
This topic last updated - Webseite n
29
Official reprint from UpToDate www.uptodate.com ©2017 UpToDate, Inc. and/or its affiliates. All Rights Reserved. Gallbladder polyps and cholesterolosis Authors: Wisam F Zakko, MD, Salam F Zakko, MD, FACP Section Editor: Sanjiv Chopra, MD, MACP Deputy Editor: Shilpa Grover, MD, MPH, AGAF All topics are updated as new evidence becomes available and our peer review process is complete. Literature review current through: Sep 2017. | This topic last updated: Jul 05, 2017. INTRODUCTION — Gallbladder polyps are outgrowths of the gallbladder mucosal wall. They are usually found incidentally on ultrasonography or after cholecystectomy. When detected on ultrasonography, their clinical significance relates largely to their malignant potential. The majority of these lesions are not neoplastic but are hyperplastic or represent lipid deposits (cholesterolosis). Imaging studies alone are insufficiently specific to exclude the possibility of gallbladder carcinoma or premalignant adenomas. Furthermore, even benign lesions can occasionally lead to symptoms similar to those caused by gallbladder stones. While the widespread use of ultrasonography has made the diagnosis of polypoid lesions of the gallbladder increasingly frequent, optimal strategies for evaluating these lesions have not been fully established. This topic will review the clinical significance and differential diagnosis of gallbladder polyps, and will provide a practical approach to their management. Gallbladder cancer is discussed in detail elsewhere. (See "Gallbladder cancer: Epidemiology, risk factors, clinical features, and diagnosis".) EPIDEMIOLOGY — Gallbladder polyps have been observed in 0.004 to 13.8 percent of resected gallbladders [1], and in 1.5 to 4.5 percent of gallbladders assessed by ultrasonography [2,3]. In one report, no association was observed between the presence of polyps and the patient's age, sex, weight, number of pregnancies, use of exogenous female hormones, or any other risk factors that are generally believed to be associated with gallstones [3]. Gallbladder polyps have only rarely been described in children, in whom they occur either as a primary disorder or in association with other conditions, including metachromatic leukodystrophy, Peutz-Jeghers syndrome, or pancreatobiliary malunion [4]. (See "Epidemiology of and risk factors for gallstones".) ® Seite 1 von 29 Gallbladder polyps and cholesterolosis - UpToDate 29.10.2017 https://www.uptodate.com/contents/gallbladder-polyps-and-cholesterolosis/print?source=search_result&search=gallenblasenpolypen&sel...
Transcript of This topic last updated - Webseite n

Official reprint from UpToDatewww.uptodate.com ©2017 UpToDate, Inc. and/or its affiliates. All Rights Reserved.
Gallbladder polyps and cholesterolosis
Authors: Wisam F Zakko, MD, Salam F Zakko, MD, FACPSection Editor: Sanjiv Chopra, MD, MACPDeputy Editor: Shilpa Grover, MD, MPH, AGAF
All topics are updated as new evidence becomes available and our peer review process is complete.Literature review current through: Sep 2017. | This topic last updated: Jul 05, 2017.
INTRODUCTION — Gallbladder polyps are outgrowths of the gallbladder mucosal wall. They are usually found incidentally on ultrasonography or after cholecystectomy. When detected on ultrasonography, their clinical significance relates largely to their malignant potential. The majority of these lesions are not neoplastic but are hyperplastic or represent lipid deposits (cholesterolosis). Imaging studies alone are insufficiently specific to exclude the possibility of gallbladder carcinoma or premalignant adenomas. Furthermore, even benign lesions can occasionally lead to symptoms similar to those caused by gallbladder stones.
While the widespread use of ultrasonography has made the diagnosis of polypoid lesions of the gallbladder increasingly frequent, optimal strategies for evaluating these lesions have not been fully established. This topic will review the clinical significance and differential diagnosis of gallbladder polyps, and will provide a practical approach to their management. Gallbladder cancer is discussed in detail elsewhere. (See "Gallbladder cancer: Epidemiology, risk factors, clinical features, and diagnosis".)
EPIDEMIOLOGY — Gallbladder polyps have been observed in 0.004 to 13.8 percent of resected gallbladders [1], and in 1.5 to 4.5 percent of gallbladders assessed by ultrasonography [2,3]. In one report, no association was observed between the presence of polyps and the patient's age, sex, weight, number of pregnancies, use of exogenous female hormones, or any other risk factors that are generally believed to be associated with gallstones [3]. Gallbladder polyps have only rarely been described in children, in whom they occur either as a primary disorder or in association with other conditions, including metachromatic leukodystrophy, Peutz-Jeghers syndrome, or pancreatobiliary malunion [4]. (See "Epidemiology of and risk factors for gallstones".)
®
Seite 1 von 29Gallbladder polyps and cholesterolosis - UpToDate
29.10.2017https://www.uptodate.com/contents/gallbladder-polyps-and-cholesterolosis/print?source=search_result&search=gallenblasenpolypen&sel...
CLASSIFICATION — The classification of gallbladder polyps was first proposed in 1970 based upon a review of 180 benign tumors [5]. As a general rule, polypoid lesions can be categorized as benign or malignant (table 1) [6,7]. Benign lesions have been further subdivided into neoplastic or non-neoplastic:
CHOLESTEROLOSIS AND CHOLESTEROL POLYPS — Cholesterolosis has been recognized since 1857, when Virchow described it in a report on the role of the gallbladder in fat metabolism [9]. Cholesterolosis is characterized by the accumulation of lipids in the mucosa of the gallbladder wall. It is a benign condition that is usually diagnosed incidentally during cholecystectomy or on ultrasonography. However, in some patients it can lead to symptoms and complications similar to those caused by gallstones.
Epidemiology of cholesterolosis — Cholesterolosis is common; its prevalence in surgical studies varies from 9 to 26 percent [9]. A large autopsy series of 1300 cases found the prevalence to be 12 percent [10]. Cholesterolosis in association with gallstones is by far the most common pathologic finding in the gallbladder [3]. Most surgical series suggest risk factors that are similar to those for gallstone formation. However, as noted above, an ultrasound study showed no association with any of the known risk factors for gallstones [3]. (See 'Epidemiology' above.)
Similarly, while gallstone disease is known to be more common in women, an autopsy series found the prevalence of cholesterolosis to be equal between men and women [10]. These contradictory observations may be explained by the observation that surgical series generally focus on gallbladders from patients who were symptomatic, which is not necessarily the case in autopsy or ultrasonographic studies.
Pathology of cholesterolosis — Cholesterolosis results from abnormal deposits of triglycerides, cholesterol precursors, and cholesterol esters into the gallbladder mucosa. The lipid accumulation creates yellow deposits that are generally visible to the naked eye. The appearance of the yellow deposits on a background of hyperemic mucosa led to the description of this finding as a "strawberry gallbladder" (picture 1).
The most common benign neoplastic lesion is an adenoma. Benign mesodermal tumors such as leiomyomas and lipomas are rare.
The most common benign non-neoplastic lesions (pseudotumors) are cholesterol polyps (the presence of which is referred to as "cholesterolosis"), followed by adenomyomas (the presence of which is referred to as "adenomyomatosis"), and inflammatory polyps [1,5]. Cholesterolosis and adenomyomatosis are mucosal abnormalities of the gallbladder. They have been referred to as "hyperplastic cholecystosis," a term introduced in 1960 to differentiate them from inflammatory conditions such as acute cholecystitis, since they lack inflammatory features but exhibit features of hyperplasia [8]. Some data suggest that adenomyomatosis may be associated with an increased risk of gallbladder cancer. (See 'Adenomyomatosis' below.)
The most common malignant lesion in the gallbladder is adenocarcinoma. Gallbladder adenocarcinomas are much more common than gallbladder adenomas, in contrast to the colon where adenomas are much more common than adenocarcinomas. Squamous cell carcinomas, mucinous cystadenomas, and adenoacanthomas of the gallbladder are rare.
Seite 2 von 29Gallbladder polyps and cholesterolosis - UpToDate
29.10.2017https://www.uptodate.com/contents/gallbladder-polyps-and-cholesterolosis/print?source=search_result&search=gallenblasenpolypen&sel...

The main microscopic feature is the presence of fat laden macrophages within elongated villi. Most of the lipid in the cytoplasm of the macrophages is in the form of liquid crystals, which are birefringent under polarized light microscopy, giving the macrophages a characteristic foamy appearance (picture 2).
The hyperplastic villus is filled and distended with these cells, creating the small yellow nodules under the epithelium. In about two-thirds of cases, these nodules are less than 1 mm in diameter, which gives the mucosa the coarse and granular appearance that is characteristic of the diffuse or planar type of cholesterolosis. The nodules in the remaining one-third of cases are larger and polypoid in appearance (polypoid form) [10].
In the polypoid form, the deposits give rise to solitary or multiple cholesterol polyps that are attached to the underlying mucosa with a fragile epithelial pedicle, the core of which is composed of lipid filled macrophages. These polyps can break off, leading to complications similar to those caused by small gallstones including biliary pain, pancreatitis, and obstructive jaundice.
ADENOMYOMATOSIS — Adenomyomatosis is an abnormality of the gallbladder characterized by overgrowth of the mucosa, thickening of the muscle wall, and intramural diverticula. Despite the name, this condition does not involve any adenomatous changes in the gallbladder epithelium. While generally not considered to be a premalignant condition, adenomyomatosis is sometimes encountered in gallbladders resected for cancer, which has led to the suggestion that it is a premalignant condition [11]. However, the association and its magnitude remain unclear (see 'Adenomyomatosis and gallbladder cancer' below). There is, however, a clear association of adenomyomatosis with cholelithiasis, particularly with the segmental type, which was reported in 89 percent of patients with segmental adenomyomatosis in one series [12].
Epidemiology of adenomyomatosis — Adenomyomatosis of the gallbladder is less common than cholesterolosis in most reports [13], with some exceptions [14]. In one report, for example, only 103 cases of adenomyomatosis were found in over 10,000 cholecystectomies (1 percent) [13]. This is compared with the much higher prevalence of cholesterolosis (9 to 26 percent) [9]. Adenomyomatosis is more common in women.
Pathology of adenomyomatosis — The abnormality can be diffuse, segmental (annular), or localized to the fundus of the gallbladder.
Diffuse adenomyomatosis causes thickening and irregularity of the mucosal surface and the muscle coat leading to cystic-like structures in the gallbladder wall or polypoid projections from the mucosa of the gallbladder. In the early phases, the intramural extension of the epithelium creates tubules and crypts in the lamina propria that accumulate mucous. Fluid filled mucosal pockets eventually herniate into the wall of the gallbladder and through the muscularis propria, forming cystic structures that are visible on gross inspection as pools of bile in the gallbladder wall (Rokitansky-Aschoff sinuses). The point of herniation may appear sealed due to hypertrophy of the muscularis.
In the segmental type, a circumferential ring divides the gallbladder into separate interconnected compartments.
In the localized type, the cystic structure forms a nodule, usually in the fundus, that projects into the lumen giving the appearance of a polyp on ultrasonography [11,14-16]. The muscle layer in the involved area is usually thickened to three to five times its usual thickness [11,15].
Seite 3 von 29Gallbladder polyps and cholesterolosis - UpToDate
29.10.2017https://www.uptodate.com/contents/gallbladder-polyps-and-cholesterolosis/print?source=search_result&search=gallenblasenpolypen&sel...

Adenomyomatosis and gallbladder cancer — While generally not considered to be a premalignant condition, there have been several reports of gallbladder cancer arising in an area of segmental or fundal adenomyomatosis, but this association has not been a consistent finding in published series:
In a series of 3197 consecutive, unselected cholecystectomies, gallbladder cancer was found in 6.4 percent of patients with segmental adenomyomatosis compared with 3.1 percent of all other cholecystectomies [17].
At this time, there is no conclusive evidence that the presence of adenomyomatosis increases the risk of gallbladder cancer. If the risk is increased, the magnitude of the increased risk appears to be small (probably not more than twice the average risk). Finally, there is evidence that the presence of adenomyomatosis is associated with more advanced gallbladder cancer, possibly because its presence prevents early diagnosis of cancer on imaging studies.
INFLAMMATORY POLYPS — Inflammatory polyps are the least common of the non-neoplastic polyps. They appear as either sessile or pedunculated on an ultrasonographic examination and are composed of granulation and fibrous tissue with plasma cells and lymphocytes. Polyps are usually 5 to 10 mm in diameter, although inflammatory polyps larger than 1 cm have been described. These large polyps can be confused with gallbladder carcinoma [22].
In a similar retrospective series of 4560 patients, gallbladder cancer was identified in 6.6 percent of patients with segmental adenomyomatosis versus 4.3 percent in those without (p = 0.049) [18].
On the other hand, in a series of 4704 cholecystectomies, adenomyomatosis was found in 2.4 percent, but no cancer was identified in any of these patients' resected gallbladders [19].
In a series of 30 patients with adenomyomatosis of the gallbladder identified over seven years and comprising 3.3 percent of all cholecystectomies in that center, there were no cases of gallbladder cancer in any of these patients, but there was an association with gallstones [20].
In a series of 1099 patients who underwent cholecystectomy, adenomyomatosis was found in 14.2 percent with a strong association with gallstones but with no cases of cancer diagnosed [12].
One series suggested that gallbladder cancer in patients with adenomyomatosis may be associated with more advanced cancer; in a series of 97 patients with gallbladder cancer, 25 percent were positive for adenomyomatosis, and in these patients there was an increased risk for a more advanced T stage, lymph node, and distant metastasis. The authors suggested that the presence of adenomyomatosis may prevent early detection of gallbladder cancer [21].
Seite 4 von 29Gallbladder polyps and cholesterolosis - UpToDate
29.10.2017https://www.uptodate.com/contents/gallbladder-polyps-and-cholesterolosis/print?source=search_result&search=gallenblasenpolypen&sel...
ADENOMAS — Adenomatous polyps of the gallbladder are the most common benign tumors of the gallbladder but, unlike their colonic counterpart, are rare. Although the true incidence is unknown, in most series it is less than 0.5 percent. In one study, nine adenomatous polyps were identified among 2145 cholecystectomies (0.4 percent) [23].
Pathology of adenomas — Adenomas of the gallbladder are benign epithelial tumors composed of cells resembling biliary tract epithelium. These lesions are classified into papillary and non-papillary types on histology [5]. A classification similar to that of intestinal polyps has been proposed in which the adenomas are divided into tubular, papillary, and mixed [24].
The frequency of adenomas progressing to adenocarcinoma is unknown. In a series from Japan, 18 patients with adenomas were identified among 1605 cholecystectomies. Of these, seven adenomas contained foci of carcinoma [25]. Similar to intestinal adenomas, the risk of malignancy is related to the size of the polyp. In the Japanese series, none of the polyps less than 12 mm contained foci of malignancy.
In another review from 15 Japanese institutions, a 6 percent incidence of carcinoma was reported in lesions less than 1.0 cm, while the incidence was 37.5 percent in adenomas that were 1.0 to 2.0 cm [26]. In a third report in which nine adenomas were diagnosed among 2145 cholecystectomies, all of the nine polyps were less than 1 cm and none showed evidence for malignant changes [23]. (See "Gallbladder cancer: Epidemiology, risk factors, clinical features, and diagnosis", section on 'Molecular pathogenesis'.)
MISCELLANEOUS POLYPS — Other benign neoplasms of the gallbladder, such as fibromas, lipomas, and leiomyomas, are extremely rare. The natural history of these polyps is not well defined, but is probably similar to their counterparts in other regions of the gastrointestinal tract.
CLINICAL FEATURES — Polyps of the gallbladder are typically incidental findings detected during radiologic imaging of the abdomen. Their significance is related to their potential for malignancy. (See "Gallbladder cancer: Epidemiology, risk factors, clinical features, and diagnosis".)
Regardless of their type or etiology, gallbladder polyps can be associated with biliary pain. Proposed mechanisms of pain include prolapse of the polyp into Hartmann's pouch, which, if it occurs during gallbladder ejection, can lead to biliary-type pain that subsides upon spontaneous reduction [27]. Another possible mechanism is that a detached portion of a polyp lying free in the gallbladder lumen can obstruct the cystic duct in much the same way a gallstone would, leading to biliary colic or cholecystitis [28]. The detached portion can also obstruct the common bile duct, leading to obstructive jaundice [29] and pancreatitis [30].
In a review of 3,797 cholecystectomies, 55 cases of gallbladder cholesterolosis without cholelithiasis were identified. Twenty-seven of these patients presented with recurrent attacks of acute pancreatitis, which disappeared after cholecystectomy. The gallbladders had frank cholesterolosis with a polypoid appearance. The authors postulated that detached cholesterol polyps temporarily impact at the sphincter of Oddi, leading to pancreatitis [30].
In addition to biliary pain, cholesterolosis and adenomyomatosis have also been associated with chronic dyspeptic abdominal pain. In a study of 269 patients who underwent cholecystectomy and were found to have cholesterolosis, 96 percent had abdominal pain that was described as severe and in
Seite 5 von 29Gallbladder polyps and cholesterolosis - UpToDate
29.10.2017https://www.uptodate.com/contents/gallbladder-polyps-and-cholesterolosis/print?source=search_result&search=gallenblasenpolypen&sel...

a majority, the pain had persisted for more than two years. Other symptoms reported in the same study were nausea and vomiting (61 percent) and dyspepsia (60 percent). Most of these symptoms resolved after cholecystectomy [31]. In another study, 35 of 55 patients with chronic abdominal pain underwent cholecystectomy; cholesterolosis was found in 20 patients, 19 of whom had improvement in symptoms [32].
It has been suggested that polyps, cholesterolosis, and adenomyomatosis can lead to poor gallbladder emptying and compartmentalization that may be responsible for dyspeptic symptoms. However, the mechanism of these symptoms remains unclear since these observations have not been confirmed in other studies and the results of surgery are variable. Thus, it remains debatable whether these lesions can lead to chronic dyspeptic pain.
RISK OF MALIGNANCY — The most useful predictive feature for malignancy is the size of the polyp. Polyps larger than 2 cm are almost always malignant and, in many cases, the cancer is advanced. Polyps 1 to 2 cm in size should be regarded as possibly malignant. Several pathologic studies support this, with the incidence of carcinoma being 43 to 77 percent in polyps larger than 1 cm [33] and 100 percent in polyps larger than 2 cm [34]. Age is another risk factor. Several studies demonstrated that age older than 50 to 60 years is associated with a higher risk for malignant polyps [35]. (See "Gallbladder cancer: Epidemiology, risk factors, clinical features, and diagnosis".)
DIAGNOSIS — Advances in diagnostic imaging have resulted in improved sensitivity for the detection of gallbladder polyps. Although none of the available modalities can reliably predict polyp type, histology, or the presence of malignancy, a combination of features seen on an ultrasound, computed tomographic (CT) scan, and endoscopic ultrasound (EUS) can provide valuable information.
Ultrasonography
Conventional ultrasonography — Polyps are easily identified on ultrasonography as single or multiple echogenic foci. They can be easily differentiated from gallstones because they are fixed and do not move when the patient is rolled from one side to another. In addition, they do not cast a shadow (image 1). Ultrasonography can delineate other useful distinguishing characteristics in the appearance of polyps, including echogenicity, surface architecture, and the presence or absence of a pedicle.
The following characteristics have been noted [36]:
Cholesterol polyps are usually multiple, homogeneous, and pedunculated polypoid lesions that are more echogenic than the liver parenchyma (image 2). They may or may not contain hyperechoic spots and have a mulberry-like surface. Cholesterol polyps are usually smaller than 1 cm.
Adenomas are homogeneous, are isoechoic with the liver parenchyma, have a smooth surface, and usually do not have a pedicle (image 3).
Adenocarcinomas are homogeneous or heterogeneous polypoid structures that are usually isoechoic with the liver parenchyma and exhibit a mulberry-like surface [36].
Seite 6 von 29Gallbladder polyps and cholesterolosis - UpToDate
29.10.2017https://www.uptodate.com/contents/gallbladder-polyps-and-cholesterolosis/print?source=search_result&search=gallenblasenpolypen&sel...

In a report that used these criteria, preoperative ultrasonography correctly identified 89 percent of cholesterol polyps, 81 percent of malignant polyps, 50 percent of adenomas, and 0 percent of inflammatory polyps (table 2) [36].
In contrast to cholesterol polyps, diffuse cholesterolosis has no specific ultrasonographic finding. As a result, the diagnosis is usually made during surgery.
Contrast enhanced ultrasonography — Contrast enhancement using microbubble forming agents injected into the peripheral circulation is widely used with echocardiography in the United States, but it is also used for diagnostic ultrasonography in Europe and Japan to differentiate benign from malignant tumors. A few small studies suggest that contrast-enhanced ultrasound may facilitate the detection of gallbladder polyps by helping to distinguish them from mural folds, gallbladder contents, or sludge and also to detect invasion into the liver and metastasis [38,39].
Doppler ultrasonography — Several studies, primarily from Japan, have demonstrated that the use of Doppler ultrasound may also help differentiate benign lesions from primary gallbladder malignancies. These reports demonstrated that the presence of color signal, the pattern of the signal, the resistive index, and particularly flow velocity help to identify primary malignancy of the gallbladder from benign lesions. In most of these studies, color Doppler was more useful than conventional abdominal ultrasound in diagnosing gallbladder lesions, mostly due to estimation of arterial flow velocity; however, there was overlap in velocities, and depending on the cut-off of the flow velocity used, it was not fully capable of identifying all malignant lesions, particularly early T1 lesions, perhaps related to low sensitivity in detecting fine blood flow in these lesions [40-46].
High-resolution ultrasonography — High-resolution ultrasonography was found to have a diagnostic accuracy for gallbladder polyps comparable to EUS and superior to multidetector CT scan in one study [47].
Oral cholecystography — Oral cholecystography (OCG) has fallen out of favor since ultrasonography is much more sensitive and specific. OCG requires a functioning gallbladder and a patent cystic duct to visualize the gallbladder. Polyps appear as immobile filling defects which are usually difficult to differentiate from gallstones. Adenomyomatosis has a characteristic appearance of an invagination in the wall that may occasionally show Rokitansky-Aschoff sinuses (image 5). (See "Uncomplicated gallstone disease in adults", section on 'Oral cholecystography'.)
Computed tomography — CT scanning has low sensitivity for detecting small polyps. It is most useful in patients with gallbladder cancer since it can stage the disease by revealing liver invasion or metastasis. (See "Gallbladder cancer: Epidemiology, risk factors, clinical features, and diagnosis".)
When located in the fundus, adenomyomatosis can produce a mucosal projection that can give the appearance of a polyp on ultrasonography (image 4). These polypoid lesions are about 10 to 20 mm in diameter [37].
In patients with adenomyomatosis, ultrasonography shows non-specific focal thickening (>4 mm) of the gallbladder wall. Careful examination may predict the presence of adenomyomatosis by revealing diffuse or segmental thickening with round anechoic foci that represent the intramural diverticula.
Seite 7 von 29Gallbladder polyps and cholesterolosis - UpToDate
29.10.2017https://www.uptodate.com/contents/gallbladder-polyps-and-cholesterolosis/print?source=search_result&search=gallenblasenpolypen&sel...
There are only limited data regarding the use of the CT scan in the evaluation of gallbladder polyps:
A novel CT technique similar to CT colonography ("virtual colonoscopy") has been applied to the gallbladder. A pilot study suggested that it was more sensitive than standard CT and as sensitive as ultrasound for detecting gallbladder polyps [51]. It was more accurate than ultrasound in characterizing the three dimensional structure of the polyps. A clinical role for this technique remains to be defined.
Endoscopic ultrasonography — EUS has been increasingly used to diagnose malignancies and undefined lesions of the gastrointestinal tract. It is regarded as the most sensitive test for gallbladder imaging because of the advantage of imaging the gallbladder through the gastric wall, without deleterious attenuation by subcutaneous fat or interference from intestinal gas, which may limit the usefulness of conventional transabdominal ultrasonography. These benefits render EUS a more accurate imaging modality than transabdominal ultrasonography for differentiating between cholesterol and neoplastic polyps [52-57]. However, the role of EUS in establishing a strategy for the management of gallbladder polyps is not well defined.
One retrospective study attempted to define certain criteria for diagnosing cholesterol polyps, adenomyomatosis, and adenocarcinoma on EUS [52]. The presence of internal echo patterns characterized as tiny echogenic spots or an aggregation of multiple highly echogenic 1 to 3 mm spots, with or without echogenic areas, was considered diagnostic for cholesterol polyps. Adenomyomatosis (localized type) was associated with a sessile echogenic mass containing multiple microcysts (corresponding to the dilated Rokitansky-Aschoff sinuses) or a comet tail artifact. Lesions lacking these findings were found to be neoplastic (adenoma or adenocarcinoma).
One study noted 100 percent sensitivity of contrast enhanced CT for detecting gallbladder polyps in 20 patients who subsequently underwent cholecystectomy [48]. As in other studies, the size of the polyp was a predictor of malignancy. None of the six polyps less than 10 mm in diameter were neoplastic, while 5 of 14 polyps more than 10 mm in diameter were malignant and two were adenomas. Unenhanced CT detected four of five malignancies and both adenomas, whereas it missed all cholesterol and hyperplastic polyps. In addition, all cholesterol polyps were pedunculated, while most of the carcinomas were sessile (table 3). The authors concluded that pedunculated polyps smaller than 10 mm in diameter that are seen only on enhanced CT are very likely to be cholesterol polyps.
Similar results were noted in a study involving 59 patients who underwent ultrasound and CT scanning prior to laparoscopic cholecystectomy [49]. In that study, 36 percent of cholesterol polyps were seen by ultrasound and not by CT.
In a more recent study, 31 patients with 32 non-neoplastic polyps and 67 patients with 73 neoplastic polyps 10 mm or larger underwent unenhanced and dual-phase (arterial and portal venous phases) multi-detector row CT scan. Polyps larger than 15 mm, sessile polyps, and visualization on unenhanced images were associated with neoplastic polyps, differentiating them from non-neoplastic lesions [50]. However, multidetector CT scan was inferior to high-resolution ultrasound and EUS in detecting gallbladder polyps and predicting malignancy [47].
Seite 8 von 29Gallbladder polyps and cholesterolosis - UpToDate
29.10.2017https://www.uptodate.com/contents/gallbladder-polyps-and-cholesterolosis/print?source=search_result&search=gallenblasenpolypen&sel...

In a follow-up study by the same group using the same EUS criteria, a total of 194 patients with small (<20 mm) polypoid lesions underwent both transabdominal ultrasonography and EUS. Fifty-eight of these patients underwent surgery either because of symptoms or a suspicion of a neoplastic lesion on EUS. Using these criteria, EUS correctly predicted the histology in 97 percent of the patients compared with 76 percent for transabdominal ultrasonography (table 4) [53].
In other reports, investigators have relied on contour and internal echo patterns for differentiating neoplastic from non-neoplastic polyps [54,55]. In one study, the presence of hypoechoic foci on EUS was suggestive of adenomatous polyps, with a sensitivity and specificity of 90 and 89 percent, respectively. Contrast-enhanced harmonic EUS was used in two reports from Korea to differentiate between adenomatous and cholesterol polyps, with a reported sensitivity and specificity of 75 and 66 percent, respectively, with a slight increase in accuracy compared with conventional EUS[58,59].
Positron emission tomography (PET) — When gallbladder cancer is suggested by ultrasound findings, FDG-PET can help establish if the lesion is benign or malignant. However, it cannot be relied upon to exclude malignancy when ultrasound is highly suggestive of a neoplastic polyp [60].
MANAGEMENT — The only effective treatment for gallbladder polyps or cholesterolosis is cholecystectomy, which should be considered in symptomatic patients or as prophylaxis to prevent malignant transformation. Optimal follow-up of patients who do not undergo cholecystectomy is unclear since there have been few studies and no controlled trials comparing cholecystectomy to observation [61]. However, a reasonable approach is suggested below.
Although most gallbladder polyps are benign, the main objective is to exclude the presence of malignancy because advanced gallbladder cancer carries a poor prognosis and resection at an early stage offers the only hope for cure. What complicates matters is that none of the available imaging modalities can unequivocally distinguish neoplastic from non-neoplastic polyps. This can be achieved only by microscopic examination after surgery. Nevertheless, as discussed above, transabdominal ultrasonography and endoscopic ultrasonography can provide valuable information in the differential diagnosis of gallbladder polyps.
Polyps along with gallstones or primary sclerosing cholangitis — Patients who have gallbladder polyps and concomitant gallstones should undergo cholecystectomy regardless of the polyp size or the presence of symptoms, since gallstones are a risk factor for gallbladder cancer in patients with gallbladder polyps [1,62,63].
Gallbladder mass lesions/polyps are frequently encountered in patients with primary sclerosing cholangitis (PSC) and exhibit a high rate of malignancy. In a study of 102 patients with PSC undergoing cholecystectomy, 14 percent had mass lesions, and 57 percent of these were adenocarcinomas [64]. The American and European associations for the study of liver disease suggest an annual ultrasound for patients with primary sclerosing cholangitis and cholecystectomy when gallbladder polyps are found, regardless of the size [65]. This, however, is challenged by observations that gallbladder cancer is seen only in polyps greater than 8 mm and that cholecystectomy in patients with PSC and cirrhosis is
Seite 9 von 29Gallbladder polyps and cholesterolosis - UpToDate
29.10.2017https://www.uptodate.com/contents/gallbladder-polyps-and-cholesterolosis/print?source=search_result&search=gallenblasenpolypen&sel...

associated with high morbidity [66,67]. Nevertheless, there are reports of gallbladder cancer in PSC with polyps of 6 mm in size [68]. It is our approach to recommend a cholecystectomy for all patients with a polyp larger than 8 mm if they have PSC with cirrhosis and are good surgical candidates. If such patients have a less than 8 mm gallbladder polyp, we normally suggest close observation with an ultrasound evaluation every three to six months. However, for patients with PSC but without cirrhosis who are at average surgical risk, we consider a cholecystectomy for any polyp size. (See "Primary sclerosing cholangitis in adults: Clinical manifestations and diagnosis".)
Adenomyomatosis — Based on case reports and retrospective series that suggest a possible increased risk of gallbladder cancer in patients with adenomyomatosis, some authors recommend considering cholecystectomy for patients with adenomyomatosis. However, as discussed above, the association between gallbladder malignancy and adenomyomatosis is doubtful. (See 'Adenomyomatosis and gallbladder cancer' above.)
Furthermore, even if there is an increased risk of gallbladder cancer, the absolute risk for an individual patient remains small. Given the uncertainty and apparent small risk, we do not recommend cholecystectomy for patients with asymptomatic adenomyomatosis. While we do not have enough data to make preoperative predictions of which patients are at increased risk for cancer based on ultrasound or other imaging modalities, it should be kept in mind that the presence of adenomyomatosis may obscure an underlying cancer. In cases where there is concern that adenomyomatosis may be obscuring a malignancy, cholecystectomy is a reasonable alternative in patients who are fit for surgery.
Symptomatic patients — Cholecystectomy is recommended for patients who have biliary colic or pancreatitis, since an appreciable proportion of such patients with cholesterolosis or adenomyomatosis improve after cholecystectomy [29,31,32,69]. On the other hand, patients with non-specific dyspeptic symptoms but without symptoms consistent with biliary colic should be managed conservatively (unless other indications for polyp removal are present) since the pathogenesis of these symptoms is unclear and cholecystectomy may not relieve the symptoms. Such patients should be treated symptomatically, as are other patients with chronic functional dyspepsia [32]. (See "Approach to the adult with dyspepsia".)
Asymptomatic patients — Recommendations for patients who do not fall into any of the above categories depend upon the size of the polyps (algorithm 1).
Lesions larger than 20 mm — Lesions larger than 20 mm in diameter are usually malignant and should be resected. Because these lesions may represent advanced cancer, patients should undergo preoperative staging with a computed tomographic (CT) scan and endoscopic ultrasound. An extended cholecystectomy with lymph node dissection and partial hepatic resection in the gallbladder bed is required when performing cholecystectomy for malignancy [36]. (See "Gallbladder cancer: Epidemiology, risk factors, clinical features, and diagnosis".)
Lesions from 10 to 20 mm — Polyps 10 to 20 mm in diameter should be regarded as possibly malignant. Cancer of this size is usually at an early stage and laparoscopic cholecystectomy with full thickness dissection (removal of the entire connective tissue layers of the gallbladder bed to expose the liver surface) is recommended [36,69]. (See 'Risk of malignancy' above.)
Seite 10 von 29Gallbladder polyps and cholesterolosis - UpToDate
29.10.2017https://www.uptodate.com/contents/gallbladder-polyps-and-cholesterolosis/print?source=search_result&search=gallenblasenpolypen&sel...

Lesions from 6 to 9 mm — Lesions 6 to 9 mm in diameter may represent cholesterol polyps, adenomas, or carcinomas. Multiple polyps, pedunculated polyps, and those that are hyperechoic compared with the liver are usually cholesterol polyps, while solitary and sessile polyps that are isoechoic with the liver are more likely to be neoplastic. (See 'Conventional ultrasonography' above.)
The most reassuring finding is the stability of a polyp on repeated follow-up examinations, though there is no consensus regarding the frequency of follow-up ultrasounds. One group recommends follow-up ultrasounds of polyps 5 to 10 mm in diameter at three months, six months, and then yearly [33,70], whereas the American Society for Gastrointestinal Endoscopy recommends follow-up ultrasounds yearly [69].
The need for follow-up was demonstrated in a study of 1027 patients with gallbladder polyps who were followed for more than one year [71]. An increase in polyp size was noted in 36 patients (3.5 percent), of which nine (0.8 percent) were neoplastic (defined as either malignant or premalignant). Of those nine polyps, six were less than 10 mm in size prior to the start of follow-up. A more recent study with follow-up of 346 patients found no neoplastic polyps when the polyps were smaller than 6 mm, but it found one neoplastic polyp at 7 to 9 mm and two at 10 mm or larger [72].
We suggest following these polyps with an ultrasound every six months for a year and then yearly only if the polyp size is stable. Surgery is indicated in patients with an increase in polyp size.
Lesions 5 mm or smaller — Polyps 5 mm are usually benign and most frequently represent cholesterolosis. In a review of 203 patients with gallbladder polyps, 143 patients had polyp diameters 5 mm. On follow-up, these polyps were unchanged or decreased in size, and none of the 13 patients who underwent cholecystectomy had neoplastic or malignant polyps [73]. Asymptomatic patients with cholesterol polyps do not need treatment. However, a repeat ultrasound examination in 12 months is appropriate. Follow-up examinations are not necessary if the polyp is stable. Medical management aimed at increasing the solubility of cholesterol in bile by administering ursodeoxycholic acid is without benefit in patients with cholesterolosis [74].
SUMMARY AND RECOMMENDATIONS
Polypoid lesions in the gallbladder can be categorized as benign or malignant (table 1). Benign lesions are further subdivided into neoplastic (adenomas, leiomyomas, lipomas) or non-neoplastic (cholesterol polyps, inflammatory polyps). While generally not considered to be a premalignant condition, adenomyomatosis is sometimes encountered in gallbladders resected for cancer, which has led to the suggestion that it is a premalignant condition. However, the association and its magnitude remain unclear. (See 'Classification' above.)
Cholesterolosis results from abnormal deposits of triglycerides, cholesterol precursors, and cholesterol esters into the gallbladder mucosa. In about two-thirds of cases, these nodules are less than 1 mm in diameter. The nodules in the remaining one-third of cases are larger and polypoid in appearance (polypoid form). (See 'Cholesterolosis and cholesterol polyps' above.)
Seite 11 von 29Gallbladder polyps and cholesterolosis - UpToDate
29.10.2017https://www.uptodate.com/contents/gallbladder-polyps-and-cholesterolosis/print?source=search_result&search=gallenblasenpolypen&sel...

Use of UpToDate is subject to the Subscription and License Agreement.
REFERENCES
1. Yang HL, Sun YG, Wang Z. Polypoid lesions of the gallbladder: diagnosis and indications for surgery. Br J Surg 1992; 79:227.
2. Heyder N, Günter E, Giedl J, et al. [Polypoid lesions of the gallbladder]. Dtsch Med Wochenschr 1990; 115:243.
3. Jørgensen T, Jensen KH. Polyps in the gallbladder. A prevalence study. Scand J Gastroenterol 1990; 25:281.
4. Stringer MD, Ceylan H, Ward K, Wyatt JI. Gallbladder polyps in children--classification and management. J Pediatr Surg 2003; 38:1680.
5. Christensen AH, Ishak KG. Benign tumors and pseudotumors of the gallbladder. Report of 180 cases. Arch Pathol 1970; 90:423.
6. Weedon D. Benign mucosal polyps. In: Pathology of the gallbladder, Mason, New York 1984. p.195.
7. Laitio M. Histogenesis of epithelial neoplasms of human gallbladder II. Classification of carcinoma on the basis of morphological features. Pathol Res Pract 1983; 178:57.
8. JUTRAS JA. Hyperplastic cholecystoses; Hickey lecture, 1960. Am J Roentgenol Radium Ther Nucl Med 1960; 83:795.
9. SALMENKIVI K. CHOLESTEROSIS OF THE GALL-BLADDER. A CLINICAL STUDY BASED ON 269 CHOLECYSTECTOMIES. Acta Chir Scand Suppl 1964; 105:SUPPL 324:1.
10. FELDMAN M, FELDMAN M Jr. Cholesterosis of the gallbladder; an autopsy study of 165 cases. Gastroenterology 1954; 27:641.
Polyps of the gallbladder are typically incidental findings detected during radiologic imaging of the abdomen. Their significance is related to their potential for malignancy. (See 'Clinical features' above.)
Advances in diagnostic imaging have resulted in improved sensitivity for the detection of gallbladder polyps. Although none of the available modalities can reliably and unequivocally predict the type, histology, or the presence of malignancy, a combination of features seen on ultrasound, computed tomography, and endoscopic ultrasonograph can provide valuable information. (See 'Diagnosis' above.)
The only effective treatment for gallbladder polyps or cholesterolosis is cholecystectomy, which should be considered in symptomatic patients or as prophylaxis to prevent malignant transformation in some settings. We suggest cholecystectomy for patients with gallbladder polyps who also have gallstones, primary sclerosing cholangitis, biliary colic, or pancreatitis. Recommendations for patients who do not fit into these categories depend upon the size of the polyps (algorithm 1). (See 'Management' above.)
Seite 12 von 29Gallbladder polyps and cholesterolosis - UpToDate
29.10.2017https://www.uptodate.com/contents/gallbladder-polyps-and-cholesterolosis/print?source=search_result&search=gallenblasenpolypen&sel...

11. Maccarty WC. IV. The Pathology of the Gall-bladder and some Associated Lesions: A Study of Specimens from 365 Cholecystectomies. Ann Surg 1910; 51:651.
12. Nishimura A, Shirai Y, Hatakeyama K. Segmental adenomyomatosis of the gallbladder predisposes to cholecystolithiasis. J Hepatobiliary Pancreat Surg 2004; 11:342.
13. Shepard VD, Walters W, Dockerty MB. Benign neoplasms of the gallbladder. Arch Surg 1942; 45:1.
14. Jutras JA, Levesque HP. Adenomyoma and adenomyomatosis of the gallbladder, radiologic and pathologic correlations. Rad Clin N Amer 1966; 4:483.
15. BEAN BC, BERENS DL, CULVER GJ. The relationship of stenosis to Rokitansky Aschoff sinuses of the gallbladder. Am J Roentgenol Radium Ther Nucl Med 1957; 77:47.
16. King ES, McCallum P. Cholecystitis glandularis Proliferans. Br J Surg 1931; 19:310.
17. Ootani T, Shirai Y, Tsukada K, Muto T. Relationship between gallbladder carcinoma and the segmental type of adenomyomatosis of the gallbladder. Cancer 1992; 69:2647.
18. Nabatame N, Shirai Y, Nishimura A, et al. High risk of gallbladder carcinoma in elderly patients with segmental adenomyomatosis of the gallbladder. J Exp Clin Cancer Res 2004; 23:593.
19. Kim JH, Jeong IH, Han JH, et al. Clinical/pathological analysis of gallbladder adenomyomatosis; type and pathogenesis. Hepatogastroenterology 2010; 57:420.
20. Kasahara Y, Sonobe N, Tomiyoshi H, et al. Adenomyomatosis of the gallbladder: a clinical survey of 30 surgically treated patients. Nihon Geka Hokan 1992; 61:190.
21. Kai K, Ide T, Masuda M, et al. Clinicopathologic features of advanced gallbladder cancer associated with adenomyomatosis. Virchows Arch 2011; 459:573.
22. Maeyama R, Yamaguchi K, Noshiro H, et al. A large inflammatory polyp of the gallbladder masquerading as gallbladder carcinoma. J Gastroenterol 1998; 33:770.
23. Farinon AM, Pacella A, Cetta F, Sianesi M. "Adenomatous polyps of the gallbladder" adenomas of the gallbladder. HPB Surg 1991; 3:251.
24. Albores-Saaverdra J, Henson DE. Tumors of the gallbladder and the extrahepatic bile duct, 17-25. US Armed Forces Institute of Pathology, Washington, DC 1989.
25. Kozuka S, Tsubone N, Yasui A, Hachisuka K. Relation of adenoma to carcinoma in the gallbladder. Cancer 1982; 50:2226.
Seite 13 von 29Gallbladder polyps and cholesterolosis - UpToDate
29.10.2017https://www.uptodate.com/contents/gallbladder-polyps-and-cholesterolosis/print?source=search_result&search=gallenblasenpolypen&sel...

26. [Collective review of 503 cases of small polypoid lesions (less than 20mm in maximum diameter) of the gallbladder: size distribution in various diseases and the depth of carcinomatous invasion]. Nihon Shokakibyo Gakkai Zasshi 1986; 83:2086.
27. McGregor JC, Cordiner JW. Papilloma of the gallbladder. Br J Surg 1974; 61:356.
28. KANE CF, BROWN CH, HOERR SO. Papilloma of the gallbladder; report of eight cases. Am J Surg 1952; 83:161.
29. Takii Y, Shirai Y, Kanehara H, Hatakeyama K. Obstructive jaundice caused by a cholesterol polyp of the gallbladder: report of a case. Surg Today 1994; 24:1104.
30. Parrilla Paricio P, García Olmo D, Pellicer Franco E, et al. Gallbladder cholesterolosis: an aetiological factor in acute pancreatitis of uncertain origin. Br J Surg 1990; 77:735.
31. MITTY WF Jr, ROUSSELOT LM. Cholesterosis of the gall bladder. Gastroenterology 1957; 32:910.
32. Kmiot WA, Perry EP, Donovan IA, et al. Cholesterolosis in patients with chronic acalculous biliary pain. Br J Surg 1994; 81:112.
33. Koga A, Watanabe K, Fukuyama T, et al. Diagnosis and operative indications for polypoid lesions of the gallbladder. Arch Surg 1988; 123:26.
34. Ishikawa O, Ohhigashi H, Imaoka S, et al. The difference in malignancy between pedunculated and sessile polypoid lesions of the gallbladder. Am J Gastroenterol 1989; 84:1386.
35. Sarkut P, Kilicturgay S, Ozer A, et al. Gallbladder polyps: factors affecting surgical decision. World J Gastroenterol 2013; 19:4526.
36. Kubota K, Bandai Y, Noie T, et al. How should polypoid lesions of the gallbladder be treated in the era of laparoscopic cholecystectomy? Surgery 1995; 117:481.
37. Berk RN, van der Vegt JH, Lichtenstein JE. The hyperplastic cholecystoses: cholesterolosis and adenomyomatosis. Radiology 1983; 146:593.
38. Meacock LM, Sellars ME, Sidhu PS. Evaluation of gallbladder and biliary duct disease using microbubble contrast-enhanced ultrasound. Br J Radiol 2010; 83:615.
39. Tsuji S, Sofuni A, Moriyasu F, et al. Contrast-enhanced ultrasonography in the diagnosis of gallbladder disease. Hepatogastroenterology 2012; 59:336.
40. Li D, Dong BW, Wu YL, Yan K. Image-directed and color Doppler studies of gallbladder tumors. J Clin Ultrasound 1994; 22:551.
41. Hirooka Y, Naitoh Y, Goto H, et al. Differential diagnosis of gall-bladder masses using colour Doppler ultrasonography. J Gastroenterol Hepatol 1996; 11:840.
42. Li D. [Color Doppler flow imaging in gallbladder tumors]. Zhonghua Yi Xue Za Zhi 1992; 72:394.
43. Pradhan S, Shukla VK, Agrawal S, et al. Sonographic and colour doppler morphology in carcinoma gallbladder. Indian J Cancer 2002; 39:143.
Seite 14 von 29Gallbladder polyps and cholesterolosis - UpToDate
29.10.2017https://www.uptodate.com/contents/gallbladder-polyps-and-cholesterolosis/print?source=search_result&search=gallenblasenpolypen&sel...

44. Sato M, Ishida H, Konno K, et al. Localized gallbladder carcinoma: sonographic findings. Abdom Imaging 2001; 26:619.
45. Komatsuda T, Ishida H, Konno K, et al. Gallbladder carcinoma: color Doppler sonography. Abdom Imaging 2000; 25:194.
46. Hayakawa S, Goto H, Hirooka Y, et al. Colour Doppler-guided spectral analysis of gall-bladder wall flow. J Gastroenterol Hepatol 1998; 13:181.
47. Jang JY, Kim SW, Lee SE, et al. Differential diagnostic and staging accuracies of high resolution ultrasonography, endoscopic ultrasonography, and multidetector computed tomography for gallbladder polypoid lesions and gallbladder cancer. Ann Surg 2009; 250:943.
48. Furukawa H, Takayasu K, Mukai K, et al. CT evaluation of small polypoid lesions of the gallbladder. Hepatogastroenterology 1995; 42:800.
49. Choi JH, Yun JW, Kim YS, et al. Pre-operative predictive factors for gallbladder cholesterol polyps using conventional diagnostic imaging. World J Gastroenterol 2008; 14:6831.
50. Park KW, Kim SH, Choi SH, Lee WJ. Differentiation of nonneoplastic and neoplastic gallbladder polyps 1 cm or bigger with multi-detector row computed tomography. J Comput Assist Tomogr 2010; 34:135.
51. Lou MW, Hu WD, Fan Y, et al. CT biliary cystoscopy of gallbladder polyps. World J Gastroenterol 2004; 10:1204.
52. Sugiyama M, Xie XY, Atomi Y, Saito M. Differential diagnosis of small polypoid lesions of the gallbladder: the value of endoscopic ultrasonography. Ann Surg 1999; 229:498.
53. Sugiyama M, Atomi Y, Yamato T. Endoscopic ultrasonography for differential diagnosis of polypoid gall bladder lesions: analysis in surgical and follow up series. Gut 2000; 46:250.
54. Kimura K. [Diagnosis for pedunculated polypoid lesions of the gallbladder by endoscopic ultrasonography]. Nihon Shokakibyo Gakkai Zasshi 1997; 94:249.
55. Matsumoto J. Endoscopic ultrasonography diagnosis of gallbladder lesions. Endoscopy 1998; 30 Suppl 1:A124.
56. Azuma T, Yoshikawa T, Araida T, Takasaki K. Differential diagnosis of polypoid lesions of the gallbladder by endoscopic ultrasonography. Am J Surg 2001; 181:65.
57. Muguruma N, Okamura S, Ichikawa S, et al. Endoscopic sonography in the diagnosis of gallbladder wall lesions in patients with gallstones. J Clin Ultrasound 2001; 29:395.
58. Park CH, Chung MJ, Oh TG, et al. Differential diagnosis between gallbladder adenomas and cholesterol polyps on contrast-enhanced harmonic endoscopic ultrasonography. Surg Endosc 2013; 27:1414.
59. Choi JH, Seo DW, Choi JH, et al. Utility of contrast-enhanced harmonic EUS in the diagnosis of malignant gallbladder polyps (with videos). Gastrointest Endosc 2013; 78:484.
Seite 15 von 29Gallbladder polyps and cholesterolosis - UpToDate
29.10.2017https://www.uptodate.com/contents/gallbladder-polyps-and-cholesterolosis/print?source=search_result&search=gallenblasenpolypen&sel...

60. Rodríguez-Fernández A, Gómez-Río M, Medina-Benítez A, et al. Application of modern imaging methods in diagnosis of gallbladder cancer. J Surg Oncol 2006; 93:650.
61. Gurusamy KS, Abu-Amara M, Farouk M, Davidson BR. Cholecystectomy for gallbladder polyp. Cochrane Database Syst Rev 2009; :CD007052.
62. Patiño JF, Quintero GA. Asymptomatic cholelithiasis revisited. World J Surg 1998; 22:1119.
63. Terzi C, Sökmen S, Seçkin S, et al. Polypoid lesions of the gallbladder: report of 100 cases with special reference to operative indications. Surgery 2000; 127:622.
64. Buckles DC, Lindor KD, Larusso NF, et al. In primary sclerosing cholangitis, gallbladder polyps are frequently malignant. Am J Gastroenterol 2002; 97:1138.
65. Chapman R, Fevery J, Kalloo A, et al. Diagnosis and management of primary sclerosing cholangitis. Hepatology 2010; 51:660.
66. Eaton JE, Thackeray EW, Lindor KD. Likelihood of malignancy in gallbladder polyps and outcomes following cholecystectomy in primary sclerosing cholangitis. Am J Gastroenterol 2012; 107:431.
67. Razumilava N, Gores GJ, Lindor KD. Cancer surveillance in patients with primary sclerosing cholangitis. Hepatology 2011; 54:1842.
68. Schramm C, Lohse AW. Gallbladder polyps in primary sclerosing cholangitis: indication for early intervention. Hepatology 2012; 56:396; author reply 396.
69. American Society for Gastrointestinal Endoscopy (ASGE) Standards of Practice Committee, Anderson MA, Appalaneni V, et al. The role of endoscopy in the evaluation and treatment of patients with biliary neoplasia. Gastrointest Endosc 2013; 77:167.
70. Koga A, Yamauchi S, Nakayama F. Primary carcinoma of the gallbladder. Am Surg 1985; 51:529.
71. Park JY, Hong SP, Kim YJ, et al. Long-term follow up of gallbladder polyps. J Gastroenterol Hepatol 2009; 24:219.
72. Corwin MT, Siewert B, Sheiman RG, Kane RA. Incidentally detected gallbladder polyps: is follow-up necessary?--Long-term clinical and US analysis of 346 patients. Radiology 2011; 258:277.
73. Pedersen MR, Dam C, Rafaelsen SR. Ultrasound follow-up for gallbladder polyps less than 6 mm may not be necessary. Dan Med J 2012; 59:A4503.
74. Yamamoto T. [A study of cholesterol gallstone formation in cases of cholesterolosis of the gallbladder (author's transl)]. Nihon Shokakibyo Gakkai Zasshi 1979; 76:91.
Topic 646 Version 16.0
Seite 16 von 29Gallbladder polyps and cholesterolosis - UpToDate
29.10.2017https://www.uptodate.com/contents/gallbladder-polyps-and-cholesterolosis/print?source=search_result&search=gallenblasenpolypen&sel...

GRAPHICS
Relative frequency of the different pathologic types of gallbladder polyps
Type Frequency
Benign polyps
Cholesterol polyps 60%
Adenomyomas 25%
Inflammatory polyps 10%
Adenomas 4%
Miscellaneous: 1%
Leiomyomas
Fibromas
Lipomas, etc
Malignant polyps
Adenocarcinoma 80%
Miscellaneous: 20%
Mucinous cystadenomas
Squamous cell carcinoma
Adenoacanthomas
Data from: Weedon, D. Benign mucosal polyps. In pathology of the gallbladder, Mason, New York 1984. p.195. and Laitio, M, Pathol Res Pract 1983; 178:57.
Graphic 56347 Version 2.0
Seite 17 von 29Gallbladder polyps and cholesterolosis - UpToDate
29.10.2017https://www.uptodate.com/contents/gallbladder-polyps-and-cholesterolosis/print?source=search_result&search=gallenblasenpolypen&sel...
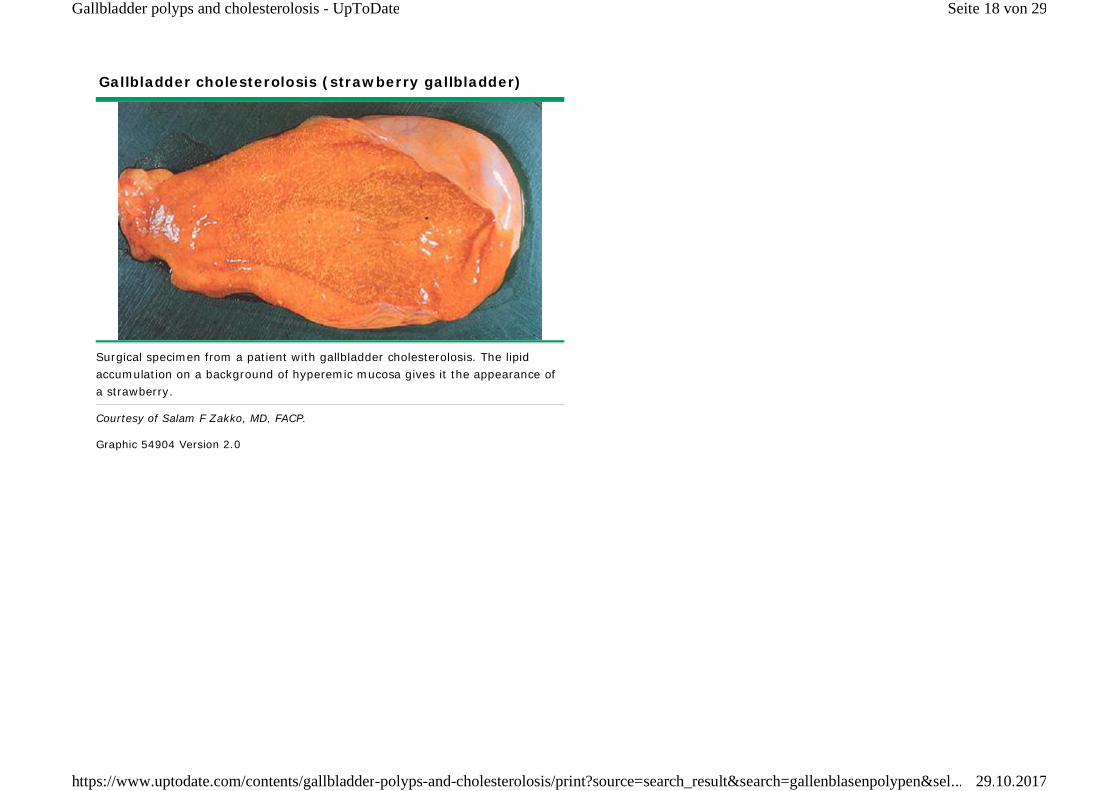
Gallbladder cholesterolosis (strawberry gallbladder)
Surgical specimen from a patient with gallbladder cholesterolosis. The lipid accumulation on a background of hyperemic mucosa gives it the appearance of a strawberry.
Courtesy of Salam F Zakko, MD, FACP.
Graphic 54904 Version 2.0
Seite 18 von 29Gallbladder polyps and cholesterolosis - UpToDate
29.10.2017https://www.uptodate.com/contents/gallbladder-polyps-and-cholesterolosis/print?source=search_result&search=gallenblasenpolypen&sel...

Gallbladder cholesterolosis
Microscopic appearance of the gallbladder wall from a specimen demonstrating cholesterolosis. The villi are elongated and contain lipid-laden macrophages.
Courtesy of Salam F Zakko, MD, FACP.
Graphic 60481 Version 2.0
Seite 19 von 29Gallbladder polyps and cholesterolosis - UpToDate
29.10.2017https://www.uptodate.com/contents/gallbladder-polyps-and-cholesterolosis/print?source=search_result&search=gallenblasenpolypen&sel...

Gallbladder polyp versus gallstone on ultrasound
Ultrasound images of a gallbladder adenomatous polyp (arrow) compared with a gallstone (arrowhead). Note the shadow cast by the stone (dashed arrow) compared with the absence of a shadow behind the polyp.
Courtesy of Salam F Zakko, MD, FACP.
Graphic 70175 Version 4.0
Seite 20 von 29Gallbladder polyps and cholesterolosis - UpToDate
29.10.2017https://www.uptodate.com/contents/gallbladder-polyps-and-cholesterolosis/print?source=search_result&search=gallenblasenpolypen&sel...

Cholesterolosis and multiple cholesterol gallbladder polyps
Ultrasound imaging demonstrating cholesterol polyps and thickening of the gallbladder wall. Note that the polyps appear much denser than the surrounding liver tissue.
Courtesy of Salam F Zakko, MD, FACP.
Graphic 73242 Version 2.0
Seite 21 von 29Gallbladder polyps and cholesterolosis - UpToDate
29.10.2017https://www.uptodate.com/contents/gallbladder-polyps-and-cholesterolosis/print?source=search_result&search=gallenblasenpolypen&sel...

Gallbladder adenomatous polyp
Gallbladder ultrasonography showing an adenomatous polyp. Note its homogeneous appearance and density that is similar to the surrounding liver tissue.
Courtesy of Salam F Zakko, MD, FACP.
Graphic 71629 Version 2.0
Seite 22 von 29Gallbladder polyps and cholesterolosis - UpToDate
29.10.2017https://www.uptodate.com/contents/gallbladder-polyps-and-cholesterolosis/print?source=search_result&search=gallenblasenpolypen&sel...

Gallbladder adenomyomatosis
Ultrasound image of localized adenomyomatosis in the gallbladder fundus (arrow) producing a polypoid appearance.
Courtesy of Salam F Zakko, MD, FACP.
Graphic 80707 Version 2.0
Seite 23 von 29Gallbladder polyps and cholesterolosis - UpToDate
29.10.2017https://www.uptodate.com/contents/gallbladder-polyps-and-cholesterolosis/print?source=search_result&search=gallenblasenpolypen&sel...

Preoperative ultrasonographic accuracy for histologic diagnosis of gallbladder polyps
Preoperative diagnosis Number of patientsHistologic diagnosis
Cholesterol polyp Adenoma Cancer Inflammatory polyp
Cholesterol polyp 47 42 3 1 1
Adenoma 7 1 4 2 0
Cancer 18 4 1 13 0
Total 72 47 8 16 0
Data from: Kubota, K, Bandai, Y, Noie, T, et al, Surgery 1995; 117:481.
Graphic 79560 Version 1.0
Seite 24 von 29Gallbladder polyps and cholesterolosis - UpToDate
29.10.2017https://www.uptodate.com/contents/gallbladder-polyps-and-cholesterolosis/print?source=search_result&search=gallenblasenpolypen&sel...
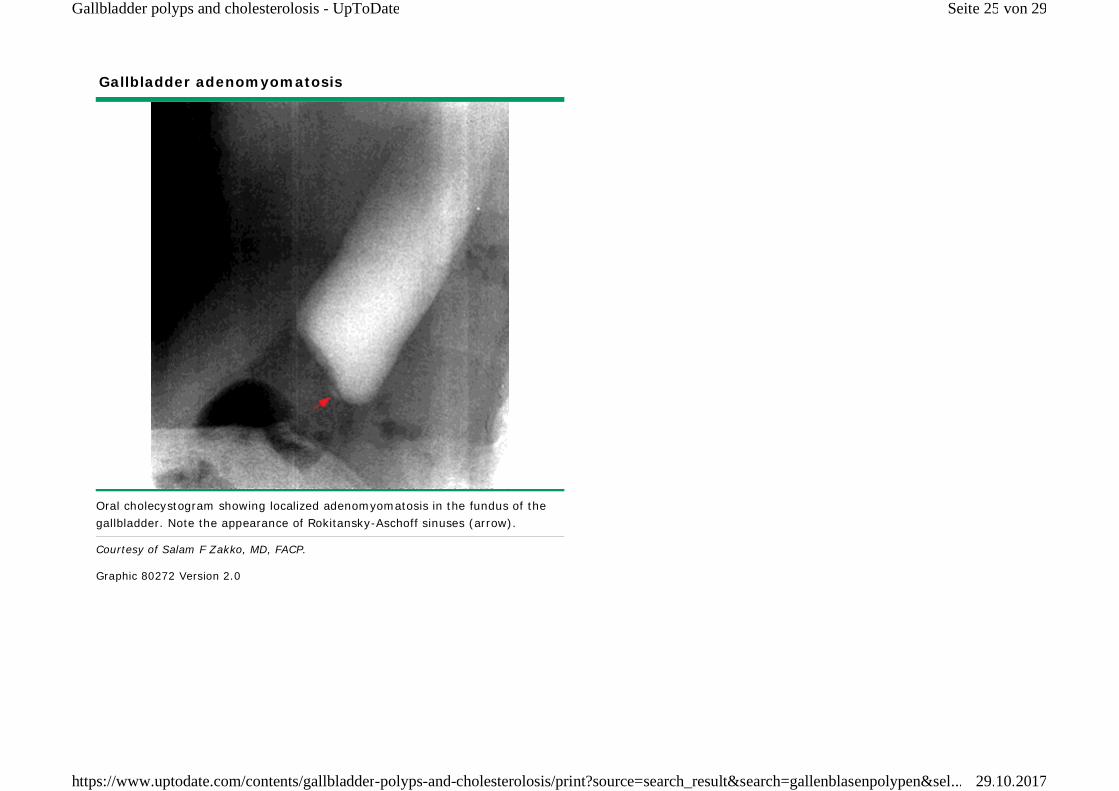
Gallbladder adenomyomatosis
Oral cholecystogram showing localized adenomyomatosis in the fundus of the gallbladder. Note the appearance of Rokitansky-Aschoff sinuses (arrow).
Courtesy of Salam F Zakko, MD, FACP.
Graphic 80272 Version 2.0
Seite 25 von 29Gallbladder polyps and cholesterolosis - UpToDate
29.10.2017https://www.uptodate.com/contents/gallbladder-polyps-and-cholesterolosis/print?source=search_result&search=gallenblasenpolypen&sel...

Computed tomography of gallbladder polyps
Histopathology No. of patients Plain CT Contrast CTType of lesion Size of polyp
Pedunculated Sessile Mass <1 cm 1-2 cm
Cholesterol polyp 9 0 8 9 0 0 4 5
Hyperplastic polyp 2 0 2 2 0 0 2 0
Adenomyomatosis 2 2 2 0 0 2 0 2
Adenoma 2 2 2 1 0 1 0 2
Adenocarcinoma 5 4 5 1 4 0 0 5
Total 20 8 20 13 4 3 6 14
Data from: Furukawa, H, Takayasu, K, Mukai, K, et al, Hepatogastroenterology 1995; 42:800.
Graphic 50583 Version 1.0
Seite 26 von 29Gallbladder polyps and cholesterolosis - UpToDate
29.10.2017https://www.uptodate.com/contents/gallbladder-polyps-and-cholesterolosis/print?source=search_result&search=gallenblasenpolypen&sel...

Endoscopic ultrasonography for the differential diagnosis of polypoid gallbladder lesions
Number of patientsHistologic diagnosis
Cholesterol polyp Adenomyomatosis Neoplastic
Preoperative diagnosis with endoscopic US
Cholesterol polyp 34 34 0 0
Adenomyomatosis 7 0 7 0
Neoplastic 17 2 0 15
Preoperative diagnosis with transabdominal US
Cholesterol polyp 24 24 0 0
Adenomymatosis 5 0 5 0
Neoplastic 29 12 2 15
US: ultrasound.
Data from: Sugiyama, M, Xie, XY, Atomi, Y, Saito, M, Ann Surg 1999; 229:498.
Graphic 52861 Version 2.0
Seite 27 von 29Gallbladder polyps and cholesterolosis - UpToDate
29.10.2017https://www.uptodate.com/contents/gallbladder-polyps-and-cholesterolosis/print?source=search_result&search=gallenblasenpolypen&sel...

Contributor Disclosures
Wisam F Zakko, MD Nothing to disclose Salam F Zakko, MD, FACP Nothing to disclose Sanjiv Chopra, MD, MACP Nothing to disclose Shilpa Grover, MD, MPH, AGAF Other Financial Interest: Honorarium (travel)- Novartis ($3,000)
A suggested algorithm for managing gallbladder polyps found on ultrasound
* An extended cholecystectomy includes lymph node dissection and partial hepatic resection in the gallbladder bed.¶ Symptoms: Biliary type pain, common duct obstruction, cholangitis, or recurrent pancreatitis. Dyspepsia is not an indication for surgery.
Graphic 73510 Version 5.0
Seite 28 von 29Gallbladder polyps and cholesterolosis - UpToDate
29.10.2017https://www.uptodate.com/contents/gallbladder-polyps-and-cholesterolosis/print?source=search_result&search=gallenblasenpolypen&sel...

Contributor disclosures are reviewed for conflicts of interest by the editorial group. When found, these are addressed by vetting through a multi-level review process, and through requirements for references to be provided to support the content. Appropriately referenced content is required of all authors and must conform to UpToDate standards of evidence.
Conflict of interest policy
Seite 29 von 29Gallbladder polyps and cholesterolosis - UpToDate
29.10.2017https://www.uptodate.com/contents/gallbladder-polyps-and-cholesterolosis/print?source=search_result&search=gallenblasenpolypen&sel...

















