
Thyrotoxicosis
57
Thyrotoxicosis Dr.P.Viswakumar M.S Assistant professor, Dept of General Surgery, PSGIMSR
-
Upload
viswa-kumar -
Category
Health & Medicine
-
view
155 -
download
2
Transcript of Thyrotoxicosis

Thyrotoxicosis
Dr.P.Viswakumar M.S
Assistant professor,
Dept of General Surgery,
PSGIMSR

Thyroid PhysiologyIodine Metabolism: • The average daily iodine requirement is 0.1 mg.• Sources : Fish, milk, and eggs or as additives in
bread or salt.• In the stomach and jejunum, iodine is rapidly
converted to iodide and absorbed into the bloodstream.
• Iodide is actively transported into the thyroid follicular cells by an adenosine triphosphate (ATP)–dependent process.
• The thyroid is the storage site of >90% of the body's iodine content

Thyroid Hormone synthesis
1) Iodide trapping, involves active (ATP-dependent) transport of iodide across the basement membrane of the thyrocyte via an intrinsic membrane protein, the sodium/iodine (Na+/I–) symporter.
2) Oxidation of iodide to iodine and iodination of tyrosine residues on Tg, to form monoiodotyrosines (MIT) and diiodotyrosines(DIT).
3) Coupling of two DIT molecules to form tetra-iodothyronine or thyroxine (T4 ), and one DIT molecule with one MIT molecule to form 3,5,3'-triiodothyronine (T3).

Thyroid Hormone synthesis
• Tg is hydrolyzed to release free iodothyronines(T3 and T4) and mono- and diiodotyrosines by stimulation of TSH and engulfing within thyroid follicle.
• The latter are deiodinated in the fifth step to yield iodide, which is reused in the thyrocyte.




• In the euthyroid state, T4 is produced and released entirely by the thyroid gland, whereas only 20% of the total T3 is produced by the thyroid.
• Most of the T3 is produced by peripheral deiodination (removal of 5'-iodine from the outer ring) of T4 in the liver, muscles, kidney, and anterior pituitary, a reaction that is catalyzed by 5'-mono-deiodinase.
• Thyroid hormones are transported in serum bound to carrier proteins such as T4-binding globulin, T4-binding prealbumin, and albumin.


• Only a small fraction (0.02%) of thyroid hormone (T3 and T4) is free (unbound) and is the physiologically active component.
• T3 is the more potent of the two thyroid hormones, although its circulating plasma level is much lower than that of T4.
• T3 is three to four times more active than T4 per unit weight, with a half-life of about 1 day, compared to approximately 7 days for T4.

Hypothalamic-pituitary-thyroid hormone axis

• The thyroid gland also is capable of autoregulation, which allows it to modify its function independent of TSH.
• As an adaptation to low iodide intake, the gland preferentially synthesizes T3 rather than T4 , thereby increasing the efficiency of secreted hormone.
• In situations of iodine excess, iodide transport, peroxide generation, and synthesis and secretion of thyroid hormones is inhibited.
• Excessively large doses of iodide may lead to initial increased organification, followed by suppression, a phenomenon called the Wolff-Chaikoff effect.
Thyroid Hormone Function• In humans, two types of T3 receptor genes (alpha
and beta) are located on chromosomes 3 and 17.
• Alpha form is abundant in the central nervous system, whereas the beta form predominates in the liver.
• Thyroid hormones affect almost every system in the body. They are important for fetal brain development and skeletal maturation.
• T3 increases oxygen consumption, basal metabolic rate, and heat production by stimulation of Na+/K+
ATPase in various tissues

Thyroid Hormone Function
• It also has positive inotropic and chronotropiceffects on the heart(actions of catecholaminesare amplified).
• They also increase GI motility, leading to diarrhea in hyperthyroidism and constipation in hypothyroidism.
• Thyroid hormones also increase bone and protein turnover and the speed of muscle contraction and relaxation.

Tests of Thyroid Function
Serum Thyroid-Stimulating Hormone (Normal 0.5–5 U/mL): Serum TSH levels reflect the ability of the anterior pituitary to detect free T4 levels. Small changes in free T4 lead to a large shift in TSH levels (Inverse relation).
Total T4 (Reference Range 55–150 nmol/L) and T3(Reference Range 1.5–3.5 nmol/L).
Free T4 (Reference Range 12–28 pmol/L) and Free T3(3–9 pmol/L).
Thyroid Antibodies : Thyroid antibodies include anti-Tg, antimicrosomal, or anti-TPO and thyroid-stimulating immunoglobulin (TSI).

Thyrotoxicosis
Hyperthyroidism
Thyrotoxicosis
• Biochemical and physiological manifestation of Excessive thyroid hormone.
• Thyrotoxicosis need not be due to hyperthyroidism
• But hyperthyroidism mostly produce thyrotoxicosis.

Hyperthyroidism
• It is a term reserved for disorder that result in over production of hormone by the thyroid gland.
• In short hyperthyroidism the pathology is in the thyroid gland itself

Hyperthyroidism and thyrotoxicosisNo Hyperthyroidism Toxicosis without
hyperthyroidism
1, Grave’s disease Subacute thyroiditis
2, Toxic nodular goitre Ectopic functioning thyroid
3, Toxic adenoma Silent thyroiditis
4, Jod – Basedow’sdisease
Struma ovarii
5, Metastatic follicular carcinoma
6, Trophoblastic tumours
7, Postpartum thyroiditis
8, Thyrotoxicosis factitia

Diffuse toxic goitre(Grave’s disease)
• This disorder is known as Graves' disease after Robert Graves, an Irish physician who described three patients in 1835.
• It is an autoimmune disease with a strong familial predisposition, female preponderance (5:1).
• Peak incidence between the ages of 40 to 60 years.
• Graves' disease is characterized by thyrotoxicosis, diffuse goiter, and extrathyroidal conditions including ophthalmopathy, dermopathy (pretibial myxedema), thyroid acropachy, gynecomastia, and other manifestations.

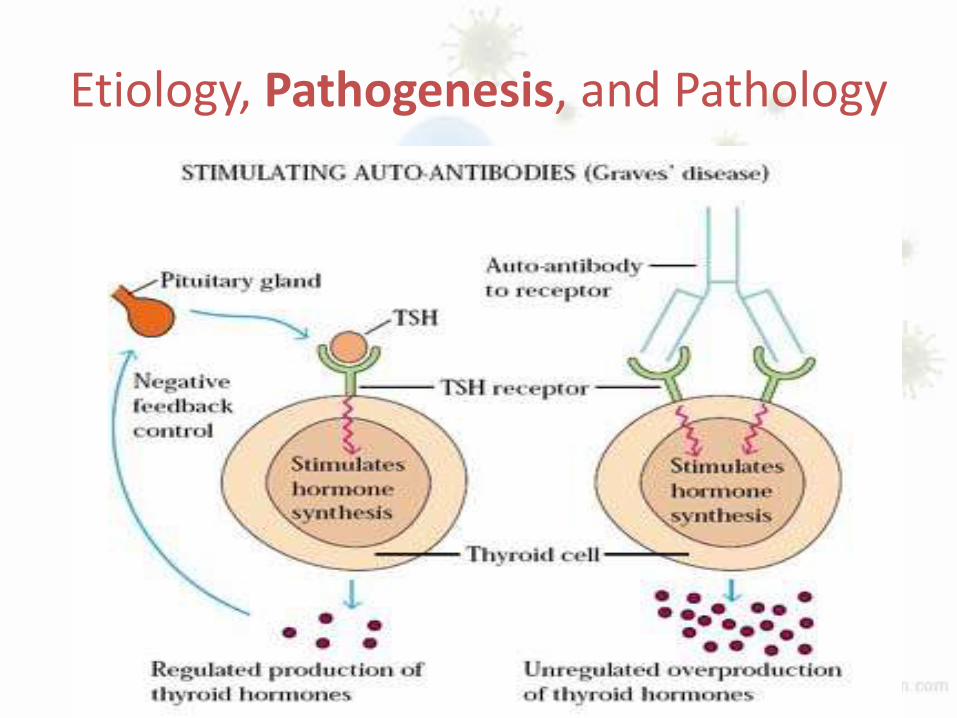
Etiology, Pathogenesis, and Pathology
• The exact etiology of the initiation of the autoimmune process in Graves' disease is not known.
• Postpartum state, iodine excess, lithium therapy, and bacterial and viral infections have been suggested as possible triggers.
• Genetic factors also play a role-HLA-B8 and HLA-DR3 and HLADQA1*0501.
Etiology, Pathogenesis, and Pathology
• Stimulate B lymphocytes, which produce antibodies directed against the thyroid hormone receptor.
• TSIs or antibodies that stimulate the TSH-R, as well as TSH-binding inhibiting immunoglobulins or antibodies have been described.
• The thyroid-stimulating antibodies stimulate the thyrocytes to grow and synthesize excess thyroid hormone, which is a hallmark of Graves' disease.
• Graves' disease also is associated with other autoimmune conditions such as type I diabetes mellitus, Addison's disease, pernicious anemia, and myasthenia gravis.
Etiology, Pathogenesis, and Pathology

Etiology, Pathogenesis, and Pathology
• Macroscopically, the thyroid gland in patients with Graves' disease is diffusely and smoothly enlarged, with a concomitant increase in vascularity.
• Microscopically, the gland is hyperplastic, and the epithelium is columnar with minimal colloid present.
• The nuclei exhibit mitosis, and papillary projections of hyperplastic epithelium are common.

Clinical manifestation
• Divided into those related to hyperthyroidism and those specific to Graves' disease.
• Hyperthyroid symptoms
-Heat intolerance
-Increased sweating and thirst
-Weight loss despite adequate caloric intake

Clinical manifestation
• Symptoms of increased adrenergic stimulation-palpitations, nervousness, fatigue, emotional lability, hyperkinesis, and tremors.
• The most common GI symptoms include increased frequency of bowel movements and diarrhea.
• Female patients often develop amenorrhea, decreased fertility, and an increased incidence of miscarriages.
• Children experience rapid growth with early bone maturation.
• Older patients may present with cardiovascular complications such as atrial fibrillation and congestive heart failure.

Other manifestation of Grave’s• Approximately 50% of patients with Graves'
disease also develop clinically evident ophthalmopathy, and dermopathy occurs in 1 to 2% of patients.
• Eye signs - lid lag (von Graefe's sign), spasm of the upper eyelid revealing the sclera above the corneoscleral limbus (Dalrymple's sign), and a prominent stare, due to catecholamine excess.
• True infiltrative eye disease results in periorbitaledema, conjunctival swelling and congestion (chemosis), proptosis, limitation of upward and lateral gaze (from involvement of the inferior and medial rectus muscles, respectively), keratitis, and even blindness due to optic nerve involvement.

• Rare bony involvement leads to subperiostealbone formation and swelling in the metacarpals (thyroid acropachy).
• Onycholysis, or separation of fingernails from their beds, is a more commonly observed finding.


Clinical signs• Weight loss and facial flushing may be evident.
• The skin is warm and moist and African American patients often note darkening of their skin.
• Tachycardia or atrial fibrillation is present with cutaneous vasodilation leading to a widening of the pulse pressure and a rapid falloff in the transmitted pulse wave (collapsing pulse).
• A fine tremor, muscle wasting, and proximal muscle group weakness with hyperactive tendon reflexes often are present.
• The thyroid usually is diffusely and symmetrically enlarged, as evidenced by an enlarged pyramidal lobe.
• Overlying bruit or thrill and loud venous hum in the supraclavicular space




Diagnostic Tests• Suppressed TSH with or without an elevated free T4 or
T3 level.• If eye signs are present, other tests are generally not
needed.• In the absence of eye findings, an 123I uptake and scan
should be performed. • An elevated uptake, with a diffusely enlarged gland,
confirms the diagnosis of Graves' disease • It helps to differentiate it from other causes of
hyperthyroidism.• Anti-Tg and anti-TPO antibodies are elevated in up to
75% of patients.• Elevated TSH-R or thyroid-stimulating antibodies (TSAb)
are diagnostic of Graves' disease and are increased in about 90% of patients
Management• Graves' disease may be treated by any of
three treatment modalities—
- Antithyroid drugs
- Thyroid ablation with radioactive 131I
- Thyroidectomy

Anti Thyroid Drugs
• Antithyroid medications generally are administered in preparation for RAI ablation or surgery.
• The drugs commonly used are propylthiouracil(PTU, 100 to 300 mg three times daily) and methimazole (10 to 30 mg three times daily, then once daily).
• Both drugs reduce thyroid hormone production by inhibiting the organic binding of iodine and the coupling of iodotyrosines (mediated by TPO).
• PTU also inhibits the peripheral conversion of T4 to T3, making it useful for the treatment of thyroid storm.
• PTU has a lower risk of transplacental transfer.

Anti Thyroid Drugs• Side effects of treatment include reversible
granulocytopenia, skin rashes, fever, peripheral neuritis, polyarteritis, vasculitis, and, rarely, agranulocytosis and aplastic anemia.
• The catecholamine response of thyrotoxicosis can be alleviated by administering beta-blocking agents.
• Propranolol is the most commonly prescribed medication in doses of about 20 to 40 mg four times daily.

Radioactive Iodine Therapy (131I)
Radioactive Iodine Therapy (131I)
• RAI forms the mainstay of Graves' disease treatment in North America.
• The major advantages of this treatment are the avoidance of a surgical procedure and its concomitant risks.
• The 131I dose is calculated after a preliminary scan, and usually consists of 8 to 12 mCi administered orally.
• After standard treatment with RAI, most patients become euthyroid within 2 months.
• However, only about 50% of patients treated with RAI are euthyroid 6 months after treatment, and the remaining are still hyperthyroid or already hypothyroid

Radioactive Iodine Therapy (131I)
• RAI therapy is therefore most often used in older patients with small or moderate-sized goiters, those who have relapsed after medical or surgical therapy.
• Contraindication :Absolute : Women who are pregnant or
breastfeeding.
Relative : Young patients (i.e., especially children and adolescents), those with thyroid nodules, and those withophthalmopathy.

Surgical Treatment
• Surgery is recommended when RAI is contraindicated
(a) Have confirmed cancer or suspicious thyroid nodules.
(b) Young.(c) Pregnant or desire to conceive soon
after treatment.(d) Severe reactions to antithyroid medications(e) Large goiters causing compressive
symptoms.(f) Reluctant to undergo RAI therapy.

Surgical Treatment
• What surgical Procedure ?
1) Near total thyroidectomy
2) Subtotal thyroidectomy
3) Total thyroidectomy
4) Hartley- Dunhill procedure
- Solely based on discretion of surgeon and their experience.

Toxic MNG

Toxic MNG
• Toxic multinodular goiters usually occur in older individuals, who often have a prior history of a nontoxic multinodular goiter.
• Over several years, enough thyroid nodules become autonomous to cause hyperthyroidism.
• Hyperthyroidism also can be precipitated by iodide-containing drugs such as contrast media and the antiarrhythmic agent amiodarone (jodbasedowhyperthyroidism).
• Symptoms and signs of hyperthyroidism are similar to Graves' disease, but extrathyroidalmanifestations are absent.

Toxic MNG
• Blood tests are similar to Graves' disease with a suppressed TSH level and elevated free T4 or T3 levels.
• RAI uptake also is increased, showing multiple nodules with increased uptake and suppression of the remaining gland.
• Treatment – After adequately controlling hyperthyroid state total thyroidectomy is treatment of choice.

Toxic Adenoma (Plummer's Disease)
• Hyperthyroidism from a single hyperfunctioning nodule typically occurs in younger patients who note recent growth of a long-standing nodule along with the symptoms of hyperthyroidism.
• Most hyperfunctioning or autonomous thyroid nodules have attained a size of at least 3 cm before hyperthyroidism occurs.
• Physical examination usually reveals a solitary thyroid nodule without palpable thyroid tissue on the contralateral side.
• RAI scanning shows a "hot" nodule with suppression the rest of the thyroid gland. These nodules are rarely malignant.
• Surgery (lobectomy and isthmusectomy) is preferred to treat young patients and those with larger nodules.
Thyroid Storm• Thyroid storm is a condition of hyperthyroidism
accompanied by fever, central nervous system agitation or depression, cardiovascular dysfunction that may be precipitated by infection, surgery, or trauma.
• Beta blockers are given to reduce peripheral T4 to T3conversion and decrease the hyperthyroid symptoms.
• Oxygen supplementation and hemodynamic support should be instituted.
• Non-aspirin compounds can be used to treat pyrexia and Lugol's iodine or sodium ipodate (intravenously) should be administered to decrease iodine uptake and thyroid hormone secretion.
• PTU therapy blocks the formation of new thyroid hormone and reduces peripheral conversion of T4 to T3.
• Corticosteroids often are helpful to prevent adrenal exhaustion and block hepatic thyroid hormone conversion.


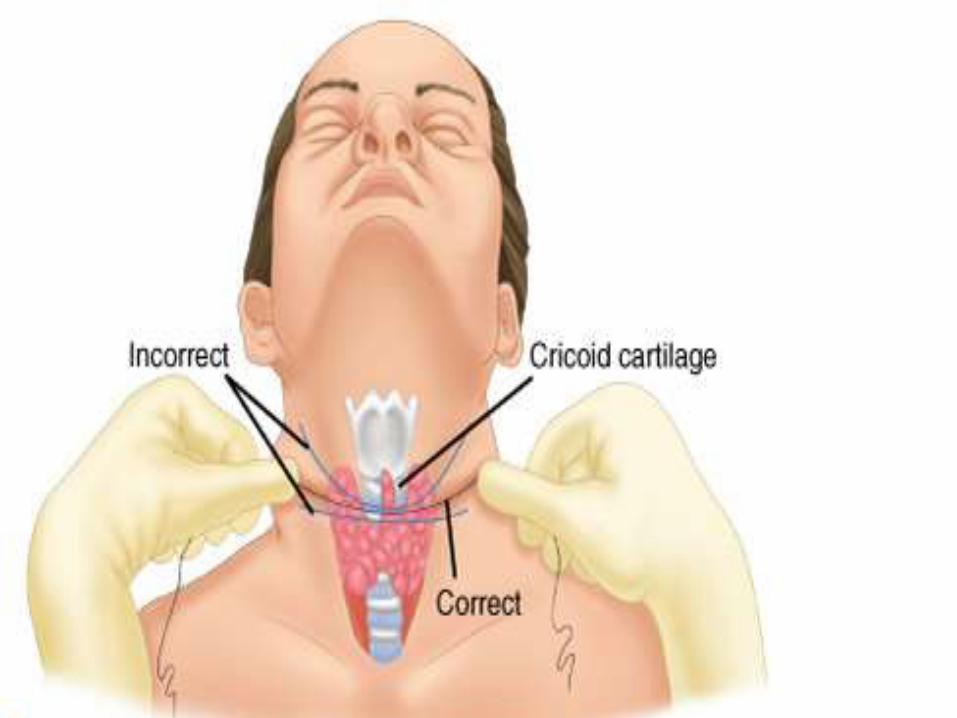
Steps of Thyroidectomy






Thank you for your patient listening.Hope you will handle our hyperness with care.
Yours lovingly,
Thyroid gland.


















