Tissue microarrays for early target evaluation
8
TECHNOLOGIES DRUGDISCOVERY TODAY Tissue microarrays for early target evaluation Ronald Simon, Martina Mirlacher, Guido Sauter * Division of Molecular Pathology, Institute of Pathology, Basel University Hospital, Schoenbeinstrasse 40, CH-4031 Basel, Switzerland Early assessment of the probable biological importance of drug targets, the potential market size of a successful new drug, and possible treatment side effects are critical for risk management in drug development. A comprehensive molecular epidemiology analysis involving thousands of well-characterized human tissues will thus provide vital information for strategic decision-making. Tissue microarray (TMA) technology is ideally suited for such projects. The simultaneous analysis of thousands of tissues enables highly standar- dized, fast and affordable translational research studies of unprecedented scale. Section Editors: Wolfgang Fischer, Rob Hooft, Michael Walker The analysis of human tissue is a key step in the identification of drug targets. This analysis is usually done with individual tissues, focusing on the investigation of individual genes. Often, however, this process is time-consuming and can give controversial results. Tissue microarrays enable the analysis of a large number of small sample sections of tissue simultaneously; thereby combining increased statistical accuracy and high throughput. In this review, the authors describe the benefits, the proper handling to address-specific questions, and the limitations of this technique. Introduction A variety of powerful high-throughput technologies are avail- able for the identification of potential new drug targets. At the same time, high-throughput compound screening facil- itates the identification of applicable drug substances. These tools generally identify more potentially rewarding drug targets than resources are available for their further develop- ment. Thus, an efficient target prioritization strategy is cru- cial for competitive drug development. Whereas target identification is usually performed in experimental systems like cell lines or animal models because of the almost unlim- ited availability of resources, target evaluation and prioritiza- tion should be optimally based on findings from patient tissue specimens representing the disease the drug is devel- oped against. In situ analyses methods are optimally suited for target gene analyses as they allow a cellular and sub-cellular localization of the gene product of interest. However, tradi- tional slide-by-slide analysis cannot catch up with the speed of modern high-throughput target identification technolo- gies. Tissue microarrays (TMAs) permit a completely new early evaluation strategy of drug targets. The simultaneous and rapid analysis of thousands of human tissues allows determination of the frequency of target gene expression, for example, in all human tumor types, associations with disease progression, and expression in normal tissues. TMA technology Hundreds of cylindrical samples measuring up to 4 mm (usually 0.6 mm) in diameter are removed from formalin fixed or frozen tissues and are deposited into one recipient block [1]. Sections from such TMA blocks containing hun- dreds of different tissues are then placed on a glass slide. All methods for in situ tissue analysis, like immunohistochem- istry (IHC), fluorescence in situ hybridization (FISH) and RNA in situ hybridization, can be performed on TMAs using similar protocols as for conventional large sections (Fig. 1). After its initial description in 1998 [1], TMAs have become widely used in recent years. More than 150 publications Drug Discovery Today: Technologies Vol. 1, No. 1 2004 Editors-in-Chief Kelvin Lam – Pfizer, Inc., USA Henk Timmerman – Vrije Universiteit, The Netherlands Target identification *Corresponding author: (G. Sauter) [email protected] 1740-6749/$ ß 2004 Elsevier Ltd. All rights reserved. DOI: 10.1016/j.ddtec.2004.08.003 www.drugdiscoverytoday.com 41
-
Upload
ronald-simon -
Category
Documents
-
view
212 -
download
0
Transcript of Tissue microarrays for early target evaluation

TECHNOLOGIES
DRUG DISCOVERY
TODAY
Drug Discovery Today: Technologies Vol. 1, No. 1 2004
Editors-in-Chief
Kelvin Lam – Pfizer, Inc., USA
Henk Timmerman – Vrije Universiteit, The Netherlands
Target identification
Tissue microarrays for early targetevaluationRonald Simon, Martina Mirlacher, Guido Sauter*Division of Molecular Pathology, Institute of Pathology, Basel University Hospital, Schoenbeinstrasse 40, CH-4031 Basel, Switzerland
Early assessment of the probable biological importance
of drug targets, the potential market size of a successful
new drug, and possible treatment side effects are
critical for risk management in drug development.
A comprehensive molecular epidemiology analysis
involving thousands of well-characterized human
tissues will thus provide vital information for strategic
decision-making. Tissue microarray (TMA) technology
is ideally suited for such projects. The simultaneous
analysis of thousands of tissues enables highly standar-
dized, fast and affordable translational research studies
of unprecedented scale.
*Corresponding author: (G. Sauter) [email protected]
1740-6749/$ � 2004 Elsevier Ltd. All rights reserved. DOI: 10.1016/j.ddtec.2004.08.003
Section Editors:Wolfgang Fischer, Rob Hooft, Michael Walker
The analysis of human tissue is a key step in the identification of drug
targets. This analysis is usually done with individual tissues, focusing onthe investigation of individual genes. Often, however, this process is
time-consuming and can give controversial results. Tissue microarraysenable the analysis of a large number of small sample sections of tissue
simultaneously; thereby combining increased statistical accuracy andhigh throughput. In this review, the authors describe the benefits, the
proper handling to address-specific questions, and the limitations of thistechnique.
Introduction
A variety of powerful high-throughput technologies are avail-
able for the identification of potential new drug targets. At
the same time, high-throughput compound screening facil-
itates the identification of applicable drug substances. These
tools generally identify more potentially rewarding drug
targets than resources are available for their further develop-
ment. Thus, an efficient target prioritization strategy is cru-
cial for competitive drug development. Whereas target
identification is usually performed in experimental systems
like cell lines or animal models because of the almost unlim-
ited availability of resources, target evaluation and prioritiza-
tion should be optimally based on findings from patient
tissue specimens representing the disease the drug is devel-
oped against. In situ analyses methods are optimally suited for
target gene analyses as they allow a cellular and sub-cellular
localization of the gene product of interest. However, tradi-
tional slide-by-slide analysis cannot catch up with the speed
of modern high-throughput target identification technolo-
gies. Tissue microarrays (TMAs) permit a completely new
early evaluation strategy of drug targets. The simultaneous
and rapid analysis of thousands of human tissues allows
determination of the frequency of target gene expression,
for example, in all human tumor types, associations with
disease progression, and expression in normal tissues.
TMA technology
Hundreds of cylindrical samples measuring up to 4 mm
(usually 0.6 mm) in diameter are removed from formalin
fixed or frozen tissues and are deposited into one recipient
block [1]. Sections from such TMA blocks containing hun-
dreds of different tissues are then placed on a glass slide. All
methods for in situ tissue analysis, like immunohistochem-
istry (IHC), fluorescence in situ hybridization (FISH) and RNA
in situ hybridization, can be performed on TMAs using similar
protocols as for conventional large sections (Fig. 1).
After its initial description in 1998 [1], TMAs have become
widely used in recent years. More than 150 publications
www.drugdiscoverytoday.com 41

Drug Discovery Today: Technologies | Target identification Vol. 1, No. 1 2004
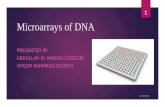
Figure 1. TMA manufacturing and applications. (a) Donor block from which several 0.6 mm tissue cores have been removed. Note that the original tissue
block remains fully interpretable. (b) Completed TMA. Removed tissue cores from several hundreds of different donor blocks have been assembled in the so-
called ‘recipient block’. (c) Hematoxilin and Eosin (H&E) stained tissue section of the TMA. (d) Higher magnification of a tissue spot analyzed by IHC. Brown
staining indicates high expression of membraneous HER2 receptor protein. (e) TMA sector analyzed by RNA in situ hybridization. This TMA was coated with a
photographic emulsion to detect the radioactively labeled antisense-RNA probe. (f) Magnification (630�) of a tissue spot analyzed by fluorescence in situ
hybridization (FISH). Green signals indicate centromere 7. Excess of red signals demonstrates EGFR gene amplification. Cell nuclei are counterstained with
blue fluorescence.
published in 2003 have utilized TMAs (using ‘‘tissue micro-
array’’ and ‘‘2003’’ as search terms in Medline). Some of the
most powerful applications of TMAs for drug discovery and
development are described below.
TMAs for economical evaluation
Data onthe expression ofa given target gene areoften available
from the literature.However, examplesofgenes that have been
extensively analyzed suggest that such data might often have
little practical importance. For example, HER2, the target gene
for trastuzamab (Herceptin) has been analyzed in thousands of
publications. However, the data are highly controversial, with
published expression frequencies ranging from<10% to>90%
for many important tumor types (reviewed in [2]). For exam-
ple, published incidences for HER2 positivity in non-small cell
lung cancers range between 4% and 100%. High expression
rates reported in some studies might have contributed to the
costly decision to undertake large but disappointing clinical
trials with Herceptin in lung cancer patients [3]. One of these
studies was recently closed early because of an unexpected low
42 www.drugdiscoverytoday.com
number of HER2 positive cases and the lack of response
reported in other studies [4]. The paramount impact of experi-
mental parameters like antibody selection, IHC protocol, tis-
sue characteristics, and scoring criteria on the results of IHC
analyses greatly reduce the comparability of IHC data derived
from different groups.
TMAs containing samples from all different tumor types
make it now possible to analyze a gene of interest in a TMA
format under fully standardized conditions in one experi-
enced laboratory. For such epidemiology studies we used a set
of TMAs containing more than 3500 different samples from
more than 120 different tumor types and subtypes [2,5]. In
recent studies this set of TMAs was used to investigate target
genes for established drug targets like KIT/CD117 (Imatinib;
Glivec) [5], epidermal growth factor (EGFR) (Tarceva, Iressa,
Cetuximab, Erbitux) [2], or HER2 (trastuzamab; Herceptin).
These studies confirmed expression of these targets in a wide
variety of tumor entities. The example of successful applica-
tion of Glivec in KIT-positive gastrointestinal stroma tumors
(GIST) shows the potential clinical and economical impor-

Vol. 1, No. 1 2004 Drug Discovery Today: Technologies | Target identification
Table 1. Summary of studies investigating the prognostic role of BCL2 expression in breast cancer
Authors Year Number
of cases
Follow-up
(years)
Association with
overall survival
Silvestrini et al. [20] 1994 283 6 Yes
Joensuu et al. [16] 1994 174 5 Yes
Lipponen et al. [19] 1995 140 10 Yes
Hellemans et al. [15] 1995 124 7 No
Barbareschi et al. [23] 1996 178 5 n/a
Van Slooten et al. [21] 1996 202 4 n/a
Krajewski et al. [18] 1997 53 53 No
Kapranos et al. [17] 1997 90 10 n/a
Charpin et al. [14] 1998 82 10 No
Veronese et al. [22] 1998 98 5 Yes
All previous studies 1424 ?
TMA study (unpublished) 2221 10 Yes (P < 0.0001)
tance of also including less frequent tumor entities in early
epidemiological target gene evaluations [6].
A TMA study investigating a representative number of all
different tumor types results in a reliable ranking list of
positive tumor entities. In combination with the published
incidence rates of these tumor entities the total number of
annual new positive cases can be calculated either across all
tumor types or for a specific tumor type [2]. These numbers
are useful for calculating the potential economical value of a
successful drug and also to select optimal tumor entities for
later clinical trials.
TMAs for biological evaluation
TMAs containing a large number of samples from one tumor
type with attached clinico-pathological information allow an
estimation of the biological importance of a drug target.
Associations with advanced stage, high grade, presence of
metastases, or poor clinical outcome argue for a role in tumor
progression. Potential drug targets with an association to
tumor progression, metastasis or poor prognosis might have
higher priority for further development than targets that are
unrelated to clinical outcome. The HER2 protein is a prime
example of a gene product strongly related to poor patient
prognosis in breast cancer and also constitutes an excellent
therapeutic target [7]. TMAs are highly efficient for identify-
ing associations between molecular features and prognosis.
For example, significant associations were found between
estrogen or progesterone expression [8] or HER-2 alterations
[9] and survival in breast cancer patients, between vimentin
expression and prognosis in kidney cancer [10], and between
Ki67 labeling index and prognosis in urinary bladder cancer
[11], soft tissue sarcoma [12], and in Hurthle cell carcinoma
[13]. The example of Bcl2 in breast cancer demonstrates the
importance of using large enough TMAs for such studies. Ten
studies had previously analyzed the relationship between loss
of Bcl-2 expression and prognosis in breast cancer. The results
were controversial with four studies finding a significant
association with poor prognosis, and six studies failing to
see such an association [14–23]. Using a TMA containing
more than 2000 breast cancers with clinical follow up data
we analyzed 50% more tumors than in all previous studies
together (Table 1). Our result of a strong association between
loss of Bcl-2 expression and poor prognosis provides strong
proof of the prognostic importance of Bcl-2 analysis in breast
cancer (Fig. 2a). A study analyzing ‘‘only’’ 200–300 tumors
would have been yet another study without the potential to
clarify the issue. The evaluation of potential clinico-patho-
logical associations can be facilitated by software solutions
that help to systematically evaluate different cutoff levels
(Fig. 2b). The comparison of the expression of a target gene
with previously collected molecular data can also provide
further information on the biologic role of target genes.
TMAs for toxicity evaluation
High expression of a target protein in vital normal tissues is a
possible drawback during drug development. The early use of
normal tissue TMAs avoids such unpleasant surprises. A cell
type-specific in situ expression analysis enables comparison of
the expression level for each individual cell type with the
expression in cancer cells, allowing the identification of
possible therapeutic windows. Cell type-specific comparisons
would not be possible if non-in situ methods were used. For
example, EpCam, a target for several anticancer therapies, is
expressed in bile ducts of the liver. Because bile ducts con-
stitute a very small (<1%) component of the liver, compar-
isons of the expression level in normal liver and tumors
would suggest a comfortable therapeutic window for anti-
EpCam drugs (Fig. 3). The in situ analysis of tissues does
reveal, however, the high level of expression in a small but
vital normal liver compartment. TMAs composed of normal
tissues can massively facilitate the process of normal
tissue cross reactivity testing. For example, frozen tissue
www.drugdiscoverytoday.com 43

Drug Discovery Today: Technologies | Target identification Vol. 1, No. 1 2004
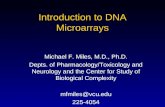
Figure 2. (a) Prognostic value of BCL2 in breast cancer. Analysis of 2221 breast cancer samples revealed that weak or lost expression of the anti-apoptotic
protein BCL2 is associated with poor patient survival. Numbers do not add up to 2221, because survival was calculated from the subset of ductal breast
cancers. (b) ThresholdFinderTM (TF) software. Following TMA analysis, TF software can be used to select and simultaneously link thresholds for staining
intensity groups to patient’s outcome and other parameters – panels in the right of the image show associations between expression levels and other
pathological parameters like nodal stage (pn) or tumor stage (pt). The example shows the prognostic influence of estrogene receptor (ER) staining in breast
cancer. Patients with strong (red line) or moderate (orange line) ER expression had a significantly better prognosis than patients with weak or no ER positivity.
The thresholds for these four groups can be modified with the sliders at the bottom of the screen.
TMAs composed of 32 tissues from multiple different donors
reflecting the panel of tissues required by the US Food and
Drug Administration (FDA) for cross-reactivity testing (CRT)
of new biological drugs are used for normal tissue analysis in
our laboratory (Fig. 4). This frozen TMA platform allows for
rapidly executing CRT studies on 4–5 TMA sections. The TMA
format especially facilitates the use of multiple different anti-
body dilutions as recommended by authorities.
Technical issues
The value of TMAs for large-scale tissue analysis is undisputed.
Although the technology is simple and easily applicable, some
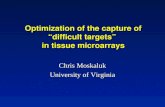
Figure 3. EpCam expression in normal liver. (a) Overview. (b) Magnification.
intensity, however, can also be seen in cancer cells. This emphasizes the importa
tissue for such an expression comparison (like northern or western blots) wo
44 www.drugdiscoverytoday.com
aspects of the TMA area are controversially discussed, whereas
others are underestimated. These include the importance of
tissue heterogeneity, the potential for automation, and the
importance ofpathology expertise.Understanding these issues
is critical for successfully using TMAs.
Tissue heterogeneity
Initially, it was feared that minute tissue samples (diameter
0.6 mm) might not be sufficiently representative of whole
tumors. Many studies have therefore addressed the question
as to whether a higher concordance of TMA and large
section data can be obtained if multiple samples of each
EpCam expression is confined to small areas of bile ducts. A similar staining
nce of in situ analyses for normal tissue evaluation. The use of disaggregated
uld suggest a negligible low expression level in normal liver.

Vol. 1, No. 1 2004 Drug Discovery Today: Technologies | Target identification
Figure 4. Cross reactivity testing (CRT) TMA. (a) Overview of the first of three TMA slides covering the FDA recommended panel of normal tissues for
cross-reactivity testing. (b) Schematic representation of the TMA showing the localization of each tissue type. Samples of every tissue type have been included
from many different patients, according to FDA recommendations.
tumor are arrayed. As expected, these studies show that the
results obtained on TMAs approach large section results as
more samples are being analyzed [10,11,24–37]. However,
after analyzing several million tumor samples on TMAs, we
feel that one tissue sample per tumor is not only the least
expensive but also the scientifically optimal procedure for
research applications of TMAs. The reasons for this are
explained below (Table 2).
Costs
The use of multiple samples increases the costs of a study.
The costs for tissue engineering and the interpretation of
each staining must by multiplied with the number of
samples per tumor. Investing in a higher number of tumors
thus is much more efficient than analyzing more samples
per tumor.
Table 2. Disadvantages of using multiple samples per tumor
Breast cancer study
(p53 IHC analysis)
200 patients
(four samples per tumor)
Tissue analyses 800
Interpretable cases 194
Time for reading (h) 8
Statistical bias issue Yes
Tissue costs ($) 3000
Pathologist costs ($) 2000
P value prognosis P = 0.0545
Rate of positivity (%) 23.7
IHC, immunohistochemistry.
Statistical bias
Not all arrayed tissues contain interpretable tumor
cells. Having multiple samples per tumor on a TMA will thus
always cause a variable number of interpretable tissue
samples per tumor ranging between 1 and the maximal
number of arrayed samples per tumor. The analysis of three
to five times more tissue for some tumors than for other
tumors introduces statistical problems [38]. At least this
issue must be considered and compensated by statistical
means.
Representativity of large sections
Large sections are gold standard for molecular in situ
tests. However, large sections contain only a small fraction
(<1/10,000) of the entire tumor mass [2]. Because the repre-
sentativity of large sections is therefore questionable by itself,
800 patients
(one sample per tumor)
800 patients
(four samples per tumor)
800 3200
606 774
8 32
No Yes
3000 12000
2000 8000
P < 0.0001 P < 0.0001
18.2 20.4
www.drugdiscoverytoday.com 45

Drug Discovery Today: Technologies | Target identification Vol. 1, No. 1 2004
reproducing the findings of large sections is not an optimal
endpoint for validating the TMA method. By contrast, study-
ing associations of TMA results with clinico-pathological
endpoints are more informative. All previously well estab-
lished associations between molecular features and clinical
endpoints, such as the prognostic importance of ER, PR, p53
and HER2 expression in breast cancer [9,24], Ki67 labeling
index in bladder cancer [11], or vimentin expression in
kidney cancer [10] have been confirmed on TMAs using
one spot per tumor. We are unaware of studies where such
associations could be found on large sections but not on
TMAs made from the same tumors and analyzed by the same
laboratory. Remarkably, there is one study finding clinico-
pathological associations on TMAs but not on corresponding
large sections (see below).
Risk of false positive results
The more samples are placed on a TMA per tumor, the higher
the likelihood of obtaining similar results to those obtained
for large sections. Although this is desirable at first sight, one
must not forget that some of the positive results on large
sections can be ‘‘artificial’’. This issue is nicely demonstrated
by Torhorst et al. [24]. This study shows a strong association
between p53 immunostaining and breast cancer prognosis on
four different TMAs containing one arrayed sample from each
of 500 breast cancers but fails to find a similar association in
large sections despite a much higher rate of positivity [2,24].
Overall, the available data suggest that analyzing one
sample each of an as large as possible cohort of tumors is
the most efficient and economical use of TMAs. The high
level of standardization (all tissues on a single slide are
analyzed under absolutely identical conditions) and the
greater objectivity of the staining interpretation on a small
tissue spot are important factors that apparently compensate
for the conceptual disadvantage of the small size of tissues
analyzed (for review see [2]). The greatest advantage of taking
multiple samples per tumor is the higher fraction of tumors
with interpretable data. This has, however, little importance
if a sufficiently large number of individual tumors are avail-
able. Taking multiple samples per tumor might be justified in
cases where there are very small tumor sets. However, raising
the number of informative cases by 10–20% will unfortu-
nately not massively reduce the risk of non-conclusive study
results in such a scenario.
Pathology expertise and automation
Although TMA technology is often discussed in the context
of other array techniques like DNA or protein arrays, for
which array construction, analysis and data recording can
easily be automated; the TMA method is fundamentally
different. TMAs represent the ultimate miniaturization of
molecular pathology and share their inherent strengths
and limitations. The level of pathology expertise is therefore
46 www.drugdiscoverytoday.com
decisive for the success of TMA studies, whereas classical array
tools like automation are less relevant. Automated TMA
manufacturing lacks importance, because sufficiently large
ready-to-use ‘‘tissue libraries’’ are lacking. Selection and pre-
paration of appropriate tissues make up for 95% of the TMA
manufacturing process and cannot be automated. More than
20,000 different tissues have been arrayed in our laboratory
and manual TMA making was never perceived a bottleneck.
Classical pathology skills including classification of arrayed
tissues, experimental design, and staining interpretation are
critical for using TMAs. More than 100 studies can be based
on one TMA block. As the molecular data will be compared
with pathological information, the quality of this informa-
tion is of highest importance. A systematic review of all
tumors included in a TMA by a specialized pathologist is
recommended and should include a reclassification of all
tissues according to current classifications.
The difficulties related to the development of a reliable IHC
protocol are underestimated. Non-specific positivity is a fre-
quent problem and requires the use of multiple controls. A
significant fraction of antibodies cannot be optimized for use
on tissue sections. IHC staining results are greatly dependent
on antibody selection, antigen retrieval strategy, staining
protocol and on minor variables such as the section age.
For example, the use of three different antibodies for EGFR
resulted – after state of the art protocol development – in an
up to fivefold difference in the rate of positivity [2]. Using 6-
month-old TMA sections we found a significant decrease of
immunoreactivity for multiple antibodies [39].
Manual (visual) analysis of the TMA staining provides the
greatest level of reading precision and will remain the gold
standard for TMA staining interpretation. It is tempting to
consider automated TMA interpretation in the case of high-
throughput operations. The biggest difficulty for automated
IHC analysis is the selection of a representative tissue area.
This has been solved during the TMA manufacturing process.
Automated TMA imaging systems have great importance for
result documentation but – for most antibodies – they cannot
replace the pathologist for analysis. Technically, IHC staining
quantification is more objective than manual reading, espe-
cially if fluorescent labels are used [40]. However, reading
TMAs includes many components of classical pathology
analysis and goes way beyond pure staining quantification.
Pathologists can rapidly comprehend the full information
provided on a 0.6 mm tissue sample. This includes recogni-
tion of the stained cell types and subcellular compartments
and a reliable distinction of cancer cells from normal or
precancerous tissues. The pathologist will automatically
exclude all necrotic, crushed or damaged tissue elements.
Also he is probable to identify any unexpected staining
patterns. The greatest challenge for automated analysis is
suboptimal IHC, which cannot be avoided for most antibo-
dies at least in a fraction of samples.

Vol. 1, No. 1 2004 Drug Discovery Today: Technologies | Target identification
Table 3. Comparison of different means of tissue analysis
TMA Large section analysis Lysate array Western blot Northern blot Southern blot PCR
Cell type/compartment-specific analysis +++ +++ ��� ��� ��� ��� ���
DNA copy number analysis +++ +++ ��� ��� ��� ++ ++
RNA expression analysis (frozen tissue) ++ ++ ��� ��� +++ ��� +++
RNA expression analysis (Fo-fixed tissue) �� �� ��� ��� ��� ��� ++
Protein expression analysis +++ +++ +++ +++ ��� ��� ���
Detection of RNA splice variants ��� ��� ��� ��� +++ ��� ++
Detection of protein isoforms + + ++ +++ ��� ��� ���
Mutation analysis ��� ��� ��� ��� ��� ��� +++
Standardization of analysis ++++ �� ++++ + + + +++
Quantitative measurements + + ++ + + + +++
Automation of analysis + ��� +++ �� �� �� +++
Reagent economy +++ �� +++ + + + ��
Analysis speed +++ ��� +++ �� �� �� ++
TMA, tissue microarray; PCR, polymerase chain reaction, Fo, formalin; ++++, excellent; +++, very good; ++, good; +, possible; ��, limited; ���, not possible.
Attempts to improve automated TMA analysis are paral-
leled by an increased use of lysate arrays composed of protein
extracts from tumor tissues [41,42]. These are spotted on glass
slides in a DNA array-like manner and can be analyzed with
the same software used DNA arrays. If morphologic informa-
tion is not needed, lysate arrays might represent a better
option than complicated and expensive systems for auto-
mated TMA analysis.
Conclusions
TMAs allow a high-throughput analysis of large numbers of
well characterized tissues by in situ methods. As such, TMAs
allow a new dimension of molecular tissue analysis. Thou-
sands of normal and diseased tissues can be analyzed in one
project. However, TMAs are not a classical array method but
rather reflect the ultimate miniaturization of classical mole-
cular pathology. IHC and tissue expertise are thus critical
components for the successful use of TMAs. As compared to
other tissue analysis methods, TMAs combine the advan-
tage of preserved tissue morphology with the high speed of
true array methods (Table 3). TMA studies are ideally suited
to rapidly identify suitable indications and possible areas of
side effects of potential new drugs and at the same time
allow an early economical evaluation. Allocation of
resources for costly functional evaluations can then be
prioritized according to the results of the initial TMA
analysis.
References1 Kononen, J. et al. (1998) Tissue microarrays for high-throughput molecular
profiling of tumor specimens. Nat. Med. 4, 844–847
2 Sauter, G. et al. (2003) Tissue microarrays in drug discovery. Nat. Rev.
Drug Discov. 2, 962–972
3 Hirsch, F.R. and Langer, C.J. (2004) The role of HER2/neu expression and
trastuzumab in non-small cell lung cancer. Semin. Oncol. 31, 75–82
4 Lara, P.N. Jr. et al. (2004) Trastuzumab plus docetaxel in HER2/neu-
positive non-small-cell lung cancer: a California Cancer Consortium
screening and phase II trial. Clin. Lung Cancer 5, 231–236
5 Went, P., et al. Low immunohistochemical expression of KIT in malignant
tumors. J. Oncol. (in press)
6 Dagher, R. et al. (2002) Approval summary: imatinib mesylate in the
treatment of metastatic and/or unresectable malignant gastrointestinal
stromal tumors. Clin. Cancer Res. 8, 3034–3038
7 Pegram, M.D. et al. (1998) Phase II study of receptor-enhanced chemo-
sensitivity using recombinant humanized anti-p185HER2/neu monoclonal
antibody plus cisplatin in patients with HER2/neu-overexpressing meta-
static breast cancer refractory to chemotherapy treatment. J. Clin. Oncol.
16, 2659–2671
8 Torhorst, J. et al. (2001) Tissue microarrays for rapid linking of molecular
changes to clinical endpoints. Am. J. Pathol. 159, 2249–2256
9 Barlund, M. et al. (2000) Detecting activation of ribosomal protein S6
kinase by complementary DNA and tissue microarray analysis. J. Natl.
Cancer Inst. 92, 1252–1259
10 Moch, H. et al. (1999) High-throughput tissue microarray analysis to
evaluate genes uncovered by cDNA microarray screening in renal cell
carcinoma. Am. J. Pathol. 154, 981–986
11 Nocito, A. et al. (2001) Microarrays of bladder cancer tissue are highly
representative of proliferation index and histological grade. J. Pathol. 194,
349–357
12 Hoos, A. et al. (2001) High Ki-67 proliferative index predicts disease
specific survival in patients with high-risk soft tissue sarcomas. Cancer 92,
869–874
www.drugdiscoverytoday.com 47

Drug Discovery Today: Technologies | Target identification Vol. 1, No. 1 2004
13 Hoos, A. et al. (2002) Clinical significance of molecular expression profiles
of Hurthle cell tumors of the thyroid gland analyzed via tissue microarrays.
Am. J. Pathol. 160, 175–183
14 Charpin, C. et al. (1998) bcl-2 automated and quantitative immunocyto-
chemical assays in breast carcinomas: correlation with 10-year follow-up.
J. Clin. Oncol. 16, 2025–2031
15 Hellemans, P. et al. (1995) Prognostic value of bcl-2 expression in invasive
breast cancer. Br. J. Cancer 72, 354–360
16 Joensuu, H. et al. (1994) Bcl-2 protein expression and long-term survival in
breast cancer. Am. J. Pathol. 145, 1191–1198
17 Kapranos, N. et al. (1997) Prognostic significance of apoptosis related
proteins Bcl-2 and Bax in node-negative breast cancer patients. Anticancer
Res. 17, 2499–2505
18 Krajewski, S. et al. (1997) Analysis of Bax and Bcl-2 expression
in p53-immunopositive breast cancers. Clin. Cancer Res. 3, 199–
208
19 Lipponen, P. et al. (1995) Apoptosis suppressing protein bcl-2 is expressed
in well-differentiated breast carcinomas with favourable prognosis. J.
Pathol. 177, 49–55
20 Silvestrini, R. et al. (1994) The Bcl-2 protein: a prognostic indicator
strongly related to p53 protein in lymph node-negative breast cancer
patients. J. Natl. Cancer Inst. 86, 499–504
21 van Slooten, H.J. et al. (1996) Expression of Bcl-2 in node-negative breast
cancer is associated with various prognostic factors, but does not predict
response to one course of perioperative chemotherapy. Br. J. Cancer 74,
78–85
22 Veronese, S. et al. (1998) Bax immunohistochemical expression in
breast carcinoma: a study with long term follow-up. Int. J. Cancer 79,
13–18
23 Barbareschi, M. et al. (1996) Bcl-2 and p53 expression in node-negative
breast carcinoma: a study with long-term follow-up. Hum. Pathol. 27,
1149–1155
24 Torhorst, J. et al. (2001) Tissue microarrays for rapid linking of molecular
changes to clinical endpoints. Am. J. Pathol. 159, 2249–2256
25 Hoos, A. et al. (2001) Validation of tissue microarrays for immunohisto-
chemical profiling of cancer specimens using the example of human
fibroblastic tumors. Am. J. Pathol. 158, 1245–1251
26 Mucci, N.R. et al. (2000) Neuroendocrine expression in metastatic prostate
cancer: evaluation of high throughput tissue microarrays to detect hetero-
geneous protein expression. Hum. Pathol. 31, 406–414
27 Rubin, M.A. et al. (2002) Tissue microarray sampling strategy for prostate
cancer biomarker analysis. Am. J. Surg. Pathol. 26, 312–319
48 www.drugdiscoverytoday.com
28 Sallinen, S.L. et al. (2000) Identification of differentially expressed genes
in human gliomas by DNA microarray and tissue chip techniques. Cancer
Res. 60, 6617–6622
29 Engellau, J. et al. (2001) Tissue microarray technique in soft tissue
sarcoma: immunohistochemical Ki-67 expression in malignant fibrous
histiocytoma. Appl. Immunohistochem. Mol. Morphol. 9, 358–363
30 Hedvat, C.V. et al. (2002) Application of tissue microarray technology to
the study of non-Hodgkin’s and Hodgkin’s lymphoma. Hum. Pathol. 33,
968–974
31 Camp, R.L. et al. (2000) Validation of tissue microarray technology in
breast carcinoma. Lab. Invest. 80, 1943–1949
32 Fernebro, E. et al. (2002) Evaluation of the tissue microarray technique for
immunohistochemical analysis in rectal cancer. Arch. Pathol. Lab. Med.
126, 702–705
33 Ginestier, C. et al. (2002) Distinct and complementary information pro-
vided by use of tissue and DNA microarrays in the study of breast tumor
markers. Am. J. Pathol. 161, 1223–1233
34 Rassidakis, G.Z. et al. (2002) Apoptotic rate in peripheral T-cell lympho-
mas. A study using a tissue microarray with validation on full tissue
sections. Am. J. Clin. Pathol. 118, 328–334
35 Yosepovich, A. and Kopolovic, J. (2002) Tissue microarray technology – a
new and powerful tool for the molecular profiling of tumors. Harefuah 141,
1039–1041
36 Hendriks, Y. et al. (2003) Conventional and tissue microarray immuno-
histochemical expression analysis of mismatch repair in hereditary color-
ectal tumors. Am. J. Pathol. 162, 469–477
37 Tzankov, A. et al. (2003) High-throughput tissue microarray analysis of
G1-cyclin alterations in classical Hodgkin’s lymphoma indicates over-
expression of cyclin E1. J. Pathol. 199, 201–207
38 Simon, R. et al. (2001) Patterns of her-2/neu amplification and over-
expression in primary and metastatic breast cancer. J. Natl. Cancer Inst. 93,
1141–1146
39 Mirlacher, M., et al. Influence of slide aging on results of translational
research studies using immunohistochemistry. Mod. Pathol. (in press)
40 Camp, R.L. et al. (2002) Automated subcellular localization and quantifica-
tion of protein expression in tissue microarrays. Nat. Med. 8, 1323–1327
41 Nath, N. and Chilkoti, A. (2003) Fabrication of a reversible protein array
directly from cell lysate using a stimuli-responsive polypeptide. Anal.
Chem. 75, 709–715
42 Nishizuka, S. et al. (2003) Proteomic profiling of the NCI-60 cancer cell
lines using new high-density reverse-phase lysate microarrays. Proc. Natl.
Acad. Sci. USA 100, 14229–14234