2nd Year Pathology 2010 Vascular Disturbances II Thrombosis and Embolism.
description

Thrombosis and embolism
By Dr S Homathy

Thrombosis• Thrombosis is the formation of a solid mass
(blood clot) from the constituents of blood– Platelets– Fibrin– Entrapped red cells and white cells• Within the heart or vascular system in a living
organism

• The development of a clot is life-saving when a large vessel ruptures or is severed.
• However, when a thrombus develops within the vascular system, it may be life-threatening

• Thrombosis is the consequence of inappropriate activation ( pathological) of the processes of normal haemostasis

Normal Haemostasis
• Maintain blood in a fluid, clot-free state in normal vessels
• Also inducing the rapid formation of a localized haemostatic plug at the site of injury.
• Both are influenced by – components of the blood vessel wall,– platelets – the clotting sequence.

• The integrity of the blood vessel wall is crucial in normal haemostasis as well as in thrombosis.

Normal Haemostasis Vessel injury –– brief period of arteriolar vasoconstriction
(neurogenic reflex ,endothelin)
• Endothelial injury exposes ECM (highly thrombogenic material).
• Platelets adhere to endothelial cells and ECM, and are activated.

• They release their secretary granules.
• Platelet aggregation occurs forming haemostatic plug (Primary haemostasis)
• Tissue factor (produced by endothelium) activates coagulation –– formation of thrombin which act on finbrinogen to
form fibrin (secondary Haemostsis)

• The process continues to form the permanent plug formed by polymerized fibrin and platelet aggregates.
• At the same time tissue plasminogen activator (t-PA) is formed and it limits haemostatic plug.
• Fibrinolysis is also activated to limit haemostatic plug to the site of injury

Normal Endothelium
• Endothelial cells are activated by injury, infection, plasma mediators and cytokines.
• They have pro-thrombotic and anti-thrombotic functions

Endothelium• The endothelial cells serve to protect against thrombi
formation by
• Anti-thrombotic properties:1. Anti-platelet effect:
– Non activated platelets do not adhere to endothelium.– PGI2, and NO (produced by endothelium) prevent platelet adhesion
2. Anticoagulant properties:– Heparin-like molecule activate anti-thrombin III– Thrombomodulin binds thrombin which activate protein C
(anticoagulant)3. Fibrinolytic properties:
– Endothelium synthesize t-PA (fibrinolysis

Endothelial cells also have the procoagulant properties
• Pro-thrombotic properties:1. Von Willebrand factor:– It enhances binding of platelets to ECM.
2.Tissue factor– Produced by endothelium, it activates extrinsic
clotting pathway3. Plasminogen activator inhibitors (PAI)

Platelets
• Platelets are assigned a central role in normal haemostasis and thrombosis.
• They adhere to sites of endothelial injury,
• aggregate to form platelet masses,

• release granules rich in a variety of secretary products and synthesize several types of prostaglandins.
• In normal haemostasis, platelets adhere to the severed margins of a vessel within seconds to a few minutes.
• The most important stimulus to such adherence is the exposure of collagen fibrils

• Once adhered, platelets release two types of granules:
(1) alpha granules which contain– fibrinogen, – beta thromboglobulin,– cationic protein – platelet factor 4 (a heparin neutralizing protein)
(2) dense bodies, which are rich in– serotonin, – ADP, – ATP – ionized calcium

• Initially, the platelet aggregation forms a temporary haemostatic plug – which is friable and easily dislocated in rapidly
flowing bloodstreams – at this time, the clotting sequence leads to the
formation of thrombin • which is the most powerful platelet aggregator yet
identified

Platelets : (1) provide a temporary plug capable of controlling
blood flow in small vessels in low pressure systems,
(2) initiate the development of a permanent plug composed of aggregated platelets and fibrin,
(3) release serotonin which augments vasoconstriction and
(4) contributes to the coagulation mechanism.

Coagulation system• The coagulation system plays a major role in
normal haemostasis.
• Maintenance of normal fluidity of blood involves the interplay between procoagulants and anticoagulants.
• When the procoagulants dominate and clotting is triggered inappropriately in the intact cardiovascular system,– thrombi result.

• The critical events in blood clotting are the conversion of prothrombin to thrombin
• the subsequent conversion of soluble fibrinogen into the stable fibrin polymer

Thrombosis
Thrombosis is influenced by three major factors:
VIRCHOW’S TRIAD(1) injury to vascular endothelium, (2) alterations in normal blood flow and (3) alterations in the blood
(hypercoagulability).


Endothelial injury• Endothelial injury plays a dominant role in the
formation of thrombi in arteries and in the heart.
• Once the endothelium is damaged, subendothelial collagen may be exposed and
• tissue thromboplastin, etc., is released and
• the sequence of platelet adherence and activation of the clotting sequence follows

Endothelial injury occurs in • myocardial infarction, • ulcerated atherosclerosis, • trauma, and• inflammatory disease of vessels.• Endothelial dysfunction is also a predisposing factor
for thrombosis.
Eg:– Hypertension, – bacterial endotoxins, – hypercholestrolemia, – radiation,– cigarette smoking.

Blood Stasis and Turbulence of FlowTurbulence enhances endothelial injury.Stasis enhances venous thrombosis.
• Both result in:1. Bringing platelets close to endothelium2. Accumulation of clotting factors3. Prevent clotting factors inhibitors4. Endothelial activation Eg:
– aortic aneurysm, – MI, – valve stenosis,– rheumatic heart disease, – hyperviscosity, – sickle cell disease.

Stasis and turbulence
• Distrupt laminar flow
• Prevent dilution of activated clotting factors by fresh flowing blood
• Retard the inflow of clotting factor inhibitors and permits build – up of thrombi
• Promote endothelial cell activation

HypercoagulabilityIt is an alteration in coagulation leading to thrombosis.
• Primary: (genetic)– Factor V mutation– Prothrombin mutation– Antithrombin III deficiency– Protein C or S deficiency

• Secondary:( acquired )
High risk for thrombosis– Prolonged immobilization– Myocardial infarction– Tissue damage– Cancer– Prosthetic cardiac valves– DIC– Lupus anticoagulant
Low risk for thrombosis– AF– Cardiomyopathy– Sickle cell anaemia– Nephrotic syndrome– Contraceptive pills– Smoking

• Increased numbers of platelets, • increased platelet stickiness, • elevated levels of fibrinogen, • increased generation of thrombin, etc.,– have been identified as causing hypercoagulability
in various clinical conditions.

Special categories among acquired causes
1.Heparin-induced Thrombocytopenia: ( HIT syndrom)–When heparin is administered it induces the
formation of antibodies that bind platelets and activate them.
– Occurs when unfractionated heparin is given.– Solution – give low-molecular Wt heparin• Have anticoagulant activity• Do not interact with platelets• Prolonged serum half life

2.Antiphospholipid syndrome (Lupus anticoagulant):– Antibodies to phospholipid (eg. Cardiolipin)– In-vitro: it inhibits coagulation( inhibit assembly
of phospholipid cpx)– In-vivo: it induces coagulation
• Approximately 20% of patients with a recent sroke were found to have anticardiolipin antibody

Morphology
• Thrombi may develop in the heart, arteries, veins and capillaries.
• Arterial thrombi and cardiac thrombi occur at site of endothelial injury or turbulence of flow.
• Venous thrombi occur in areas of blood stasis.
• Thrombi usually are attached to the underlying vessel wall (mural thrombi)

• Arterial thrombi grow back(retrograde
direction) to the heart.
• Venous thrombi grow toward the heart.

• Arterial and cardiac thrombi are firmly attached to the wall
Grossly and microscopically show
– lines of Zahn (layers of fibrin and platelets alternate with layers of RBC and WBC.
– Implies thrombosis at a site of blood flow
• Venous thrombi do no show clear lamination.– Resemble coagulated blood( like clotted in test
tube)

Microscopic appearance of thrombi

• In the heart:– Attached to the underlying structure• Mural thrombi
• common causes: –MI, – dilated cardiomyopathy, – arrhythmia,– myocarditis, – valvular disease.

In arteries:• common causes: – atherosclerosis,– aneurysm.
• Arterial thrombi usually occlude the lumen, • common in – coronary,– cerebral– femoral arteries.

Deep Vein thrombosis (phlebothrombosis) – are almost always occlusive,– Red / stasis thrombi, – 90% occur in lower extremities.– Resemble postmortem clots– Firmer , almost always have a point of attachment– Transection reveal vague strands of pale gray
fibrin

Under special circumstances thrombi may form on heart vales.
• Bacterial and fungal blood-born infection may lead to– valve damage– Development of large thrombotic masses/
vegetations ( infective endocarditis)

• Sterile vegetations can also develop on noninfected valves(NBTE)– Hypercoagulable states
• Libman-sacks endocarditis – Occurs in SLE

Classification of Thrombus according to Color
Pale, formed of platelets and fibrin, small, grayish white, firm
and adherent
Red, formed of red cells and fibrin, dark soft and loosely
attached to the vessel
Mixed, common and has pale and red components
Presence or absence of bacteria Infected or septic
Non infected or aseptic

Sites of Thrombus Formation
1.Thrombus in veins:
More common because of thin wall and slow blood flow:
Thrombophlebitis ----Septic
Phlebothrombosis---- occurs in the veins of the calf Ms and femoral ,iliac veins------ pulmonary emboli
In the varicose veins

2.Thrombosis in Arteries
– less common than veins because of rapid flow and thick elastic wall but occur in arteries affected by:
Atheroma, polyarteritis nodosa and thromboangitis obliterans (roughness of the intima)Aneurysm due to stasisLead to ischaemia

3.Thrombosis in the heart
– more common in the the left sideMural---- occur over infarctionVegetations---- pale over the valveAuricular--- adherent to valve, if detach called ball thrombusAgonal--- red thrombi occurring in Rt. V at the time of death specially lobar pneumonia
• Arterial and cardiac thrombosis possibly embolise to brain, kidneys, spleen

Coronary artery thrombosis

4.Thrombosis in capillaries (very rare):– occur in acute inflammation ,sever cold and frost bite


Fate of thrombus

1-septic thrombus• fragmented by the proteolytic enzymes into
septic emboli causes pyaemic abscesses
2-Aseptic thrombus• its element disintegrate and form a pale red
structure less mass
If mass is small it dissolves by 1).fibrinolysis(dissolution)
If mass is large it undergoes:

2.Propagation (progression)3.Embolization4.Organization and recanalization (inflammation
and fibrosis)

If mass is large it undergoes
Organization: – the thrombus is invaded by capillaries and
fibroblast – change to fibrous mass– lead to permanent vascular occlusion
Organization and Canalization; – some time capillaries dilated and allow Passage of
blood through the thrombus;

Incorporation :– the fibrosed thrombus shrinks from the vascular
wall leaving a space which gets lined by endothelium
Dystrophic calcification– phlebolith
Detachment– aseptic emboli--- infarctions
Propagating thrombus--- due to spread of venous thrombosis


• Propagation– progressive spread of thrombosis– distally in arteries– proximally in veins

• Organisation– reparative process– ingrowth of fibroblasts and capillaries
(similar to granulation tissue)– lumen remains obstructed

Effects of thrombosis
• Arterial– ischaemia– infarction• depends on site and
collateral circulation
• Venous– congestion–oedema– ischaemia– infarction

Post-mortem clots( occur in cardiac chambers after death) there are two types: 1-Red or current jelly clot: –occur when the components of the blood
are evenly distributed throughout the clot. –This type develops when there is rapid
clotting of blood– formed of fibrin ,red and white blood cells

2-Yellow or chicken fat clot:– result from a settling and separation of
erythrocytes from the fluid phase of the blood.– Such clots occur when postmortem clotting is
delayed–which allow sedimentation of red cells with
plasma, fibrin and white cells above.

Venous Thrombosis• Superficial: eg. Saphenous vein– Local congesion, – edema, – swelling, – pain, – tenderness, – ischemia, – risk of infection
Rarely embolize

Venous thrombosis• Thrombosis is commoner in vein than in arteries
• The venous system is capacious, and of low pressure and velocity– Liable to injury
• Two types of venous thrombosis– Phlebothrombosis
• Due to stasis of blood in uninflamed veins• Usually in the calves of the legs
– Thrombophlebitis• Vein wall is inflamed

• Deep Vein Thrombosis: eg. Popliteal, femoral, iliac veins.
– There is a lot of collaterals so the congestion and edema are not prominent.
– 50% are asymptomatic.
–Most serious as itCan embolize

Causes of DVT

• Blood stasis– is common predisposing factor for deep vein
thrombosis. –Mostly in leg veins, whenever the cardiac output is
reduced– Local factors responsible for regional venous stasis

Eg.1. General conditions a.Heart failure, b.Shock due to bleeding, trauma, burn c.low metabolic rate
2. Local causes
a. Lack of muscular activity b. incompetent valves c.pressure from outside
• Also can occur in variety of hypercoagulable state
Eg: pregnancy , cancer (Trousseau syndrome / migratory thrombophlebitis)

• Advanced age• Bed rest• Immobilization– Increase the risk of DVT– Reduced physical activity diminishes the milking
action of muscles in the lower leg and slows venous return

Site affected• Commonly starts in the deep veins of the calf• Then spread to the posterior tibial vein• From here it may extend to involve the – Poplitial, femoral and iliac veins– Even to the IVC– Iliac thrombosis is more common on left side than
right ( compression of L iliac vein by the R common iliac artery)

Pathogenesis of DVTFive stages 1. Primary platelet thrombosis– Following trivial intimal damage platelets
adhere to the vein wall– Aggregate to form a pale thrombus– Stasis is paramount important• Accumulation of clotting factors and • Promote an increase in the Fibrin element-– stabilizes the mass of platelets and leads to
the next stage

2.Coralline thrombus– Primary platelet thrombus encourages further
platelet accumulation– Which take the form of upstanding laminae growing
across the stream– They are bent in the direction of the blood flow by
the force of the stream– These laminae anastomose to form an intricate
structure • Resemble coral



• This is an example of a mixed thrombus• Up to this stage it is possible for the process to
cease

3.Occluding thrombus– Growth of the coralline thrombus progressively
occludes the lumen of the vein.– Causes further stasis– Formation of more thrombus• Which completely occlude the lumen• Trails away from the coralline thrombus in the direction
of the blood flow– This thrombus composed of blood clot with a
smaller platelet element.• Red thrombus

4. Consecutive clot• Once the vein is occluded blood flow stops
– It stops thrombosis• Can occur only in the streaming blood
– Stationary column of blood beyond the occluding thrombus clots to form a consecutive clot.
• Which extends up to the entrance of the next venous tributary

5. Propagated clot• Can occur by two methods
1. Clot when reaches the entrance of the venous tributary• Lead to the formation of another platelet and coralline
thrombus– Occlusion of the ostium of the tributary
• Then a consecutive clot will form up to the osteum of the next venous tributary

2. Sometimes the column of blood above the consecutive clot is so stagnant– Forming one long cord of clotted blood• Anchored only at the site of thrombus formation
– This clot retracts and lies loose in the vein except at its one point of anchorage
– It can easily break off and be carried to the heart as a massive pulmonary embolus.



Morphology
• Long propagated clot or tail – Red in colour–With retraction- thin, pale – Loosly attached
• Head (platelet and coralline thrombus)– Is small– Firmly attached to the vein wall

Clinical features
• Remarkably silent• Tenderness • Pain on passive dorsiflexion of the foot (Homans’s sign)• Oedema distal to the obstructed veins• All the clinical signs are unreliable • Frequently the first indication is the
occurrence of pulmonary embolism.

Venous thrombosis

Specialized diagnostic procedure• Phlebography • Radioactive iodine- labelled fibrinogen test• Doppler ultrasound


Complications
• Massive pulmonary embolism
• Smaller pulmonary emboli, with or withoutpulmonary infarction
• Repeated episodes of silent embolization leading to a syndrome of progressive pulmonary HT

Thrombophlebitis • Inflammation of a vein wall causes damage to the
endothelial lining
• On this platelets are deposisted
• Blood flow is either normal or accelerated
• Thrombosis proceeds to complete obstruction
• Thrombus is so firmly adherent to the wall
• Danger of embolism is negligible except pyogenic inflammtion

DisseminatedIntravascularCoagulation(DIC)
• This condition occurs under two circumstances–Which may be found separately or in
combination1. The release of clotting factors into the
blood stream2. Extensive endothelial damage

• The result is the formation of fibrin in the circulation – This produces vascular obstruction and
micro-infarction– The extensive intravascular coagulation
consumes the coagulation factors• Characteristic features are– Afibrinogenaemia– thrombocytopaenia

Disseminated IntravascularCoagulation(DIC)• Refers to widespread microthrombi formation – in capillaries,– arterioles– venules

• Thrombi are not visible on gross inspection• Leading to circulatory insufficiency: –brain , lung, heart, kidneys

• the development of the multiple thrombi–Although the fibrinolytic system is
activated, it cannot effectively deal with the large deposits of fibrin.
–As a result, there is rapid consumption and eventually a deficiency of clotting factors,
– including fibrinogen, platelets, prothrombin and factor V, VII, and X

Two effects of DIC are • a sever bleeding– a deficiency of• fibrinogen, • platelets and• prothrombin is required for the diagnosis of DIC.
• Tendency to infarction– Primarily microscopic in extent

• DIC have bleeding tendencies on hemorrhagic diathesis.
• Also the widespread occlusion of the microcirculation may induce – signs of shock, – acute respiratory distress, – central nervous system depression, – heart failure or renal failure.
• Affected tissues may not necessarily disclose the microthrombi because of prompt activation of the fibrinolytic system.

Disseminated IntravascularCoagulation(DIC)
A variety of disorders may be complicated by DIC• In abruptio placentae with amniotic fluid
embolism• Intrauterine retention of a dead fetus• Incompatible blood transfusion• After – Sever trauma– Fat embolism– Open-heart surgery

• In the newborn after – Abruptio placenta– Birth asphyxia– Hypothyroidism– Rhesus immunisation
• Sever infection• Purpura fulminans

• Metastatic cancers– Usually of prostate– Occationally of the lung, pancreas stomach
• Acute leukamia• Certain vascular disorders (giant
haemangiomas, aneurysms of aorta and other large vessels, cyanotic congenital heart disease.

Clinical features
• Bleeding ,ecchymosis and haemorrhage from the body’s orifices
• Thrombocytopaenia• Mild haemolytic anaemia• It is an emergency condition– Is treated with transfusion of fresh blood or
fibrinogen

Embolism• Definition
Embolism is the blockage of a blood vessel by detached intravascular – solid, – liquid or– gaseous mass• That is carried by the blood to a site distant from its
point of origin.
Embolus: An insoluble solid, liquid or gaseous mass circulating in blood stream

Virtually 99% of emboli are thrombo-emboli
• Arterial (systemic) emboli
• Venous (pulmonary) emboli

• Rare forms ( non-thrombotic )– fat– Bubbles of air / nitrogen– AS debris (cholesterol emboli)– Tumour fragments– bits of bone marrow– Foreign bodies– Amniotic fluid embolism

Pulmonary Thromboembolism• 20-25/ 100,000 of hospital patients
• 95% coming from DVT (above knee)
• Depending on the size of the embolus it may occlude – main pulmonary artery (Saddle embolus)– in small branches of vessels (multiple)– Paradoxical embolus: • cardiac embolus passing to the right side
through septal defect

Effects of emboli of Thrombotic origin depends upon
Size and nature (septic or aseptic) State of the collateral circulation in affected
organ Aseptic produces transient ischemia if it has
good collateral circulation and infarction if poor
Septic produces pyaemic abscess at the site of impaction

• Size of occluded artery• Number of occluded arteries• Release of pro-thrombogenic vs thrombolytic
factors locally• Background cardiovascular status

Pathophysiological consequences of PE
PE
unperfused but ventilated segment
respiratory compromise
haemodynamic compromise
↑ resistance to pulmonary blood flow

Pulmonary Thromboembolism• Most pulmonary emboli (60-80%) are
asymptomatic because they are small. – most organized and incorporated into the vessel
wall
• Can also lead to right ventricular failure (cor pulmonale) / sudden death.– Cardiovascular collapse occur when 60% or more
of the pulmonary circulation is obstructed with emboli

• Obstruction of medium- sized arteries may result – in hemorrhage, and rarely infarction
• Obstruction of small vessels lead to small infarctions
• Multiple emboli over time may lead to pulmonary hypertension

Pulmonary arterial thrombo-embolism - sequelae
• Resorption and resolution (asymptomatic or transient SOB)
• Organisation → pulmonary hypertension → cor pulmonale
• Pulmonary infarction (pleuritic chest pain, cough, SOB, haemoptysis, hypoxaemia)
• Sudden death




• It is important to differentiate embolus from post-mortem clot
• Post mortem clot is– Moist, shiny and gelatinous– Loosely inserted into the pulmonary trunk– Shape conforms to that of the situation where it is found
• Thromboembolus is– Dry, friable and granular– Already retracted in the leg veins– Ripple of platelets may be visible on its surface– Shape does not conform to that of its surroundings– Tightly inserted into the pulmonary tree
• Removal is difficult

Clinical Features
Massive Pulmonary Embolism• Shock• Dyspnea• Apprehension• tachycardia• Sweating• Chest pain• Faintness• Cyanosis• AF• collapse
• 2/3 die in the first 2 hours.• It is a Medical Emergency

• Dyspnea 73% • Pleuritc Pain 66% • Cough 43% • Leg Swelling 33% • Leg Pain 30% • Hemoptysis 15% • Palpitations 12% • Wheezing 10% • Angina-Like pain 5%

Differential Diagnosis
• Myocardial Infarction.• Dissecting Aortic Aneurysm.• Peumothorax.• Major Pulmonary Collapse.• Shock.• Perforating Peptic Ulcer.• Acute Pancreatitis

Diagnosis of Pulmonary Embolism (PE)
• Clinical picture.• Look for risk or predisposing factors for DVT• Look for ventilation-perfusion mismatch• Testing for PE. – chest radiograph – ECG– Ventilation-perfusion scanning (V/Q scanning). – Angiography– Spiral CT– D-dimer

D-dimer• -A marker for thrombosis and fibrinolysis,• can be useful in the exclusion of PE.
• Specific conditions that will give positive Ddimer tests include – trauma, postoperative state, – malignancies.
• -30% with PE will have normal D-dimer



Systemic emboli
• 80% cardiac– 2/3rd associated with LV wall infarction– 1/4th – dilated left atria- in MS– On the mitral or aortic valves- infective endocarditis/ valvular prosthesis– Cardiomyopathy
• 20% aortic– AS– Aneurysms– Valvular vegetations
• Very small fraction –paradoxical emboli

• Embolization lodging site is proportional to the degree of flow (cardiac output) that area or organ gets, – Lower extremities (75%)– brain (10%), – kidneys – splanchnic – liver

• Consequence depends on the – extent of the collateral supply in the affected tissue– Tissue’s vulnerability to ischaemia– Caliber of the vessel occluded

Effects of systemic emboli
• Ischaemia in various organs• Septic emboli according to anatomical
circumstancesproduce– Pyaemic abscesses– Septic infarcts mycotic aneurysms
• Spontaneous embolistion can occur with aortic AS





Fat Embolism
• A process by which fat emboli passes into the bloodstream and lodges within a blood vessel.
• Fat Embolism Syndrome (FES): serious manifestation of fat embolism occasionally causes multi system dysfunction, the lungs are always involved and next is brain


Causes of FES
• Blunt Trauma – Long bone (Femur, tibia, pelvic) factures

• Non Trauma: agglutination of chylomicrons and VLDL by high levels of plasma CRP.– disease-related
• Diabetes, • acute pancreatitis, • burns, • SLE, • sickle cell crisis
– drug-related• parenteral lipid infusion
– procedure-related• Orthopedic surgery, liposuction

Pathophysiology of FES
Exact mechanism unknown, but two main hypothesis
1. Mechanical Hypothesis
2. Biochemical Hypothesis

Mechanical Hypothesis
Obstruction of vessels and capillaries• Increase in intermedullary pressure forces fat
and marrow into bloodstream• Bone marrow contents enter the venous
system and lodge in the lungs as emboli


• Smaller fat droplets may travel through the pulmonary capillaries into the systemic
circulation and hence to the brain and other organs.
• Embolization to cerebral vessels or renal vessels also leads to central nervous system and renal dysfunction

Biochemical Hypothesis
Toxicity of free fatty acids• circulating free fatty acids directly affect the
pneumocytes, producing abnormalities in gas exchange
• Coexisting shock, hypovolemia and sepsis impair liver function and augment toxic effects of free fatty acids

• hormonal changes caused by trauma and/or sepsis induce systemic release of free fatty acids as chylomicrons.
• Acute-phase reactants, such as C-reactive proteins, cause chylomicrons to coalesce and create the physiologic reactions described above.
• The biochemical theory helps explain nontraumatic forms of fat embolism syndrome and why symptoms take 12 hours to develope.

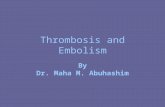
Fat embolism
http://www-medlib.med.utah.edu/WebPath


http://www-medlib.med.utah.edu/WebPath

Clinical Manifestations
• Pulmonary fat embolism
• Systemic fat embolism– Fat emboli enters the systemic circulation

Asymptomatic for the first 12-48 hours
Pulmonary Dysfunction• Respiratory Failure and ARDS (tachypnea,
dyspnea, crackles, cyanosis)• Hypoxemia• systemic arterial hypotension, a decrease in
cardiac output, and arrhythmias

• Systemic fat embolism– Fat emboli enters the systemic circulation – Lodged in the capillaries of the brain, kidney, skin
and other organs– Serious event– Constitutes the fat embolism syndrome– Lungs are certainly always involved

• In sever cases, the patient become comatose within a few hours of injury – Dies with 1-2 days
• Most usually symptoms occur 24-48hours after injury
• Fever, cyanosis, restlessness, respiratory distress, cerebral symptoms

Neurological (nonspecific)• acute confusion, headache, stupor, coma, rigidity or
convulsions• If brain damage is severe, coma and death results
Dermatological Signs• A reddish brown petechial rash - helpful diagnostically– But it is not manifest until the 2nd or 3rd day
• distributed to the upper body, chest, neck, upper arm, axilla, shoulder, oral mucous membranes and conjunctivae
• Subconjunctival and retinal haemorrhages also

Laboratory Studies• Arterial Blood Gases (ABGs)
• Urine and sputum examination– Examination of the urine may reveal fat, the test is
unreliable
• Haemotological Tests– Platelet count is invariably lowered
• Biochemical tests

Imagining• Chest x-ray
– shows multiple flocculent shadows (snow storm appearance). picture may be complicated by infection or pulmonary edema.
• CT Scan brain – may be normal or may reveal diffuse white-matter petechial
haemorrhages
• Helical CT Scan chest– may be normal as the fat droplets are lodged in capillary beds.
Can detect lung contusion, acute lung injury, or ARDS may be evident.

Risk Factors

Gaseous emboli
Air may be introduced into a systemic vein in various situations
• Operations on the head and neck• Mismanaged blood transfusion• During haemodialysis• Insufflations of the uterine tubes

Nitrogen • Enters the circulation in decompression sickness
( caisson disease)• Occurs in people who have been exposed to a high
pressure• Eg :
deep sea divers those encased in a diving bell(caisson) under water tunnellers returns to a normal atmospheric pressure too rapidly

• As the pressure is reduced – Bubbles of air come out of solution from the blood
and interstitial fluid– O2 and CO2 are readily absorbed and removed– Inert nitrogen remains in the tissues for some time• Its presence causes mechanical damage

Clinical features• Prutitus• Severe pain around the joints and muscle(‘the
bends’)• ARDS(‘the chokes’)• Involvement of nervous system– Paralysis– Confusion, seizure, coma and death
• Chronic decompression syndrome–Multiple foci of bone necrosis– arthritis

Amniotic fluid embolism
• Amniotic fluid containing meconium and squamous cells – may enter the uterine veins and travel to the lungs
• Characterized by the sudden onset of respiratory difficulty, cyanosis and shock.