Thrive, not just survive - Quality Forum · 2019-03-01 · Thrive, not just survive … Improving...
24
Thrive, not just survive … Improving staff psychological wellness following critical incidents Simone Prince BSN, RN, CCN February 27, 2019 BREAKOUT SESSION NO. 5 SUPPORTING CARE PROVIDERS TO THRIVE IN DIFFICULT TIMES
Transcript of Thrive, not just survive - Quality Forum · 2019-03-01 · Thrive, not just survive … Improving...

Thrive, not just survive …
Improving staff psychological wellness following critical incidents
Simone Prince BSN, RN, CCN
February 27, 2019
BREAKOUT SESSION NO. 5SUPPORTING CARE PROVIDERS TO THRIVE IN DIFFICULT TIMES

DISCLOSURE
I have no conflicts of interest to disclose.

CONTEXT

CONTEXT
• Health care providers deal with traumatic situations at work
• Heavy workload = little time for recovery
• Experiencing critical incidents frequently can “contribute to staff burnout, which ultimately detracts from care quality”
(Hanna & Romana, 2007, p. 40)

DEFUSING VS. DEBRIEFING
DEBRIEFING
• A formal structured group meeting
• Lead by a trained professional
• May only be necessary in certain situations
• Longer (45+ mins)
DEFUSING
• Happens first• Addresses initial emotional
needs• Recaps the event• Offers a place to discuss
staff’s feelings, and experiences
• Focuses more on emotions than on education
• Assesses need for formal debrief
• Short (15-30 mins)

WHAT WAS HAPPENING?
• No consistent, meaningful process in place to debrief or defuse following critical incidents
• Survey results show the majority of staff members WANTdebriefing or defusing

GOAL
• Our FOCUS is: DEFUSING
• Defusing sessions to be offered after each code blue
• Defusing for staff becomes an expectation post-code blue and becomes part of the unit culture

Why isn’t defusing occurring already?



CODE BLUE

CHECK-IN
Talk with each staff member and set time to defuse within 1-2 hours of the event

SET GROUND RULES
eg. confidential, no-blame culture, safe
space

RECAP OF EVENT
To have everyone in agreement of what occurred, keep brief

THOUGHTS
Everyone has the opportunity to speak,
anyone may pass

ACKNOWLEDGE EMOTIONS
Offer your own emotions about the event “That was an
intense experience…”

TEACHING
“It’s normal to feel this way”
“What went well?”“What can we improve on?”

FINAL THOUGHTS
Need for formal debrief?

0
10
20
30
40
50
60
70
80
90
100
Per
cen
tage
of
Staf
f O
ffer
ed a
Def
usi
ng
Sess
ion
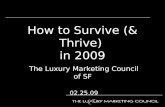
RESULTS
Learning module and algorithm education
done with CNLs
Dates of Code Blues

RESULTS
• What did we learn?
• Algorithm and learning module were a success
• 100% success rate is unrealistic
• What was critical to our success?
– Leadership support
– Advertising
– Staff participation

NEXT STEPS
• Spreading to other units within Providence Health Care

REFERENCES
American Association of Nurse Anesthetists. (2014). Guidelines for critical incident stress management. Retrieved from https://www.aana.com/docs/default-source/practice-aana-com-web-documents-(all)/guidelines-for-critical-incident-stress management.pdf?sfvrsn=ba0049b1_
Canada Border Services Agency. (2006). Critical incident stress management (CISM) program. Retrieved from https://www.cpa.ca/cpasite/UserFiles/Documents/sections/Extremism%20and%20Terrorism/Resources/CISM_MASS_EVENT_B.pdf
Hanna, D.R. & Romana, M. (2007). Debriefing after a crisis. Nursing Management, 38(8): 38-47.
Mitchell, J.T. Critical incident stress debriefing. American Academy of Experts in Traumatic Stress and Clinical Professor of Emergency Health Services. Retrieved from http://www.info-tra uma.org/flash/media-f/mitchellCriticalIncidentStressDebriefing.pdf
Mullan, P.C., Wuestner, E., Kerr, T.D., Christopher, D.P. & Patel, B. (2012). Implementation of an in situ qualitative debriefing tool for resuscitations. Resuscitation, 84(7) 946-951.

CONTACT INFORMATION
Simone Prince
Registered Nurse
Cardiac Surgery Intensive Care Unit (CSICU)
St. Paul’s Hospital
Providence Health Care
Email: [email protected]

QUESTIONS?