
This training will provide attendees with an overview of...
24
This training will provide attendees with an overview of the USDA risk factor changes that will be implemented September 1, 2017. 1
Transcript of This training will provide attendees with an overview of...

This training will provide attendees with an overview of the USDA risk factor changes that will be implemented September 1, 2017.
1

The risk factors which have been revised are listed on the slide. We will be addressing each revised risk factor’s criteria as well as any changes which may occur in MOWINS.
2

Risk factor 135 Slowed/Faltering Growth Pattern is defined as a growth rate below that which is appropriate for an infant’s age and sex. An example of weight faltering is a drop in weight after a minor illness or a measurement/plotting error. The new risk category is assigned to infants up to 6 months of age. Risk Factor 135 will not be assigned to infants greater than six months of age and children. The Participant Category section no longer includes children, as the literature does not support identification of slowed or faltering growth based on weight measurements alone for children.
3
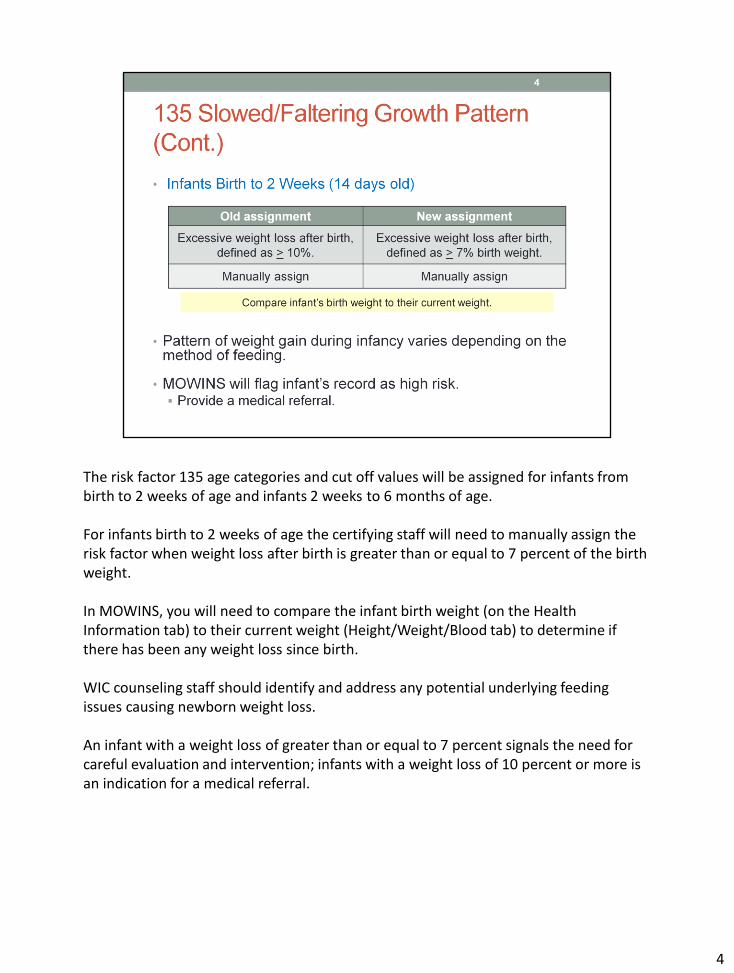
The risk factor 135 age categories and cut off values will be assigned for infants from birth to 2 weeks of age and infants 2 weeks to 6 months of age. For infants birth to 2 weeks of age the certifying staff will need to manually assign the risk factor when weight loss after birth is greater than or equal to 7 percent of the birth weight. In MOWINS, you will need to compare the infant birth weight (on the Health Information tab) to their current weight (Height/Weight/Blood tab) to determine if there has been any weight loss since birth. WIC counseling staff should identify and address any potential underlying feeding issues causing newborn weight loss. An infant with a weight loss of greater than or equal to 7 percent signals the need for careful evaluation and intervention; infants with a weight loss of 10 percent or more is an indication for a medical referral.
4

Infant weight loss in the early postpartum period is physiologically normal, and nearly universal but the amount of weight loss varies. Weight loss of 5% and 7% of birth weight is not unusual for formula-fed or breastfed infants. Healthy infants are expected to regain their birth weight within 8-10 days after birth. However, if a breastfed infant loses 7% of birth weight in the first 72 hours after birth, an evaluation and review of the mother-infant dyad is needed and any problems resolved immediately. Risk of dehydration and failure to thrive in breastfed newborns can be alleviated by early screening and providing lactation support in the early postpartum period. A weight loss of up to 10% of birth weight is the maximum acceptable weight loss for newborn infants, with any additional loss a potential emergency.
5

Infants with a weight loss of ten percent or more is an indication for a medical referral. Contributing factors are listed on the slide.
6

To determine the exact weight loss: Subtract current weight from birth weight and divide by birth weight. As you can see from the example on the slide the calculation result is 4.2% weight loss.
7

Risk factor 135 will be system assigned for infants 2 weeks to 6 months of age when any weight loss has occurred. The risk factor is based on two separate weight measurements which are taken at least eight weeks apart. No single measurement on its own is adequate for identifying nutritional growth delay. The primary goal of the intervention is to enhance infant health outcomes by addressing causes of slowed growth and keeping vulnerable infants tracking along growth percentiles established in infancy.
8

In most situations, growth may not simply be a factor of undernutrition, but rather a combination of environmental and other factors which will require a broad intervention strategy. Intervention strategies may include screening for environmental health factors, such as those which are listed on this slide.
9

Previous records with assignment of risk factor 135 prior to October 1, 2017 will be converted to 135Z to save historical data for infants and children. You can resolve the care plan, or continue to provide nutrition education and counseling, for infants greater than 6 months of age and children who previously had 135 assigned and a high risk care plan. It is possible that infants greater than six months of age and children, who were previously assigned RF 135, may qualify for assignment of risk factor 103 Underweight or At Risk of Underweight. Risk factor 134 Failure to Thrive (FTT) may be assigned to an infant or child when they meet the criteria listed in the policy. As a reminder, the new risk criteria is for infants less than or equal to six months of age.
10

Risk factor 352 Infectious Diseases criterion has been divided into two parts: acute and chronic. Acute infectious diseases is assigned 352a and chronic infectious diseases is assigned 352b. The information was separated to better address the distinctions between acute and chronic conditions. The USDA Justification, Implications for WIC Nutrition Services and Reference sections have been expanded and updated.
11

Risk factor 352a Infectious Diseases – Acute is characterized by a single or repeated episode of relatively rapid onset and short duration. The list of diseases and/or conditions include, but are not limited to the ones listed on this slide. The infectious disease must be present within the past six months, and diagnosed, documented or reported by a health care provider or as self-reported by the applicant/participant. HIV (Human Immunodeficiency Virus) has been placed in the risk factor 352b Infections Disease – Chronic risk factor description. Tuberculosis has been removed from risk factor 352.
12

Risk factor 352b Infectious Diseases – Chronic are conditions likely lasting a lifetime and requiring long-term management of symptoms. These diseases and/or conditions include, but are not limited to, HIV, AIDS, and Hepatitis B, C, and D. An extensive listing of infectious diseases can be found by clicking the link on the slide.
13

WIC can improve the management of acute infectious diseases by offering WIC foods, nutrition education, counseling, and referrals to community resources.
14

The definition for risk factor 359 Recent Major Surgery, Physical Trauma, Burns has been revised. The definition includes major surgery (including cesarean sections), physical trauma, or burns severe enough to compromise nutritional status. USDA changed the risk factor criteria from trauma to physical trauma. This risk factor includes any occurrence within the past two months which is self-reported, or any occurrence more than two months must have continued need for nutritional support and be diagnosed by a physician or a health care provider.
15
Most surgeries, physical traumas, and burns are unexpected. The education and supplemental food that WIC provides can help ensure that the individual is in good nutritional health prior to the surgery, physical trauma or burn.
16

Risk factor 411 is defined as routine use of feeding practices that may result in impaired nutrient status, disease, or health problems. Risk factor 411 Inappropriate Nutrition Practices for Infants has 11 components to assess for inappropriate nutrition practices. USDA has revised 4 of the 11 components. The components are 411.3, 411.5, 411.7 and 411.9. Each revised component will be explained on the next few slides.
17

The 411.3 component was revised to include introducing any food other than human milk or iron-fortified infant formula before 6 months of age.
18

The 411.5 section was revised to include donor human milk acquired directly from individuals or the internet. Although sharing human milk between those with an excess milk supply and those seeking milk for their infant may be growing in popularity, both the American Academy of Pediatrics (AAP) and the Food and Drug Administration (FDA) recommend against feeding infant human milk obtained directly from individuals or through the internet. Obtaining donor human milk via these means is discouraged due to the lack of adequate screening for infectious diseases and the risk of contamination.
19
The 411.7 component was revised to remove the restriction of less than 6 feedings in 24 hours if the infant is between 2 and 6 months of age. The key point is that frequent breastfeeding is critical to the establishment and maintenance of adequate milk supply for the infant.
20

Published guidelines on the handling and storage of human milk were revised. The revised risk criteria related to human milk addresses adding freshly expressed unrefrigerated human milk to already frozen human milk in a storage container.
21

The risk criteria was revised to also address formula that is not prepared according to physician’s instructions. Until infants are 3 months of age, it is recommended that water for infant formula preparation be brought to a rolling boil for 1 to 2 minutes, and then cooled. Encourage caregivers to consult their healthcare provider about whether to boil the water used to prepare infant formula after 3 months of age. Reference NTM Infant Feeding page 29. USDA has removed the criteria for sanitation from the Justification. It is better to yield to the manufacturer’s or physician’s recommendations regarding sterilization of water.
22

We have developed one policy ER# 2.03500 for all the risk factors which will link to the individual USDA Justification/Reference documents.
23

Questions after this training can be directed to your district nutritionist.
24


















