THROMBOTIC THROMBOCYTOPENIC PURPURA Emily O. Jenkins MD AM Report 10.21.09.
16
THROMBOTIC THROMBOCYTOPENIC PURPURA Emily O. Jenkins MD AM Report 10.21.09
-
Upload
jerome-fox -
Category
Documents
-
view
216 -
download
0
Transcript of THROMBOTIC THROMBOCYTOPENIC PURPURA Emily O. Jenkins MD AM Report 10.21.09.

THROMBOTIC THROMBOCYTOPENIC PURPURA
Emily O. Jenkins MDAM Report10.21.09

Presentation
Nonspecific: Abdominal pain Nausea Vomiting Weakness
½ of patients will have severe neurologic abnormalities such as seizures and fluctuating focal deficits

The Pentad
Microangiopathic hemolytic anemia
Thrombocytopenia, often with purpura but not usually
severe bleeding
Acute renal insufficiency that may be associated with anuria
and may require acute dialysis
Neurologic abnormalities, usually fluctuating
Fever
With the advent of plasma exchange, however, the full pentad is rare Only MAHA and thrombocytopenia without another apparent cause are necessary to initiate PLEX therapy

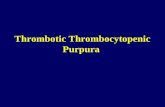
Peripheral blood smear from a patient with a microangiopathic hemolytic anemia with marked red cell fragmentation. The smear shows multiple helmet cells (small black arrows), other fragmented red cells (large black arrow); microspherocytes are also seen (blue arrows). The platelet number is reduced; the large platelet in the center (red arrow) suggests that the thrombocytopenia is due to enhanced destruction.
Fragmented red cells (schistocytes), polychromatophilic red cells (reticulocytes), and a lack of platelets, consistent with the presence of microangiopathic hemolysis.

Epidemiology
Suspected TTP-HUS — 11 cases/million population per
year
Idiopathic TTP-HUS — 4.5 cases/million per year
Severe ADAMTS13 deficiency — 1.7 cases/million per year
Incidence rates are higher for women, african americans
and obese patients
91% of HUS cases in children survive without PLEX therapy
and supportive care only

Renal Disease
Renal thrombotic microangiopathy: usually associated with a urinalysis that is near normal with only mild proteinuria (usually between 1 to 2 g/day) and few cells or casts Chronic renal failure, as defined by a creatinine clearance <40 mL/minute one year after diagnosis, has occurred in about one-fourth of our patients with TTP-HUS

Concentric onion-skin thickening of a muscular renal artery, leading to complete obliteration of the vascular lumen, during the later healing phase of previous fibrinoid injury in any of the forms of the hemolytic-uremic syndrome, including scleroderma and malignant hypertension.
Immunofluorescence microscopy in the hemolytic-uremic syndrome shows fibrin deposition (bright yellow areas) in branches of a muscular renal artery

Subintimal fibrin deposition without inflammation (arrow) in an interlobular artery as can be seen acutely in any of the forms of the hemolytic-uremic syndrome, including scleroderma. The marked narrowing of the vascular lumen will diminish distal perfusion, potentially leading to tissue necrosis if there is near total or total occlusion.
Mucoid intimal thickening of muscular renal arteries (arrows) as an early healing response to previous fibrinoid injury in any of the forms of the hemolytic-uremic syndrome, including scleroderma and malignant hypertension.

Neurologic Symptoms
Present in most patients
Most common are more subtle changes such as confusion
or severe headache
Focal, objective abnormalities (eg, transient ischemic
attack, stroke) are less frequent, but grand mal seizures and
coma can occur
Even in patients with typical TTP associated with severe
acquired ADAMTS13 deficiency, approximately one-third of
patients will have no neurologic abnormalities, confusion, or
headache

Cardiac Involvement
Diffuse platelet thrombi and associated hemorrhage in cardiac tissues (eg, coronary arteries, myocardium, conducting system) May lead to complications such as arrhythmia, sudden cardiac death, myocardial infarction, cardiogenic shock, and/or heart failure in patients with TTP-HUS Incidence of acute heart failure - about 10% High mortality if present (38 versus 17 percent) Acute MI - 18% in one series Lactate dehydrogenase >1000 IU/L + serum troponin I level >0.20 ng/mL at presentation had a sensitivity and specificity of 86% and 95% to predict AMI

A specimen from the heart shows multiple intramyocardial microthrombi, hemorrhage, and early ischemic changes,with scattered foci of contraction-band necrosis.

Causes
Idiopathic — 37 percent
Drug-associated — 13 percent
Autoimmune disease — 13 percent
Infection — 9 percent
Pregnancy/postpartum — 7 percent
Bloody diarrhea prodrome — 6 percent
Hematopoietic cell transplantation — 4 percent

ADAMTS13 Deficiency
VWF-cleaving protease; normally cleaves long VWF
multimers secreted by endothelial cells
Without ADAMTS13, long sticky VWF multimers
accumulate, react with platelets and and cause
formation of disseminated platelet thrombi

In Panel A, in normal subjects, normal ADAMTS 13 molecules attach to binding sites on endothelial-cell surfaces and cleave unusually large multimers of von Willebrand factor as they are secreted by stimulated endothelial cells. The smaller von Willebrand factor forms that circulate after cleavage do not induce the adhesion and aggregation of platelets during normal blood flow. In Panel B, absent or severely reduced activity of ADAMTS 13 in patients with thrombotic thrombocytopenic purpura prevents timely cleavage of unusually large multimers of von Willebrand factor as they are secreted by endothelial cells. The uncleaved multimers induce the adhesion and aggregation of platelets in flowing blood.

Testing for ADAMTS13 Deficiency Assay not always available
Results may take a long time to come back
Assay techniques for ADAMTS13 are not
completely standardized and can yield different
or inconsistent results
However, if present, severe deficiency predicts
an increased risk of relapse

Treatment
** More intensive immunosuppressive therapies includerituximab, cyclophosphamide, vincristine,or cyclosporine.