Thyroid gland. Anatomy Bi-lobed gland over second and third tracheal ring piramidal lobe : 40 – 50...
112
Thyroid gland
-
Upload
richard-montgomery -
Category
Documents
-
view
220 -
download
2
Transcript of Thyroid gland. Anatomy Bi-lobed gland over second and third tracheal ring piramidal lobe : 40 – 50...

Thyroid gland

Anatomy
Bi-lobed gland over second and third tracheal ring
piramidal lobe : 40 – 50 % Weight : 20 – 30 gr Epithelium lined follicle Colloid : glycoprotein ( thyroglobulin ) Vascular stroma True connective tissue capsule

It is important to ligate the superior thyroid artery close to the gland to avoid injury to the nerve during thyroidectomy

Inferior thyroid artery
Inferior thyroid artery :
Thyrocervical trunk
Absent in up to 6% Thyroidea ima :
directly from aorta , innominate artery or right common carotid artery
Present in up to 12%

Superior thyroid vein : IJV or common facial vein
Inferior jugular vein : innominate vein or IJV Middle thyroid vein : IJV Lymphatic → paratracheal nodes → superior
mediastinum & middle deep cervical node and lateral the neck

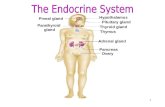
Embryology
Median endodermal derivative that migrates from the tongue base to its normal position in the neck by 7th week .
The distal portion of this thyroglossal duct forms the thyroid gland

Physiology
Concentrate iodine 20 – 30 % is store in thyroid Small percentage in hormone and nonthyroid
tissue All tyrosine compounds are bound to
thyroglubulin and store in thyroid follicles as colloid
The unbound thyroid hormone is responsible for influencing metabolism .

Thyroglossal duct anomaly
7% of the population has remnants of the thyroglossal duct
Cyst : anywhere along the length of duct
60% infrahyoid , 24% suprahyoid ,
1% intralingual 1-2 cm cystic mass that is mobile on
swallowing & protruding of the tongue

60% contain thyroid tissue Malignancy is rare Acute infection Contain mucus like clear fluid If it is become symptomatic it must be
removed Sistrunk operation

Lingual thyroid
Failure of thyroglossal duct to descend A mass at the foramen cecum Aysmptomatic or present with airway
obstruction May be the only thyroid tissue

Ectopic thyroid tissue
Anywhere along the migratory route of the thyroid
Mediastinum , larynx , trachea , pericardium or esophagus

Congenital intrathyroid cysts
Present in children persistent ultimobranchial bodies or an intrathyroidal thyroglossal duct cyst

Infectious and inflammatory disorder

Acute suppurative thyroiditis
M=F Preceded by an upper respiratory tract
infection Staph. The most common organism Painful enlargement of the gland Fever Abscess formation

Painless thyroiditis

Sporadic form
More common in female Difuse thyroid enlarement Without pain or thyroid enlargement Temporary hyperthyroidism 50% become hypothyroid which resolves in
6 month

Postpartum thyroiditis
Initial hypothyroidism is mild Lymphocytic infiltration and follicle disruption Self-limiting disease Steroid may be of value

Subacute thyroiditis ( De Quervain´thyroiditis )
At all age most common at 5th decade F>M May be viral Painful thyroiditis Defuse thyroid enlargement Malaise and fever thyrotoxic

Endocrine phases
Hyperthyroidism : 1-3 month Euthyroid : 1-3 weeks Hypothyroid : 2-6 month Recovery which is complete

Lymphocyte , monoycyte and giant cell infiltration .
Treatment consist of analgesic steroid and antiinflammatory agents .

Hashimoto´s thyroiditis
Common Affecting 2 population 95 % in female Autoimmune etiology with
strong genetic predisposition Diffusely enlarge with nodularity firm Disrupted follicle with lymphocyte and plasma
cell infiltration and variable fibrosis Residual hypothyroidism

A thyroid scan demonstrated a salt and pepper pattern

Anti thyroglobulin and antimicrosomsal ab are present up to 90%
FNA is diagnostic Increased risk for developing B – cell
lymphoma

Riedel‘s thyroiditis
Uncommon F>M Older patient May be mediastinal & retroperitoneal fibrosis Fixed rock-hard thyroid enlargement Gland replaced with fibrosisAirway obstruction and
dysphagia Palliative surgery to relieve obstruction

Hyperthyroidism

Graves‘ Disease
3th and 4th decade F/M : 7/1 Autoimmune etiology : abnormal Ig that fix on
TSH receptor of thyroid epithelial cell Diffuse toxic goiter ophthalmopathy 55% Dermophathy 5%

Cont.
↑ T3 , T4 , T3RU Thionamide , sympathetic blocker , iodine Radioactive iodine

Pregnant women should not be treated with this modility

Surgical indication
Refuse radioactive therapy Thyroid nodules suspicious for malignancy Must be rendered euthyroid prior to surgery

Subtotal thyroidectomy leaving 7-8 gr of nodule free tissue is recommended however ,
total thyroidectomy is proposed by many

Toxic multinodular goiter
Older patient no ophthalmopathy or dermophathy
Total thyroidectomy Radioactive iodine but not successfully as
surgery

Toxic adenoma
Younger patient Quite large ( 2.5 – 3 cm ) Surgical excision

Multinodular nontoxic goiter
Compensatory response Common in female Secondary to dietry
deficiency Symptom and sign of pressure

A small percentage (1-2%) may harbor a malignancy

Treatment
Thyroid suppression Surgery:
cosmetic deformity
pressure symptom refractory to suppression
Fear of malignancy
Development of toxicity

Neoplasm & Cyst

Benign adenoma
Encapsulated tumor Glandular epithelium with intratumoral
degenerative changes ( hemorrhage , fibrosis , calcification )
Rare thyrotoxicosis Type : follicular,colloid , embryonal, fetal ,
Hurthle ???

Malignant

Papillary carcinoma60 – 65 %
Third – 5th decade F/M : 2/1 Indolent with overall excellent prognosis May arise from benign adenoma Low-dose and high dose external RT

Macroscopic pattern
Occult ; <1.5 cm Intrathyroid ( 70% ) Extrathyroid : infiltrate larynx , trachea , strap
muscle , great vessel

Microscopic pattern
Purely papillary Some may have area of follicular Anaplastic transformation is rar Venous invasion in 10%

Intraglandular lymphatic invasion results in high incidence of multicentricity

Neither multicentricity nor regional LN metastasis have any prognostic
significance

Negative prognostic indicator
Advance age Male gender extrathyroid extension Distant metastasis

Cont.
Dedifferentiation Vascular invasion Atypical variants ( tall cell, columnar ,
sclerosing ) may have negative prognostic significance

Follicular carcinoma15%
Vascular invasion Metastasis to bone brain and liver Anaplastic transformation is more common Overtly invasive : infiltrate surrounding
structure ( MR 20-50%) Minimally invasive : microscopically has
capsular invasion (MR 5%)

Definitive diagnosis can often be established only on permanent section

Poor prognostic indicator
Advanced age Male gender extrathyroid extension Distant metastasis Vascular invasion anaplastic transformation trabecular growth
pattern

Hurthle cell carcinoma 5%
As a variant of follicular tumors Overtly invasive :higher mortality rate
Higher LN metastasis
Minimally invasive

Not all nodule containing Hurthle cell are neoplastic .The vast majority are Hurtule cell
changes in benign follicular adenomatous nodules or thyroiditis

Medullary carcinoma 3-5%
10 – 20 % familial Sporadic : in 5th decade Multicentric ,lateral upper 2/3 of gland Encapsulated , diffuse infiltrative 50% nodal metastasis 15-25% distant metastasis

MEN type 2A
Medullary thyroid cancer C-cell hyperplasia Adrenal pheochromocytoma Adrenal medullary hyperplasia Parathyroid hyperplasia

MEN type 2B
In addition : Mucosal neuromas GI ganglioneuroma Musculoskeletal abnormality

Poor prognostic indicator
MEN type 2B Nodal & distant metastasis Extrathyroid extension Small cell tumor pleomorphism Poor calcitonin staining High CEA

Anaplastic carcinoma 1-5%
Rare tumor Arise in well-differentiated tumor Older women Advance stage early infiltration of
surrounding structure Small cell , giant cell Extremely poor prognosis

Lymphoma 1-3.5%
Primarily in the thyroid As a part of systemic disease Arises in a gland with Hashimoto´s thyroiditis Elderly women Diffusely enlarged gland or nodule Hypothyroidism Diffuse large cell lymphoma Good prognosis

Miscellaneous
Sarcoma Mucoepidermoid carcinoma SCC Kidney , colon , melanoma are the most
common distant site

Clinical presentation

Thyroid enlargement
Smooth and diffuse ( usually benign ) Nodular Multinodular goiter may harbor a
neoplasm( 10-15% ) :
90% benign
10 % malignent

Overall incidence of malignancy in a multinodular goiter is only 1-2%

Symptom & sign of pressure
Dysphagia ( discomfort on swallowing → obstruction )
Mild to moderate stridor → chondromalacia → airway obstruction
TVC edema & RLN paralysis → hoarseness Retrosternal extension → tracheal deviation
& SVC

Symptom & sign of infiltration
Stridor and hemoptysis Rapid increasing in mass RLN paralysis Dysphagia & odynophagia Brachial plexus infiltration Painful enlargement

Evidence of regional and distant metastasis
It is the only obvious clinical evidence of thyroid cancer
Papillary metastasis may be cystic ( 20%) Follicular carcinoma : distant metastasis Medullary and anaplastic : extracapsular
extension

Evidence of endocrine dysfunction
Most patients are euthyroid Occasionally : hypothyroid Rarely : hyperthyroid Medullary : ↑ calcitonin , ACTH , PG
secretion

Evaluation of a thyroid mass

Neck X-ray
Patchy calcification :
Benign thyroid disease
Well –differentiated carcinoma
Medullary carcinoma

Chest X-Ray
Retrosternal extension Tracheal deviation Mediastinal nodal involvement Pulmonary metastasis

CXR should always be done

Esophagogram
It should be done if the patient complains of significant dysphagia
It differentiate thyroid from nonthyroid causes of dysphagia

Radionuclide scan
Determine the functional status of gland Differentiate diffusely enlarge from nodular Differentiate single nodule from multinodular
goiter

Tc-99
Low cost Ready available Short – half life Optimal imaging Only trapped , not organified

Radioactive Iodine
It is able to determine function ¹²³I is the best but is expensive and have
very short half life

Thallium 201
Detecting :
lymph node metastasis
retrosrernal extension
recurrent disease functioning nodule within suppressed gland

Octreotide scintigraphy is useful for detecting metastatic medullary and
Hurthle cell carcinoma

Radionuclide scan no longer used as a first line imaging study

Ultrasonography

High – resolution real time US enable the radiologist to detect nodule as small as
3mm

US usage
Screening high risk patient ( prior RT ) Differentiating single nodule from multiple Cystic or solid status Facilitating FNA Monitoring medically treated patient Evaluating clinically negative neck for
metastasis Recurrent disease after surgery

CT scaning & MRI
Extrathyroidal extension Retrosternal involvement Metastatic disease Unnecessary in the evaluation of a routine
thyroid mass

Metastatic workup
Bone scan CT scan of abdomen and chest Octreotide study
Blood test
T3 T4 TSH Thyroid Ab for Hashimoto thyroiditis Serum thyroglobulin Serum calcitonin in medullary carcinoma
especially if there is a family history

These level may increases after FNA and should be performed prior to it

Postoperative serum thyroglobulin levels under 10 ng/ml in patients under
supression therapy are indicative of cancer control

FNA biopsy
Obtain satisfactory specimen from nodule it is of no value in microinvasive follicular If the report is suspicious the patient should
probably proceed to surgery Inadequate specimen repeat FNA

FNA biopsy
The best results obtains from periphery Multiple aspirates are frequently necessary

A negative FNA should never preclude surgical exploration in a patient with
highly suspicious lesion

Large bore needle aspiration
A portion of capsule and surrounding tissue can be included
It is rarely indicated

Surgical exploration indication

Obvious malignancy
Clinical or radiographic evidence of infiltration
Clinical or radiographic evidence of regional or distant metastasis
FNA positive for malignancy ( papillary , medullary , anaplastic )
Thyroid mass with raised serum level of calcitonin

Suspicion of malignancy
Suspicious fine – needle aspiration Nodule refractory to suppression Solitary thyroid nodule with raised serum
thyroglobulin level Recurrent cyst refractory to two aspirations and
thyroid suppression Nodule going wrong , a solitary nodule increasing in
size and associated with pain True single nodule in males elderly women children ,
or in any patient with a history of prior RT

Management of thyroid Tumor

Every patient undergoing a thyroid exploration should sign a very specific
detail and inform that should include the possibility of performing throidectomy

Total thyroidectomy
Better oncologic operation in the case of multicentric disease
Difficult residual thyroid suppression and anaplastic transformation risk
Good postoperative scanning and radioactive ablation
Postoperative thyroglobulin titrage

Subtotal thyroidectomy
Simpler & time –consuming Lower morbidity Not affected the prognosis of well
differentiated tumor
Extrathyroid extension
Well-differentiated tumor : 9-16% If gross tumor would be left using the shaving
technique wild field resection should be performed .

RLN enveloped & paralyzed it should be sacrificed .
If it is the only functioning nerve and the tumor and the tumor can be dissected off this should be done
Superficial invasion can be shaved but direct extension into the lumen : sleeve
or wedge resection and primary anastomosis

Superficial thyroid cartilage : shave resection Hemilarynx : vertical partial laryngectomy Anterior larynx : hemilaryngectomy And
reconstruction Cricoid and bilateral laryngeal involvement :
total laryngectomy

Postoperative RT and iodine is indicated

Regional lymph node
In all patient : pericapsular and paratracheal node need to be removed routinely
Overt node in these area : sup. Mediastimun and lateral neck exploration

Papillary carcinoma
Clinical node : 20-25% Pathological node : 30-79% It has no adverse effect on prognosis Extracapsular extension does not appear to
have an ominous prognosis

Follicular carcinoma
Very rare < 10% clinically & 20% pathologically
Neck dissection are performed only for overt metastasis
Hurthle cell carcinoma
30% lymphatic metastasis Functional neck dissection should be
performed when disease is encountered

Medullary carcinoma
Metastasis : 50 – 63 % Prophylactic paratracheal , superior
mediastinal and lateral neck dissection Or : positive node in mediastinum and lateral
neck dissection is performed

Follow -up

Well-differentiated tumor
Become hypothyroid and after 4-6 week radioiodine scan
Any residual tissue : I ablation In overt local or regional remnant & distant
metastasis should be used Further 6 and 12 months scan and then
every 2 year Serum thyroglobulin every 6 months

Medullary carcinoma
Calcitonin level : every 3 months ( in first year )
Every six months there after High calcitonin level : full metastatic work up
CT & MRI of the neck and octreotide scan No overt disease : neck dissection and if it
done before RT to neck

Postoperative RT
Residual and inoperable disease or cancer that has undergone anaplastic transformation
50 Gy RT appears more effective than radioactive iodine in
treating local recurrence in WD cancer I radioactive is the treatment of choice for distant
metastasis RT is the treatment of choice in anaplastic carcinoma

Role of chemotherapy
Most disappointing results

Postoperative thyroid hormone
Total thyroid ablation : T4 supplement It is useful in controlling any microscopic
residual WD thyroid cancer that may have been left locally , regionally or distantly

Prognosis
Low risk patient : 1-2 % MR High risk patient : 40 – 50 % Hereditary & sporadic cancer have similar
survival ( 82% at 5 year ) Anaplastic cancer has a dismal survival Early stage medullary : good prognosis