Three Cases of C-ANCA-Positive Vasculitis Treated with Immunoadsorption: Possible Benefit in...
5
Three Cases of C-ANCA-Positive Vasculitis Treated with Immunoadsorption: Possible Benefit in Early Treatment *Goran Matic, ²Ann Michelsen, ²Doris Hofmann, ²Roland Winkler, ²Michael Tiess, ²Jana Maria Schneidewind, *Waltraud Mu ¨ ller, and ²Wolfgang Ramlow *Labor Mu ¨ ller, and ²Dialysegemeinschaft Nord, Rostock, Germany Abstract: Wegener’s granulomatosis is a vasculitic disease predominantly affecting the upper respiratory tract, lungs, and kidneys. Three patients with Wegener’s granulomato- sis and rapidly progressive glomerulonephritis were treated with an intensified regimen of immunoadsorption (IA) (Excorim or Therasorb) in addition to cyclophospha- mide (CYC) and methylprednisolone (PRE). Patient A had been in remission under oral CYC/PRE. The first ex- acerbation was treated successfully with 4 IA treatments without changing medication. Patient B experienced 3 flares within 1 year, which were treated with 28 IA (3–7 IAs/course), intravenous CYC after each course, and PRE. A fall of creatinine levels from 120 to 190 mmol/L to 100 mmol/L was noted after IA and before administration of CYC. Patient C presented in uremia. Autoantibodies were eliminated by 11 IA treatments parallel to CYC/PRE therapy. They remained within a normal range for >1 year’s follow-up; however, kidney function did not return. In conclusion, the observations in Patients A and B sug- gest a beneficial therapeutic effect of early IA in WG. Key Words: Plasma exchange—Plasmapheresis— Therapeutic apheresis—Antineutrophil cytoplasmic anti- bodies—Anti-Proteinase 3—Rapidly progressive glomer- ulonephritis—Immunoadsorption. Rapidly progressive glomerulonephritis (RPGN) is a frequent and dramatic complication observed in systemic Wegener’s granulomatosis. Without treat- ment kidney function can rapidly deteriorate, and patients may become dialysis dependent within a short period of time. The most common traditional Fauci drug therapy scheme (daily regimens of corti- costeroids and cyclophosphamide) is very effective; however, it also is frequently accompanied by seri- ous drug toxicity (1–6). Due to varying degrees and reversibility of destruction at the glomerulus, the ac- companying drug therapy, and variability between study groups, no additional effect has been observed in clinical studies of classical plasma exchange (2,3). The evaluation of therapeutic efficiency becomes even more complicated if treated plasma volume, number of applied plasma exchanges, and substitu- tion fluids are added into consideration. Many re- ports have appeared to date, but detailed consensus has not been reached (2,3,5,7). In addition to larger clinical studies attempting to define the role of classical plasma exchange in RPGN, a number of case series and case reports have been published to delineate the therapeutic effects of extracorporeal plasma purification proce- dures, including lymphocytapheresis, double mem- brane filtration, and various forms of immunoad- sorption (IA) (8–14). A number of IA systems are currently approved in the United States and in the European Community, all of which have been used to treat autoimmune disorders. The adsorbers consist of single-use col- umns with fillings based on protein A-silica (Pro- sorba, Fresenius HemoCare, Redmond, WA, U.S.A.) or amino acid-polyvinylethanol (Immu- sorba, Asahi Medical Co., Tokyo, Japan), or car- tridges that can be regenerated and reused on the same patient on a sepharose basis with either protein A (Immusorba Excorim AB, Lund, Sweden) or sheep antihuman immunoglobulin (Ig-Therasorb, Plasmaselect, Teterow, Germany) as ligands. Since the systems vary considerably in their capacity and affinity for pathogens (autoantibodies, immune com- plexes), results of clinical studies are not directly comparable. Received November 1999, revised July 2000. Address correspondence and reprint requests to Dr. Wolfgang Ramlow, Dialysegemeinschaft Nord, Nobelstr. 53, 18059 Rostock, Germany. E-mail: [email protected] Therapeutic Apheresis 5(1):68–72, Blackwell Science, Inc. © 2001 International Society for Apheresis 68
-
Upload
goran-matic -
Category
Documents
-
view
212 -
download
0
Transcript of Three Cases of C-ANCA-Positive Vasculitis Treated with Immunoadsorption: Possible Benefit in...
Three Cases of C-ANCA-Positive Vasculitis Treated withImmunoadsorption: Possible Benefit in Early Treatment
*Goran Matic, †Ann Michelsen, †Doris Hofmann, †Roland Winkler, †Michael Tiess,†Jana Maria Schneidewind, *Waltraud Muller, and †Wolfgang Ramlow
*Labor Muller, and †Dialysegemeinschaft Nord, Rostock, Germany
Abstract: Wegener’s granulomatosis is a vasculitic diseasepredominantly affecting the upper respiratory tract, lungs,and kidneys. Three patients with Wegener’s granulomato-sis and rapidly progressive glomerulonephritis weretreated with an intensified regimen of immunoadsorption(IA) (Excorim or Therasorb) in addition to cyclophospha-mide (CYC) and methylprednisolone (PRE). Patient Ahad been in remission under oral CYC/PRE. The first ex-acerbation was treated successfully with 4 IA treatmentswithout changing medication. Patient B experienced 3flares within 1 year, which were treated with 28 IA (3–7IAs/course), intravenous CYC after each course, and
PRE. A fall of creatinine levels from 120 to 190 mmol/L to100 mmol/L was noted after IA and before administrationof CYC. Patient C presented in uremia. Autoantibodieswere eliminated by 11 IA treatments parallel to CYC/PREtherapy. They remained within a normal range for >1year’s follow-up; however, kidney function did not return.In conclusion, the observations in Patients A and B sug-gest a beneficial therapeutic effect of early IA in WG.Key Words: Plasma exchange—Plasmapheresis—Therapeutic apheresis—Antineutrophil cytoplasmic anti-bodies—Anti-Proteinase 3—Rapidly progressive glomer-ulonephritis—Immunoadsorption.
Rapidly progressive glomerulonephritis (RPGN)is a frequent and dramatic complication observed insystemic Wegener’s granulomatosis. Without treat-ment kidney function can rapidly deteriorate, andpatients may become dialysis dependent within ashort period of time. The most common traditionalFauci drug therapy scheme (daily regimens of corti-costeroids and cyclophosphamide) is very effective;however, it also is frequently accompanied by seri-ous drug toxicity (1–6). Due to varying degrees andreversibility of destruction at the glomerulus, the ac-companying drug therapy, and variability betweenstudy groups, no additional effect has been observedin clinical studies of classical plasma exchange (2,3).
The evaluation of therapeutic efficiency becomeseven more complicated if treated plasma volume,number of applied plasma exchanges, and substitu-tion fluids are added into consideration. Many re-ports have appeared to date, but detailed consensushas not been reached (2,3,5,7).
In addition to larger clinical studies attempting todefine the role of classical plasma exchange inRPGN, a number of case series and case reportshave been published to delineate the therapeuticeffects of extracorporeal plasma purification proce-dures, including lymphocytapheresis, double mem-brane filtration, and various forms of immunoad-sorption (IA) (8–14).
A number of IA systems are currently approved inthe United States and in the European Community,all of which have been used to treat autoimmunedisorders. The adsorbers consist of single-use col-umns with fillings based on protein A-silica (Pro-sorba, Fresenius HemoCare, Redmond, WA,U.S.A.) or amino acid-polyvinylethanol (Immu-sorba, Asahi Medical Co., Tokyo, Japan), or car-tridges that can be regenerated and reused on thesame patient on a sepharose basis with either proteinA (Immusorba Excorim AB, Lund, Sweden) orsheep antihuman immunoglobulin (Ig-Therasorb,Plasmaselect, Teterow, Germany) as ligands. Sincethe systems vary considerably in their capacity andaffinity for pathogens (autoantibodies, immune com-plexes), results of clinical studies are not directlycomparable.
Received November 1999, revised July 2000.Address correspondence and reprint requests to Dr. Wolfgang
Ramlow, Dialysegemeinschaft Nord, Nobelstr. 53, 18059 Rostock,Germany. E-mail: [email protected]
Therapeutic Apheresis5(1):68–72, Blackwell Science, Inc.© 2001 International Society for Apheresis
68

This presentation is based on an intensified regi-men of extracorporeal IA therapy with the Excorimprotein A and the Therasorb anti-Ig systems that arevery similar in their immunoglobulin elimination ca-pacities (15). The simultaneous perfusion of one col-umn of the double-column systems and regenerationof the second column allows continuous treatment oflarger plasma volumes, thereby increasing autoanti-body elimination rates high above values that can beexpected with plasma exchange or other IA proce-dures (15).
PATIENTS AND METHODS
Technical equipmentStandard technical equipment included Excorim
Citem 10 for perfusion of the Excorim protein Acolumns and Excorim PEM 10 for plasma filtration(Excorim AB). Plasma filtration on the ExcorimPEM 10 was performed with various filters accord-ing to availability and individual patient need.
Sheep antihuman-IgG IA columns were pur-chased from Therasorb. Perfusion of anti-IgG col-umns was controlled, as recommended by the manu-f a c t u r e r , b y t h e A D A s y s t e m ( m e d i c a pMedizintechnik GmbH, Ullrichstein, Germany), andplasma was filtered by the Autopheresis C TPS-system with standard disposables (Baxter Health-care Corp., Fenwal Division, Deerfield, IL, U.S.A.).Technical equipment was serviced and operated ac-cording to the manufacturer’s instructions.
ImmunoadsorptionAn intensified treatment regimen was commenced
with 5 to 8 IA treatments within 2 to 3 weeks untilcomplete elimination of antineutrophil cytoplasmicantibodies (ANCA). Additional IA therapy (1–5 IAtreatments within 1–2 weeks) followed when clinicalsigns of recurrence coincided with increasing ANCAvalues. During IA, the flow rate was 60 to 100 ml ofblood/min. A total of 2 to 3 plasma volumes weretreated per session. Treatment resulted in loweringof plasma IgG to levels below 2 g/L. Immunoglobu-lin, nonspecifically depleted by protein A or antihu-man IgG columns, was substituted by prophylactici.v. immunoglobulin (0.2–0.4 g/kg of body weight)after the last IA session of each course. Antibodyelimination of reusable protein A (Excorim) andsheep antiimmunoglobulin columns (Therasorb) arealmost identical as shown by our previous investiga-tions (15). At our center, the systems are used inparallel, and treatment decisions are made uponavailability.
Laboratory evaluationBlood was drawn immediately before and after
the immunoadsorption session from an antecubitalvein or an arteriovenous shunt. The Vaccutainer sys-tem from Becton-Dickinson (Franklin Lakes, NJ,U.S.A.) was used. All blood samples were deliveredto 1 affiliated clinical laboratory. T-cell subsets(CD3/HLA-DR+ cells) were analyzed by flow cy-tometry (Epics XL, Coulter Corp., Hialeah, FL,U.S.A.). Anti-Proteinase 3 (c-ANCA)/anti-GBM)antibodies and circulating immune complexes weremeasured by ELISA or immunofluorescence. CRPwas assessed by nephelometry (Image, Beckman In-struments Inc., Fullerton, CA, U.S.A.).
Patients
Patient AA 43-year-old male presented with affection of the
respiratory tract, arthralgia, fever, and signs of vas-culitis and nephritis in September 1996. Diagnosis ofWegener’s granulomatosis was established by detec-tion of anti-Proteinase 3 antibodies. The patient re-ceived acute i.v. cyclophosphamide (CYC) and i.v.methylprednisolone (PRE) (Fauci scheme) (1). Kid-ney biopsy in April 1997 showed glomerulonephritis(GN) with sclerosis or crescent formation in 50% ofthe glomeruli.
Patient BA 60-year-old female presented with nonspecific
chills, fever, weakness, and an elevated erythrocytesedimentation rate. Hematuria led to a kidney bi-opsy in July 1997 (showing extracapillary, necrotiz-ing, and sclerosing GN in >80% of the glomeruli).This, together with elevated c-ANCA levels, led tothe diagnosis of Wegener’s granlomatosis.
Patient CA 58-year-old female presented with coughing,
pulmonary infiltrations, and nonspecific symptomsof illness in October 1997. She was referred to ne-phrology in June 1998 with a creatinine value of 453mmol/L; diagnosis was established with pathologictiters of anti-GBM and anti-Proteinase 3 antibodies.
RESULTS
Patient AThe first course of IA (5 IAs within 2 weeks) was
started on the Excorim system in June 1997 parallelto immunosuppression. The patient remitted, buthad his first flare in September 1997 despite continu-ous oral medication with daily oral CYC (0.5 mg/kg)and PRE (0.1 mg/kg). He received a second courseof 4 IAs within 10 days. Impairment of kidney func-tion (serum creatinine levels ∼170 mmol/L) due to
WEGENER’S GRANULOMATOSIS TREATED WITH IMMUNOADSORPTION 69
Ther Apher, Vol. 5, No. 1, 2001

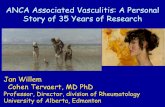
glomerulosclerosis was apparently fixed and couldnot be restored through therapeutic apheresis. Thefirst and only flare was treated successfully with IAwithout changing the drug regimen, completelyeliminating c-ANCA, and demonstrating immuno-modulatory potency of apheresis (Fig. 1). The pa-tient has remained in remission up to the time ofwriting.
Patient BThe first course of IA (5 IAs within 2 weeks) was
commenced on the Excorim system 4 days after kid-ney biopsy parallel to 1 bolus of i.v. CYC (12 mg/kg)and 5 boli of i.v. PRE (4 mg/kg). The patient remit-ted for 1 year. Thereafter, she developed 3 consecu-tive flares (lung granuloma, nephritis, fever, and vas-culitic meningitis) within approximately 1 year,
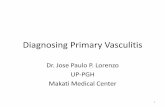
which were treated with a total of 28 IAs on theTherasorb system (3–7 IAs per course). In parallel,she received monthly i.v. CYC (12 mg/kg) and dailyoral PRE (0.2–1 mg/kg) supplemented several timesby i.v. PRE (4 mg/kg). Complete regression of lunginfiltrates was achieved. Creatinine levels fell mark-edly within a few days after IA and before adminis-tration of i.v. CYC (Fig. 2). This surprising findingwill be challenged by further studies; c-ANCA anti-bodies were eliminated successfully, as in the otherpatients (Fig. 3). However, an aseptic pachymenin-gitis with severe headache, a complication of Wege-ner’s vasculitis, did not respond to IA. The conse-quent treatment by daily i.v. CYC (2 mg/kg) and i.v.PRE (start: 1 mg/kg and continuously decreasing)for 3 weeks finally led to a sustained remission undercontrol of daily oral CYC and PRE (1 mg/kg and 0.2mg/kg). At the time of writing, the patient was in thefirst remission for more than 1 year with creatininelevels of approximately 90 mmol/L.
Patient CThe Fauci drug scheme (1) was applied immedi-
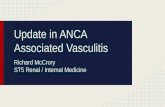
ately after diagnosis, and IA treatment on the Ex-corim system commenced within 1 week after diag-nosis (8 IAs within 3 weeks followed by a secondcourse of 3 IAs after 6 weeks). A kidney biopsy wasassumed to be unnecessary since its results wouldnot have affected therapeutic considerations in lightof pulmonary symptoms and laboratory-confirmeddiagnosis. In fact, the possibility exists that the kid-neys were already scarred. Kidney insufficiencycould not be reversed by IA, and the patient re-mained on dialysis. However, pulmonary complica-tions were controlled, and both autoantibodies wereeliminated and have not reappeared for more than 1year (Fig. 4).
FIG. 1. The graphs show a flare-up of Wegener’s granulomatosisin Patient A treated by 4 immunoadsorption sessions withoutchange of concomitant medication. Complete remission withelimination of c-ANCA and circulating immune complexes isshown.
FIG. 2. Shown is a decrease of the serum creatinine level in Pa-tient B induced solely by immunoadsorption and before admin-istration of i.v. cyclophosphamide. Creatinine values immediatelybefore 2 or 3 consecutive immunoadsorption sessions, respec-tively, performed until complete elimination of c-ANCA. Ex-amples of treatment courses within a 1 year period are shown.
G. MATIC ET AL.70
Ther Apher, Vol. 5, No. 1, 2001

DISCUSSION
Untreated systemic Wegener’s granulomatosis isassociated with a mean survival time of 5 months(16). If treated solely by glucocorticoids, mean sur-vival is prolonged up to 12 months (16). Combinedtreatment with an alkylating agent (cyclophospha-mide) and glucocorticoids (Fauci scheme) notablyimproves survival time and induces remission in>70% of patients (1,2,16,17). Despite the well-documented therapeutic effect and low costs, theFauci regime has been challenged by alternative, lesstoxic drugs such as methotrexate or azathioprine.However, it remains the gold standard (2).
Plasmapheresis has been applied as adjunctivetherapy in cases not responding to drugs or in addi-tion to drug treatment in severe cases with kidneyinvolvement (2,3,5). One rationale has been the re-moval of ANCA and antiglomerular basal mem-brane antibodies that were considered, at least inpart, as disease driving (18). The basic idea of extra-corporeal elimination of pathologic autoantibodieshas led to the development of systems removing im-munoglobulins semiselectively. These systems offerthe advantage of not eliminating valuable plasmaproteins such as coagulation or complement factors.Thus, considerably higher plasma volumes can betreated in 1 session without the side effects notedwith plasma exchange. Consequently, elimination ratesof pathologic antibodies are increased (12,13,15).
Although the effects of IA by both double-columnsystems are convincing in theory, only a few clinicalstudies have been conducted (7,12,13). A recentlypublished controlled and randomized Swedish studycompared protein A IA with plasma exchange (7).The multicenter study could not confirm a differencein outcome between the Excorim protein A IA andplasma exchange in ANCA-positive crescenticRPGN or in Goodpasture’s syndrome. It is impor-tant to note, however, that more patients came offdialysis when treated with IA. Complex in detail, theresults of the Swedish study are not surprising, re-membering the beneficial clinical effects of plasmaexchange added to standard drug regimes only ap-peared in a meta-analysis of studies that by them-selves could not prove a positive effect of plasmaexchange (3).
Our patients tolerated the IA procedures verywell with no signs of biointolerance such as flushing,fever, or even anaphylactoid reactions. Rare occur-rences of hypotension were treated symptomaticallyand did not lead to cessation of the session. Once thediagnosis had been made, immunoadsorption wasquickly commenced. In Patients A and B, the drugregimen and the approach to extracorporeal treat-
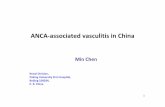
FIG. 3. Displayed is the efficiency of anti-Proteinase 3 elimina-tion by single immunoadsorptions for Patient B (A). The averagereduction was approximately 80%, measured in serum before anddirectly after immunoadsorption (B).
FIG. 4. Complete and rapid elimination of anti-GBM and c-ANCA for >9 months by 11 immunoadsorptions and additionalcyclophosphamide/methylprednisolone therapy is shown for Pa-tient C. No recurrence of lung symptoms was seen. The patientstayed on dialysis.
WEGENER’S GRANULOMATOSIS TREATED WITH IMMUNOADSORPTION 71
Ther Apher, Vol. 5, No. 1, 2001

ment made it possible to distinguish between drug-induced effects and improvements most likely to beattributable to IA. In addition, unlike most pub-lished series, Patients A and B received IA therapyearly in the course of the disease and not as a lastmeasure. A case similar to Patient B with an identi-cal therapeutic effect was mentioned in an Englishstudy published in 1991 (13). The outcome in PatientC was, unfortunately, comparable to the previouslymentioned Swedish study (7): All 6 patients withGoodpasture’s syndrome remained on dialysis. Onemight speculate that outcome would have been bet-ter if aggressive removal of the pathogenic autoan-tibody had been achieved earlier in the course of thedisease.
The Fauci drug regime (1) appears to be a veryefficient drug treatment, and additional plasma ex-change or IA seems to be of added benefit only incertain patients (2–4). Application of therapeuticapheresis in desperate cases of RPGN therefore maybe beneficial in the hands of experienced cliniciansand cost effective in the cases saved from dialysis,and even life saving in Goodpasture’s syndrome.
The situation remains unclear in less severe casesas in the presented Patients A and B. One could wishfor a controlled clinical study, but it appears that thediseases are too rare to interest a sponsor. As a con-sequence, the treatment decision of the involvedphysician is dependent on the individual case and thereimbursement situation.
CONCLUSIONS
Aggressive immunoglobulin elimination with ap-propriate IA systems can be beneficial in cases ofANCA positive vasculitis with crescentic RPGN.The demonstrated effect was additive to immuno-suppressive drugs. Early diagnosis and treatmentmay be crucial.
REFERENCES
1. Fauci AS, Katz P, Haynes BF, Wolff SM. Cyclophosphamidetherapy of severe systemic necrotizing vasculitis. N Engl JMed 1979;301:235–8.
2. Jindal KK. Management of idiopathic crescentic and diffuseproliferative glomerulonephritis: Evidence-based recommen-dations. Kidney Int Suppl 1999;70:S33–40.
3. Kaplan AA. Therapeutic apheresis for renal disorders. TherApheresis 1999;3:25–30.
4. Harada T, Miyazaki M, Ozono Y, Sasaki O, Shioshita K,Kohno S. Nishikido M, Saito Y, Taguchi T. Therapeuticapheresis for renal diseases [editorial]. Ther Apheresis 1998;2:193–8.
5. Hricik DE, Chung-Park M, Sedor JR. Glomerulonephritis. NEngl J Med 1998;339:888–99.
6. Grotz W, Wanner C, Keller E, Bohler J, Peter HH, RohrbachR, Schollmeyer P. Crescentic glomerulonephritis in Wegen-er’s granulomatosis: morphology, therapy, outcome. ClinNephrol 1991;35:243–51.
7. Stegmayr BG, Almroth G, Berlin G, Fehrman I, Kurkus J,Norda R, Olander R, Sterner G, Thysell H, Wikstrom B,Wiren JE. Plasma exchange or immunoadsorption in patientswith rapidly progressive crescentic glomerulonephritis. ASwedish multi-center study. Int J Artif Organs 1999;22:81–7.
8. Omote A, Muramatsu M, Sugimoto Y, Hosono S, MurakamiR, Tanaka H, Watanabe Y, Sano H, Kato K. Myeloperoxi-dase-specific anti-neutrophil cytoplasmic autoantibodies—Related scleroderma renal crisis treated with double-filtrationplasmapheresis. Intern Med 1997;36:508–13.
9. Furuta T, Hotta O, Yusa N, Horigome I, Chiba S, Taguma Y.Lymphocytapheresis to treat rapidly progressive glomerulo-nephritis: A randomized comparison with steroid-pulse treat-ment [letter]. Lancet 1998;352:203–4.
10. Elliott JD, Lockwood CM, Hale G, Waldmann H. Semi-specific immuno-absorption and monoclonal antibodytherapy in ANCA positive vasculitis: Experience in fourcases. Autoimmunity 1998;28:163–71.
11. Yorioka N, Taniguchi Y, Amimoto D, Katsutani M, KumagaiJ, Yamakido M. Plasmapheresis for removal of myeloperoxi-dase antineutrophil cytoplasmic antibodies: a case report.Ther Apheresis 1998;2:314–6.
12. Esnault VL, Testa A, Jayne DR, Soulillou JP, Guenel J. In-fluence of immunoadsorption on the removal of immunoglob-ulin G autoantibodies in crescentic glomerulonephritis. Neph-ron 1993;65:180–4.
13. Palmer A, Cairns T, Dische F, Gluck G, Gjorstrup P, ParsonsV, Welsh K, Taube D. Treatment of rapidly progressive glo-merulonephritis by extracorporeal immunoadsorption, pred-nisolone and cyclophosphamide. Nephrol Dial Transplant1991;6:536–42.
14. Schneider M, Berning T, Waldendorf M, Glaser J, Gerlach U.Immunoadsorbent plasma perfusion in patients with systemiclupus erythematosus. J Rheumatol 1990;17:900–7.
15. Matic G, Hofmann D, Winkler R, Tiess M, Michelsen A,Schneidewind JM, Keysser M, Muller W, Kienze EM, Ram-low W. Removal of immunoglobulins by a protein A versus ananti-human-immunoglobulin-G based system: Evaluation of602 sessions of extracorporeal immunoadsorption. Artif Or-gans 2000;24:103–07.
16. Jayne DR, Rasmussen N. Treatment of antineutrophil cyto-plasm autoantibody-associated systemic vasculitis: Initiativesof the European Community Systemic Vasculitis Clinical Tri-als Study Group. Mayo Clin Proc 1997;72:737–47.
17. de Groot K, Gross WL. Wegener’s granulomatosis: diseasecourse, assessment of activity and extent and treatment. Lu-pus 1998;7:285–91.
18. Salant DJ. ANCA: Fuel for the fire or the spark that ignitesthe flame? [editorial comment]. Kidney Int 1999;55:1125–7.
G. MATIC ET AL.72
Ther Apher, Vol. 5, No. 1, 2001