Three Rs Approaches in the Quality Control of Inactivated …staging-ecvam.jrc.it/publication/ECVAM...
26
Preface This is the report of the forty-eighth of a series of workshops organised by the European Centre for the Validation of Alternative Methods (ECVAM). ECVAM’s main goal, as defined in 1993 by its Scientific Advisory Committee, is to promote the scientific and regulatory acceptance of alternative methods which are of importance to the biosciences and which reduce, refine or replace the use of labo- ratory animals. One of the first priorities set by ECVAM was the implementation of procedures which would enable it to become well-informed about the state-of-the-art of non-animal test devel- opment and validation, and the potential for the possible incorporation of alternative tests into reg- ulatory procedures. It was decided that this would be best achieved by the organisation of ECVAM workshops on specific topics, at which small groups of invited experts would review the current status of various types of in vitro tests and their potential uses, and make recommendations about the best ways forward (1). The joint ECVAM/AGAATI (Advisory Group on Alternatives to Animal Testing in Immuno- biologicals) workshop on Three Rs Approaches in the Quality Control of Inactivated Rabies Vaccines was held in Langen, Germany, on 19–21 April 2002, under the co-chairmanship of Lukas Bruckner (Institute of Virology and Immuno- prophylaxis, Mittelhäusern, Switzerland) and Klaus Cussler (AGAATI, Utrecht, The Nether- lands). The participants, all experts in vaccine quality control or rabies disease, came from inter- national regulatory or government organisations, national control laboratories, vaccine manufactur- ers and academia. The objectives of the workshop were: a) to review the current status of Three Rs (replacement, reduc- tion, refinement) methods for the quality control of inactivated rabies vaccines; and b) to make propos- als on the best way forward. Three Rs Approaches in the Quality Control of Inactivated Rabies Vaccines The Report and Recommendations of ECVAM Workshop 48 1,2 Lukas Bruckner, 3 Klaus Cussler, 4 Marlies Halder, 5 Jacques Barrat, 6 Peter Castle, 7 Karin Duchow, 8 Donna M. Gatewood, 9 Richard Gibert, 10 Jan Groen, 11 Bernhard Knapp, 12 Robin Levis, 13 Catherine Milne, 7 Simon Parker, 14 Karin Stünkel, 15 Nico Visser 16 and Peter Volkers 8 3 Institut für Viruskrankheiten und Immunprophylaxe, 3147 Mittelhäusern, Switzerland; 4 AGAATI, Yalelaan 17, 3584 CL Utrecht, The Netherlands; 5 ECVAM, Institute for Health & Consumer Protection, European Commission Joint Research Centre, 21020 Ispra (VA), Italy; 6 Laboratoire d’Etudes et de Recherches sur la Rage et la Pathologie des Animaux Sauvage, Agence Française de Sécurité Sanitaire des Aliments (AFSSA), 54220 Malzéville, France; 7 European Department for the Quality of Medicines, Council of Europe, 67029 Strasbourg Cedex, France; 8 Paul-Ehrlich-Institut, Paul-Ehrlich-Strasse 51–59, 63207 Langen, Germany; 9 Licensing and Policy Development, Center for Veterinary Biologics, Suite 104, 510 South 17th Street, Ames, IA 50010, USA; 10 Agence Française de Securité Sanitaire des Produits de Santé (AFSSAPS), Lyon Site, 321 Avenue Jean-Jaurès, 69007 Lyon, France; 11 Institute of Virology, University Hospital Rotterdam, Dr Molenwaterplein 40, 3015 GD Rotterdam, The Netherlands; 12 Chiron-Behring GmbH & Co, Emil von Behring Strasse 76, 35041 Marburg, Germany; 13 Division of Viral Products, Center for Biologics Evaluation and Review, HFM-451, 1401 Rockville Pike, Rockville, MD 20852, USA; 14 Division of Virology, NIBSC, Blanche Lane, South Mimms, Potters Bar, Hertfordshire EN6 3QG, UK; 15 Essex Animal Health, Im langen Felde 5, 30938 Burgwedel, Germany; 16 Intervet International BV, Wim de Körverstraat 35, 5831 AN Boxmeer, The Netherlands Address for correspondence: Dr L. Bruckner, Institut für Viruskrankheiten und Immunprophylaxe, 3147 Mittelhäusern, Switzerland. Address for reprints: ECVAM, Institute for Health & Consumer Protection, European Commission Joint Research Centre, 21020 Ispra (VA), Italy. 1 ECVAM — The European Centre for the Validation of Alternative Methods. 2 This document represents the agreed report of the participants as individual scientists. ATLA 31, 429–454, 2003 429
-
Upload
truongthuy -
Category
Documents
-
view
217 -
download
2
Transcript of Three Rs Approaches in the Quality Control of Inactivated …staging-ecvam.jrc.it/publication/ECVAM...

Preface
This is the report of the forty-eighth of a series ofworkshops organised by the European Centre forthe Validation of Alternative Methods (ECVAM).ECVAM’s main goal, as defined in 1993 by itsScientific Advisory Committee, is to promote thescientific and regulatory acceptance of alternativemethods which are of importance to the biosciencesand which reduce, refine or replace the use of labo-ratory animals. One of the first priorities set byECVAM was the implementation of procedureswhich would enable it to become well-informedabout the state-of-the-art of non-animal test devel-opment and validation, and the potential for thepossible incorporation of alternative tests into reg-ulatory procedures. It was decided that this wouldbe best achieved by the organisation of ECVAMworkshops on specific topics, at which small groupsof invited experts would review the current statusof various types of in vitro tests and their potential
uses, and make recommendations about the bestways forward (1).
The joint ECVAM/AGAATI (Advisory Group onAlternatives to Animal Testing in Immuno-biologicals) workshop on Three Rs Approaches inthe Quality Control of Inactivated Rabies Vaccineswas held in Langen, Germany, on 19–21 April2002, under the co-chairmanship of LukasBruckner (Institute of Virology and Immuno-prophylaxis, Mittelhäusern, Switzerland) andKlaus Cussler (AGAATI, Utrecht, The Nether-lands). The participants, all experts in vaccinequality control or rabies disease, came from inter-national regulatory or government organisations,national control laboratories, vaccine manufactur-ers and academia.
The objectives of the workshop were: a) to reviewthe current status of Three Rs (replacement, reduc-tion, refinement) methods for the quality control ofinactivated rabies vaccines; and b) to make propos-als on the best way forward.
Three Rs Approaches in the Quality Control of InactivatedRabies Vaccines
The Report and Recommendations of ECVAM Workshop 481,2
Lukas Bruckner,3 Klaus Cussler,4 Marlies Halder,5 Jacques Barrat,6 Peter Castle,7 KarinDuchow,8 Donna M. Gatewood,9 Richard Gibert,10 Jan Groen,11 Bernhard Knapp,12 RobinLevis,13 Catherine Milne,7 Simon Parker,14 Karin Stünkel,15 Nico Visser16 and Peter Volkers8
3Institut für Viruskrankheiten und Immunprophylaxe, 3147 Mittelhäusern, Switzerland; 4AGAATI, Yalelaan17, 3584 CL Utrecht, The Netherlands; 5ECVAM, Institute for Health & Consumer Protection, EuropeanCommission Joint Research Centre, 21020 Ispra (VA), Italy; 6Laboratoire d’Etudes et de Recherches sur laRage et la Pathologie des Animaux Sauvage, Agence Française de Sécurité Sanitaire des Aliments (AFSSA),54220 Malzéville, France; 7European Department for the Quality of Medicines, Council of Europe, 67029Strasbourg Cedex, France; 8Paul-Ehrlich-Institut, Paul-Ehrlich-Strasse 51–59, 63207 Langen, Germany;9Licensing and Policy Development, Center for Veterinary Biologics, Suite 104, 510 South 17th Street,Ames, IA 50010, USA; 10Agence Française de Securité Sanitaire des Produits de Santé (AFSSAPS), Lyon Site,321 Avenue Jean-Jaurès, 69007 Lyon, France; 11Institute of Virology, University Hospital Rotterdam, DrMolenwaterplein 40, 3015 GD Rotterdam, The Netherlands; 12Chiron-Behring GmbH & Co, Emil vonBehring Strasse 76, 35041 Marburg, Germany; 13Division of Viral Products, Center for Biologics Evaluationand Review, HFM-451, 1401 Rockville Pike, Rockville, MD 20852, USA; 14Division of Virology, NIBSC,Blanche Lane, South Mimms, Potters Bar, Hertfordshire EN6 3QG, UK; 15Essex Animal Health, Im langenFelde 5, 30938 Burgwedel, Germany; 16Intervet International BV, Wim de Körverstraat 35, 5831 ANBoxmeer, The Netherlands
Address for correspondence: Dr L. Bruckner, Institut für Viruskrankheiten und Immunprophylaxe, 3147 Mittelhäusern,Switzerland.
Address for reprints: ECVAM, Institute for Health & Consumer Protection, European Commission Joint Research Centre,21020 Ispra (VA), Italy.1ECVAM — The European Centre for the Validation of Alternative Methods. 2This document represents the agreed reportof the participants as individual scientists.
ATLA 31, 429–454, 2003 429

The outcome of the discussions and the recom-mendations agreed by the workshop participantsare summarised in this report.
Introduction
Rabies disease
Rabies is a very old viral disease which occurs allover the world, with the exception of several coun-tries, including Australia, Japan and Hawaii, and anumber of Western and Northern European coun-tries, namely Belgium, Cyprus, Denmark, Finland,France, Great Britain, Ireland, Italy, Luxembourg,The Netherlands, Norway, Portugal, the mainlandof Spain, Sweden and Switzerland. Since 1990, thenumber of rabies cases in animals has been reducedby 80% in European countries that have conductedcampaigns to orally immunise foxes; however, theoccurrence of the disease has increased in severalcountries in the continents of Africa, Asia and theAmericas. Each year, the World Health Org-anization (WHO) reports at least 50,000 humanrabies deaths world-wide. The actual number mustbe greater, since the disease is under-diagnosed andunder-reported in many countries (2). Most deathsoccur in countries where rabies is endemic and thedelivery of healthcare is poor. It is difficult to obtainprecise figures on people vaccinated either pre-exposure or post-exposure, but the WHO estimatesthat, each year, 10–12 million people receive one ormore doses of post-exposure rabies vaccine (3).
Rabies is caused by an RNA virus, which is amember of the Lyssavirus genus of the Rhabdo-viridae family. Under the electron microscope, thevirus particles are seen to be bullet-shaped, withspikes on the viral envelope which are composed ofa glycoprotein. The glycoprotein is responsible forthe induction of virus-neutralising antibodies aftervaccination. The core of the virus consists of atightly wound helix of ribonucleoprotein, whichcontains structural proteins, RNA transcriptaseand non-segmented negative RNA.
All mammals, including humans, are susceptibleto rabies. The virus is classically inoculated into thebody by a bite that results in the injection of viru-lent saliva. After a possible local replication, thevirus enters the nervous tissue and is passivelytransported inside the nerve cells to the spinal cordand then to the brain. In the brain, the virus repli-cates, and is then distributed to other organs,including the salivary glands.
In the central nervous system, replication of thevirus will induce clinical signs, depending on theareas that are infected. Some of these signs are quitespecific for rabies, such as hydrophobia in humansand bi-tonal barking in dogs, whereas other signs aremore typical of nervous disorders than of rabies (for
example, convulsions, tetany, and absence of fear ofwildlife toward humans). In the acute stage, signs ofhyperactivity or paralysis predominate. Once theclinical signs are manifest, the disease leads to death.On post-mortem examination, diagnosis can beestablished by the detection of antigens in brainspecimens (immunofluorescence) or of virulent par-ticles with inoculation tests (on cells or mice). It isalso possible to detect RNA in infected tissues, butthis is not recommended by the WHO or the OfficeInternational des Epizooties (OIE) for routine diag-nosis.
Vaccination
Vaccination is the only effective way of controllingrabies. Research began in 1882, when the Frenchscientist, Louis Pasteur, discovered that rabies wastransmitted by agents that were too small to beseen under a microscope. He developed techniquesto cultivate and attenuate the virus in animals, andeventually developed a vaccine which was able toprotect dogs against rabies. He then started to usethe vaccine to successfully treat humans bitten byrabid dogs. The principle of this post-exposuretreatment is that the protective immunity inducedby the vaccine is in place before the virus reachesthe brain.
Today, several types of product are available forthe active immunisation of mammals. There areinactivated vaccines for use in humans and animals,and live attenuated or genetically modified vaccinesfor use in baits for wildlife such as foxes.Immunoglobulins and antisera against rabies arealso used for rapid, passive immunisation in humans.
Regulatory framework for quality control
The quality control of rabies vaccines is regulatedby various guidelines and monographs, for example,on a broad international level by the guidelines ofthe WHO (4) and the OIE (5), on a European levelby the European Pharmacopoeia (Ph. Eur.; 6)monographs, and on an American level by the USCode of Federal Regulations (CFR; 7).
The guidelines outline tests to be performed atthe different stages of production of the vaccines,which are meant to monitor quality and safetyaspects of the vaccine, and, at present, some ofthese prescribed tests require the use of animals.For example, inactivated rabies vaccines are madefrom infectious material, and their production is abiological process and therefore is inherently vari-able. All the processes have to be strictly controlledto ensure a safe, reliably efficacious and consistentvaccine production. Consequently, each batch ofvaccine is checked by a panel of quality controltests. Among them are tests for safety, inactivation,
430 L. Bruckner et al.

pyrogenicity, and potency, which are legally stipu-lated and require the use of animals. Table 1 liststhe tests performed by five companies which pro-duce veterinary rabies vaccines for the Germanmarket.
In practice, a very large number of animals arenecessary, especially for potency testing, with atleast 120 mice being needed for each batch of vac-cine. Table 2 gives an overview of the numbers ofanimals used for batch potency testing by variousmanufacturers and control authorities, which wereprovided by workshop participants.
Current policies on Three Rs alternatives inthe regulatory framework
The European Pharmacopoeia
In the introduction to the Ph. Eur., the EuropeanPharmacopoeia Commission makes a clear state-ment on its commitment to the reduction of animaluse, and encourages individuals involved in phar-macopoeial testing to seek alternative procedures.The European Pharmacopoeia Commission adoptsan alternative or modified method once it has beenclearly demonstrated that it offers satisfactory con-trol for pharmacopoeial purposes (8).
Mechanism for reducing in vivo testing by OfficialMedicines Control Laboratories (OMCLs)
Various guidelines and notes for guidance havebeen written to assist the OMCLs in performing
official control authority batch release testing,which is carried out independently and in additionto tests performed by the manufacturer. By agree-ing to fixed common schedules of testing for specifictypes of products, the OMCL network has enhancedthe transparency of the system and facilitatedmutual confidence between laboratories. The choiceof tests performed is based on scientific knowledgeof the product and the technical experience of theOMCLs, and an important element of the systemrequires that it does not become inflexible and pre-scriptive.
Efforts are ongoing to replace laboratory animalsin routine testing. However, the use of in vivo testsremains an important tool for evaluating certainproducts. Nevertheless, in some cases, the re-per-formance of in vivo tests by the OMCL on every pro-duction batch may not be justifiable as necessaryfor official batch release. OMCLs are encouraged toevaluate their testing procedures, and to identifycandidates for which in vivo testing can be reducedwithout compromising product quality and safety.An OMCL performing batch release testing mightidentify a product where the number of in vivo testsperformed by the OMCL could be reduced. TheOMCL would then prepare a dossier giving thebackground and scientific rationale for this pro-posal, and should also indicate how it intends tomaintain its expertise in the testing procedure inthe light of the reduced batch testing scheme. Theinformation provided should clearly show consis-tency of the product over a significant period oftime.
The frequency of testing should be decided on acase-by-case basis, depending on the method of pro-duction and the characteristics of the material to be
ECVAM Workshop 48: inactivated rabies vaccines 431
Table 1: In vivo final product testing of rabies vaccines for veterinary use, as performed bydifferent manufacturers producing for Germany
Abnormal Safety Inactivation Potency: Potency:Manu- toxicity test test serology challengefacturer test Identity in dogs in mice in mice in mice
A + – + +a – +
B – + + – – +(bulk) (bulk)
C – – + +a – +
D – +b + +a – +(+)c
E – – + + – +
aFinal product and in-process.bPerformed on each sub-batch with reference to (37).cOnly when no safety test in dogs is performed.

tested. It should be sufficiently randomised in orderto ensure effective sampling of batches, and shouldallow for sufficient monitoring of consistency of theproduct.
The final proposal and support documentation iscirculated confidentially within the OMCL batchrelease network for evaluation. If the proposal isapproved by the Member States, the reduced test-ing scheme can be applied by the applicant OMCLand will be recognised throughout the OMCL batchrelease network. The application of this procedureremains confidential within the network and maybe re-evaluated at any time, given an appropriatestimulus.
The USA
Human rabies vaccine lots are submitted to the USFood and Drug Administration (FDA) for release.The release protocols are reviewed, and decisionsfor control testing of a submitted batch are based ondata submitted in the release protocol. To reducethe number of animal-based tests conducted at theCenter for Biologics Evaluation and Review(CBER), the release protocols are evaluated anddecisions for testing are based on product charac-terisation, rather than on a prescribed number oftests. To replace the current animal-based potencytest, the manufacturers would have to submit asupplement to the rabies vaccine license, detailingthe new test and including a validated alternativetest protocol and appropriate data to show therationale for the new test. The CBER would reviewthe submission and determine whether the new testprocedure was an adequate alternative to the exist-ing test.
For veterinary products, the implementation ofan in vitro test can be accomplished if that test hasbeen shown to correlate directly with efficacy. Thisusually requires a dose–response study to prove
that the in vitro test will be able to identify anunsatisfactory product (i.e. one which does not pro-tect vaccinees to an acceptable degree).
The WHO
By 1992, the WHO had already expressed the hopethat the potency tests for inactivated rabies vac-cines in animals would be replaced with an antigenquantification procedure. However, as consensushas not yet been achieved on suitable methods, theactual requirements are still based on the vaccina-tion-challenge test (4).
The Quality Control of InactivatedRabies Vaccines: Potency Testing andThree Rs Approaches
Potency testing
The standard method for potency testing of inacti-vated rabies vaccines is a multiple-dilution vaccina-tion-challenge test in mice, i.e. groups of animals areintraperitoneally (i.p.) immunised with differentdilutions of the test vaccine and, after a given period,the mice are intracerebrally (i.c.) infected with rabiesvirus. The test is evaluated by comparing the num-ber of animals protected from rabies in the groupsreceiving the vaccine under test and the referencevaccine. In general, 50% of the animals die or showsigns of rabies, which involves severe suffering.
The test is generally known as the NIH test, sinceit was initially developed at the National Institutesof Health (USA; 9). Table 3 shows the numerousvariants of the test stipulated for regulatory pur-poses. All of the test methods have in common: theroute of vaccination (i.p.); the route of challenge(i.c.); the challenge virus strain (CVS27); and thedose of the challenge virus used. The most impor-tant difference is in the number of vaccinations, i.e.there are two injections at an interval of 7 days inthe original NIH test, whereas the Ph. Eur. forrabies vaccines for veterinary use stipulates onlyone injection. The number of animals required perdilution and the number of dilutions also differ inthe various requirements, which determine theoverall number of animals needed.
In practice, the NIH test or its variants are used bymanufacturers and control authorities before therelease of each single batch. In addition, the test isused for stability testing by manufacturers and bycontrol authorities according to the WHO require-ments (10). In conducting this testing, manufactur-ers and control authorities are obliged to use largenumbers of mice on an ongoing basis (see Table 2).
The NIH test results are highly variable, and differ-ences of up to 400% in the estimated potency by dif-
Table 2: Numbers of mice used for thebatch potency testing of rabiesvaccines
Number of Manufacturer/control authority animals/year
Rabies vaccines for human useUS control authority 1500–2000European control authority 3000–4200European manufacturer 13,000–19,500
Rabies vaccines for veterinary useEuropean control authority 2000US control authority 1500–3000US manufacturers 30,000–40,000
432 L. Bruckner et al.

Tab
le 3
: P
ote
ncy
tes
tin
g o
f in
acti
vate
d r
abie
s va
ccin
es:
the
NIH
tes
t an
d i
ts v
aria
nts
Inte
rval
Nu
mb
erN
um
ber
In
terv
alb
etw
een
Ob
serv
atio
nN
um
ber
ofN
um
ber
Dil
uen
tof
bet
wee
nva
ccin
atio
nC
hal
len
gep
erio
d a
fter
Cri
teri
a of
tes
tsM
ice
anim
als/
ofto
be
vacc
ina-
vacc
inat
ion
san
d c
hal
len
ged
ose
chal
len
gefo
rre
qu
ired
to b
e u
sed
dil
uti
ond
ilu
tion
su
sed
tion
sa(d
ays)
(day
s)(L
D50
)b(d
ays)
eval
uat
ion
Ph
. Eu
r.fo
r—
Fem
ale
Suit
able
c3
n.s
.2
77
afte
r∼5
05–
14D
eath
or
hum
an u
se (
38)
± 4
wee
ksse
con
dsi
gns
of11
–15g
rabi
es
WH
O (
4)2
13–1
6g≥
165
PB
S2
714
aft
er12
≤25
≤50
> 5
–14
Dea
th(≥
3)fi
rst
Ph
. Eu
r. f
or—
Fem
ale
≥10
≥3
n.s
.1
n.a
.14
∼50
5–14
Sign
s of
vete
rin
ary
use
(33)
≥4
wee
ksra
bies
SAM
0308
.01
1F
emal
e16
5P
BS
27
± 1
14 ±
112
–50
6–14
Dea
th o
r(1
5)(3
, wh
enC
F-1
afte
r fi
rst
sign
s of
repe
ated
)13
–15g
rabi
es
OIE
(5)
—3–
4 w
eeks
≥10
n.s
.n
.s.
1 or
27
if14
day
s≥
10n
.s.
n.s
.ap
plic
able
late
r
9CF
R2
13–1
6g≥
165
PB
S2
714
aft
er12
≤25
≤50
> 5
–14
Dea
th11
3.20
9 (7
)(≥
3)fi
rst
Sim
plif
ied
sin
gle-
—F
emal
e10
1—
1n
.a.
14?
14≥
80%
dilu
tion
tes
t (1
2)su
rviv
al
a In
ject
ion
vol
um
e: 0
.5m
l; i
nje
ctio
n r
oute
: in
trap
erit
onea
l.b C
hal
len
ge v
iru
s: C
VS
27; c
hal
len
ge r
oute
: in
trac
ereb
ral;
in
ject
ion
vol
um
e: 0
.03m
l.c A
su
itab
le n
um
ber
of a
nim
als
shou
ld b
e u
sed
to m
eet
the
stat
isti
cal
requ
irem
ents
for
a v
alid
tes
t.
n.a
. = n
ot a
ppli
cabl
e; n
.s. =
not
spe
cifi
ed; P
BS
= p
hos
phat
e-bu
ffer
ed s
alin
e.
9CF
R =
US
Cod
e of
Fed
eral
Reg
ula
tion
s, T
itle
9; N
IH =
Nat
ion
al I
nst
itu
tes
of H
ealt
h; O
IE =
Off
ice
Inte
rnat
ion
al d
es E
pizo
otie
s; P
h. E
ur.=
Eu
rope
an P
har
mac
opoe
ia;
SA
M =
Su
pple
men
tal
Ass
ay M
eth
od; W
HO
= W
orld
Hea
lth
Org
aniz
atio
n.
ECVAM Workshop 48: inactivated rabies vaccines 433

ferent laboratories are considered to be acceptable.For example, Ph. Eur. monograph No. 0216 statesthat, for the evaluation of the potency test, the fiduciallimits of error (p = 0.95) should not be less than 25%and not more than 400% of the estimated potency.
As an example, the Ph. Eur. Biological ReferencePreparation (BRP) Batch Number 3 for rabies vac-cine (inactivated) for veterinary use (RVIVU) wasrecently established in a collaborative study (11),which involved an immunogenicity test based onthe NIH test, in which mice were vaccinated andthe protection obtained was measured by subse-quent i.c. challenge with live rabies virus. Thepotency of the reference preparation was calculatedin international units (IU) by comparing it in paral-lel to the protection evident in mice vaccinated withthe 5th International Standard for rabies vaccine.The data showed that potency estimates from indi-vidual assays were highly variable, and when valid-ity criteria were strictly applied on individualassays, data from five out of the eight laboratorieshad to be excluded. The high variability and the dif-ficulty of obtaining valid results in individual testsillustrate the disadvantage of using this in vivo testand emphasise that serious effort should be made,by using newly available technologies, to develop amore robust test that would be more reliable andwould reduce the number of animals required (11).
The data provided for a 2-year period by the rep-resentative of a vaccine manufacturer at the work-shop showed a standard deviation of 45% in 24 NIHtests carried out with the reference vaccine, and115% when 38 NIH tests were carried out.
Conclusion
The current potency tests require a large number ofanimals and inflict great suffering on them. Thetests are time-consuming and pose a risk of infec-tion to the laboratory staff. There is an urgent needfor a more reliable test, which uses fewer animals,involves less suffering and provides more-consis-tent results.
The disadvantages of the NIH test and its vari-ants and, in particular, their high variability andthe frequency of invalid results, make it very diffi-cult or even impossible to demonstrate a good cor-relation between in vitro and in vivo data. Its use asa “gold standard” for the validation of in vitromethods is therefore not recommended.
Possibilities for reduction
Single-dilution test
A simplified form of the multiple-dilution vaccina-tion-challenge test, i.e. a single-dilution test, can be
used as a screening test, once experience has beengained in a given laboratory. This test (12) does notgive a precise value for the vaccine, but each vaccinethat passes this test at least satisfies the minimalrequirements for potency. A multiple-dilution testmust be applied where a vaccine fails the screeningtest. This testing strategy can lead to a considerablereduction in the number of animals used.
Single-dilution tests are generally performed in acontrol session that includes other vaccines testedwith “complete” tests. This permits the same refer-ences to be used, thus reducing the numbers of ani-mals required.
Since most laboratories have abundant data onthe performance of the multiple-dilution test, areview of the historical data should enable the sin-gle-dilution test to be introduced on this basis formany rabies vaccines. However, it must be recog-nised that this testing scheme may not be applica-ble to all the rabies vaccines on the market.
This strategy has already been implemented inFrance for veterinary rabies vaccines. During a 3-year period (from 1999 to 2001), 203 batches ofveterinary vaccines were tested in 74 control ses-sions. The single-dilution test was performed on 53vaccine batches, which saved 1590 mice.
Recommendations1. National control authorities should follow the
French approach, and should investigatewhether the single-dilution test could be intro-duced in their laboratories for the batch potencytesting of veterinary rabies vaccines.
2. Whether this testing strategy could also beapplied to rabies vaccines for human use shouldbe evaluated.
Number of animals per group
At present, the regulatory requirements differ in thenumber of animals to be used (Table 3). Somerequirements give the exact number to be used,whereas others specify a minimum number or thenumber is not specified, but it is indicated that theminimum number to meet statistical validity require-ments should be used. The present practice is to usethree to five groups of equal size, i.e. 10–16 animalsper group, for the test and reference vaccines.
Recommendation3. Depending on the type of assay used and the
information already available, the use of equallysized groups is not essential in all cases.Therefore, all available information should beused in an optimised way to minimise the num-ber of animals needed for the selection of dosesand/or group sizes. Furthermore, statisticalmethods such as Bayesian methods or sequential
434 L. Bruckner et al.

approaches, which sometimes provide for more-efficient use of the data, should be consideredwhen planning an in vivo test.
Verification of the challenge dose
The current requirements stipulate that the chal-lenge dose has to be verified for each assay. It mustbe high enough to kill 100% of the control animalsreceiving the working dilution. According to the Ph.Eur., groups of ten mice are inoculated i.c. withserial dilutions of the challenge virus strain.
Recommendations4. Whenever it is feasible, the potency testing of
several vaccine batches should be performed inparallel. Thus, only one test for verification ofthe challenge dose and the reference vaccinewould be needed, and the total number of ani-mals used would be reduced.
5. It should be investigated whether the number ofanimals per group and the number of dilutionscould be reduced.
Frequency of testing
The WHO and FDA require two tests for the potencytesting of rabies vaccines for human use. Althoughthe Ph. Eur. does not stipulate two tests, manyEuropean manufacturers perform the potency testtwice, in order to meet the requirements of non-European vaccine-importing countries.
Recommendation6. Only one potency test should be performed,
since a second test does not contribute to thetest precision. The WHO and the FDA shouldmodify their requirements accordingly.
Possibilities for refinement
Immunisation and challenge dose
As an alternative to the classical NIH test, a testinvolving subcutaneous immunisation and intra-muscular challenge was proposed by severalresearch groups (13). However, intramuscular chal-lenge was difficult to reproduce in different labora-tories. Due to this disadvantage, furtherinvestigation of this approach was halted.
The use of anaesthetics
Intracerebral injection is considered to be a verysevere and painful procedure, which could be some-
what improved with the use of anaesthetics.Currently, the anaesthetisation of mice prior to i.c.injection is only recommended by the WHO for testsfor diagnostic purposes (14), and none of therequirements for the quality control of rabies vac-cine stipulates the use of anaesthetics.
Recommendation7. All regulatory authorities and other relevant
organisations should stipulate the use of appro-priate anaesthetics (for example, halothane,isoflurane) in their guidelines, in order to reducethe pain and distress caused by i.c. injection.
Intracerebral injection technique
Inappropriate i.c. injection may cause severe dam-age and death of the mice. This fact is reflected inall of the regulations, which consider death within 4days of injection to be non-specific. There is someguidance on the injection technique in the WHOManual (14) and in the US Department ofAgriculture (USDA) Supplemental Assay Method(SAM; 15). However, it became evident during thediscussion at the workshop that the procedureneeds a lot of experience, and that the proper per-formance may even be restricted to very few per-sons or even a single person.
Recommendation8. Scientists and technicians should be trained in
appropriate i.c. injection techniques. A BestPractice Guide agreed by the workshop partici-pants is presented in Appendix 1.
Criteria for evaluation of the potency test
As shown in Table 3, the various guidelines andmonographs differ in their criteria for test evalua-tion, and they stipulate death, death or signs ofrabies, or signs of rabies, as the endpoint. The Ph.Eur. and Title 9 CFR (9CFR) allow the use of non-lethal endpoints in order to reduce the suffering ofthe mice. The WHO Manual and the USDA SAMmention convulsions and paralysis as clinical signs.The clinical signs of rabies are progressive, and itmay take 2–6 days for an animal to die once theyhave begun. Due to the severe course of rabiesinfection in mice and the suffering involved, deathis not an appropriate endpoint.
In a recent study, it was investigated whetherclinical signs, body weight and body temperaturecould be used as non-lethal endpoints. It was foundthat clinical signs, such as ruffled fur, shaky move-ments, trembling, and convulsions (combined witha significant reduction in body weight) form a reli-able indicator for the lethal outcome of the rabiesinfection and could therefore be used as non-lethal
ECVAM Workshop 48: inactivated rabies vaccines 435

endpoints (16). Appendix 2 summarises the studyand gives guidance on the application of non-lethalendpoints (for example, identification of the mice,use of score sheets, and frequency of monitoring).
Recommendations9. Only non-lethal endpoints should be used as
criteria for test evaluation. Clinical signs offerthe possibility of terminating the potency testas soon as typical signs of neurological disorderare evident (for example, shaky movements,trembling, and convulsions), without any lossof scientific data, but avoiding a slow progres-sive death for the animals.
10. Scientific and technical staff should be trainedin the application of non-lethal endpoints. Thevideo on non-lethal endpoints for the potencytesting of rabies vaccines, which has been pro-duced by the Humane Endpoints — LethalParameters (HELP) Group (17), could be usedfor training purposes (see also, Appendix 2).
Possibilities for replacement
Current status of replacement alternatives
There is an urgent need for replacement of the NIHtest and its variants for batch potency testing, sta-bility testing and in-process testing. The ideal invitro test should measure the functional glycopro-tein which induces the production of rabies virusneutralising antibodies. It should be better than thecurrent in vivo test and as good as the currentlyused in-house in vitro methods and, ideally, itshould recognise all vaccine strains, whether or notin combination with an adjuvant.
Various alternative methods have been developedand reviewed by Meslin & Kaplan (13) and Weisser& Hechler (18). These methods are either based onthe estimation of rabies virus neutralising antibod-ies in the serum of immunised mice or on the quan-tification of rabies virus antigen in the vaccine.Table 4 gives an overview on the current status ofthese methods, and summarises their advantagesand disadvantages.
Alternatives based on the quantification of neutralising antibodies (serology)
Various serological tests allow the quantification ofrabies virus neutralising antibodies in the serum ofimmunised animals. The rapid fluorescent focusinhibition test (RFFIT; 19) and the fluorescentantibody virus neutralisation test (FAVN; 20) arethe reference methods recommended by the WHOand the OIE. Serially diluted test sera are pre-incu-
bated with a given amount of rabies virus prior toinoculation on a sensitive cell culture, i.e. BHK-21cells. After incubation, the quantity of unneu-tralised rabies virus is revealed by immunofluores-cence.
According to the Ph. Eur., the RFFIT may beused for inactivated veterinary vaccines after asuitable correlation with the mouse challenge testhas been established. However, in practice, no man-ufacturer uses the serological method, for the fol-lowing reasons.
a) The serological assay in mice, as described inthe monograph, has to be performed 14 daysafter single immunisation with one-fifth of therecommended dose. This test has never beenvalidated, and the data provided by partici-pants revealed that the method in this form isnot suitable. This may be due to the short timeperiod between vaccination and blood sam-pling. Other approved serological assays (forexample, the ToBI test for tetanus vaccinepotency, and the ELISA for erysipelas vaccinepotency) involve a longer time period (> 21days).
b) As already mentioned in the introduction to theNIH test and its variants, the test has manydisadvantages, which make it difficult to estab-lish a good correlation between in vivo data andserological data.
Since these serological methods still require the useof animals, they are not complete replacementalternatives. It should also be considered that theantibodies estimated shortly after vaccinationmight not correlate directly with protection againstrabies. Further disadvantages are the high degreeof individual animal variability, the duration of thetest (up to 3 weeks), the need to handle infectiousrabies virus, and the need for a category III labora-tory.
If using serological methods for potency testing,and provided that the safety testing in the targetspecies (see below) will still be required in future,the animals involved could be used to provide bloodsamples for a serological potency estimation, espe-cially if they were immunised with the recom-mended vaccination dose. Despite the statisticallylow number of animals used in this test, the datareceived from two or three animals of the targetspecies may be more relevant than data from a lab-oratory animal test which requires far higher ani-mal numbers.
Alternatives based on antigen quantification
The antibody binding test (ABT) was developed atthe beginning of the 1970s, and became a WHO pro-
436 L. Bruckner et al.

tocol in 1973 (21). Serial dilutions of antigen aremixed with a constant dose of specific antiserum, andthe amount of unbound antibody is determined bytitration against live virus by using the RFFIT (22),which has several disadvantages, as listed above.
The single radial immunodiffusion (SRD) testwas first described by Ferguson et al. in 1984 (23).The rabies virus contained in the vaccine is split bymeans of a detergent, and the concentration of freeglycoprotein is then estimated by measurement ofdiffusion zones in a gel containing antibody specificfor the glycoprotein. The SRD test is accepted inAustria for batch release testing of inactivatedrabies vaccines for human use (24). The results of arecently conducted collaborative study in SouthAmerican and Caribbean laboratories showed thatthe SRD test can be easily standardised and usedfor in-process control (25). It is rapid, inexpensiveand does not require special equipment.
Several types of ELISA procedures have beendeveloped over the past decade (Table 4), and the
following variants can be distinguished: antigencapture assays involving either polyclonal or mono-clonal antibodies (mAbs), antigen competitionassays, and direct ELISA systems. The majoradvantages of ELISAs are that they are rapid,robust, precise, inexpensive, highly reproducibleand quantitative. Depending on the mAb used inthe system, it might be possible to differentiatebetween the vaccine strains. The mAbs which arecurrently available are described in Table 5.
There are currently several studies in progresson the potential use of these ELISA proceduresfor the potency testing of rabies vaccines. AnELISA competition assay test is now commerciallyavailable, which measures residual vaccine prod-uct after incubation with defined antibodies thatrecognise either the viral glycoprotein or the viralnucleoprotein (unpublished data). A direct ELISAhas been developed by binding the test vaccinedirectly to the surface of the plate in the presenceof detergent. The antigen content is measured
Table 4: Potency testing of inactivated rabies vaccines: summary of alternatives to the NIHtest and its variants
Refer-Status ence Advantages Disadvantages
Antibody quantificationRapid fluorescent focus WHO method 19 — still use animalsinhibition test (RFFIT) OIE method 5 — serology (shortly after
Ph. Eur. method 33 vaccination) is not directly correlated to protection
— high degree of individualFluorescent antibody virus WHO method 20 — good interlaboratory animal variabilityneutralisation test (FAVN) OIE method 5 reproducibility — require up to 3 weeks
— must be done in a category III laboratory
Antigen quantificationSingle radial diffusion WHO method 23 — inexpensive — does not differentiate
Accepted in Austria 24 — does not require — does not detect protective for batch release special equipment epitopes of the vaccines
— cannot be used for adjuvantedvaccines
— relatively insensitive— requires 3 days
Antibody binding test WHO method 21 — difficult to validate— 3-day long test— precision is less than ELISA— process cannot be automated
ELISA procedures 39 — fast — product-specific (not standardised40 — inexpensive across products)41 — highly reproducible — reagents, by definition, are not 42 — robust universally available
— quantitative— precise
OIE = Office International des Epizooties; Ph. Eur. = European Pharmacopoeia; WHO = World Health Organization.
ECVAM Workshop 48: inactivated rabies vaccines 437

with mAb TW-1 or mAb TW-17 (see Table 5). Thedirect ELISA method is currently being evaluatedin several laboratories. A third test in develop-ment is a capture ELISA that utilises a polyclonalantiserum against the rabies glycoprotein. Thebound vaccine is then quantified with mAb TW-17. This test is being developed in a collaborativeresearch study. When this study is completed, thistest and the necessary reagents will be madeavailable for a defined collaborative study involv-ing more institutes. Other ELISA tests in thecourse of development involve the use of mAbs asboth capture and detecting reagents.
The Ph. Eur. monograph on veterinary rabiesvaccines permits the replacement of the in vivopotency test for batch release testing by a suitablevalidated alternative. Methods based on antigenquantification are widely used for in-process controlby manufacturers and also by OMCLs; for example,the French and Austrian control authorities usethem for batch release testing. However, the possi-bility offered by the Ph. Eur. monograph on veteri-nary rabies vaccines to use the quantification ofrabies virus glycoprotein for batch release testinghas not yet resulted in variations. All companies (atleast those which produce for the German market)only use the animal test (Table 1).
Conclusions All of the ELISA procedures have promising prop-erties, but none in their current form could beapplied universally across vaccines. While a single
uniform test that could measure the potency ofboth human and veterinary vaccines would beideal, technical limitations may require the devel-opment of product-specific or strain-specificassays.
Recommendations11. A pool of potential tests and reagents are now
available. Industry, and control and otherlaboratories should use it for further collabo-rative evaluations of alternatives based onantigen quantification.
12. With regard to the validation of antigenquantification-based alternatives to the NIHtest and its variants, several important issuesshould be considered: a) whatever test isselected should measure an antigen that cor-relates with protection; b) an acceptableassay should be able to distinguish potentversus sub-potent batches; and c) the devel-opment of an alternative assay shouldinclude a definition of potency and the desig-nation of an international standard based onantigen mass units.
13. As the use of the in vivo potency test as a“gold standard” in developing an in vitroreplacement method is not recommended,criteria for the acceptance of alternativemethods should be defined.
Table 5: Monoclonal antibodies used for the antigen quantification of rabies vaccines
Monoclonalantibody Characteristics Reference
TW-17 Murine Available from Chiron-BehringDerived against LEP Flury laboratory strain (after agreeing to a materialSpecific for the rabies glycoprotein transfer agreement), for useNeutralising activity in test developmentNo cross-reactivity to other reagents in the vaccine
TW-1 Human Available from Chiron-BehringDerived against LEP Flury laboratory strain Enssle et al. (43)Specific for the rabies glycoproteinNeutralising activityThe only monoclonal antibody which binds antigen
2-22-C5 Murine Used in two commercial ELISADerived against Pitman Moore strain kits from EVL and MeddensSpecific for the rabies glycoprotein, directed against site 2 DiagnosticsNeutralising activity Bunschoten et al. (44)Reacts also with Pasteur, Flury and SAD strains
D1 Murine Lafon (45)IgG 1-type monoclonal antibodySpecific for the rabies glycoprotein, directed against site 3Neutralises lyssaviruses belonging to genotype 1 and genotype 6
438 L. Bruckner et al.

The use of national and international standards inpotency testing
Potency estimation of a vaccine batch with the NIHtest and its variants is always performed in compar-ison with a reference preparation, which is calibratedin IU. The reference preparation can be an interna-tional or national standard, and in Europe, the BRPis used. A recent collaborative study to establish Ph.Eur. BRP No. 3 (11), emphasised the high variabilityof the in vivo assays, as described above in the intro-duction to NIH tests and its variants.
Some evidence indicates that reference prepar-ations calibrated in vivo might not be appropriateas references for in vitro methods based on antigenquantification, since the manufacturers use anti-genically different virus strains for the productionof their rabies vaccines (4). For example, the WHO5th International In Vivo Standard was also cali-brated for in vitro tests, but the IU values obtainedwere somewhat confusing — the same standard wasassigned 16IU and 50IU, depending on the test usedfor estimation (26).
ConclusionThe development of in vitro methods will mostprobably require the development of new referencepreparations.
Recommendations14. Despite the fact that national and international
standards or reference preparations calibratedin vivo may not be suitable for potency testingwith in vitro methods, it is recommended thatfuture collaborative studies for their establish-ment could be used to evaluate, in parallel, can-didate in vitro methods, in order to gaininformation and experience with these meth-ods and to encourage the phasing out of the invivo tests.
15. Standards which were calibrated in vivo shouldnot be used as reference preparations in invitro tests. Specific standards should be cali-brated for this purpose, once an in vitro methodhas been established.
The Quality Control of Inactivated RabiesVaccines: Safety Testing and Three RsApproaches
Possibilities for deletion
The abnormal toxicity test/general safety test
The purpose of the abnormal toxicity test (ATT) ofthe Ph. Eur. (called the general safety test in the
CFR, or the innocuity test in the WHO guidelines)is to detect any toxicity which is not related to theproduct. A controversial discussion about the use-fulness of this test went on for many years (27, 28).As a consequence of a detailed study of the PaulEhrlich Institute (Langen, Germany) on the rele-vance of this test (29), the Ph. Eur. has abolishedthe ATT as a routine batch control test (28).
The WHO still requires the test, but the WHOExpert Committee on Biological Standardisationrecently recommended the initiation of an interna-tional enquiry to establish the usefulness of theATT (30). The CFR still requires a general safetytest or an ATT for all batches of human rabies vac-cine submitted for release.
For veterinary vaccines, the use of the ATT hasbeen abolished in Europe. However, elimination of thetest from routine quality control is obviously a veryslow process. Even 5 years after the decision to deletethe test came into force, some companies still performthe test (see Table 1). The 9CFR 113.209 for veteri-nary rabies vaccines also does not require an ATT.
Recommendations16. In the interests of international harmonisation,
the deletion of the ATT/general safety testshould be considered.
17. National control authorities, being responsiblefor batch release testing, should demand thatcompanies which are still performing the ATTshould cease to do so.
Possibilities for reduction and refinement
The target animal safety test (TAST) for vaccinesfor veterinary use
Both the Ph. Eur. and the 9CFR 113.209 requiresafety testing in target animals; however, the testsdiffer in detail (Table 6). The OIE does not mentiona TAST for inactivated vaccines (5). According tothe 9CFR requirements, three animals of the mostsusceptible species have to be injected with one rec-ommended dose, if the vaccine is intended for use inmore than one species. According to the Ph. Eur.monograph on inactivated rabies vaccines for vet-erinary use, the test is usually carried out in twodogs, which are injected with twice the vaccinatingdose. A further difference is evident in the observa-tion period — the Ph. Eur. monograph stipulates 14days, whereas the 9CFR stipulates 28 days.
At the workshop, there was no agreement as towhether this test could lead to added value in termsof the safety of vaccine batches. The statistical rele-vance of the test was questioned, since experimentsperformed with two animals do not provide statisti-cally sound data. Table 7 shows that, even when no
ECVAM Workshop 48: inactivated rabies vaccines 439

local or systemic reactions occur in a sample of twoanimals, it can only be concluded with 95% confi-dence that the true probability of no reaction is < 77.6%. For a sample size of n = 3 animals, it canonly be concluded with 95% confidence that thetrue probability of no reaction is < 63.2%. Some ofthe participants felt that the test should be deleted,whereas others wanted to keep it in the monograph.
There are obviously major differences in the testconditions applied by the various manufacturers —some use commercial breeding colonies outside theirfacilities under well-controlled field conditions. Thoseanimals are considered as laboratory animals onlyduring this safety test, and are available for theiroriginal purpose after the test, which can be regardedas a part of the ordinary vaccination programme.Other manufacturers perform the test under closedlaboratory Good Laboratory Practice conditions with
dogs (mainly beagles), which are specially bred forexperimental purposes.
The Ph. Eur. monograph on veterinary vaccinesis currently being revised, and the draft proposalpublished in Pharmeuropa (31) stipulates that thetarget animal safety test should be carried out onten consecutive batches and can then be discontin-ued, subject to the agreement of the CompetentAuthority, unless there is a change in the produc-tion conditions. Furthermore, a new chapter will beincluded in the Ph. Eur., describing the applicationof the batch safety test in more detail (32).
Recommendations18. If the TAST is to be maintained, it should be
carried out as part of ordinary vaccination pro-grammes in commercial dog breeding colonies,as is already the practice for several vaccinemanufacturers.
19. Also, if the TAST is to be maintained, the testperformance should be harmonised betweenthe USA and Europe. A test using two animalsand the recommended dose could provide areduction and refinement alternative, andcould also be used for potency testing, if serumantibodies were measured at the end of theobservation period, with one of the serologicalmethods given above.
Possibilities for replacement
Residual live virus testing (confirmation of inactivation)
This test is designed to detect non-inactivatedrabies virus, and is required for rabies vaccines forhuman and veterinary use (Table 8). For human
Table 6: Target animal safety test for rabies vaccines for veterinary use
Ph. Eur. 9CFR
Animal Species Target species; if carnivores included, use dogs Most susceptible species
Animal number 2 3
Age of animals Not specified “Young”
Route of application Route stated on the label Intramuscular
Dose Twice the dose One recommended dose
Observation period 14 days 28 days
Evaluation criteria No abnormal local or systemic reactions No unfavourable reaction
9CFR = US Code of Federal Regulations, Title 9; Ph. Eur. = European Pharmacopoeia.
Table 7: Target animal safety test:confidence intervals and samplesize
n animals 95% confidencewith reaction % interval
n = 2 animals according to Ph. Eur.0 0 0.0–77.61 50 1.3–98.72 100 22.4–100.0
n = 3 animals according to 9CFR0 0 0.0–63.21 33.3 0.8–90.62 66.6 9.4–99.23 100 36.8–100.0
9CFR = US Code of Federal Regulations, Title 9;Ph. Eur. = European Pharmacopoeia.
440 L. Bruckner et al.

vaccines, the WHO requires that the test on the fin-ished product is carried out in mice, whereas thePh. Eur. stipulates an in vitro test using cell cul-tures, and the CBER does not directly stipulate howthe test should be conducted; for example, there isno requirement for the use of animals for this test.However, one US rabies vaccine manufacturer stilluses animals for this test. For veterinary products,the USDA requirements prescribe that 20 mice andtwo rabbits should be injected intracerebrally with0.25ml of the product and observed each day for 21days. If any animals die between day 4 and day 21,material from each brain is recovered and injectedinto each of five mice. The OIE allows the use of acell culture method or the test in mice. With regardto the Ph. Eur., the monograph for veterinaryrabies vaccines still includes the in vivo test in micefor the finished product, but, according to the gen-eral monograph on veterinary vaccines, the manu-facturer should only perform the cell culture test onthe bulk material and should omit the test in mice.However, in practice, all manufacturers still use theanimal test (see Table 1), and some of the manufac-turers at the workshop reported that some controlauthorities even ask them to carry out the test inmice on the finished product, although this is incontradiction to the general Ph. Eur. monograph,Rabies Vaccine (Inactivated) for Veterinary Use (33).
The volume injected into rabbits or mice is rela-tively small. The use of the cell culture methodallows the testing of a much higher number ofequivalent doses, and the in vitro test is more sen-sitive than the in vivo test. For example, the resultsof a study carried out by Blum et al. (34) demon-strate that the fluorescent antibody technique is atleast as sensitive as the mouse test. The authorsrecommend that the test should be carried outbefore the addition of adjuvants and preservative.
Recommendations20. The test for residual live virus should be con-
ducted on the bulk material by using cell cul-
tures, and the test in mice and rabbits shouldbe deleted as a finished product test.
21. The Ph. Eur. should clearly state that the man-ufacturers do not have to carry out the test inmice for residual live virus testing of the fin-ished product.
Pyrogenicity testing
The Ph. Eur., the WHO, and the FDA require thatinactivated rabies vaccines for human use aretested for pyrogens with the Limulus amoebocytelysate (LAL) test and the classical pyrogenicity testin rabbits, whereby the LAL test measures theendotoxin levels and the rabbit test measures non-endotoxin pyrogens.
It is questionable whether the current test inrabbits mimics the situation in humans. Oneconcern is the route of administration: the ani-mals are intravenously injected over a period of 3minutes with a single vaccine dose diluted to atotal volume of 10ml, which corresponds to a ten-fold dilution of the vaccine. However, the vaccineis administered intramuscularly into humans.
A number of in vitro methods, which are basedon the human fever reaction, have been devel-oped for the detection of pyrogens and arereviewed in ECVAM workshop report 43 (35). Sixmethods are currently being validated within theframework of a Shared Cost Action projectfunded by DG Research of the EuropeanCommission (36).
Another approach could be the direct measure-ment of cytokines in the vaccines, by using com-mercially available ELISA kits.
Recommendations22. It should be further investigated whether the
in vitro methods based on the human feverreaction, or commercially available kits for
Table 8: Tests stipulated for residual live virus testing of inactivated rabies vaccines
Method Animals
Vaccines for human usePh. Eur. Cell culture test —WHO Cell culture test on bulk and final product test in mice MiceFDA Cell culture test —
Vaccines for veterinary usePh. Eur. Manufacturers test bulk in cell culture; control laboratories use mouse test 10 miceUSDA Mouse/rabbit inoculation 20 mice and 2 rabbits
FDA = US Food and Drug Administration; Ph. Eur. = European Pharmacopoeia; USDA = US Department ofAgriculture; WHO = World Health Organization.
ECVAM Workshop 48: inactivated rabies vaccines 441

cytokine determination, could replace the pyro-genicity test in rabbits.
23. If the pyrogen test in rabbits is maintained, theLAL test (which needs animals to produce thereagents) should be deleted.
Animal tests on virus seed lots
The current regulations in the Ph. Eur. for virus seedlot production for human vaccine manufacturerequire three different animal tests for extraneousagents. The test is conducted by neutralising live vac-cine virus with antibodies, then using the mix toinoculate adult mice, suckling mice and guinea-pigs.The animals are observed for 21 days, 14 days and 42days, respectively. The mice are observed for survival.Guinea-pigs are observed for survival, and are alsoanalysed both microscopically and culturally for evi-dence of infection. This secondary analysis is per-formed on guinea-pigs, both for animals which dieduring the test period and for those which survive theobservation period. In contrast, virus seed lots forveterinary vaccines are tested in vitro by using a cellculture system. This tissue culture system should beapplicable to use for the seed lot testing of virus usedto manufacture human vaccines.
Recommendation24. According to the Ph. Eur. monograph, animal
tests are used for the extraneous agents testingof seed lots for rabies vaccines for human use,whereas in vitro methods are used for veteri-nary vaccines. There should be an assessmentof whether these in vitro methods could beapplied to human vaccine virus strains.
In fact, the WHO has already removed the in vivotest from its vaccine production guidelines andallows the use of cell cultures.
List of Recommendations
Potency testing: reduction
Single-dilution test
1. National control authorities should follow theFrench approach, and should evaluate whetherthe single-dilution test could be introduced intheir laboratories for the batch potency testingof veterinary rabies vaccines.
2. Whether this testing strategy could also beapplied to rabies vaccines for human use shouldbe evaluated.
Number of animals per group
3. Depending on the type of assay used and theinformation already available, the use of equallysized groups is not essential in all cases.Therefore, all available information should beused in an optimised way to minimise the num-ber of animals needed for the selection of dosesand/or group sizes. Furthermore, statisticalmethods such as Bayesian methods or sequen-tial approaches, which sometimes provide formore-efficient use of the data, should be con-sidered when planning an in vivo test.
Verification of the challenge dose
4. Whenever it is feasible, the potency testing ofseveral vaccine batches should be performed inparallel. Thus, only one test for verification ofthe challenge dose and the reference vaccinewould be needed, and the total number of ani-mals used would be reduced.
5. It should be investigated whether the numberof animals per group and the number of dilu-tions could be reduced.
Frequency of testing
6. Only one potency test should be performed,since a second test does not contribute to thetest precision. The WHO and the FDA shouldmodify their requirements accordingly.
Potency testing: refinement
The use of anaesthetics
7. All regulatory authorities and other relevantorganisations should stipulate the use of appro-priate anaesthetics (for example, halothane,isoflurane) in their guidelines, in order to reducethe pain and distress caused by i.c. injection.
Intracerebral injection technique
8. Scientists and technicians should be trained inappropriate i.c. injection techniques. A BestPractice Guide agreed by the workshop partici-pants is presented in Appendix 1.
Criteria for evaluation of the potency test
9. Only non-lethal endpoints should be used ascriteria for test evaluation. Clinical signs offer
442 L. Bruckner et al.

the possibility of terminating the potency testas soon as typical signs of neurological disorderare evident (for example, shaky movements,trembling, and convulsions), without any lossof scientific data, but avoiding a slow progres-sive death for the animals.
10. Scientific and technical staff should betrained in the application of non-lethal end-points. The video on non-lethal endpoints forthe potency testing of rabies vaccines, whichhas been produced by the Humane Endpoints— Lethal Parameters (HELP) Group (17), couldbe used for training purposes (see also,Appendix 2).
Potency testing: replacement
Alternatives based on antigen quantification
11. A pool of potential tests and reagents are nowavailable. Industry, and control and other labo-ratories should use it for further collaborativeevaluations of alternatives based on antigenquantification.
12. With regard to the validation of antigen quan-tification-based alternatives to the NIH test andits variants, several important issues should beconsidered: a) whatever test is selected shouldmeasure an antigen that correlates with protec-tion; b) an acceptable assay should be able todistinguish potent versus sub-potent batches;and c) the development of an alternative assayshould include a definition of potency and thedesignation of an international standard basedon antigen mass units.
13. As the use of the in vivo potency test as a “goldstandard” in developing an in vitro replacementmethod is not recommended, criteria for theacceptance of alternative methods should bedefined.
The use of national and international standards in potency testing
14. Despite the fact that national and internationalstandards or reference preparations calibratedin vivo may not be suitable for potency testingwith in vitro methods, it is recommended thatfuture collaborative studies for their establish-ment could be used to evaluate, in parallel, can-didate in vitro methods, in order to gaininformation and experience with these methodsand to encourage the phasing out of the in vivotests.
15. Standards which were calibrated in vivo shouldnot be used as reference preparations in in vitrotests. Specific standards should be calibratedfor this purpose, once an in vitro method hasbeen established.
Safety testing: deletion
The abnormal toxicity test/general safety test
16. In the interests of international harmonisation,the deletion of the ATT/general safety testshould be considered.
17. National control authorities, being responsiblefor batch release testing, should demand thatcompanies which are still performing the ATTshould cease to do so.
Safety testing: reduction and refinement
The target animal safety test (TAST) for vaccinesfor veterinary use
18. If the TAST is to be maintained, it should be car-ried out as part of ordinary vaccination pro-grammes in commercial dog breeding colonies,as is already the practice for several vaccinemanufacturers.
19. Also, if the TAST is to be maintained, the testperformance should be harmonised betweenthe USA and Europe. A test using two animalsand the recommended dose could provide areduction and refinement alternative, andcould also be used for potency testing, ifserum antibodies were measured at the endof the observation period, with one of theserological methods given above.
Safety testing: replacement
Residual live virus testing (confirmation of inactivation)
20. The test for residual live virus should be con-ducted on the bulk material by using cell cul-tures, and the test in mice and rabbits shouldbe deleted as a finished product test.
21. The Ph. Eur. should clearly state that the manu-facturers do not have to carry out the test inmice for residual live virus testing of the fin-ished product.
ECVAM Workshop 48: inactivated rabies vaccines 443

Pyrogenicity testing
22. It should be further investigated whether the invitro methods based on the human fever reac-tion, or commercially available kits for cytokinedetermination, could replace the pyrogenicitytest in rabbits.
23. If the pyrogen test in rabbits is maintained, theLAL test (which needs animals to produce thereagents) should be deleted.
Animal tests on virus seed lots
24. According to the Ph. Eur. monograph, animaltests are used for the extraneous agents testingof seed lots for rabies vaccines for human use,whereas in vitro methods are used for veteri-nary vaccines. There should be an assessment ofwhether these in vitro methods could beapplied to human vaccine virus strains.
References
1. Anon. (1994). ECVAM News & Views. ATLA 22,7–11.
2. WHO (1998). World Survey of Rabies No. 34 for theyear 1998. WHO/CDS/CSR/APH/99.6, 44pp. Geneva,Switzerland: World Health Organization.
3. Dreesen, D.W. (1997). A global review of rabies vac-cines for human use. Vaccine 15, Suppl., S2–S6.
4. WHO (1994). Requirements for rabies vaccine (inac-tivated) for human use produced in continuous celllines. Amendment 1992. WHO Technical ReportSeries No. 840, pp. 205–207. Geneva, Switzerland:World Health Organization.
5. OIE (2000). Rabies. In Manual of Standards forDiagnostic Tests and Vaccines, 4th edn, pp.276–291. Paris, France: Office International desEpizooties. Web site http://www.oie.int/eng/normes/mmanual/A_summry.htm (Accessed 11.8.03).
6. Council of Europe (2002). The European Pharm-acopoeia, 4th edn, 2416pp. Strasbourg, France:Council of Europe.
7. CFR (1999). US Code of Federal Regulations, Title 9,Chapter I: Animal and Plant Health InspectionService, Department of Agriculture, Subchapter E –Viruses, Serums, Toxins, and Analogous Products;Organisms and Vectors, Part 113.209, RabiesVaccine, Killed Virus, pp. 601–603. Washington, DC,USA: US Government Printing Office.
8. Council of Europe (2002). Introduction. In TheEuropean Pharmacopoeia, 4th edn, p. iv. Strasbourg,France: Council of Europe.
9. Wilbur, L.A. & Aubert, M.F.A. (1996). The NIH testfor potency. In Laboratory Techniques in Rabies, 4thedn (ed. F-X. Meslin, M.M. Kaplan & H. Koprowski),pp. 360–368. Geneva, Switzerland: World HealthOrganization.
10. WHO (1987). Requirements for rabies vaccine (inac-tivated) for human use produced in continuous celllines. WHO Technical Report Series No. 760, pp. 167–194. Geneva, Switzerland: World HealthOrganization.
11. Milne, C., Daas, A., Spieser, J-M. & Bruckner, L.(2001). Collaborative study for the establishment ofrabies vaccine (inactivated) for veterinary use.European Pharmacopoeia Biological ReferencePreparation Batch No. 3. Pharmeuropa, SpecialIssue, BIO 2000-2, 57–64.
12. Aubert, M.F.A. & Blancou, J. (1982). Test simplifiéde contrôle d’activité des vaccins antirabiques àvirus inactivés. Revue Scientifique et TechniqueOffice International des Epizooties 1, 811–822.
13. Meslin, F-X. & Kaplan, M.M. (1996). An overview oflaboratory techniques in the diagnosis and preven-tion of rabies and in rabies research. In LaboratoryTechniques in Rabies, 4th edn (ed. F-X. Meslin, M.M.Kaplan & H. Koprowski), pp. 9–27. Geneva,Switzerland: World Health Organization.
14. Koprowski, H. (1996). The mouse inoculation test.In Laboratory Techniques in Rabies, 4th edn (ed. F-X. Meslin, M.M. Kaplan & H. Koprowski), pp.80–87. Geneva, Switzerland: World HealthOrganization.
15. USDA (1999). Supplemental Assay Method forPotency Testing of Inactivated Rabies Vaccine inMice Using the National Institutes of Health Test;MVSAM0308.01, 19pp. Ames, IA, USA: USDA,APHIS.
16. Cussler, K., Morton, D.B. & Hendriksen, C.F.M.(1998). Humane endpoints for the estimation oflethality rates in the potency testing of rabies vac-cines. Alternativen zu Tierexperimenten 15, Suppl.98, 40–42.
17. The HELP Group (2001). Humane Endpoints –Lethal Parameters: Humane Endpoints ReplaceLethal Parameters in Batch Potency Tests of RabiesVaccines, 11pp. Bilthoven, The Netherlands: TheHELP Group.
18. Weisser, K. & Hechler, U. (1997). Animal WelfareAspects in the Quality Control of Immunobiologicals.A Critical Evaluation of Animal Tests in Pharm-acopoeial Monographs, 348pp. Nottingham, UK:FRAME for ECVAM and the Paul-Ehrlich-Institut.
19. Smith, J.S., Yager, P.A. & Baer, G.M. (1996). A rapidtissue culture test for determining rabies neutralis-ing antibody. In Laboratory Techniques in Rabies,4th edn (ed. F-X. Meslin, M.M. Kaplan & H.Koprowski), pp. 354–357. Geneva, Switzerland:World Health Organization.
20. Cliquet, F., Aubert, M. & Sagne, L. (1998).Development of a fluorescent antibody virus neu-tralisation test (FAVN test) for the quantitation ofrabies-neutralising antibody. Journal of Immuno-logical Methods 212, 79–87.
21. Arko, R.J., Wiktor, T.J. & Sikes, R.K. (1973). Theantibody binding test for vaccine potency. InLaboratory Techniques in Rabies (ed. M.M. Kaplan& H. Koprowski), pp. 292–294. Geneva, Switzerland:World Health Organization.
22. Barth, R., Gruschkau, H., Milcke, L., Jaeger, O. &Weinmann, E. (1986). Validation of an in vitroassay for the determination of rabies antigen.Developments in Biological Standardization 64,87–92.
23. Ferguson, M., Seagroatt, V. & Schild, G.C. (1984). Acollaborative study on the use of single radialimmunodiffusion for the assay of rabies virus glyco-protein. Journal of Biological Standardization 12,283–294.
24. Vogel, I., Kundi, M. & Gerstl, F. (1989). A modifica-tion of the single radial immunodiffusion potency
444 L. Bruckner et al.

test (SRD) for rabies vaccines. Journal of BiologicalStandardization 17, 75–83.
25. Miceli, G.S., Torraba, J., Torres, W., MaderoEsteves, J. & Diaz, A.M. (2000). Evaluation of stan-dard reagents for radial immunodiffusion assays. Invitro control of rabies vaccines. Revista do Institutode Medicina Tropical Sao Paulo 42, 153–156.
26. Lyng, J., Bentzon, M.W., Ferguson, M. & Fitzgerald,E.A. (1992). Rabies vaccine standardization: Inter-national Collaborative Study for the character-ization of the fifth International Standard for rabiesvaccine. Biologicals 20, 301–313.
27. Gupta, R.K. (1996). Is the test for abnormal toxicity,general safety or innocuity necessary for vaccines?Vaccine 14, 1718.
28. Schwanig, M., Nagel, M., Duchow, K. & Krämer, B.(1997). Elimination of abnormal toxicity test for seraand certain vaccines in the European Pharma-copoeia. Vaccine 15, 1047–1048.
29. Duchow, K., Schwanig, M., Krämer, B. & Nagel, M.(1996). Abnormal Toxicity: a Study in the Relevanceof the Requirement V.2.1.5 of the German Pharma-copoeia for Vaccines, Immunosera and Immuno-globulins. German Ministry of Research andTechnology. Project No. 0310624, Final Report.Langen, Germany: Paul-Ehrlich-Institut.
30. WHO (2002). Abnormal toxicity test. WHO Tech-nical Report Series No. 904, p. 10. Geneva, Switzer-land: World Health Organization.
31. Council of Europe (2001). Vaccines for veterinaryuse. Pharmeuropa 13, 363–369.
32. Council of Europe (2002). Evaluation of safety ofeach batch of veterinary vaccines and immunosera.Pharmeuropa 14, 712–713.
33. Council of Europe (2002). Rabies vaccine (inacti-vated) for veterinary use (Monograph No. 0451). InThe European Pharmacopoeia, 4th edn, pp.2282–2284. Strasbourg, France: Council of Europe.
34. Blum, S.A.E., Braunschweiger, M., Krämer, B.,Duchow, K. & Cussler, K. (2001). Inactivation test forrabies vaccines ad us. vet.: a comparison of test resultsfrom in vivo and in vitro methods. Pharmeuropa,Special Issue – Proceedings – Biologicals Beyond 2000,p. 390.
35. Hartung, T., Aaberge, I., Berthold, S., Carlin, G.,Charton, E., Coecke, S., Fennrich, S., Fischer, M.,Gommer, M., Halder, M., Haslov, K., Jahnke, M.,Montag-Lessing, T., Poole, S., Schechtman, L.,Wendel, A. & Werner-Felmayer, G. (2001). Novelpyrogen tests based on the human fever reaction.
Report and recommendations of ECVAM workshop43. ATLA 29, 99–123.
36. Anon. (1999). DG Research Shared Cost Action –Comparison and Validation of Novel Pyrogen TestsBased on the Human Fever Reaction; QLK3-CT-1999-00811; Web site http://www.cordis.lu (Accessed20.9.02).
37. WHO (1984). WHO Expert Committee on rabies.Seventh report. WHO Technical Report Series No.709, 104pp. Geneva, Switzerland: World HealthOrganization.
38. Council of Europe (2002). Rabies vaccine for humanuse prepared in cell cultures (Monograph No. 0216).In The European Pharmacopoeia, 4th edn, pp.2213–2214. Strasbourg, France: Council of Europe.
39. Gamoh, K., Senda, M., Itoh, O., Muramatsu, M.,Hirayama, N., Koike, R., Endoh, Y.S. & Minamoto,N. (1996). ELISA for in vitro potency test of rabiesvaccines. Biologicals 24, 95–101.
40. Rooijakkers, E., Groen, J., Uittenbogarrd, J., vanHerwijnen, J. & Osterhaus, A. (1996). Developmentand evaluation of alternative testing methods for thein vivo NIH potency test used for the quality controlof inactivated rabies vaccines. Developments inBiological Standardization 86, 137–145.
41. Perrin, P., Morgeaux, S. & Sureau, P. (1990). Invitro rabies vaccine potency appraisal by ELISA:advantages of the immunocapture method with aneutralising anti-glycoprotein monoclonal antibody.Biologicals 18, 321–330.
42. Lafon, M., Perrin, P., Versmisse, P. & Sureau, P.(1985). Use of a monoclonal antibody for quantitationof rabies vaccine glycoprotein by enzyme immunoassay.Journal of Biological Standardization 13, 295–301.
43. Enssle, K., Kurrle, R., Kohler, R., Muller, H., Kanzy,E.J., Hilfenhaus, J. & Seiler, F.R. (1991). A rabies-specific human monoclonal antibody that protectsmice against lethal rabies. Hybridoma 10, 547–556.
44. Bunschoten, H., Gore, M., Claassen, I.J., Uytdehaag,F.G., Dietzschold, B., Wunner, W.H. & Osterhaus,A.D. (1989). Characterization of a new virus-neu-tralizing epitope that denotes a sequential determi-nant on the rabies virus glycoprotein. Journal ofGeneral Virology 70, 291–298.
45. Lafon, M. (1996). Technique for the production,screening and characterization of monoclonal anti-bodies. In Laboratory Techniques in Rabies, 4th edn(ed. F-X. Meslin, M.M. Kaplan & H. Koprowski), pp.133–144. Geneva, Switzerland: World HealthOrganization.
ECVAM Workshop 48: inactivated rabies vaccines 445

Introduction
ECVAM workshop report 48 includes a number of rec-ommendations on the application of the Three Rs inthe quality control of inactivated rabies vaccines (1).With regard to the possibilities of reduction, twoimportant aspects, which significantly reduce theoverall number of animals, are repeated here: thegrouping of controls, which leads to reduction whenthe same control groups are used for back titration ofthe challenge virus and for the reference vaccine; andthe introduction of a single-dilution test, providedthat it has been validated in the laboratory (2).
The current methods used for the potency testingof inactivated rabies vaccines for human and veteri-nary use are based on the intracerebral (i.c.) chal-lenge of mice that have previously been vaccinatedintraperitoneally. This guideline is not meant as acomplete protocol for rabies vaccine potency test-ing, but focuses on techniques which should beapplied in order to refine the animal procedure,thus minimising the suffering of the animals.
The following preconditions should be met:
— quality control of rabies vaccines should be aroutine procedure in the laboratory, includingthe follow-up of the challenge virus titre, thepotency of the reference vaccine and theinjected dose of virus with control charts;
— the staff should be experienced in the properhandling of mice and should be regularly
trained; and at least two persons experienced inthe animal procedure should be working in thelaboratory;
— the animal housing facilities should fulfil thelegal requirements;
— animals entering the test should be of knownorigin and in good condition.
I.c. injection into mice is stipulated also for otherpharmacopoeial tests (for example, the pertussisvaccine potency test [3] or extraneous agents test-ing [4, 5]), and is used for diagnostic purposes (forexample, for the diagnosis of rabies [6]).
In the following paragraphs, step-by-step guid-ance is given for the necessary animal procedures,taking into account all possibilities for refinementof the techniques applied.
Vaccination of Mice
Groups of animals are vaccinated with differentdilutions of the test vaccine. Each group is kept ina box or in several boxes, depending on the num-ber of animals required. The animals in a groupshould be individually marked for identification;small spots of picric acid, applied at different sitesof the body, are suitable for this purpose.Vaccination is performed by intraperitoneal injec-tion of the vaccine, using a 25ga × 5/8 needle, asillustrated in Figures 1 and 2. This procedure is
Appendix 1
Best Practice Guide for the Batch Potency Testing of Inactivated RabiesVaccine Using Mice
Figure 1: Catching and immobilisation of the mouse
a) Catching; b) immobilisation.
a) b)
446 L. Bruckner et al.

not painful, and anaesthesia of the mice is there-fore not necessary.
I.c. Challenge with Virulent Rabies Virus
The i.c. challenge should be carried out only onanaesthetised animals, since it involves consider-able pain and might induce shock. The techniqueapplied should permit the anaesthetisation of theanimals in their boxes and should avoid the risk ofmixing animals between groups; moreover, itshould be rapid and safe.
Anaesthetisation technique
Gaseous anaesthesia (for example, with isoflurane,or halothane) is routinely used, as it is necessary tohave a rapid induction with a recovery time of
10–20 minutes. Premedication with an analgesicshould not be performed, since the effects on theoutcome of the test are not known.
Furthermore, it should be possible to anaes-thetise mice in their boxes. For example, a gaseoussystem with a home-made box in which severalcages can be installed, could be used. Among theproducts available, halothane has a “wake-up time”of more than 10 minutes, which allows the removalof the anaesthetisation device from the box, and theinoculation of all the mice. A trained person willneed less than 2 minutes to inoculate ten mice.
I.c. injection procedure
In order to reduce the risk of contamination for theperson carrying out the inoculation, the mouseshould be immobilised in the abdominal position, asshown in Figures 3 and 4. The syringe (WorldHealth Organization: 0.25–0.5ml tuberculinsyringe; 7) should be held vertically, and the needleshould point toward the plate and not toward thefingers of the person carrying out the inoculation. A27ga (8) needle, which is either sheathed or veryshort, as shown in Figure 5, should be used to per-mit penetration of not more than 5mm.Modifications concerning the position for the i.c.injection were described by Koprowski (9).
Humane endpoints
The i.c. injection of even small volumes is likely tocause brain damage, even if it is performed prop-erly. The two European Pharmacopoeia mono-graphs on rabies vaccines for human and veterinaryuse (10, 11) consider death occurring before day 5after challenge to be non-specific and not attributa-ble to rabies infection. Therefore, it is necessary to
Figure 2: Intraperitoneal vaccination
Figure 3: Injection site
ECVAM Workshop 48: inactivated rabies vaccines 447
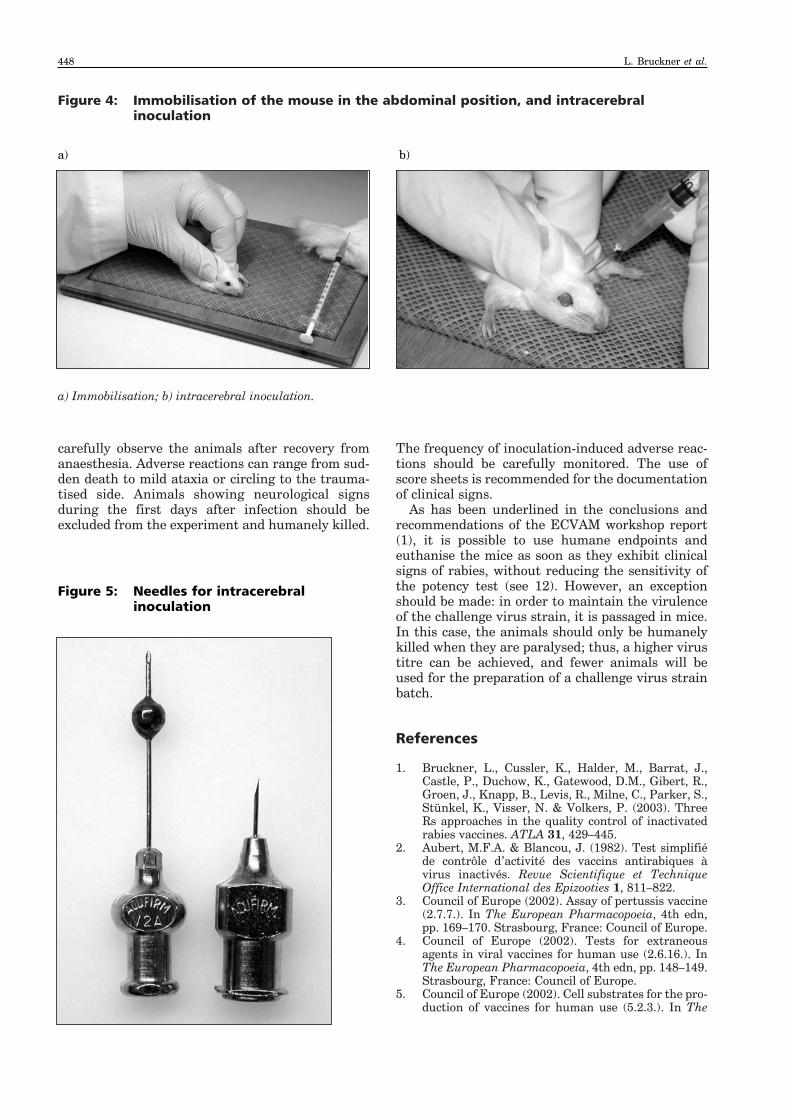
carefully observe the animals after recovery fromanaesthesia. Adverse reactions can range from sud-den death to mild ataxia or circling to the trauma-tised side. Animals showing neurological signsduring the first days after infection should beexcluded from the experiment and humanely killed.
The frequency of inoculation-induced adverse reac-tions should be carefully monitored. The use ofscore sheets is recommended for the documentationof clinical signs.
As has been underlined in the conclusions andrecommendations of the ECVAM workshop report(1), it is possible to use humane endpoints andeuthanise the mice as soon as they exhibit clinicalsigns of rabies, without reducing the sensitivity ofthe potency test (see 12). However, an exceptionshould be made: in order to maintain the virulenceof the challenge virus strain, it is passaged in mice.In this case, the animals should only be humanelykilled when they are paralysed; thus, a higher virustitre can be achieved, and fewer animals will beused for the preparation of a challenge virus strainbatch.
References
1. Bruckner, L., Cussler, K., Halder, M., Barrat, J.,Castle, P., Duchow, K., Gatewood, D.M., Gibert, R.,Groen, J., Knapp, B., Levis, R., Milne, C., Parker, S.,Stünkel, K., Visser, N. & Volkers, P. (2003). ThreeRs approaches in the quality control of inactivatedrabies vaccines. ATLA 31, 429–445.
2. Aubert, M.F.A. & Blancou, J. (1982). Test simplifiéde contrôle d’activité des vaccins antirabiques àvirus inactivés. Revue Scientifique et TechniqueOffice International des Epizooties 1, 811–822.
3. Council of Europe (2002). Assay of pertussis vaccine(2.7.7.). In The European Pharmacopoeia, 4th edn,pp. 169–170. Strasbourg, France: Council of Europe.
4. Council of Europe (2002). Tests for extraneousagents in viral vaccines for human use (2.6.16.). InThe European Pharmacopoeia, 4th edn, pp. 148–149.Strasbourg, France: Council of Europe.
5. Council of Europe (2002). Cell substrates for the pro-duction of vaccines for human use (5.2.3.). In The
Figure 4: Immobilisation of the mouse in the abdominal position, and intracerebralinoculation
a) Immobilisation; b) intracerebral inoculation.
a) b)
Figure 5: Needles for intracerebralinoculation
448 L. Bruckner et al.
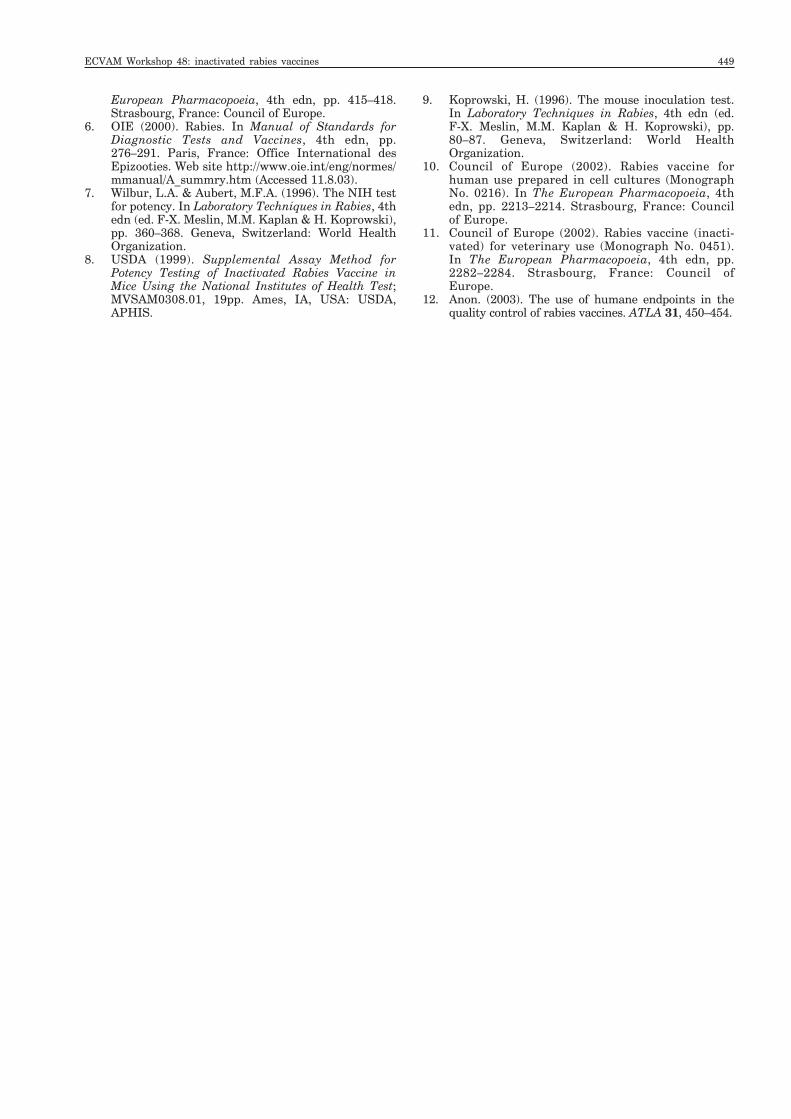
European Pharmacopoeia, 4th edn, pp. 415–418.Strasbourg, France: Council of Europe.
6. OIE (2000). Rabies. In Manual of Standards forDiagnostic Tests and Vaccines, 4th edn, pp.276–291. Paris, France: Office International desEpizooties. Web site http://www.oie.int/eng/normes/mmanual/A_summry.htm (Accessed 11.8.03).
7. Wilbur, L.A. & Aubert, M.F.A. (1996). The NIH testfor potency. In Laboratory Techniques in Rabies, 4thedn (ed. F-X. Meslin, M.M. Kaplan & H. Koprowski),pp. 360–368. Geneva, Switzerland: World HealthOrganization.
8. USDA (1999). Supplemental Assay Method forPotency Testing of Inactivated Rabies Vaccine inMice Using the National Institutes of Health Test;MVSAM0308.01, 19pp. Ames, IA, USA: USDA,APHIS.
9. Koprowski, H. (1996). The mouse inoculation test.In Laboratory Techniques in Rabies, 4th edn (ed. F-X. Meslin, M.M. Kaplan & H. Koprowski), pp.80–87. Geneva, Switzerland: World HealthOrganization.
10. Council of Europe (2002). Rabies vaccine forhuman use prepared in cell cultures (MonographNo. 0216). In The European Pharmacopoeia, 4thedn, pp. 2213–2214. Strasbourg, France: Councilof Europe.
11. Council of Europe (2002). Rabies vaccine (inacti-vated) for veterinary use (Monograph No. 0451).In The European Pharmacopoeia, 4th edn, pp.2282–2284. Strasbourg, France: Council ofEurope.
12. Anon. (2003). The use of humane endpoints in thequality control of rabies vaccines. ATLA 31, 450–454.
ECVAM Workshop 48: inactivated rabies vaccines 449

Introduction
Rabies vaccines for human and veterinary use areimportant medicinal products for preventing thisfatal disease. Animal tests are the basic experi-ments for demonstrating the efficacy and potency ofrabies vaccines. Since laboratory mice are highlysusceptible to rabies infection, a virulent challenge(the so-called NIH test) is used to demonstrate theprotective effect of a vaccine on a batch-to-batchbasis (1).
While considerable effort has been made toreplace this test, and several promising in vitrotests are currently being evaluated, all the regula-tory requirements still include the challenge test.Rabies challenge procedures are prescribed withprecise protocols for vaccine potency testing inmonographs of the European Pharmacopoeia (Ph.Eur.), the US Code of Federal Regulations, andguidelines of the World Health Organization andthe Office International des Epizooties (2–6). As itis necessary to calculate the potency in interna-tional units by means of the classical multiple-dilu-tion assay, more than 100 animals are required totest each batch of these vaccines. The assays have tobe performed in such a way that more than half ofthe animals succumb to infection, to ensure fulfil-ment of the evaluation criteria.
For animal welfare reasons, such animal tests areof great concern. Due to the length of time that isnecessary for the introduction and validation ofalternative techniques, progress concerning thechange of testing requirements has so far been lim-ited. Therefore, it is likely that the challenge testwill continue to be used to estimate the potency ofrabies vaccines for the foreseeable future, for bothhuman and veterinary applications. The large num-ber of mice required, together with the severity ofthe procedure, emphasise the relevance of therabies vaccine challenge test to the Three Rs and toanimal welfare concerns. To improve the situationon behalf of the animals, much more emphasisshould be placed on the refinement of vaccine test-ing procedures.
In general, legislation controlling animalresearch requires scientists to select proceduresthat cause the least suffering for the animals used.One possibility for refinement is through reducingthe duration of the animal tests, in order to shortenthe period of suffering. For example, the humanekilling of animals should be permitted when typicalclinical signs of infection occur. Legal requirements(for example, the Council of Europe ConventionETS 123 [7] and Directive 86/609/EEC [8]) state
that, in a choice between procedures, those methodsshould be selected which cause the least sufferingand which are most likely to provide satisfactoryresults. This implies the use of humane endpoints.The monographs of the Ph. Eur. usually do notspecify such criteria; however, a paragraph whichrequires the use of humane endpoints in generalhas recently been included in the general mono-graphs, Vaccines for Human Use and Vaccines forVeterinary Use (9).
The possibility of using humane endpointslargely relies on the availability of typical clinicalsigns and other relevant parameters such as varia-tions in body weight and body temperature. Scoresheets specifically designed for the documentationof all relevant information concerning the diseaseunder study are necessary for all these infectionmodels (10).
A refined test that will cause less animal suffer-ing, and which can be considered to be sufficientlywell validated to replace the traditional lethalassay with mice, is described. It is proposed thatclinical signs of rabies can be used as an endpoint,instead of death. Specific behaviour and loss ofbody weight are suitable signs, which can be usedas reliable surrogate and humane endpoints toterminate an experiment at a stage much earlierthan death.
Rabies Vaccine Potency Test
Routine potency tests were used to perform thesestudies, to avoid the use of additional animals, andwere carried out in accordance with the Ph. Eur.monograph for Rabies Vaccine for Human UsePrepared in Cell Cultures (2). Animals were vacci-nated intraperitoneally with several vaccine dilu-tions, and challenged two weeks later with anintracerebral (i.c.) injection of rabies virus underanaesthesia. The animals were then allowed torecover from the anaesthetic and were monitoredcarefully over the next 14 days.
Score Sheets
Score sheets were developed for the challenge pro-cedures (11). They included data on clinical signs,body weight and body temperature (Table 1).During the experiment, the animals were observedtwice daily, between 8 a.m. and 9 a.m., and between3 p.m. and 4 p.m. In the morning, the body temper-ature was recorded and the animals were weighedimmediately afterwards.
Appendix 2
The Use of Humane Endpoints in the Quality Control of Rabies Vaccines
450 L. Bruckner et al.

Clinical Signs
The first signs of the disease do not usually appearbefore day 4 after challenge. Before that time, anyclinical sign is most likely to have been caused bythe i.c. injection procedure, so animals showingsuch early signs are normally excluded from theexperiment. The clinical signs of rabies are progres-sive, and it may take between 2 and 6 days for ananimal to die.
The following five stages can be recognised inmice infected with rabies virus, and which thereforehave not been protected by the vaccine.
Stage 1: ruffled fur, hunched back (Figure 1)Ruffled fur (sometimes referred to as a starey coator harsh coat) indicates the first signs of clinical dis-ease. This is a rather general sign of illness in miceand can be observed in many other diseases. Thesame is true for hunched back. Therefore, theseclinical signs in Stage 1 are not specific indicatorsfor rabies, but do reflect that the animal is unwell,and that its welfare is compromised.
Stage 2: slow movements, circular movements(Figure 2)During Stage 2, animals lose their alertness. Theywalk more slowly than usual, and if observed care-fully for a while, they sometimes show circlingmovements, mainly in one direction. These are thefirst clinical indicators of neurological disorder.
Stage 3: shaky movements, trembling, convulsions(Figure 3)In Stage 3, the neurological signs become increas-ingly obvious, with trembling and shaky move-ments, and convulsions appear which can often beprovoked. By this time, there is a marked loss ofbody weight. This stage, with severe and unequivo-cal clinical signs, clearly indicates rabies infection.
Stage 4: signs of paralysis (Figure 4)Lameness and paresis, usually of the hind legs,are also clear indicators of progressive infection
Table 1: Example of the use of a score sheet in the rabies vaccine potency test
Days after infection
–1 0 1 2 3 4 5 6 7 8 9 10 11 12a
Body weight (g) 22.2 22.3 21.6 21.9 22.1 22.3 21.8 21.2 18.5 16.9 15.4 14.2 13.9
Temperature (°C) 38.1 38.4 37.5 37.8 37.9 37.8 37.9 37.7 37.1 36.5 35.7 34.0 33.7
Clinical signs (score) 0 0 0 0 0 0 0 1 2 3 4 4 5— ruffled fur × × × × × ×— hunched back × × × × × ×— slow movements ×— circular movements × ×
— trembling × ×— shaky movements ×— convulsions × × ×— paresis × ×— paralysis ×
— prostration— agony, coma ×
aThe score sheet shows the parameters for an individual mouse during the course of the potency test, beginning 1 dayprior to infection, and ending on day 12 with the death of the mouse.
Figure 1: Stage 1 — ruffled fur, hunchedback
ECVAM Workshop 48: inactivated rabies vaccines 451

with rabies, and are soon followed by completeparalysis. The animals become clearly dehy-drated.
Stage 5: moribund animalsIn Stage 5, animals become moribund. They can beseen to be prostrate and recumbent, and they obvi-ously do not feed or drink; yet they may still survivefor 1 or 2 days.
Overall, rabies infection in mice is characterised bya slow onset of the disease, usually beginningbetween day 4 and day 6 after infection. In contrastto most other mammals with rabies, mice do notshow any signs of aggression. The study showedthat all mice which had developed Stage 3 signs didnot recover and died a few days later. Clinical signstherefore offer the possibility of terminating the
experiment as soon as typical signs of neurologicaldisorder are evident (Stage 3 at the latest), withoutany loss of scientific data, but avoiding a slow pro-gressive death for the animals.
Body Weight
Body weight was measured with electronic scalesand recorded on the score sheet. Since the anaes-thetic and i.c. route of infection had a negativeeffect on body weight for 1 day, the weight on day 2after the infection was used as the basis for bodyweight loss.
Interestingly, the measurement of body weightrevealed a very early decrease, even before typicalclinical signs of the disease were obvious. A signifi-cant loss of body weight (> 20%) proved to be theearliest pre-lethal endpoint for rabies in laboratorymice. Figure 5 shows that body weight loss wasnoted, even before other clinical signs were evident.Weight loss progressed continuously and couldreach 30–50% shortly before death.
Body Temperature
To measure body temperature, temperature-sensi-tive transponders (incorporating a unique identi-fier) were implanted under the skin of the necks ofthe mice, and temperatures were measured twicedaily. Interestingly, hyperthermia, an early sign ofinfection in other mammals, especially humans,never developed in the mice; hypothermia alwaysbecame marked in the final stage of the disease.However, this was much too late to be considereda suitable endpoint, and other markers were seenearlier and were more reliable.
Figure 2: Stage 2 — slow movements,circular movements
Figure 3: Stage 3 — shaky movements,trembling, convulsions
Figure 4: Stage 4 — signs of paralysis
452 L. Bruckner et al.

Conclusions
The appearance of typical clinical signs (Stage 3),alone or Stage 2, in combination with a decrease inbody weight, are suitable humane endpoints. Therelatively slow progression of the disease, with anincrease in severity of the clinical signs, makes theuse of score sheets for rabies easy. If a decrease ofbody weight of more than 15% and clinical signs ofneuronal dysfunction, as in Stages 2 or 3, occur incombination, a point of no return has been reached.Consideration of these two combined endpointsallows the experiment to be terminated at an evenearlier phase. This reduces the duration of animalsuffering by an average of 2–3 days. Figure 5 givesa typical example of the development of all threeparameters.
Only a suitable balance and score sheets have tobe used to identify an early humane endpoint inrabies challenge tests. The clinical signs of rabiesare easy to observe, and staff can readily be trainedto recognise the early stages of the disease.
A combination of clinical signs and recording ofbody weight are suitable humane endpoints for therabies challenge test and would lead to a consider-able reduction of animal suffering. Hopefully, manyinstitutions and companies will rely on the use of
humane endpoints instead of lethality. A video isavailable, which might help to change the currentsituation and reduce the causation of unnecessaryanimal suffering (12).
Acknowledgement
Appendix 2 is based on the results of a study(Alternative methods to replace, reduce and/or refinethe use of laboratory animals in vaccine production,quality control and assessment) funded by theEuropean Commission via ECVAM (EC contractnumber 11274-95-10F1ED ISP NL).
References
1. Wilbur, L.A. & Aubert, M.F.A. (1996). The NIH testfor potency. In Laboratory Techniques in Rabies, 4thedn (ed. F-X. Meslin, M.M. Kaplan & H. Koprowski),pp. 360–368. Geneva, Switzerland: World HealthOrganization.
2. Council of Europe (2002). Rabies vaccine for humanuse prepared in cell cultures (Monograph No. 0216).In The European Pharmacopoeia, 4th edn, pp.2213–2214. Strasbourg, France: Council of Europe.
3. Council of Europe (2002). Rabies vaccine (inacti-vated) for veterinary use (Monograph No. 0451). In
Figure 5: Body weight, temperature and development of clinical signs in a mouse duringrabies infection
Body weight was normalised to day 2 after infection.
= body weight; = body temperature; = score of clinical signs.
120
100
80
60
38.5
38.0
37.5
37.0
36.5
36.0
35.5
35.0
34.5
34.0
33.50 1 2 3 4 5 6 7 8 9 10 11 12
days after infection
body
wei
ght (
%)
body
tem
pera
ture
(°C
)
1
2
3
4 4
5
ECVAM Workshop 48: inactivated rabies vaccines 453

The European Pharmacopoeia, 4th edn, pp.2282–2284. Strasbourg, France: Council of Europe.
4. CFR (1999). US Code of Federal Regulations, Title 9,Chapter I: Animal and Plant Health InspectionService, Department of Agriculture, Subchapter E –Viruses, Serums, Toxins, and Analogous Products;Organisms and Vectors, Part 113.209, RabiesVaccine, Killed Virus, pp. 601–603. Washington, DC,USA: US Government Printing Office.
5. WHO (1994). Requirements for rabies vaccine (inac-tivated) for human use produced in continuous celllines. Amendment 1992. WHO Technical ReportSeries No. 840, pp. 205–207. Geneva, Switzerland:World Health Organization.
6. OIE (2000). Rabies. In Manual of Standards forDiagnostic Tests and Vaccines, 4th edn, pp. 276–291.Paris, France: Office International des Epizooties.Web site http://www.oie.int/eng/normes/mmanual/A_summry.htm (Accessed 11.8.03).
7. Council of Europe (1986). European Convention forthe Protection of Vertebrate Animals Used forExperimental and Scientific Purposes ETS No. 123,51pp. Strasbourg, France: Council of Europe.
8. European Commission (1986). Council Directive86/609/EEC on the approximation of laws, regula-tions and administrative provisions of the MemberStates regarding the protection of animals used forexperimental and other scientific purposes. OfficialJournal of the European Communities L358, 1–28.
9. Council of Europe (2002). The EuropeanPharmacopoeia, 4th edn, 2416pp. Strasbourg,France: Council of Europe.
10. Morton, D.B. (1995). Advances in refinement in ani-mal experimentation over the past 25 years. ATLA23, Suppl. 1, 812–822.
11. Cussler, K., Morton, D.B. & Hendriksen, C.F.M.(1998). Humane endpoints for the estimation oflethality rates in the potency testing of rabies vac-cines. Alternativen zu Tierexperimenten 15, Suppl.98, 40–42.
12. The HELP Group (2001). Humane Endpoints –Lethal Parameters: Humane Endpoints ReplaceLethal Parameters in Batch Potency Tests of RabiesVaccines, 11pp. Bilthoven, The Netherlands: TheHELP Group.
454 L. Bruckner et al.