
Thyroid
103
THYROID DISORDERS
-
Upload
miami-dade -
Category
Health & Medicine
-
view
2.409 -
download
1
Transcript of Thyroid
THYROID DISORDERS
The thyroid gland secretes thyroxine (T4) and smaller amts of tri-
iodothyronine (T3) T3 is three to eight more times potent than T4 both modulate energy use, heat production and
facilitate growth thyroid hormones exert metabolic effects in several
body tissues increasing O2 consumption and heat production which increases metabolic rate
2

Thyroid hormones affect several organ systems which are lacking in hypothyroidism and exaggerate in hyperthyroidism
Thyroid evaluation can be evaluated for functional status
euthyroid, hypothyroid or Hyperthyroid
etiology of dysfunction, or structural abnormalities causing dysfunction
3
Tests of Serum Thyroid Hormone levels Total T4 and T3
measures total amt of hormone bound to thyroid binding proteins (TBG) and in the free state by radio-immunoassay
Total T4 and Total T3 are elevated in hyperthyroidism and low in hypothyroidism increase in TBG from pregnancy or estrogen tx increases
Total T4 and T3 in absence of hyperthyroidism cirrhosis and nephrotic syndrome can lower TBG and thus
lower Total T4 and T3
4
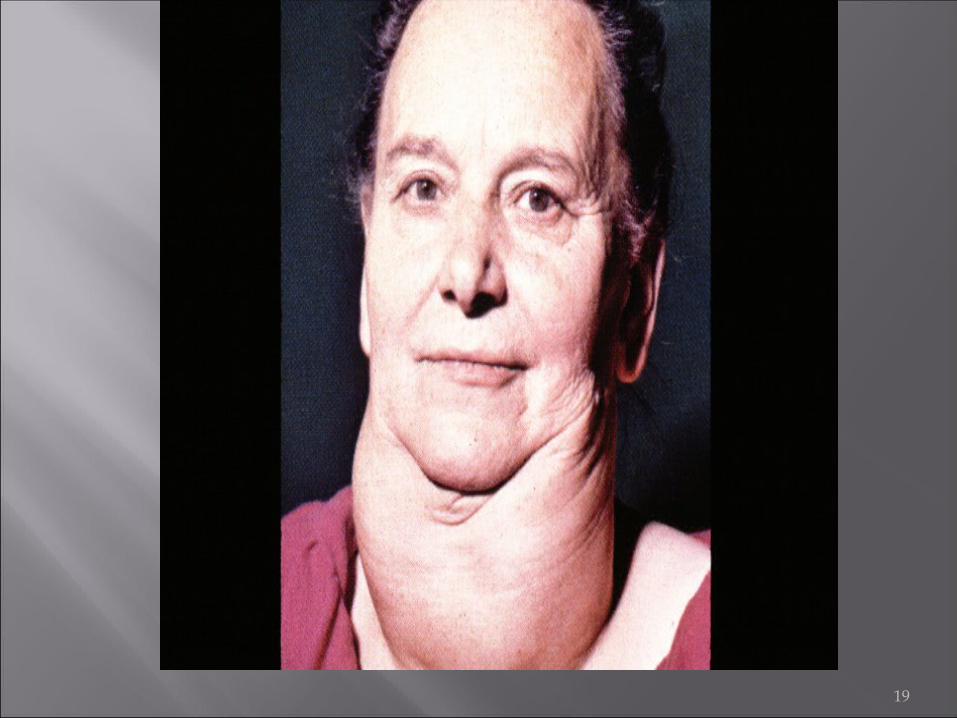
Apathetic hyperthyroidism pt’s present w/flat affect, emotional lability, weight
loss, muscle weakness, atrial fibrillation resistant to tx or congestive ht failure
Separation of nail beds (onycholysis) often occurs in Graves disease
5

Lab findings elevated free T4 and a suppressed TSH confirm Dx
for thyrotoxicosis increased uptake of 123I differentiates Graves
disease from early sub-acute or Hashimoto’s thyroiditis 123I is low in sub-acute or Hashimoto’s thyroiditis
MRI or ulta-sound can show orbital muscle enlargement w/o signs of opthalmopathy
6

Onset may be insidious Atrial fib is rare in young patient but occur in
over 50% of males patient over 60 y/o Results from IgG antibodies against the TSH –
receptor These antibodies are termed thyroid –
stimulating antibodies (TSAb) May be responsible for thyroid enlargement in
this disease
7
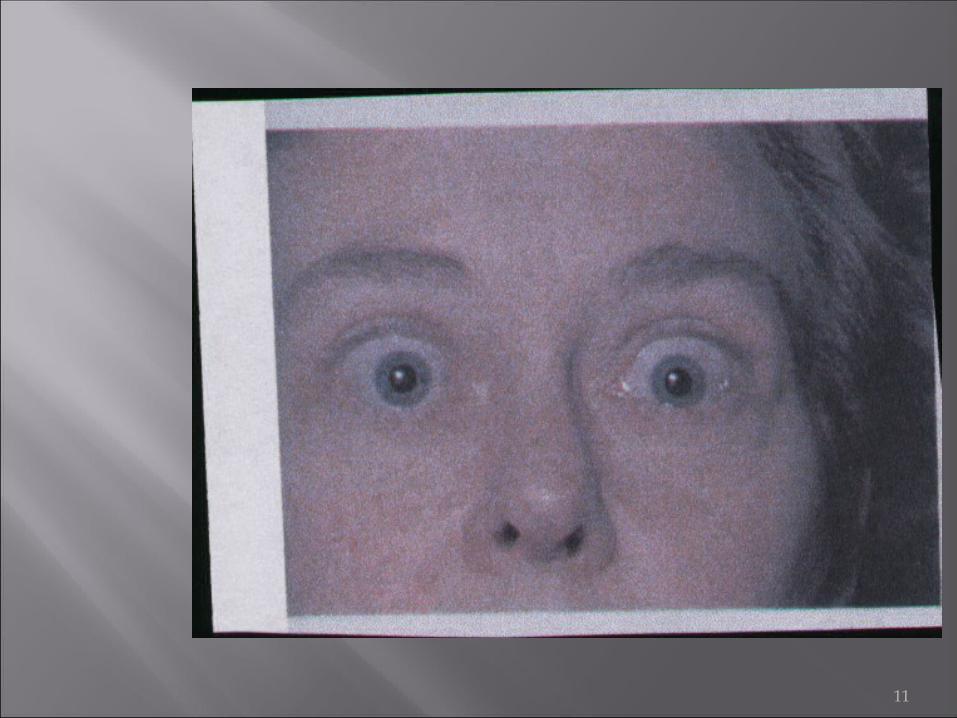
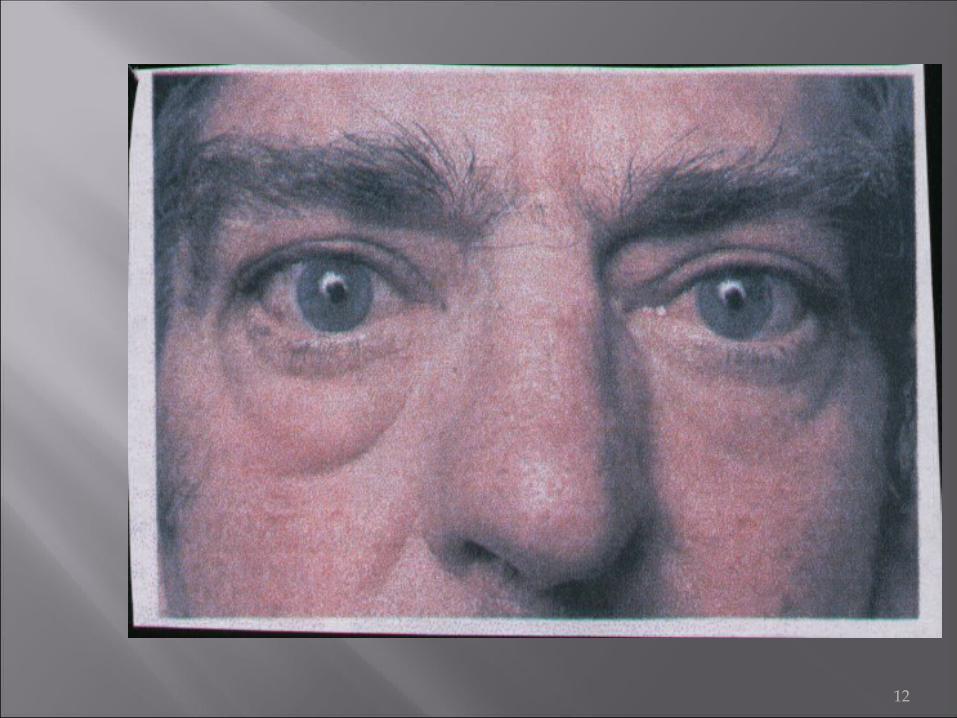
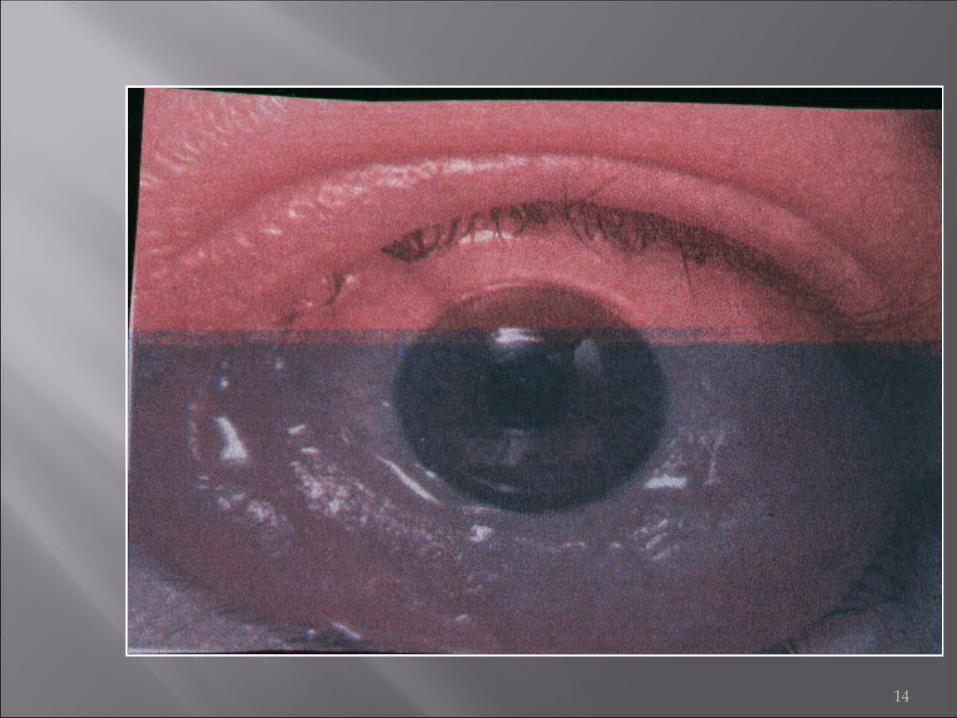
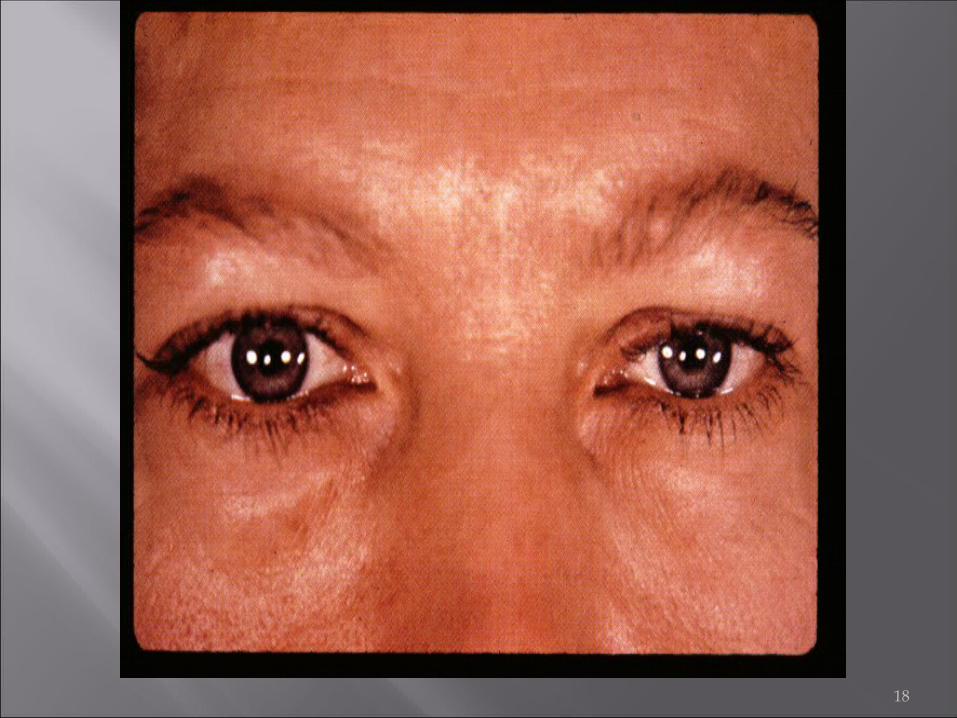
The cardinal signs of Graves’ disease are: Diffuse goiter Vascular bruit can be heard over these goiters Pretibial myxoedema Tachycardia with a bounding pulse Exophthalmos Lid lag (usually on downward eye movement) Lid retraction Peri-orbital puffiness Increased lacrimation Conjunctival edema and ulceration
8

In the elderly a ‘masked’ hyperthyroidism may be found. If presentation of a 60 y/o with atrial fib, heart failure and weight loss
THINK HYPERTHYROIDISM!!! Diagnosis is made clinically with
confirmation by labs:
T3 and T4 and undetectable TSH levels if a single nodule is suspected a thyroid scan
may provide useful information
9

10
11
12
13
14

15
16
17
18
19

20
Graves disease tx: Anti-thyroid drugs: thiocarbamide drugs,
propylthiouracil, methimazole, and carbimazole block thyroid hormone synthesis propythiouracil partially inhibits peripheral conversion
of T4 to T3 tx must be given until ds undergoes spontaneous
remission (12 to 18 months) only 20-30% remain in remission pts who relapse must undergo surgery or radioactive
iodine tx
21

Pts must be instructed to d/c med if sore throat or fever develops → agranulocytosis
beta blockers can be given at onset to alleviate cardiac abnormalities
Radioactive iodine 131I in terms of cost, ease, efficacy and short-term side-
effects, radioactive iodine has benefits that exceed anti-thyroid drugs or surgery pts w/severe thyrotoxicosis, or very large thyroids should
tx’ed first w/anti-thyroid drugs to become euthyroid
22
Pt’s become euthyroid w/radioactive iodine in 3wks to 6 months
10-20% become hypothyroid in first yr 50-80% who receive radioactive tx eventually become
hypothyroid Surgery: subtotal thyroidectomy is tx of choice in pt’s as a treatment for thyroid cancer
when an enlarged thyroid (goiter) or multiple nodules cause cosmetic, breathing or swallowing problems
in a pregnant woman, when her hyperthyroidism is not controllable by antithyroid drugs, and requires immediate treatment
23
when other forms of treatment for hyperthyroidism -- i.e,. antithyroid drugs or radioactive iodine have not been effective. (This is applicable in the U.S. Outside the U.S., surgery is sometimes performed as a hyperthyroidism treatment before or instead of radioactive iodine.)
in children, if the practitioner or parent wishes to avoid radioactive iodine
when the patient refuses antithyroid medications or radioactive iodine
when a patient wants to try to get pregnant quickly after treatment
24
Toxic adenoma solitary toxic nodules occur more frequently in older
pt’s usually benign S&S are those of thyrotoxicosis TSH is suppressed w/ high levels of T3 w/a
moderate elevation of T4 thyroid scan shows a “hot” nodule usually managed w/131I, may need unilateral
thyroidectomy if nodule is large
25
Toxic Multi-nodular Goiter occurs in older pts w/long standing multi-nodular
goiter S&S usually are tachycardia, heart failure and
arrthymias PE reveals a multi-nodular goiter TSH is suppressed, markedly elevated T3 and a
moderately elevated T4 tx of choice is subtotal thyroidectomy
heart disease may be contraindication to surgery toxic nodules tx’ed w/131I
26
Thyroiditis can be classified as acute, sub-acute, or chronic
may eventually result in hypothyroidism easily differentiated from other causes of
hyperthyroidism by a suppressed 123I uptake Acute suppurative thyroiditis is a rare complication
of septicemia S&S: high fever, redness over gland, tenderness
may be confused w/sub-acute thyroiditis if blood cultures are neg, needle aspiration can identify
organism; tx w/antibiotics or Incision &Drainage (I&D)
27

Sub-acute thyroiditis (de Quervain’s thyroiditis or granulomatous thyroiditis) an acute inflammatory disorder probably due to
viral infection resolves in a few months in 90% of pts S&S: hyperthyroidism, fever, anterior neck pain;
classical feature is an exquisitely tender gland labs vary w/course of ds: initially T4 is elevated, TSH is
suppressed, 123I uptake is very low may fluctuate from euthyroid to hypothyroid and back
28

Increase in 123I on scan reflects recovery of gland tx is usually non-steroidal anti-inflammatory drugs
(NSAID’s), short course of prednisone may be needed if fever and pain are severe; levothyroxine may be needed for clinical symptoms of hypothyroidism
29
Chronic Thyroiditis (Hashimoto’s thyroiditis, lymphocytic thyroiditis) results from destruction of normal thyroidal
architecture by lymphocytic infiltration resulting in hypothyroidism and goiter
Hashimoto’s thyroiditis is more common in women and most common cause of hypothyroidism and goiter in the US
30
Occasionally pts may have transient hyperthyroidism w/ low 123I uptake
gland non-tender to palpation serum T4 and T3 are nl or low, when low TSH is
elevated FNA reveals lymphocytes and Hurthle cells
(enlarged basophilic follicular cells) hypothyroidism and goiter are indications for
levothyroxine tx
31

Thyrotoxicosis Factitia presents w/ clinical features of thyrotoxicosis from
ingestion of large amts of thyroxine often occurs in an attempt to lose weight TSH is suppressed, T4 and T3 levels are elevated 123I uptake is absent pts may require psychotherapy
32
Rare causes of thyrotoxicosis1. Struma ovarii: occurs when an ovarian teratoma
contains thyroid tissue and secrets thyroid hormone
dx confirmed by 123I uptake in pelvis on body scan
1 Hydatidiform mole: due to proliferation and swelling of trophoblasts during pregnancy w/excess production of chorionic gonatrophin which has intrinsic TSH-like activity form sharing a common TSH alpha-subunit; tx surgery
33

Hypothyroidism due to deficiency of thyroid hormone in infants and children hypothyroidism causes
growth and development retardation; can result in mental and motor retardation
congenital causes include: s agenesis (complete absence of thyroid gland), t hypoplastic thyroid, o thyroid dyshormogenesis and g central hypothyroidism
34
Also known as Myxoedema results from the reduced secretion of T3 and T4 from the thyroid.
Hashimoto’s accounts for over 90% of the cases Secondary hypothyroidism is much less
common and is caused by pituitary disease [ absence of TSH leads to atrophy of thyroid gland]
35
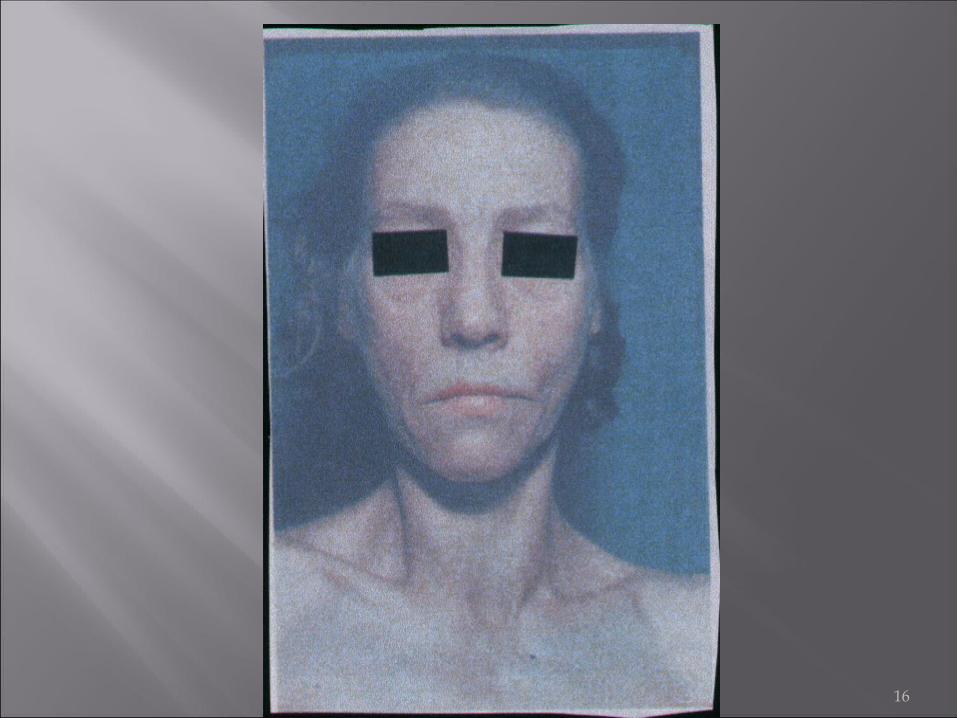
Affects all the systems of the body, but the wide range of clinical features means that the diagnosis will be missed.
Dominant features in children are: Reduction in growth velocity Arrest of pubertal development
Clinical presentation in adults may vary greatly
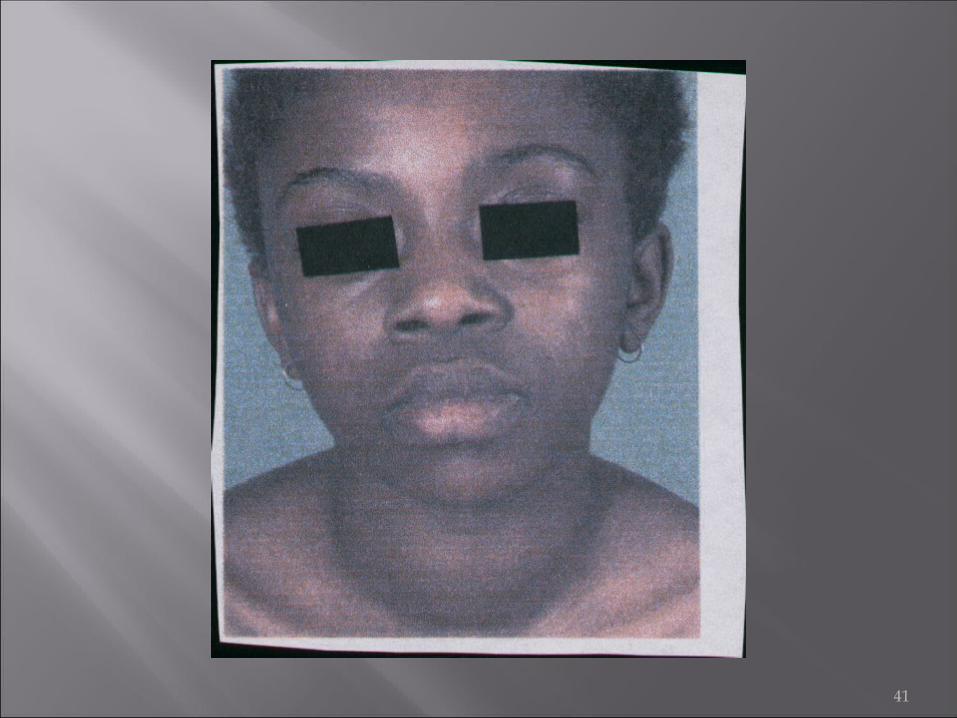
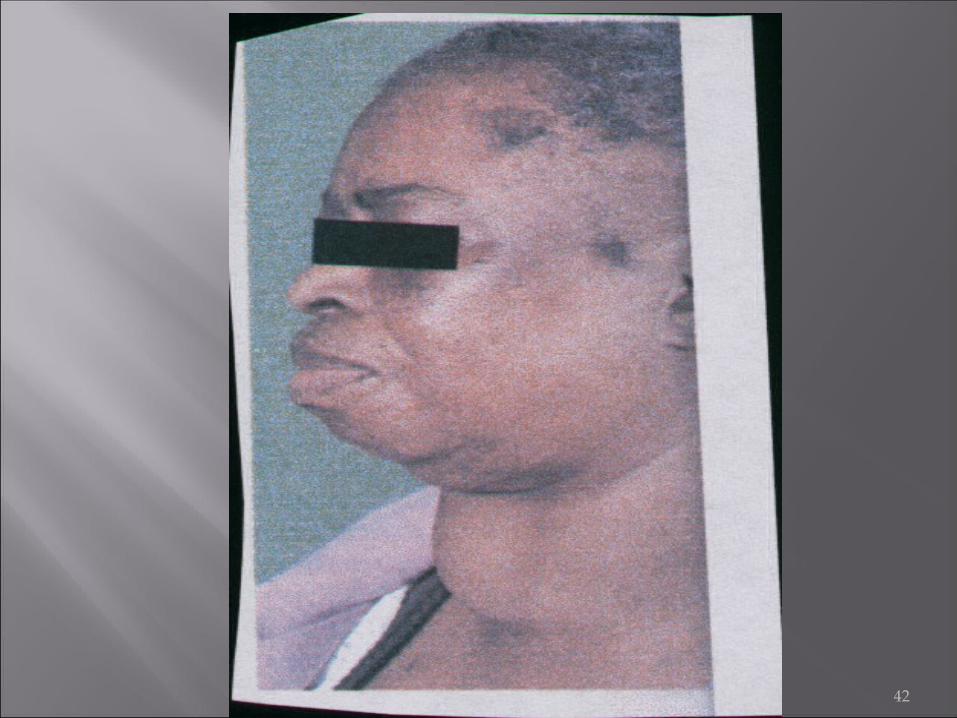
36

Non – pitting edema [most marked on the skin of the eyelids and hands] often associated with loss of eyebrow and scalp hair
Dryness of the skin Reduced body hair Bradycardia Hypothermia Pericardial and pleural effusions [ can occur
and is life threatening]
37
Diagnosis is based on Clinical suspicion Prolonged relaxation time of peripheral reflexes A low voltage EKG Biochemical estimation of T4 and TSH Thyroid Antibodies Assays
Causes of hypothyroidism Autoimmune (most common Hashimotos) Drugs induced (Lithium carbonate- which like
iodide inhibits the release of thyroid hormones goiter and hypothyroidism
38

39

40
41
42
Adult hypothyroidism results in slowed metabolic processes which are reversible w/tx
hypothyroidism is usually primary (thyroid failure), can be secondary (pituitary deficiency) or tertiary (hypothalamus deficiency), or from resistance at thyroid hormone receptor.
In adults, auto-immune thyroiditis (Hashimoto’s thyroiditis) is the most common cause
43

Iatrogenic causes include; 131I tx, thyroidectomy, and tx w/amiodarome or lithium, iodine excess or deficiency can cause hypothyroidism
clinical presentations depends on age of onset infants w/congenital hypothyroidism (cretinism) may
have feeding problems, open posterior fontanelle, hypotonia, and/or edematous hands and face short stature, mental retardation and delayed puberty can
occur if not tx’ed early
44
In adults, hypothyroidism usually develops insidiously S&S: fatigue, lethargy, cold intolerance, weakness,
menstrual abnormalities, cool dry skin, coarse hair or hair loss, wght gain, constipation, brittle nails, delayed tendon reflexes (severe hypothyroidism), myxedema (severe hypothyroidism), bradycardia
severe untreated hypothyroidism can result in myxedema coma S&S: hypothermia, extreme weakness, stupor,
hypoventilation, hypoglycemia and hyponatremia often precipitated by by exposure, infection, psychoacitve
drugs
45
Lab eval serum TSH is elevated, and low free T4 pts w/ mild hypothyroidism; TSH is elevated w/a
low to nl T4 due to pituitary sensitivity to decreased levels of circulating T3 resulting in increased TSH output
TSH levels >8 microU/ml should receive tx w/levothyroxine even w/ nl levels of T4
46
Secondary hypothyroidism has a low or low nl morning serum TSH in the setting
of hypothalamic or pituitary dysfunction often serum total and free T4 are at lower limit of nl secondary hypothyroidism may be due to biologically
inactive, but immunulogically active TSH causing morning TSH levels to be only mildly subnormal or from nocturnal surge of TSH
47
Central (Secondary) Hypothyroidism a diurnal test w/ a mid-night value of serum TSH level
<1.5 times the afternoon value is indicative of central hypothyroidism
Hypothyroidism is associated w/ other abnormal labs
s hypercholesterolemia, e elevated creatinine phosphokinase w/ and increase in
MB bands (fraction characteristic of cardiac muscle), o anemia (normocytic, normochromic but may be
macrocytic (vit B deficiency from pernicious anemia) or microcytic (nutritional deficiency or menstrual blood loss)
48

Hypothyroidism Differential Dx initial S&S of hypothyroidism are subtle early dx depends S&S, early symptoms often
overlooked are: menorrhagia, arthralgias and myalgias
euthyroid sick syndrome: total and occasionally free T4 are low, TSH mildly elevated
must not give these pts levothyroxine can be distinguished from hypothyroidism by absence of
goiter, absence of antithyroid antibodies and elevated rT3 levels as well as S&S
49

Hypothyroidism tx synthetic L-thyroxine
Tri-iodothyronine should be avoided due to rapid absorption and disappearance from stream causing uneven blood levels
therapeutic responses should be evaluated by S&S and TSH levels
pt’s w/myxedema coma: IV L-thyroxine, IV hydrocortisone, IV fluids many pts recover in 2-3days w/full recovery
50
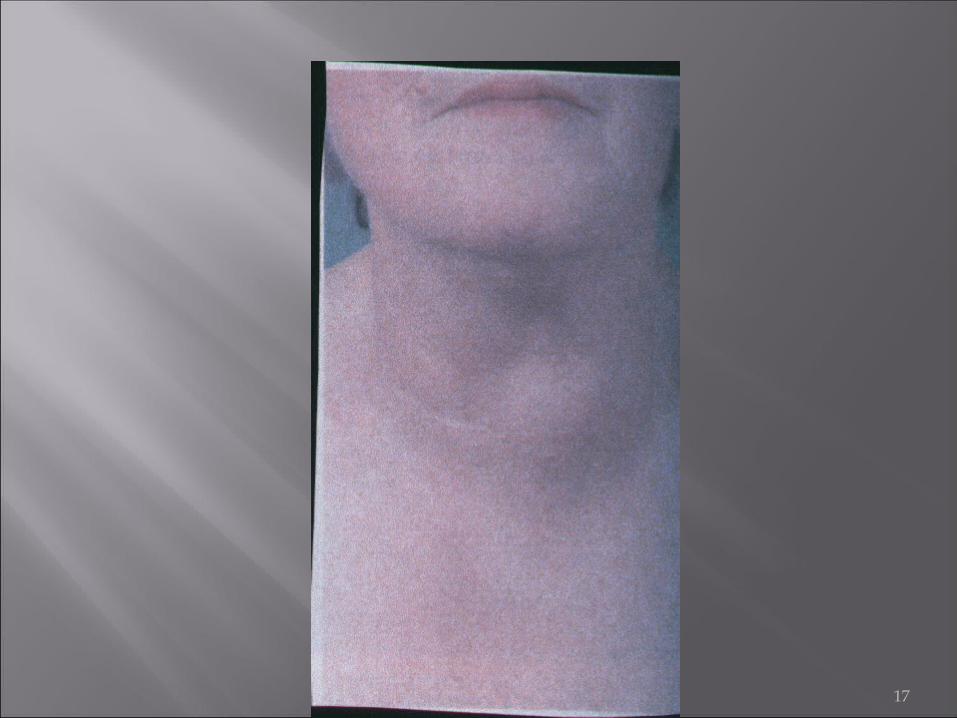
Goiter enlargement of thyroid gland
pt’s may be euthyroid (simple goiter), hyperthyroid (toxic nodular goiter or Grave’s ds) or hypothyroid (non-toxic goiter or Hashimoto’s thyroiditis), may also be focal (adenoma or carcinoma)
in non-toxic goiter; inadequate thyroid hormone synthesis leads to TSH stimulation resulting in an enlarged thyroid gland → iodine deficiency was most common cause hormone replacement quickly shrinks the goiter
51
Dietary goitrogens can cause goiter iodine is most common; lithium, cabbage
goiters may become very large causing respiratory distress, dysphagia, or hoarseness surgery indicated if obstructive symptoms are present
Solitary Thyroid Nodules thyroid nodules are common; detected in about 4% of
population and about 50% at autopsy Benign thyroid nodules are usually benign cyst,
follicular adenomas, nodular thyroiditis, or colloid nodules
52

Although a majority are benign, some are malignant major etiologic factor for thyroid cancer is childhood
or adolescent exposure to head and neck radiation pts w/hx of irradiation should have their thyroids
palpated q 2yrs “cold “lesions require FNA because benign nodules can
be “cold” benign nodules should be tx’ed w/L-thyroxine w/
follow up in 6 months
53
In general, the recommended dosage is:
GOITER: ADULTS: 100-150 (200) mcg daily. CHILDREN UP TO AGE 14: 50-100 (150) mcg daily.
PREVENTIVE TREATMENT FOR RELAPSE AFTER GOITER REMOVAL: 100 mcg daily.
THYROID DEFICIENCY: ADULTS: Initial dose of 50 mcg daily (for approximately two weeks). The
daily dose may be increased by 50 mcg by intervals of approximately 14-15 days until reaching the maintenance dose of 100-200 (300) mcg daily; 2-2.5 mcg/kilo of body weight daily on the average.
SMALL CHILDREN: 0-6 months: 10 mcg/kilo of body weight/day; 6-12 months: 8 mcg/kg of body weight/day; 1-5 years: 6 mcg mcg/kg of body weight/day; 5-10 years: 4 mcg/kg of body weight/ day.
54
Thyroid Carcinoma most common type is papillary carcinoma (60%),
Follicular carcinoma (20%), anaplastic carcinoma (14%), medullary carcinoma (5%) and lymphoma (1%)
papillary carcinoma is associated w/ lymph node spread and local invasion
poor prognosis : thyroid capsule invasion, sz > 2.5 cm, age of onset >45 y/o, tall cell variant, and lymph node involvement
55
Follicular carcinoma is a bit more aggressive than papillary carcinoma
Anaplastic carcinoma occurs in >50 y/o, very aggressive,causes pain, dysphagia, and hoarseness; pt’s die within 1st yr
Medullary carcinoma is derived from calcitonin-producing follicular cells may be sporadic or familial measurement of serum calcitonin levels can confirm
etiology
56

Thyroid Carcinoma tx lobectomy for papillary or follicular carcinomas <1.5
cm in sz pts require lifelong L-thyroxine tx and yearly thyroid
exams anaplastic carcinoma requires an isthmusectomy to
confirm dx and prevent tracheal compression
57

Prognosis of well differentiated thyroid carcinoma is good age of onset most important indicator men >40 and women >50 y/o have higher
recurrence rate of death 5 yr survival rate for invasive medullary carcinoma
is 50% mean survival for anaplastic carcinoma is 6 months
58
The Parathyroid Glands four are situated around thyroid
occasionally one may be in thyroid or in mediastinum Parathyroid hormone (PTH)
secretion is controlled by serum ionized calcium primarily serum level falls → PTH secretion stimulated serum level rises above nl →secretion suppressed main function → defend against hypocalcemia
59

PTH actions bone reabsorption stimulated by osteoclasts
causes release of phosphate and calcium into extracellular fluid (ECF)
stimulation of renal tubular reabsorption of calcium (and magnesium)
inhibition of renal tubular reabsorption of bicarbonate and phosphate
stimulation of synthesis of active form of vitamin D, calcitrol PTH indirectly enhances intestinal absorption of calcium
60

Hypercalcemia common may be found in serious underlying ds or in
asymptomatic patients on routine labs Primary Hyperparathyroidism mcc (metastatic
calcinosis cutis) in adults malignancy mcc in hospitalized pt’s
>90% of pts w/hypercalcemia have either Primary hyperparathyroidism or a malignancy
61
Primary Hyperparathyroidism S&S: CNS: lethargy progressing to coma;
Neuromuscular: proximal muscle weakness, hyporeflexia GI: N/V, anorexia, constipation, peptic ulcer ds (PUD), pancreatitis Renal: polyuria, polydipsia, decreased urine concentration, impaired renal function, nephrocalcinosis, nephrolithiasis Cardiac: HTN, short QT interval, bradycardia, increased sensitivity to digitalis
62

Arthralgias, bone pain, bone cysts, gout , pseudogout due to effects of PTH on bones and joints
Etiol: peak incidence 20-40’s more common in women 85% of cases present w/single parathyroid gland
enlargement (Parathyroid adenoma) can appear as a familial disorder or in association w/
other disorders causing hypersecretion of PTH
63
Labs: serum calcium levels continuously elevated or
intermittently serum phosphate usually low elevated urine calcium levels help distinguish pts
with primary hyperparathyroidism from familial hypocalciuric hypercalcemia
most pts w/primary hyperparathyroidism show no radiographic evidence of bone ds if found, most common finding is osteopenia
64

Primary Hyperparathyroidisn DX is based on finding hypercalcemia w/ an elevate
or inappropriately nl PTH lvl 24hr urine should be done to R/O familial
hypocalciuric hypercalcemia nodule in neck more likely be a thyroid nodule than a
parathyroid adenoma Tx: surgical removal for symptomatic pts
65
Surgical tx for asymptomatic pts when: serum calcium lvl 1.0-1.6 mg/dl above upper limit hx of life threatening hypercalcemia kidney stone found of abdominal x-ray creatinine clearance reduced by 30% reduced bone density >2 standard deviations below age
and sex controls Hypercalcemia of malignancy
occurs in 20-30% of cancer pt’s during course of their injury
66
Hypercalcemia frequently seen in pts w/breast cancer, squamous
carcinoma of hd, neck, lung, and kidney and hematologic malignancies , T-cell lymphomas pts w/malignancies, localized bone destruction often
important cause of hypercalcemia hypercalcemia due to vitamin D intoxication can be due
to excess ingestion of vit D or endogenous production
67
Tx of Hypercalcemia aimed toward reversing underlying abnormality tx indicate if symptomatic or serum calcium levels >
or equal to 13mg/dl hydration furosemide (or etharcrynic acid) loop diuretics facilitate
sodium and calcium excretion glucocorticoids may lower serum lvls calcitonin inhibits osteoclastic bone reabsorption phosphate (caution w/severe hypercalcemia; may
cause metastic calcification
68
Biophosphates inhibit osteoclast mediated bone absorption
gallium nitrate in selected pts w/malignancy dialysis
Hypocalcemia an abnormal reduction in serum ionized calcium
concentration causes: hypoparathyroidism, parathyroid hormone
resistance, Vit D deficiency or resistance, chronic renal failure, hyperphosphatemia, prostate CA, acute pancreatitis, gram-neg sepsis, drugs
69

Chronic renal failure is the mcc of hypocalcemia S&S: often asymptomatic
most frequent symptoms are: neuromuscular irritability, paresthesias (hands, ft, circumoral, muscle cramps)
in severe hypocalcemia bronchospasm, laryngeal stridor, diplopia,
blepharospasm, and seizures QT prolongation, CHF, (+) chovtecks sign, (+)
Troussseu sign
70
Lab findings hypocalcemia due to hypoparathyroidism
characterized by hyperphosphatemia serum PTH is undetectable or inappropriately low for
serum calcium level hypocalcemia caused by malabsorption or vit D
deficiency serum inorganic phosphate lvs are low or nl, serum
PTH increased TX: calcium or vit D, thiazide diuretic in absence of
PTH
71

Adrenal Gland lie at superior pole of each kidney composed of two distinct regions:
cortex medulla
Adrenal cortex three anatomical zones
outer: zona glumerulosa ☛ aldosterone intermediate: zona fascicualata ☛ cortisol inner: zona reticularis ☛ adreanal androgens
72

Adrenal medulla functionally related to sympathetic nervous system
☛ catecholemines (norepinephrine and epinephrine) Synthesis of all steroids ☛ cholesterol Glucocorticoids affect metabolism, CV
function, behavior and inflammatory/immune response
73

Cortisol natural human glucocorticoid secreted by adrenal glands in response to ultradian,
circadian, and stress-induced hormonal stimulation by adrenocorticotropin hormone (ACTH: corticotropin)
plasma levels; highest in morning secretion of ACTH ☛ pituitary; regulated by
corticotropin-releasing hormone (CRH) and vasopressin
74

Glucocorticoids exert negative feedback on CRH and ACTH secretion
Hypothalamic-pituitary-adrenal (HPA) axis interacts w/ and influences function of reproductive, growth, and thyroid axes
Renin-angiotensin system ☛ aldosterone angiotensin II predominant regulator of aldosterone
75

Adrenal androgens dehydroepiandosterone (DHEA) dehydroepiandosterone sulfate (DHEAS) androstenedione
all synthesized in zona reticularis under influence of ACTH
no intrinsic androgenic activity contribute to androgenicity by peripheral conversion to
testosterone and dihydrotestosterone
76
Adrenal insufficiency primary: resulting from destruction or dysfunction
of adrenal cortex secondary: ACTH hyposecretion
Addison’s Disease autoimmune destruction of adrenal glands mcc of primary adrenal insufficiency
glucocorticoid and mineralcorticoids diminished if untreated; fatal approx 70% of pts have antiadrenal antibodies
77

Tuberculosis was formerly mcc of adrenal insufficiency; now account for <20% calcified glands ☛ 50% of cases of tuberculous adrenal
insufficiency Congenital causes : congenital adrenal hyperplasia,
adrenal unresponsiveness to ACTH, congenital adrenal hypoplasia, and two demyelinating lipid metabolism disorders
78

Adrenal insufficiency commonly presents as: weight loss, increasing
fatigue, vomiting, nausea, diarrhea and salt craving muscle and jt pain , abdominal pain, postural
dizziness increased pigmentation (extensor surfaces, creases of
palms, and buccal mucosa) lab: hyponatremia and hyperkalemia, metabolic
acidosis, azotemia, hypercalcemia, lymphocytosis, eosinophilia
79
Acute adrenal insufficiency medical emergency
plasma cortisol level >18 micrograms/dl r/o’s dx of adrenal crisis
<18 micrograms/dl consistent w/ adrenal insufficiency Once dx of adrenal insufficiency is made
need to distinguish between primary or secondary Secondary adrenal insufficiency
results from inadequate stimulation of adrenal cortex by ACTH can be from lesions anywhere in HPA axis or prolonged
suppression of HPA axis by exogenous glucocorticoids
80

Secondary adrenal insufficiency same manifestations as primary; except
no hyperpigmentation, no salt craving, no abnormalities of hyperkalemia or metabolic acidosis
hyponatremia often due to inapproprite ADH secretion which accompanies glucocorticoid insufficiency pt’s w/ secondary adrenal insufficiency due to a pituitary
lesion usually have same labs and symptoms of : hypothroidism, hypogonadism, or growth hormone deficiency
81
Labs Primary adrenal insufficiency: morning plasma
ACTH >50 pico-grams/dl; standing plasma renin >3 nano-grams/ml/hr
Secondadry adrenal insufficiency: morning plasma ACTH < 20 pico-grams/dl; standing plasma renin <3 nano-grams/ml/hr
Secondary adrenal insufficiency occurs commonly after d/c of long term
glucocorticoid therapy
82

Addisons Ds requires life-long replacement of glucocorticoids and
mineralocorticoids initial regimen of 15-20 mg of hydrocortisone in a.m
and 5 mg around 4 p.m mimics physiologic dose mineralocorticoid tx varies greatly
synthetic mineralocorticoid fludrocortisone (florinef) 100 micrograms/dl adjusted to keep standing plasma level above 3 nano-grams/ml/hr
standing plasma rnin level >3 nano-grams w/ pt on correct glucocorticoid dose suggests undertreatment w/ florinef
83

Under stress of a minor illness (nausea , vomiting, or fever >100.5F) hydocortisone dose should be doubled for a short time period
under major stress (surgery or major trauma) 150 mg -300mg of IV hydorcortisone given in 3 divided doses; then rapidly tapering during recovery
pts should wear a medical alert bracelet and instructed in the use of IM hydorcortisone in emergencies
84

Hyporeninemic hypoaldosteronism decreased renin secretion by kidney
hyperkalemia and hyperchloremic metabolic acidosis occurs
plasma sodium concentration usually normal plasma renin and aldosterone are low and
unresponsive to stimuli Diabetes melitus (DM) and chronic tubulointerstitial
ds of kidney are the most common underlying conditions
85
Hypersecretion of glucocorticoid hormone, cortisol, causes Cushing syndrome
Cushing syndrome a metabolic disorder affecting carbohydrate, protein
and lipid metabolism increased production of cortisol seen in physiologic
states: stress, last trimester of pregnancy; chronic strenuous exercise
86
Pathologic states: exogenous or endogenous Cushing syndrome, several psychiatric states (depression, alcoholism, anorexia nervosa, panic disorder, and alcohol or narcotic withdrawal)
Cushing syndrome may be due to exogenous ACTH or glucorticoid tx or endogenous hypersecretion endogenous Cushing syndrome is either ACTH
dependant or ACTH independant
87

ACTH dependant ☛ 85% of cases (pituitary causes of ACTH (Cushing Ds), ectopic sources of ACTH and ectopic sources of CRH
Pituitary Cushing Ds ☛ 80% of ACTH dependant Cushing syndrome
Ectopic ACTH ☛ sm cell lung ca remaining pts have pancreatic, adrenal, or thyroid
secreting tumors of ACTH ACTH independent cases ☛ 15% of Cushing syndrome
( adrenal adenomas, adrenal carcinoma, micronodular adrenal ds & autonomous macronodular adrenal ds
88
Cushing Ds seen in 20-30 y/o
Ectopic Cushing syndrome bimodal age increased incidence in children and
young adults <20 y/o and in 50-60’s usually insidious; mena duration for dx 3-5 yrs
clinical manifestations: centripetal obesity, wasting of arms and legs, rounding of face (moon facies), facial plethora, supraclavicular and temporal filling
89
Proximal muscle weakness menstrual irregularities in females; decreased libido
in males and impotence adult onset acne or hirsutism in females violacious ( purple or dark red) skin striae thinning of back of hands very specific sign in
young adults growth arrest in pediatrics pts, pubertal arrest,
virilization and menstrual irregularities frequently seen
90
Labs elevated plasma alkaline phosphatase,
granulocytosis, thrombocytosis, hypercholesterolemia, hypertriglyceremia and glucose intolerance/DM central hypothyroidism occurs in about 70%
Dx approach initially 90% have a urinary free cortisol (UFC) 24 hr
urine collection >90 micrograms/dl lvl >300 micrograms/dl very specific
91

Pseudo-Cushing states from psychiatric disorders or alcoholism frequently have levels between 90-300 micrograms/dl
ectopic ACTH syndrome and cortisol secreting adenomas or carcinomas frequently have UFC lvls >1000 micrograms/dl cortisol normally secreted in a diurnal fashion: highest
plasma concentration in a.m, lowest around midnight Cushing syndrome similar to normals, afternoon and
evening lvls higher, p.m lvls > 50% of a.m ☛ Cushing syndrome
92
Imaging may be helpful in eval for etiol of hypercortisolism MRI of pituitary CT and MRI of adrenal gland; CT and MRI of chest and
abdomen useful for ectopic ACTH secreting tumors if suspected
Tx surgery of all Cushing syndrome tumors
pituitary Cushing ds tx by transphenoidal surgery (TSS)
93
pts who fail initial pituitary surgery or have recurrent Cushing ds can be tx’ed w/ pituitary radioation almost all pts w/develop panhypopituitarism; so
thyroid, gonadal, and even steroid tx may be needed pt’s w/Cushing Ds who remain hypercortisolemic
after surgery and radiation should undergo B/L adrenalectomy
94
Primary Mineralcorticoid Excess manifested by salt retention, HTN, and metabolic
alkalosis Primary adosteronism can be due to aldosterone-
producing adenoma (75%). B/L adrenal hyperplasia (22%) adrenal carcinoma (1%)
Secondary aldosteronism results from overactivation of the renin-angiotensin system
95
Primary aldosteronism usually recognized during eval of HTN or hypokalemia curable cause of HTN less than 2% of pts w/HTN have primary
aldosteronism Clinical manifestation
HTN, hypokalemia, and metabolic acidosis most presenting symptoms are relate to hypokalemia mild hypokalemic pts have fatigue, muscle weakness,
nocturia, lassitude and HA’,
96

Severe hypokalemic pt’s have polydypsia, polyuria, paresthesias, paralysis and tetany can occur positve Trousseu or Chovstek sign may occur from
metabolic alkalosis BP can range from borderline to severely hypertensive
lvls; rarely malignant HTN DX
hypokalemia in presence of HTN elevated urinary aldosterone lvl >15 microgram/dl and
a suppressed plasma renin lvl <2 nano-grams/ml/hr suggest hyperaldosteronism
97

Basal plasma aldosterone lvl <8 nano-gram/dl is found in nl individuals
lvls 8-20 nan-grams/dl usually found in pt’s w/ B/L adrenal hyperplasia tx’ed w/spironolactone
lvls > 20 nano-grams/dl suggest adrenal adenoma
98
Adrenal Medulla Hyperfunction adrenal medulla synthesizes the catecholamines:
norepinephrine, epinephrine and dopamine from amino acid tyrosine
norepinephrine-the major catecholemine produce by adrenal medulla predominantly has alpha-agonist actions ☛ vasoconstriction
epinephrine acts primarily on beta receptors ☛ inotropic and chronotropic effects on ht ☛ vasodilation, ’s plasma glucose in response to hypoglycemia
99
Norepinephrine synthesized in CNS and in sympathetic postganglionic neurons
epinephrine synthesized almost entirely in adrenal medulla
Hypersecretion of catecholemines produces the clinical syndrome of Pheochromcytoma can occur in any sympathetic ganglion >90% arise in adrenal medulla
100
Pheochromocytoma occurs as part of multiple endocrine neoplasia (MEN) type 2A or 2B syndromes former (Sipple’s syndrome) marked by medullary
carcinoma or thyroid, hyperparathyroidism, and pheochromocytoma
latter characterized by medullary carcinoma of thyroid, mucosal neuromas, intestinal ganglioneuromas, marfanoid habitus and pheochromocytoma
101

Clinical manifestation HTN most common finding
may be associated w/common triad: HA, palpitations, and sweating
other symptoms : flushing, anxiety, nausea, fatigue,, weight loss, abd and chest pain may be precipitated by emotional stress, exercise,
anesthesia, abd pressure, or intake of tyramine containin foods
wide fluctuations in BP may occur HTN if pheochromocytoma usually does not respond
to tx for HTN
102
DX elevated urinary excretion of catecholamines or their
metabolites metenephrines, and vanillylmandelic acid (VMA) lvls checked during periods of HTN measurement of plasma catecholemines may also be
useful plasma norepinephrine lvls >1500 pico-grams/ml or an
epinephrine lvl >500 pico-grams/ml Tx: surgical excision
103















![Papillary thyroid carcinoma coexists with undifferentiated ... · Papillary thyroid carcinoma (PTC) is the commonest thyroid carcinoma worldwide [1], while undifferentiated thyroid](https://static.fdocuments.in/doc/165x107/605714f9a806da25134f71a8/papillary-thyroid-carcinoma-coexists-with-undifferentiated-papillary-thyroid.jpg)


