
Thesis_Wave Based Modelling Methods for Steady State Vibro Accoustics
Upload
ralph-fitzgeraldCategory
view
216download
0
Tissue Fluorescence Spectroscopy
Lecture 16

Outline• Steady-state fluorescence
– Instrumentation and Data Analysis Methods• Statistical methods: Principal components analysis• Empirical methods: Ratio imaging• Modeling: Quantitative extraction of biochemical info
– Fluorescence in disease diagnostics– Fluorescence in disease therapeutics


Fluorescence spectra provide a rich source of information on
tissue state
-1
-0.5
0
0.5
1
1.5
350 400 450 500 550 600300
350
400
450
Emission (nm)
Exc
itatio
n (
nm)
NADH
FAD
Collagen
Trp
Protein expression
Structural integrity
Metabolic activity
Courtesy of Nimmi Ramanujam, University of Wisconsin, Madison

Development of cancer involves a series of changes some of which can be probed by fluorescence
•protein expression (Trp)•metabolic activity (NADH/FAD)•nuclear morphology
•organization•structural integrity (collagen)•angiogenesis

Instrumentation for clinical tissue fluorescence measurements can be very simple, compact and
relatively cheap
Courtesy of Urs Utzinger, University of Arizona
Light Source
CCD
Control
ImagingSpectrograph
Optical fiber probe

Consistent autofluorescence differences have been detected between normal, pre-
cancerous and cancerous spectra
300 400 500 600 700
0.0
0.2
0.4
0.6
0.8
1.0
Non-dysplastic Barrett’s esophagus Low-grade dysplasiaHigh-grade dysplasia
Wavelength (nm)
Nor
mal
ized
fluo
res c
enc e
inte
nsi ty
Promising studies in•GI tract•Cervix•Lung•Oral cavity•Breast•Artery•Bladder

Methods of data analysis
• Main goal for fluorescence diagnostics: Identify fluorescence features that can be used to identify/classify tissue as normal or diseased.
• Main approaches– Statistical– Empirical – Model Based

Data analysis: Empirical and statistical algorithms
Data pre-processing
Normalization
Data reductionand
Feature extraction
Principal ComponentAnalysis Ratio methods
Classification

Detection of cervical pre-cancerous lesions using
fluorescence spectroscopy: Principal components analysis
Rebecca Richards Kortum group UT Austin
Detection of cervical pre-cancerous lesions
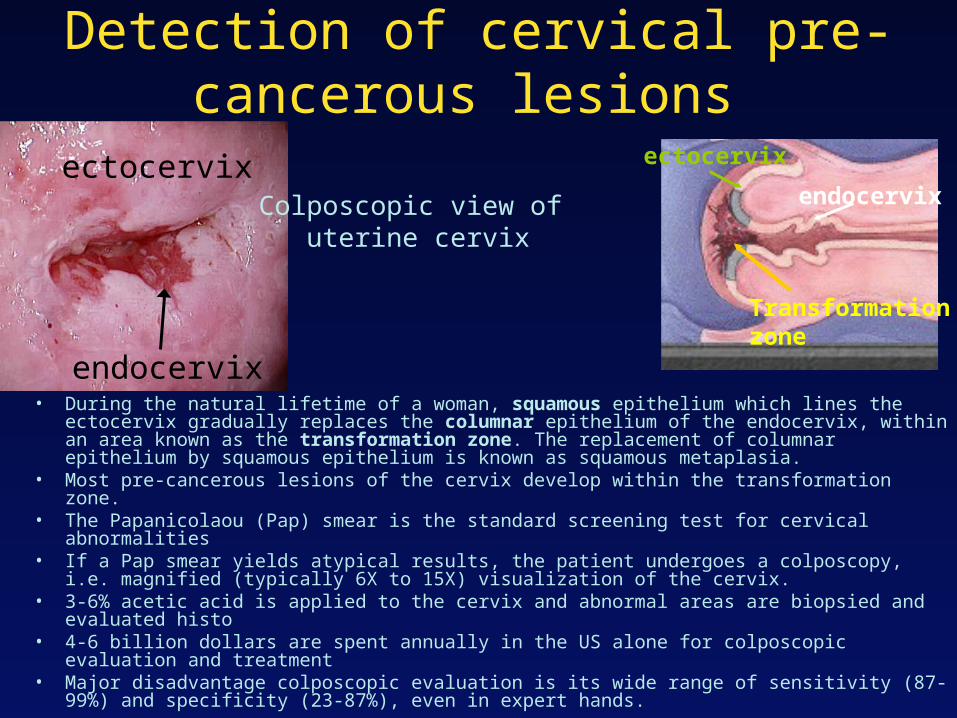
• During the natural lifetime of a woman, squamous epithelium which lines the ectocervix gradually replaces the columnar epithelium of the endocervix, within an area known as the transformation zone. The replacement of columnar epithelium by squamous epithelium is known as squamous metaplasia.
• Most pre-cancerous lesions of the cervix develop within the transformation zone.• The Papanicolaou (Pap) smear is the standard screening test for cervical abnormalities• If a Pap smear yields atypical results, the patient undergoes a colposcopy, i.e. magnified
(typically 6X to 15X) visualization of the cervix.• 3-6% acetic acid is applied to the cervix and abnormal areas are biopsied and evaluated
histo• 4-6 billion dollars are spent annually in the US alone for colposcopic evaluation and treatment• Major disadvantage colposcopic evaluation is its wide range of sensitivity (87-99%) and
specificity (23-87%), even in expert hands.
endocervix
ectocervix
Transformation zone
Colposcopic view of uterine cervix
ectocervix
endocervix

Major tissue histopathological classifications
• Normal squamous epithelium• Squamous metaplasia• Low-grade squamous intraepithelial lesion• High-grade squamous intraepithelial lesion• Carcinoma

Instrumentation
Nitrogen Pumped Dye
Laser
Nitrogen Pumped Dye
Laser
337 nm
380 nm
460 nm
PolychromatorIntensifiedDiode Array
Gate Pulser Controller Computer
collection fibers
excitation fibers
excitation fiberscollection fibers quartz
shield
Spectral Resolution: 10 nm
30 Hz rep rate5 ns pulse duration
probe

PRE-PROCESSING
Normalized Spectra at Three Excitation Wavelengths
Normalized, Mean-scaled Spectra at Three Excitation Wavelengths
DIMENSION REDUCTION: PRINCIPAL COMPONENT ANALYSIS
CLASSIFICATION: LOGISTIC DISCRIMINATION
Posterior Probability of being NS or SIL
Posterior Probability of being LG or HG
Posterior Probability of being NC or SIL
Posterior Probability of being SIL or NON SIL
Posterior Probability of being HG SIL or NON HG SIL
DEVELOPMENT OF COMPOSITE ALGORITHMS
Constituent Algorithm 1 Constituent Algorithm 3 Constituent Algorithm 2
(1,2) (1,2,3)
SELECTION OF DIAGNOSTIC PRINCIPAL COMPONENTS: T-TEST
Composite Screening Algorithm Composite Diagnostic Algorithm
337 nm Excitation 380 nm Excitation 460 nm Excitation
0
0.1
0.2
0.3
0.4
0.5
350 400 450 500 550 600 650
Wavelength (nm)
Flu
ores
cenc
e In
tens
ity
NS
NC
LGHG
0
0.1
0.2
0.3
400 450 500 550 600 650
Wavelength (nm)
Flu
ores
cenc
e In
tens
ity
NS
NCHG
LG
0
0.1
0.2
0.3
460 510 560 610 660
Wavelength (nm)
Fluo
resc
ence
Inte
nsity
NS
NCLG
Courtesy of N. Ramanujam; Photochem. Photobiol. 64: 720-735, 1996

00.10.20.30.40.5
350 450 550 650
Wavelength (nm)F
luo
resc
ence
In
ten
sity
(c
.u.)
00.20.40.60.8
11.2
350 450 550 650
Wavelength (nm)
No
rmali
zed
Flu
ore
scen
ce I
nte
nsit
y
(c.u
.)
-0.4-0.2
00.20.4
350 450 550 650
Wavelength (nm)
Nor
mal
ized
, m
ean-
scal
ed
Flu
ores
cenc
e
Data
Pre-ProcessingStep 1
Pre-ProcessingStep 2
Normal squamousLow-gradeHigh-gradeNormal columnar

Principal Component Analysis
Spectrum= wi*Bi
w=component weightB=component loading describing data variance
00.20.40.60.8
11.2
350 450 550 650
Wavelength (nm)
No
rmali
zed
Flu
ore
scen
ce I
nte
nsi
ty
(c.u
.)
spectra Component loadings

Dimension reduction: Principal Component Analysis
00.20.40.60.8
11.2
350 450 550 650
Wavelength (nm)
No
rmali
zed
Flu
ore
scen
ce I
nte
nsit
y
(c.u
.)
0
0.2
0.4
0.6
0.8
1
1.2
400 500 600
Wavelength (nm)
No
rm
alized
F
lu
orescen
ce
In
ten
sity
(c.u
.)
0
0.2
0.4
0.6
0.8
1
460 560 660
Wavelength (nm)
Norm
ali
zed F
luo
rescence
Inte
nsit
y (
c.u
.)
Component loadingsspectra337 nm
380 nm
460 nm

PCA Step 2: Calculate probability of belonging to category based on component weights and classify
Sample Number
Post
erio
r Pr
obab
ilit
y of
SIL
0
0.25
0.5
0.75
1
0 50 100 150 200
Low Grade SIL
High Grade SIL
Normal Squamous
Sample Number
Post
erio
r Pr
obab
ilit
y of
SIL
0
0.25
0.5
0.75
1
80 100 120 140 160 180 200
Low Grade SIL
High Grade SIL
Normal Columnar
▲Low-grade SIL
●High-grade SIL
□Normal squamous
▲Low-grade SIL
●High-grade SIL
□Normal columnar□ Non-dysplastic Barrett’s esophagus
X Dysplatic Barrett’s esophagus
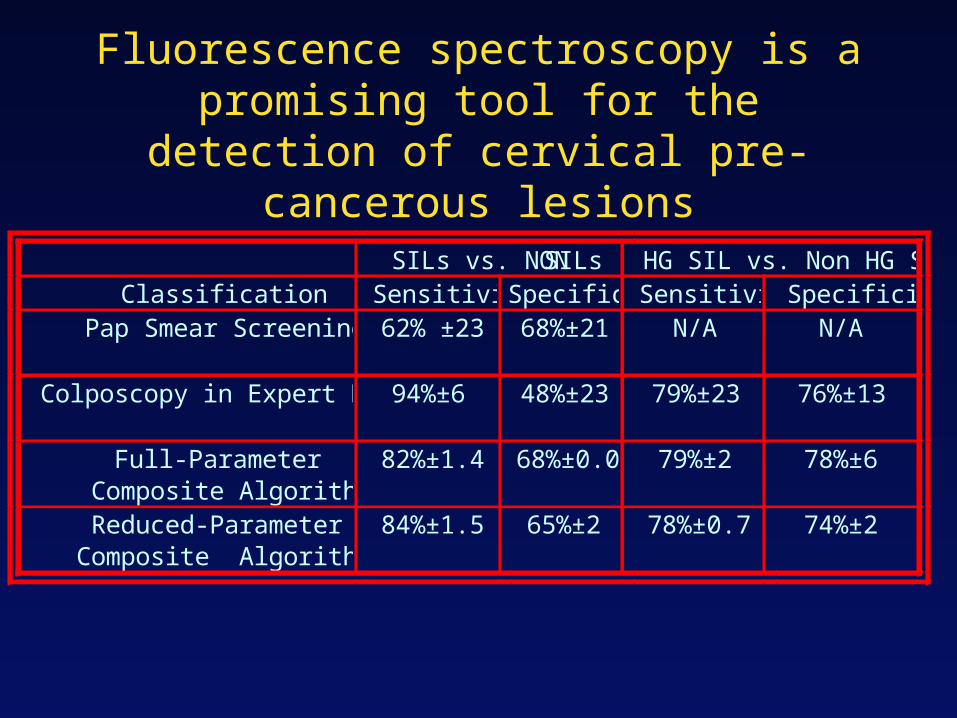
Fluorescence spectroscopy is a promising tool for the detection of cervical pre-
cancerous lesions
SILs vs. NON SILs HG SIL vs. Non HG SILClassification Sensitivity Specificity Sensitivity Specificity
Pap Smear Screening 62% ±23 68%±21 N/A N/A
Colposcopy in Expert Hands 94%±6 48%±23 79%±23 76%±13
Full-Parameter Composite Algorithm
82%±1.4 68%±0.0 79%±2 78%±6
Reduced-ParameterComposite Algorithm
84%±1.5 65%±2 78%±0.7 74%±2

Spectroscopic analysis using PCA
• Uses full spectrum information to optimize sensitivity and specificity
• Relatively easy to implement (automated software)
• Provides no intuition with regards to the origin of spectral differences

Spectroscopic imaging: fluorescence ratio methods for
detection of lung neoplasia
B. Palcic et al, Chest 99:742-3, 1991

LIFE schematic
B. Palcic et al, Chest 99:742-3, 1991

Detection of lung carcinoma in situ using the LIFE imaging
system
Courtesy of Xillix Technologies (www.xillix.com)
White light bronchoscopy Autofluorescence ratioimage
Carcinoma in situ

Autofluorescence enhances ability to localize small neoplastic lesions
Severe dysplasia/Worse Intraepithelial Neoplasia WLB WLB+LIFE WLB WLB+LIFE
Sensitivity 0.25 0.67 0.09 0.56
Positive predictive value
0.39 0.33 0.14 0.23
Negative predictive value
0.83 0.89 0.84 0.89
False positive rate 0.10 0.34 0.10 0.34
Relative sensitivity 2.71 6.3
S Lam et al. Chest 113: 696-702, 1998

Test DefinitionsHas disease Does not have
disease
Tests positive (A)
True positive
(B)
False positive
(A+B)
Total # who test positive
Tests negative (C)
False negative
(D)
True negative
(C+D)
Total # who test negative
(A+C)
Total # who have disease
(B+D)
Total # who do not have disease
Sensitivity=A/(A+C)Specificity=D/(B+D)
Positive predictive value=A/(A+B)Negative predictive value=D/(C+D)
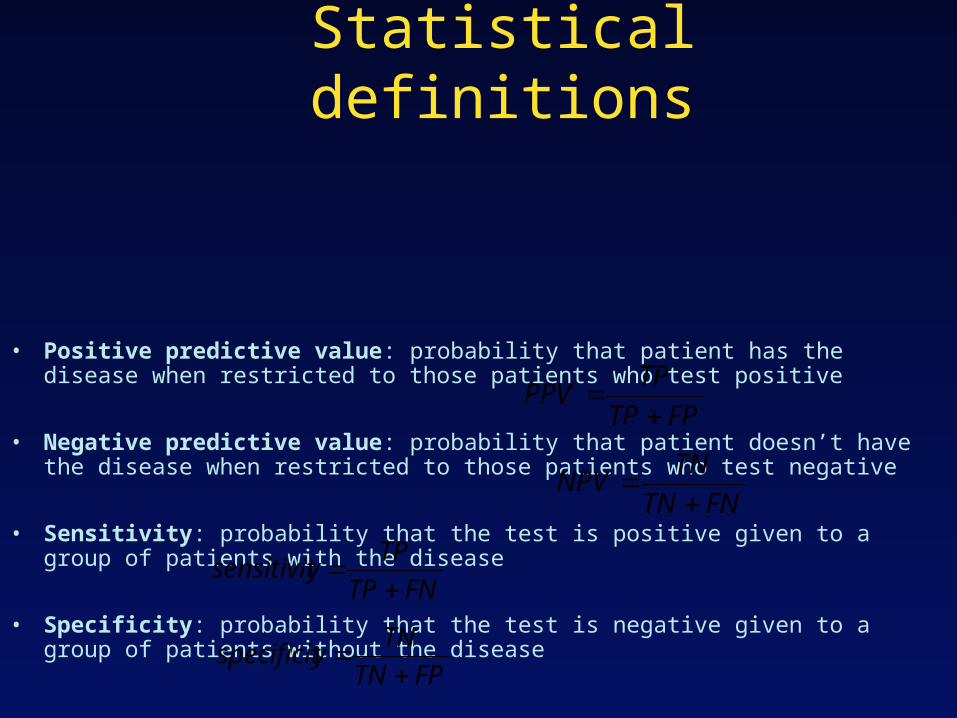
Statistical definitions
• Positive predictive value: probability that patient has the disease when restricted to those patients who test positive
• Negative predictive value: probability that patient doesn’t have the disease when restricted to those patients who test negative
• Sensitivity: probability that the test is positive given to a group of patients with the disease
• Specificity: probability that the test is negative given to a group of patients without the disease
FPTP
TPPPV
FNTN
TNNPV
FNTP
TPysensitivit
FPTN
TNyspecificit

Fluorescence imaging based on ratio methods
• Wide field of view (probably a huge advantage for most clinical settings)
• Eliminates effects of distance and angle of illumination
• Easy to implement• Provides no intuition with regards to
origins of spectral differences

What are the origins of the observed differences?
350 400 450 500 550 600 650 700 750
0.00
0.02
0.04
0.06
0.08
0.10
0.12
350 400 450 500 550 600 650 700 750
0.00
0.02
0.04
0.06
0.08
0.10
0.12
wavelength (nm)wavelength (nm)
Intr
insi
c fl
uo
resc
ence
Intr
insi
c fl
uo
resc
ence
337 nm excitation358 nm excitation381 nm excitation
397 nm excitation412 nm excitation425 nm excitation
Collagen NADH

Collagen and NADH spectra are sufficiently distinct only for some excitation
wavelengths
337 nm excitation 358 nm excitation

Tissue absorption and scattering may affect significantly tissue
fluorescence• scattering
– elastic scattering• multiple scattering
• absorption– Hemoglobin, beta carotene
• fluorescence
• single scattering
epithelium
Connective tissue

Is hemoglobin absorption a problem?
300 400 500 600 700 800
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
flu
ore
scen
ce
300 400 500 600 700 800
0.10
0.15
0.20
0.25
0.30
0.35
0.40
wavelength (nm)
refl
ecta
nce
337 nm excitation
wavelength (nm)
To get answer use
Monte Carlo simulations
Analytical Modeling


















