woundhealing and also in liver regeneration. Many proteins of theextracellular matrix are subject to turnover (Kim et al., 1997).The first evidence of activation of metalloproteinase 9 (MMP9)is seen at 30 min and further into the first 24–48 h after PHx(Kim et al., 2000). Studies from wound healing and tumorbiology have shown that matrix remodeling causes signalingthough integrins and is associated with release of locally boundgrowth factors and peptides that have signaling capabilities(Swindle et al., 2001). While there is not much proteinaceousmatrix in the liver visible under the microscope, there is a greatabundance of heavily glycosylated proteins in the pericellularspace surrounding hepatocytes. Glycosaminoglycans are veryabundant in liver and heparin, a shorter derivative, owes itsname to liver (‘‘hepar’’). Overall regulation of extracellularmatrix during liver regeneration is a very complex process,involving metalloproteinases and tissue inhibitors ofmetalloproteinases (Mohammed and Khokha, 2005a). Hepaticextracellular matrix binds many growth factors. Prominentamong matrix binding growth factors in the liver is hepatocytegrowth factor (HGF) (Masumoto and Yamamoto, 1991, 1993).Inactive, single-chain HGF bound to hepatic biomatrix is locallyreleased during matrix remodeling and activated to its activeheterodimeric form by uPA (Mars et al., 1993, 1995) (HGF ishighly homologous to plasminogen, the recognized classictarget of uPA; HGF and plasminogen have the same consensussequence (RVV) at their activation site). Activated HGF isavailable locally, but it also overflows in the circulation(Lindroos et al., 1991). Pre-existing stores of inactive and activeHGF rapidly diminish with the first 3 h after PHX, as HGF risesin the plasma by 10- to 20-fold (Pediaditakis et al., 2001).Metalloproteinases and TIMP levels are important in regulationof release of HGF and its availability for activation duringregeneration (Mohammed et al., 2005b). Studies withhepatocytes in culture suggest that TNF may play a role in this
JOURNAL OF CELLULAR PHYSIOLOGY DOI 10.1002/JCP
L I V E R R E G E N E R A T I O N 287
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
pathways leading to proliferation. At 6 h after PHx there is clearevidence for activation of cyclin D1. Amino acids and TOR playa regulatory role in this process (Nelsen et al., 2003). In the rat,the first round of DNA synthesis in hepatocytes begins at 12 hafter PHx, with a peak of DNA synthesis seen at 24 h. In themouse, these events are frame-shifted later by 6–12 h(Michalopoulos and DeFrances, 1997). Throughout the first 2–3 days of regeneration, there is decrease in the ratio of C/EBPatoC/EBPb, a process thought as underlying some of the shifts inmetabolism that occur in liver during this time, such asenhanced lipid synthesis (Friedman et al., 2004). Analysis of thegene expression networks operating during liver regenerationhas revealed alterations dependent on both growth factors andcytokines (Taub et al., 1999; White et al., 2005).
The events occurring in the early period of 0–5 h after PHxhave often been called ‘‘priming’’ (Fausto, 2000). The term is auseful one, in that it denotes not only events associated forpreparation for entry into the cell cycle, but also events andstrategies of hepatocytes aimed at modifying patterns of geneexpression so that they continue to deliver their homeostaticfunctions. ‘‘Priming,’’ however, has also been used to denote atime in which events occurring are induced only by cytokines,with events induced by growth factors occurring after thecytokine-mediated events. The findings described above,however, clearly denote that there is no demarcation point thatcan be ascribed to separate events induced only by cytokines oronly by growth factors. The time kinetics in changes and effectsof both cytokines and growth factors (see below) areintertwined and synchronous, for example, activationof growthfactor receptors (Met and EGFR) occurs fully within 30 minafter PHx, similar to activation of Stat3 and NFkB. A partial listof the concurrent events occurring in the first 60 min after PHxis shown in Table 1.
Mitogenic Signals Associated With Initiationof Liver Regeneration
A key endpoint of liver regeneration is the restoration of thetotal number and mass of hepatocytes, the main functional cellsof the liver responsible for delivering most of the hepaticfunctions important for body homeostasis. Hepatocytes are thefirst cells of the liver to enter into the cell cycle and undergoproliferation, and they produce mitogenic signals for otherhepatic cell types (Fig. 2). Quiescent hepatocytes in normal liverexpress a variety of growth factor receptors. These includereceptors for PDGF, VEGF, fibroblast growth factor receptors,c-Kit, Studies with hepatocytes in primary culture howeverhave shown that despite the expression of many mitogenicreceptors, the only mitogens for hepatocytes in chemicallydefined serum-free media are HGF and ligands of the EGFR(EGF, TGFa, Amphiregulin, HB-EGF, etc). These ligands are directmitogens, in that they induce a strong mitogenic response in
hepatocytes in primary culture and clonal expansion of theirpopulation (Block et al., 1996). FGF1 and FGF2 are also weakmitogens (Houck et al., 1990). HGF, EGF, and TGFa also inducehepatocyte proliferation and liver enlargement when injectedalone into intact normalmice and rats (Bucher et al., 1977; Patijnet al., 1998). In addition to these proteins, however, there areother substances which, although not directly mitogenic tohepatocytes, enhance the effect of the direct mitogens. Theseinclude TNF (Webber et al., 1998),Norepinephrine (Cruise et al.,1985), and estrogens (Ni and Yager, 1994). Several studies haveemphasized the role of these substances and the kinetics oftheir expression during liver regeneration. Recent studies havealso focused on pro-regenerative effects of components ofcomplement, bile acids, and serotonin, substances not known ortested to have direct or indirect mitogenic effects. Some of theabove signaling molecules were implicated based on decreasedregeneration when their signaling is eliminated (e.g., HGF, TNF,IL6, bile acids, norepinephrine, serotonin). Others have beenimplicated because they are mitogenic for hepatocytes in cellculture or in vivo and their signaling receptors appear activatedduring liver regeneration (e.g., HGF and EGF). We will brieflydescribe below themain line of evidence associating each of theabove signaling molecules in liver regeneration. In general,however, there are two important considerations:
1. With the possible exception of the HGF/Met signalingpathway (see below), all other signaling pathways maytemporarily dampen but do not stop liver regeneration. Otherthan xenobiotics such as AAF, there is no known signal whoseabsence or presence permanently arrests liver regeneration.Even with high doses of radiation to the liver, regenerationoccurs (primarily by increase in the size of hepatocytes(Michalopoulos and DeFrances, 1997).
2. The fact that complete elimination of a signaling pathway doesnot entirely abrogate liver regeneration should not imply that thespecific signaling pathway is not important. The precise or-chestration of events occurring early after partial hepa-tectomy probably requires simultaneous presence of all thehitherto discovered extracellular signals. (Precise timing ofevents is important not only in experimental conditions butalso in clinical settings, in which rapid regeneration of theliver makes a ‘‘life or death’’ difference to the organism).
With these two principles in mind, the main signalingpathways known today and implicated for initiation andmaintenance of liver regeneration are as follows:
Hepatocyte growth factor (HGF)
It is present in liver matrix in relatively large quantities; it is alsofound in the matrix of other organs, such as lungs, spleen,placenta, brain, etc. (Matsumoto and Nakamura, 1996; Stellaand Comoglio, 1999). Systemically injected HGF is sequesteredby the liver more than any other organ (Appasamy et al., 1993).Its receptor, cMet, is expressed in most epithelial cells,endothelial cells and neurons, and mediates all the effects ofHGF (Naldini et al., 1991). In addition to its mitogenic andmotogenic effects, Met also binds the apoptotic receptor Fasand preventing its trimerization, thus having an anti-apoptoticeffect (Wang et al., 2002). Genetic elimination of HGF or itsreceptor (cMet) is associated with embryonic lethality involvingabnormalities in many organs, most notably in placenta(Schmidt et al., 1995; Dietrich et al., 1999; Uehara et al., 2000).Livers of the embryos are smaller than the wild type controls.HGF was isolated from the plasma of partially hepatectomizedrats, from studies in search for circulatingmitogens increasing inthe blood after PHx (Michalopoulos et al., 1984). HGF has beenimplicated as involved in liver regeneration for the followingreasons:
TABLE 1. Chronology of concurrent early (first 1 h) signaling events after
PHx
Multiple signaling pathways involving both growth factors, cytokines, paracrinesignals, and neuroendocrine factors occur simultaneously within the first60 min after PHx. These include:� Increase in urokinase activity (first 5 min)� Translocation of N(otch) ICD to the nucleus (15 min)� Translocation of beta-catenin to the nucleus (5–10 min to 6 h)� Decrease in HGF biomatrix stores (30 min to 3 h)� Activation of the HGF receptor (within 30–60 min)� Activation of the EGF receptor (within 30–60 min)� Increase of HGF, Norepinephrine, IL6, TNFa, TGFb1 and hyaluronic acid
in the plasma (1–2 h)� Activation of AP1, NFkB, and STAT3 (30–60 min)� Extensive gene expression reprogramming of hepatocytes within 30 min
after PHx
JOURNAL OF CELLULAR PHYSIOLOGY DOI 10.1002/JCP
L I V E R R E G E N E R A T I O N 289
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
a. HGF levels in plasma increase 10- to 20-fold after PHx(Lindroos et al., 1991).
b. Active HGF is consumed from intrahepatic stores in thefirst 3 h after PHx, followed by newHGF synthesis from 3 to48 h (Pediaditakis et al., 2001).
c. HGF causes a strong mitogenic response and clonal ex-pansion of hepatocytes in culture (Block et al., 1996).
d. HGF injection in portal vein of normal rats and mice causesproliferation of hepatocytes and enlargement of the liver(Liu et al., 1994a; Patijn et al., 1998).
e. Liver HGF receptor (cMet) becomes activated by tyrosinephosphorylation at 30–60 min after PHx (Stolz et al., 1999).
f. Activation of Met in hepatocyte cultures drives activation ofbeta catenin by its phosphorylation on tyrosine residues andpromotes its translocation to hepatocyte nucleus (Mongaet al., 2002).
g. Targeted genetic elimination of cMet from the liver isassociated with very diminished or absent regenerativeresponse (Borowiak et al., 2004; Huh et al., 2004).
h. RNA interference after PHx in vivo against cMet isassociated with complete blockade of the cell cycle. Thiseffect lasts as long as the RNA interference against Metis active (Paranjpe et al., 2007). The degree of suppressionof regeneration in (f) and (g) above suggests that there areunique signaling pathways associated with Met that are notcompensated by EGFR or other mechanisms. It should benoted that the same dependence on c-Met has also beenfound in wound healing (Chmielowiec et al., 2007).
i. Urokinase is involved in activation of HGF in regeneratingliver and mice genetically deficient in urokinase havedefective liver regeneration (Roselli et al., 1998). It shouldbe noted that HGF can also be activated by a protease withconsiderable homology to factor X, known as HGF acti-vator and subject to complex regulation by anti-proteases(Shimomura et al., 1999). This protein is soluble in theplasma and there has been no role identified for it duringliver regeneration.
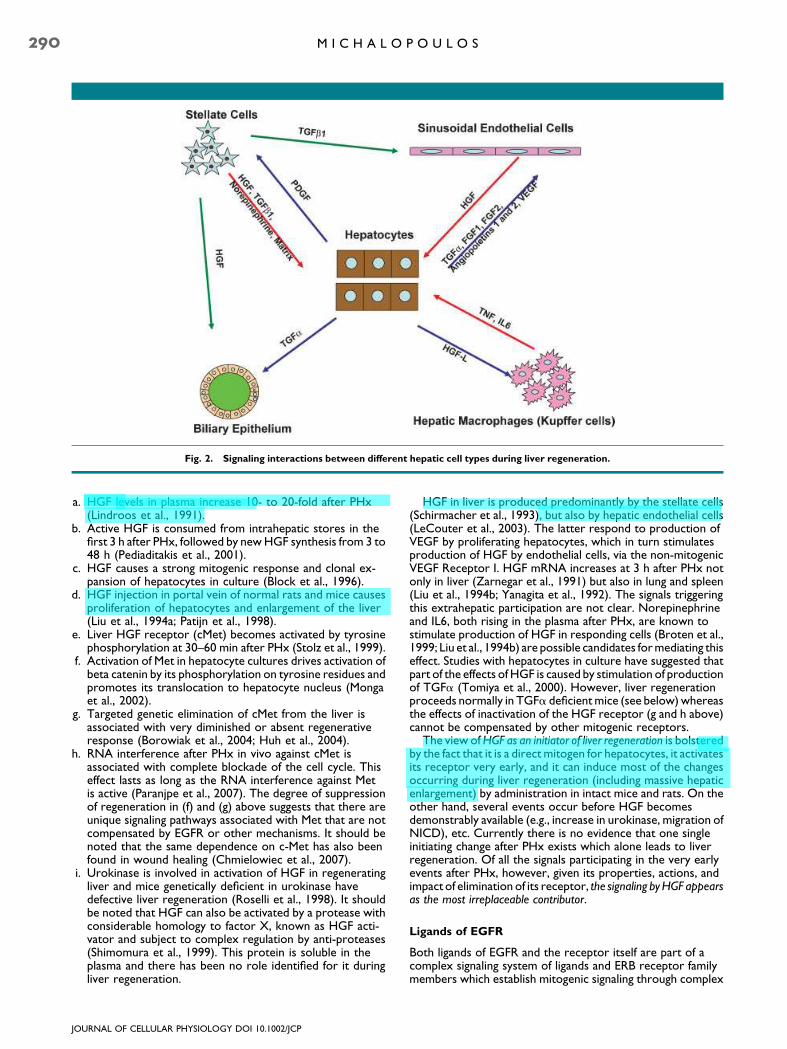
HGF in liver is produced predominantly by the stellate cells(Schirmacher et al., 1993), but also by hepatic endothelial cells(LeCouter et al., 2003). The latter respond to production ofVEGF by proliferating hepatocytes, which in turn stimulatesproduction of HGF by endothelial cells, via the non-mitogenicVEGF Receptor I. HGF mRNA increases at 3 h after PHx notonly in liver (Zarnegar et al., 1991) but also in lung and spleen(Liu et al., 1994b; Yanagita et al., 1992). The signals triggeringthis extrahepatic participation are not clear. Norepinephrineand IL6, both rising in the plasma after PHx, are known tostimulate production of HGF in responding cells (Broten et al.,1999; Liu et al., 1994b) are possible candidates formediating thiseffect. Studies with hepatocytes in culture have suggested thatpart of the effects ofHGF is caused by stimulation of productionof TGFa (Tomiya et al., 2000). However, liver regenerationproceeds normally in TGFa deficientmice (see below)whereasthe effects of inactivation of the HGF receptor (g and h above)cannot be compensated by other mitogenic receptors.
The view ofHGF as an initiator of liver regeneration is bolsteredby the fact that it is a direct mitogen for hepatocytes, it activatesits receptor very early, and it can induce most of the changesoccurring during liver regeneration (including massive hepaticenlargement) by administration in intact mice and rats. On theother hand, several events occur before HGF becomesdemonstrably available (e.g., increase in urokinase, migration ofNICD), etc. Currently there is no evidence that one singleinitiating change after PHx exists which alone leads to liverregeneration. Of all the signals participating in the very earlyevents after PHx, however, given its properties, actions, andimpact of elimination of its receptor, the signaling byHGF appearsas the most irreplaceable contributor.
Ligands of EGFR
Both ligands of EGFR and the receptor itself are part of acomplex signaling system of ligands and ERB receptor familymembers which establish mitogenic signaling through complex
Fig. 2. Signaling interactions between different hepatic cell types during liver regeneration.
JOURNAL OF CELLULAR PHYSIOLOGY DOI 10.1002/JCP
290 M I C H A L O P O U L O S
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight

interactions involving receptor ligation, endocytosis, potentialrecycling to the plasma membrane, etc. This was discussed inthe context of liver regeneration in a recent review(Michalopoulos and Khan, 2005c). Though there is high level ofredundancy between receptors and ligands, the redundancy ofthis system is not complete. TGFa deficient mice apparentlyhave normal liver regeneration (Russell et al., 1996), whereasmice deficient in Amphiregulin or HB EGF are reported to havedeficient regeneration.
a. EGF is continually available to the liver through the portalvein, produced from Brunner’s glands of the duodenum and,in male mice, from circulating high levels of EGF producedby the salivary glands (Skov Olsen et al., 1988; Jones et al.,1995). Catecholamines, including epinephrine and norepi-nephrine, are known to stimulate production of EGF fromBrunner’s glands of the duodenum (Olsen et al., 1985) andthey rise in plasma after PHx. However, there has not beenany direct measurement of portal vein concentration ofEGF after PHx. All tested EGFR ligands are direct and strongmitogens for hepatocytes in culture. EGF given in intactanimals causes hepatocyte proliferation (Bucher et al.,1977). EGFR is phosphorylated within 30–60 min after PHx.The capacity of liver to regenerate following suppression ortargeted elimination of EGFR has not been tested as yet.
b. TGFa is produced by hepatocytes during regeneration,starting at about 2–3 h after PHx and continuing at highlevels for more than 48 h (Mead and Fausto, 1989). TGFa isproduced as an inactive precursor penetrating through theplasma membrane. The extracellular domain is cleaved byproteases such as TACE (Lee et al., 2003), to generate theactive form. Since hepatocytes express EGFR, the possibilitythat TGFa production generates an autocrine loop hasbeen considered. Mice with targeted transgenic expressionof TGFa in hepatocytes have dramatic liver enlargementand develop tumors (Webber et al., 1994). On the otherhand, genetic elimination of TGFa does not affect liverregeneration and despite the large increase in TGFamRNA, the actual measured increase in protein is rathersmall (Russell et al., 1993, 1996). TGFa is also a mitogen forendothelial cells and bile duct epithelial cells. It is possiblethat TGFa production by hepatocytes triggers paracrineeffects stimulated by hepatocytes and aimed to engageadjacent hepatic cells into proliferation. This is comparableto observed increases in TGFa in other normal cells inproliferation or tissue repair (e.g., keratinocytes duringwound healing, mammary epithelial cells followingstimulation by estrogens, and most carcinomas are knownto produce high levels of TGFa (Aaronson et al., 1990;Derynck, 1992; Purup et al., 2000).
c. Heparin Binding EGF (HB EGF) is produced by endothelialcells and Kupffer cells (Kiso et al., 1995). HB EGF pro-duction increases within 1.5 h after PHx. HB EGF transgenicmice with liver-targeted production have enhanced re-generation (Kiso et al., 2003) whereas HB EGF knockoutmice have deficient regenerative response (Mitchell et al.,2005).
d. Amphiregulin is another member of the family of EGFRligands. Mice deficient in Amphiregulin have deficient liverregeneration (Berasain et al., 2005).
Tumor necrosis factor (TNF)
This is a protein known to have a variety of effects onmany cellsand tissues. Contrary to what its name implies, TNF can oftenhave promitogenic effects on cells, depending on conditionswhich regulate activation of NFkB (Kirillova et al., 1999). Ifconditions favor activation of NFkB, then TNF may enhanceother concurrently delivered growth signals. Alternatively, if
activation of NFkB cannot be mediated by TNF, then TNF mayelicit an apoptotic response (Iimuro et al., 1998). The status offree radicals (Pierce et al., 2000), energy levels and otherintracellular factors determine the emergence of complexpathway involving activation of NFkB by removal of theinhibitory IkB through phosphorylation mediated by the kinaseIKK (Karin et al., 2004; Luo et al., 2005; Park et al., 2005).Oneofthe factors determining the activation ofNFkB and theoutcomeof interaction of TNF with cells is altered integrin signaling.With all the matrix remodeling occurring during regeneration,such alterations in integrin signaling are bound to occur andthey may be associated with directing the signaling of TNFtowards a promitogenic effect (Chen et al., 2007). Antibodiesagainst TNF administered at the time of hepatectomy decreasethe regenerative response (Akerman et al., 1992). Mice withgenetic deletions of theTNF receptor 1 (TNFR1) have slow anddeficient response following PHx (Yamada et al., 1997, 1998;Yamada and Fausto, 1998). Activation of Stat3 and NFkB inthese mice is diminished. Liver regeneration eventuallybecomes completed albeit much later. Even though deletion ofNFkB components does not seem to affect liver regeneration(DeAngelis et al., 2001), given the promitogenic effects ofactivated NFkB in many cells and tissues, it is likely that TNFexercises its effects on liver regeneration in major part by thispathway. TNF is involved in induction of TACE, a plasmamembrane associated protease which controls activation ofTGFa. Enhanced activation of TGFa causes transactivation ofEGFR (Argast et al., 2004). TNF is also a regulator of iNOS(Nussler et al., 1995), and mice with deficiency in iNOS havedefective liver regeneration (Rai et al., 1998).
TNF is not a direct mitogen for hepatocytes. It does notinduce DNA synthesis in primary cultures of hepatocytes inserum freemedia nor does it induce hepatocyteDNA synthesiswhen injected in whole animals. It does, however, enhance themitogenic effects of direct mitogens such as HGF, both in vivoand in cell culture (Webber et al., 1998) and is mitogenic forhepatocytes with transgenic expression of TGFa (Pierce et al.,2000). TNF increases in plasma after PHx. Its cellular source isconsidered to be the hepatic macrophages (Kupffer cells) butproduction by other cell types has not been excluded. Astimulus thatmay induceTNF after PHx is endotoxin, producedby bacteria from the gut. Given the absence of direct mitogeniceffects on hepatocytes, TNF should not be viewed as theinitiator of liver regeneration, but rather as one of the manyconcurrent and contributory extracellular signals that alltogether orchestrate the early events of the response.
Interleukin 6 (IL6)
There is abundant literature documenting the crucial role ofIL6 in initiation of the acute phase response in hepatocytes. Thisis a rapid increase in production by hepatocytes of manyproteins which assist in controlling acute or chronicinflammation (Fey et al., 1991; Geisterfer et al., 1993). IL6 isproduced by hepatic macrophages. Previous studies howeverhave shown that it is produced by hepatoma cell lines,suggesting that it may also be produced by hepatocytesthemselves (Northemann et al., 1990). IL6 binds to a solublereceptor, and the complex binds to the receptor gp130, whichIL6 shareswith other cytokines, includingOncostatinM,CNTF,LIF, etc. (Benigni et al., 1996). There was a previous reportclaiming that mice deficient in IL6 have deficient liverregeneration. This was associated with deficient activation ofStat3 (Cressman et al., 1996). Other studies however haveshown that liver regeneration in thesemice is essentially normaleven though there is decreased activation of Stat3 (Sakamotoet al., 1999). Mice over-expressing both IL6 and its solublereceptor have areas of periportal hepatocyte hyperplasia(Maione et al., 1998). Mice with genetic deletions of gp130 are
JOURNAL OF CELLULAR PHYSIOLOGY DOI 10.1002/JCP
L I V E R R E G E N E R A T I O N 291
userr
Highlight
userr
Highlight
userr
Highlight
Z
Squiggly
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight

more sensitive to toxic effects but have essentially normal liverregeneration (Streetz et al., 2003). IL6 is not a direct mitogenfor hepatocytes and does not enhance the mitogenic effect ofother growth factors. It is, however, a direct mitogen for biliarycells (Liu et al., 1998) and it has important effects on integrity ofthe intrahepatic biliary tree by regulating production of smallproline-rich proteins by cholangiocytes (Nozaki et al., 2005;Demetris et al., 2006). IL6 does increase in plasma followingPHx. IL6 is probably a factor contributing to optimizingprocesses of the early stage of liver regeneration, but it shouldnot be viewed as the initiator of the process.
Norepinephrine
This is a neurotransmitter in the central and peripheralautonomic nervous system. Epinephrine and norepinephrineare released in peripheral circulation from nerve endings, aswell as from the adrenal medulla. Interest in the role ofnorepinephrine in liver regeneration arose when it was shownthat norepinephrine substantially enhances the mitogeniceffects of EGF and HGF in hepatocyte cultures and it decreasesthemito-inhibitory effects of TGFb1 (Cruise et al., 1985; Houcket al., 1988). In cultures of hepatocytes with balancedconcentrations of EGF and TGFb1 such that the final effect isneutral (EGFmitogenic effect is balanced by themito-inhibitoryeffect of TGFb1), addition of norepinephrine triggers high-levelhepatocyte DNA synthesis (Houck and Michalopoulos, 1989).Norepinephrine induces synthesis of HGF in myofibroblasts(Broten et al., 1999). It is produced by and required for DNAsynthesis of stellate cells in vivo and in culture (Oben et al.,2003). Another effect of norepinephrine and epinephrine ofpotential importance to liver regeneration is enhancement ofproduction of EGF by Brunner’s glands of the duodenum (Olsenet al., 1985). This has not been directly linked to liverregeneration but norepinephrine rises rapidly in plasma afterPHx and it may have an effect on EGF production. Blockade ofthe alpha-1 adrenergic receptor by prazosin inhibits DNAsynthesis after PHx for 72 h (Cruise et al., 1987). It is not clearwhether this effect reflects blockade of norepinephrinesecreted peripherally or locally released by the stellate cells.
Bile acids and xenobiotics
It has been a long standing observation from liver pathology thathepatic cholestasis (chemically induced or due to mechanicalbiliary obstruction) is associated with proliferation ofhepatocytes. A recent study provided evidence that bile acidsincrease in circulating blood after PHx and that depletion of bileacids leads to decreased regeneration (Huang et al., 2006). Theelevation of bile acids in plasma occurs several hours after PHx,thus it is unlikely that they contribute to the immediate earlychanges after PHx described above. Nonetheless, the finding isvery interesting. In the same study, mice with genetic deficiencyof FXR, a transcription factor mediating nuclear events inducedby bile acids, also have defective regeneration. There are severalexamples of xenobiotics ligating specific transcription factors ornuclear hormone receptors in hepatocytes and inducing liverenlargement. These include triiodothyronine (T3) (Short et al.,1980; Ledda-Columbano et al., 2000), agonists of PPARa(Reddy and Chu, 1996), estrogens (Yager et al., 1994),barbiturates (acting on CAR and PXR) (Columbano et al.,2005), and others. Hepatic enlargement is mediated in part byhepatocyte proliferation and in part by hepatocyte enlargement.The signaling pathways by which these chemicals exert theseeffects, are not clear. These pathways have not been shown sofar to be associated with signaling patterns seen during liverregeneration (Columbano and Shinozuka, 1996; Columbanoet al., 1997; Menegazzi et al., 1997; Ledda-Columbano et al.,2002). FXR is the first nuclear hormone receptor to beassociated with proliferative events leading to regeneration of
the liver and it sets a paradigm for discovery of other suchnuclear hormone receptors as potentially having similar effects.
Serotonin
Mice with decreased platelet numbers have attenuated liverregeneration. Platelets contain many bioactive substances,including HGF, TGFb1 and serotonin. A recent study (Lesurtelet al., 2006) demonstrated that supplementation ofthrombocytopenic mice with serotonin reversed many of theeffects of platelet depletion. Mice with low levels of serotonin(deficient in tryptophan hydroxylase 1) have low levels ofplatelet serotonin and they also have deficient regeneration.The mechanisms by which serotonin exerts these effects arenot clear. Serotonin is not a direct or indirect mitogen forhepatocytes in culture, thus its effects on this process are likelyto be indirect. It may affect the concentration and/or release ofother platelet components (HGF, TGFb1) known to have aneffect on regeneration. It effects on hepatocytes in culture needto be investigated, as with norepinephrine, in order to sort outthe mechanism of its action.
Components of complement
Mice deficient in components of complement C3 and C5 havedefective regenerative responses to both PHx and to recoveryfrom centrilobular necrosis following injury with CCl4.Administration of the missing components restores theefficiency of the regenerative response (Strey et al., 2003;DeAngelis et al., 2006; Tsonis et al., 2006). The mechanism forthis is not clear and the phenomenon warrants detailmechanistic investigation.
Leptin, steatosis, and liver regeneration
There is emerging literature to suggest that excessiveaccumulation of fat in hepatocytes interferes with liverregeneration (Torbenson et al., 2002; Diehl, 2005). Leptindeficient db/db mice have excessive hepatic steatosis andimpaired liver regeneration (Yamauchi et al., 2003). Themechanisms are not clear. In a similar model (ob/ob mice),neither administration of leptin nor correction of steatosiscorrect the regeneration response (Leclercq et al., 2006).Further complicating the issue, regenerating liver hepatocytesnormally accumulate fat micro-droplets. This transient fattyliver occurs in the rat from 24 to 72 h after PHx and disappearsby itself (Michalopoulos and DeFrances, 1997). The process isthought to represent a metabolic adaptation of hepatocytes sothat the emerging new cells have readily available energy as wellas materials they can use to build cellular membranes etc.Recent studies have shown that this phenomenon is an essentialcomponent of the regenerative process and that interferencewith the accumulation of fat actually blocks liver regeneration(Shteyer et al., 2004). This physiologic accumulation of fatmicro-droplets is dependent on caveolin, and caveolin-knockout mice have defective liver regeneration (Fernandezet al., 2006).
Notch and jagged
There are several members to this family of proteins and theycompose a complex network mediating ligand–receptorinteractions between cells, in tissues undergoing differentiationand proliferation related changes (Mumm and Kopan, 2000;Baron et al., 2002; Baron, 2003).Notch proteins are consideredto be the receptors, but both Notch and Jagged protein familymembers are anchored on the plasma membrane with atransmembrane domain. Binding of Jagged to Notch leads to acomplex cascade of proteolytic events whereby theintracellular domain of Notch (NICD) is cleaved andmigrates to the nucleus, where it functions as a transcriptionfactor (co-activator) and mediates expression of several genes
JOURNAL OF CELLULAR PHYSIOLOGY DOI 10.1002/JCP
292 M I C H A L O P O U L O S
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight

animal) or vice versa would tend to initiate (or eliminate) someof the stimuli of the regenerative process, albeit at a smallerscale. As an example, small grafts for the size of the recipient areassociated with increased plasma levels of both HGF andTGFb1 in the human, as with response to PHx in the rat(Ninomiya et al., 2003).
The liver weight changes associated with physiologic events(e.g., hepatic enlargement during pregnancy) are likely to bemediated not through the classic pathways associated withregeneration, but through hepatic enlargement mediated bynuclear hormone receptors. Estrogens (acting through the ERreceptors) have such an effect. Of interest, estradiol alsoenhances effects of mitogens and suppresses effects of TGFb1in hepatocytes cultures, similar to norepinephrine (see above).Many xenobiotics cause liver enlargement. The pathwaysleading to this are not fully understood and it seems thattranscription factors such as PPAR (for peroxisomeproliferators) and CAR may play a role (Ueda et al., 2002).Some of the liver enlargement is caused by direct effects on thesize of hepatocytes. Phenobarbital, associated with adramatic enlargement of liver in humans and rodents, causesprimarily hepatocyte hypertrophy. This is probably due toinduction and enhanced nuclear translocation of HNF4 byphenobarbital (Bell and Michalopoulos, 2006). This effect isindependent of CAR or PXR. Removal of the xenobioticcausing liver enlargement is always associated with a return tothe original liver size, mediated by a wave of hepatocyteapoptosis until liver weight returns to normal (Reddy et al.,1978). Extracellular matrix signaling may be involved. Acuteremoval of ILK and matrix signaling from hepatocytes causesmassive hepatic apoptosis (Gkretsi et al., 2007b). Thisprocess of liver weight adjustment by apoptosis is very littleunderstood.
If Hepatocytes Cannot Proliferate, What Are theRegenerative Alternatives?
Hepatocyte proliferation may be blocked if the tissue injury istoo severe, as in humans with fulminant hepatitis.Experimentally, hepatocyte proliferation is blocked by the useof the chemical AAF (N-acetylaminofluorene). On long-termadministration, AAF is a carcinogenic substance. Given for ashort period of time, it blocks hepatocyte proliferation,probably by forming AAF-DNA adducts which triggerproliferative arrest via p53 and p21 (Ohlson et al., 1998).WhenPHx is performed in animals given AAF, hepatocytes cannotproliferate. Starting at day 2–3 after PHx, biliary epithelial cellsof the portal ductules and canals of Herring (small tubules linedby epithelium with biliary morphology, which connect thenetwork of hepatocyte bile canaliculi to the portal biliaryductules) begin expressing hepatocyte-associated transcriptionfactors (Nagy et al., 1994). Shortly thereafter, there is anincreasing number of cells with mixed biliary and hepatocyticgene expression patterns, as well as somemarkers of their own(Sell, 1994). These cells have been called ‘‘oval’’ cells, from theshape of their nucleus. Oval cells proliferate intensely in theperiportal areas of the hepatic lobule and they are heavilyinfiltrated by stellate cells; the latter intertwine with the ovalcells and produce HGF, FGF1, FGF2, and VEGF (Evarts et al.,1993; Fujio et al., 1994). Other factors, such as somatostatin,stromal cell derived factor 1 (SDF1) and connective tissuegrowth factor also play a role (Pi et al., 2005; Jung et al., 2006;Zheng et al., 2006). Oval cells express both albumin and alphafetoprotein. Four to five days after their expansion as apopulation, they become basophilic hepatocytes and eventuallymature hepatocytes, and they restore liver size and histology(Evarts et al., 1989, 1996). The origin of the oval cells has been
Fig. 3. Schematic of a feedback loop between growth factors, TGFb1, and extracellular matrix, controlling early and late stages ofregeneration. Mitogens (HGF and EGF) upregulate expression of TGFb1 by stellate cells. The latter stimulates synthesis of new extracellularmatrix, while eventually blocking synthesis of new HGF and expression of urokinase. The newly synthesized extracellular matrix supportsbinding of single chain HGF and TGFb1 around hepatocytes and restoration of quiescence (G0 phase). Arrows of the same color denotesimilar origin of the input and output of the same signaling process.
JOURNAL OF CELLULAR PHYSIOLOGY DOI 10.1002/JCP
L I V E R R E G E N E R A T I O N 295
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight

much debated. A strong argument for their origin from biliarycells is their early gene expression patterns which stronglyresemble biliary cells, and the fact that biliary cells beginexpressing hepatocyte-associated transcription factors beforeoval cells appear. Additionally, when DAPM (a toxin whichselectively destroys biliary cells), is given before the initiation ofthe AAF/PHx protocol, it destroys the biliary epithelium andprevents the appearance of the oval cells (Petersen et al., 1997).There is no histologic observation demonstrating an oval cellpopulation in any non-biliary compartment in a normal liver.Cells equivalent to oval cells, called ‘‘ductular hepatocytes,’’ arealso seen in humans during fulminant hepatitis followingextensive liver injury (by chemicals, viruses, etc.) and they areassumed to pay a role similar to oval cells in restoringhepatocyte populations. It should be noted that pancreaticductules have also been viewed as the source of progenitor cellsfor both acinar cells and islet cells of the pancreas (Rao andReddy, 1995).
Hepatocytes and Biliary Epithelial Cells as FacultativeStem Cells for Each Other
As discussed above, biliary epithelial cells can become oval cellsand they in turn become hepatocytes, restoring liverregeneration when hepatocytes cannot proliferate. Thisimparts properties of facultative stem cells (Alison et al., 2001) tobiliary cells for hepatocytes. The term ‘‘facultative’’ implies thatbiliary cells under normal circumstances perform their normalfunctions (transport of bile). Under selective circumstances,however, they can become stem cells for hepatocytes. Clinicalhistologic observations have suggested that periportalhepatocytes may also be facultative stem cells for biliary cells,transforming into biliary cells when the latter cannot proliferateto repair biliary epithelium during chronic injury (e.g., primarybiliary cirrhosis, primary sclerosing cholangitis) (Crosby et al.,1998). This phenomenon has now been demonstratedexperimentally in rats with chimeric livers (Laconi et al., 1998).Periportal hepatocytes can transform into biliary epithelial cellswhen the latter are destroyed by DAPM and bile ducts are
simultaneously obstructed. Biliary obstruction is known to leadto bile ductule proliferation and, under the conditionsdescribed above, more than 50% of the newly emergingductules carry markers unique to one of the two populations ofthe hepatocytes of the chimeric liver (Michalopoulos et al.,2005a). These findings clearly demonstrate that hepatocytesare also facultative stem cells for the biliary epithelium. Asshown in Figure 4, the two types of epithelial cells of the liver(hepatocytes and biliary cells) constitute a bipolar system offacultative stem cells for each other, fully capable of repairingliver histology even when the classic regeneration fails.
Stems Cells in the Liver: Do They Exist? Are TheyNeeded? Where do They Come From?
The findings for hepatocytes and biliary cells discussed aboveraise questions about the very existence of full-time,committed, stem cells in the liver. Such cells exist in theepidermis (basal layer), intestine (cells of the crypts), and bonemarrow (hematopoietic stem cells, isolated and demonstrableby cell sorting). In these other tissues, the stem cells of thetissue exist on a full-time basis, they can be seen by casualexamination of the histology of the tissue and they arecommitted to ‘‘stemness’’ as their single function. Liverhistology does not contain any cells that appear to be full-time,committed, stem cells. The term ‘‘progenitor cells’’ has oftenbeing used for oval cells, and it is a useful term as long as it isremembered that these cells normally do not exist. It is quitepossible that there are subpopulations of both hepatocytes(periportal cells?) and biliary cells (canals of Herring?) whichmay have a higher propensity to function as facultative stemcells compared to other cells of their kind. All these cells,however, function as hepatocytes and biliary epithelial cellsunder normal circumstances.
There also has been considerable discussion that bonemarrow derived hematopoietic stemcells can trans-differentiateinto hepatocytes or oval cells and rescue the liverwhen all othermeans of regeneration fail (Petersen et al., 1999). A dramaticdemonstration of this phenomenonwas the rescue ofmicewith
Fig. 4. Cells from the biliary compartment (portal ductules and canals of Herring) transform into oval cells and these become hepatocyteswhen proliferation of hepatocytes is inhibited during regeneration. Periportal hepatocytes can also convert to biliary cells when there isinjury to biliary cells but their capacity for self-repair is inhibited. Hepatocytes and biliary cells are facultative stem cells for each other.
JOURNAL OF CELLULAR PHYSIOLOGY DOI 10.1002/JCP
296 M I C H A L O P O U L O S
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight

Baron M, Aslam H, Flasza M, Fostier M, Higgs JE, Mazaleyrat SL, Wilkin MB. 2002. Multiplelevels of Notch signal regulation (review). Mol Membr Biol 19:27–38.
Battle MA, Konopka G, Parviz F, Gaggl AL, Yang C, Sladek FM, Duncan SA. 2006.Hepatocyte nuclear factor 4alpha orchestrates expression of cell adhesion proteinsduring the epithelial transformation of the developing liver. Proc Natl Acad Sci U S A103:8419–8424.
Bell AW, Michalopoulos GK. 2006. Phenobarbital regulates nuclear expression of HNF-4alpha in mouse and rat hepatocytes independent of CAR and PXR. Hepatology 44:186–194.
Benigni F, Fantuzzi G, Sacco S, Sironi M, Pozzi P, Dinarello CA, Sipe JD, Poli V, Cappelletti M,Paonessa G, Pennica D, Panayotatos N, Ghezzi P. 1996. Six different cytokines that shareGP130 as a receptor subunit, induce serum amyloid A and potentiate the induction ofinterleukin-6 and the activation of the hypothalamus-pituitary-adrenal axis by interleukin-1. Blood 87:1851–1854.
Berasain C, Garcia-Trevijano ER, Castillo J, Erroba E, Lee DC, Prieto J, Avila MA. 2005.Amphiregulin: An early trigger of liver regeneration in mice. [See comment].Gastroenterology 128:424–432.
Block GD, Locker J, Bowen WC, Petersen BE, Katyal S, Strom SC, Riley T, Howard TA,Michalopoulos GK. 1996. Population expansion, clonal growth, and specific differentiationpatterns in primary cultures of hepatocytes induced by HGF/SF, EGF and TGF alpha in achemically defined (HGM) medium. J Cell Biol 132:1133–1149.
Borowiak M, Garratt AN, Wustefeld T, Strehle M, Trautwein C, Birchmeier C. 2004. Metprovides essential signals for liver regeneration. Proc Natl Acad Sci U S A 101:10608–10613.
Broten J, Michalopoulos G, Petersen B, Cruise J. 1999. Adrenergic stimulation of hepatocytegrowth factor expression. Biochem Biophys Res Commun 262:76–79.
Bucher NL. 1976. Insulin, glucagon, and the liver. Adv Enzyme Regul 15:221–230.Bucher NL, Patel U, Cohen S. 1977. Hormonal factors concerned with liver regeneration.Ciba Found Symp 55:95–107.
Bucher NL, Weir GC. 1976. Insulin, glucagon, liver regeneration, and DNA synthesis.Metabolism 25:1423–1425.
Cassiman D, Denef C, Desmet VJ, Roskams T. 2001. Human and rat hepatic stellate cellsexpress neurotrophins and neurotrophin receptors. Hepatology 33:148–158.
Chari RS, Price DT, Sue SR, Meyers WC, Jirtle RL. 1995. Down-regulation of transforminggrowth factor beta receptor type I, II, and III during liver regeneration. Am J Surg 169:126–131; discussion 126–131.
Chen CC, Young JL, Monzon RI, Chen N, Todorovic V, Lau LF. 2007. Cytotoxicity ofTNFalpha is regulated by integrin-mediated matrix signaling. EMBO J 26:1257–1267.
Chmielowiec J, Borowiak M, Morkel M, Stradal T, Munz B,Werner S,Wehland J, BirchmeierC, BirchmeierW. 2007. c-Met is essential forwound healing in the skin. J Cell Biol 177:151–162.
Columbano A, Ledda-Columbano GM, Pibiri M, Cossu C, Menegazzi M, Moore DD, HuangW, Tian J, Locker J. 2005. Gadd45beta is induced through a CAR-dependent, TNF-independent pathway in murine liver hyperplasia. Hepatology 42:1118–1126.
Columbano A, Ledda-Columbano GM, Pibiri M, Piga R, Shinozuka H, De Luca V, Cerignoli F,Tripodi M. 1997. Increased expression of c-fos, c-jun and LRF-1 is not required for in vivopriming of hepatocytes by the mitogen TCPOBOP. Oncogene 14:857–863.
Columbano A, Shinozuka H. 1996. Liver regeneration versus direct hyperplasia. Faseb J10:1118–1128.
Cressman DE, Diamond RH, Taub R. 1995. Rapid activation of the Stat3 transcriptioncomplex in liver regeneration. Hepatology 21:1443–1449.
Cressman DE, Greenbaum LE, DeAngelis RA, Ciliberto G, Furth EE, Poli V, Taub R. 1996.Liver failure and defective hepatocyte regeneration in interleukin-6- deficientmice. Science274:1379–1383.
Croquelois A, Blindenbacher A, Terracciano L,Wang X, Langer I, Radtke F, HeimMH. 2005.Inducible inactivation of Notch1 causes nodular regenerative hyperplasia in mice. [Seecomment]. Hepatology 41:487–496.
CrosbyHA,Hubscher S, Fabris L, Joplin R, Sell S, Kelly D, Strain AJ. 1998. Immunolocalizationof putative human liver progenitor cells in livers from patients with end-stage primarybiliary cirrhosis and sclerosing cholangitis using the monoclonal antibody OV-6. Am JPathol 152:771–779.
Cruise JL, Houck KA, Michalopoulos GK. 1985. Induction of DNA synthesis in cultured rathepatocytes through stimulation of alpha 1 adrenoreceptor by norepinephrine. Science227:749–751.
Cruise JL, Knechtle SJ, Bollinger RR, Kuhn C, Michalopoulos G. 1987. Alpha 1-adrenergiceffects and liver regeneration. Hepatology 7:1189–1194.
DeAngelis RA, Kovalovich K, CressmanDE, Taub R. 2001. Normal liver regeneration in p50/nuclear factor kappaB1 knockout mice. Hepatology 33:915–924.
DeAngelis RA, Markiewski MM, Lambris JD. 2006. Liver regeneration: A link to inflammationthrough complement. Adv Exp Med Biol 586:17–34.
Demetris AJ, Lunz JG 3rd, Specht S, Nozaki I. 2006. Biliary wound healing, ductular reactions,and IL-6/gp130 signaling in the development of liver disease. World J Gastroenterol12:3512–3522.
Derynck R. 1992. The physiology of transforming growth factor-alpha. Adv Cancer Res58:27–52.
Diehl AM. 2005. Lessons from animal models of NASH. Hepatol Res 33:138–144.Dietrich S, Abou-Rebyeh F, Brohmann H, Bladt F, Sonnenberg-Riethmacher E, Yamaai T,Lumsden A, Brand-Saberi B, Birchmeier C. 1999. The role of SF/HGF and c-Met in thedevelopment of skeletal muscle. Development 126:1621–1629.
Evarts RP, Hu Z, Fujio K, Marsden ER, Thorgeirsson SS. 1993. Activation of hepatic stem cellcompartment in the rat: Role of transforming growth factor alpha, hepatocyte growthfactor, and acidic fibroblast growth factor in early proliferation. Cell Growth Differ 4:555–561.
Evarts RP, Hu Z, Omori N, Omori M, Marsden ER, Thorgeirsson SS. 1996. Precursor-product relationship between oval cells and hepatocytes: Comparison between tritiatedthymidine and bromodeoxyuridine as tracers. Carcinogenesis 17:2143–2151.
Evarts RP,NagyP,NakatsukasaH,MarsdenE, ThorgeirssonSS. 1989. In vivo differentiationofrat liver oval cells into hepatocytes. Cancer Res 49:1541–1547.
Evarts RP, Raab M, Marsden E, Thorgeirsson SS. 1986. Histochemical changes in livers fromportacaval-shunted rats. J Natl Cancer Inst 76:731–738.
Fausto N. 2000. Liver regeneration. J Hepatol 32:19–31.Fausto N. 2004. Liver regeneration and repair: Hepatocytes, progenitor cells, and stem cells.Hepatology 39:1477–1487.
Fausto N, Campbell JS, Riehle KJ. 2006. Liver regeneration. Hepatology 43:S45–53.Fernandez MA, Albor C, Ingelmo-Torres M, Nixon SJ, Ferguson C, Kurzchalia T, Tebar F,Enrich C, Parton RG, Pol A. 2006. Caveolin-1 is essential for liver regeneration. Science313:1628–1632.
Fey GH, Hattori M, Hocke G, Brechner T, Baffet G, Baumann M, Baumann H, NorthemannW. 1991. Gene regulation by interleukin 6. Biochimie 73:47–50.
FitzGerald MJ, Webber EM, Donovan JR, Fausto N. 1995. Rapid DNA binding by nuclearfactor kappa B in hepatocytes at the start of liver regeneration. Cell Growth Differ 6:417–427.
Friedman JR, Larris B, Le PP, Peiris TH, Arsenlis A, Schug J, Tobias JW, Kaestner KH,Greenbaum LE. 2004. Orthogonal analysis of C/EBPbeta targets in vivo during liverproliferation. Proc Natl Acad Sci U S A 101:12986–12991.
Fujio K, Evarts RP, Hu Z, Marsden ER, Thorgeirsson SS. 1994. Expression of stem cell factorand its receptor, c-kit, during liver regeneration from putative stem cells in adult rat. LabInvest 70:511–516.
Gallai M, Sebestyen A, Nagy P, Kovalszky I, Onody T, Thorgeirsson SS. 1996. Proteoglycangene expression in rat liver after partial hepatectomy. Biochem Biophys Res Commun228:690–694.
Gebhardt R, Baldysiak-Figiel A, Krugel V, Ueberham E, Gaunitz F. 2007. Hepatocellularexpression of glutamine synthetase: An indicator of morphogen actions as masterregulators of zonation in adult liver. Prog Histochem Cytochem 41:201–266.
Geisterfer M, Richards C, Baumann M, Fey G, Gywnne D, Gauldie J. 1993. Regulation of IL-6and the hepatic IL-6 receptor in acute inflammation in vivo. Cytokine 5:1–7.
Gkretsi V, Bowen WC, Yang Y, Wu C, Michalopoulos GK. 2007a. Integrin-linked kinase isinvolved in matrix-induced hepatocyte differentiation. Biochem Biophys Res Commun353:638–643.
Gkretsi V, Mars WM, Bowen WC, Barua L, Yang Y, Guo L, St-Arnaud R, Dedhar S, Wu C,Michalopoulos GK. 2007b. Loss of integrin linked kinase from mouse hepatocytes in vitroand in vivo results in apoptosis and hepatitis. Hepatology 45:1025–1034.
Gohda E, Matsunaga T, Kataoka H, Yamamoto I. 1992. TGF-beta is a potent inhibitor ofhepatocyte growth factor secretion by human fibroblasts. Cell Biol Int Rep 16:917–926.
HaruyamaT, Ajioka I, AkaikeT,WatanabeY. 2000. Regulation and significanceof hepatocyte-derived matrix metalloproteinases in liver remodeling. Biochem Biophys Res Commun272:681–686.
Higgins GM, Anderson RM. 1931. Experimental pathology of the liver, 1:Restoration of theliver of the white rat following partial surgical removal. Arch Pathol 12:186–202.
Ho J, de Guise C, Kim C, Lemay S,Wang XF, Lebrun JJ. 2004. Activin induces hepatocyte cellgrowth arrest through induction of the cyclin-dependent kinase inhibitor p15INK4B andSp1. Cell Signal 16:693–701.
Holifield JS, Arlen AM, Runyan RB, Tomanek RJ. 2004. TGF-beta1, -beta2 and -beta3cooperate to facilitate tubulogenesis in the explanted quail heart. J Vasc Res 41:491–498.
Houck KA, Cruise JL, Michalopoulos G. 1988. Norepinephrine modulates the growth-inhibitory effect of transforming growth factor-beta in primary rat hepatocyte cultures.J Cell Physiol 135:551–555.
Houck KA, Michalopoulos GK. 1989. Altered responses of regenerating hepatocytes tonorepinephrine and transforming growth factor type beta. J Cell Physiol 141:503–509.
Houck KA, Zarnegar R, Muga SJ, Michalopoulos GK. 1990. Acidic fibroblast growth factor(HBGF-1) stimulates DNA synthesis in primary rat hepatocyte cultures. J Cell Physiol143:129–132.
HuangW,K.M, J. Z, M.Q, J. C, J. L, B. D, X.H,DD.M. 2006.Nuclear receptor-dependent bileacid signaling is required for normal liver regeneration. Science 312:233–236.
Huh CG, Factor VM, Sanchez A, Uchida K, Conner EA, Thorgeirsson SS. 2004. Hepatocytegrowth factor/c-met signaling pathway is required for efficient liver regeneration andrepair. Proc Natl Acad Sci U S A 101:4477–4482.
Ichikawa T, Zhang YQ, Kogure K, Hasegawa Y, Takagi H, Mori M, Kojima I. 2001.Transforming growth factor beta and activin tonically inhibit DNA synthesis in the rat liver.Hepatology 34:918–925.
Iimuro Y, Nishiura T, Hellerbrand C, Behrns KE, Schoonhoven R, Grisham JW, Brenner DA.1998. NFkappaB prevents apoptosis and liver dysfunction during liver regeneration[published erratum appears in J Clin Invest 1998Apr 1;101(7):1541]. J Clin Invest 101:802–811.
Ikeda H, Nagoshi S, Ohno A, Yanase M, Maekawa H, Fujiwara K. 1998. Activated rat stellatecells express c-met and respond to hepatocyte growth factor to enhance transforminggrowth factor beta1 expression and DNA synthesis. Biochem Biophys Res Commun250:769–775.
Jakowlew SB, Mead JE, Danielpour D, Wu J, Roberts AB, Fausto N. 1991. Transforminggrowth factor-beta (TGF-beta) isoforms in rat liver regeneration: Messenger RNAexpression and activation of latent TGF-beta. Cell Regul 2:535–548.
Jirtle RL, Carr BI, Scott CD. 1991. Modulation of insulin-like growth factor-II/mannose 6-phosphate receptors and transforming growth factor-beta 1 during liver regeneration[published erratum appears in J Biol Chem 1991 Dec 25;266(36):24860]. J Biol Chem266:22444–22450.
Jirtle RL, MichalopoulosG. 1982. Effects of partial hepatectomy on transplanted hepatocytes.Cancer Res 42:3000–3004.
Jo M, Stolz DB, Esplen JE, Dorko K, Michalopoulos GK, Strom SC. 2000. Cross-talk betweenepidermal growth factor receptor and c-Met signal pathways in transformed cells. J BiolChem 275:8806–8811.
Jones DE, Jr., Tran-Patterson R, Cui DM, Davin D, Estell KP, Miller DM. 1995. Epidermalgrowth factor secreted from the salivary gland is necessary for liver regeneration. Am JPhysiol 268:G872–878.
Jung Y, Oh SH, Zheng D, Shupe TD, Witek RP, Petersen BE. 2006. A potential role ofsomatostatin and its receptor SSTR4 in the migration of hepatic oval cells. Lab Invest86:477–489.
Karin M, Yamamoto Y, Wang QM. 2004. The IKK NF-kappa B system: A treasure trove fordrug development. Nat Rev Drug Discov 3:17–26.
Khan Z, Michalopoulos GK, Stolz DB. 2006. Peroxisomal localization of hypoxia-induciblefactors and hypoxia-inducible factor regulatory hydroxylases in primary rat hepatocytesexposed to hypoxia-reoxygenation. Am J Pathol 169:1251–1269.
Kim TH, Mars WM, Stolz DB, Michalopoulos GK. 2000. Expression and activation of pro-MMP-2 and pro-MMP-9 during rat liver regeneration. Hepatology 31:75–82.
Kim TH, Mars WM, Stolz DB, Petersen BE, Michalopoulos GK. 1997. Extracellularmatrix remodeling at the early stages of liver regeneration in the rat. Hepatology 26:896–904.
Kirillova I, Chaisson M, Fausto N. 1999. Tumor necrosis factor induces DNA replication inhepatic cells through nuclear factor kappaB activation. Cell Growth Differ 10:819–828.
Kiso S, Kawata S, Tamura S, Higashiyama S, Ito N, Tsushima H, Taniguchi N, Matsuzawa Y.1995. Role of heparin-binding epidermal growth factor-like growth factor as ahepatotrophic factor in rat liver regeneration after partial hepatectomy. Hepatology22:1584–1590.
Kiso S, Kawata S, Tamura S, Inui Y, Yoshida Y, Sawai Y, Umeki S, ItoN, YamadaA,Miyagawa J,Higashiyama S, Iwawaki T, Saito M, Taniguchi N, Matsuzawa Y, Kohno K. 2003. Liver
JOURNAL OF CELLULAR PHYSIOLOGY DOI 10.1002/JCP
298 M I C H A L O P O U L O S
userr
Highlight
regeneration in heparin-binding EGF-like growth factor transgenic mice after partialhepatectomy. Gastroenterology 124:701–707.
Kogure K, Zhang YQ, Maeshima A, Suzuki K, Kuwano H, Kojima I. 2000. The role of activinand transforming growth factor-beta in the regulation of organ mass in the rat liver.Hepatology 31:916–921.
Kohler C, Bell AW, BowenWC, Monga SP, FleigW, Michalopoulos GK. 2004. Expression ofNotch-1 and its ligand Jagged-1 in rat liver during liver regeneration. Hepatology 39:1056–1065.
Kortlever RM, Bernards R. 2006. Senescence, wound healing and cancer: The PAI-1connection. Cell cycle 5:2697–2703.
Laconi E, Oren R, Mukhopadhyay DK, Hurston E, Laconi S, Pani P, Dabeva MD, Shafritz DA.1998. Long-term, near-total liver replacement by transplantationof isolated hepatocytes inrats treated with retrorsine. Am J Pathol 153:319–329.
Lagasse E, Connors H, Al-DhalimyM, ReitsmaM, DohseM,Osborne L,Wang X, FinegoldM,Weissman IL, Grompe M. 2000. Purified hematopoietic stem cells can differentiate intohepatocytes in vivo. [See comment]. Nat Med 6:1229–1234.
LaMarre J, Hayes MA, Wollenberg GK, Hussaini I, Hall SW, Gonias SL. 1991. An alpha 2-macroglobulin receptor-dependent mechanism for the plasma clearance of transforminggrowth factor-beta 1 in mice. J Clin Invest 87:39–44.
Leclercq IA, Vansteenberghe M, Lebrun VB, VanHul NK, Abarca-Quinones J, Sempoux CL,Picard C, Starkel P, Horsmans YL. 2006. Defective hepatic regeneration after partialhepatectomy in leptin-deficient mice is not rescued by exogenous leptin. Lab Invest86:1161–1171.
LeCouter J, Moritz DR, Li B, Phillips GL, Liang XH, Gerber HP, Hillan KJ, Ferrara N. 2003.Angiogenesis-independent endothelial protection of liver: Role of VEGFR-1. Science299:890–893.
Ledda-Columbano GM, Perra A, Loi R, Shinozuka H, Columbano A. 2000. Cell proliferationinduced by triiodothyronine in rat liver is associated with nodule regression and reductionof hepatocellular carcinomas. Cancer Res 60:603–609.
Ledda-ColumbanoGM, Pibiri M, ConcasD, CossuC, TripodiM, ColumbanoA. 2002. Loss ofcyclin D1 does not inhibit the proliferative response of mouse liver to mitogenic stimuli.Hepatology 36:1098–1105.
Lee CS, Friedman JR, Fulmer JT, Kaestner KH. 2005. The initiation of liver development isdependent on Foxa transcription factors. Nature 435:944–947.
Lee DC, Sunnarborg SW, Hinkle CL, Myers TJ, Stevenson MY, Russell WE, Castner BJ,Gerhart MJ, Paxton RJ, Black RA, Chang A, Jackson LF. 2003. TACE/ADAM17 processingof EGFR ligands indicates a role as a physiological convertase. AnnNYAcad Sci 995:22–38.
Leong GF, Grisham JW, Hole BV, Albright ML. 1964. Effect of Partial Hepatectomy on DNASynthesis and Mitosis in Heterotopic Partial Autografts of Rat Liver. Cancer Res 24:1496–1501.
Lesurtel M, Graf R, Aleil B,Walther B, Tian Y, JochumW,Gaget C, Bader M, Clavien P. 2006.Platelet-derived serotonin mediates liver regeneration. Science 312:104–107.
Leu JI, Crissey MA, Craig LE, Taub R. 2003. Impaired hepatocyte DNA synthetic responseposthepatectomy in insulin-like growth factor binding protein 1-deficientmicewith defectsin C/EBP beta and mitogen-activated protein kinase/extracellular signal-regulated kinaseregulation. Mol Cell Biol 23:1251–1259.
Li W, Liang X, Kellendonk C, Poli V, Taub R. 2002. STAT3 contributes to the mitogenicresponse of hepatocytes during liver regeneration. J Biol Chem 277:28411–28417.
Lindroos PM, Zarnegar R, Michalopoulos GK. 1991. Hepatocyte growth factor(hepatopoietin A) rapidly increases in plasma beforeDNA synthesis and liver regenerationstimulated by partial hepatectomy and carbon tetrachloride administration. Hepatology13:743–750.
LiuML, MarsWM, Zarnegar R, MichalopoulosGK. 1994a. Collagenase pretreatment and themitogenic effects of hepatocyte growth factor and transforming growth factor-alpha inadult rat liver. Hepatology 19:1521–1527.
LiuY,MichalopoulosGK,ZarnegarR. 1994b. Structural and functional characterizationof themouse hepatocyte growth factor gene promoter. J Biol Chem 269:4152–4160.
Liu Z, Sakamoto T, Ezure T, Yokomuro S, Murase N, Michalopoulos G, Demetris AJ. 1998.Interleukin-6, hepatocyte growth factor, and their receptors in biliary epithelial cells duringa type I ductular reaction in mice: Interactions between the periductal inflammatory andstromal cells and the biliary epithelium. Hepatology 28:1260–1268.
Luo JH, Ren B, Keryanov S, Tseng GC, Rao UN, Monga SP, Strom S, Demetris AJ,Nalesnik M, Yu YP, Ranganathan S, Michalopoulos GK. 2006. Transcriptomic and genomicanalysis of human hepatocellular carcinomas and hepatoblastomas. Hepatology 44:1012–1024.
Luo JL, Kamata H, Karin M. 2005. IKK/NF-kappaB signaling: Balancing life and death--a newapproach to cancer therapy. J Clin Invest 115:2625–2632.
Maione D, Di Carlo E, Li W, Musiani P, Modesti A, Peters M, Rose-John S, Della Rocca C,Tripodi M, Lazzaro D, Taub R, Savino R, Ciliberto G. 1998. Coexpression of IL-6 andsoluble IL-6R causes nodular regenerative hyperplasia and adenomas of the liver. EMBO J17:5588–5597.
Mars WM, Kim TH, Stolz DB, Liu ML, Michalopoulos GK. 1996. Presence of urokinase inserum-free primary rat hepatocyte cultures and its role in activating hepatocyte growthfactor. Cancer Res 56:2837–2843.
Mars WM, Liu ML, Kitson RP, Goldfarb RH, Gabauer MK, Michalopoulos GK. 1995.Immediate early detection of urokinase receptor after partial hepatectomy and itsimplications for initiation of liver regeneration. Hepatology 21:1695–1701.
MarsWM, Zarnegar R, Michalopoulos GK. 1993. Activation of hepatocyte growth factor bythe plasminogen activators uPA and tPA. Am J Pathol 143:949–958.
Marubashi S, SakonM,NaganoH,GotohK,HashimotoK,KubotaM,Kobayashi S, YamamotoS, Miyamoto A, Dono K, Nakamori S, Umeshita K, Monden M. 2004. Effect of portalhemodynamics on liver regeneration studied in a novel portohepatic shunt rat model.Surgery 136:1028–1037.
Masumoto A, Yamamoto N. 1991. Sequestration of a hepatocyte growth factor inextracellular matrix in normal adult rat liver. Biochem Biophys Res Commun 174:90–95.
Masumoto A, Yamamoto N. 1993. Stimulation of DNA synthesis in hepatocytes byhepatocyte growth factor bound to extracellular matrix. Biochem Biophys Res Commun191:1218–1223.
Matsumoto K, Nakamura T. 1996. Emerging multipotent aspects of hepatocyte growthfactor. J Biochem 119:591–600.
Mead JE, Fausto N. 1989. Transforming growth factor alpha may be a physiological regulatorof liver regeneration by means of an autocrine mechanism. Proc Natl Acad Sci U S A86:1558–1562.
Menegazzi M, Carcereri-De Prati A, Suzuki H, Shinozuka H, Pibiri M, Piga R, Columbano A,Ledda-Columbano GM. 1997. Liver cell proliferation induced by nafenopin andcyproterone acetate is not associated with increases in activation of transcription factorsNF-kappaB and AP-1 or with expression of tumor necrosis factor alpha. Hepatology25:585–592.
Michalopoulos G, Houck KA, Dolan ML, Leutteke NC. 1984. Control of hepatocytereplication by two serum factors. Cancer Res 44:4414–4419.
Michalopoulos GK, Barua L, Bowen WC. 2005a. Transdifferentiation of rathepatocytes into biliary cells after bile duct ligation and toxic biliary injury. Hepatology41:535–544.
Michalopoulos GK, Bowen WC, Mule K, Stolz DB. 2001. Histological organization inhepatocyte organoid cultures. Am J Pathol 159:1877–1887.
Michalopoulos GK, Bowen WC, Zajac VF, Beer-Stolz D, Watkins S, Kostrubsky V,Strom SC. 1999. Morphogenetic events in mixed cultures of rat hepatocytes andnonparenchymal cells maintained in biological matrices in the presence of hepatocytegrowth factor and epidermal growth factor [see comments]. Hepatology 29:90–100.
Michalopoulos GK, DeFrances M. 2005b. Liver regeneration. Adv Biochem Eng Biotechnol93:101–134.
Michalopoulos GK, DeFrances MC. 1997. Liver regeneration. Science 276:60–66.Michalopoulos GK, Khan Z. 2005c. Liver regeneration, growth factors, and amphiregulin.Gastroenterology 128:503–506.
Miki T, Strom SC. 2006. Amnion-derived pluripotent/multipotent stem cells. Stem Cell Rev2:133–142.
Mitchell C, Nivison M, Jackson LF, Fox R, Lee DC, Campbell JS, Fausto N. 2005. Heparin-binding epidermal growth factor-like growth factor links hepatocyte primingwith cell cycleprogression during liver regeneration. J Biol Chem 280:2562–2568.
Miyazaki M, Masaka T, Akiyama I, Nakashima E, Sakaguchi M, Huh NH. 2004. Propagation ofadult rat bone marrow-derived hepatocyte-like cells by serial passages in vitro. CellTransplant 13:385–391.
Mohammed FF, Khokha R. 2005a. Thinking outside the cell: Proteases regulate hepatocytedivision. Trends Cell Biol 15:555–563.
Mohammed FF, Pennington CJ, Kassiri Z, Rubin JS, Soloway PD, Ruther U, Edwards DR,KhokhaR. 2005b.Metalloproteinase inhibitor TIMP-1 affects hepatocyte cell cycle viaHGFactivation in murine liver regeneration. Hepatology 41:857–867.
Monga SP, Mars WM, Pediaditakis P, Bell A, Mule K, Bowen WC, Wang X, Zarnegar R,Michalopoulos GK. 2002. Hepatocyte growth factor induces Wnt-independent nucleartranslocation of beta-catenin after Met-beta-catenin dissociation in hepatocytes. CancerRes 62:2064–2071.
Monga SP, Pediaditakis P, Mule K, StolzDB, MichalopoulosGK. 2001. Changes inWNT/beta-catenin pathway during regulated growth in rat liver regeneration. Hepatology 33:1098–1109.
Moolten FL, Bucher NL. 1967. Regeneration of rat liver: Transfer of humoral agent by crosscirculation. Science 158:272–274.
Mumm JS, Kopan R. 2000. Notch signaling: From the outside in. Dev Biol 228:151–165.
Murphy MO, Ghosh J, Fulford P, Khwaja N, Halka AT, Carter A, Turner NJ, Walker MG.2006. Expression of growth factors and growth factor receptor in non-healing and healingischaemic ulceration. Eur J Vasc Endovasc Surg 31:516–522.
Nagy P, Bisgaard HC, Thorgeirsson SS. 1994. Expression of hepatic transcription factorsduring liver development and oval cell differentiation. J Cell Biol 126:223–233.
Naldini L, Vigna E, Narsimhan RP, Gaudino G, Zarnegar R, MichalopoulosGK, Comoglio PM.1991. Hepatocyte growth factor (HGF) stimulates the tyrosine kinase activity of thereceptor encoded by the proto-oncogene c-MET. Oncogene 6:501–504.
NelsenCJ, RickheimDG, TuckerMM,Hansen LK, Albrecht JH. 2003. Evidence that cyclinD1mediates both growth and proliferation downstream of TOR in hepatocytes. J Biol Chem278:3656–3663.
Neubauer K, Knittel T, Aurisch S, Fellmer P, Ramadori G. 1996. Glial fibrillaryacidic protein—A cell type specific marker for Ito cells in vivo and in vitro. J Hepatol24:719–730.
NiN, Yager JD. 1994. Comitogenic effects of estrogens onDNA synthesis induced by variousgrowth factors in cultured female rat hepatocytes. Hepatology 19:183–192.
Ninomiya M, Harada N, Shiotani S, Hiroshige S, Minagawa R, Soejima Y, Suehiro T, NishizakiT, Shimada M, Sugimachi K. 2003. Hepatocyte growth factor and transforming growthfactor beta1 contribute to regeneration of small-for-size liver graft immediately aftertransplantation. Transpl Int 16:814–819.
Northemann W, Hattori M, Baffet G, Braciak TA, Fletcher RG, Abraham LJ, Gauldie J,Baumann M, Fey GH. 1990. Production of interleukin 6 by hepatoma cells. Mol Biol Med7:273–285.
Nozaki I, Lunz JG, III, Specht S, Stolz DB, Taguchi K, Subbotin VM, Murase N, Demetris AJ.2005. Small proline-rich proteins 2 are noncoordinately upregulated by IL-6/STAT3signaling after bile duct ligation. Lab Invest 85:109–123.
Nozawa K, Kurumiya Y, Yamamoto A, Isobe Y, Suzuki M, Yoshida S. 1999. Up-regulation oftelomerase in primary cultured rat hepatocytes. J Biochem 126:361–367.
Nussler AK, Di Silvio M, Liu ZZ, Geller DA, Freeswick P, Dorko K, Bartoli F, Billiar TR. 1995.Further characterization and comparison of inducible nitric oxide synthase in mouse, rat,and human hepatocytes. Hepatology 21:1552–1560.
Oben JA, Yang S, Lin H, Ono M, Diehl AM. 2003. Norepinephrine and neuropeptide Ypromote proliferation and collagen gene expression of hepatic myofibroblastic stellatecells. Biochem Biophys Res Commun 302:685–690.
Oe S, Lemmer ER, Conner EA, Factor VM, Leveen P, Larsson J, Karlsson S, Thorgeirsson SS.2004. Intact signaling by transforming growth factor beta is not required for termination ofliver regeneration in mice. Hepatology 40:1098–1105.
Oh SH, Witek RP, Bae SH, Zheng D, Jung Y, Piscaglia AC, Petersen BE. 2007. Bonemarrow-derived hepatic oval cells differentiate into hepatocytes in 2-acetylaminofluorene/partial hepatectomy-induced liver regeneration. Gastroenterology 132:1077–1087.
Ohlson LC, Koroxenidou L, Hallstrom IP. 1998. Inhibition of in vivo rat liver regeneration by2-acetylaminofluorene affects the regulation of cell cycle-related proteins. Hepatology27:691–696.
Olle EW, Ren X, McClintock SD,Warner RL, Deogracias MP, Johnson KJ, Colletti LM. 2006.Matrix metalloproteinase-9 is an important factor in hepatic regeneration after partialhepatectomy in mice. Hepatology 44:540–549.
Olsen PS, Poulsen SS, Kirkegaard P. 1985. Adrenergic effects on secretion of epidermalgrowth factor from Brunner’s glands. Gut 26:920–927.
Overturf K, al-Dhalimy M, Ou CN, Finegold M, Grompe M. 1997. Serial transplantationreveals the stem-cell-like regenerative potential of adult mouse hepatocytes. Am J Pathol151:1273–1280.
Papastefanou VP, Bozas E, Mykoniatis MG, Grypioti A, Garyfallidis S, Bartsocas CS,Nicolopoulou-Stamati P. 2007. VEGF isoforms and receptors expression throughout acuteacetaminophen-induced liver injury and regeneration. Arch Toxicol (Epub ahead of print).
Paranjpe S, Bowen WC, Bell AW, Nejak-Bowen K, Luo JH, Michalopoulos GK. 2007. Cellcycle effects resulting from inhibition of hepatocyte growth factor and its receptor c-Met inregenerating rat livers by RNA interference. Hepatology 45:1471–1477.
JOURNAL OF CELLULAR PHYSIOLOGY DOI 10.1002/JCP
L I V E R R E G E N E R A T I O N 299
userr
Highlight

© 2004 Nature Publishing Group
836 | OCTOBER 2004 | VOLUME 5 www.nature.com/reviews/molcellbio
R E V I E W S
The liver is an important organ within the body thathas a central role in metabolic homeostasis, as it isresponsible for the metabolism, synthesis, storage andredistribution of nutrients, carbohydrates, fats andvitamins1. The liver produces large numbers of serumproteins including albumin and ACUTE-PHASE PROTEINS,enzymes and cofactors. Importantly, it is the maindetoxifying organ of the body, which removes wastesand xenobiotics by metabolic conversion and biliaryexcretion. The main cell type of the liver that carriesout most of these functions is the parenchymal cell, orhepatocyte, which makes up ~80% of hepatic cells.The other 20% comprises the non-parenchymal cells,which include endothelial cells, KUPFFER CELLS, lympho-cytes and STELLATE CELLS. Endothelial cells line the intra-hepatic circulatory vessels, or SINUSOIDS, of the liver,which provide a large surface area for nutrientabsorption. Kupffer cells also reside in the sinusoidsand are essential for the phagocytosis of foreign parti-cles and infecting organisms, as well as the produc-tion of CYTOKINES. Lymphocytes are also part of theinnate immune system that resides within the liver tohelp resist infection. Hepatic stellate cells have variousfunctions, including the storage of vitamin A and theproduction of the extracellular matrix. All of thesecell types are activated by hepatic injury and the stel-late cells produce most of the factors that lead tohepatic FIBROSIS.
Although adult hepatocytes are long lived and nor-mally do not undergo cell division, they maintain theability to proliferate in response to toxic injury andinfection. The amazing regenerative capacity of the
liver was first described in Greek mythology (BOX 1) and ismost clearly shown by the two-thirds PARTIAL-HEPATECTOMY
model in rodents, which was pioneered by Higgins andAnderson2 in 1931. In this model, two thirds of theliver is surgically removed, and the remaining liverenlarges until the original liver mass is restored —approximately 1 week after surgery — after which theregenerative process stops. The word ‘regeneration’ is amisnomer because the lobes of the liver that areremoved do not grow back, unlike the regeneration oflimbs in amphibian models. Instead, there is a hyper-plastic response that involves the replication of virtu-ally all of the mature functioning cells in the remnantliver. So, in this experimental system, liver regenerationdoes not require the recruitment of liver stem cells orprogenitor cells, but involves replication of the maturefunctioning liver cells. The regenerative process is com-pensatory because the size of the resultant liver is deter-mined by the demands of the organism, and, once theoriginal mass of the liver has been re-established, pro-liferation stops.
There are various central questions regarding theprocess of liver regeneration. First, what are the signalsthat trigger the early events in the regenerative process?Second, how are the architecture and function of theliver retained during regeneration? Third, which signalsare responsible for turning off the growth responseonce the mass of the liver is reconstituted? Investigatorshave begun to answer these questions by using molecu-lar and genetic approaches to identify the importantregulatory pathways that control the regenerativeprocess.
LIVER REGENERATION:FROM MYTH TO MECHANISMRebecca Taub*‡
Abstract | The unusual regenerative properties of the liver are a logical adaptation by organisms,as the liver is the main detoxifying organ of the body and is likely to be injured by ingested toxins.The numerous cytokine- and growth-factor-mediated pathways that are involved in regulatingliver regeneration are being successfully dissected using molecular and genetic approaches. So what is known about this process at present and which questions remain?
*University of PennsylvaniaSchool of Medicine,Philadelphia, Pennsylvania19004, USA.‡Metabolic Diseases,Hoffman-La RocheIncorporated, 340 KingslandStreet, Nutley, New Jersey07110, USA.e-mail:[email protected]:10.1038/nrm1489
ACUTE-PHASE RESPONSE
A defence reaction of theorganism to toxic or infectiousagents that seeks to eliminate thecausative agent and restrictorgan damage through theproduction of cytokines such asinterleukin (IL)-6 and -1 andtumour necrosis factor (TNF)α.These cytokines upregulate theproduction of acute-phaseproteins, such as complement(C)-reactive protein and serumamyloid protein, which protectagainst damage in the liver andother organs.
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Textbox
5. Taub2004 (truncated)

© 2004 Nature Publishing Group
NATURE REVIEWS | MOLECULAR CELL BIOLOGY VOLUME 5 | OCTOBER 2004 | 837
R E V I E W S
KUPFFER CELL
A macrophage, or monocyticcell, of the liver that ispermanently located in the liverwithin gaps between sinusoidalendothelial cells. Kupffer cellsform the largest population ofmacrophages within the bodyand can migrate within the liverto sites of injury.
STELLATE CELL
A cell that resides within thespace of Disse, in recessesbetween hepatocytes. Theyamount to 2–20 per 100hepatocytes, and their mainfunction lies in the storage ofvitamin A. Stellate cells areactivated during liver injury andbecome myofibroblasts thatproduce extracellular matrix.They are important in theprogression of fibrosis and liverdisease.
regeneration but have not yet been associated with spe-cific growth-factor- or cytokine-regulated signal-trans-duction pathways. This review does not include adetailed discussion of such molecules, but a recentreview describes many of these transcription factorsincluding CREM (cAMP-response-element modula-tor), the Foxo proteins and others9.
Basic characteristics of liver regenerationCell division is rarely seen in hepatocytes in the nor-mal adult liver, as these cells are in the G0 phase of thecell cycle3,5. However, after partial hepatectomyapproximately 95% of hepatic cells, which are nor-mally quiescent, rapidly re-enter the cell cycle. In therat liver, the rate of DNA synthesis in hepatocytesbegins to increase after about 12 hours — as theyenter the S phase of the cell cycle — and peaksaround 24 hours (FIG. 2). However, the induction ofDNA synthesis occurs later in the non-parenchymalcells (at ~48 hours for Kupffer and biliary epithelial cells,and at ~96 hours for endothelial cells). Subsequentlevels of DNA synthesis in hepatocytes are lower, ascomplete restoration of liver mass requires an averageof ~1.6 cycles of replication in all cells. By compari-son, the peak in DNA synthesis in mice occurs later(36–40 hours after partial hepatectomy) and variesbetween strains. The onset of DNA synthesis is well-synchronized in hepatocytes, beginning in cells thatsurround the portal vein of the LIVER LOBULE and pro-ceeding towards the central vein. The incidence ofmitosis (M phase) is lower than is predicted on thebasis of the number of hepatocytes that undergoDNA synthesis, and the PLOIDY of hepatocytes and per-centage of binucleate cells increases with successiverounds of DNA synthesis, which ultimately limits fur-ther regeneration10. Moreover, circadian rhythmsmight affect the timing of DNA synthesis and theexpression of cyclins after partial hepatectomy11.Most of the increase in liver mass has occurred by 3days after partial hepatectomy and mass restoration iscomplete in 5–7 days12.
In animal models, in which hepatocytes are directlydamaged and thereby induced to undergo necrosis,similar growth-factor- and cytokine-mediated path-ways are activated as occurs after partial hepatectomy13.Proliferation of hepatocytes is also involved in the liverregeneration that occurs after massive hepatocytenecrosis, or apoptosis that is induced by hepatic toxinssuch as CCl
4or systemically introduced Fas LIGAND — but
the cell-cycle response is not as synchronized6–8. Asexpected, there are also significant changes in liverarchitecture during liver regeneration — both after par-tial hepatectomy and liver necrosis. The induction ofnew forms of FIBRONECTIN, cell-adhesion proteins andother basement-membrane proteins is observed.Changes in intra- and inter-cellular junctions occurtransiently during regeneration, and reformation of thenormal liver architecture occurs only after the restora-tion of the original liver mass. However, little is knownabout the complex process that regulates the reorgani-zation of the liver architecture.
This review focuses on two main pathways — acytokine-dependent and a cytokine-independent path-way — that are crucial for this process, and attempts tobegin defining regions of overlap2–8 (FIG. 1). ManyGROWTH FACTORS and cytokines have been implicated inregulating liver regeneration. The growth factorsinclude hepatocyte growth factor (HGF), epidermalgrowth factor (EGF), transforming growth factors(TGFs), insulin and glucagons. And the cytokinesinclude tumour necrosis factor (TNF)α and inter-leukin (IL)-6. There are several individual transcriptionfactors or proteins that are required for normal liver
Box 1 | The myth of Prometheus
Liver regeneration has evolved to protect animals in thewild from the catastrophic results of liver loss that canbe caused by ingested toxins. The process has beenrecognized by scientists for many years and was evendescribed by the ancient Greeks, who mentioned liverregeneration in the myth of Prometheus. Having stolenthe secret of fire from the gods of Olympus, Prometheusdrew down on himself the anger of Zeus, the ruler ofgods and men. Zeus punished Prometheus by chaininghim to Mount Caucasus where he was tormented by aneagle. The eagle preyed on Prometheus’ liver, which wasrenewed as fast as it was devoured. Adapted fromBulfinch’s Mythology (see online links box).
Figure 1 | Liver regeneration is triggered by partial hepatectomy or liver damage. Afterpartial hepatectomy or liver injury, several signals are initiated simultaneously in the liver. Gut-derived factors, such as lipopolysaccharide (LPS), are upregulated after liver injury or hepatectomyand reach the liver through the portal blood supply. They activate hepatic non-parenchymal cells(including Kupffer cells and stellate cells) and increase the production of tumour necrosis factor(TNF)α and interleukin (IL)-6. Other factors are released from the pancreas (insulin), duodenum orsalivary gland (epidermal growth factor; EGF), adrenal gland (norepinepherine), thyroid gland(triodothronine; T3) and stellate cells (hepatocyte growth factor; HGF). Cooperative signals fromthese factors allow the hepatocytes to overcome cell-cycle checkpoint controls and move from G0, through G1, to the S phase of the cell cycle. This leads to DNA synthesis and hepatocyteproliferation. Transforming growth factor β (TGFβ) signalling, which inhibits hepatocyte DNAsynthesis, is blocked during the proliferative phase but is restored at the end of the process ofregeneration by helping to return hepatocytes to the quiescent state.
Partial hepatectomyor liver injury
LPS↑ (portal blood flow)
Hepatocyte
G0/G1
Hepatocyte
G1/S
Hepatocyte
G1
Kupffer cell
Thyroid Pancreas Adrenalgland
Duodenum
T3Insulin
Norepinephrine
EGF
IL-6
TNFα
HGF TGFβ
Stellate cell
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight

© 2004 Nature Publishing Group
838 | OCTOBER 2004 | VOLUME 5 www.nature.com/reviews/molcellbio
R E V I E W S
And, intracellular-signalling pathways that involvemitogen-activated protein kinase (MAPK) and, morespecifically, pERKs (phosphorylated extracellular sig-nal-regulated kinases), Jun amino-terminal kinase(JNK) and receptor tyrosine kinases, are rapidly acti-vated according to a similar time frame, thereby pro-viding clues to the initiating signals. Genetic andpharmacological approaches have confirmed thatregeneration is a complex process6–8,18,19,29–67.
A thorough discussion of all of these proteins is notpossible within the scope of this review. However, it isnow possible to connect many of the proteins that areinvolved to two distinct linear pathways that are eithercytokine or growth-factor dependent, and to identifyregions of overlap between these two main regulatorymechanisms (FIG. 3). Cytokines bind to their cellularreceptors, thereby generating intracellular signals thatlead to transcription-factor activation. What distin-guishes them from growth factors is their ability to acti-vate selective intracellular-signalling pathways that arenot linked to MITOGENESIS68,69. These distinctions are not
Hepatocytes are unable to replicate in response tocertain types of injury. Agents such as dipin, retror-sine or galactosamine inflict liver damage in animals;however, the replicative capacity of most normalhepatocytes is diminished and a population of cellsknown as OVAL CELLS proliferates to replace the hepaticparenchyma13,14. The origin of oval cells is controversial.Although they were thought to be derived from biliaryepithelial cells3, recent studies indicate that they mightoriginate from hepatocytes that have somehow escapedinjury15.
Individual hepatocytes have an amazing replicativecapacity, as only a few hepatocytes are required torestore liver mass after profound liver injury16,17.Telomere length is important for the replicative poten-tial of hepatocytes, as telomerase deficiency (caused bygene knockouts) impairs DNA synthesis in a subset ofcells that have critically short telomeres, and shortensthe lifespan of hepatocytes in general — thereby lead-ing to impaired hepatic regeneration18,19. Other liver-repopulation and transplantation studies indicate thatbone-marrow stem cells might have the capacity todifferentiate into hepatocytes20,21. But, it is unclearwhether this transition is a rare event or the normalmeans by which the liver replenishes its hepatocytepool when faced with certain types of injury. Recentstudies have indicated that rare cell-fusion eventsbetween bone-marrow stem cells and hepatocytescould give the appearance that the resulting cells arederived from bone-marrow stem cells when they are,in fact, of hepatocyte origin22,23.
Discovering liver-regeneration pathwaysExperiments that were carried out by Moolten andBucher24 showed that circulating growth factors thatare present in the serum of hepatectomized rats caninduce hepatocyte replication in PARABIOSED animalswith normal livers. Early studies using isolated hepa-tocytes led to the identification of several potentialhepatocyte growth factors such as HGF, TGFα and theanti-proliferative factor TGFβ. However, it was diffi-cult to prove that any of these factors had an essentialrole in liver regeneration itself.
Molecular studies of gene-expression cascades inthe regenerating liver have provided insights into thesignalling pathways that are rapidly activated in theremnant liver post-hepatectomy. More than 100IMMEDIATE-EARLY GENES have been identified, which areactivated by normally latent transcription factors atthe transition between G0 and G1, before the onsetof de novo protein synthesis. The advent of microar-rays expanded this list even further25–28, and gene-expression profiles indicate that some genes showtransient upregulation, whereas others — particu-larly those involved in protein synthesis and cellgrowth — are elevated throughout the main prolif-erative response in the regenerating liver (FIG. 2).Specific transcription factors, such as nuclear factor(NF)-κB, signal transducer and activator of transcrip-tion (STAT)3 and AP1, are rapidly activated in rem-nant hepatocytes minutes after partial hepatectomy4.
SINUSOID
Hepatic microcirculatory vesselwith its base at the perimeter of the classic lobule that includesthe portal vein, hepatic arteryand apex of the central vein. It isthe basic blood-circulatory unitof the liver. A single inlet portalvenule serves ~19 blood-deliverycapillaries or sinusoids thatsurround the hepatocytes andare lined by fenestratedendothelial cells.
CYTOKINE
A member of a large family ofsecreted proteins that interactwith a cellular receptor. Cytokineproduction results in theactivation of an intracellular-signalling cascade thatcommonly regulates processessuch as immune function andinflammation.
LIVER FIBROSIS AND CIRRHOSIS
A process that leads to theaccumulation of extracellularmatrix and collagen. Thesesubstances are primarily laiddown by activated hepaticstellate cells during chronic liverinjury, which is caused byhepatotoxins, such as alcohol, orby viral hepatitis. Fibrosis andcirrhosis are part of the sameprocess, cirrhosis being end-stage, generally irreversible, liverfibrosis that is associated withclinical signs such as portalhypertension.
PARTIAL HEPATECTOMY
The removal of specific lobes ofthe liver, generally by ligation ofthe blood supply and resection.The procedure normally doesnot involve a specific incision ina liver lobe.
GROWTH FACTOR
A member of a large family ofsecreted proteins that interactwith a cellular receptor, whichleads to a mitogenic responsethat results in DNA synthesisand progression through the cellcycle. Growth factors commonlyinteract with receptor tyrosinekinases.
LIVER LOBULE
A microscopic unit of liverparenchyma. This hexagonalunit contains portal tracts at itsperiphery and a central veinfrom which one-cell-deep platesof hepatocytes radiate.
Figure 2 | Patterns of DNA synthesis and induction ofgene expression during rat liver regeneration. a | Afterpartial hepatectomy, DNA synthesis in hepatocytes (H; green)peaks around 24 hours, whereas DNA synthesis in the non-parenchymal cells (NP; yellow) peaks around 36–48 hours. Re-accumulation of liver mass (red) is complete within a week.b | The induction pattern of gene expression for growth-regulated genes, such as β-actin. c | The induction pattern ofgene expression for cell-cycle-regulated genes, such asinsulin-like-growth-factor-binding protein-1 (IGFBP1). d | Somegenes, such as that encoding the α isoform of CCAAT-enhancer-binding protein (C/EBPα), are downregulated duringthe period of maximal growth and are re-expressed after thegrowth phase has occurred. Modified with permission fromREF. 6 © 2003 Elsevier.
b Growth-regulated genes
a
c Cell-cycle-regulated genes
d Gene expression after growth phase
Hours post-hepatectomy
0 2 4 8 24 36 48 60 72 168 216
Liver mass
NPDNAH
DNA
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
userr
Highlight
© 2004 Nature Publishing Group
846 | OCTOBER 2004 | VOLUME 5 www.nature.com/reviews/molcellbio
R E V I E W S
1. Saxema, R., Zucker, S. D. & Crawford, J. M. in Hepatology:A Textbook of Liver Disease. (eds Zakim, D. Z. & Boyer, T. D.)Ch. 1 (Saunders, Philadelphia, USA, 2003).
2. Higgins, G. M. & Anderson, R. M. Experimental pathology ofthe liver. I. Restoration of the liver of the white rat followingpartial surgical removal. Arch. Pathol. 12, 186–202 (1931).Original description of liver regeneration after partialhepatectomy, which is basically the same techniquethat is used today.
3. Michalopoulos, G. K. & DeFrances, M. C. Liver regeneration.Science 276, 60–66 (1997).
4. Taub, R., Greenbaum, L. E. & Peng, Y. Transcriptionalregulatory signals define cytokine-dependent and -independent pathways in liver regeneration. Semin. Liver Dis. 19, 117–127 (1999).
5. Fausto, N. & Webber, E. M. in The Liver: Biology andPathobiology (eds Arias, I. M., Boyer, J. L., Fausto, N.,Jacoby, W. B., Schachter, D. & Shafritz, D. A.) 53–68 (RavenPress Ltd, New York, USA, 1994).
6. Taub, R. in Hepatology: A Textbook of Liver Disease. (edsZakim, D. Z. & Boyer, W. B.) Ch. 2 (Saunders, Philadelphia,USA, 2003).
7. Koniaris, L. G., McKillop, I. H., Schwartz, S. I. & Zimmers, T. A. Liver regeneration. J. Am. Coll. Surg. 197,634–659 (2003).
8. Fausto N. Lessons from genetically engineered animalmodels. V. Knocking out genes to study liver regeneration:present and future. Am. J. Physiol. 277, G917–G921 (1999).
9. Costa, R. H., Kalinichenko, V. V., Holterman, A.-X. L. &Wang, X. Transcription factors in liver development,differentiation, and regeneration. Hepatology 38,1331–1347 (2003).
10. Sigal, S. H. et al. Partial hepatectomy-induced polyploidyattenuates hepatocyte replication and activates cell agingevents. Am. J. Physiol. 276, G1260–G1272 (1999).
11. Matsuo, T. et al. Control mechanism of the circadian clockfor timing of cell division in vivo. Science 302, 255–259(2003).
12. Grisham, J. W. A morphologic study of deoxyrobonucleicacid synthesis and cell proliferation in regenerating rat liver:autoradiography with thymidine-H. Cancer Res. 22,842–849 (1962).Reports the critical timing of liver regeneration andassesses DNA synthesis in different cell types.
13. Dabeva, M. D. & Shafritz, D. A. Activation, proliferation, anddifferentiation of progenitor cells into hepatocytes in the D-galactosamine model of liver regeneration. Am. J. Pathol.143, 1606–1620 (1993).
14. Fausto, N. Liver regeneration. J. Hepatol. 32 (Suppl. 1),19–31 (2000).
15. Braun, K. M. & Sandgren, E. P. Cellular origin of regeneratingparenchyma in a mouse model of severe hepatic injury. Am. J. Pathol. 157, 561–569 (2000).
16. Sandgren, E. P. et al. Complete hepatic regeneration aftersomatic deletion of an albumin-plasminogen activatortransgene. Cell 66, 245–256 (1991).
17. Overturf, K., Al-Dhalimy, M., Finegold, M. & Grompe, M. Therepopulation potential of hepatocyte populations differing insize and prior mitotic expansion. Am. J. Pathol. 155,2135–2143 (1999).
18. Rudolph, K. L. et al. Inhibition of experimental liver cirrhosisin mice by telomerase gene delivery. Science 287,1253–1258 (2000).Provides insight into the mechanism by which thereplicative potential of hepatocytes is maintainedthrough many generations.
19. Satyanarayana, A. et al. Telomere shortening impairs organregeneration by inhibiting cell cycle re-entry of asubpopulation of cells. EMBO J. 22, 4003–4013 (2003).
20. Petersen, B. E. et al. Bone marrow as a potential source ofhepatic oval cells. Science 284, 1168–1170 (1999).
21. Ilagasse, E. et al. Purified hematopoietic stem cells candifferentiate into hepatocytes in vivo. Nature Med. 6,1229–1234 (2000).
22. Vassilopoulos, G., Wang, P. R. & Russell, D. W. Transplantedbone marrow regenerates liver by cell fusion. Nature 922,901–904 (2003).
23. Fausto, N. & Campbell, J. S. The role of hepatocytes andoval cells in liver regeneration and repopulation. Mech. Dev.120, 117–130 (2003).
24. Moolten, F. L. & Bucher, N. L. Regeneration of rat liver:transfer of humoral agent by cross circulation. Science 158,272–274 (1967).An important article, which established thatcirculating factors can induce liver regeneration. Thissubsequently led to efforts to identify and isolatehepatocyte growth factors.
25. Haber, B. A., Mohn, K. L., Diamond, R. H. & Taub, R.Induction patterns of 70 genes during nine days afterhepatectomy define the temporal course of liverregeneration. J. Clin. Invest. 91, 1319–1326 (1993).
26. Su, A. I., Guidotti, L. G., Pezacki, J. P., Chisari, F. V. &Schultz, P. G. Gene expression during the priming phase ofliver regeneration after partial hepatectomy in mice. Proc. Natl Acad. Sci. USA 99, 11181–11186 (2002).
27. Kelley-Loughnane, N., Sabla, G. E., Ley-Ebert, C., Aronow, B. J. & Bezerra, J. A. Independent and overlappingtranscriptional activation during liver development andregeneration in mice. Hepatology 35, 525–534 (2002).
28. Arai, M. et al. Gene expression profiling reveals themechanism and pathophysiology of mouse liverregeneration. J. Biol. Chem. 278, 29813–29818 (2003).
29. Currier, A. R. et al. Plasminogen directs the pleiotropiceffects of uPA in liver injury and repair. Am. J. Physiol.Gastrointest. Liver Physiol. 284, G508–G515 (2003).
30. Wheeler, M. D. et al. Impaired Ras membrane associationand activation in PPARα knockout mice after partialhepatectomy. Am. J. Physiol. Gastrointest. Liver Physiol.284, G302–G312 (2003).
31. Bustos, M. et al. Protection against liver damage bycardiotrophin-1, a hepatocyte survival factor up-regulated inthe regenerating liver in rats. Gastroenterology 125,192–201 (2003),
32. Leclercq, I. A., Field, J. & Farrell, G. C. Leptin-specificmechanisms for impaired liver regeneration in ob/ob miceafter toxic injury. Gastroenterology 124, 1451–1464 (2003).
33. Kiso, S. et al. Liver regeneration in heparin-binding EGF-likegrowth factor transgenic mice after partial hepatectomy.Gastroenterology 124, 701–707 (2003).
34. Schwabe, R. F. et al. c-Jun-N-terminal kinase drives cyclinD1 expression and proliferation during liver regeneration.Hepatology 37, 824–832 (2003).
35. Kalinichenko, V. V. et al. Foxf1+/– mice exhibit defectivestellate cell activation and abnormal liver regenerationfollowing CCl4 injury. Hepatology 37, 107–117 (2003).
36. Malik, R., Mellor, N., Selden, C. & Hodgson, H.Triiodothyronine enhances the regenerative capacity of theliver following partial hepatectomy. Hepatology 37, 79–86(2003).
37. Nelsen, C. J., Rickheim, D. G., Tucker, M. M., Hansen, L. K.& Albrecht, J. H. Evidence that cyclin D1 mediates bothgrowth and proliferation downstream of TOR inhepatocytes. J. Biol. Chem. 278, 3656–3663 (2003).Shows that TOR could be an important factor inestablishing liver size.
38. Leu, J. I., Crissey, M. A., Craig, L. E. & Taub, R. Impairedhepatocyte DNA synthetic response posthepatectomy ininsulin-like growth factor binding protein 1-deficient micewith defects in C/EBPβ and mitogen-activated proteinkinase/extracellular signal-regulated kinase regulation. Mol. Cell. Biol. 23, 1251–1259 (2003).
39. Ren, X., Carpenter, A., Hogaboam, C. & Colletti, L.Mitogenic properties of endogenous and pharmacologicaldoses of macrophage inflammatory protein-2 after 70%hepatectomy in the mouse. Am. J. Pathol. 163, 563–570(2003).
40. Casado, M. et al. Contribution of cyclooxygenase 2 to liverregeneration after partial hepatectomy. FASEB J. 15,2016–2018 (2001).
41. Hogaboam, C. M. et al. Novel CXCR2-dependent liverregenerative qualities of ELR-containing CXC chemokines.FASEB J. 13, 1565–1574 (1999).
42. Selzner, N. et al. ICAM-1 triggers liver regeneration throughleukocyte recruitment and Kupffer cell-dependent release ofTNF-α/IL-6 in mice. Gastroenterology 124, 692–700 (2003).
43. Luedde, T. et al. p18INK4c collaborates with other CDK-inhibitory proteins in the regenerating liver. Hepatology 37,833–841 (2003).
44. Anderson, S. P. et al. Delayed liver regeneration inperoxisome proliferator-activated receptor-α-null mice.Hepatology 36, 544–554 (2002).
45. Behrens, A. et al. Impaired postnatal hepatocyte proliferationand liver regeneration in mice lacking c-jun in the liver.EMBO J. 21, 1782–1790 (2002).Together with other studies, this article shows thesignificance of Jun in providing an important linkbetween immediate-early genes and DNA synthesis.
46. Shimizu, M. et al. Mechanism of retarded liver regenerationin plasminogen activator-deficient mice: impaired activationof hepatocyte growth factor after Fas-mediated massivehepatic apoptosis. Hepatology 33, 569–576 (2001).
47. Ren, X., Hogaboam, C., Carpenter, A. & Colletti, L. Stem cellfactor restores hepatocyte proliferation in IL-6 knockoutmice following 70% hepatectomy. J. Clin. Invest. 112,1407–1418 (2003).
Establishes a potentially important link between IL-6and a downstream growth factor, which could link thecytokine- and growth-factor-mediated pathways.
48. Strey, C. W. et al. The proinflammatory mediators C3a andC5a are essential for liver regeneration. J. Exp. Med. 198,913–923 (2003).
49. Temme, A., Ott, T., Dombrowski, F. & Willecke, K. The extentof synchronous initiation and termination of DNA synthesis inregenerating mouse liver is dependent on connexin32expressing gap junctions. J. Hepatol. 32, 627–635 (2000).
50. Mastellos, D., Papadimitriou, J. C., Franchini, S., Tsonis, P. A. & Lambris, J. D. A novel role of complement:mice deficient in the fifth component of complement (C5)exhibit impaired liver regeneration. J. Immunol. 166,2479–2486 (2001).
51. Hayashi, E. et al. Loss of p27Kip1 accelerates DNA replicationafter partial hepatectomy in mice. J. Surg. Res. 111,196–202 (2003).
52. Imai, T., Jiang, M., Kastner, P., Chambon, P. & Metzger, D.Selective ablation of retinoid X receptor α in hepatocytesimpairs their lifespan and regenerative capacity. Proc. NatlAcad. Sci. USA 98, 4581–4586 (2001).
53. LeCouter, J. et al. Angiogenesis-independent endothelialprotection of liver: role of VEGFR-1. Science 299, 890–893(2003).
54. Wang, X., Kiyokawa, H., Dennewitz, M. B. & Costa, R. H.The Forkhead Box m1b transcription factor is essential forhepatocyte DNA replication and mitosis during mouse liverregeneration. Proc. Natl Acad. Sci. USA 99, 16881–16886(2002).
55. Cressman, D. E. et al. Liver failure and defective hepatocyteregeneration in interleukin-6-deficient mice. Science 274,1379–1383 (1996).The first study to link the cytokine IL-6 to liverregeneration.
56. Yamada Y. et al. Initiation of liver growth by tumor necrosisfactor: defective liver regeneration in mice lacking type Itumor necrosis factor receptor. Proc. Natl Acad. Sci. USA94, 1441–1446 (1997).Establishes the critical link between cytokineactivation and liver regeneration.
57. Greenbaum, L. E. et al. CCAAT enhancer-binding protein βis required for normal hepatocyte proliferation in mice afterpartial hepatectomy. J. Clin. Invest. 102, 996–1007 (1998).
58. Smith, A. J., Ronald, P. J. & Elferink, O. Liver genedisruption: winners by KO? J. Hepatology 31, 752–759(1999).
59. Loranger, A. et al. Simple epithelium keratins are required formaintenance of hepatocyte integrity. Am. J. Pathol. 151,1673–1683 (1997).
60. Reimold, A. M. et al. An essential role in liver developmentfor transcription factor XBP-1. Genes Dev. 14, 152–157(2000).
61. Rai, R. M. et al. Impaired liver regeneration in inducible nitricoxide synthase-deficient mice. Proc. Natl Acad. Sci. USA95, 13829–13834 (1998).
62. Ueki, T. et al. Hepatocyte growth factor gene therapy of livercirrhosis in rats. Nature Med. 5, 226–230 (1999).
63. Matsuda, Y. et al. Preventive and therapeutic effects in ratsof hepatocyte growth factor infusion on liverfibrosis/cirrhosis. Hepatology 26, 81–89 (1997).
64. Beg, A. A. et al. Embryonic lethality and liver degeneration inmice lacking the RelA component of NF-κB. Nature 376,167–170 (1995).Establishes the importance of NFκB inhepatoprotection against apoptosis.
65. DeAngelis, R. A., Kovalovich, K., Cressman, D. E. & Taub, R.Normal liver regeneration in p50/nuclear factor κB1knockout mice. Hepatology 33, 915–924 (2001).
66. Li, W., Liang, X., Kellendonk, C., Poli, V. & Taub, R. STAT3contributes to the mitogenic response of hepatocytes duringliver regeneration. J. Biol. Chem. 277, 28411–28417 (2002).
67. Servillo, G., Della Fazia, M. A. & Sassone-Corsi, P.Transcription factor CREM coordinates the timing ofhepatocyte proliferation in the regenerating liver. Genes Dev.12, 3639–3643 (1998).
68. Levy, D. E. & Lee, C. K. What does Stat3 do? J. Clin. Invest.109, 1143–1148 (2002).
69. Heinrich, P. C. et al. Principles of interleukin (IL)-6-typecytokine signalling and its regulation. Biochem. J. 374, 1–20(2003).
70. Sakamoto, T. et al. Mitosis and apoptosis in the liver ofinterleukin-6-deficient mice after partial hepatectomy.Hepatology 29, 403–411 (1999).
71. Wuestefeld, T. et al. Interleukin-6/glycoprotein 130-dependent pathways are protective during liverregeneration. J. Biol. Chem. 278, 11281–11288 (2003).
72. Blindenbacher, A. et al. Interleukin-6 is important for survivalafter partial hepatectomy in mice. Hepatology 38, 674–682(2003).
userr
Highlight


















