Thorax and Abdomen Orthopedic Assessment III – Head, Spine, and Trunk with Lab PET 5609C.
73
Thorax and Thorax and Abdomen Abdomen Orthopedic Assessment III – Orthopedic Assessment III – Head, Spine, and Trunk with Lab Head, Spine, and Trunk with Lab PET 5609C PET 5609C
-
Upload
ignacio-abbs -
Category
Documents
-
view
221 -
download
0
Transcript of Thorax and Abdomen Orthopedic Assessment III – Head, Spine, and Trunk with Lab PET 5609C.

Thorax and Thorax and AbdomenAbdomen
Orthopedic Assessment III Orthopedic Assessment III – Head, Spine, and Trunk – Head, Spine, and Trunk
with Labwith Lab
PET 5609CPET 5609C

Clinical AnatomyClinical Anatomy
Thorax – bone cavityThorax – bone cavity Formed by 12 pairs of ribs that join Formed by 12 pairs of ribs that join
posteriorly with the thoracic spine and posteriorly with the thoracic spine and anteriorly with the sternumanteriorly with the sternum
Thoracic Cavity:Thoracic Cavity: Lined with a thin layer of tissue (pleura)Lined with a thin layer of tissue (pleura) One lung in each thoracic cavityOne lung in each thoracic cavity Mediastinum is between the chest cavityMediastinum is between the chest cavity
Heart, Aorta, Superior and Inferior Vena Cava, Heart, Aorta, Superior and Inferior Vena Cava, Trachea, Major Bronchi, and EsophagusTrachea, Major Bronchi, and Esophagus
Spinal cord – protected by vertebral columnSpinal cord – protected by vertebral column


Clinical AnatomyClinical Anatomy Muscles of Muscles of
Inspiration:Inspiration: Diaphragm:Diaphragm:
Separates thoracic and Separates thoracic and abdominal activitiesabdominal activities
Innervation: phrenic Innervation: phrenic nervenerve
Inhalation – diaphragm Inhalation – diaphragm contracts enlarging the contracts enlarging the thoracic cavity and thoracic cavity and reducing intra-thoracic reducing intra-thoracic pressure (air drawn into pressure (air drawn into lungs)lungs)
Exhalation – diaphragm Exhalation – diaphragm relaxes and air is relaxes and air is exhaled by elastic recoil exhaled by elastic recoil of the lungsof the lungs

Clinical AnatomyClinical Anatomy

Clinical AnatomyClinical Anatomy Muscles of Inspiration:Muscles of Inspiration:
Intercostal muscles:Intercostal muscles: External intercostal muscles: (outside of the ribcage) External intercostal muscles: (outside of the ribcage)
Elevate the ribs and expand the transverse dimensions of Elevate the ribs and expand the transverse dimensions of the thoracic cavity (aid in quiet and forced inhalation)the thoracic cavity (aid in quiet and forced inhalation)
Internal intercostal muscles: (inside the ribcage)Internal intercostal muscles: (inside the ribcage) Depress the ribs decreasing the transverse dimensions of Depress the ribs decreasing the transverse dimensions of
the thoracic cavity (aid in forced expiration)the thoracic cavity (aid in forced expiration) Scalene muscles:Scalene muscles:
Elevate the 1Elevate the 1stst and 2 and 2ndnd ribs ribs SCM, trapezius, serratus anterior, pectoralis SCM, trapezius, serratus anterior, pectoralis
major/minor and latissimus dorsi (secondary major/minor and latissimus dorsi (secondary muscles)muscles)
Muscles of Expiration:Muscles of Expiration: Abdominal muscles (rectus abdominis, Abdominal muscles (rectus abdominis,
internal/external obliques, transverse internal/external obliques, transverse abdominisabdominis


Clinical AnatomyClinical Anatomy Respiratory Tract Anatomy:Respiratory Tract Anatomy:
Trachea:Trachea: Connects larynx to 2 principle bronchiConnects larynx to 2 principle bronchi Left bronchus → 2 segmental bronchi (2 lobes)Left bronchus → 2 segmental bronchi (2 lobes) Right bronchus → 3 segmental bronchi (3 lobes)Right bronchus → 3 segmental bronchi (3 lobes)
Pleura:Pleura: Parietal pleura – lines thoracic wallParietal pleura – lines thoracic wall Visceral pleura – surrounds lungsVisceral pleura – surrounds lungs
Alveoli:Alveoli: Terminal branches of bronchiolesTerminal branches of bronchioles Gas exchangeGas exchange Capillary system → blood exchanged (pulmonary Capillary system → blood exchanged (pulmonary
arteries and veins)arteries and veins)


Heart Heart ChamberChamber
FunctionFunction
Right Right AtriumAtrium
Receives deoxygenated blood via:Receives deoxygenated blood via:
Superior vena cava (head, neck, upper Superior vena cava (head, neck, upper extremities)extremities)
Inferior vena cava (trunk and lower Inferior vena cava (trunk and lower extremities)extremities)
Role: Delivers blood to right ventricleRole: Delivers blood to right ventricle
Right Right VentricleVentricle
Receives deoxygenated blood from right Receives deoxygenated blood from right atriumatrium
Role: Delivers blood to lungs via left and Role: Delivers blood to lungs via left and right pulmonary arteriesright pulmonary arteries
Left AtriumLeft Atrium Receives oxygenated blood from lungs via Receives oxygenated blood from lungs via right and left pulmonary veinsright and left pulmonary veins
Role: Delivers blood to left ventricleRole: Delivers blood to left ventricle
Left Left VentricleVentricle
Delivers oxygenated blood through aortic Delivers oxygenated blood through aortic valve to ascending aortavalve to ascending aorta


Clinical AnatomyClinical Anatomy
Digestive Tract Anatomy:Digestive Tract Anatomy: Esophagus:Esophagus:
Carries food/liquid to stomachCarries food/liquid to stomach Small intestine:Small intestine:
Duodenum, jejunum, ileumDuodenum, jejunum, ileum Large intestine:Large intestine:
Cecum, ascending colon, transverse Cecum, ascending colon, transverse colon, descending colon, sigmoid coloncolon, descending colon, sigmoid colon
Rectum and AnusRectum and Anus

Clinical AnatomyClinical Anatomy
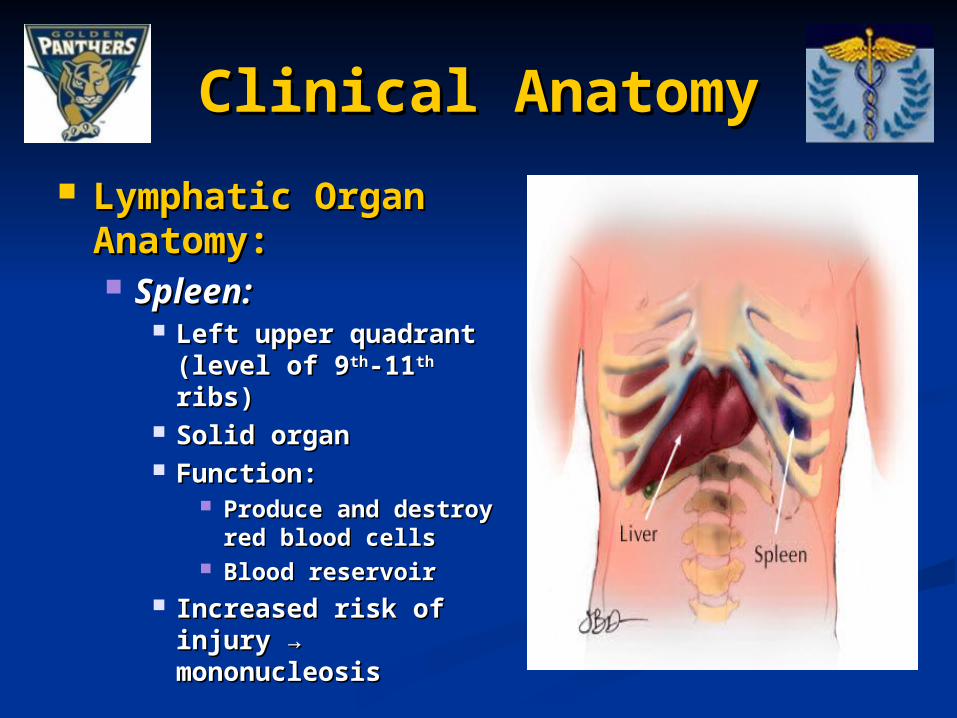
Lymphatic Organ Lymphatic Organ Anatomy:Anatomy: Spleen:Spleen:
Left upper quadrant Left upper quadrant (level of 9(level of 9thth-11-11thth ribs) ribs)
Solid organSolid organ Function:Function:
Produce and destroy Produce and destroy red blood cellsred blood cells
Blood reservoirBlood reservoir Increased risk of Increased risk of
injury → injury → mononucleosismononucleosis
Clinical AnatomyClinical Anatomy
Urinary Tract Anatomy:Urinary Tract Anatomy: Kidneys:Kidneys:
Filter bloodFilter blood Regulate electrolyte levels:Regulate electrolyte levels:
Maintain balance of water, sodium, potassiumMaintain balance of water, sodium, potassium Location:Location:
Posterior part of the abdominal cavity: (level of Posterior part of the abdominal cavity: (level of T12 – L3 vertebrae)T12 – L3 vertebrae)
Right kidney: sits below the diaphragm and Right kidney: sits below the diaphragm and posterior to the liver; sits slightly lower than posterior to the liver; sits slightly lower than left kidneyleft kidney
Left kidney: sits below the diaphragm and Left kidney: sits below the diaphragm and posterior to the spleenposterior to the spleen
Note: Lower portion of kidneys susceptible to Note: Lower portion of kidneys susceptible to trauma (unprotected by ribs)trauma (unprotected by ribs)


Clinical AnatomyClinical Anatomy
Urinary Tract Anatomy:Urinary Tract Anatomy: Ureters:Ureters:
Muscular ducts that propel urine from the kidneys Muscular ducts that propel urine from the kidneys to the urinary bladderto the urinary bladder
Length: 10-12 inches (adults)Length: 10-12 inches (adults)
Urinary Bladder:Urinary Bladder: Solid, muscular, and elastic organ Solid, muscular, and elastic organ Collects urine excreted by the kidneys Collects urine excreted by the kidneys Urine enters the bladder via the ureters and exits Urine enters the bladder via the ureters and exits
by urethraby urethra Urethra:Urethra:
Tube connects urinary bladder to outside the bodyTube connects urinary bladder to outside the body excretory function in both sexes (pass urine); excretory function in both sexes (pass urine);
reproductive function in males (passage for semen) reproductive function in males (passage for semen)


Clinical AnatomyClinical Anatomy
Reproductive Tract Anatomy:Reproductive Tract Anatomy: Testes:Testes:
Produce sperm and male sex hormones (testosterone) Produce sperm and male sex hormones (testosterone) Epididymis:Epididymis:
Coiled tube on posterior aspect of testes (stores Coiled tube on posterior aspect of testes (stores sperm)sperm)
Ovaries:Ovaries: Produce estrogen and progesterone and house Produce estrogen and progesterone and house
reproductive eggsreproductive eggs Fallopian Tubes:Fallopian Tubes:
Tubules lead from ovaries to uterusTubules lead from ovaries to uterus Uterus:Uterus:
Accepts the fertilized ovumAccepts the fertilized ovum


Clinical EvaluationClinical Evaluation Anatomy:Anatomy:
Abdominal cavity Abdominal cavity separated from the separated from the thorax by the thorax by the diaphragmdiaphragm
Lined with a Lined with a membrane membrane (Peritoneum)(Peritoneum)
Lower portion of Lower portion of abdominal cavity: abdominal cavity: (Pelvic region) (Pelvic region)
Surrounded by Surrounded by pelvis, vertebrae, pelvis, vertebrae, and sacrumand sacrum

Clinical EvaluationClinical Evaluation
Upper Right QuadrantUpper Right Quadrant Upper Left QuadrantUpper Left Quadrant
LiverLiver Heart, LungHeart, Lung
KidneyKidney SpleenSpleen
PancreasPancreas KidneyKidney
LungLung StomachStomach
Lower Right QuadrantLower Right Quadrant Lower Left QuadrantLower Left Quadrant
AppendixAppendix UreterUreter
UreterUreter BladderBladder
BladderBladder ColonColon
ColonColon GonadsGonads
GonadsGonads

Clinical EvaluationClinical Evaluation
History:History: Location of Pain:Location of Pain:
Musculoskeletal pain → ribs, costal cartilage, Musculoskeletal pain → ribs, costal cartilage, abdominal muscles (tender at injury site)abdominal muscles (tender at injury site)
Injury to internal organs → diffuse pain; referred Injury to internal organs → diffuse pain; referred pain sites (Kehr’s sign)pain sites (Kehr’s sign)
Onset of Symptoms:Onset of Symptoms: Gradual (internal bleeding can accumulate Gradual (internal bleeding can accumulate
within cavity)within cavity) Pain Pain ↑ ↑ with breathing (rib, abdominal injury)with breathing (rib, abdominal injury)
Mechanism of Injury:Mechanism of Injury: Direct blow (thoracic, abdominal, pelvic injuries)Direct blow (thoracic, abdominal, pelvic injuries)


Clinical EvaluationClinical Evaluation
History:History: Symptoms:Symptoms:
Pain, difficulty breathingPain, difficulty breathing Diffuse abdominal painDiffuse abdominal pain Nausea, dizzinessNausea, dizziness Vomiting of blood, blood in urine/stoolVomiting of blood, blood in urine/stool
Medical History:Medical History: Not common (acute injury)Not common (acute injury) Exercise-induced asthmaExercise-induced asthma Illnesses (mononucleosis)Illnesses (mononucleosis)
General Medical Health:General Medical Health: MedicationsMedications

Clinical EvaluationClinical Evaluation
Inspection:Inspection: Start → observe Start → observe
patient’s posturepatient’s posture Throat:Throat:
Position of trachea Position of trachea and larynx and larynx
Breathing pattern:Breathing pattern: Rate, respiration Rate, respiration
rate, depth, qualityrate, depth, quality Nail beds:Nail beds:
Capillary refill Capillary refill (cyanosis)(cyanosis)
Inspection:Inspection: Muscle toneMuscle tone Discoloration of Discoloration of
skin:skin: Contusions, Contusions,
wounds, abrasionwounds, abrasion Vomiting:Vomiting:
Presence of bloodPresence of blood HematuriaHematuria

Clinical EvaluationClinical Evaluation
Inspection:Inspection: Auscultation:Auscultation:
Lungs:Lungs: Inhalation – Inhalation –
smooth smooth unobstructed unobstructed soundsound
Absence: Absence: pneumothorax, pneumothorax, collapsed lungcollapsed lung
Rales: Rales: pneumoniapneumonia
Abdomen:Abdomen: Gurgling noises Gurgling noises
(peristalsis)(peristalsis)

Clinical EvaluationClinical Evaluation
Palpation:Palpation: Sternum:Sternum:
Manubrium, Manubrium, body, xiphoid body, xiphoid processprocess
Costal cartilage Costal cartilage and ribs:and ribs:
Palpate anterior Palpate anterior to posteriorto posterior
Pain, crepitus, Pain, crepitus, deformitydeformity

Clinical EvaluationClinical Evaluation
Palpation:Palpation: Spleen:Spleen:
Palpate for Palpate for enlarged spleen enlarged spleen under left rib cageunder left rib cage
Have patient raise Have patient raise arms above headarms above head

Clinical EvaluationClinical Evaluation
Palpation:Palpation: Kidneys:Kidneys:
Location → Location → under under posterolateral posterolateral portion of rib portion of rib cagecage
Right kidney Right kidney rests more rests more inferior than inferior than leftleft

Clinical EvaluationClinical Evaluation
Palpation: LiverPalpation: Liver Method 1:Method 1:
Place your fingers Place your fingers just below the just below the costal margin and costal margin and press firmlypress firmly
Ask the patient to Ask the patient to take a deep breathtake a deep breath
May feel the edge May feel the edge of the liver press of the liver press against or slide against or slide under your handunder your hand
Normal liver is not Normal liver is not tendertender

Clinical EvaluationClinical Evaluation
Palpation: LiverPalpation: Liver Method 2:Method 2:
Hands "hooked" Hands "hooked" around the costal around the costal margin from margin from aboveabove
Instruct patient Instruct patient to breath deeply to breath deeply to force the liver to force the liver down toward your down toward your fingersfingers

Clinical EvaluationClinical Evaluation
Palpation: Palpation: McBurney’s PointMcBurney’s Point Location → one-Location → one-
third of way third of way between right between right ASIS and navalASIS and naval
Tenderness → may Tenderness → may indicate acute indicate acute appendicitisappendicitis

Clinical EvaluationClinical Evaluation Palpation: Palpation:
AbdomenAbdomen Rigidity:Rigidity:
Occurs secondary to Occurs secondary to muscle guarding or muscle guarding or blood accumulationblood accumulation
Indication of Indication of internal injuryinternal injury
Rebound Rebound Tenderness:Tenderness:
Tests for peritoneal Tests for peritoneal irritation.irritation.
Palpate deeply and Palpate deeply and then quickly then quickly release pressurerelease pressure
↑ ↑ pain = peritoneal pain = peritoneal irritationirritation

Clinical EvaluationClinical Evaluation Palpation: AbdomenPalpation: Abdomen
Tissue density: PercussionTissue density: Percussion Patient position: hook-lyingPatient position: hook-lying Examiner: Lightly places one Examiner: Lightly places one
hand over abdomen (palm hand over abdomen (palm down); Index/middle fingers of down); Index/middle fingers of opposite hand tap the DIP opposite hand tap the DIP jointsjoints
Findings: (normal)Findings: (normal) Solid organs have a dull thumpSolid organs have a dull thump Hollow organs more resonant Hollow organs more resonant
soundsound Findings: (positive)Findings: (positive)
Hard, solid sounding echo over Hard, solid sounding echo over areas that should sound hollowareas that should sound hollow
Internal bleedingInternal bleeding
Clinical EvaluationClinical Evaluation
Palpation: Palpation: PercussionPercussion Hollow OrgansHollow Organs
Allow materials to Allow materials to pass through them pass through them (stomach, large (stomach, large intestine, small intestine, small intestine, pancreas) intestine, pancreas) or act as “holding or act as “holding tanks” (gall tanks” (gall bladder and urinary bladder and urinary bladder)bladder)
Less risk for injury Less risk for injury when emptywhen empty
Palpation: Palpation: PercussionPercussion Solid Organs:Solid Organs:
Significant blood Significant blood supplysupply
Liver, Spleen, Liver, Spleen, Pancreas, Kidney, Pancreas, Kidney, Ovaries, TestesOvaries, Testes
Higher risk of Higher risk of injuryinjury
BruisingBruising TearingTearing

Clinical EvaluationClinical Evaluation
UpperUpper Liver:Liver: Pain Pain associated with associated with cholecystitis or cholecystitis or liver lacerationliver lacerationGall bladder: Pain Pain without trauma without trauma indicates gall indicates gall bladder diseasebladder disease
Spleen:Spleen: Rigidity Rigidity under the last under the last several ribsseveral ribs
LowerLower Appendix:Appendix: Rebound Rebound tenderness tenderness indicates indicates appendicitisappendicitis
Colon:Colon: Colitis or Colitis or diverticulitis may diverticulitis may cause paincause pain
Pelvic Pelvic inflammation:inflammation: Diffuse tendernessDiffuse tenderness
Colon:Colon: Colitis or Colitis or diverticulitis may diverticulitis may cause paincause pain
Pelvic Pelvic inflammation:inflammation: Diffuse tendernessDiffuse tenderness
Quadrant Pain: Right Quadrant Pain: Right Left Left
Clinical EvaluationClinical Evaluation Vital Signs:Vital Signs:
Heart Rate:Heart Rate: Pulse: Pulse:
Regular / IrregularRegular / Irregular Strong / Weak Strong / Weak
Normal pulse is 60-100 beats Normal pulse is 60-100 beats per minuteper minute
Athletes tend to have a Athletes tend to have a slower pulse than non slower pulse than non athletes (well-conditioned athletes (well-conditioned strong heart)strong heart)
Normal pulse is 60-100 beats Normal pulse is 60-100 beats per minuteper minute
Athletes tend to have a Athletes tend to have a slower pulse than non slower pulse than non athletes (40-60 bpm)athletes (40-60 bpm)
Abnormal:Abnormal: Tacchycardia: > 100 bpmTacchycardia: > 100 bpm Bradycardia: < 60 bpmBradycardia: < 60 bpm

Clinical EvaluationClinical Evaluation
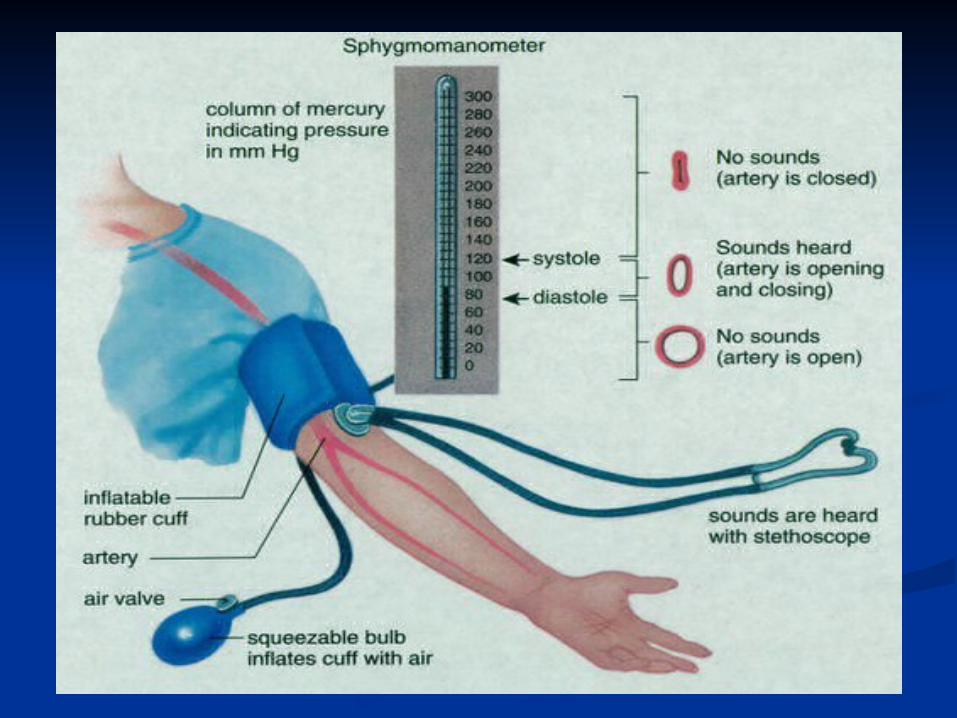
Vital Signs: Blood Vital Signs: Blood PressurePressure Patient position:Patient position:
Seated or supineSeated or supine Procedure:Procedure:
Cuff secured over upper armCuff secured over upper arm Stethoscope placed over Stethoscope placed over
brachial arterybrachial artery Inflate cuff to 180-200 mm Inflate cuff to 180-200 mm
HgHg Air slowly releasedAir slowly released Note point at which 1Note point at which 1stst pulse pulse
sound is heardsound is heard Note point at which last Note point at which last
pulse sound is heardpulse sound is heard

Clinical EvaluationClinical Evaluation
Vital Signs: Blood PressureVital Signs: Blood Pressure Affected by:Affected by:
Decrease in blood volume (severe Decrease in blood volume (severe bleeding or dehydration) – Hypovolemic bleeding or dehydration) – Hypovolemic shockshock
Decreased capacity of vessels (shock)Decreased capacity of vessels (shock) Rapid/weak pulse; ↓ BPRapid/weak pulse; ↓ BP
Decreased ability of heart to pump Decreased ability of heart to pump bloodblood
↓ ↓ nutrients/oxygen to organs of body nutrients/oxygen to organs of body (anoxia)(anoxia)

Clinical Evaluation
Vital Signs: Respiratory Rate Normal: 12 – 20 bpm Abnormal:
Rapid, shallow breaths:
Internal injury Shock
Deep, quick breaths: Pulmonary instruction Asthma
Noisy, raspy breaths: Airway obstruction

Clinical Evaluation
Rib Fractures: Most common injured:
5th-9th ribs (anterior and lateral portions) History:
Onset: acute (single traumatic blow) Pain: over fracture site
↑ pain with deep inspirations, coughing, sneezing, movement of torso
MOI: Force (anteroposterior direction) – outward
displacement Force (lateral side) – inward displacement
Internal injury (i.e. lungs)

Clinical Evaluation
Rib Fractures: Inspection:
Splinting posture: Holding the painful area to limit chest wall
movement during inspiration Discoloration / swelling Shallow, rapid respirations (minimize chest
movement) Palpation:
Point tenderness, crepitus, possible deformity Functional Tests:
Movement of torso causes pain ↑ pain with deep respiration, coughing, sneezing

Clinical Evaluation
Rib Fractures: Stress Fractures:
Rowing, swimming, golf Posterolateral portion of 4th-9th ribs Causes:
Overtraining, sudden increases in training Improper biomechanics
Special Tests: Rib compression test:
Contraindicated in presence of obvious fracture/lung trauma


Clinical Evaluation Lateral Rib
Compression Test: Test position:
Subject supine Action:
Examiner compresses the lateral aspect of the rib cage then quickly releases
Positive finding: Pain with compression
or release of pressure indicates possible rib fracture, contusion, or costochondral separation

Clinical Evaluation Anterior/Posterior
Rib Compression Test: Test position:
Subject supine Action:
Compress rib cage anterior to posterior and quickly release
Positive test: Pain with compression
or release of pressure indicates possible fracture, rib contusion, costochondral separation
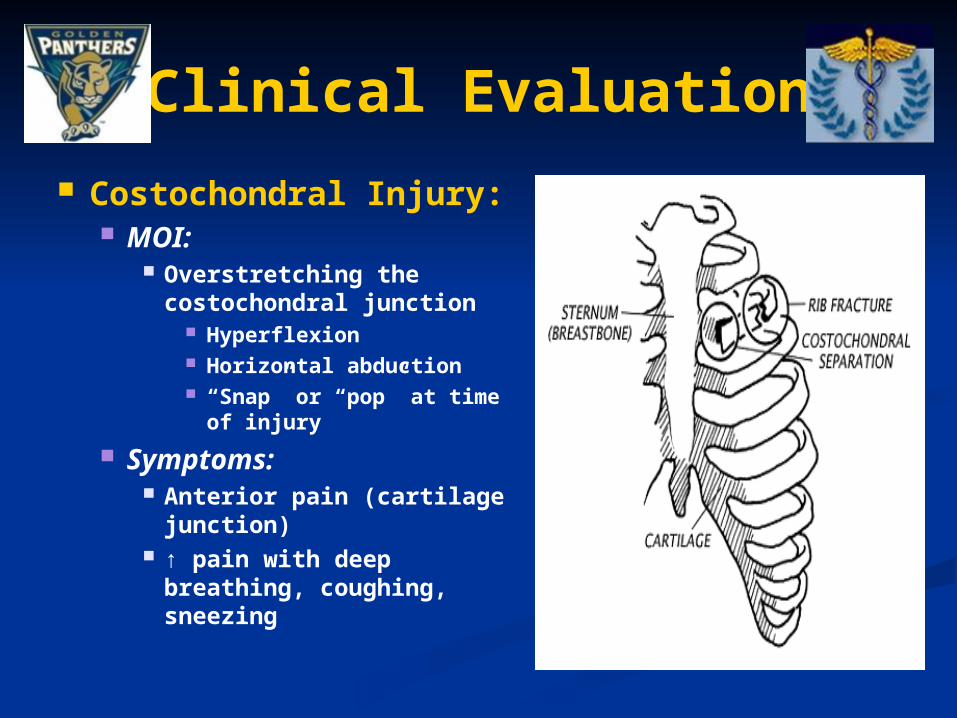
Clinical Evaluation
Costochondral Injury: MOI:
Overstretching the costochondral junction
Hyperflexion Horizontal abduction “Snap” or “pop” at time
of injury
Symptoms: Anterior pain (cartilage
junction) ↑ pain with deep
breathing, coughing, sneezing

Clinical Evaluation Pneumothorax:
Accumulation of air in pleural activity Spontaneous pneumothorax:
Diagnosis dependent on signs/symptoms – rare condition
Chest pain, dyspnea, diminished breath sounds Chest pain – usually localized to the side of the
affected lung Can radiate to shoulder, neck, back
Contributing Factors: Family history, tall and thin body build Sports-related spontaneous pneumothorax –
documented in weight lifting, football, jogging Primary spontaneous pneumothorax:
Primary cause: Bleb (imperfection in the lining of the lung) bursts causing lung to deflate
Tall thin men (ages 20-40) Secondary spontaneous pneumothorax:
Chronic obstructive pulmonary disease (COPD)

Clinical Evaluation
Pneumothorax: Tension pneumothorax:
One-way valve is created from either blunt or penetrating trauma
Air can enter, CANNOT leave the pleural space
↑ Intrathoracic pressure will collapse the lung and ↑ pressure on mediastinum
Pressure will eventually collapse superior and inferior vena cava (loss of venous return)

Clinical Evaluation Pneumothorax:
Clinical Signs: Apprehension / Agitation Cyanosis Diminished breath
sounds Distended neck veins /
Tracheal deviation Palpation:
Trauma induced – point tenderness
Vital Signs: Labored, shallow
respirations BP drops rapidly Right tension
pneumothorax

Clinical Evaluation Hemothorax:
Blood enters the pleural space
Massive Hemothorax – at least 1500cc of blood loss into thoracic cavity
Penetrating injury Can occur from blunt trauma
Blood accumulates → lung on the affected side is compressed
Mediastinum may shift away from hemothorax
Inferior and superior vena cava and contralateral lung may become compressed

Clinical Evaluation
Hemothorax: Clinical
signs/symptoms: Produced by
hypovolemia and respiratory compromise
Anxiety, apprehension Symptoms of
hypovolemic shock Decreased breath
sounds or absence at injury site
Flat neck veins

Clinical Evaluation
Spleen Injury: History:
Acute (symptoms may take a few hours to develop)
Pain: Upper left quadrant Kehr’s sign – pain in upper left shoulder
Predisposing conditions: Mononucleosis:
↑ mass, ↓ elasticity
Inspection: Impact site – contusion Nausea and vomiting

Clinical Evaluation
Spleen Injury: Palpation:
Cold and clammy skin (shock) Pont tenderness Rebound tenderness Distention in upper left quadrant
Functional Tests: Kerh’s sign Low blood pressure

Clinical Evaluation
Kidney Pathologies: Contused/Lacerated Kidney:
History: Onset: acute Pain: posterolateral portion of upper lumbar
and lower thoracic region MOI: blunt trauma or penetrating injury to
kidney Inspection:
Contusion or laceration Hematuria:
Severe bleeding → noticeable blood Laboratory analysis needed
Signs/symptoms of shock

Clinical Evaluation
Kidney Pathologies: Palpation:
Point tenderness Abdominal rigidity
Functional Testing: Pain with urination
Laboratory Testing: Hematuria

Clinical Evaluation
Kidney Stones: Collection of
incomplete kidney filtration
Crystals of uric acid, calcium
1mm – 2.5 cm
Causes: Family history, stress,
diet
Signs: Pain with urination Pain (stone passed from
bladder through urethra)
Clinical Evaluation
Urinary Tract Infections: Bacterial infections of bladder or urethra Similar signs/symptoms of kidney stones Dysuria → frequent need to urinate Hematuria (abnormal urine color)
Urethritis: Inflammation of urethra Causes: chlamydia, gonorrhea, syphilis More common in males


Clinical Evaluation Appendicitis and
Appendix Rupture: Anatomy Location: Lower Right
Quadrant of Abdomen Elongated tube connected
to the cecum (pouch-like structure of the colon)
Function of the human appendix is unknown
Considered to be a remnant of a portion of the digestive tract which was once more functional and is now in the process of evolutionary regression

Clinical Evaluation Appendicitis:
Cause: Inflammation caused by
fecal obstruction, lymph swelling, tumor
High incidence in males (ages 15 – 25)
If bursts can bleed into peritoneal cavity and cause bacterial infection
Signs and Symptoms: Mild to severe pain in
lower abdomen Nausea, vomiting, fever,
cramping, abdominal rigidity, point tenderness
McBurney’s Point – between ASIS and umbilicus

Clinical Evaluation Hollow Organ Rupture:
Blunt trauma (non-rupture): able to absorb forces (deform/return to original shape without permanent injury)
Rupture: Can be fatal (secondary to hemorrhage,
peritoneal contamination) MOI and Signs/Symptoms:
Blow to abdomen Abdominal pain, possible nausea Palpation reveals guarding, rigidity, tenderness
(point, rebound) Bowel sounds are absent (auscultation) Blood in stool

Clinical Evaluation Gastritis:
Inflammation of stomach lining Causes:
Aspirin or anti-inflammatory medications Alcohol Infection, bile entering stomach
Esophageal Reflux: Backflow of gastric juices into esophagus
Heartburn, regurgitation of stomach acid Ulcer-like pain
Intestinal Ulcers: Irritation of duodenum (peptic ulcer)
Abdominal pain, nausea, vomiting, dark stools, fatigue Causes:
Bacteria Long-term use of aspirin or anti-inflammatory
medications

Clinical Evaluation Dyspepsia:
Pain in upper abdomen Common causes:
Gastroesophageal reflux disease (GERD), stomach ulcers
GERD – stomach acid splashes out of upper valve onto walls of esophagus
Burning pain in mid-upper abdomen / heartburn
Stomach Ulcers – wounds in lining of stomach
Common causes: Stress, virus, diet
Potential for bleeding if ulcers go untreated (open wounds)

Clinical Evaluation Colitis:
Inflammation of the large intestine Symptoms:
Frequent diarrhea Abdominal pain, increased bowel sounds, fever, painful
defecation, nausea, vomiting Causes:
Disease, irritation of bowel, ulcers, ischemia, bacteria, stress
Regional Enteritis (Crohn’s Disease): Affects the ileum Produces LRQ pain, cramping
Irritable Bowel Syndrome: Alters motility of the muscles of large intestine Alternating bouts of diarrhea and constipation Abdominal pain Gas build-up, nausea, vomiting

Clinical Evaluation Testicular Contusion:
MOI: Direct blow Inspection:
Patient instructed to inspect for normal size/consistency
Ruptured testicle – soft, inconsistent texture
Testicular Torsion: Spermatic cord and testicle
twisted within scrotum Symptoms:
Acute testicular pain, swelling, tenderness
Note: Immediate referral needed

Clinical Evaluation
Menstrual Irregularities: (associated with physical activity) Female Athlete Triad:
Combination: Disordered eating Amenorrhea Osteoporosis
Disorder that often goes unrecognized Lost bone mineral density Premature osteoporotic fractures Lost bone mineral density may never be
regained

Clinical Evaluation
Female Athlete Triad: Disordered Eating:
Anorexia, Bulimia, ENDOS Amenorrhea:
Related to athlete training/weight fluctuation is caused by changes in the hypothalamus
Result: Decreased levels of Estrogen Primary Amenorrhea:
No spontaneous uterine bleeding: By the age of 14 without development of 20
sexual characteristics By the age of 16 with otherwise normal
development
Clinical Evaluation
Female Athlete Triad: Amenorrhea:
Secondary Amenorrhea: 6-month absence of menstrual bleeding in a
woman with primary regular menses 12-month absence with previous
oligomenorrhea Osteoporosis:
Loss of bone mineral density and inadequate formation of bone
Premature osteoporosis: Risk for stress fractures Fx of hip, vertebral column


















