Tishk International University FACULTY OF DENTISTRY ...
38
Tishk International University FACULTY OF DENTISTRY Department Of Endodontics 3 rd Grade ENDO - 352 A TOPIC: INTRODUCTION TO ENDODONTICS Instructor: Dr. Niladri Maiti
Transcript of Tishk International University FACULTY OF DENTISTRY ...

Tishk International University FACULTY OF DENTISTRY
Department Of Endodontics
3rd Grade ENDO - 352 ATOPIC: INTRODUCTION TO ENDODONTICS
Instructor: Dr. Niladri Maiti

INTRODUCTION
TO ENDODONTICSDR. NILADRI MAITI
MDS(Conservative Dentistry & Endodontics), M.Sc (Laser Dentistry)
PhD(Dental Science)
Fellowship in Aesthetic Dentistry

DEFINITION
Endodontics is that branch of Dentistry concerned
with the morphology, physiology
and pathology of the dental pulp and the peri-
radicular tissues. The study and
practice of Endodontics encompasses the basic
clinical sciences including the biology of the
normal pulp, root and periradicular tissues. It also
includes the aetiology, prevention, diagnosis and
treatment of diseases and injuries that affect the
pulp and the peri-radicular tissues.
AUSTRALIAN SOCIETY OF ENDODONTOLOGY
DR. NILADRI MAITI

Necessity was the mother of invention: experimentingwith new techniques, materials, and instruments, eventhough very rudimentary, the aim of Endodontics hasbeen to relieve pain, treat exposed pulp, and preserveteeth

HISTORY
In 1687, Charles Allen,
describing the techniques of
dental transplants, wrote the
first English-language
book devoted exclusively to the
field of dentistry
DR. NILADRI MAITI

Pierre Fauchard (1678-1761), considered thefounder of modern dentistry, who in histextbook “Le chirurgien dentiste” preciselydescribed the dental pulp and dispelled thelegend of the “tooth worm,” which had beenconsidered the cause of caries and toothachessince the time of the Assyrians
DR. NILADRI MAITI

In 1725, Lazare Riviere introducedthe use of oil of cloves for itssedative properties.In 1746, Pierre Fauchard describedthe removal of pulp tissue.In 1820, Leonard Koeckercauterized exposed pulp with aheated instrument and protectedit with lead foil.

In 1836, Shearjashub Spoonerrecommended arsenic trioxide forpulp devitalization.In 1838, Edwin Maynard ofWashington, D.C. introduced thefirst root canal instrument, whichhe created by filing a watch spring.In 1847, Edwin Truman introducedgutta-percha as a filling material.
DR. NILADRI MAITI

Professor Wilhelm Conrad Roentgen on
November 8th, 1895 : – Discovery of X – RAYS
In 1900, Price described periapicalradiolucencies as “blind abscesses” and advised the use of radiography for establishing the diagnosis of pulplessteeth

1867, Magitot suggested the useof an electric current to test pulpvitality
In 1891, the German dentist OttoWalkhoff introduced the use ofcamphorated chlorophenol as amedication to sterilize root canals.
DR. NILADRI MAITI

In 1859, Albert Niemann refined the coca extract
to the pure alkaloid form and named this new drug
“cocaine.” Niemann recognized the anesthetic effect
of cocaine when he noted that “it benumbs the
nerves of the tongue
American surgeon William Halsted was the first
person to inject cocaine for nerve conduction blockade,
performing infraorbital and inferior alveolar nerve
blocks for dental procedures in November 1884.3
Halsted subsequently developed numerous other
regional nerve block injection techniques, many of
which are still fundamental to dental practice

Endodontic treatment dates all the way back to the
second or third century B.C. In 1985, archeologists
discovered evidence of early root canal surgery in
Israel’s Negev Desert. After examining the jaw of a 2000
year deceased Nabataen soldier, Joseph Zias, of Israel’s
national Department of Antiquities and Museums,
unearthed a one-tenth of an inch bronze wire, which had
been embedded in the nerve cavity of one of the skull’s
teeth. The location of the wire was in the exact spot
of infection, where modern root canal treatment
would be targeted. Apparently, the wire was used to
reduce infected tooth pulp, as the soldier suffered from
three abscesses and a cyst.
DR. NILADRI MAITI

FIELD OF ENDODONTICS
Clinical undergraduate endodontics
should encompass the following areas:
Diagnosis of pulp and periapical conditions.
Endodontic radiography.
Emergency treatment procedures - including
the relief of pain and management of
infections.
Pulp therapy - including dentine desensitisation
and protection; direct pulp capping; indirect pulp
capping; partial pulpotomy; pulpotomy; and
partial pulpectomy.
DR. NILADRI MAITI

Pulpectomy and associated endodontic
procedures - including consideration of:
Indications and contra-indications for
treatment
Diagnosis and management of orofacial
pain
Microbiological and immunological
aspects of endodontics
Materials and instruments
Instrumentation of root canals
Irrigation of root canals
Intra-canal medication
Root filling techniques.
DR. NILADRI MAITI

Treatment of pulpless teeth with or
without associated periapical pathosis.
The role and scope of periapical
surgery.
The management of traumatic injuries
to the teeth and mouth - including
crown
fractures, crown/root fractures, root
fractures, concussion, subluxations,
luxations,
avulsions, alveolar bone fractures,
abrasions, contusions and lacerations.
DR. NILADRI MAITI

Apexification and apexogenesis.
Management of combined
endodontic/periodontal lesions.
Recognition and treatment of resorptive
defects.
Bleaching of teeth.
Treatment of medically compromised
patients.
Assessment of treatment outcomes following
endodontic management of teeth.
Restoration of endodontically treated teeth.
Alternatives to endodontic therapy -
including the role of endodontics in preserving
bone for potential implant therapy
DR. NILADRI MAITI

ENDODONTICS -- YESTERDAY, TODAY & TOMORROW
Dr. Grossman, the pioneer of
endodontics, published an
excellent history of
endodontics in the July 1976
issue of JADA in which he
divides the evolution of the
science of endodontics over
four half centuries from 1776
to 1976.
DR. NILADRI MAITI

DENTAL PULP

MEAN VOLUME OF SINGLE ADULT HUMAN PULP : 0.02CC
TOTAL VOLUMES OF ALL PERMANENT TEETH
PULP ORGAN IS: 0.38CC
The dental pulp resides in a rigid chamber
comprising dentine, enamel and
cementum, which provide strong
mechanical support and protection from
the microbial rich oral environment
DR. NILADRI MAITI


An inflamed or injured pulp may have to be removedand replaced with a root filling – a procedure termedpulpectomy. This measure is undertaken especially incases when the condition of the pulp is such that aninflammatory breakdown is deemed imminent.

The objective of endodontic treatment
The consequences of inflammatory lesions in the pulp and periapical tissue have tormented humankind for thousands of years.
Historically, therefore, the main task of endodontic treatment has been to cure toothache due to inflammatory lesions in the pulp (pulpitis) and the periapical tissue (apical periodontitis).

The vital pulp
Under normal, physiological conditions the pulp is wellprotected from injury and injurious elements in the oralcavity by the outer hard tissue encasement of the tooth and an intact periodontium
When the integrity of these tissue barriers is breached for any reason, microorganisms and the substances they produce may gain access to the pulp and adversely affect its healthy condition. The most common microbial challenge of the pulp derives from caries.
DR. NILADRI MAITI
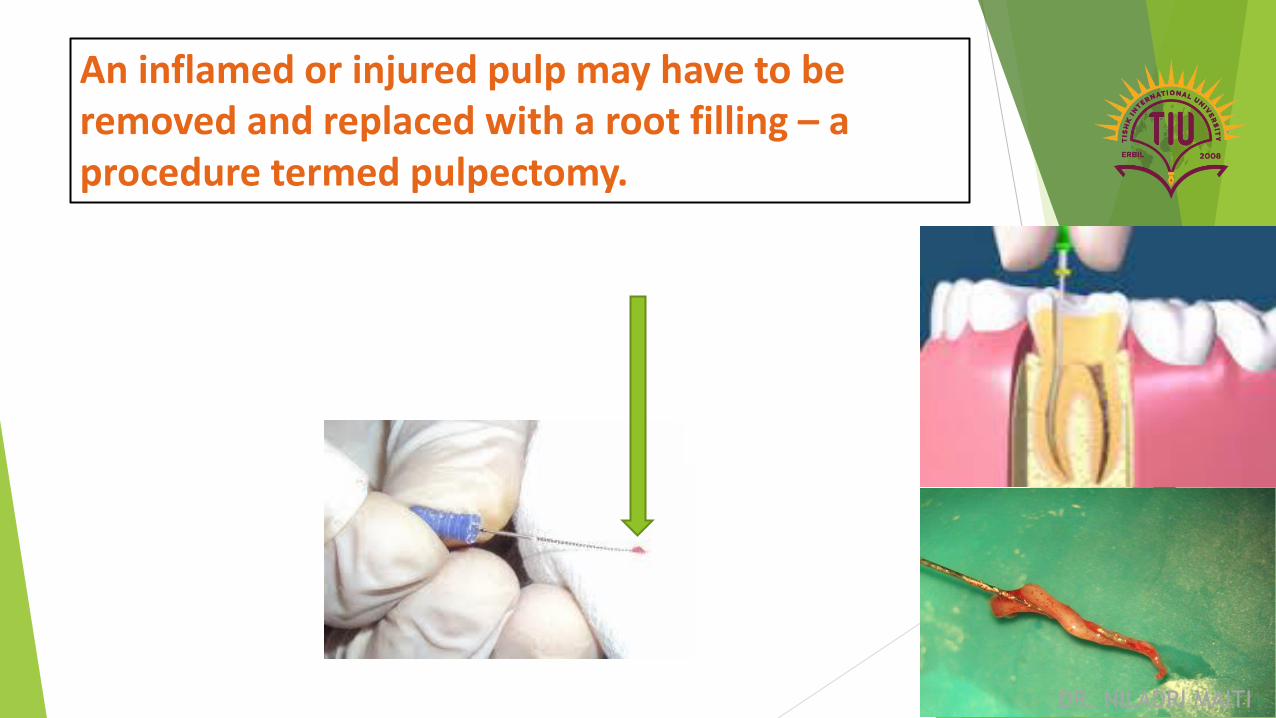
An inflamed or injured pulp may have to be removed and replaced with a root filling – a procedure termed pulpectomy.
DR. NILADRI MAITI

A pulpectomy procedure is carried out under localanesthesia and with the use of specially designed root canal instruments.
These instruments remove the diseased pulp and prepare the canal system so that it can be filled properly. The purpose of the filling is to preventmicrobial growth and multiplication in the pulpal chamber.

The necrotic pulp
As mentioned above, injury to the pulp may lead tonecrosis of the tissue . The necrotic pulp isdefenseless against microbial invasion and will allowmicroorganisms indigenous to the oral cavity to reachthe pulp chamber, either along an open direct exposureor through uncovered dentinal tubules or cracks in theenamel and dentin.

The specific environment in the root canal, characterized by the degrading pulp tissue and lack of oxygen, will favor a microbiota dominated by proteolytic, anaerobic bacteria. These microorganisms may organize themselves in clusters and in microbial communities attached to the root canal walls as well as inside the dentinal tubules of the root.

A chronic inflammatory lesion will ensue, normally aroundthe root tip, and remain for as long as no treatment isinitiated.

Response to deep caries
Once the carious lesion with its bacterial front has penetrated the primary dentin and progressed into reparative dentin and/or to the pulp tissue proper, a massive mobilization of the inflammatory defense will take place

A most conspicuous feature is the aggregation of neutrophils. Often a local abscess develops. Clinically, upon excavation of caries, a dropletof pus may sometimes appear at the exposure site.

Treatment of the necrotic pulp is by root canal treatment (RCT) and is aimed to combat the intracanal infection.The canal is cleaned with files in order to remove microbes as well as their growth substrate.

SCOPE OF ENDODONTICSThere has been massive growth in
endodontic treatment in recent years.
By the early 1960’s about 3 million
teeth were endodontically treated in
the United States annually.
In the early 1990’s, U.S. dentists were
treating 40 million cases per year, and currently the profession is performing over 50 million endodontic procedures
each year.
DR. NILADRI MAITI

The good news is: hundreds of millions of
teeth are salvaged through combinations of
endodontics, periodontics, and restorative
dentistry. The bad news is: if we treat 50
million
cases per year and if the failure rate is just
10%, then there would be 5 million treatment
failures per year.

Extrapolating over the past three
to four decades reveals that the
number of failing endodontically
treated teeth is massive, and
could approach tens of millions!

The most important innovations have been the utilization of the dental operating microscope, ultrasonic technologyand related instruments, nickel-titanium (NiTi) rotaryshaping files, and mineral trioxide aggregate (MTA) LASERS etc.

There are many advantages
for utilizing NiTi rotary
instruments for shaping root
canals. Traditionally, canal
preparations have been
performed using a series of
stainless steel files, oftentimes
in conjunction with gates
glidden drills or peeso
reamers
DR. NILADRI MAITI

Advantageously, NiTi rotary
shaping files have nearly
eliminated these iatrogenic
events.
Other important advantages of
shaping canals with NiTi files
are improved efficiency, the
opportunity to schedule more
“one visit” endodontic
procedures, and improved
profitability.
DR. NILADRI MAITI