BENIGN DISEASES OF THE THYROID Rivka Dresner Pollak M.D Endocrinology.
Upload
selvaraj-balasubramaniCategory
view
553download
5
THYROID- BENIGN SWELLINGS
DR.B.SELVARAJ MS;MCH;FICS
MMMC;MALAYSIA

ANATOMY
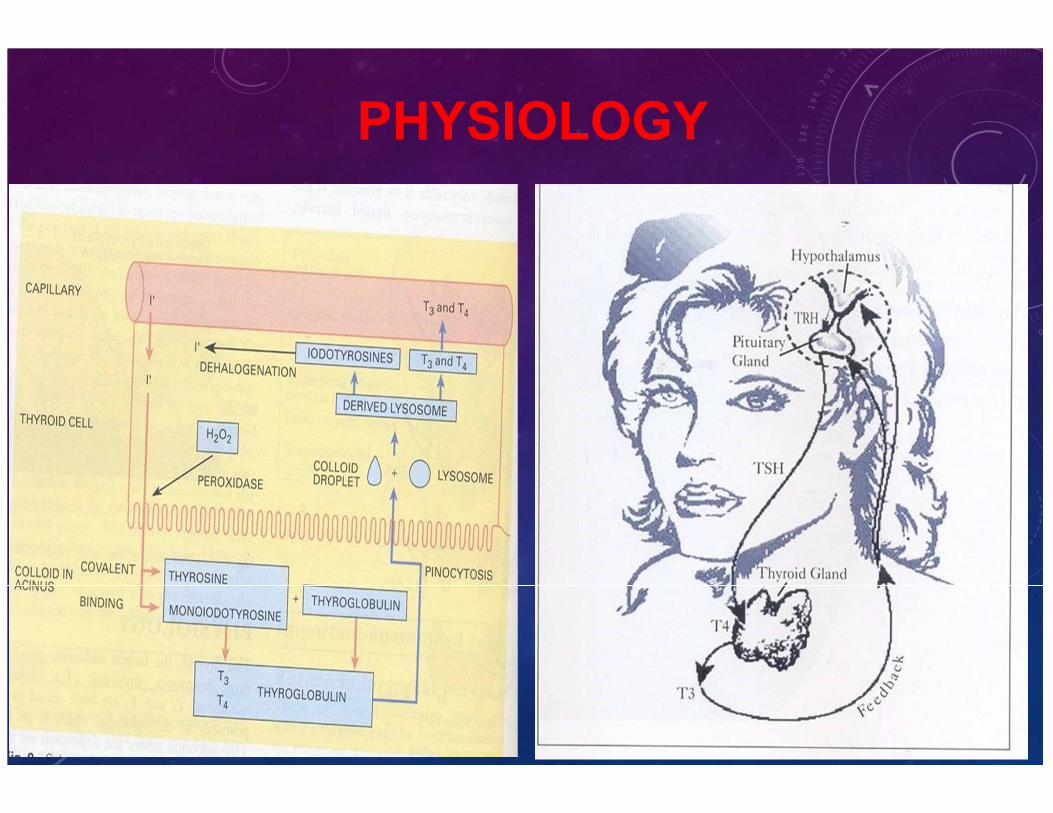
PHYSIOLOGY

DEFINITIONS
• GOITER: any enlargement of thyroid gland
• Thyrotoxicosis : Symptoms of thyroid hormone excess due to increased synthesis or release due to destruction of thyroid follicles or exogenous thyroid hormone supplementation.
• Hyperthyroidism : Features of thyroid hormone excess due to increased synthesis of thyroid hormone by the gland.

CONDITIONS CAUSING
THYROTOXICOSIS
• Diffuse toxic goitre (Grave’s disease)
• Toxic nodular goitre (Toxic MNG)- Plummer’s disease
• Toxic nodule (Toxic adenoma)- Goetsch’s disease
• Thyrotoxicosis factitia (Due to excess exogenous thyroid hormone supplementation)
• Jod-Basedow thyrotoxicosis (Iodide induced)
• Thyroiditis
• Malignancies of thyroid.
• Trophoblastic tumor (Due to thyroid stimulating action of HCG produced by this tumor)
• Ectopic thyroid tissue (Struma ovarii)
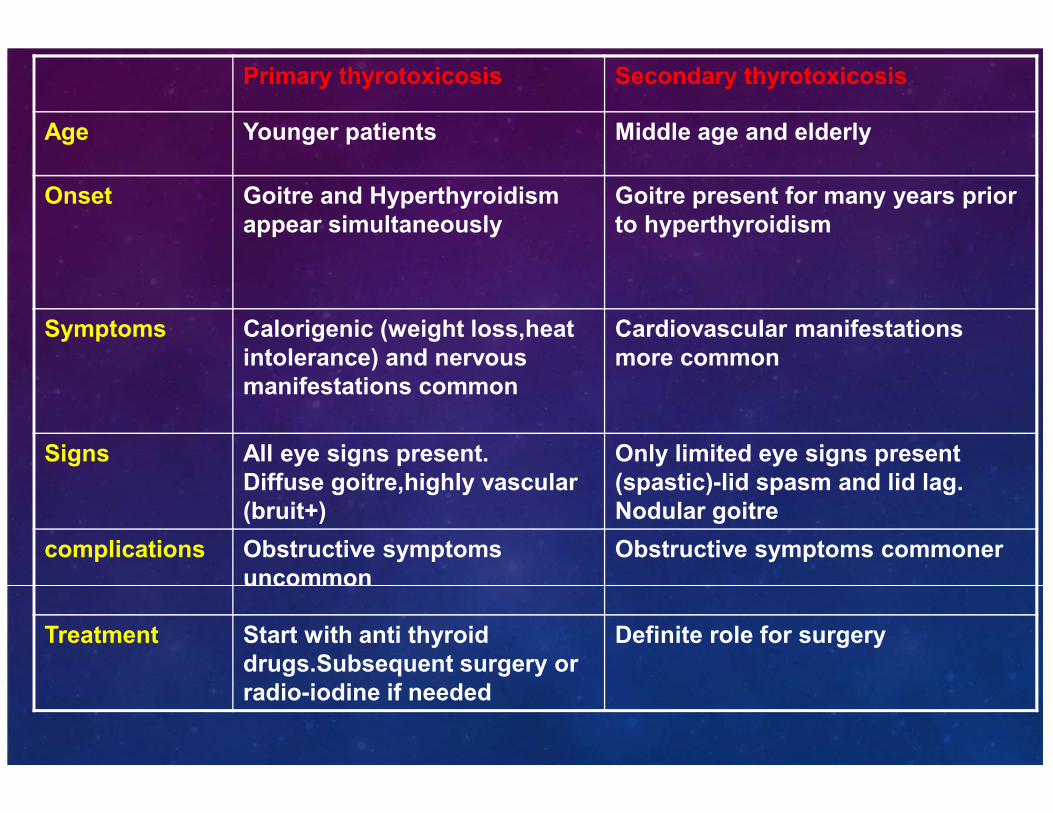
Primary thyrotoxicosis Secondary thyrotoxicosis
Age Younger patients Middle age and elderly
Onset Goitre and Hyperthyroidism
appear simultaneously
Goitre present for many years prior
to hyperthyroidism
Symptoms Calorigenic (weight loss,heat
intolerance) and nervous
manifestations common
Cardiovascular manifestations
more common
Signs All eye signs present.
Diffuse goitre,highly vascular
(bruit+)
Only limited eye signs present
(spastic)-lid spasm and lid lag.
Nodular goitre
complications Obstructive symptoms
uncommon
Obstructive symptoms commoner
Treatment Start with anti thyroid
drugs.Subsequent surgery or
radio-iodine if needed
Definite role for surgery
GRAVE’S DISEASE
• Described by Irish physician Dr.Robert Graves in 1835
• Common in females
• Age : 20-40 years
• Pathogenesis:
• Thyroid stimulating immunoglobulins (TSI) of IgG class produced
by lymphocytes stimulate TSH receptor.
• Ophthalmopathy: Fibroblast proliferation and increased
glycosaminoglycans production induced by TSI (?antigenic
similarity between orbital tissues and thyroid.)

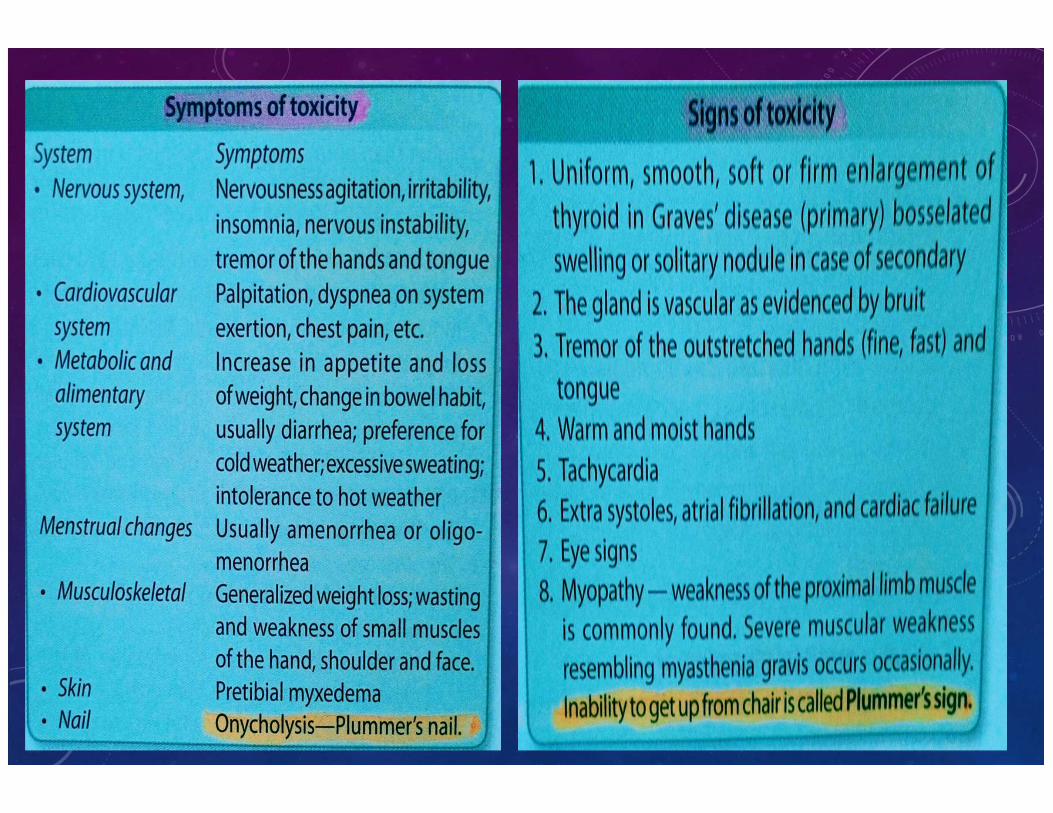
CLINICAL FEATURES - SYMPTOMS
• Calorigenic : Increased appetite,weight loss,heat intolerance,
increased sweating, tiredness
• Nervous : Tremors,anxiety,nervousness,increased activity
• CVS: Dyspnoea, palpitations, pedal edema (due to CCF)
• Ocular : Diplopia, pain and increased lacrimation (due to
corneal ulcer)
CLINICAL FEATURES- SYMPTOMS
• Menstrual : Amenorrhoea/ oligomenorrhoea
• Miscellaneous: Loose stools.
THYROTOXICOSIS- SIGNS
• Thyroid :Diffuse enlargement with bruit and visible
pulsations
CVS
• Pulse : Increased sleeping pulse rate with wide pulse
pressure.
• Stages of development of thyrotoxic arrhythmias : Multiple
extra systoles → Paroxysmal atrial tachycardia →
Paroxysmal atrial fibrilla?on → Persistent AF not responding
to digoxin.

EYE SIGNS
Seen in both Primary and secondary thyrotoxicosis (due to
increased thyroid hormone levels which sensitizes the
Muller's muscle to sympathetic system)
• Von Graefe’s sign (lid lag)
• Stellwag’s sign (characteristic stare with infrequent blinking)
• Dalrymple’s sign (widened palpebral fissure)

EYE SIGNS
• Naffziger’s sign : For proptosis
• Moebius sign : Loss of convergence (Due to ophthalmoplegia)
• Joffroy’s sign: Absence of wrinkling of forehead on looking up.

THYROTOXICOSIS- SIGNS
• Dermopathy : Pretibial myxedema due to increased
mucopolysaccharide deposition.
• Thyroid acropachy : Dermopathy associated with
clubbing of toes
• Tremors: Outstretched hands,tongue
• Grave’s disease is diagnosed when features of
thyrotoxicosis is associated with ophthalmopathy +/-
dermopathy

GRAVE’S DISEASE-OPHTHALMOPATHY
DIAGNOSIS
• Most cases can be diagnosed clinically.
• Thyroid function test : Raised T3,T4 with decreased TSH.
• Thyroid scan : I123 scan-Diffuse increased uptake.
• FNAC : Relative contraindication in the presence of
thyrotoxicosis.

HISTOPATHOLOGY OF GRAVE’S DISEASE-
FOLLICULAR HYPERTROPHY WITH SCANTY COLLOID


TREATMENT OPTIONS
• Medical
• Radio-Iodine
• Surgery

MEDICAL TREATMENT –DRUGS USED
• Anti thyroid drugs : Carbimazole and propylthiouracil
• Mechanism of action : Inhibit thyroid peroxidase and thereby interfere with
iodination of tyrosine residues in thyroglobulin and coupling of iodotyrosine
residues to form T3 and T4.
• Dose : Start with high dose (Carbimazole 10mg TDS ) once control is
achieved dose is reduced (5 mg BD or TDS)
• Alternatively block and replacement regimen is used – Continue with high
dose of antithyroid drugs with thyroxine supplementation (0.1 mg OD) .
Decreased risk of iatrogenic hypothyroidism .
• Adverse effects : Agranulocytosis less common but serious adverse effect.
Needs monitoring of counts.

MEDICAL TREATMENT- ADVANTAGES:
• Can be used even in children and young adults.
• Hypothyroidism if induced is reversible
• No complications associated with surgery.
Disadvantages:
• Prolonged treatment is required since relapse rate is high.
• Drug toxicity

BETA BLOCKERS
• Propranolol most commonly used
Indications :
• For symptomatic control
• When antithyroid drugs are initiated till biochemical
control is achieved
• Thyroid storm
• Along with iodide for preop preparation.
• Dose : 20-40 mg QID (Max dose – 600mg/day)
IODIDES
• Lugol’s iodine most commonly used preparation (5% iodine in 10% potassium iodide solution).
Mechanism of action :
• Inhibition of thyroid hormone release (Thyroid constipation)
• Decreases vascularity of the gland
Uses:
• Preop preparation : 10-14 days prior to surgery
• Thyroid storm :iodinated contrast agents (sodium ipodate ) given i.v.
Dose : Lugol’s iodine 5 drops TDS in milk.

RADIOACTIVE IODINE ABLATION
• I131 most commonly used
Indications :
• Patients with small to moderate enlargement of gland and antithyroid drugs have clearly not worked.
• Patients not willing for surgery or for whom surgery is contraindicated.
• Recurrence after surgical or medical therapy.

RADIOACTIVE IODINE ABLATION
Euthyroid state achieved by using antithyroid drugs for
3-4weeks before treatment.
↓
Interruption of antithyroid drugs for 3-4 days before and after Iodine treatment to permit adequate accumulation and retention of administered iodine.
↓
Pretreatment radioiodine scan done (25-100 micro curie of I131 given) to calculate therapeutic dose.
↓
Therapeutic dose of radio-iodine given (usually 8-12 milli curie) orally.

RADIOACTIVE IODINE ABLATION
• Patient rendered euthyroid by 8-12 weeks after treatment.
Disadvantages :
• Hypothyroidism : incidence 10-15% by 1 year which
increases by 3% in each succeeding year.
• Exacerbation of cardiac arrhythmias in elderly
• Fetal damage-hence contraindicated in pregnant and
lactating women
• Worsening of ophthalmopathy – avoided by using
prophylactic steroids
• Can induce Thyroid storm if patients are not rendered
euthyroid before radio-iodine administration.
RADIOACTIVE IODINE ABLATION
• Carcinogenic effect of radio-iodine has been
ruled out and hence radio-iodine can be safely
used in all individuals over 25 years i.e when
development is complete.

SURGERY
Indications :
• Failure of medical/radioiodine treatment
• Younger patients particularly adolescents
• Pregnant patients
• Patients with suspicious masses contained within the large thyroid.
• Patients with severe cosmetic deformities or tracheal compression causing discomfort.

SURGERY
• Extent of surgery : Subtotal or total thyroidectomy
Advantage of total thyroidectomy :
• Recurrence is avoided
• Patients with ophthalmopathy are stabilized most
successfully by total thyroidectomy.(Due to removal of
entire antigenic focus)
• Patients should be rendered euthyroid before surgery
to avoid thyroid storm.

THYROID STORM-TREATMENT
• Supportive measures : Correction of dehydration with I.v fluids and hyperpyrexia with cooling blankets
• Antithyroid drugs : Propylthiouracil preferred.Given through Ryle’s tube if patient can’t take orally.(Parenteral forms not available).
• Iodinated contrast agents (sodium ipodate)-1gm given I.v
• Propranolol 2mg I.v with ECG monitoring (if patient cannot take orally) or 40-80mg Q6h
• Large doses of dexamethasone : 2mg Q6h (inhibit hormone release,peripheral conversion of T4toT3 and provide adrenal support.
• Life threatening circumstances : Peritoneal or hemodialysis to lower T3 andT4 levels.
OPHTHALMOPATHY-TREATMENT
• Mild disease – Conservative measures: Elevating the head at
night ,Protection of eye ball and avoiding corneal drying by
applying 1%methylcellulose eye drops or plastic shields.
• Severe cases –large doses of prednisolone (100-120
mg/day)
• Malignant exopthalmos : Orbital decompression.

THYROTOXICOSIS IN
PREGNANCY
• Radio-Iodine : Contraindicated.
• Surgery : Can be done in second trimester
• Chance of miscarriage present with surgery.
• Antithyroid drugs : Propylthiouracil preferred
(Placental transfer less)
• Can cause fetal goitre.
• Avoided by keeping antithyroid drug dosage to
minimum to prevent rise in TSH.

TOXIC MULTINODULAR GOITER-
PLUMMER’S DISEASE
• Seen in long standing goitre when one or more nodules become autonomous.
• Cardiovascular symptoms predominate
• Radionuclide scan: Can demonstrate autonomous nodules.
• Treatment :
• Antithyroid drugs : Can control symptoms but relapse invariably occurs with discontinuation of medications.
• Propranolol can be used for symptomatic control.
• Radio-iodine : Effective.But larger doses are required 20-30 milli curie)
TOXIC MULTINODULAR GOITER-PLUMMER’S
DISEASE
• Chance of hypothyroidism with
radio-iodine is less compared to
grave’s disease due to variable
activity of different portion of the
gland allowing previously
quiescent area to function in
place of those destroyed by I131.
• Surgery : Preferred treatment
(Subtotal thyroidectomy)

TOXIC ADENOMA- GOETSCH’S
DISEASE

THYROID SURGERY

ROUTINE INVESTIGATIONS BEFORE
THYROID SURGERY
• X-ray soft tissue neck – AP and lateral view
• Indirect laryngoscopy
• Serum calcium : Baseline value to detect post-op hypocalcemia
due to hypoparathyroidism (Optional)

TYPES
• Hemithyroidectomy
• Subtotal thyroidectomy
• Near total/total thyroidectomy

TECHNIQUE
• Anaesthesia : GA with ET tube
• Position : Supine with table tilted up by 15 degree to reduce venous
engorgement
• Neck extended by placing sandbags under shoulder.
• Incision : Skin crease incision about 2 finger breadths above
suprasternal notch.
TECHNIQUE
• Flaps of skin,subcutaneous tissue and platysma raised upwards
to superior thyroid notch and downwards to the suprasternal
notch.
• Deep cervical fascia is divided in the midline between the
sternothyroid muscles down to the plane of thyroid capsule.

THE THYROID LOBE IS EXPOSED BY MOBILIZING THE
STRAP MUSCLES AWAY FROM THE LOBE BY MEANS OF
LATERAL RETRACTION ON THE MUSCLES
THE MIDDLE THYROID VEIN IS EXPOSED, DIVIDED, AND
LIGATED.

BABCOCK CLAMPS ARE APPLIED TO INFERIOR AND
SUPERIOR (NOT SHOWN) ASPECTS OF THE THYROID
LOBE TO FACILITATE MEDIAL RETRACTION ON THE
GLAND.
TECHNIQUE
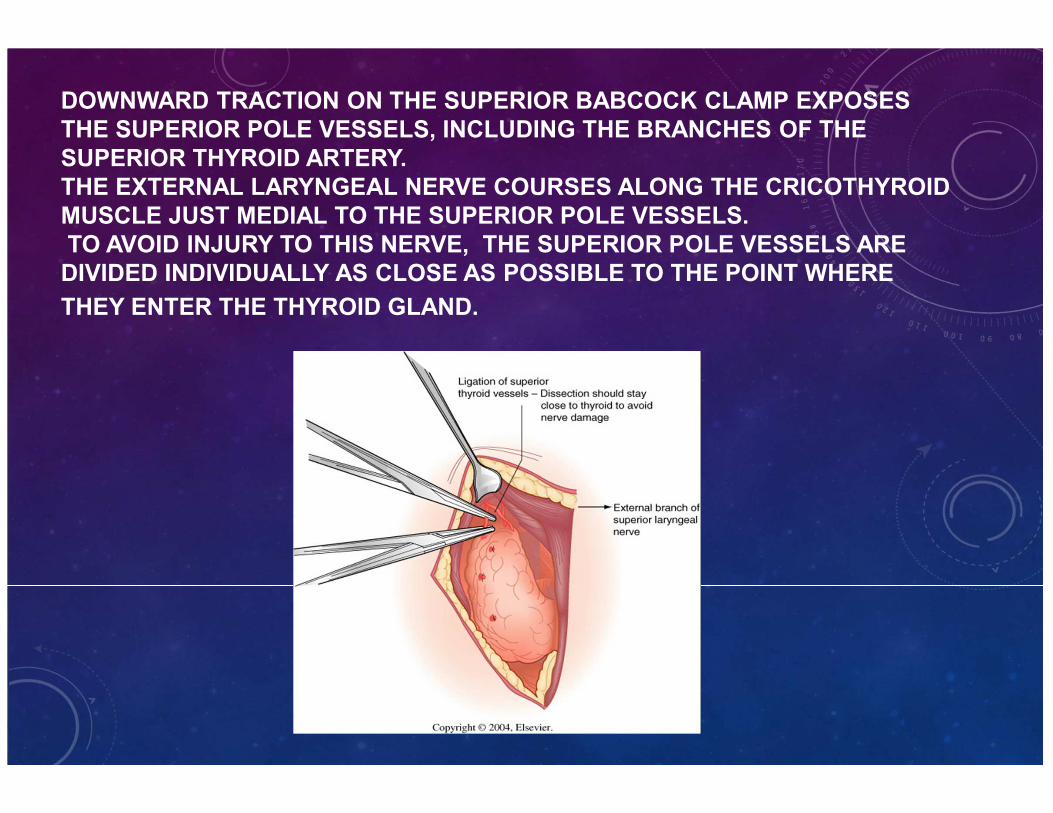
DOWNWARD TRACTION ON THE SUPERIOR BABCOCK CLAMP EXPOSES
THE SUPERIOR POLE VESSELS, INCLUDING THE BRANCHES OF THE
SUPERIOR THYROID ARTERY.
THE EXTERNAL LARYNGEAL NERVE COURSES ALONG THE CRICOTHYROID
MUSCLE JUST MEDIAL TO THE SUPERIOR POLE VESSELS.
TO AVOID INJURY TO THIS NERVE, THE SUPERIOR POLE VESSELS ARE
DIVIDED INDIVIDUALLY AS CLOSE AS POSSIBLE TO THE POINT WHERE
THEY ENTER THE THYROID GLAND.

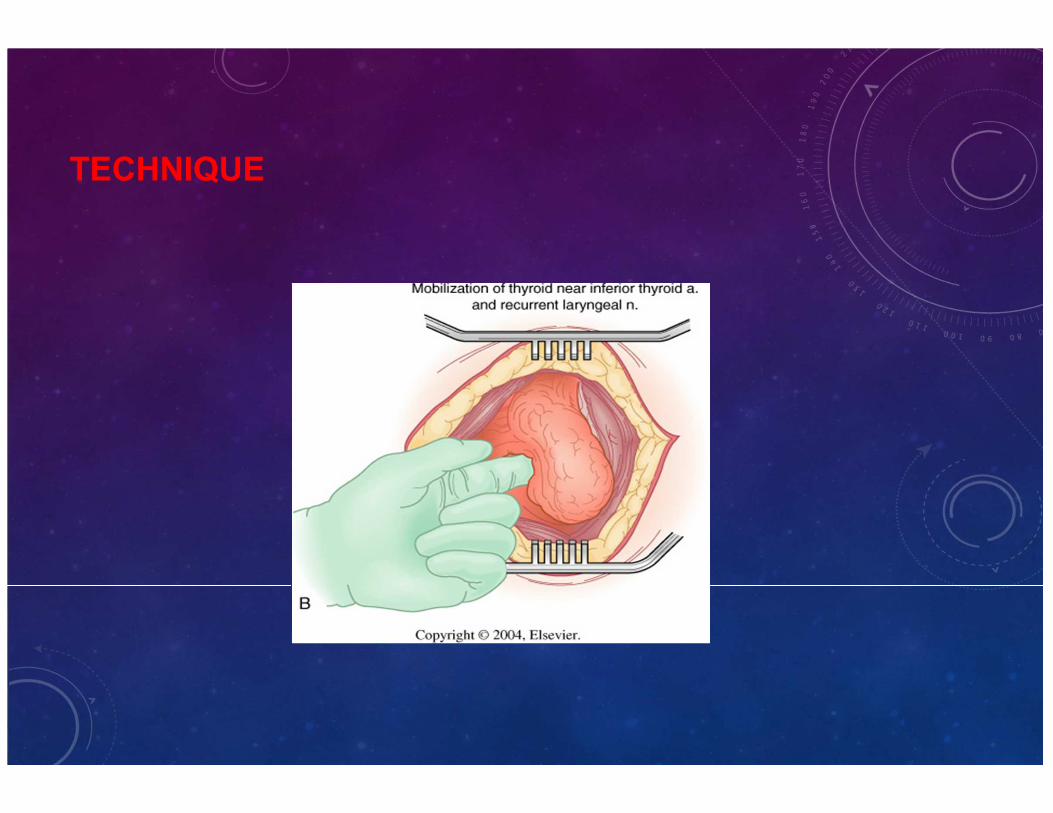
AS THE THYROID IS RETRACTED MEDIALLY, GENTLE
DISSECTION IS USED TO EXPOSE THE PARATHYROID
GLANDS, INFERIOR THYROID ARTERY, AND RECURRENT
LARYNGEAL NERVE.

TO PERFORM TOTAL LOBECTOMY, THE BRANCHES OF THE INFERIOR THYROID
ARTERY ARE DIVIDED AT THE SURFACE OF THE THYROID GLAND. THE INFERIOR
THYROID VEINS CAN NOW BE LIGATED AND DIVIDED. SUPERIORLY, THE CONNECTIVE
TISSUE (LIGAMENT OF BERRY), WHICH BINDS THE THYROID TO THE TRACHEAL
RINGS, IS CAREFULLY DIVIDED. THERE ARE USUALLY SEVERAL SMALL
ACCOMPANYING VESSELS, AND THE RECURRENT NERVE IS CLOSEST TO THE
THYROID AND MOST VULNERABLE AT THIS POINT.

THE DISSECTION OF THE THYROID FROM THE TRACHEA CAN BE
PERFORMED WITH THE CAUTERY BY DIVISION OF THE LOOSE
CONNECTIVE TISSUE BETWEEN THESE STRUCTURES. DISSECTION IS
EXTENDED UNDER THE ISTHMUS, AND THE SPECIMEN IS DIVIDED SO
THAT THE ISTHMUS IS INCLUDED WITH THE RESECTED LOBE.

SUBTOTAL LOBECTOMY NECESSITATES IDENTIFICATION OF THE PARATHYROID
GLANDS, INFERIOR THYROID ARTERY, AND RECURRENT LARYNGEAL NERVE, AS
PREVIOUSLY DESCRIBED. THE LINE OF RESECTION IS SELECTED TO PRESERVE THE
PARATHYROID GLANDS AND THEIR BLOOD SUPPLY AND TO PROTECT THE
RECURRENT LARYNGEAL NERVE. IT SHOULD BE BASED ON THE INFERIOR THYROID
ARTERY OR ITS MAJOR BRANCHES.

CLAMPS ARE PLACED ALONG THE LINE OF RESECTION AND THE
THYROID GLAND IS DIVIDED. THE DIVIDED TISSUE IS LIGATED OR
SUTURE-LIGATED WITH 3-0 SILK SUTURES.

DURING THYROIDECTOMY, THE RECURRENT LARYNGEAL NERVE IS AT
GREATEST RISK FOR INJURY (1) AT THE LIGAMENT OF BERRY, (2)
DURING LIGATION OF BRANCHES OF THE INFERIOR THYROID ARTERY,
AND (3) AT THE THORACIC INLET.


POST-OP COMPLICATIONS
• Hemorrhage : Tension hematoma deep to cervical fascia usually
result from slipping of ligature on the superior thyroid
artery.Requires emergency re-exploration.
• Respiratory Obstruction : Due to tension hematoma or
Tracheomalacia.
• Thyroid insufficiency- hypothyroidism
• Recurrent laryngeal nerve paralysis
• Superior laryngeal nerve paralysis
• Parathyroid insufficiency- hypocalcemia
• Wound infection
• Hypertrophic scar