
Tissue engineering in heart and valve failure management.
28
Tissue engineering in heart and valve failure management Dr. Alexander Lyon Senior Lecturer and Consultant Cardiologist Royal Brompton Hospital and Imperial College, London
-
Upload
drucsamal -
Category
Healthcare
-
view
240 -
download
3
Transcript of Tissue engineering in heart and valve failure management.

Tissue engineering in heart and valve failure management
Dr. Alexander LyonSenior Lecturer and Consultant Cardiologist
Royal Brompton Hospital and Imperial College, London

Declaration of interest
• Nothing to declare

Overview
• Concepts for cardiovascular tissue engineering• Making a cardiac patch• Testing a cardiac patch in vivo• Heart valve engineering• Whole heart engineering• Clinical perspective


Fukushima, S. et al. Circulation 2007;115:2254-2261
Why do we need a patch in cell and tissue therapyRetention and Survival of grafted cells
Bone marrow cells - intramyocardial
Bone marrow cells - intracoronary
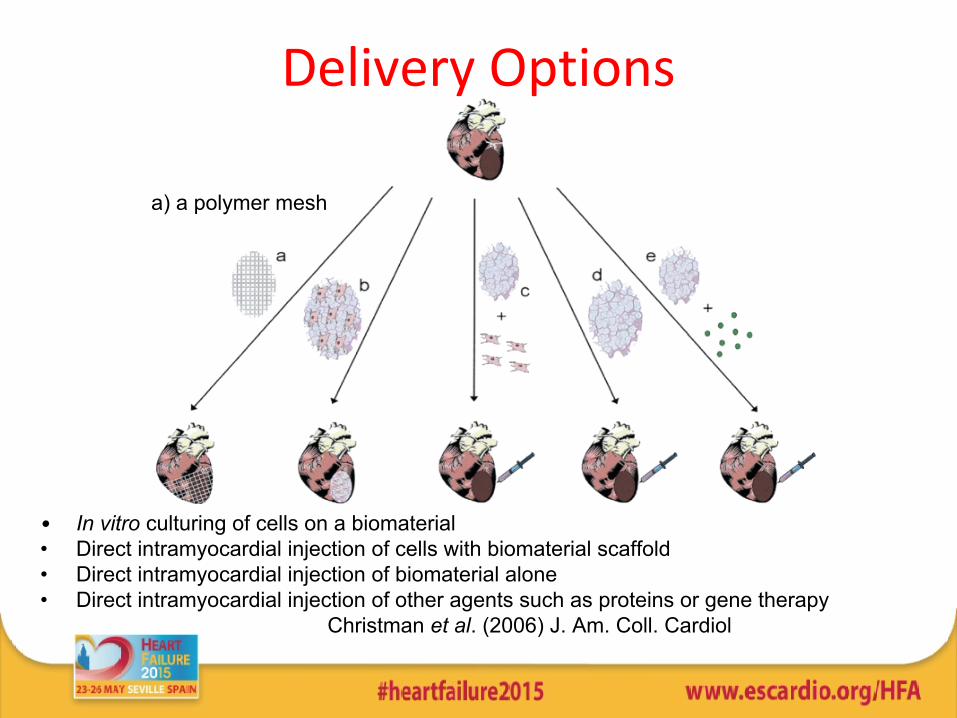
• In vitro culturing of cells on a biomaterial• Direct intramyocardial injection of cells with biomaterial scaffold• Direct intramyocardial injection of biomaterial alone• Direct intramyocardial injection of other agents such as proteins or gene therapy
Christman et al. (2006) J. Am. Coll. Cardiol
Delivery Options
a) a polymer mesh

Materials for myocardial scaffolds:ideal properties
• Mechanical properties matching host tissue
• Biocompatible
• Adherent
• Allow cell contraction/proliferation
• Vascularisation
• Biodegradable
• Non-toxic including degradation products

Materials to enhance cell attachment or survival
Material Advantages DisadvantagesNaturally occurring materials•Collagen•Alginate•Hyaluronic acid•Fibrin•Gelatin•Chitosan•Matrigel•Peritoneal membranes
BiocompatibilityPorousBiodegradableBioresorbable
Poor processibility
Poor mechanical properties
Possible immunogenic problems
Biodegradable synthetic polymers
•Poly(lactic acid)•Poly(ethylene terephthalate) = PED•Poly(glycerol sebacate) = PGS•Poly(lactic-co-glycolic acid)•Polypropylene fumarate•Poly(orthoesters)•Poly(anhydrides)
Good biocompatibilityOff-the-shelf availabilityGood processibility BioresorbableBiodegradable (wide range of rates)Added value from material tailoring• Controlled porosity• Mechanical support•Electrical conductivity•Controlled release of factors
Inflammation or nanotoxicity from degradation products
Loss of mechanical properties after degradation
Non-degradable synthetic polymers
Off-the-shelf availabilityNo foreign-body reactionsTailored mechanical properties
Effect of long term presence in the body

Biodegradable synthetic polymersPassive Stress-Strain Curves
Chen et al Biomaterials 2008 and 2010
(31)
(34)(30)
(33)(33)
(32)
E = 0.056 MPa
E = 0.22 MPa
PED/TiO2PGS@120C
PGS@110C
PED

Optimising engineered tissue properties
• Mechanical stimulation• Electrical stimulation• Physical patterning• Anti-apoptotic cocktail• Cell mix• Vascularisable scaffolds

Mechanical and electrical stimulation improveEngineered Heart Tissue maturation
Neonatal rat cardiomyocytes in collagenhuman embryonic stem cell-derived cardiomyocytes
T Eschenhagen, WH Zimmermann
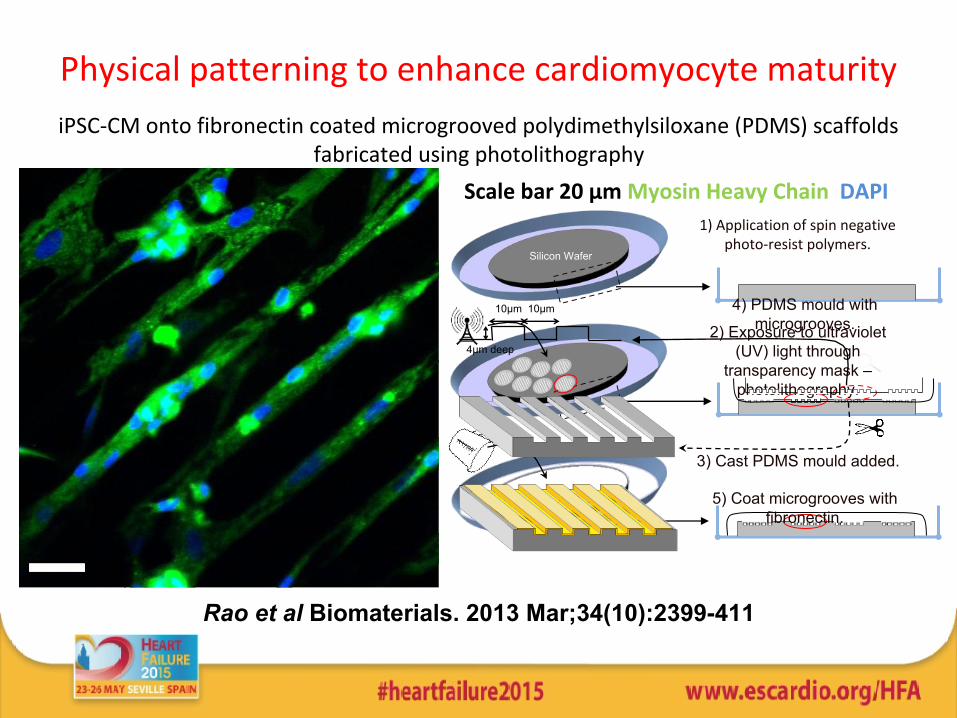
1) Application of spin negative photo-resist polymers.
3) Cast PDMS mould added.
2) Exposure to ultraviolet (UV) light through
transparency mask – photolithography.
Silicon Wafer
Scale bar 20 µm Myosin Heavy Chain DAPI
10µm 4) PDMS mould with microgrooves.
10µm
4µm deep
5) Coat microgrooves with fibronectin.
Physical patterning to enhance cardiomyocyte maturityiPSC-CM onto fibronectin coated microgrooved polydimethylsiloxane (PDMS) scaffolds
fabricated using photolithography
Rao et al Biomaterials. 2013 Mar;34(10):2399-411

Rao et al Biomaterials. 2013 Mar;34(10):2399-411
Physical patterning to enhance cardiomyocyte maturity

Physical patterning to enhance cardiomyocyte maturity
Rao et al Biomaterials. 2013 Mar;34(10):2399-411

In vivo testing in preclinical models1 cm diameter patch, 0.5mm thick, sutured onto left ventricle, 2 weeks
(N=6-8 per column)
Control SO ST Qizhi 0
50
100
Max Pressurens
nsns
mm
Hg
Untreated PED PED/TiO2 PGS0
2500
5000
7500
10000
12500
dp/dt maxns ns
ns
mm
Hg/
sec
Untreated PED PED/TiO2 PGS0.0
2.5
5.0
7.5
10.0
12.5
ns nsns
LVEDP
mm
Hg
Untreated PED PED/TiO2 PGS
0
25
50
75
100
ns nsns
LVEF
mm
Hg
Untreated PED PED/TiO2 PGS
Hikaru Ishii
No obvious impact of sutured patch on normal cardiac function

Ex vivo MRI of cardiac scaffolds
PED biopolymer PED + TiO2
Dan Stuckey

Hearts imaged in vivo at 1 and 6 weeksPGS scaffold degraded
In vivo myocardial scaffold degradation
Stuckey et al Tissue Engineering 2010

Scaffolds attached infarcted rat heart epicardium (n = 12)Hearts imaged in vivo at 1 week at 11.7T
In vivo detection of scaffold motion
PED + TiO2 PGS
Stuckey et al Tissue Engineering 2010

Tissue engineered trileaflet valve made ofB PGA/P4HB seeded with human cells
C PCL scaffold seeded with human cellsPoly e-caprolactone (PCL):
biocompatible and biodegradablestrong mechanical properties
slow degradation rate
Brugmans, M.M., et al., Journal of tissue engineering and regenerative medicine, 2013.
Collagen deposition (in red)
Heart Valve Engineering

easy to setup and handlehigh productivity
average fibre diameter: 300 – 1100 nmfibre diameter span: 100-700 nm to 100-2000 nm
Heart Valve Engineering at Imperial CollegeJet spraying to make Polymer nanofibres

Cells follow fibre orientation
Sohier J, Carubelli I, et al Biomaterials. 2014 Feb;35(6):1833-44
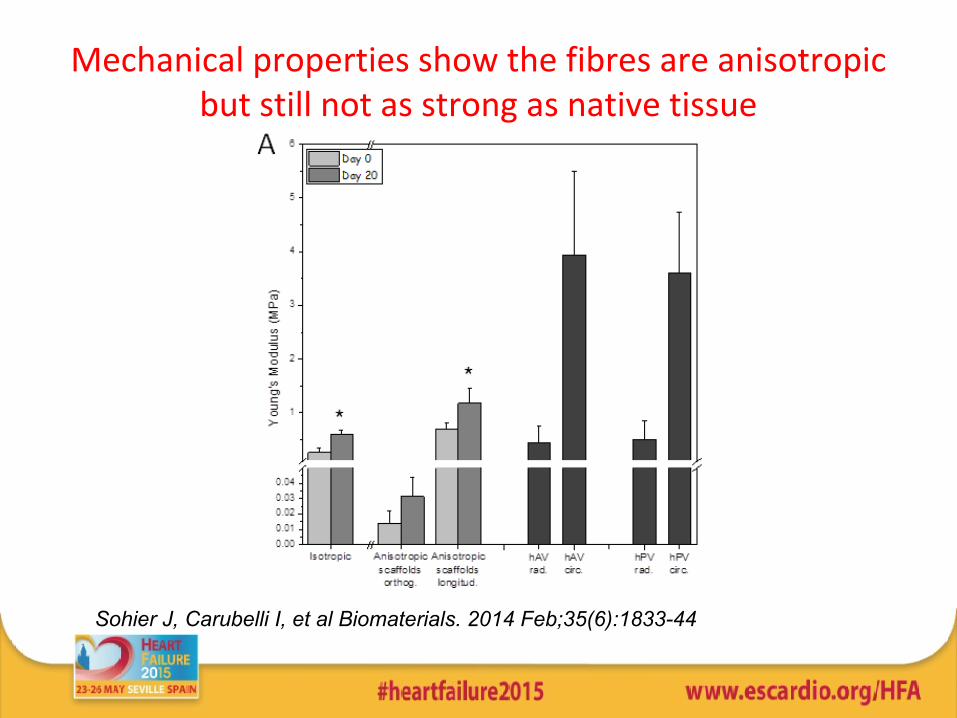
Mechanical properties show the fibres are anisotropic but still not as strong as native tissue
Sohier J, Carubelli I, et al Biomaterials. 2014 Feb;35(6):1833-44

3D Printing – Tissue Engineering
Murphy and Atala Nature Biotechnol. 2014 Aug;32(8):773-85.

Murphy and Atala Nature Biotechnol. 2014 Aug;32(8):773-85.
3D Printing – Tissue EngineeringScaffold biosynthesis

Can we build a whole heart?Decellularised rat heart repopulated with neonatal cardiomyocytes

Clinical PerspectiveMyocardial tissue engineering
• Clinical unmet need• Efficacy
– Who to enrol first? • LVAD patients• CABG + LV aneurysmectomy• Large Anterior MI
• How to measure efficacy?– Physical
• Durability• New myocardium• Electrically coupled
– Functional impact• Regional• Global
– Clinical• Symptoms• Exercise tolerance• Hard endpoints

Clinical PerspectiveMyocardial tissue engineering
• Safety– Arrhythmias– Perforation/rupture– Immunosuppression– Tumour– Adhesions

Acknowledgements
• Professor Sian Harding• Professor Cesare Terracciano• Dr. Dan Stuckey (CMR)• Dr. Hikaru Ishii (in vivo studies)• Dr. Ivan Carubelli
(Valve studies)• Dr. Adrain Chester
(Valve studies)


















