There’s only one - Science | AAAS · ii There’s only one Galileo Galilei Career advice I Job...
72
Transcript of There’s only one - Science | AAAS · ii There’s only one Galileo Galilei Career advice I Job...

ii
There’s only one Galileo Galilei
Career advice I Job postings I Job Alerts I Career Forum I Crafting resumes/CVs I Preparing for interviews
For your career in science, there’s only one
Careers
ScienceCareers.org
orn in 1564, Galileo Galilei once contemplated a career in the priesthood. It’s perhaps fortunate for science that upon the urging of his father, he instead decided to enroll at the University of Pisa. His career in science began with medicine and from there he subsequently went on to become a philosopher, physicist, mathematician, and astronomer, for which he is perhaps best known. His astronomical observations and subsequent improvements to telescopes built his reputation as a leading scientist of his time, but also led him to probe subject matter counter to prevailing dogma. His expressed views on the Earth’s movement around the sun caused him to be declared suspect of heresy, which for some time led to a ban on the reprinting of his works. Galileo’s career changed science for all of us and he was without doubt a leading light in the scientifi c revolution, which is perhaps why Albert Einstein called him the father of modern science. Want to challenge the status quo and make the Earth move? At Science we are here to help you in your own scientifi c career with expert career advice, forums, job postings, and more — all for free. For your career in science, there’s only one Science. Visit Science today at ScienceCareers.org.
B
Galileo_full.indd 1 8/2/12 1:49 PM

Introductions
3.... High-Altitude Medical Research in China: Importance and Relevance Wu Tianyi, M.D.
4.... Research Atop the Roof of the World Alan Leshner, Ph.D.
High-Altitude Medicine
1
Table of Contents
6.... A Unique Challenge in High-Altitude Medicine: The Qinghai-Tibet Railroad
7.... Human Performance Engineering at High Altitude
9.... Intrinsic Characteristics in Tibetans of Tolerance to Hypoxia Following Long Periods at Sea Level
10.... Exploration and Evidence of High-Altitude Adaptation in Tibetan Highlanders
12.... Peopling of the Tibetan Plateau and Genetic Adaptation to High-Altitude Hypoxia in Tibetans
14.... New Approaches for Facilitating High-Altitude Acclimatization
15.... Evidence for Genetic Contribution to High-Altitude Pulmonary Edema in Chinese Railway Construction Workers
17.... Studies on the Prevention of Acute Mountain Sickness in People Entering High Altitudes by Airplane
18.... Adaptive Responses of the Brain to High-Altitude
20.... Mechanism of Chronic Intermittent Hypoxia-Induced Impairment in Synaptic Plasticity and Neurocognitive Dysfunction
22.... Chinese Herbs and Altitude Sickness: Lessons from Hypoxic Pulmonary Hypertension Research
24.... Fast Acclimatization to High Altitude Using an Oxygen-Enriched Room
25.... A Comparison of Perimenopausal Sex Hormone Levels Between Tibetan Women at Various Altitudes and Han Women at Sea Level
26.... Diagnosis and Treatment of HAPE and HACE in the Tibet High-Altitude Region in the Last Decade
27.... Cardiac Surgery on the Tibetan Plateau: From Impossible to Successful
28.... Acute Mountain Sickness on the Tibetan Plateau: Epidemiological Study and Systematic Prevention
29.... Study on Erythrocyte Immune Function and Gastrointestinal Mucosa Barrier Function After Rapid Ascent to High Altitude
30.... Basic Methods and Application of Altitude Training on the Chinese Plateau
31.... Hypoxic Preconditioning at High Altitude Improves Cerebral Reserve Capacity
33.... The Dynamic Balance Between Adaptation and Lesions of the Cardiovascular System in Tibetans Living at High-Altitude
34.... Establishment of an Improved Bundle Therapy Procedure for Acute High-Altitude Disease
36.... Differences in Physiological Adaptive Strategies to Hypoxic Environments in Plateau Zokor and Plateau Pika
Section One

2
Table of Contents
38.... Cardioprotective Effect of Chronic Intermittent Hypobaric Hypoxia
40.... Corticotropin-Releasing Factor Type-1 Receptors Play a Crucial Role in the Brain-Endocrine Network Disorder Induced by High-Altitude Hypoxia
42.... The Key Role of Vascular Endothelial Dysfunction in Injuries Induced by Extreme Environmental Factors at High Altitude
45.... Targeting Endothelial Dysfunction in High-Altitude Illness with a Novel Adenosine Triphosphate-Sensitive Potassium Channel Opener
47.... Adaptation to Intermittent Hypoxia Protects the Heart from Ischemia/ Reperfusion Injury and Myocardial Infarction
49.... Mild Hypoxia Regulates the Properties and Functions of Neural Stem Cells In Vitro
51.... Hypobaric Hypoxia or Hyperbaric Oxygen Preconditioning Reduces High-Altitude Lung and Brain Injury in Rats
53.... Mitochondria: A Potential Target in High-Altitude Acclimatization/ Adaptation and Mountain Sickness
55.... Mimicking Hypoxic Preconditioning Using Chinese Medicinal Herb Extracts
57.... Molecular Path Finding: Insight into Cerebral Ischemic/Hypoxic Injury and PreconditioningbyStudyingPKC-isoformSpecificSignalingPathways
59.... Hypoxic Preconditioning Enhances the Potentially Therapeutic Secretome from Cultured Human Mesenchymal Stem Cells in Experimental Traumatic Brain Injury
61.... Mitochondrial Adaptation and Cell Volume Regulation in Hypoxic Preconditioning Contribute to Anoxic Tolerance
62.... The Effects of Ratanasampil, a Traditional Tibetan Medicine, on β-amyloidPathologyinaTransgenicMouseModelandClinicalTrial of AlzheimerÕ s Disease
63.... Duoxuekang, a Traditional Tibetan Medicine, Reduces Hypoxia-Induced High Altitude Polycythemia in Rats
64.... k-opioid Receptor and Hypoxic Pulmonary Hypertension
66.... Paracrine-Autocrine Mechanisms in the Carotid Body Function at High Altitude and in Disease
Hypoxic Physiology
Section Two
This booklet was produced by the Science/AAASCustomPublishingOfficeandsponsoredby the National Key Basic Research Program of China (Ò 973Ó Program). Materials that appear in this booklet were commissioned, edited, and published by the Science/AAAS CustomPublishingOfficeandwerenotreviewedorassessedbytheScience Editorial staff.
This booklet was produced in association with the Beijing Institute of Basic Medical Sciences.
Editors: Sean Sanders, Ph.D.; Fan Ming, Ph.D. Assistant Editor: Lingling Zhu, Ph.D.Proofing:YuseLajiminmuhip;Design:AmyHardcastle
© 2012 by The American Association for the Advancement of Science. All rights reserved. 14 December 2012
ABOUT THE COVER: Mount Qomo Lhari, which stands 7,314 m high and is known in Tibetan as the Ò Goddess Peak,Ó has yet to be conquered by humans. The sharp and forbidding peak, with its encircling white clouds, carries the message of good luck to those setting out to explore the unknown.Photo credit: Gesang Luobu and Shilie Jiangca

3
In the last 30 years, great strides have been made in high-altitude medical research in China due in large part to the unique set of circumstances in the country. China encompasses a vast andmountainousregionwithfourhighplateaus(theQinghai-Tibet,InnerMongolia,Yun-Gui,andtheYellowLandPlateaus).TheQinghai-TibetPlateau,theEarth’slargestandhighest,issometimes called the Ò the roof of the world.Ó Altitude-related health problems are particularly important in China since nearly 80 million people live above 2,500 m with more than 12 million residing on the Qinghai-Tibet Plateau alone. Additionally, large, rich deposits of valuable ores, precious metals, and oil have been discovered recently in Tibet, where the most important mines are located above 4,000 m and the miners living there experience chronic hypoxia (reduced oxygen supply). Finally, to support industrial development in western China, the new 1,142 km long Qinghai-Tibet Railway has been recently completed. Over 85% of the rail line is above 4,000 m, even reaching 5,072 m. During construction of the railway from 2001 to 2005, approximately 140,000 workers were required to labor in a severely hypoxic environment, emphasizingtheneedtounderstandandtreataltitude-specificillnesses.
In Tibet, native populations of differing origin have been living at high altitude for varying lengths of time, making the Tibetan plateau a natural location for comparing the effect of high altitude on biologically distinct populations. Han Chinese inhabitants are newcomers to these higher elevations, having come from low altitudes within the past one to three generations. They therefore typically tolerate hypoxia poorly and are only weakly acclimatized to high altitude. By contrast, the Tibetans are an indigenous Himalayan population who are reproductively isolated and genetically stable due to limited intermarriage. Archaeological evidence indicates that primitive societies have existed in northern Tibet for 25,000 to 50,000 years. Tibetans are therefore considered to be well-adapted to hypoxic conditions and form a unique group for the study of the chronic effects of hypoxia on human physiology and disease.
Recently studies have shown that Tibetans, compared with Han lowlanders, maintain higher arterial oxygen saturation at rest and during exercise with increasing altitude, and show reduced loss of aerobic performance. Tibetans have greater hypoxic and hypercapnic ventilatory responsiveness, large lungs, better lung function, and greater lung diffusing capacity than Han lowlanders. Additionally, Tibetans develop only minimal hypoxic pulmonary vasoconstriction and have higher levels of exhaled nitric oxide. The sleep quality of Tibetans at altitude is better thanHan lowlandersandtheirbloodoxygen levelsdrop lessatnight.Thesefindingsareallindicative of remarkable high-altitude adaptation.
The Tibetan and Han Chinese populations also provide an ideal opportunity to study genetic predisposition to high-altitude disease. Chronic mountain sickness (CMS) in particular is a public health problem in Qinghai-Tibet. Epidemiological data indicates that CMS is found in Han immigrants at a rate of 5% to 10%. In contrast, CMS is rare in Tibetans (0.5% prevalence). Physiological data from multiple studies supports the possibility that the Tibetans carry protective genetic factors. Of particular interest is the lower average hemoglobin concentration in Tibetans compared with Han Chinese living at the same altitude. Excessive hemoglobin, known as polycythemia, is a hallmark of CMS and is caused by the bodyÕ s overreaction to altitude hypoxia, resulting in characteristically viscous blood. Tibetans maintain relatively low hemoglobin at high altitude, a trait that makes them less susceptible to CMS than immigrants. To pinpoint the genetic origin underlying TibetansÕ relatively low hemoglobin levels, recent research in China, England, Ireland, and the United States comparing DNA from Tibetans with their Han lowland counterparts, found variations in a gene called EPAS1 (endothelial PAS domain protein 1, also known as HIF2A, hypoxia inducible factor 2A). These genetic differences are thought to be responsible for the low blood hemoglobin and resulting CMS protective effects. Although muchworkremainstodetermineifotherphysiologicalfactorsmaybeatwork,thesefindingshave opened a new era in our understanding of genetic adaptation among Tibetans.
With an increasing number of people moving to the higher altitudes, the study of physiological adaptation to hypoxia and related diseases is growing in importance, making life on the Tibetan plateauoneofthemostrelevantresearchfieldsinourregion.
Wu Tianyi, M.D.Member of the Chinese Academy of EngineeringProfessor, High Altitude Medical Research Center, University of Tibet, Lhasa, ChinaDirector, High Altitude Medical Research Institute, Qinghai, China
High-Altitude Medical Research in China: Importance and Relevance
Tibetans are considered to be well-adapted to hypoxic conditions and form a unique group for the study of the chronic effects of hypoxia on human physiology and disease.

4
It would make sense that a primary reason for the success of the human race at populating almost every corner of the planetÕ s surface is our ability to adapt to the majority of climates and environmental conditions. From the hottest deserts to the coldest and most barren arctic landscapes, humans have made their homes. It hasnÕ t always been easy, though.
One of the more extreme climes that humans have settled must surely be the Qinghai-Tibet region of western China, the worldÕ s largest and highest plateau. This often inhospitable landscape offers its courageous inhabitants frigid temperatures, thin atmosphere, and hypoxic (low oxygen) conditions.Thisbooklet,aneditorialcollaborationbetweentheCustomPublishingOfficeatthejournal
Scienceand topresearchers in thefieldofhigh-altitudemedicineandhypoxicphysiology inChina, provides scientists around the globe with a window into some of the fascinating research beingcarriedoutinthisfield,usingtheQinghai-TibetPlateauasatestbed.Briefreviewsinanarray of different areas of study are presented, together highlighting the many advances that have been made in the understanding, treatment, and prevention of high-altitude sickness.
Each year, chronic and acute mountain sickness claims the lives of many unsuspecting or even well-prepared travelers to these high-altitude regions, and a greater number are sickened or permanently disabled. Extensive efforts are under way by doctors and researchers in China to develop improved treatments and preventative measures that will allow for safer travel and long-term habitation in the region. An array of studies are under way attempting to elucidate the underlying mechanism for high-altitude illnesses and thereby development suitable treatments. Interventions range from the use of conventional Western medicine to specialized physical exercise regimens that speed acclimation and minimize potential health issues. Traditional Chinese medicines that, in some cases, have been used for many hundreds of years are alsobeingmorecloselyandsystematicallystudiedfortheirefficacyinpreventingorreducingaltitude-related ailments.
Also intensively studied is the role that genetics and evolution might play in the adaptation of long-term plateau dwellers. Although hard evidence of sustained occupation is scarce, native Tibetans are believed to have lived on the Qinghai-Tibet Plateau for upward of 25,000 years, potentially enough time for them to gain a genetic advantage over their lowland ancestors. Elucidation of the particular DNA changes they might have acquired may provide researchers with some clues about where to look for possible drug targets.
So whether by genetic adaptation or through the application of our knowledge, experience, and intellect, humans are continuing to adjust to harsh conditions on the Tibetan plateau and expand our understanding of the effect of extreme environments on our bodies. What researchers learn will have implications for the health and well-being of all high-altitude populations.
Alan Leshner, Ph.D.CEO, AAASExecutive Publisher, Science
Research Atop the Roof of the World
So whether by genetic adaptation or through the application of our knowledge, experience, and intellect, humans are continuing to adjust to harsh conditions on the Tibetan plateau and expand our understanding of the effect of extreme environments on our bodies.

Section One: High-Altitude MedicineResearch Atop the Roof of the World
CR
EDIT
: © IS
TOC
KPH
OTO
.CO
M/D
EIM
AGIN
E

High-Altitude Medicine
6
A Unique Challenge in High-Altitude Medicine: The Qinghai-Tibet RailroadWu Tianyi1,*, Ding Shou Quan2, Liu Jin Liang3, Bengt Kayser4
nesses allows the prevention of high-altitude–induced deterioration of a preexisting health condition (3).
AMS Risk AssessmentA more significant question is which individuals are at greater risk of AMS, as an understanding of the risk factors may affect clinical man-agement by providing measures for intervention and prevention. A to-tal of 11,182 workers were surveyed and a risk model was developed using multiple logistic regression. Our findings suggest that multiple risk factors usually affect individuals who are at risk. Combinations of rapid ascent, a higher altitude reached, and greater physical exer-tion increase the likelihood that illness will develop. Newcomers from sea-level areas, obese persons, and younger people are advised to take care when traveling to high altitude (4). Additionally, altitude exposure was a risk factor for upper gastrointestinal tract bleeding, especially in combination with alcohol, aspirin, and dexamethasone intake (5). Risk factors that can be modified should be attended to, and physicians should perform check-ups and tests to identify sub-jects who are at greater risk, to effectively control the risk factors of AMS (4).
AMS and SmokingIt has been suggested that smokers have a lower risk of AMS at high altitudes (6). However, the relationship between cigarette smoking and AMS is not clear. To assess AMS risk and altitude acclimatization in relation to smoking, 200 healthy nonsmokers and 182 cigarette smok-ers were recruited from a population of male Han Chinese lowlanders. These subjects were without prior altitude exposure, were matched for age, health status and occupation, and were transported to an altitude of 4,525 m. AMS scores, smoking habits, arterial saturation, hemoglobin, lung function, and mean pulmonary artery pressure were assessed upon arrival, and after three and six months at high altitude. Interestingly, smokers may initially be at less risk at altitude, but not in the long term (6). This study allowed us to advise smokers on altitude exposure using the epidemiological data and suggested new avenues for research on AMS pathophysiology.
HACE StudiesHACE is a serious type of acute altitude sickness with a high mortality rate. An early diagnosis is therefore critical. We observed 66 lowland railway workers suffering from HACE who had ascended to altitudes of greater than 4,000 m. Ataxia was present in 48 workers (73%) and was observed to have occurred earlier than the most common signs of HACE such as disturbance of consciousness (79%) in the major-ity of patients. There was a high concordance (96%) between ataxia and computed tomography scans or magnetic resonance imaging in the diagnosis of HACE. Ataxia can be measured in mountainous regions by simple coordination tests including a modified Romberg test. These tests can serve as an early diagnostic predictor of HACE, indicating that death due to HACE can be avoided if the early symptoms and signs are recognized (2).
A s a result of industrial development in western China, the Chinese government decided to build the Qinghai-Tibet Railway (QTR) in 2001. This railroad, between Gol-mud (2,808 m) and Lhasa (3,658 m), is 1,142 km long
and over 85% of the rail line is above 4,000 m. The highest pass is 5,072 m, through the Mt. Kun Lun and Tanggula ranges, making the QTR the highest railroad in the world (1, 2). From 2001 to 2005, the new railroad was built by more than 140,000 workers, of whom 80% traveled from their lowland habitat to an altitude of approximately 5,000 m. Construction of the railroad represented a unique challenge in high altitude medicine. Initially, the overall incidence of acute mountain sickness (AMS), high-altitude pulmonary edema (HAPE), and high-altitude cerebral edema (HACE) in workers was approxi-mately 45% to 95%, 0.49%, and 0.26%, respectively (2). The chal-lenge in terms of treatment and prevention of high altitude sickness was significant.
Our research team worked continuously for five years in three of the highest local hospitals along the rail line in the Fenghoushan (altitude: 4,779 m, barometric pressure (PB) ~417 Torr), Kekexili (4,505 m, PB ~440 Torr) and Dangxiang areas (4,292 m, PB ~447 Torr). The study was approved by the Qinghai High Altitude Research Institute Commit-tee on Human Research.
Preexisting ConditionsThe construction of the QTR resulted in several challenging problems in high-altitude medicine (1–8). First, identifying which individuals are not suited for high altitudes is not easy for patients with preexisting dis-orders, thus making it difficult for physicians to give clear advice. We studied the medical conditions of 14,050 high-altitude workers, paying particular attention to preexisting illnesses. All subjects were observed at low and high altitude. Based on our findings, we believe that neither taking a rather permissive stance nor setting rigid rules of contraindica-tion is correct. The former may put some persons at risk whereas the latter may exclude too many subjects from traveling to high altitudes, even when this may be safe. Obviously, conditions that are related to hypoxia at low altitude will be exacerbated at high altitude. Such con-ditions include chronic obstructive pulmonary disease with arterial de-saturation, recent cardiac infarction or heart failure, obesity with sleep apnea, or severe hypertension. Subjects with such conditions should be advised against travel to high altitude. Conversely, patients with mild anemia or allergic asthma do not appear to have increased risk of devel-oping ailments at high altitudes and their conditions may even improve. We have suggested that careful evaluation of preexisting chronic ill-
1National Key Laboratory of High Altitude Medicine, High Altitude Medical Research Institute, Xining, China; 2Qinghai-Tibet Railroad Hospital at Fenghuoshan, Qinghai, China; 3Qinghai-Tibet Railway Hospital at Kekexili, Qinghai, China; 4Institut des Sciences du Movement et de la Macute Medécine du Sport, Faculté de Médecine, Université de Genève, Geneva, Switzerland.*Corresponding author: [email protected]

Section One
7
Intermittent Altitude ExposureThe construction of the QTR also provided a unique opportunity to study the relationship between intermittent altitude exposure and AMS (7). For five years, workers spent seven-month periods at high altitude interspersed with five-month periods at sea level. The incidence, sever-ity, and risk factors of AMS were prospectively investigated. A group of 600 lowlanders who commuted between sea level and 4,500 m for five years was compared with 600 lowland workers recruited each year upon their first ascent to high altitude. AMS was assessed using the Lake Louise Scoring System. We noted that a long-term, 7/5 month commut-ing pattern led to a gradual reduction in the incidence and severity of AMS, and thus reduced susceptibility. This suggested that exposure to high altitude may help minimize the development of high altitude sick-ness during each subsequent exposure (7). These data support clinical guidelines for lowlanders periodically ascending to high altitude for work and may help prevent illness and improve performance.
Occasional Altitude ExposureAfter completion of the railroad in June 2006, about two million pas-sengers each year are rapidly exposed to high-altitude travel on this train. How would people tolerate traveling at high-altitudes by the QTR? An initial study observed that the AMS incidence varied from 16% to 31% in passengers even when an oxygen concentrator was pres-ent in the train. To curb the health risk of rapid travel at high altitudes by train, prospective travelers should be better informed, medical per-sonnel aboard the train should be well trained, and a staggered travel
schedule with one to two days at intermediate altitudes should be sug-gested to non-acclimatized subjects (8).
Future ResearchAfter the completion of the QTR, the Chinese government launched several other important engineering projects in Tibet including the construction of a new railroad from Lhasa to Xigatse (altitude: 3,890 m) (7). These projects put many subjects at risk for altitude sickness, and it remains to be investigated if the incidence of alti-tude sickness can be reduced further using the results obtained from our studies.
REFERENCES1. T.Y.Wu, High Alt. Med. Biol. 5, 1 (2004).2. T. Y. Wu et al., High Alt. Med. Biol. 7, 275 (2006).3. T.Y.Wuet al., High Alt. Med. Biol. 8, 88 (2007).4. T. Y. Wu et al., Chin. Med. J. (Engl.) 125, 1393 (2012).5. T.Y.Wuet al., World J. Gastroenterol. 13, 774 (2007).6. T. Y. Wu et al., Thorax 67, 914 (2012).7. T.Y.Wuet al., High Alt. Med. Biol. 10, 221 (2009).8. T. Y. Wu et al., High Alt. Med. Biol. 11, 189 (2010).
ACKNOWLEDGMENTSThis work was supported by the National Ò 973Ó Program of China (Grant No. 2006 CB708514 and 2012CB518202) and the National Natural Science Foundation of China (Grant No. NNSF-30393130).
Human-performance engineering can be regarded as human-centered system engineering focused on maintaining and im-proving the homeostatic level in humans to improve quality of life and develop natural potential (1). High-altitude health
care is an example of human-performance engineering, the goal of which is to solve human-performance problems in high-altitude envi-ronments.
Our research group carried out human-performance engineering at high altitudes in accordance with the principles of system engineering, which regards human beings as large, open, and complex systems, as first proposed by Qian Xuesen (2, 3). Based on the initial idea of hu-man-performance engineering, the focus of research has shifted from the “disease” (altitude sickness) to the process of altitude acclimatiza-tion in a hypoxic environment. In other words, there has been a shift in focus from a “cure” to the “dynamic regulation” of homeostasis during altitude acclimatization, which can improve the synergy of the physi-cal system with the hypoxic environment to achieve normal function at high altitudes.
Institute of Aviation Medicine BeijingNo. 28, Fucheng Road, Haidian, Beijing, China.Corresponding author: [email protected]
Human-Performance Engineering at High AltitudeYu Mengsun
Studies have shown that sleep is crucial for maintaining optimal meta-bolic performance and homeostasis (4). Aviation medicine has demon-strated that a change in sleep quality is a common feature in response to various psychological, physical, and environmental stressors. Thus, managing stress reactions may improve acclimatizing ability. Altitude-related hypoxic stress can result in sleep disorders, as well as physical and psychological reactions, when the environmental change (increas-ing hypoxia) is too rapid for the body’s self-organizing process, which attempts to compensate and maintain homeostasis. Additionally, it may prolong the time needed to adapt and could result in an inability to fully acclimate. This scenario can be represented as follows:
Environment Variation Rate (EVR) >> Physical Self-organizing and Self-Adapting Rate (PSSR) (1)
As shown by equation 1, altitude stress can be prevented in two ways. First, a lower EVR could be artificially induced. Second, the PSSR could be increased. Thus, the relationship between EVR and PSSR could be changed from 1 to 2, as follows:
EVR>>PSSR (1)EVR≤PSSR (2)
A technical approach is therefore proposed to prevent altitude-related stress; (i) Administering progressive, intermittent hypoxic exposure

High-Altitude Medicine
8
(IHE) training in which the environmental conditions are adjusted to be more in line with the time constant―a term that describes how fast the system can react following a trigger―required for self-organizing adaption by the body; (ii) Evaluating the reaction of the body during training using sleep monitoring techniques in order to maintain the EVR as close to the PSSR as possible. As a result, the efficiency of training will be improved.
In this study, we attempted to clarify the mechanisms at work dur-ing human altitude acclimatization. The changes seen in physiological parameters (e.g., arterial blood oxygen saturation, heart rate, and deep sleep time) due to altitude stress can be approximately fitted to first-or-der function curves (5). Figure 1 shows the arterial blood oxygen satura-tion (SaO2) curves for a team of four men flying to 3,800 m and the cor-responding dynamic model. Here, τ is the time constant or time scale.
In principle, the acclimatizing process during IHE training should approximate a first-order time function. Because of the intermittent na-ture of the training, the model expression includes four other variables, besides τ, related to intermittent training, such as the training intensity each time point, the interval of training, frequency of training, and the rate at which adaptation changes (“fading factor”). Additionally, it in-volves an individual optimal training intensity, S0(H), which is a func-tion of the degree of adaptation achieved (5). The model expression of IHE training is explained in full in reference 3. It has been suggested that the training intensity should be as close as possible to S0(H) for each exercise course, and the efficiency of training will reach a maximum value when EVR equals PSSR. We designed two similar protocols for incremental IHE training. One is IHE training before going to a high altitude area, while the other is IHE training at high altitude after acute hypoxia exposure. The two training patterns are illustrated in Figure 2.
Results showed that the two types of IHE training were equivalent both in principle and in their practical effects (6). In our study, the time constant, τ, of the untrained group during the process of acclimatiza-tion was 3.2 days at 3,800 m above sea level. The τ value of the group
trained at altitude was significantly decreased, to 0.633 days, while for the group trained before hypoxia, it was still less than 0.633 days at 0.434 days. This demonstrated that subjects could completely avoid reactions to altitude and ensure minimal health impact on exposure to hypoxia if a suitable amount of training is done.
To maintain homeostasis in a hypoxic environment, the management of diet and physical exercise is important. Permanent residents at high altitudes risk suffering from oxygen toxicity when moving to lower al-titudes, caused by the rate of environmental change being greater than that of acclimatization to the hyperoxic environment of the plains. In these cases, we recommend introducing intermittent hyperbaric oxygen training to prevent the risk of severe disease resulting from acute oxy-gen exposure.
This research describes the first practice of human performance en-gineering at high altitude. It has shown that maintaining homeostasis in a human system can be achieved when we fully understand the limits and self-organizing ability of human beings, such as acclimatizing to environmental changes and recovering from illness.
REFERENCES 1. Z. L. Tao, Ò Comprehensive ReportÓ (Report on Advances in Biomedical
Engineering (2011-2012), China Science and Technology Press, Beijing, 2012).
2. X. S. Qian, Systemic Engineering (Shanghai Jiao Tong Univ. Press, Shanghai, 2007), pp. 288-299.
3. X. S. Qian, Establish Systematology (Shanghai Jiao Tong Univ. Press, Shanghai, 2007), pp. 125-129.
4. M. S. Yu, H. J. Zhang. China Medical Device Information 3, 4 (2003). 5. M.S.Yu,“Humanperformanceengineeringathighaltitude”(Reporton
Advances in Biomedical Engineering (2011Ð 2012), China Science and Technology Press, Beijing, 2012).
6. J. Yang, M. S. Yu, Z. T. Cao. Chinese Journal of Aerospace Medicine. doi:10.3760/cma.j.issn.1007-62392012.03.004.
FigureÊ 1. Ê SystemÊ modelÊofÊ altitudeÊ acclimatization.ÊSSE,Ê errorÊ sumÊ ofÊ squares;ÊHR,Ê heartÊ rate.Ê G1,Ê G2,Ê G3Ê areÊtransferÊ functions:Ê G1,Ê instantÊresponseÊ toÊ hypoxicÊ environ-ment;Ê G2,Ê feedbackÊ param-eterÊ relatedÊ toÊ theÊ abilityÊ forÊregainingÊ homeostasis;Ê G3,ÊcharactersticÊ parameterÊ re-latedÊ toÊ theÊ personalÊ accli-matizationÊ process.
FigureÊ 2.Ê TwoÊ patternsÊ ofÊ IHEÊ training.
Section One
9
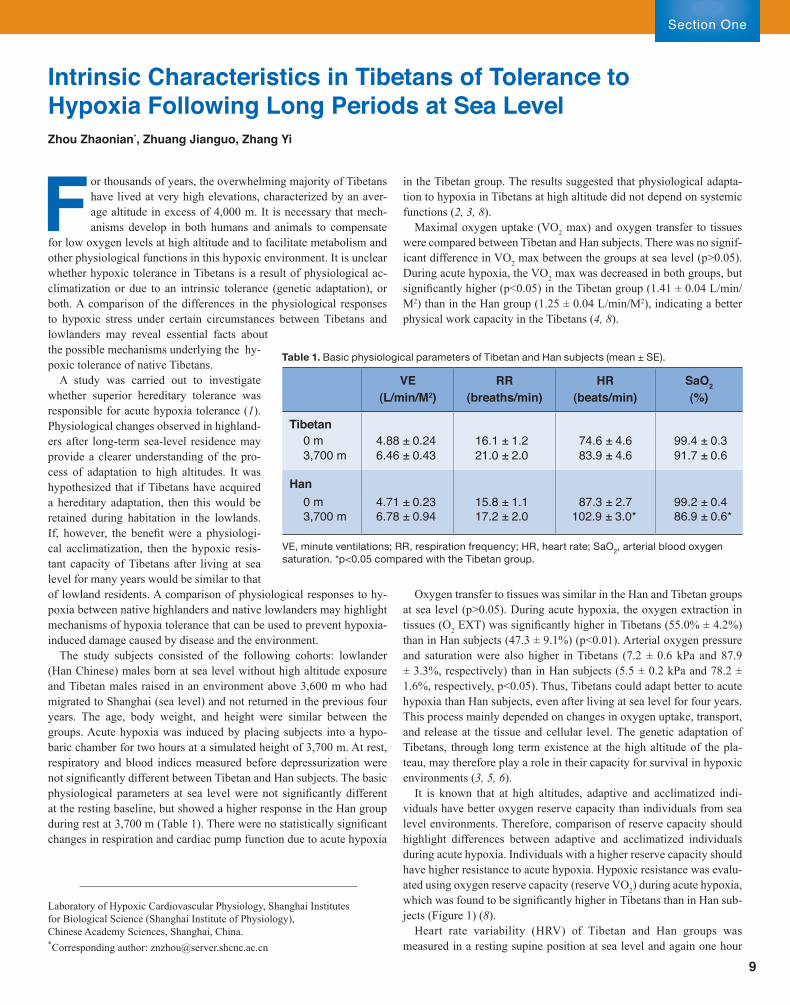
F or thousands of years, the overwhelming majority of Tibetans have lived at very high elevations, characterized by an aver-age altitude in excess of 4,000 m. It is necessary that mech-anisms develop in both humans and animals to compensate
for low oxygen levels at high altitude and to facilitate metabolism and other physiological functions in this hypoxic environment. It is unclear whether hypoxic tolerance in Tibetans is a result of physiological ac-climatization or due to an intrinsic tolerance (genetic adaptation), or both. A comparison of the differences in the physiological responses to hypoxic stress under certain circumstances between Tibetans and lowlanders may reveal essential facts about the possible mechanisms underlying the hy-poxic tolerance of native Tibetans.
A study was carried out to investigate whether superior hereditary tolerance was responsible for acute hypoxia tolerance (1). Physiological changes observed in highland-ers after long-term sea-level residence may provide a clearer understanding of the pro-cess of adaptation to high altitudes. It was hypothesized that if Tibetans have acquired a hereditary adaptation, then this would be retained during habitation in the lowlands. If, however, the benefit were a physiologi-cal acclimatization, then the hypoxic resis-tant capacity of Tibetans after living at sea level for many years would be similar to that of lowland residents. A comparison of physiological responses to hy-poxia between native highlanders and native lowlanders may highlight mechanisms of hypoxia tolerance that can be used to prevent hypoxia-induced damage caused by disease and the environment.
The study subjects consisted of the following cohorts: lowlander (Han Chinese) males born at sea level without high altitude exposure and Tibetan males raised in an environment above 3,600 m who had migrated to Shanghai (sea level) and not returned in the previous four years. The age, body weight, and height were similar between the groups. Acute hypoxia was induced by placing subjects into a hypo-baric chamber for two hours at a simulated height of 3,700 m. At rest, respiratory and blood indices measured before depressurization were not significantly different between Tibetan and Han subjects. The basic physiological parameters at sea level were not significantly different at the resting baseline, but showed a higher response in the Han group during rest at 3,700 m (Table 1). There were no statistically significant changes in respiration and cardiac pump function due to acute hypoxia
in the Tibetan group. The results suggested that physiological adapta-tion to hypoxia in Tibetans at high altitude did not depend on systemic functions (2, 3, 8).
Maximal oxygen uptake (VO2 max) and oxygen transfer to tissues were compared between Tibetan and Han subjects. There was no signif-icant difference in VO2 max between the groups at sea level (p>0.05). During acute hypoxia, the VO2 max was decreased in both groups, but significantly higher (p<0.05) in the Tibetan group (1.41 ± 0.04 L/min/M2) than in the Han group (1.25 ± 0.04 L/min/M2), indicating a better physical work capacity in the Tibetans (4, 8).
Oxygen transfer to tissues was similar in the Han and Tibetan groups at sea level (p>0.05). During acute hypoxia, the oxygen extraction in tissues (O2 EXT) was significantly higher in Tibetans (55.0% ± 4.2%) than in Han subjects (47.3 ± 9.1%) (p<0.01). Arterial oxygen pressure and saturation were also higher in Tibetans (7.2 ± 0.6 kPa and 87.9 ± 3.3%, respectively) than in Han subjects (5.5 ± 0.2 kPa and 78.2 ± 1.6%, respectively, p<0.05). Thus, Tibetans could adapt better to acute hypoxia than Han subjects, even after living at sea level for four years. This process mainly depended on changes in oxygen uptake, transport, and release at the tissue and cellular level. The genetic adaptation of Tibetans, through long term existence at the high altitude of the pla-teau, may therefore play a role in their capacity for survival in hypoxic environments (3, 5, 6).
It is known that at high altitudes, adaptive and acclimatized indi-viduals have better oxygen reserve capacity than individuals from sea level environments. Therefore, comparison of reserve capacity should highlight differences between adaptive and acclimatized individuals during acute hypoxia. Individuals with a higher reserve capacity should have higher resistance to acute hypoxia. Hypoxic resistance was evalu-ated using oxygen reserve capacity (reserve VO2) during acute hypoxia, which was found to be significantly higher in Tibetans than in Han sub-jects (Figure 1) (8).
Heart rate variability (HRV) of Tibetan and Han groups was measured in a resting supine position at sea level and again one hour
VE RR HR SaO2
(L/min/M2) (breaths/min) (beats/min) (%)
Tibetan0 m 4.88 ± 0.24 16.1 ± 1.2 74.6 ± 4.6 99.4 ± 0.33,700 m 6.46 ± 0.43 21.0 ± 2.0 83.9 ± 4.6 91.7 ± 0.6
Han0 m 4.71 ± 0.23 15.8 ± 1.1 87.3 ± 2.7 99.2 ± 0.43,700 m 6.78 ± 0.94 17.2 ± 2.0 102.9 ± 3.0* 86.9 ± 0.6*
VE,Ê minuteÊ ventilations;Ê RR,Ê respirationÊ frequency;Ê HR,Ê heartÊ rate;Ê SaO2,Ê arterialÊ bloodÊ oxygenÊsaturation.Ê *p<0.05Ê comparedÊ withÊ theÊ TibetanÊ group.
TableÊ 1.Ê BasicÊ physiologicalÊ parametersÊ ofÊ TibetanÊ andÊ HanÊ subjectsÊ (meanÊ ±Ê SE).
Intrinsic Characteristics in Tibetans of Tolerance to Hypoxia Following Long Periods at Sea Level Zhou Zhaonian*, Zhuang Jianguo, Zhang Yi
Laboratory of Hypoxic Cardiovascular Physiology, Shanghai Institutes for Biological Science (Shanghai Institute of Physiology), Chinese Academy Sciences, Shanghai, China.*Corresponding author: [email protected]

High-Altitude Medicine
10
after simulated ascent to 3,700 m in a hypobaric chamber. HRV may better clarify levels of sympathetic and parasympathetic activity. The results indicated that Tibetans exhibited greater parasympathetic tone at rest at sea level, and ascent to an altitude of 3,700 m did not significantly alter their heart beat. However, Han subjects at 3,700 m had a significantly reduced vagal tonic activity of the heart. Therefore, it is likely that Tibetans’ greater adaptation to hypoxia and their specific
Modern humans migrated from the African continent approx-imately 200,000 years ago and, during migration, humans adapted to different extreme environments, including those of high altitude (1). The Qinghai-Tibet Plateau is the largest
and highest plateau in the world and although there are controversial theories about the origins of settlers on this plateau based on archeolog-ical findings (2), Tibetans may have resided in this harsh environment for up to 3,000 years despite the physiological challenges associated with chronic hypoxia and increased ultraviolet light exposure (3).
Physiological Evidence for Tibetan AdaptationPopulations at high altitudes have evolved physiological adaptations to counter the environmental hypobaric hypoxia at high altitudes. How-ever, studies of hypoxia-related physiological traits in different high altitude populations indicate independent patterns of adaptive pheno-types amongst them. For example, Tibetan women are relatively pro-tected from hypoxia-influenced maternal physiological responses that can cause low child survival rates and low birth weight (4). Studies have demonstrated that placental growth and development are remark-ably well protected among certain high altitude female populations (5).
In 1890, Francois-Gilbert Viault identified polycythemia in his blood at 4,500 m in Peru, and in 1924, T. Howard Somervell observed that the hemoglobin concentration in Tibetans was significantly lower than in the expedition team during a climb of Mt. Everest (6). It has since been shown that chronic exposure to hypoxia in lowland populations leads
FigureÊ 1.Ê OxygenÊ reserveÊ capacityÊ duringÊ acuteÊ hypoxia.Ê ThereÊ wereÊno significant differences in the reserve of oxygen consumption (reserve VO2) among the groups at sea level (0 m), but it was significantly higher in TibetansÊ thanÊ inÊ HanÊ subjectsÊ duringÊ acuteÊ hypoxiaÊ (3,700Ê m).Ê T,Ê TibetanÊgroup;Ê H,Ê HanÊ group.Ê ResultsÊ representÊ meanÊ ±Ê SE.Ê *p<0.05Ê comparedÊtoÊt heÊ TibetanÊ group.
Research Center for High Altitude Medicine, Qinghai University, Xining, Qinghai China. *Corresponding author: [email protected]
Exploration and Evidence of High-Altitude Adaptation in Tibetan HighlandersWuren Tana and Ge Ri-Li*
characteristics of autonomic control are inherited traits (7).In conclusion, our studies demonstrated that superior tolerance
to acute hypoxia and better physical performance were still present in Tibetans after living at sea level for four years, implying that the intrinsic characteristics of hypoxic adaptation exist in native high altitude-dwelling Tibetans.
REFERENCES 1. X. H. Ning, Z. N. Zhou, X. Z. Lu, X. C. Hu, In Proceedings of
Symposium On Qinghai-Xizang (Tibet) Plateau (Beijing, China). Geological and Ecological Studies of Qinghai-Xizang plateau. (Gordon andBranchScience,Press,NewYork,1981),p.1407.
2. Z. N. Zhou et al., Chin. Sci. Bull. 37, 1657 (1982).3. Z.N.Zhou,F.Yuan,L.Gu,Y.Xiao,Chin. J. Appl. Physiol. 9, 193
(1993).4. Z.N.Zhou,Y.Xiao,H.Y.Jiang,L.Q.He,Space Med. Medic. Eng. 8,
202 (1995).5. Z.N.Zhou,X.F.Wu,H.Y.Jiang,L.Q.He,Hypoxia Med. J. 3, 13
(1996). 6. Z. N. Zhou, J. G. Zheng, X. F. Wu, L. Q. He, In Progress in Mountain
Medicine and High Altitude Physiology (Dogura & Co. Ltd. Kyoto. Press, 1998), p. 52.
7. J. G. Zhuang, H. F. Zhu, Z. N. Zhou, Jpn. J. Physiol. 52, 51 (2002).8. Z.N.Zhou,J.G.Zhuang,X.F.Wu,Y.Zhang,P.Cherdrungsi,J.
Physiol. Sci. 58, 167 (2008).
ACKNOWLEDGMENTS This work was funded by a grant from the National Basic Research Program of China, (Grant No. 2006CB504100 and 2012CB518200) and the National Natural Science Foundation of China (Grant No.3927089 and 30393130).

Section One
11
to an elevation of hematocrit due to increased numbers of erythrocytes (polycythemia) whereas the majority of Tibetan highlanders maintain comparable hematocrit levels to populations living at sea level (7). While increased hemoglobin concentration may be considered a beneficial adaptation to hypoxia, at certain threshold levels the increased number of erythrocytes results in higher blood viscosity, which could impair capillary blood flow and oxygen delivery (8). Therefore, the genetic basis of low hemoglobin levels in Tibetans warrants further investigation.
Human energy demands and metabolic adaptation have been studied extensively with respect to diet, but metabolic adaptation in response to unique environments has only recently been closely examined. Previous studies of native high altitude populations suggested that decreased fatty acid oxidation could be a favorable adaptation to hypoxia (9), while a study from our group demonstrated that Tibetans have comparatively higher free fatty acid concentrations compared to individuals living at sea level. This suggests that anaerobic glucose metabolism is increased and fatty acid oxidation may be decreased in Tibetans (10). To better understand the physiological significance of these patterns, largersample sizes, better controls, and broader studies at different altitudes are needed. Meanwhile the genetic basis and metabolic implications of high altitude adaptation requires further investigatation.
Genetic Evidence for Tibetan Adaptation to High AltitudeTo detect natural selection for particular genetic variants in high alti-tude populations during the evolution of high altitude adaptation, sev-eral population genetics methods have been employed.
In a previous study, we used two statistical tests, the High Integrated Haplotype Score (iHS) and Cross Population Extended Haplotype Homozygosity (XP-EHH) to determine whether Tibetans evolved adaptively under positive selection. We found that among 240 genes related to the hypoxia pathway in gene ontology categories, 10 genes were involved in high altitude adaptation in Tibetans, and were present in regions of strong positive selection (11). The 10 candidate genes included endothelial PAS domain-containing protein 1 (EPAS1), prolyl hydroxylase domain-containing protein/Egl nine homolog 1 (PHD2/EGLN1), and peroxisome proliferator-activated receptor alpha (PPARA). These may be important because individuals carrying additional copies of a putatively advantageous haplotype of PHD2 [build 36 (Hg18), chromosome 1 positions 229793717, 229667980, and 229665156] and PPARA (Hg18, chromosome 22 positions 44827140, 44832376, and 44842095) have significantly lower hemoglobin concentration, suggesting that these haplotypes are associated with protection against polycythemia in Tibetan highlanders (11).
A study of Andean and Tibetan populations also revealed that both populations had experienced positive selection for hypoxia-inducible factor (HIF) pathway genes, including PHD2/EGLN1 (11, 12). In nor-moxia conditions, PHD enzymes are involved in HIF-1α and HIF-2α ubiquitinization and their rapid destruction in proteasomes (13). Thus, PHD and Von Hippel–Lindau tumor suppressor proteins (VHL) are ma-jor negative regulators of HIFs (13). We identified a novel missense mutation in the PHD2 gene, which together with another previously reported but unvalidated PHD2 single nucleotide polymorphism (SNP) that results in missense mutation, correlated with lower hemoglobin levels in Tibetan highlanders (unpublished data).
Other studies have shown that Tibetans experienced positive selec-
tion for variants of EPAS1, which regulates expression of the erythro-poietin gene. Based on phenotype/genotype association analysis, high-ly differentiated SNPs in the EPAS1 region were related to decreased hemoglobin levels in two independent studies of high-altitude adapta-tion in Tibetans (14, 15).
A more recent study that analyzed another groups of Tibetans from the Tuo Tuo River area suggested that EPAS1 and PPARA putative adaptive haplotypes were associated with elevated serum lactate and free fatty acid levels, which suggests that adaptation to decreased oxygen availability may be enhanced by a shift in fuel preference to glucose oxidation and glycolysis, at the expense of fatty acid catabolism (10).
Considering the lack of genetic differences detected by analysis of the protein-coding regions of Han Chinese and Tibetans (14), it is pos-sible that many genetic targets of selection are in noncoding, regulatory regions of the genome. Our analyses of individuals living in Maduo County (elevation ~4,300 m), the highest county in China, have identi-fied an miRNA near the PPARA gene and a noncoding, highly con-served region in a Tibetan population that may be involved in high-altitude adaptation (unpublished data).
Perspective Studies from our group and others regarding indigenous Tibetans have identified genes that may be involved in adaptation to hypoxia. It is clear that during this adaptation process, Tibetans developed unique genetic changes compared with neighboring lowland popu-lations. Genetic and statistical analysis from these studies have pro-vided interesting data, but to understand this complex process it will be necessary to integrate these results with functional analyses to ob-tain a more complete picture of the mechanisms involved in hypoxia adaptation. Ultimately, we hope that genetic and functional analy-ses may be used in the prevention and treatment of hypoxia-related diseases.
REFERENCES 1. A. Lawler. Science 331, 387 (2011). 2. M. Aldenderfer, High Alt. Med. Biol. 12, 141 (2011). 3. M. Aldenderfer, World Archaeol. 38, 357 (2006b). 4. L. Postigo et al., J. Physiol. 587, 15 (2009). 5. L. G. Moore et al., Resp. Physiol. Neurobiol. 178, 181 (2011). 6. M. C. T. van Patot, M. Gassmann, High Alt. Med. Biol. 12, 157 (2011). 7. C. M. Beall, Resp. Physiol. Neurobiol. 158, 161 (2007). 8. J. T. Prchal, in Williams Hematology. K. Kaushansky, M.A. Lichtman, T.
J. Kipps, E. Beutler, U. Seligsohn, J. T. Prchal, Eds. (McGraw Hill, New York, ed. 8, 2010), pp. 435-449.
9. J. E. Holden et al., J. Appl. Physiol. 79, 222 (1995).10. R.-L. Ge et al., Mol. Genet. Metabol. 106, 244 (2012). 11. T. Simonson et al., Science 329, 72 (2010).12. A. Bigham et al., PLoS Genetics 6, 1 (2010). 13. G. L. Semenza, Physiology 24, 97 (2009). 14. X. Yi, Y. Liang et al., Science 329, 75 (2010).15. C. M. Beall et al., Proc. Natl. Acad. Sci. U.S.A. 107, 11459 (2010).
ACKNOWLEDGMENTSThis project was supported by the National Basic Research Ò 973Ó Program of China (Grant No. 2012CB518200), the Program of International S&T Cooperation of China (Grant No. 0S2012GR0195), and the National Natural Science Foundation of China (Grant No. 30393133).

High-Altitude Medicine
12
T he Tibetan Plateau, with a mean elevation of more than 4,000 m, is characterized by extremely harsh environmental conditions such as cold temperatures during winter, strong ultraviolet radiation, and low oxygen concentrations. For
people living in these inhospitable terrains, high-altitude hypoxia is a condition that cannot be overcome by traditional treatments. Currently, there are nearly five million indigenous Tibetans living on the plateau, and two thirds of them live at an altitude exceeding 3,500 m (1). Modern Tibetans have physiologically adapted to the high-altitude hypoxic environment (2). For example, compared with lowlanders, Tibetans have greater hypoxic and hypercapnic ventilatory responsiveness, larger lungs, better lung function, greater lung diffusion capacity, minimal hypoxic pulmonary hypertension, and higher levels of exhaled nitric oxide (2). This environmental adaptation in Tibetans may result from long-term natural selection that has been taking place since the ancestors of modern Tibetans permanently settled on the plateau. To elucidate the molecular mechanism underlying this genetic adaptation to hypoxia, it is necessary to answer two key questions: (i) when did the ancestors of modern Tibetans first permanently settle on the Tibetan Plateau and (ii) how did genetic modifications in Tibetans improve their physiological functions and endow them with the ability to thrive in hypoxic conditions?
Regarding the question of when the Tibetan Plateau was populated, no human fossils have been found on the plateau, and consequently no direct biological evidence is available to infer that humans previously inhabited the region. However, archaeological findings based on limited cultural artifacts suggest that the earliest human occupation likely occurred at relatively low altitude areas (<3,000 m) around 40–30 thousand years ago (kya) during the early Upper Paleolithic period, while the permanent occupation at high altitude (>3,000 m) did not begin until the advent of farming and pastoral economy about 8.2–6kya (3). The ice sheet hypothesis describing human occupation of the Tibetan Plateau during the Last Glacial Maximum (LGM, 22–18 kya) may support this notion (4, 5). It is generally believed that even though modern humans might have successfully settled on the plateau during the Upper Paleolithic period, the early settlers would not have survived the LGM, and thus present-day Tibetans are likely descendants of post-glacial immigrants.
Recent genetic studies of present-day Tibetan populations haveprovided a different picture of the prehistoric peopling of the plateau. Interestingly, by examining the genetic composition of the paternal (Y chromosome) and maternal (mitochondrial DNA) lineages of Tibetans,
both ancient and recent genetic components were identified (6, 7). This suggests that modern Tibetan populations may have been formed genetically from two distinct ancestral populations that ventured into the plateau region during both the Paleolithic and the Neolithic periods(6, 7). We recently screened more than 6,000 Tibetan individuals from 41 geographic populations across the Tibetan Plateau. We found that the majority of lineages in Tibetans (87.80% of Y-chromosomal and 90.99% of mitochondrial) were of East Asian lineages dating back to 51–18 kya, a coalescence age falling into the Upper Paleolithic period(Figure 1). We also identified a molecular signature indicating a recent population expansion within Tibetans around 10–7 kya during the early Neolithic period, likely caused by a second migratory wave of modern humans onto the plateau (Figure 1). Both the Paleolithic migration and Neolithic expansion had a significant impact on the genetic makeup of present-day Tibetan populations. The ancient peopling of the Tibetan Plateau suggests that the ancestors of modern Tibetans had undergone a lengthy natural selection process against hypoxic stress and may explain why Tibetans have the most effective genetic adaptation to high-altitude hypoxia in the world (2). Hence, Tibetans are an ideal population for delineating the molecular mechanism of genetic adaptation to high-altitude hypoxia.
Regarding the question of how Tibetans improved their physiological functions, we and other research groups have recently conducted ge-nome-wide analyses aimed at identifying genes involved in the genetic adaptation to hypoxia (8–10). These genome-wide studies revealed a set of candidate genes that likely play important roles in physiologi-cal adaptation to hypoxia in Tibetans (Table 1). Of these, EPAS1 (also called hypoxia-inducible factor 2α, HIF2α) and its negative regulator, PHD2/EGLN1, appear to play major roles (8–10). However, functional studies (both in vitro and in vivo) have yet to be conducted to delineate the molecular pathways and physiological mechanisms at work.
REFERENCES 1. T. Wu, High Alt. Med. Biol. 2, 489 (2001). 2. T. Wu, B. Kayser, High Alt. Med. Biol. 7, 193 (2006). 3. M. Aldenderfer, High Alt. Med. Biol. 12, 141 (2011). 4. M. Kuhle, Universitas 27, 281 (1985).5. Y.-F. Shi, B.-X. Zheng, S.-J. Li, Chinese Geographical Science 2, 293
(1992). 6. H. Shi et al., BMC Biol. 6, 45 (2008). 7. B. Su et al., Hum. Genet. 107, 582 (2000).8. Y. Peng et al., Mol. Biol. Evol. 28, 1075 (2011).
9. C. M. Beall, High Alt. Med. Biol. 12, 101 (2011).10. T. S. Simonson, D. A. McClain, L. B. Jorde, J. T. Prchal, Hum.
Genet. 131, 527 (2012).
ACKNOWLEDGMENTSThis work was supported by the National Basic Research Ò 973Ó Program of China (Grant No. 2012CB518202 and 2011CB512107) and the National Natural Science Foundation of China (Grant No. 91231203, 30870295, and 91131001).
1State Key Laboratory of Genetic Resources and Evolution, Kunming Institute of Zoology, Chinese Academy of Sciences, Kunming, China; 2High Altitude Medical Research Center, School of Medicine, Tibetan University, Lhasa, China; 3National Key Laboratory of High Altitude Medicine, High Altitude Medical Research Institute, Xining, China.*Corresponding author: [email protected]
Peopling of the Tibetan Plateau and Genetic Adaptation to High-Altitude Hypoxia in TibetansQi Xuebin1, Shi Hong1, Cui Chaoying2, Bianba2, Ouzhuluobu2, Wu Tianyi3, Su Bing1,*

Section One
13
TableÊ 1.Ê CandidateÊ genesÊ thoughtÊ toÊ beÊ involvedÊ inÊ high-altitudeÊ hypoxiaÊ adaptationÊ inÊ Tibetans.
Candidate genes Gene Functions Predicted in UniProtKB/Swiss-Prot Database
EPAS1 EndothelialPASdomainprotein1,alsoknownashypoxia-induciblefactor2-alpha(HIF2α)
EGLN1 Egl nine homolog 1, also known as prolyl hydroxylase domain-containing protein 2 (PHD2) or hypoxia-inducible factor prolyl hydroxylase 2 (HIF-PH2)
EP300 E1A binding protein p300
ARNT Arylhydrocarbonreceptornucleartranslocator,alsoknownashypoxia-induciblefactor1-beta(HIF1β)
HBB Hemoglobin subunit beta
HBG2 Hemoglobin subunit gamma-2
EPO Erythropoietin, involved in erythrocyte differentiation and erythrocyte circulation.
EDN1 Endothelin 1, endothelium-derived vasoconstrictor peptides EDNRA Endothelin receptor type AHMOX2 Heme oxygenase 2
ANGPTL4 Protein with hypoxia-induced expression in endothelial cells
ANGPT1 Angiopoietin 1, involved in angiogenesis, endothelial cell survival, proliferation, migration, adhesion, and cell spreading
PPARA Peroxisome proliferator-activated receptor alphaTGFBR3 Transforming growth factor beta receptor III
RYR1 Ryanodine receptor 1 (skeletal)
ECE1 Endothelin converting enzyme 1
FigureÊ 1.Ê TheÊ migratoryÊ routeÊ ofÊ theÊ twoÊ proposedÊ prehistoricÊ migrationsÊ ofÊ modernÊ humansÊ ontoÊ theÊ TibetanÊ Plateau.Ê TheÊ shadedÊ areaÊ representsÊtheÊ entireÊ regionÊ ofÊ theÊ TibetanÊ Plateau,Ê andÊ theÊ smallÊ redÊ areaÊ indicatesÊ theÊ earliestÊ NeolithicÊ siteÊ inÊ ChinaÊ datedÊ toÊ 8,500Ê yearsÊ ago.Ê

High-Altitude Medicine
14
T he study of practical measures to facilitate acclimatization to high altitudes is of major importance, as poor acclimatization can lead to severe deficits in physical and cognitive perfor-mance, and to high-altitude diseases (1). A gradual ascent to
high altitude can reduce the incidence and severity of acute mountain sickness (AMS) and improve working performance, and thus has been widely accepted as a preventative measure (2). However, this measure takes time and is unsuitable for rapid ascents. We studied ways in which to facilitate high altitude acclimatization, particularly in large groups. These approaches were implemented either before ascent, within a short time after arrival, or after a certain duration at high altitude.
Hypoxia preconditioning can protect organisms against subsequent severe hypoxia-induced injury (3). Hypobaric hypoxia-induced (12,000 m, four hours) brain injury in mice was significantly ameliorated by hypoxia pretreatment (7,000 m, 2.5 hours/day for three days) (4). We recruited young males to validate the effects of hypoxia precondition-ing on the human body. We found that hypoxic gas (15% O2) inhala-tion combined with an up-and-down stepping exercise (10 minutes, six times/day for three days) could decrease AMS incidence and improve physical performance at a simulated altitude of 4,300 m. Based on these findings, we applied this procedure in the field at high altitude. We first designed a portable hypoxic respirator according to the principle of a rebreathing circuit (Chinese Patent ZL 02 222805.5), in which carbon dioxide is absorbed by soda lime. Forty young men wore the hypoxic respirators and walked rapidly (10 minutes walking followed by five minutes resting, four times in the morning and repeated in the afternoon) for five days at sea level. Oxygen saturation was reduced from 97.3 ± 1.2% to 88 ± 5.4% and the heart rate increased from 70 ± 9 beats/minute to 126 ± 16 beats/minute during walking. One day or five days after ces-sation of training, the training groups (20 subjects per group) and the control group (without training; 20 subjects) then traveled to an altitude of 4,300 m by bus. We observed that AMS incidence and severity were significantly reduced in the hypoxia preconditioned groups compared with the control group. Physical working performance, determined by maximal oxygen uptake (VO2 max) and physical working capacity at a heart rate of 170 beats/minute (PWC170), was decreased significantly in the control group, but not in the hypoxia preconditioned groups. This suggested that five-day hypoxia preconditioning can reduce the risk of AMS and improve physical working performance at 4,300 m, and that the positive effects endure for at least five days after cessation of train-ing (5). This simple method is suitable for large groups and can be ad-
ministered over a short time before ascending to high altitude.Reactive oxygen species (ROS) may be involved in stimulating the
protective pathways of hypoxia preconditioning. Since hyperoxia pre-treatment can generate ROS, it may also induce similar protective out-comes. To test our hypothesis, PC12 cells were treated with 35% O2 for three hours, followed by a 12-hour recovery period. We observed that cell death induced by a subsequent 72-hour hypoxic exposure (1% O2) was significantly reduced. Hyperoxia pretreatment increased the intra-cellular ROS level, ROS inhibitors diminished, and ROS supplements can mimic the protective effects of hyperoxia pretreatment, indicating that ROS contributes to the protective effects (6). In a separate experi-ment, young human males were subjected to hyperbaric oxygen (2.5 absolute atmospheres) two hours daily for three days before ascent to an altitude of 5,000 m. This pretreatment lowered AMS incidence and improved physical working performance, indicating hyperbaric oxygen preconditioning is an effective measure for high altitude acclimatiza-tion (7).
Previous research has suggested that acetazolamide can be used as an AMS prophylactic medication, but it has some side effects. We tested methazolamide, an analogue of acetazolamide, and found that it pro-longed the swimming time of mice in a hypobaric chamber (simulat-ing an altitude of 5,000 m) and prolonged the survival time in sealed 150 mL containers containing 5 g soda lime, which gradually induces hypoxia (8). In a field experiment, young human males were orally ad-ministrated 25 mg of methazolamide for seven consecutive days, twice daily (starting two days prior to ascent). After arrival of an altitude of 4,300 m, they had higher resting oxygen saturation and lower incidence of AMS compared with the placebo group (unpublished data). These re-sults indicated that methazolamide could be used during the early phase of acclimatization to high altitude.
Reduced exercise is favorable for oxygen supply/consumption bal-ance in a hypoxic environment. We observed skeletal muscle atrophy in rats living in a hypobaric chamber (simulating 5,000 m) for five weeks, while those that undertook swimming training (one hour/day) under a hypoxic environment showed no skeletal muscle atrophy. However, these rats showed increased capillary density in the myocardium and gastrocnemius muscle, increased metabolic enzyme activity and per-centage of α-myosin heavy chain in the myocardium, and enhanced cardiac function (9). Taken together, this indicates that appropriate exercise could be beneficial for maintaining physical performance at high altitude, but exact exercise prescriptions for optimal performance requires further study.
Octacosanol is a nutritional supplement that has been reported to be effective in improving athletic performance, suggesting it may be useful at high altitudes. Chronic hypoxic rats treated with Octacosanol (5 mg/kg daily for four weeks) showed a significant improvement in exercise capacity and lower pulmonary arterial pressure at a simulated altitude of 5,000 m (unpublished data). In a subsequent field test, human volun-teers who had lived at an altitude of 3,700 m for one to two years were administered 10 mg Octacosanol or placebo daily for 30 days. Blood
1College of High Altitude Military Medicine, Third Military Medical University, Chongqing, China; 2Key Laboratory of High Altitude Medicine, Ministry of Education, Third Military Medical University, Chongqing, China; 3Institute of High Altitude Medicine, 18th Hospital of Chinese People’s Libera-tion Army, Yecheng, Xinjiang, China.*Corresponding author: [email protected]†Contributed equally to this work.
New Approaches for Facilitating High-Altitude AcclimatizationHuang Qingyuan1,2, , Zhang Gang1,2, , Cui Jianhua3, Gao Wenxiang1,2, Fan Youming1,2, Huang Jian1,2, Cai Mingchun1,2, Li Peng1,2, Liu Fuyu1,2, Zhou Simin1,2, Gao Yixing1,2, Li Xiaoli1,2, Gao Yuqi1,2,*

Section One
15
hemoglobin concentration and resting or exercising heart rates were significantly decreased, and exercising oxygen saturation significantly elevated, in those taking Octacosanol relative to the control group (10). Traditional Chinese herbals, such as Panax notoginseng, Astragalus membranaceus, and Phyllanthus emblica may also facilitate altitude acclimatization, as suggested by animal and field experiments (11), in-dicating that Octacosanol and Chinese herbs could benefit people living at high altitude over a prolonged period.
In conclusion, to facilitate acclimatization to high altitude, hypoxia/hyperbaric oxygen preconditioning should be considered before as-cending to high altitudes. In addition, methazolamide, Octacosanol, and other traditional Chinese herbals could be taken in the early phase of acclimatization. For people living at a high altitude for extended peri-ods of time, appropriate exercise should be encouraged.
REFERENCES 1. P. Li, G. Zhang, H. You, R. Zheng, Y. Gao, Physiol. Behav. 106, 439
(2012). 2. S. R. Muza, B. A. Beidleman, C. S. Fulco, High Alt. Med. Biol. 11, 87
(2010). 3. E. Rybnikova et al., J. Neurochem. 106, 1450 (2008).4. Y. Fan, Y. Gao, F. Liu, J. Huang, W. Liao, Chin. J. Pathophysiol. 22, 93
(2006).5. Q. Y. Huang et al., Chin. J. Appl. Physiol. 27, 304 (2011).
6. Z. Cao et al., Free Radical Res. 43, 58 (2009). 7. J. H. Cui et al., Chin. J. Appl. Physiol. 24, 444 (2008). 8. G.Zhang,S.M.Zhou,J.H.Tian,Q.Y.Huang,Y.Q.Gao,Trop. J.
Pharm. Res. 11, 209 (2012). 9. M. C. Cai et al., Eur. J. Appl. Physiol. 108, 105 (2010).10. F. Y. Liu et al., Chin. J. High Alt. Med. 36, 19 (2009).11. S. Zhou et al., Phcog. Mag. 8, 197 (2012).
ACKNOWLEDGMENTSThis work was supported by grants from the National Basic Research Ò 973Ó Program in China (Grant No. 2012CB518201), the Key Project of the National Research Program of China (Grant No. 2009BAI85B06), and National Natural Science Foundation of China (Grant No. 31071036, 30771043, and 39730190).
High-altitude pulmonary edema (HAPE) is a rare and poten-tially fatal noncardiogenic pulmonary edema (1). The exact mechanism underlying the development of HAPE remains unclear. Although hypoxia is the main trigger, some individ-
uals are more susceptible to HAPE than others when exposed to identi-cal hypoxia conditions, suggesting a possible genetic predisposition (2, 3). Currently, it is not clear which genes are involved in the pathogen-esis of HAPE. We therefore sought to identify susceptibility genes and determine the synergistic effect of these genes (if any) on HAPE in a large cohort of subjects.
Research Design and SubjectsThe Chinese Government began work on the Qinghai-Tibet railway in 2001. The railroad stretches for 1,142 km with more than 960 km of the track above 4,000 m. Over a period of five years, more than 140,000 people worked in high-altitude conditions, which included a cold and unpredictable climate, dry weather, and low barometric pressure
resulting in a low ambient partial pressure of oxygen. This provided us with an opportunity to collect data relating to the epidemiological aspects of HAPE, samples from HAPE patients and controls, as well as gain insight into genetic etiologic mechanisms.
To study the underlying mechanisms of HAPE in the absence of con-founding factors, we planned a prospective cohort study. The entire co-hort of approximately 140,000 individuals involved in the construction of the railway were examined using a screening procedure that involved two physical examinations. Subjects with cardiovascular, pulmonary disease, asthma, diabetes, hepatitis, and/or other infectious diseases were excluded.
We performed a candidate gene association study to identify HAPE susceptibility genes. In this study, 23 genes were investigated for a po-tential role in HAPE. Of these 23, six genes and/or their haplotypes presented some association with HAPE susceptibility.
Genes in The Renin-Angiotensin-Aldosterone PathwayThe renin-angiotensin-aldosterone system (RAAS) plays a key role in maintaining fluid balance and regulating blood pressure. Therefore, we hypothesized that the pathogenesis of HAPE may be partially attribut-able to proteins in the RAAS cascade. To address this, we genotyped 12 gene polymorphisms evenly interspersed in six RAAS candidate genes. Single locus analysis showed that polymorphisms C-344T and K173R in the cytochrome P450 family protein CYP11B2, and the A-240T polymorphism in the angiotensin I converting enzyme (ACE) protein
1Institute of Polygenic Diseases, Qiqihar Medical University, Qiqihar, China; 2Institute of Basic Medical Sciences, Academy of Military Medical Sciences, Beijing, China; 3National Laboratory of Medical Molecular Biology, Institute of Basic Medical Sciences, Chinese Academy of Medical Sciences/Peking Union Medical College, Beijing, China.*Corresponding authors: Qiu Changchun ([email protected]) and Liu Jicheng ([email protected])
Evidence for Genetic Contribution to High-Altitude Pulmonary Edema in Chinese Railway Construction WorkersQiu Changchun1,3,*, Fan Ming2, Qi Yue3, Zhou Wenyu3, Liu Jicheng1,*

High-Altitude Medicine
16
were significantly associated with HAPE after applying the Bonferroni correction (p<0.005). Gene-gene interaction analy-sis found that the ACE A-240T, A2350G, and CYP11B2 C-344T polymorphisms had a strong synergistic effect on HAPE. In particular, the homozygous genotype combination of -240AA, 2350GG, and -344TT conferred high genetic suscep-tibility to HAPE. Our results provided further evidence for the synergistic effect of RAAS gene polymorphisms on HAPE susceptibility (4–6) (Figure 1).
Genes in the Heat Shock Protein 70 FamilyHeat shock proteins (HSPs) are a group of intracellular proteins upregu-lated during hypoxic stress. We focused on the common gene polymor-phisms in HSPA1A, HSPA1B, and HSPA1L in the HSP70 family to ex-plore their potential interactions with HAPE. Significant differences in alleles from the A-110C polymorphism of HSPA1A and alleles from the A1267G polymorphism of HSPA1B were observed between Han Chi-nese railway workers with and without HAPE. Furthermore, using hap-lotype analysis to compare the relative risk of HAPE, we observed that individuals with Hap 4 (G-C-A) (A1267G, G190C for HSPA1A, and A-110C for HSPA1B), and Hap 5 (G-C-A) had a significantly reduced risk (p=0.0009), whereas Hap 7 (A-C-C) resulted in a 2.43-fold increased risk for HAPE. When considered as diplotypes, individuals with Dip5 (Hap1-Hap7) had a significantly higher risk for HAPE (OR=3.39; 95%, CI=1.28-9.17; p=0.014). Functional assessment supported a role for the A-110C polymorphism of HSPA1A in the development of HAPE via a change in HSPA1A promoter activity (7).
Endothelial Nitric Oxide Synthase GeneThe endothelial nitric oxide synthase (eNOS) gene encodes the enzyme responsible for the production of NO, a signaling molecule involved in vasodilation. Some variants of the eNOS gene associated with HAPE have been reported (7). We conducted the largest, nested, case-con-trolled study to explore the genetic contribution to HAPE in railway construction workers living in Qinghai-Tibet at an altitude of 4,000 m above sea level. We found that the allele 894T and heterozygous G/T of the 894G/T variant of the eNOS gene was positively associated with susceptibility to HAPE. Furthermore, haplotype analysis comparing the relative risk of HAPE among co-inherited alleles, demonstrated that individuals with Hap 3 (T-T-b) and Hap 6 (C-G-a) were more suscep-tible to HAPE compared to those with other haplotypes, suggesting the interaction of multiple genetic loci within eNOS might be a major de-terminant for susceptibility to HAPE (8).
Other Candidate GenesOther specific candidate genes involving in the complex traits of HAPE have been investigated, including HLA-DR, HLA-DQ, GNB3, ADD1, ADRB2, CAT, GSTP1, CuZnSOD, MnSOD, HiF1, EPAS1, and mtD-NA. However, no significant association of these genes with suscepti-bility or resistance to HAPE was identified (9, 10).
HAPE is thought to be a multifactorial disorder resulting from the interaction of genetic and environmental factors. The combined study design of genome-wide association and epigenetic analysis should be undertaken in the future to elucidate the pathogenesis of HAPE and the complex interactions between the genome and hypoxic environment.
This project was approved by the Ethics Committee of the Institute of Basic Medical Sciences, CAMS/PUMC, and informed consent was obtained from all patients and healthy volunteers.
REFERENCES 1. P. H. Hackett, R. C. Roach, N. Engl. J. Med. 345, 107 (2001). 2. H. Mortimer, S. Patel, A. J. Peacock, Pharmacol. Ther. 101, 183 (2004). 3. M. J. MacInnis, M. S. Koehle, J. L. Rupert, High Alt. Med. Biol. 11, 349
(2010).4. Y.Qi,W.Niu,T.Zhu,W.Zhou,C.Qiu,Eur. J. Epidemiol. 23, 143 (2008).5. Y.Qi et al., J. Renin Angiotensin Aldosterone Syst. 12, 617 (2011). 6. T. Stobdan et al., J. Renin Angiotensin Aldosterone Syst. 12, 93 (2011).7. Y.Qi et al., Clin. Chim. Acta 405, 17 (2009).8. S.Yu-jing et al., Chin. Med. Sci. J. 25, 215 (2010). 9. Q. Shen et al., Bull. Med. Res. 38, 29 (2009).10. Y.Qiet al., Basic Clin. Med. 29, 811 (2009).
ACKNOWLEDGMENTSThe authors thank the volunteers for participating in this study. This work was supported by grants from the National Basic Research Ò 973Ó Program (Grant No. 2006CB504103), the Key Projects in the National Science and Technology Pillar Program (Grant No. 2006CB1190B), the National Laboratory Special Fund (Grant No. 2060204) and the National Natural Science Foundation of China (Grant No. 30393130, 30470615, and 31171146).
A
B
theÊ otherÊ wasÊ independentÊ andÊ additive.Ê TheÊ distributionÊ ofÊ HAPEÊ (leftÊ bars)ÊandÊ controlsÊ (rightÊ bars)Ê areÊ shownÊ forÊ eachÊ genotypeÊ combinationÊ inÊ eachÊ pairÊofÊ interactingÊ polymorphisms.Ê (B)Ê TheÊ ratioÊ ofÊ theÊ totalÊ numberÊ ofÊ HAPEÊ casesÊtoÊ theÊ totalÊ numberÊ ofÊ controlsÊ inÊ theÊ databaseÊ didÊ notÊ exceedÊ theÊ thresholdÊofÊ 0.97;Ê theÊ boxesÊ wereÊ labeledÊ asÊ low-riskÊ orÊ high-risk.Ê NonlinearÊ patternsÊ ofÊhigh-riskÊ (darkÊ grey)Ê andÊ low-riskÊ (lightÊ grey)Ê genotypeÊ combinationsÊ indicativeÊofÊi nteractionÊ wereÊ observed.
FigureÊ 1. Interaction dendrogram for the five polymorphisms modeled byÊ theÊ multifactor-dimensionalityÊ reductionÊ (MDR)Ê method.Ê (A)Ê ThereÊwereÊ strongÊ synergisticÊ (nonadditive)Ê effectsÊ ofÊ ACEÊ A-240T,Ê A2350G,ÊandÊ CYP11B2Ê C-344TÊ polymorphisms.Ê TheseÊ threeÊ polymorphismsÊcomprisedÊ theÊ bestÊ overallÊ MDRÊ model.Ê TheÊ relationshipÊ ofÊ eachÊ pairÊ withÊ

Section One
17
T housands of people enter high altitude (HA) areas by air-plane every year. In the past, acute mountain sickness (AMS) was the most common disease in those lacking the time for gradual acclimatization (1). To prevent AMS, a series of mea-
sures were studied and adopted including HA health education, physi-cal examinations, standardization of AMS preventive measures (2), and screening of medications for AMS (3, 4).
We studied the effects of a modified physical examination, popular-ization of health education, and disease prevention on the reduction of the causative factors for AMS. These measures have been used to draw up the five national standards for AMS prevention, which have played an important role in the prevention and control of AMS, and demonstrated that an obligatory medical management system is more
TableÊ 1. Ê IncidenceÊ ofÊ AMSÊ inÊ peopleÊ rapidlyÊ enteringÊ HAÊ areasÊ byÊ airplaneÊ sinceÊ 1987.
Year 1987 1993 1994 1998 2001 2003 2005 2007 2009 2011
Altitude (m) 3,500 3,680 3,680 3,200 3,900 3,680 3,680 3,680 3,680 3,900
Incidence (%) 48.5 38.0 31.4 20.0 22.8 10.8 5.6 3.0 2.6 1.7
TableÊ 2.Ê AMSÊ HospitalizationÊ rateÊ inÊ peopleÊ rapidlyÊ enteringÊ HAÊ areasÊ byÊ airplaneÊ sinceÊ 1993.
Year 1993 1994 1998 2001 2004 2005 2007 2009 2011
Altitude (m) 3,680 3,680 3,200 3,900 3,680 3,680 3,680 3,680 3,900
Hospitalization (%) 2.18 1.58 0 0 0.20 0.14 0.13 0.10 0.12
4,300 m above sea level (three men and two women) by airplane. Par-ticipants were 28 to 55 years old. After entering the HA area, they im-mediately performed low-intensity labor for more than eight hours a day under medical surveillance. Symptoms of reactions to HA were observed and scored daily for the first three days at HA and when they had finished the work. Based on Yin’s AMS Scoring System (9), mild symptoms and signs of reaction to HA with scores of two to four were observed in five subjects, but none suffered from AMS. No obvious symptoms and signs of HA reaction occurred in the other six subjects. All subjects satisfactorily finished their scheduled work with no ab-normal changes observed. Thus, it is not necessary to stop work com-pletely in order to prevent of AMS; low-intensity labor could also be performed under proper medical supervision.
Studies on the Prevention of Acute Mountain Sickness in People Entering High Altitudes by AirplaneNiu Wenzhong*, Fan Quanshui, Wu Qian, Yin Xudong, Pu Yonggao, Tang Bin
effective than prophylactic medication. There was a significant reduc-tion in both the incidence of AMS from 48.5% to 1.7% (Table 1) and the hospitalization rate from 2.18% to 0.12% (Table 2) (5–7) in those rapidly entering HA areas over the past 18 years.
As shown in Tables 1 and 2, AMS is no longer a severe threat to people who rapidly enter HA areas under normal circumstances. How-ever, if physical work is undertaken immediately and without enough rest after entering HA areas, AMS is still the most common risk factor (8). Therefore, several field trials at HA were performed to observe the incidence of AMS in people who worked in the plain region without a rest period after they were rapidly exposed to HA. This allowed for the study of preventive strategies for AMS in people from the plain re-gions who have to work at HA. Two groups of human volunteers were sent to either 3,680 m above sea level (five men and one woman) or
REFERENCES1. Y. Q. Gao, High Altitude Military Medicine (Chongqing Publisher,
Chongqing, China, 2005), p. 251. 2. W. Z. Niu, the XXXVI World Congress on Military Medicine, St.
Petersburg, Russia, June 2005. 3. Y. Wang, W. Z. Niu, J. J. Zhang, H. J. Wang, N. R. Chen, J. Preventive
Medicine of Chinese PeopleÕ s Liberation Army 22, 110 (2004).4. W. Z. Niu, Y. Wang, Z. W. Cao, S. X. Yu, L. Zhang, J. High Alt. Med. 16,
6 (2006). 5. W. Z. Niu et al., Medical Journal of National Defending Forces in
Southwest China 17, 822 (2007).6. W. Z. Niu, L. Fang, X. D. Yin, Q. Y. Zhai, Chin. J. Public Health Manage.
27, 416 (2011).7. W. Z. Niu, Y. Wang, J. J. Zhang, N. R. Chen, J. High Alt. Med. 12, 12
(2002). 8. W. Z. Niu, Q. S. Fan, L. Fang, X. F. Nie, W. J. Wei, J. High Alt. Med. 21,
62 (2010). 9. Z. Y. Yin et al., J. Preventive Medicine of Chinese PeopleÕ s Liberation
Army 15, 395 (1997).
Laboratory of Prevention of High Altitude Disease, Center for Disease Prevention and Control, Chengdu Military Command, Chengdu, Sichuan, China.*Corresponding author: [email protected]

High-Altitude Medicine
18
T he brain is one of the heaviest consumers of oxygen in the body. Hypoxia challenge at high altitude (HA) usually puts unacclimatized individuals at risk of acute mountain sickness that can cause neurological impairments including cerebral
edema, cortical atrophy, and cortical and subcortical lesions, accom-panied by behavioral compromises such as decline of cognitive per-formance and hallucinations (1). In contrast, under prolonged HA ex-posure, peripheral physiological systems typically employ adaptative mechanisms such as changes in respiratory and circulatory function, hemoglobin concentration, and arterial oxygen saturation. Such altera-tions change oxygen transport in the cerebral blood flow, leading to cu-mulative changes in brain structure and function. Our primary research focus is the use of a multimodal magnetic resonance imaging (MRI) approach to investigate cerebral adaptation to HA. Quantitative analy-sis methods such as voxel-based morphometry and Tract-Based Spatial Statistics were employed to measure gray matter (GM) and white mat-ter (WM) microstructural changes, while task-based and resting-state functional MRI (fMRI) were used to study functional changes.
Every year, the number of travelers to HA regions increases. We con-ducted a pre-post MRI study on 14 young, amateur mountain climb-
1Department of Physiology and Neurobiology, Medical College of Xiamen University, Xiamen, China; 2Laboratory for Higher Brain Function, Institute of Psychology, Chinese Academy of Sciences, Beijing, China; 3Huaxi Magnetic Resonance Research Center, West China Hospital, Sichuan University, Chendu, China; 4Department of Brain Protection and Plasticity, Institute of Basic Medical Sciences, Beijing, China.*Corresponding author: [email protected]
ers (19–23 years of age) who were without neurological complications before and after their travel to an altitude of approximately 6,206 m (1). No significant changes were observed in the total volumes of GM, WM, and cerebrospinal fluid after mountain climbing, although struc-tural alterations were seen in WM, but not GM. Significantly decreased WM fractional anisotropy (FA) values were observed at multiple sites of WM tracts (Table 1). Furthermore, compromises were found in the microstructural integrity of WM tracts (but not in WM volumes), sug-gesting that cytotoxic edema had occurred. We did not observe any cog-nitive changes in this population.
Every year people move from the lowlands to HA regions for work, study, or training, staying for several months to several years. An exam-ple of such a population is college students. In a previous study, we re-cruited 52 college students originally from areas at sea level, who were studying at a moderate altitude of 2,260 m over a seven-month period, with a return to sea level for 30 days in the middle of this period (2). We administered a battery of neuropsychological tests for comprehen-sive memory functions, which included short- and long-term memory, examining explicit and implicit visual and auditory memory. Results showed comparable performance with the matched sea-level control group except for a short-term visual, construction task. In another study, we obtained MRI data from 16 young healthy men (20–22 years of age) who had immigrated to the Qinghai-Tibet Plateau (2,300 to 4,400 m) for 2 years (unpublished data). Compared with matched sea level resi-dents, they showed changes in GM volumes, accompanied by changes in anisotropy and diffusivity at multiple sites of the WM tracts (Table 1). Increased GM volume in some regions had a significant positive correlation with altitude. Moreover, HA subjects developed ventilatory depression and deficits in mental rotation performance and reaction time
TableÊ 1. Ê ChangesÊ inÊ greyÊ andÊ whiteÊ matter,Ê andÊ behaviorÊ inÊ mountainÊ climbers,Ê adultÊ immigrants,Ê andÊ immigrantÊ descendants.
Mountain climbers HA adult immigrants HA immigrant descendants
Gray matter volume Nosignificantchanges (2)
Increases in: right middle frontal gyrus, right parahippocampal gyrus, right inferior and middle temporal gyri, bilateral inferior ventral pons, and right cerebellum Crus. (unpublished data)Decreases in: right postcentral gyrus and right superior frontal gyrus
Decreases in: bilateral anterior insula, right anterior cingulate cortex, bilateral prefrontal cortex, left precentral cortex, and right lingual cortex (4)
White matterFA values
Decreases in: CC (anterior and posterior body, splenium), bilateral CRT, right PCB, left SLF, and left middle cerebellar peduncle (2)
Increases in: CC (anterior body), left corticonuclear tract, bilateral SLF, and right ILF. Decreases in: CC (posterior body), bilateral hippocampus, right SCR, and right SLF (unpublished data)
Increases in: bilateral ALIC, bilateral anterior external capsule, CC, right CRT, right PCB, bilateral SLF and ILF, and bilateral SCR (4)Decreases in: the left optic radiation and left SLF (4)
Behavioral tests Nosignificantchanges(2)
Deficits in: reaction time in memory search, mental rotation, number search tasks and SRTT and mental rotation task (unpublished data), and in ROCF and visual reproduction (3)
Deficits in: digit span, ROCF, reaction time in SWM and VWM (5)
ALIC,Ê anteriorÊ limbÊ ofÊ internalÊ capsule;Ê CC,Ê corpusÊ callosum;Ê CRT,Ê corticospinalÊ tract;Ê FA,Ê fractionalÊ anisotropy;Ê HA,Ê highÊ altitude;Ê ILF,Ê inferiorÊlongitudinalÊ fasciculus;Ê PCB,Ê posteriorÊ cingulumÊ bundles;Ê ROCF,Ê Rey-OsterriethÊ ComplexÊ Figure;Ê SCR,Ê superiorÊ coronaÊ radiata;Ê SLF,Ê superiorÊlongitudinalÊ fasciculus;Ê SRTT,Ê serialÊ reactionÊ timeÊ task;Ê SWM,Ê spatialÊ workingÊ memory;Ê VWM,Ê verbalÊ workingÊ memory.
Adaptive Responses of the Brain to High AltitudeZhang Jiaxing1,*, Yan Xiaodan2, Zhang Haiyan1, Weng Xuchu2, Gong Qiyong3, Fan Ming4

Section One
19
tasks. GM volume in the parahippo-campal gyrus and middle frontal gyrus in HA subjects was negatively corre-lated with vital capacity. GM in the superior frontal gyrus had a significant positive correlation with mental rota-tion and GM in the postcentral gyrus was negatively correlated with num-ber search reaction time and memory reaction time.
Immigrant descendants are a suit-able population for studying develop-mental adaptation. Thus, 28 college students (17–23 years of age) born and raised in the Qinghai-Tibet Plateau re-gion (2,616–4,200 m) for at least 17 years were recruited. Their families had migrated from sea level areas to HA regions two to three generations ago. The control group consisted of matched subjects living at sea level. All subjects were from Han Chinese populations. HA subjects showed decreased GM volume in a number of brain regions accompanied by changes in FA values in multiple fiber pathways (Table 1) (3). HA sub-jects also showed significant differences in resting-state brain activity in multiple brain regions (4). A separate study demonstrated a decrease in cerebrovascular reactivity and a delay in hemodynamic response dur-ing a visual-cue guided maximum inspiration task (5). Since decreased appetite and weight loss were reported among travelers ascending to HA regions, we used pictures of food to elicit gustatory processing during an fMRI experiment. HA subjects showed decreased activation within the neural circuit for food craving such as the insula, accompa-nied by increased activation in regions for emotional processing such as the cingulate gyrus (6). A number of cognitive deficits were found in HA subjects, including working memory and mental construction (Table 1). An fMRI experiment with a verbal working memory task revealed decreased activation in many brain regions and decreased connectivity strength to and from the precentral cortex (7). The activa-tion and connectivity strength significantly correlated with behavioral performance. In contrast, an fMRI experiment with spatial working memory revealed an adaptive compensatory neural mechanism, show-ing no significant difference in activation in HA subjects compared with controls (8).
Based on the above studies, we observed that GM in the anterior insu-lar cortex, anterior cingulate cortex, superior prefrontal gyrus, premotor cortex, inferior and middle temporal cortex, ventral pons, parahippo-campus, and posterodorsal portion of the cerebellum and WM in the corpus callosum, corticospinal tract, and frontal cortex were most sus-ceptible to chronic hypoxia. To confirm this, 77 Tibetan natives (14–18 years of age) from the Qinghai-Tibet Plateau (2,300–5,300 m) were recruited for a study (9). Whole-brain analysis was conducted based on the mean GM volumes and WM FA values to identify significant as-sociations of structural responses with increasing altitude. The results revealed that altitude significantly correlated with GM volume in a large number of areas as observed in the previous study (Figure 1). Addition-ally, altitude had a significant positive correlation with GM volume in the occipital visual cortex, superior temporal gyrus, and temporal pole.
FigureÊ 1.Ê StatisticalÊ parametricÊ mapÊ forÊ greyÊ matterÊ volumeÊ correlatesÊ withÊ altitudeÊ (p<0.05).Ê RedÊ indicatesÊpositiveÊ correlation;Ê greenÊ indicatesÊ negativeÊ correlation.Ê UpperÊ leftÊ numbersÊ indicateÊ theÊ normalizedÊsagittalÊ sliceÊ numberÊ (y-value).Ê
In summary, GM changes occur in a number of regions of the brain responsible for HA respiratory and cardiovascular control. The WM microstructural alterations in the corpus callosum, cerebellar WM, and corticospinal tract might be related to changes in motor skills following acclimatization to HA. HA adaptation occurred at the cost of increased reaction time and deficits in working memory, as well as visual spatial construction. Observed changes in GM may help elucidate the mecha-nisms involved. The brains of youth and adults exhibit a different adap-tive response to HA, which is in agreement with previous studies show-ing that spatial memory was changed in pups, but not in adults, exposed to intermittent hypobaric hypoxia (10). In addition to developmental influences, the effects of genetic inheritance on the brain and whether brain changes recover to normal after a return to sea level should be investigated in future studies.
REFERENCES 1. H. Zhang et al., High Alt. Med. Biol. 13, 118 (2012).2. J. Zhang, H. Liu, X. Yan, X. Weng, High Alt. Med. Biol. 12, 37 (2011).
3. J. Zhang et al., PLoS One 5, e11449 (2010).4. X. Yan, J. Zhang, J. J. Shi, Q. Gong, X. Weng, Brain Res. 1348, 21
(2010). 5. X. Yan, J. Zhang, Q. Gong, X. Weng, BMC Neurosci. 12, 94 (2011).6. X.Yan,J.Zhang,Q.Gong,X.Weng, Exp. Brain Res. 209, 495 (2011). 7. X. Yan, J. Zhang, Q. Gong, X. Weng, Exp. Brain Res. 208, 437 (2011). 8. X.Yan,J.Zhang,Q.Gong,X.Weng,Brain Cogn. 77, 53 (2011). 9. J. Zhang, H. Zhang, S. Liu, Q. Gong, M. Fan, Abstract presented at
18th Annual Meeting of the Organization for Human Brain Mapping. Beijing, 10 June 2012.
10. J. Zhang et al., J. Neurosci. Res. 84, 228 (2006).
ACKNOWLEDGMENTSThis work was supported by the National Natural Science Foundation of China (Grant No. 30425008, 60628101, and 31071041), China Postdoctoral Science Foundation (Grant No. 20060390129) and the National Key Project (Grant No. 2012CB518200).
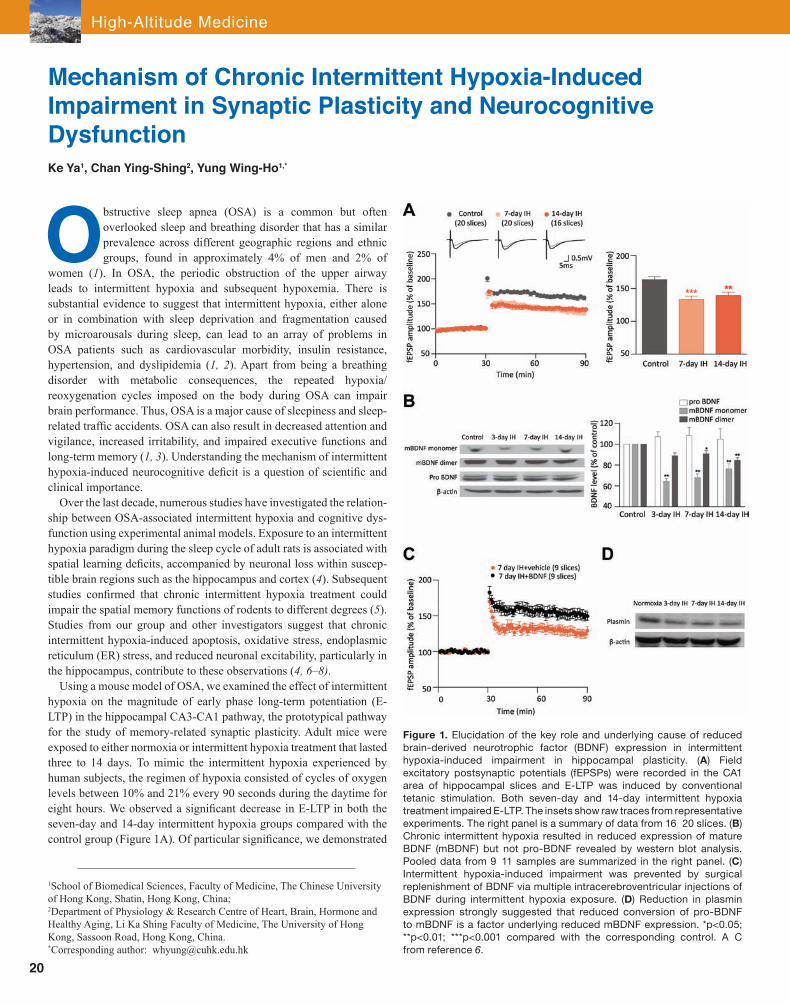
High-Altitude Medicine
20
Obstructive sleep apnea (OSA) is a common but often overlooked sleep and breathing disorder that has a similar prevalence across different geographic regions and ethnic groups, found in approximately 4% of men and 2% of
women (1). In OSA, the periodic obstruction of the upper airway leads to intermittent hypoxia and subsequent hypoxemia. There is substantial evidence to suggest that intermittent hypoxia, either alone or in combination with sleep deprivation and fragmentation caused by microarousals during sleep, can lead to an array of problems in OSA patients such as cardiovascular morbidity, insulin resistance, hypertension, and dyslipidemia (1, 2). Apart from being a breathing disorder with metabolic consequences, the repeated hypoxia/reoxygenation cycles imposed on the body during OSA can impair brain performance. Thus, OSA is a major cause of sleepiness and sleep-related traffic accidents. OSA can also result in decreased attention and vigilance, increased irritability, and impaired executive functions andlong-term memory (1, 3). Understanding the mechanism of intermittent hypoxia-induced neurocognitive deficit is a question of scientific and clinical importance.
Over the last decade, numerous studies have investigated the relation-ship between OSA-associated intermittent hypoxia and cognitive dys-function using experimental animal models. Exposure to an intermittent hypoxia paradigm during the sleep cycle of adult rats is associated with spatial learning deficits, accompanied by neuronal loss within suscep-tible brain regions such as the hippocampus and cortex (4). Subsequent studies confirmed that chronic intermittent hypoxia treatment could impair the spatial memory functions of rodents to different degrees (5). Studies from our group and other investigators suggest that chronic intermittent hypoxia-induced apoptosis, oxidative stress, endoplasmic reticulum (ER) stress, and reduced neuronal excitability, particularly in the hippocampus, contribute to these observations (4, 6–8).
Using a mouse model of OSA, we examined the effect of intermittent hypoxia on the magnitude of early phase long-term potentiation (E-LTP) in the hippocampal CA3-CA1 pathway, the prototypical pathway for the study of memory-related synaptic plasticity. Adult mice were exposed to either normoxia or intermittent hypoxia treatment that lasted three to 14 days. To mimic the intermittent hypoxia experienced by human subjects, the regimen of hypoxia consisted of cycles of oxygen levels between 10% and 21% every 90 seconds during the daytime for eight hours. We observed a significant decrease in E-LTP in both the seven-day and 14-day intermittent hypoxia groups compared with the control group (Figure 1A). Of particular significance, we demonstrated
1School of Biomedical Sciences, Faculty of Medicine, The Chinese University of Hong Kong, Shatin, Hong Kong, China; 2Department of Physiology & Research Centre of Heart, Brain, Hormone and Healthy Aging, Li Ka Shing Faculty of Medicine, The University of Hong Kong, Sassoon Road, Hong Kong, China.*Corresponding author: [email protected]
Mechanism of Chronic Intermittent Hypoxia-Induced Impairment in Synaptic Plasticity and Neurocognitive DysfunctionKe Ya1, Chan Ying-Shing2, Yung Wing-Ho1,*
FigureÊ 1.Ê ElucidationÊ ofÊ theÊ keyÊ roleÊ andÊ underlyingÊ causeÊ ofÊ reducedÊbrain-derivedÊ neurotrophicÊ factorÊ (BDNF)Ê expressionÊ inÊ intermittentÊhypoxia-inducedÊ impairmentÊ inÊ hippocampalÊ plasticity.Ê (A)Ê FieldÊexcitatoryÊ postsynapticÊ potentialsÊ (fEPSPs)Ê wereÊ recordedÊ inÊ theÊ CA1ÊareaÊ ofÊ hippocampalÊ slicesÊ andÊ E-LTPÊ wasÊ inducedÊ byÊ conventionalÊtetanicÊ stimulation.Ê BothÊ seven-dayÊ andÊ 14-dayÊ intermittentÊ hypoxiaÊtreatmentÊ impairedÊ E-LTP.Ê TheÊ insetsÊ showÊ rawÊ tracesÊ fromÊ representativeÊexperiments.Ê TheÊ rightÊ panelÊ isÊ aÊ summaryÊ ofÊ dataÊ fromÊ 16Ð 20Ê slices.Ê (B)ÊChronicÊ intermittentÊ hypoxiaÊ resultedÊ inÊ reducedÊ expressionÊ ofÊ matureÊBDNFÊ (mBDNF)Ê butÊ notÊ pro-BDNFÊ revealedÊ byÊ westernÊ blotÊ analysis.ÊPooledÊ dataÊ fromÊ 9Ð 11Ê samplesÊ areÊ summarizedÊ inÊ theÊ rightÊ panel.Ê (C)ÊIntermittentÊ hypoxia-inducedÊ impairmentÊ wasÊ preventedÊ byÊ surgicalÊreplenishmentÊ ofÊ BDNFÊ viaÊ multipleÊ intracerebroventricularÊ injectionsÊ ofÊBDNFÊ duringÊ intermittentÊ hypoxiaÊ exposure.Ê (D)Ê ReductionÊ inÊ plasminÊexpressionÊ stronglyÊ suggestedÊ thatÊ reducedÊ conversionÊ ofÊ pro-BDNFÊtoÊ mBDNFÊ isÊ aÊ factorÊ underlyingÊ reducedÊ mBDNFÊ expression.Ê *p<0.05;Ê**p<0.01;Ê ***p<0.001Ê comparedÊ withÊ theÊ correspondingÊ control.Ê AÐ CÊfromÊ referenceÊ 6.

Section One
21
in generating the cascade of events leading to neurocognitive deficits in OSA, as depicted in Figure 2. In this model, OSA-associated chronic intermittent hypoxia results in reduced neuronal excitability, decreased BDNF levels, increased oxidative stress, and ER stress. These factors interact and operate in a synergistic manner to increase apoptosis and cell injury and weaken long-term synaptic plasticity that together cause memory impairment and other neurocognitive dysfunctions. Careful dissection of the interrelationship among these factors may enable us to have a greater understanding of the pathogenesis of OSA neurobehavioral symptoms.
REFERENCES 1. W. Lee, S. Nagubadi, M. H. Kryger, B. Mokhlesi, Expert Rev. Respir.
Med. 2, 349 (2008). 2. P. Levy, M. R. Bonsignore, J. Eckel, Eur. Respir. J. 34, 243 (2009). 3. M. L. Jackson, M. E, Howard, M. Barnes, Prog. Brain Res. 190, 53
(2011). 4. D. Gozal, J. M. Daniel, G. P. Dohanich, J. Neurosci. 21, 2442 (2001). 5. B. W. Row, Adv. Exp. Med. Biol. 618, 51 (2007). 6. H. Xie et al., Neurobiol. Dis. 40, 155 (2010). 7. B. W. Row, R. Liu, W. Xu, L. Kheirandish, D. Gozal, Am. J. Respir. Crit.
Care Med. 167, 1548 (2003).8. Y.Zhuet al., J. Neurosci. 28, 2168 (2008). 9. P. Pang et al., Science 305, 487 (2004).
ACKNOWLEDGMENTSThis work was supported by the Research Grants Council of Hong Kong and the National Natural Science Foundation of China (Grant No. CUHK478308, 2900336, and 30931160433).
that intermittent hypoxia significantly impaired conventional E-LTP and to a greater extent late-phase LTP, which better correlates with the formation of long-term memory (6). These data indicate that neurocognitive deficits observed in OSA may be caused by intermittent hypoxia-induced impairment of hippocampal LTP.
We previously showed that brain-derived neu-rotrophic factor (BDNF) is crucial for the consol-idation of long-term synaptic plasticity (9). We speculated that BDNF levels in the brain might be altered by intermittent hypoxia. Indeed, in the mouse model, we found that BDNF expression was signifi cantly reduced after chronic intermit-significantly reduced after chronic intermit-reduced after chronic intermit-tent hypoxia treatment (Figure 1B). Addition-t (Figure 1B). Addition- (Figure 1B). Addition-. Addition-Addition-ally, exogenous application of BDNF restored the magnitude of LTP in hippocampal slices from hypoxia-treated mice, and microinjection of BDNF into the brain of hypoxic mice pre-vented the LTP impairment (Figure 1C). Thus, a decrease of BDNF could be a crucial factor con-tributing to the absence of normal hippocampal plasticity and therefore memory function in the intermittent hypoxia model. In line with this hy-pothesis, we recently showed that administration of ampakines, a group of AMPA receptor modu-lators, restored BDNF levels in the hippocampus and prevented the decrease in LTP magnitude caused by intermittent hypoxia (unpublished data). Thus, by targeting BDNF expression, ampakine administra-tion could be a potential therapeutic treatment for the neurocognitive symptoms of OSA subjects.
BDNF levels are upregulated during some pathological conditions of the central nervous system, a phenomenon usually regarded as a compensatory mechanism beneficial to the survival of neurons. However, during prolonged and repeated hypoxia/reoxygenation under the chronic intermittent hypoxia paradigm, the ability of brain cells to express BDNF may be compromised. The duration-dependent decrease in BDNF levels observed in the intermittent hypoxia model supports this notion. We believe that the decrease in BDNF is not simply the result of neuronal loss because other neurotrophic factors, such as NT4/5, were not affected. Additionally, we observed the reduced expression of plasmin, an extracellular enzyme that cleaves pro-BDNF to form mature BDNF, in the chronic intermittent hypoxia model (Figure 1D). This is consistent with our observation that pro-BDNF levels were not affected by chronic intermittent hypoxia treatment, and suggests that proteolytic cleavage of pro-BDNF to mature BDNF was affected, rather than transcription of the BDNF gene.
Our studies shed new light on the causes underlying intermittent hypoxia-induced impairment in long-term synaptic plasticity and neurocognitive deficits. Reduced neuronal excitability and other pathological processes such as the generation of reactive oxygen species (ROS) and ER stress may contribute to neuronal damage under chronic intermittent hypoxia condition. Since BDNF can prevent or suppress these processes, it is possible that lack of BDNF in chronic intermittent hypoxia not only underlies impaired long-term synaptic plasticity but also fails to prevent apoptosis and other neuronal injuries induced by ROS and ER stress. Thus, the lack of BDNF could play a pivotal role
FigureÊ 2.Ê ProposedÊ interactionsÊ betweenÊ BDNFÊ reductionÊ andÊ otherÊ pathologicalÊ processesÊthatÊ leadÊ toÊ neuronalÊ injuryÊ andÊ decreasedÊ neuroplasticityÊ inÊ obstructiveÊ sleepÊ apneaÊ (OSA).ÊChronicÊ intermittentÊ hypoxiaÊ causesÊ decreasedÊ neuronalÊ excitability,Ê decreasedÊ BDNFÊexpressionÊ andÊ generationÊ ofÊ oxidativeÊ stressÊ andÊ ERÊ stress.Ê TheseÊ factorsÊ actÊ synergisticallyÊtoÊ increaseÊ apoptosisÊ andÊ impairÊ long-termÊ synapticÊ plasticity,Ê resultingÊ inÊ impairedÊ memoryÊand other neurocognitive deficits. In this model, decreased expression of BDNF plays a pivotal roleÊ inÊ ROSÊ generation,Ê ERÊ stress,Ê apoptosis,Ê andÊ impairmentÊ ofÊ synapticÊ plasticity.

High-Altitude Medicine
22
High-altitude pulmonary edema (HAPE) and high-altitude pul-monary hypertension (HAPH) are two forms of altitude sick-ness that endanger the lives of people climbing or migrating to high altitudes. Hypoxic pulmonary hypertension (HPH) is
a hallmark of HAPE and HAPH. Although several drugs that are used for the prevention and treatment of pulmonary hypertension (PH) are potent in preventing or treating HPH, they are not ideal. Since large areas of China are at a high altitude, there is a perfect opportunity for scholars to observe the effects of Chinese herbs on the treatment of alti-tude sickness. The development of traditional Chinese medicine (TCM) for altitude sickness in parallel with standard drug therapies opens an avenue to study TCM in mountain medicine. Here, we summarize the history of TCM used in mountain medicine in China with a brief review of our work on HPH.
TCM and Altitude SicknessIn TCM theory, altitude sickness is a disequilibrium state of the human body that continually interacts and exchanges resources and energies with the surrounding high-altitude environment of hypoxia, cold, ir-radiation, and dryness. The development and prognosis of the illness is dependent on two opposite and complementary factors in the human body, namely “yin” and “yang,” which are important in the philosophy of TCM and ancient China. Many Chinese herbs believed to be capable of adjusting “yin” or “yang” have been used to treat altitude sickness for nearly half a century. New information regarding these medicines has been obtained from local medical journals as well as anecdotal evi-dence. The selection of candidate drugs for these trials was often expe-rience-based and most of the studies performed did not follow protocols or methodology favored by modern medicine. The herbs were usually prescribed as a mixture, with the appropriate ratio of individual herbs decided by the different states of “yin” and “yang.” The treatments used were from high-altitude plants (such as Dracocephalum heterophyllum Benth and Gymnadenia conopsea), a class of herbs to treat cardiovas-cular ailments (Salvia miltiorrhiza, Radix Codonopsis, and Radix An-gelicae Sinensis), adaptogens (Rhodiola rosea and Panax ginseng) or antioxidants (Ginkgo biloba and Lycium chinense), with some adjuvant herbs. It is thought that the different compounds play complementary roles to produce the overall effect, although evidence for beneficial ef-fects of the herbs is usually doubted or neglected by researchers who favor a reductionist approach. However, it should be noted that more robust clinical trials and experimental studies of Chinese herbs and sin-gle molecule entities have been conducted in recent years. These trials
1Department of Occupational and Environmental Health, Fourth Military Medical University, Xi’an, Shaanxi, China;2Department of Pathophysiology, Fourth Military Medical University, Xi’an, Shaanxi, China;3The Ministry of Education Key Lab of Hazard Assessment and Control in Special Operational Environment, School of Public Health, Fourth Military Medical University, Xi’an, Shaanxi, China.*Corresponding authors: Chen Jingyuan ([email protected]) and Luo Wenjing ([email protected])
report a beneficial effect of Chinese herbs on altitude sickness, such as acute mountain sickness (AMS), HAPH, or chronic mountain sickness (CMS) (Table 1) (1). Among these, S. miltiorrhiza and R. rosea were the two herbs most commonly prescribed and evaluated, and a series of studies using these herbs supported the potential for TCM in the treat-ment of altitude sickness.
Salvia Miltiorrhiza and Rhodiola Rosea: Candidate Drugs for HPHThe pathogenesis of HPH describes a process ranging from acute hy-poxic pulmonary vasoconstriction to medial hypertrophy and remodel-ing of muscular pulmonary arteries, in which oxidative stress, altered expression of ion channels in pulmonary arterial smooth muscle cells (PASMCs), dysfunction of pulmonary vascular endothelium and cal-cium mobilization, and influx in PASMCs are believed to be underlying mechanisms. Using isolated pulmonary arteries and cultured PASMCs from chronically hypoxic rats, we found that Tanshinone IIA, one of the active components found in S. miltiorrhiza, had an inhibitory effect on HPH and pulmonary vascular remodeling. Chronic hypoxia-induced increases in the mean pulmonary arterial pressure (mPAP), right ven-tricular hypertrophy (RVH), and thickening of distal pulmonary ar-teries, were all attenuated by pretreatment with Tanshinone IIA. This was further supported by the Tanshinone IIA-induced suppression of hypoxia-induced PASMC proliferation and prevention of hypoxia-in-duced downregulation of voltage-activated potassium channel mRNA and protein expression in pulmonary arteries and PASMCs (2). An antioxidant effect of Tanshinone IIA was observed as an increase in superoxide dismutase and reduction in malondialdehyde levels in the homogenates of lungs exposed to hypoxia (3). Moreover, in pulmonary artery rings from normal rats, Tanshinone IIA eliminated acute hypoxia-induced vasoconstriction and potentiated vasorelaxation. In pulmonary artery rings from hypoxic pulmonary hypertension rats, Tanshinone IIA reversed sustained constriction induced by phenylephrine and led to sustained vasodilation (4). Tanshinone IIA, which mimics the action of acetazolamide (5), achieved its effect by inhibiting hypoxia-induced Ca2+ responses, although it was endothelium independent and partially mediated by opening Ca2+-activated K+ channels.
Another potent drug for treating HPH is Rhodioloside, one of the ac-tive components of R. rosea. Rhodioloside research has benefited from multidisciplinary studies. Similar to treatment with Verapamil, a cal-cium channel blocker, Rhodioloside inhibited acute hypoxia-induced proliferation of PASMCs in rabbit lung (6), and increased the expres-sion of nitric oxide synthase and inhibited KCl-induced cell contraction in vascular smooth muscle cells (7). Pretreatment with Rhodioloside increased arterial oxygen saturation by 3% in a group of young men acutely exposed to an altitude of 3,658 m (unpublished data). Together, this provides evidence supporting a possible anti-HPH effect of Rho-dioloside. Our ongoing research with R. rosea is focused on mecha-nistic studies and active-site chemistry using chemically engineered analogues. Preliminary results demonstrate that one analogue, benzyl galactosidase, has an effect similar to Rhodioloside (8).
Chinese Herbs and Altitude Sickness: Lessons from Hypoxic Pulmonary Hypertension ResearchKe Tao1,3, Li Zhichao2, Zhang Wenbin1,3, Wang Jiye1,3, Luo Wenjing1,3,*, Chen Jingyuan1,3,*
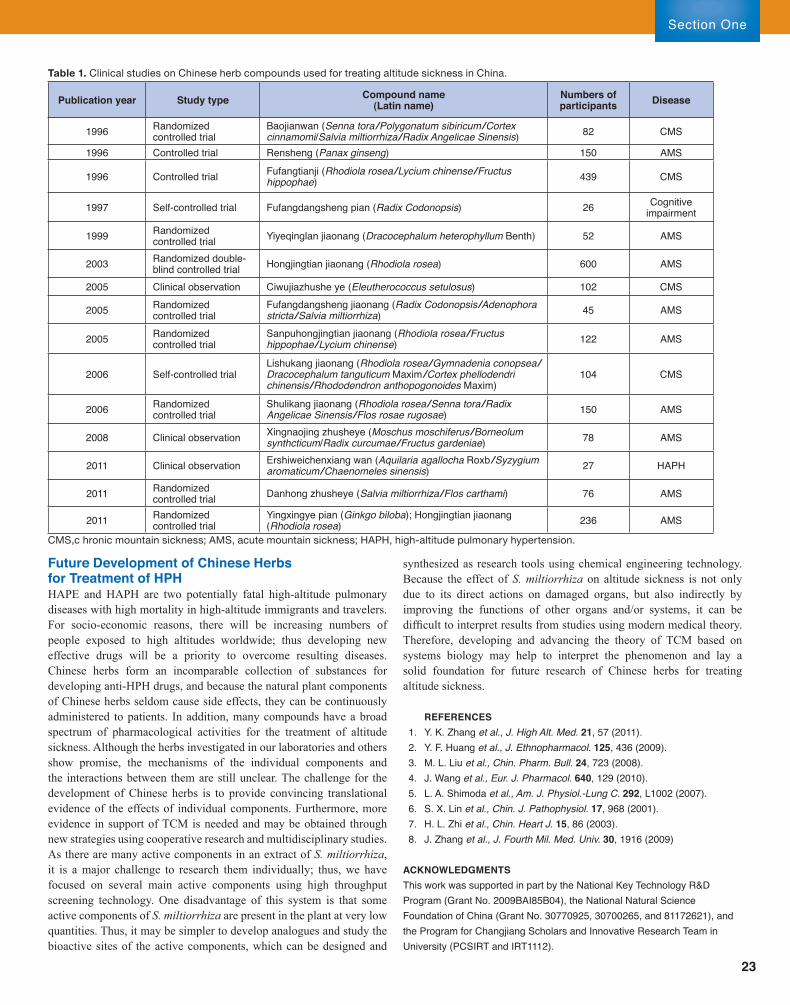
Section One
23
Future Development of Chinese Herbs for Treatment of HPHHAPE and HAPH are two potentially fatal high-altitude pulmonary diseases with high mortality in high-altitude immigrants and travelers. For socio-economic reasons, there will be increasing numbers of people exposed to high altitudes worldwide; thus developing new effective drugs will be a priority to overcome resulting diseases. Chinese herbs form an incomparable collection of substances for developing anti-HPH drugs, and because the natural plant components of Chinese herbs seldom cause side effects, they can be continuously administered to patients. In addition, many compounds have a broad spectrum of pharmacological activities for the treatment of altitude sickness. Although the herbs investigated in our laboratories and others show promise, the mechanisms of the individual components and the interactions between them are still unclear. The challenge for the development of Chinese herbs is to provide convincing translational evidence of the effects of individual components. Furthermore, more evidence in support of TCM is needed and may be obtained through new strategies using cooperative research and multidisciplinary studies. As there are many active components in an extract of S. miltiorrhiza, it is a major challenge to research them individually; thus, we have focused on several main active components using high throughput screening technology. One disadvantage of this system is that some active components of S. miltiorrhiza are present in the plant at very low quantities. Thus, it may be simpler to develop analogues and study the bioactive sites of the active components, which can be designed and
TableÊ 1. Ê ClinicalÊ studiesÊ onÊ ChineseÊ herbÊ compoundsÊ usedÊ forÊ treatingÊ altitudeÊ sicknessÊ inÊ China.
Publication year Study type Compound name (Latin name)
Numbers of participants Disease
1996 Randomized controlled trial
Baojianwan (Senna tora /Polygonatum sibiricum /Cortex cinnamomi/Salvia miltiorrhiza /Radix Angelicae Sinensis) 82 CMS
1996 Controlled trial Rensheng (Panax ginseng) 150 AMS
1996 Controlled trial Fufangtianji (Rhodiola rosea /Lycium chinense /Fructus hippophae) 439 CMS
1997 Self-controlled trial Fufangdangsheng pian (Radix Codonopsis) 26 Cognitive impairment
1999 Randomized controlled trial Yiyeqinglanjiaonang(Dracocephalum heterophyllum Benth) 52 AMS
2003 Randomized double-blind controlled trial Hongjingtian jiaonang (Rhodiola rosea) 600 AMS
2005 Clinical observation Ciwujiazhushe ye (Eleutherococcus setulosus) 102 CMS
2005 Randomized controlled trial
Fufangdangsheng jiaonang (Radix Codonopsis /Adenophora stricta /Salvia miltiorrhiza) 45 AMS
2005 Randomized controlled trial
Sanpuhongjingtian jiaonang (Rhodiola rosea /Fructus hippophae /Lycium chinense) 122 AMS
2006 Self-controlled trialLishukang jiaonang (Rhodiola rosea /Gymnadenia conopsea /Dracocephalum tanguticum Maxim /Cortex phellodendri chinensis /Rhododendron anthopogonoides Maxim)
104 CMS
2006 Randomized controlled trial
Shulikang jiaonang (Rhodiola rosea /Senna tora /Radix Angelicae Sinensis /Flos rosae rugosae) 150 AMS
2008 Clinical observation Xingnaojing zhusheye (Moschus moschiferus /Borneolum synthcticum/Radix curcumae /Fructus gardeniae) 78 AMS
2011 Clinical observation Ershiweichenxiang wan (Aquilaria agallocha Roxb /Syzygium aromaticum /Chaenomeles sinensis) 27 HAPH
2011 Randomized controlled trial Danhong zhusheye (Salvia miltiorrhiza /Flos carthami) 76 AMS
2011 Randomized controlled trial
Yingxingyepian(Ginkgo biloba); Hongjingtian jiaonang (Rhodiola rosea) 236 AMS
CMS,Êc hronicÊ mountainÊ sickness;Ê AMS,Ê acuteÊ mountainÊ sickness;Ê HAPH,Ê high-altitudeÊ pulmonaryÊ hypertension.
synthesized as research tools using chemical engineering technology. Because the effect of S. miltiorrhiza on altitude sickness is not only due to its direct actions on damaged organs, but also indirectly by improving the functions of other organs and/or systems, it can be difficult to interpret results from studies using modern medical theory. Therefore, developing and advancing the theory of TCM based on systems biology may help to interpret the phenomenon and lay a solid foundation for future research of Chinese herbs for treating altitude sickness.
REFERENCES1. Y.K.Zhanget al., J. High Alt. Med. 21, 57 (2011).2. Y. F. Huang et al., J. Ethnopharmacol. 125, 436 (2009).
3. M. L. Liu et al., Chin. Pharm. Bull. 24, 723 (2008). 4. J. Wang et al., Eur. J. Pharmacol. 640, 129 (2010). 5. L. A. Shimoda et al., Am. J. Physiol.-Lung C. 292, L1002 (2007). 6. S. X. Lin et al., Chin. J. Pathophysiol. 17, 968 (2001). 7. H. L. Zhi et al., Chin. Heart J. 15, 86 (2003). 8. J. Zhang et al., J. Fourth Mil. Med. Univ. 30, 1916 (2009)
ACKNOWLEDGMENTSThis work was supported in part by the National Key Technology R&D Program (Grant No. 2009BAI85B04), the National Natural Science Foundation of China (Grant No. 30770925, 30700265, and 81172621), and the Program for Changjiang Scholars and Innovative Research Team in University (PCSIRT and IRT1112).

High-Altitude Medicine
24
A n artificial oxygen-enriched environment at high altitudes can protect people from hypoxia and is especially suitable for flight crews (1) and tourists (2) who have had little time to acclimatize to low oxygen conditions. Here, we report a
new way to prevent high-altitude pulmonary edema using an oxygen-enriched room with a diffusion oxygen-supply system (3, 4).
To determine a suitable standard procedure for the application of the oxygen-enriched room, animal and human experiments were per-formed. Wistar rats were divided into five groups and placed at simu-lated altitudes as follows: 0 m, 6,000 m, 6,000 m with 35% or 30% continuous oxygen (physiologically equivalent to an altitude of ap-proximately 2,500 m or 3,500 m, respectively), and 6,000 m supplied with 35% oxygen for four hours at a time, with breaks of four hours. The water ratio, endothelin-1, and nitric oxide synthase (NOS) content of the lungs were remarkably different between the groups (4, 5). The group receiving 35% oxygen alternately every four hours had the best results of all hypoxic groups.
At an altitude of 3,500 m, an oxygen-enriched room with an oxygen concentration of 25.49% ± 0.26% (physiologically equivalent to an alti-tude of approximately 2,200 m) was developed by using a high altitude diffusion oxygen-supply system based on a molecular sieve oxygen generating system with pressure swing adsorption (1). Young human volunteers were divided into three groups: the oxygen rich group (O) was in the oxygen-enriched room at night, without oxygen enrichment during the day; the hypoxia group (H) was without oxygen enrichment; and a group representing low altitude plain conditions (control, P) was given no treatment. After group O and H reached a high altitude by airplane, heart rate (HR) and oxygen saturation (SaO2) levels were re-corded before oxygen was supplied, while group P remained on the plain. From 22:00 to 9:00 hours the next day, group O and H slept in the oxygen-enriched room or a normoxic room, respectively.
Results showed that the SaO2 of group O was 92.3% ± 1.0% after oxygen was supplied, which was higher than that before oxygen was supplied (82.9% ± 4.2%). The SaO2 of group O was also higher than
Institute of Aviation Medicine, No.28, Fucheng Lu, Beijing, China.*Corresponding author: [email protected]
that for group H (79.3% ± 5.9%; p<0.01), but was lower than that for group P (97.3% ± 0.8%; p<0.05). There was no significant difference in HR between group O and H before or after administration of oxy-gen. However, the HR of group H and O was higher than that of group P (p<0.01). Measurement of heart rate variability (8) showed that the normalized low frequency and low frequency/high frequency ratio of group O and H were 89.3 ± 2.9 ms2, 9.4 ± 2.8 and 90.2 ± 1.8 ms2, 9.9 ± 1.9 ms2, respectively, which was not significantly different. However, these values were significantly higher than those of group P (85.8 ± 2.9 ms2 and 6.4 ± 1.4 ms2; p<0.05).
There was no significant difference in sleep structure between group O and H, although both groups had significantly more light sleep and less deep sleep (p<0.01), as measured by a portable sleep monitor, com-pared with group P. The results of a questionnaire showed that group P had the best sleep quality and group H had the worst, while group O was in between (6).
In summary, we have developed a new high altitude diffusion oxy-gen-supply system, which is especially suitable for flight crews (1) and tourists (2). The oxygen concentration of the oxygen-enriched room should be 25% ± 0.5%, which results from an oxygen partial pressure of inspired air (75±2 mmHg) and a physiologically equivalent altitude (2,200±150 m) (7). Additionally, an intermittent oxygen supply is bet-ter than a continuous one (6). These results represent the foundation for the application of an oxygen-enriched room for use at night, which is an efficient solution for people entering Tibet who lack the time to ac-climatize gradually (9).
REFERENCES 1. H. J. Xiao, Physiology of Aviation Oxygen Protective Equipment (Military
Medicine Science Publisher, 2005) pp. 291-293. 2. H. J. Xiao, High Alt. Med. Biol. 5, 226 (2004). 3. H. J. Xiao et al., China-Japan Medical Conference, Beijing.Nov,3-
6(2002). 4. H. J. Xiao et al., J. Chin. Aerospace Med. 22, 259 (2011). 5. Z. R. Zhang et al., J. Chin. Aerospace Med. 22, 34 (2011). 6. C. L. Deng et al., J. Chin. Aerospace Med. 21, 51 (2010). 7. C. L. Deng, H. J. Xiao, J. Alt. Med. S1, 42 (2009). 8. H. J. Xiao et al., High Alt. Med. Biol. 5, 233 (2004). 9. H. J. Xiao et al., J. Chin. Aerospace Med. 19, 266 (2008).
Fast Acclimatization to High Altitude Using an Oxygen-Enriched RoomXiao Huajun*, Deng Changlei, Zhang Zhaorui, Wang Guiyou, Zang Bin, Wen Dongqing, Liu Xiaopeng, Zhang Bo

Section One
25
People from Tibet are well adapted to high altitudes. One ex-ample of adaptation can be found in the maternal-placental-fetal system in Tibetan women, where placental mechanisms ensure an adequate oxygen supply to the fetus even in hypoxic
conditions (1–5). However, few studies have looked at sex hormone levels during perimenopausal stages in women living at moderate or high altitudes. We therefore compared sex hormone levels in groups of perimenopausal Tibetan women living at various altitudes with peri-menopausal Chinese Han women living at sea level to investigate the correlation between altitude and sex hormone levels.
2009. The age and BMI values are shown in Table 1 and venous sex hormone testing results in Table 2.
It is interesting that no significant difference in sex hormone levels was observed among the two groups of perimenopausal Tibetan women and the group of Han women living at sea level, verifying the study results of previous researchers (6, 7). These results suggested that a different oxygen partial pressure (PaO2) at moderate and high altitude, or at sea level, has no effect on the Tibetan female hormonal reproduc-tive system.
Studies on the maternal-placental-fetal system in Tibetan women
Qinghai Red Cross Hospital, Xining, Qinghai, China.*Corresponding author: [email protected]
TableÊ 1. Ê AgeÊ andÊ BMIÊ comparisonÊ amongÊ TibetanÊ womenÊ atÊ moderateÊ andÊ highÊ altitudesÊ andÊ HanÊ womenÊ atÊ seaÊ level.
Group Number of Cases Age (years) BMI (kg/m2)Sea level 198 48.9±2.2 23.2±2.32,260 m 180 48.0±2.1 23.4±2.64,200 m 180 47.0±2.7 23.1±2.5
No statistically significant difference was found amongst the three groups.
TableÊ 2.Ê VenousÊ E2,Ê FSH,Ê T,Ê P,Ê PRL,Ê andÊ LHÊ levelsÊ inÊ TibetanÊ womenÊ atÊ moderateÊ andÊ highÊ altitudesÊ andÊ HanÊwomenÊ atÊ seaÊ level.Ê Ê
Target Sea level group (database) 2,260 m group (n=180) 4,200 m group (n=180)
E2 (pg/ml) 74.29±67.23 72.86±68.74 74.96±66.72FSH (IU/L) 5.80±3.41 5.61±3.81 6.00±3.78T (nmol/L) 2.11±1.56 1.84±1.83 1.82±1.74P (pg/ml) 10.9±10.6 9.80±10.4 9.0±10.8PRL (IU/L) 390.8±230.0 378.8±228.0 400.0±228.1LH (IU/L) 25.8±24.1 28.5±24.7 26.6±26.1
(n=180Ê forÊ eachÊ TibetanÊ group).Ê E2,Ê estradiol;Ê FSH,Ê follicle-stimulatingÊ hormone;Ê T,Ê testosterone;Ê P,Ê progesterone;ÊPRL,Ê prolactin;Ê LH,Ê luteinizingÊ hormone.
have suggested that people living at high altitudes for generations might develop genetic adaptations against hypoxia. Our study has identified a similar adaptive phenomenon, providing further evidence to support the belief that Tibetans are highly adapted to high-altitude living.
REFERENCES 1. C. M. Beau et al., Proc. Natl. Acad. Sci. U.S.A. 99, 17215 (2002). 2. C. M. Beau et al., Am. J. Phys. Anthropol.106, 385 (1998). 3. F. C. Villafuerte et al., J. Appl. Physiol. 96, 1581 (2004).4. Y.Zhang,Ed.Human and Plateau (Qinghai PeopleÕ s Publication,
Qinghai, 1996), pp. 1995-2911. 5. H. Liu, Medicine Innovation Research 04, 139 (2007). 6. J. Li, Chinese J. Birth Health Heredity 22, 113 (2006). 7. Z. Nong, Guide of China Medicine 08, 926 (2005).8. Y. Dai et al., Journal of Beijing University of Traditional Chinese
Medicine 27, 80 (2004).
A Comparison of Perimenopausal Sex Hormone Levels Between Tibetan Women at Various Altitudes and Han Women at Sea LevelZhang Jianqing*, Wei Chunmei, Xiao Hong, Zhang Shuna
Tibetan women were divided into two groups (180 women per group), one living at a moderate altitude (2,260 m), and the other at high altitude (4,200 m). The age of onset of menarche was 14.01 ± 1.60 years old. The data for Han women at sea level were obtained from a study entitled “Clinical significance of measuring six female sex hormones” published in the journal Chinese Clinical Professionals (8). The data were collected from residents in Beijing who were the same age and had the same body mass index (BMI) as the Tibetan women we studied.
Venous blood samples were obtained early in the follicular phase and two months after the cessation of menses from April 2008 to October

High-Altitude Medicine
26
Hundreds of thousands of people visit the high-altitude regions of Tibet for business or recreational travel each year, despite the threat that severe acute high altitude illnesses—such as high-altitude pulmonary edema (HAPE) and high-altitude
cerebral edema (HACE)—represent to their health (1, 2). Although diagnostic criteria for severe acute high-altitude illnesses have been established, the specific diagnosis of illness at a very early stage is still difficult and, therefore, the best opportunity for treatment may be missed (3). Many reports have discussed the treatment for severe acute high altitude illnesses, but there is still a lack of standardization regard-ing medication (4). Our center is located at an altitude of 3,658 m and receives many patients every year. In the last decade, the center has emphasized early-stage diagnosis and standardized treatment of HAPE and HACE, and much progress has been made.
To analyze the efficacy of early-stage diagnosis of HAPE and HACE, screening of 24,200 subjects who rapidly ascended to a high altitude was completed using a symptom scoring system for acute mountain sickness (AMS). Subsequent observation and follow-up visitation was completed for subjects strongly suspected of being sick, looking at ear-ly symptoms, physical manifestations of AMS, and auxiliary examina-tion results. Through comparative analysis of suspected individuals and diagnosed subjects, we identified a series of clinical features of early stage HAPE, including dyspnea, bilateral or unilateral/local respiratory crackles, and X-ray characteristics of decreased radiolucent lungs, in-creased or hazy lung markings, and ground-glass opacity (5). We also identified a series of clinical features of early stage HACE, including headache and vomiting with progressive severity not relieved by oxy-gen therapy, and magnetic resonance imaging features of decreased T1WI signals and increased T2WI signals of cerebral parenchyma with patchy appearance (6). Finally, we established the early-stage diagnos-tic criteria for HAPE and HACE.
For the treatment of HAPE and HACE, we set up several treatment regimens based on the major medications used in clinical practice
Center for Prevention and Treatment of High Altitude Illness, Tibet General Hospital of PLA, Lhasa, Tibet, China.*Corresponding author: [email protected]‡Contributed equally to this work.
worldwide. The results showed that a treatment regimen using oxygen, dexamethasone, aminophylline, and furosemide was the most effec-tive and safe for the treatment of HAPE (7), while a treatment regi-men using oxygen, dexamethasone, mannitol, and furosemide was the most effective and safe for the treatment of HACE (8). We es-tablished standardized treatment regimens for both HAPE and HACE that took into account general treatment principles, oxygen therapy, drug indications, medication doses and delivery method, prevention of complications, control of liquid intake, and discharge instructions. Ad-ditionally, we applied ultrashort wave therapy and digitally controlled hypothermic blanket/cap in the treatment of HAPE and HACE. We also balanced exogenous nitric oxide for treatment of HAPE, by using a normal composition of air instead of a mixture of N2 and pure oxygen or 80% oxygen. By looking at the hemodynamics, oxygen metabolism dynamics, clinical presentation of symptoms, improvements in patient wellness, and mean duration of treatment, we found that treatment with medication was more effective when combined with the therapies out-lined above.
Over the last decade, we have successfully performed research on early-stage diagnosis and standardized treatment of HAPE and HACE, and have provided a scientific basis for the early recognition, diagnosis, and therapy in order to generate a best practices regimen for clinical treatment. Through the dissemination of our research results, we have improved the medical services provided to soldiers working at high altitude and also made important contributions to providing medical services to the Qinghai-Tibet railway construction workers and to the YuShu mountain earthquake relief teams. None of the latter two groups died of AMS and no soldier has succumbed to AMS in the last decade, both considerable achievements in high-altitude medicine.
REFERENCES 1. C. Sartori et al., N. Engl. J. Med. 346, 1631 (2002). 2. M. Maggiorini et al., Prog. Cardiovasc. Dis. 52, 500 (2010). 3. F. Z. Wang et al., Clinical Focus (Chinese) 15, 426 (2000). 4. D. S. Geng et al., Medical Recapitulate (Chinese) 13, 1623 (2007). 5. S. Z. Li et al., Military Medical Journal of South China 24, 161 (2010). 6. S. Z. Li et al., Military Medical Journal of South China 24, 167 (2010). 7. S. Z. Li et al., Medical Journal of National Defending Forces in
Southwest China 20, 697 (2010). 8. S. Z. Li et al., Medical Journal of National Defending Forces in
Southwest China 20, 700 (2010).
Diagnosis and Treatment of HAPE and HACE in the Tibet High-Altitude Region in the Last DecadeLi Suzhià , Zheng Bihaià , Huang Yue, Yan Chuncheng, Xie Xiaomian*, Zhou Xiaobo, Tao Chengfang

Section One
27
A n important question in cardiology is, “Can cardiac sur-gery be carried out at high altitude in a hypoxic environ-ment?” The answer is yes, as we have carried out a large number of cardiac surgeries on the Tibetan plateau since
late 2000. Mild-hypothermia beating open heart surgery at high alti-tude, with the support of cardiopulmonary bypass, was shown to be possible when we performed the first cardiac surgery in the Tibet high altitude region (at 3,658 m) on November 10, 2000. Since then, we have performed a variety of open heart surgeries on the Tibetan plateau, including surgery for atrial septal defects, ventricular septal defects, tetralogy and trilogy of Fallot defects, transposition of great arteries, and valvular heart disease. The total success rate is approxi-mately 98.9%. Cardiac surgery at a high altitude involves a number of high altitude medical and hypoxia-related complications, which may undermine the surgical results and greatly increase the risks due to the severe hypoxic environment (1, 2). By carefully identifying the hypoxia problems and treating hypoxia-related symptoms cor-rectly, we have succeeded in almost all cardiac surgeries carried out at high altitude, which provides a basis for future advancement in high altitude surgery.
The average altitude of the Tibet plateau is above 4,000 m (3). In such a high altitude region, the severe hypoxic environment is charac-terized by a sharp fall in atmospheric pressure and a significant drop in partial pressure of atmospheric oxygen (4). Congenital heart disease is frequently encountered in this region and the incidence is approxi-mately two to three times that of the lowlands (5). Before 2000, doctors and patients were concerned about the incidence of congenital heart disease, mostly because cardiac surgery could not be performed in high-altitude regions at that time. Some children with severe congenital cardiac disease in remote areas died shortly after birth because of a lack of surgical treatment options. Since 2000, we have visited schools and villages annually throughout the high altitude region to screen for congenital heart disease among local children, and have provided free surgical treatment for affected children. We have also performed cardiac surgeries for a variety of non-congenital cardiovascular disor-ders, such as rheumatic valvular heart disease, with satisfying surgical treatment results.
Environmental hypoxia poses challenging problems for cardiac sur-gery at high altitude including severe hypoxemia, metabolic acidosis, and pulmonary artery hypertension. Even if the cardiac defects can be repaired, the environmental hypoxia can still lead to severe hypoxemia and a series of pathophysiological changes in the body (6). Chronic hypoxia can also lead to polycythemia, higher blood viscosity, and pulmonary hypertension secondary to pulmonary vasoconstriction and
Center for Prevention and Treatment of High Altitude Illness, Tibet General Hospital of PLA, Lhasa, Tibet, China.‡Contributed equally to this work.*Corresponding author: [email protected]
Cardiac Surgery on the Tibetan Plateau: From Impossible to SuccessfulLi Suzhià , Xie Xiaomianà ,*, Huang Yue, Liu Houdong, Yan Chuncheng, Zheng Bihai, Wu Qianjin, Huang Wenchao
remodeling of arterioles (1, 6). Therefore, patients were given high-flow oxygen via a face mask daily for seven days during the preop-erative stage to correct severe hypoxemia in the body. A 5% sodium bicarbonate solution was used preoperatively, intraoperatively, and postoperatively, by continuous intravenous drip, to correct metabolic acidosis of tissue cells. Sodium nitroprusside was used preoperatively and postoperatively to correct pulmonary hypertension and to decrease pulmonary pressure to a normal level. Hyperbaric oxygen was used if a patient had very severe pulmonary hypertension. Since myocardial pro-tection is very important in cardiac surgery performed at high altitude, mild-hypothermia beating open heart surgery was used in most cases, without aortic cross-clamping. Oxygen consumption of the slowly beating, empty heart decreased sharply (7–9). The operation schedule was simplified without perfusion of cold crystalloid cardioplegic solu-tions, myocardial damage was reduced, and cardiopulmonary bypass time and total operation time were shortened. All of these were impor-tant for myocardial protection and the success of cardiac surgery in a hypoxic environment.
REFERENCES 1. C. Sartori et al., N. Engl. J. Med. 346, 1631 (2002). 2. M. Maggiorini et al., Prog. Cardiovasc. Dis. 52, 500 (2010). 3. P. Tapponnier et al., Science 294, 1671 (2001). 4. A. J. Peacock, BMJ 317, 1063 (1998). 5. Q. H. Chen et al., Chin. Med. J. (Engl) 121, 2469 (2008). 6. C. Imraya et al., Prog. Cardiovasc. Dis. 52, 467 (2010). 7. A. Mo et al., Heart Lung Circ. 20, 295 (2011). 8. F. I. Macedo et al., Semin. Thorac. Cardiovasc. Surg. 23, 314 (2011). 9. D. F. Loulmet et al., Ann. Thorac. Surg. 85, 1551 (2008).
FigureÊ 1.Ê (A)Ê Doc-torsÊ screeningÊ forÊcongenitalÊ heartÊdiseaseÊ amongÊ lo-calÊ childrenÊ atÊ aÊprimaryÊ schoolÊ onÊtheÊ TibetanÊ plateau.Ê(B)Ê DoctorsÊ per-formingÊ aÊ mild-hy-pothermiaÊ beatingÊopenÊ heartÊ surgeryÊatÊ anÊ altitudeÊ ofÊ3,658Ê m,Ê withÊ theÊsupportÊ ofÊ cardio-pulmonaryÊ bypass

High-Altitude Medicine
28
T he Himalayas stretch over 2,400 km from east to west with a mean altitude over 6,000 m above sea level, and contain a large population that works and lives at a high altitude. Since July 2006, with the successful opening of the Qinghai-
Tibet railway, the highest railway in the world, increasing numbers of travelers have visited Lhasa and the Himalayan high-altitude regions. Environmental hypoxia has always presented medical challenges for the prevention, on-site rescue, and clinical treatment of acute moun-tain sickness (AMS) including acute mild altitude illness, high-altitude pulmonary edema (HAPE), and high-altitude cerebral edema (HACE).
AMS is induced or exacerbated by various causes including over-work, extreme cold, rapid ascent to a high altitude, alcohol consump-tion, psychological stress, acute respiratory infection, chronic mountain sickness (CMS), and cardiopulmonary diseases (1, 2). During the last 15 years, we have collected information on 19,118 cases of high-al-titude illnesses, and analyzed the relationship between the morbidity rates of all the types of AMS and CMS. The results suggested a high correction between these types of high-altitude illnesses (1). The mor-bidity rate of the AMS group (45.15%) and CMS group (17.40%) was significantly higher than that of the control group (4.02%), and the risk of AMS for people who had previously suffered from AMS or CMS was 11-fold or four-fold higher, respectively, than people who had not previously suffered from these disorders (3).
Through decades of epidemiological study on AMS on the Tibetan plateau, we have proposed a concept of systematic prevention of AMS in the Tibetan high-altitude region. This concept is intended to improve AMS prevention outcomes, and takes into account all elements and fac-
tors related to prevention, including the regions where AMS occurs, the current effective approaches for treatment, the various levels of preven-tative care, and the occasion when AMS is most likely to occur. The five aspects of the concept of systematic prevention are: (i) physicians specialized in high-altitude illnesses; (ii) grass-roots health workers; (iii) medical examinations before entering high altitude; (iv) dissemina-tion of knowledge to the populace; and (v) prophylactic medications for the prevention of AMS (4). Since inception of this systematic preven-tion strategy, the total incidence of AMS decreased significantly from 50%–60% to 2%–3%, and the total rate of successful rescue increased from 85.5% to 99.7% (5, 6). In our practice of treatment of AMS, we have greatly improved treatment outcomes by clinical application of the most effective medications and methods, and have also developed early-stage diagnostic criteria and standardized treatment regimens to decrease mortality and increase the rate of successful rescue of severe acute high-altitude illnesses (7).
This comprehensive, multilevel prevention system for AMS, the re-sult of over 15 years of epidemiological research, has resulted in sig-nificant medical progress and dramatically improved quality of life for many people arriving in the Tibetan plateau region.
REFERENCES1. Y.Huanget al., J. Epidemiol. (Chinese) 24, 74 (2003). 2. S. Z. Li et al., Medical Journal of National Defending Forces in
Southwest China 21, 269 (2011). 3. X. W. Huang et al., Medical Journal of National Defending Forces in
Southwest China 19, 1072 (2009). 4. L. Pan et al., High Alt. Med. (Chinese) 17, 32 (2007). 5. X. W. Huang et al., Medical Journal of National Defending Forces in
Southwest China 18, 11 (2008). 6. T. S. Xie et al., Journal of Military Surgeon in Southwest China 10, 9
(2008). 7. S. Z. Li et al., PeopleÕ s Military Surgeon (Chinese) 52, 97 (2009).
Acute Mountain Sickness on the Tibetan Plateau: Epidemiological Study and Systematic PreventionLi Suzhi, Huang Xuewen, Huang Yue, Liu Houdong, Yan Chuncheng, Zheng Bihai, Zheng Jianbao, Xie Xiaomian*
Center for Prevention and Treatment of High Altitude Illness, Tibet General Hospital of PLA, Lhasa, Tibet, China.*Corresponding author: [email protected]

Section One
29
Since an American immunologist developed the theory of erythrocyte immunology in the early 1980s, great progress has been made in this field (1, 2). Erythrocytes are able to recognize, adhere to, and destroy antigens, and can eliminate
immune complexes (2). Moreover, erythrocytes play a role in immune regulation in the body, constituting a subsystem of the immune system (3). To elucidate the role of erythrocyte immunology in the mechanisms of human acclimatization to high altitude and the its effect on acute mountain sickness (AMS), we have researched the characteristics of erythrocyte immunologic function in people who rapidly ascended to high altitudes, as well as the gastrointestinal mucosa barrier function in people and rabbits afflicted with acute anoxia at high altitudes.
Changes in Erythrocyte Immune Function by Rapid Ascent to High AltitudeThe erythrocyte C3b receptor rosette (E-C3bRR) and erythrocyte im-mune complex rosette (E-ICR) levels were monitored and analyzed in 40 low-altitude natives who rapidly ascended to high altitude (3,600 m) by airplane (test group), as well as in 36 low-altitude natives living at high altitude and 30 high-altitude natives living at the same high altitude who had not experienced a recent ascent (controls). In the test group, E-C3bRR levels decreased sharply while E-ICR levels increased dramatically after they arrived at the high altitude. E-C3bRR and E-ICR levels recovered gradually to the levels of the controls in 30 days, indicating that AMS correlates with impaired erythrocyte immune function and improving erythrocyte immune function before rapid as-cent to high altitudes may reduce the incidence of AMS (3). In another study, E-C3bRR and E-ICR levels in 36 high-altitude natives who rap-idly ascended to high altitude after a long stay at low altitude were also monitored and analyzed. The E-C3bRR levels decreased, while E-ICR levels increased, after they arrived at high altitude, but the magnitude of changes in E-C3bRR levels and E-ICR levels was significantly less than that of the low-altitude natives test group mentioned above. The results indicated that high-altitude natives have an advantage in their
adaptation to high-altitude hypoxia, which is possibly related to eryth-rocyte structure, erythrocyte immune function, and hereditary factors as well (4, 5).
Gastrointestinal Mucosa Barrier Function Is Impaired by Rapid Ascent to High AltitudeBy noting the digestive symptoms of 1,753 individuals who rapidly ascended to high altitude, we observed that 1,097 individuals (62.58%) suffered different degrees of gastrointestinal disorders. Gastroscopic examinations in 20 individuals afflicted with acute anoxia showed slow peristalsis (60%), bile reflux (50%), and mucosal damage (85%) (6). Significant changes in gastrointestinal hormones, inflammatory mediators, and oxygen free radicals after the rapid ascent to high altitude were found (7). In another study, electron microscope analysis of small intestinal mucosa from rabbits exposed to anoxia identified damage to the small intestinal villi with leakage of fibrin and erythrocytes. The activity and concentration of the serum diamine oxidase (DAO) and malondialdehyde (MDA) in rabbits at high altitude were higher than those in the control group remaining at low altitude. However, the activity and concentration of small intestinal mucosal DAO, glutamine, serum superoxide dismutase, nitric oxide, and glutamine decreased under anoxic conditions when compared with the control group (7, 8).
Taken together, these results indicate that rapid exposure to a hypoxic environment causes secondary reduction of erythrocyte immune func-tion and damage of gastrointestinal mucosal barrier function. Improv-ing erythrocyte immune function and protecting gastrointestinal muco-sal function may be of clinical importance in reducing the incidence of high-altitude diseases and improving treatment regimens.
REFERENCES 1. L. Siegel et al., Lancet 2, 566 (1981). 2. F. Guo, Immunological Journal (Chinese) 6, 60 (1990). 3. Q. G. Shi et al., Immunological Journal (Chinese) 11, 178 (1995). 4. Q. G. Shi et al., Southwest Defense Journal of Medicine (Chinese) 10,
303 (2000). 5. Q. G. Shi et al., High Alt. Med. (Chinese) 10, 11 (2000). 6. S.Z. Li et al., Occupational Health (Chinese) 27, 427 (2011). 7. S.Z. Li et al., South Military Medical Journal (Chinese) 25, 273 (2011). 8. B.H. Zheng et al., South Military Medical Journal (Chinese) 25, 4 (2011).
Center for Prevention and Treatment of High Altitude Illness, Tibet General Hospital of PLA, Lhasa, Tibet, China.*Corresponding author: [email protected]
Study on Erythrocyte Immune Function and Gastrointestinal Mucosa Barrier Function After Rapid Ascent to High AltitudeShi Quangui, Li Suzhi*, Zheng Bihai

High-Altitude Medicine
30
T he physiological function, tissue structure, and biochemi-cal metabolism of native high-altitude plateau athletes show adaptive changes to hypoxia environments when compared with low-altitude plain athletes undergoing an identical train-
ing load and intensity (1). In competitive sports, especially endurance events, athletes living in plateau and mountain areas of China (at 2,000 to 3,000 m) have achieved great success. Thus, studies on altitude train-ing of plateau athletes may have a positive effect on athletic training in general.
The “high-high” training method, besides training in a high-altitude region and living in a low-altitude region, also makes use of other ben-eficial effects of the plateau, while avoiding the disadvantages. Han et al. (1) determined that athletes who had lived and trained at an altitude of 1,900–2,000 m for many years could readily cope with training at 2,500 to 3,400 m three to four times a week. Liu et al. (2) described the advantages of alternative altitude training: 35 days at an elevation of 2,260 m, 28 days at 396 m, then altitude training for 22 days at 2,260 m. Both the high-high training and the alternative altitude train-ing methods had positive effects on the physiological function and ath-letic capacity of subjects. Ma et al. (3) did research on seven native female middle-distance runners who undertook six weeks of intermit-tent altitude training between 2,260 m and 3,150 m. They found that the cardiopulmonary function, VO2 max (peak oxygen uptake), anaero-bic threshold speed, and hemogram of the runners showed significant improvement when they training at the higher altitude (3,150 m) after training at 2,260 m, which indicated that their aerobic capacity had im-proved. However, when the native athletes arrived at low altitude after intermittent attitude training, their movement ability and some exercise physiology indexes were negatively impacted compared with the native plain athletes and non-altitude training athletes. As a result of these dif-ferences, defining the time that athletes might reach their peak competi-tion fitness was challenging. Li et al. (4) compared the effect of training at high altitude on the Chinese plateau with the same on the Japanese plains. The results showed that for better physiological function and performance it is necessary to train at an altitude of 3,200 m for a short
period. Additionally, race walkers in Mexico, at an altitude of 2,300 m, developed an alternative altitude training method that has allowed them to become world leaders in the sport (5).
In 1991, Levine (6) first proposed a particular “live high, train low” (Hi-Lo) method where athletes lived at a higher elevation to encourage the body to adapt to high-altitude hypoxia environment. This allowed athletes to achieve a larger training load and intensity in a low elevation zone. It was observed that native plateau athletes undergoing intermit-tent hypoxic training at 4,000 m failed to stimulate the kidney to release erythropoietin, while the responses of vascular endothelial growth fac-tor (VEGF) were more sensitive. This response suggests that improved muscle capillarization rather than increased red blood cell production would be a major adaptation to intermittent hypoxic training. Running at an altitude of 3,000 m resulted in increased erythropoietin release in the hypoxia group, but not in the control group.
Through the theory and practice of altitude training both at home and abroad, most research has shown some benefit in improving the performance of athletes worldwide and, in particular, of native plateau athletes. Studies are rare in the areas of optimal elevation for altitude training, the training time needed to achieve the most benefit, the tim-ing of performance peaks following altitude training, and physiological changes during altitude training. Although consensus on some of the major issues of altitude training has been reached, there are many un-answered questions, especially regarding the best altitude training regi-mens, the ideal training load and intensity, pre-altitude training prepa-ration, optimal altitude training time pre-competition, and the specific focus on strength, speed, aerobic, and anaerobic qualities.
Further studies will be valuable for improving athlete performance and will also have positive effects on developing individualized altitude training protocols for native plateau athletes. Additionally, such studies can provide a scientific basis for coaches to determine the ideal duration and intensity of training to capitalize upon the beneficial altitude train-ing effects discussed above.
REFERENCES 1. Z. Han et al., Track and Field 6, 25 (1995). 2. Z. Liu et al., Sports Science 6, 34 (1999). 3. F. Ma et al., Sports Science 6, 34 (2000). 4. H. Li et al., Sports Science 5, 30 (1995).5. Y. Shang et al., Sports Science 3, 11 (1996).
6. B. D. Levine. High Alt. Med. Biol. 3, 177 (2002).
Basic Methods and Application of Altitude Training on the Chinese PlateauMa Fuhai*, Fan Rongyun, Yu Xiaoyan, He Yingying
Qinghai Institute of Sports Science, Xining, Qinghai, China.*Corresponding author: [email protected]

Section One
31
T he Qinghai-Tibet Plateau is a natural laboratory for mountain sickness research, especially cerebral hypoxic/ischemic tol-erance, because its unique geographic environment (alpine, hypobaric, and hypoxic climate) results in a complex succes-
sion of pathophysiologic alterations. When exposed to hypoxia at high altitudes, the brain initiates autoregulation of blood flow, formation of collateral circulation, and preservation of metabolism, to maintain
Hypoxic Preconditioning at High Altitude Improves Cerebral Reserve CapacityWu Shizheng1,*, Zhang Shukun1, Chang Rong1, Li Na1, Wu Yao-An2, Feng Yuliang3, Wang Yigang3
FigureÊ 1.Ê (A),Ê PhaseÊ contrastÊ imageÊ ofÊ HUVECsÊ atÊ 24Ê hoursÊ ofÊ hypoxicÊtreatmentÊ showingÊ roundingÊ upÊ andÊ shrinkageÊ ofÊ cellsÊ withÊ non-hypoxicÊ preconditioningÊ (non-HPC),Ê whichÊ wasÊ preventedÊ byÊ hypoxicÊpreconditioningÊ (HPC).Ê (B),Ê QuantitativeÊ analysisÊ ofÊ TUNELÊ positivityÊshowingÊ decreasedÊ numbersÊ ofÊ TUNEL+Ê nucleiÊ inÊ HPCHUVECsÊ (*p<0.01ÊversusÊ normoxiaHUVECs,Ê #p<0.05Ê versusÊ non-HPCHUVECs).Ê (C,Ê D)Ê QuantitativeÊanalysisÊ ofÊ RT-PCRÊ showingÊ thatÊ expressionÊ ofÊ Ang-2Ê (C)Ê andÊ VEGFÊ (D)Êwas significantly elevated in HPCHUVECsÊ (*p<0.01Ê versusÊ normoxiaHUVECs,Ê#p<0.05Ê versusÊ non-HPCHUVECs).Ê AllÊ valuesÊ expressedÊ asÊ meanÊ ±Ê SEM,ÊnÊ =Ê 8Ê forÊ eachÊ group.Ê (E)Ê HeatÊ mapÊ ofÊ miRNAÊ microarrayÊ showingÊ theÊenrichmentÊ ofÊ angio-miRsÊ inÊ HPCHUVECs.Ê (F,Ê G)Ê GraphÊ showingÊ thatÊ theÊpercentage of cells positive for Bcl-2 (F) and NGB (G) was significantly higherÊ inÊ HPCHUVECsÊ (*p<0.01Ê versusÊ normoxiaHUVECs,Ê #p<0.05Ê versusnon-HPCHUVECs).Ê AllÊ valuesÊ expressedÊ asÊ meanÊ ±Ê SEM,Ê nÊ =Ê 10Ê forÊ eachÊgroup.Ê (H,Ê I)Ê QuantitativeÊ analysisÊ ofÊ RT-PCRÊ showingÊ Bcl-2Ê (H)Ê andÊ NGBÊ(I) expression was significantly elevated in HPCHUVECsÊ (*p<0.01Ê versusnormoxiaHUVECs,Ê #p<0.05Ê versusÊ non-HPCHUVECs).Ê AllÊ valuesÊ expressedÊasÊ meanÊ ±Ê SEM,Ê nÊ =Ê 6Ê forÊ eachÊ group.Ê NOR,Ê normoxia;Ê non-HPC,Ênon-hypoxicÊ preconditioning;Ê HPC,Ê hypoxicÊ preconditioning;Ê GAPDH,ÊglyceraldehydeÊ 3-phosphateÊ dehydrogenase.
1Qinghai Provincial People’s Hospital, Xining, China; 2The University of York, York, UK; 3Department of Pathology and Laboratory Medicine, University of Cincinnati, Cincinnati, OH, USA.*Corresponding author: [email protected]
normal blood flow and avoid impairment of cerebral reserve capacity induced by hypoxia/ischemia (1). Cerebral reserve capacity describes the ability to maintain adequate blood flow in the face of decreased perfusion pressure and oxygen supply. It has been identifi ed as the ma- and oxygen supply. It has been identifi ed as the ma-supply. It has been identifi ed as the ma-supply. It has been identifi ed as the ma-y. It has been identified as the ma-jor predictive indicator for the risk of subsequent cerebral infarction. It has been previously reported that repeated, short episodes of hypoxic preconditioning protect the brain against subsequent hypoxic insult (2). Over the past few years, we have investigated the effect of hypoxic preconditioning at high altitudes. Using an in vitro hypoxic model con-sisting of Human Umbilical Vein Endothelial Cells (HUVECs), phase contrast microscopy revealed a hypercontracted morphology of nonhy-
poxic preconditioned HUVECs (non-HPCHUVEC, at 37ºC, 1% O2 + 5% CO2 + 94% N2) whereas restored morphology was observed in hypoxic preconditioned HUVECs (HPCHUVEC, at 37ºC, 1% O2 + 5% CO2 + 94% N2 for 30 min). Following hypoxic treatment, the viability of non-HPCHU-VECs was reduced by 40%, 52%, and 59% at 8, 12, and 24 hours, respectively, compared to HPCHUVECs (25% at 24 hours). Furthermore, terminal deoxynucleotidyl transferase dUTP nick end labeling (TU-NEL) positivity, which measures the incidence of apoptosis, was mark-edly decreased in HPCHUVECs (15.2%) compared with non-HPCHUVECs

High-Altitude Medicine
32
(25.3%), but was higher than the NormoxiaHUVECs (4.3%, at 37ºC, 5% CO2), implying that hypoxic preconditioning can elicit cytoprotection against hypoxic stress. Reverse transcription polymerase chain reaction (RT-PCR) analysis demonstrated significant upregulation of vascular endothelial growth factor (VEGF) and angiopoietin (Ang)-2 in non-HP-
CHUVECs compared with NormoxiaHUVECs, and even greater increases in HPCHUVECs. VEGF and Ang-2 are mediators in angiogenesis and formation of collateral circulation (3). Our microRNA microarray data identified a cluster of angiogenesis-related microRNAs (angio-miRs) that are significantly enriched in HPCHUVECs (unpublished data). Simi-(unpublished data). Simi-. Simi-larly, hypoxic preconditioning could protect cultured neonatal neurons (NN) against lethal hypoxic insult as determined by TUNEL positivity: 1.1% in NormoxiaNN, 44.1% in non-HPCNN, and 9.8% in HPCNN (4). mRNA and protein levels of Bcl-2 and neuroglobin (NGB) were also signifi-cantly upregulated in HPCNN. This implied that coordination between the critical anti-apoptotic protein Bcl-2 (5) and oxygen carrying protein NGB (6) was involved in the significant improvement of neuronal sur-vival and cerebral reserve capacity (Figure 1).
To verify our hypothesis in vivo, 180 healthy Wistar rats were divided into three groups at different altitudes: Xining group, 2,260 m above sea level; Qaidam group, 3,500 m; Tuotuo River group, 4,500 m. All groups were placed at their specific altitude for 30 days to induce acclimatization, after which middle cerebral artery occlusion (MCAO) was induced. Immunohistochemistry of cerebral tissues on days 1, 3, 7, and 14 after cerebral infarction showed that the presence of apoptosis-stimulating protein 1 of p53 (ASPP1), a key proapoptotic protein, was decreased in the Qaidam group, relative to the others (Figure 2) (7). This
indicated that hypoxia is a proverbial “double-edged sword,” for which and an appropriate level of hypoxia can reduce apoptosis and increase cerebral reserve capacity, but severe hypoxia had no such effect.
Cerebrovascular reactivity (CVR) is a physiological characteristic of brain arteries to alter their size in response to a vasoactive stimulus.Impaired CVR is a predictive factor of imminent stroke. In a clinical study, CVR was examined using transcranial doppler technology in patients with symptomatic stenosis of the anterior intracranial artery, and compared with that in normal healthy individuals living permanently in the Xining area (2,260 m). CVR was significantly reduced in patients with anterior artery stenosis compared with the normal control. Moreover, multivariate stratified analysis revealed that patients with symptomatic anterior circulation artery stenosis had a greater reduction in CVR compared with the asymptomatic patients at the same altitude. In symptomatic patients, CVR of the stenosis side was reduced as compared with the non-stenosis side. Furthermore, we found CVR positively correlated with serum levels of nitric oxide (NO), Na+/Ca2+
exchanger type-1 (NCX1), and granulocyte colony-stimulating factor, all of which correlate with the risk of stroke, indicating its potential value for the early detection of cerebral infarction.
Interestingly, we observed that administration of butylphthalide and Mailuoning (a Chinese herbal medicine) could increase cell viability and reduce apoptosis by activating the same signaling molecules (VEGF and Ang-2) as those observed in hypoxic preconditioning. Thus, these drugs might be potential preconditioning agents that can stimulate the biochemical pathways of hypoxic preconditioning and therefore protect vascular endothelial functions (8, 9).
Taken together, our in vitro and in vivo experiments, combined with the clinical study, demonstrated that hypoxic preconditioning at high altitudes by intermittent exposure to hypobaric condition improved cerebral reserve capacity, and structural and functional restoration of the brain upon return to normoxia or low altitude. Investigating the characteristics of CVR and cerebral autoregulation in populations liv-ing at different altitudes to identify the underlying mechanisms of the formation of collateral circulation and hypoxic/ischemic tolerance may provide novel insights for stroke prevention. Thus, intermittent and op-timal hypoxic preconditioning by intermittent exposure to high altitude might be a new paradigm for neuroprotection and restoration of cere-bral reserve capacity in patients with ischemic stroke.
REFERENCES 1. H. Zhou, G. M. Saidel, J. C. LaManna. J. Adv. Exp. Med. Biol. 614, 371
(2008). 2. S. Z. Wu, Chin. J. Stroke 2, 965 (2007). 3. Z. G. Zhang et al., J. Cereb. Blood Flow Metab. 22, 379 (2002). 4. G. L. Rong, S. Z. Wu. Chin. J. New Drug 21, 06 (2012). 5. Z. M. Ding et al., Int. J. Mol. Sci. 13, 6089 (2012). 6. E. Fordel et al., IUBMB Life 56, 681 (2004). 7. J. Cheng, S. Z. Wu, S. K. Zhang. Chin. J. Pract. Prev. Med. 18, 04
(2011). 8. G. L. Rong, S. Z. Wu, S. K. Zhang. Chin. J. New Drug 20, 1015 (2011). 9. L. Na, S. Z. Wu, S. K. Zhang. Chin. J. New Drug 21, 06 (2012).
ACKNOWLEDGMENTSThis work was supported by grants from the Qinghai Provincial High Altitude Medicine Science Research Programs (Grant No. 200908-01 and 201111-01) and National Institutes of Health (Grant No.HL089824 and HL110740; YigangWang).
FigureÊ 2. Immunohistochemical quantification in cerebral tissues on daysÊ 1,Ê 3,Ê 7,Ê andÊ 14Ê afterÊ cerebralÊ infarctionÊ showedÊ downregulationÊ ofÊASPP1Ê expressionÊ inÊ theÊ QaidamÊ groupÊ (3,500Ê m)Ê comparedÊ withÊ theÊXiningÊ groupÊ (2,260Ê m)Ê andÊ TuotuoÊ RiverÊ groupÊ inÊ chronologicalÊ orderÊ(4,500Ê m)Ê (*p<0.01Ê versusÊ XiningÊ orÊ TuotuoÊ RiverÊ Group).Ê AllÊ valuesÊexpressedÊ asÊ meanÊ ±Ê SEM,Ê nÊ =Ê 60Ê forÊ eachÊ group.Ê

Section One
33
T ibetans have inhabited the Tibetan plateau for approximately 25,000 years and appear to be well adapted to high altitudes with higher arterial oxygen saturation, low incidence of chronic mountain sickness, and minimal hypoxia pulmonary
hypertension (1). We feel that it is important to better understand the damage caused by chronic hypoxia and the mechanisms of human ad-aptation to high-altitude environments through studying the impact of high-altitude environment on native Tibetans.
At high altitudes, changes in the cardiovascular system are necessary in order to transport sufficient oxygen to tissues to help the body adapt to low oxygen environments. We have previously assumed that there was a certain dynamic balance between adaptation of, and damage to, the cardiovascular system in high-altitude environments. When this balance is altered, the incidence of various cardiovascular problems—including arrhythmia, high blood pressure, pulmonary hypertension, and coronary artery disease—increases. Our early research (2) showed that the mean heart rate of Tibetans in the Lhasa area (3,658 m) over a 24 hour period was 71 beats per minute, significantly lower than the 87 beats per minute observed in Han Chinese individuals at the same alti-tude. Additionally, the prevalence of bradycardia (slowing of the heart, which reduces myocardial oxygen consumption, increases stroke vol-ume, and improves the mechanism of adaptability to an anaerobic envi-ronment) was increased in healthy Tibetans in the Lhasa area. However, the low heart rate could also increase the incidence of cardiac events such as angina and, in the most serious cases, cardiac arrest. Further studies indicated that the sinus nodal recovery time, sinus atrial conduc-tion time, and corrective sinus nodal recovery time were much longer in healthy Tibetans at high altitude than in Han individuals at sea level. This suggests that the direct influence of high-altitude–related hypoxia on the sinus node and adjustment of the sympathetic nervous system has reached a certain balance, which increases the adaptability of Tibet-ans to high-altitude environments.
Systemic Blood PressureHigh-altitude environments cause a significant change in the cardiovas-cular system including the increased occurrence of pulmonary hyper-tension (3). We performed right heart catheterization in healthy Tibet-ans living in Lhasa and found that the mean pulmonary arterial pressure was similar to that of individuals at sea level. Pulmonary hypertension was uncommon among these individuals, because native Tibetans have shown great adaptability to high-altitude environments. However, stud-ies on systemic blood pressure in hypoxic environments are relatively rare. A study from Peru showed the prevalence of hypertension was greater at sea level than at high altitude (4). This does not appear to hold true in Tibet. The results of a hypertension survey that we conducted in 1991 showed that native Tibetans have the highest prevalence of hyper-tension (5). The incidence of stroke in Tibet was the highest in China according to a national survey and a recent epidemiological survey of stroke in Lhasa performed by our group demonstrated that hypertension
Department of High Altitude Sickness, People’s Hospital of Tibet Autonomous Region, and the Tibet Institute of High Altitude Medicine, Lhasa, Tibet, China.Corresponding author: [email protected]
was the primary risk factor among Tibetan patients (6). Therefore, hy-pertension is a significant health hazard for Tibetan plateau natives. Be-sides genetic factors, high-altitude–related hypoxia may also be a risk factor. Although the adaptability of native Tibetans influences pulmo-nary circulation, further effort is required to find a relationship between the high morbidity rate of hypertension and adaptability to high-altitude environments.
Coronary Artery Disease (CAD)Acute hypoxia increases coronary blood flow in direct proportion to the reduction in arterial oxygen concentration. Conversely, coronary blood flow is reduced in permanent residents of high altitudes in Peru com-pared with people at sea level. Few data exist that quantify adverse car-diac events at high altitudes although some studies showed that casts of the coronary vessels had a greater density of peripheral branching than those of sea level controls, perhaps explaining the relatively lower in-cidence of angina and myocardial ischemia in the Peruvian population (4). However, it remains unclear to what degree hypoxia impacts the process of coronary artery disease (CAD) at high altitudes, and whether it is safe for patients with CAD to travel to high altitudes.
As the regional infrastructure has developed rapidly, it is more con-venient for people to enter high-altitude regions. Official statistics show that more than 8.6 million people entered the Tibet region in 2011 (7). Thus, it is crucial to evaluate the risk of cardiac events for travelers to Tibet, in order to provide more precise prevention plans and to deter-mine whether the high-altitude environment might have a positive or negative effect on those with CAD.
We have studied the status of CAD in native Tibetans to determine the relationship between hypoxia and CAD. In 1977, our study reported a 66.9% incidence rate of coronary atherosclerosis in Lhasa residents, and a 12% incidence of ischemia-like electrocardiogram changes or coronary insufficiency, as determined by a positive exercise test (8). With the rapid development of the Chinese economy, the population’s dietary habits have changed greatly and risk factors for CAD have in-creased in concert with the increase in patients with dyslipidemia and diabetes. From 1986 to 2003, the portion of the in-hospital patients with CAD increased from 4.33% to 9.1% and acute myocardial infarction was found to be the main reason for hospitalization (9). The fatality rate in this group was 28.5%. In Tibetan patients with CAD, the left anterior descending artery was most commonly involved, followed by the right coronary artery and then the left circumflex; however, the left main coronary artery was involved to a lesser degree (10). The distri-bution of atherosclerotic lesions did not differ from sea level patients.
The Dynamic Balance Between Adaptation and Lesions of the Cardiovascular System in Tibetans Living at High AltitudeGesang Luobu

High-Altitude Medicine
34
We speculated that the adaptation to high altitude, including decreased heart rate and reducing oxygen consumption, might induce the onset of angina pectoris and acute myocardial infarction in Tibetans. As the inci-dence rate of dyslipidemia (11) and diabetes increases (12), the balance between the advantages of adaptation and resulting increase in athero-sclerotic lesions may be altered. This hypothesis is supported by the observation that large numbers of Tibetan in-patients have acute myo-cardial infarction (9). It is not uncommon for native Tibetans to suffer from CAD. Studying CAD in the Tibetan population not only helps to identify possible risk factors, but it also helps to reveal the mechanism of CAD, and to aid in the development of novel prevention methods.
Genetic ResearchResearch initiated by our group and the University of Colorado School of Medicine in the United States found that native Tibetan newborns had higher arterial oxygen saturation at birth and during the first four months of life than Han Chinese newborns. Additionally, healthy Tibet-an’s resting pulmonary arterial pressure was normal by sea-level stan-dards and they exhibited minimal hypoxic pulmonary vasoconstriction. This implied that the Tibetan adaptation to high altitudes had a genetic basis. In 2010, in cooperation with the company BGI-Shenzhen, we found that the frequency of one single nucleotide polymorphism in the endothelial Per-Arnt-Sim (PAS) domain-containing protein 1 (EPAS1) gene differed in frequency between Tibetans and Han Chinese by 78%, providing strong genetic evidence for high altitude adaptation in Ti-betans (13). Besides traditional risk factors such as dietary habits and smoking, interactions between hypoxia and genetic factors may play a significant role in the etiology of hypertension in Tibetans. Our research showed a significant association between the D allele of the angioten-sin-converting enzyme gene and hypertension in Tibetans, and the fre-quency of the G allele was significantly higher in hypertensive than in normotensive Tibetans, but not Han Chinese (14). Thus, we speculate
that the increased incidence of hypertension among native Tibetans may be due to interactions between hypoxia and genetic factors, which helps us to further understand the mechanism involved in the adaptation of native Tibetans to high-altitude environments, as well as how these mechanisms manifest clinically.
SummaryIt is well documented that Tibetans are adapted to high altitudes. How-ever, they also suffer from cardiovascular system damage caused by hypoxia. We speculate that the increased economic activity and im-provement in living standards in China will greatly affect the balance between adaptation and cardiovascular problems in Tibetans at high altitude. Insight into this balance might be helpful to better treat the Tibetan population as well as understand the basis of human adaptation to hypoxia.
REFERENCES 1. T.Y.Wu. High Alt. Med. Biol. 5, 1 (2004).2. L. H. Yang et al., Tibet J. Med. 22, 1 (2001).
3. A. L. Baggish et al., High Alt. Med. Biol. 11,139 (2010). 4. J. B. West, R. B Schoene, J. S Milldge, in High Altitude Medicine and
Physiology, (Hodder Arnold, London, ed. 3, 2007), pp. 93-94. 5. Y. C. Hu et al., J. Hygiene Res. 35, 5 (2006).6. Y.H.Zhaoet al., Stroke 41, 2739 (2010). 7. http://www.chinatibetnews.com/xizang/node-9151.htm. 8. W. J. Cen et al., Tibet Hygiene 5,4 (1977). 9. L. B. Gesang et al., Tibet J. Med. 25, 80 (2004).10 C. R. Dawa et al., Chinese Circ. J. 27, 3 (2012).11 K. Li et al., Med. J. West. China 24, 3 (2012).12 L.H.Yanget al., Chin. J. Endocrinol. Metab. 19, 5 (2003).13 X. Yi et al., Science 329, 75 (2010).14 L. B. Gesang et al., Hypertens. Res. 25, 3 (2002).
1Department of High Altitude Diseases, Golmud People’s Hospital, Golmud, Qinghai, China; 2Department of Critical Care Medicine, Qinghai Province Hospital, Xining, Qinghai, China;3Research Center for High Altitude Medicine, Qinghai University Medical College, Xining, Qinghai, China; 4Qinghai Traffic Hospital, Xining, Qinghai, China.*Corresponding author: [email protected]
Establishment of an Improved Bundle Therapy Procedure for Acute High-Altitude DiseaseZhang Xuefeng1,*, Ma Si-Qing2, Jin Guoen3, Pei Zhiwei1, Guo Zhijian4
F or many years, the acute high-altitude diseases, pulmonary edema (HAPE) and cerebral edema (HACE), did not have standard treatment procedures. Over the last 30 years, we have continually improved the normal treatment programs and es-
tablished an improved bundle therapy strategy for acute high-altitude diseases (Figures 1 and 2).
Patients suffering from high-altitude disease (n=203), including 181 males and 22 females with a mean age of 33.64 ± 11.40 years, from different regions in the Tibetan Plateau (3,000 to 5,130 m above sea level) were selected in a prospective study. All patients were treated in Golmud (2,800 m). Diagnoses were in line with HAPE and HACE diagnostic criteria of the Chinese Medical Association Third National High Altitude Medicine Symposium (1). Cases were selected by a ran-dom number table and divided into a bundle scheme therapy group (125 cases) and a control group receiving ordinary therapy (78 cases).
HAPE diagnostic criteria were as follows. First phase (light edema): changes in interstitial lung edema determined by X-ray; secondary phase (medium edema): X-ray changes in the occurrence of unilat-eral lung edema; third phase (heavy edema): bilateral interstitial lung edema determined by X-ray; fourth phase (extremely heavy edema):

Section One
35
TableÊ 1. Ê ComparisonÊ ofÊ therapeuticÊ effectsÊ onÊ acuteÊ severeÊ high-altitudeÊ sickness.
Group Number of Cases
Hospitalization time in Days
(mean ± SD)Percentage Cured (No.) Percentage Mortality (No.)
Bundle therapy group 125 5.28 ± 3.17* 96.80 (121)* 3.20 (4)*Control group 78 6.94 ± 4.05 89.74 (70) 10.26 (8)
*p<0.05 compared with the control group.
TableÊ 2.Ê ComparisonÊ ofÊ therapeuticÊ effectsÊ onÊ acuteÊ high-altitudeÊ sickness.
Group Degree of Edema Number of Cases
Number of deaths Percentage Mortality
Bundle therapy group light/medium 50 0 0heavy 55 1 1.28
extremely heavy 20 3 15Control group light/medium 38 0 0
heavy 27 2 7.41
extremely heavy 13 6 46.15
congestive heart failure (CHF), respira-tory failure, acute respiratory distress syn-drome (ARDS), and multiple organ dys-function syndrome (MODS) (2). HACE staging and classification were based on all cases according to the diagnostic cri-teria as follows. First phase (light edema): no significant change in X-ray and com-puted tomography (CT) exam; secondary phase (medium edema): CT showed mild cerebral edema and shallow sulci; third phase (heavy edema): CT showed large areas of low density and disappearance of the gyrus and ambient cistern; fourth phase (very heavy edema): CHF, respira-tory exhaustion, ARDS, and MODS. There was no statistically significant difference (p>0.05) in age, height, weight, altitude, blood pressure, heart rate, respiratory rate, other physiological parameters by balanc-ing tests, or incidence of light, medium, heavy, or extremely heavy cerebral edema and pulmonary cerebral edema between the two groups before treatment.
The two groups were administered rest, oxygen, conventional hormone treatment, theophylline, vasoactive drugs, rehydra-tion, and hyperbaric oxygen. The types of general therapy used for the control group were not determined based on patient stag-ing and classification whereas the bundle therapeutic group was treated according to staging and typing. Results showed that mortality and number of days in hospital were decreased while the total cure rate in-creased (Tables 1 and 2) when the bundle therapy approach was used.
REFERENCES1. T.Y.Wu, J. High Alt. Med. 17, 3 (1995). 2. W. Wei et al., J. Fourth Military Medical University 26, 363 (2005).
ACKNOWLEDGMENTSThis work was supported by the Project of Qinghai Province Science and Technology Program (Grant No. 2011-N-150).
TheÊa boveÊ resultsÊ suggestÊ thatÊ weÊ haveÊ developedÊ anÊ improvedÊ bundleÊ therapyÊ strategyÊ forÊ acuteÊ high-altitudeÊ diseases.Ê However,Ê furtherÊ ÊworkÊ isÊr equired.
FigureÊ 1.Ê BundleÊ therapyÊ strategyÊ forÊ high-altitudeÊ pulmonaryÊ edemaÊ (HAPE).
a:Ê rest;Êb :Êh ighÊ pressureÊ oxygen;Ê c:Ê 654-2;Ê d:Ê respirator;Ê e:Ê intensiveÊ careÊ unit.ARDS,Êa cuteÊr espiratoryÊ distressÊ syndrome;Ê MODS,Ê multipleÊ organÊ dysfunctionÊ syndrome.
FigureÊ 2.Ê BundleÊ therapyÊ strategyÊ forÊ high-altitudeÊ cerebralÊ edemaÊ (HACE).
a:Ê rest;Êb :Êh ighÊp ressureÊ oxygen;Ê c:Ê 654-2;Ê d:Ê respirator;Ê e:Ê intensiveÊ careÊ unit;Ê f:Ê reduceÊ intracranialÊ pressure.ÊARDS,Êa cuteÊr espiratoryÊ distressÊ syndrome;Ê MODS,Ê multipleÊ organÊ dysfunctionÊ syndrome;Ê CT,Ê computedÊtomograpy.

High-Altitude Medicine
36
T he plateau zokor (Myospalax baileyi) and plateau pika (Ochotona curzoniae) are specialized rat species found on the Qinghai-Tibet plateau. Plateau zokor is a blind subterranean mole rat that spends its life underground in sealed burrows
(1). During the spring, summer, and autumn, the oxygen content in their burrow at a depth of 18 cm was found to be 18.02%, 17.04%, and 18.43%, respectively, and the carbon dioxide level was 0.22%, 1.46% and 0.81%, respectively (2). Plateau pika, which is a member of the genus Ochotona of the Ochotonidae family, is a small, nonhibernating rodent that lives in remote mountain areas at an elevation of 3,000 to 4,800 m (3). Both the zokor and pika have evolved a series of physio-logical adaptations that allow them to thrive in a hypoxic environment.
Both rodents have bigger lungs, a higher density and smaller area of pulmonary alveoli, a thinner air-blood barrier and microvessel muscle, higher red blood corpuscle counts, and lower hematocrit and mean cor-puscular volume than normal rats (4). The oxygen pressure in zokor is about 1.5-fold higher than pika in arterial blood, but only 0.36-fold that of pika in venous blood. Partial pressure for carbon dioxide in arterial and venous blood of zokor is 1.5-fold and 2.0-fold higher, respectively, than in pika, while oxygen saturation of zokor is 5.7-fold lower in ve-nous blood than that of pika. As a result, oxygen saturation in arterial blood to venous blood is twofold higher in zokor than in pika (5). Zokor have a strong oxygen uptake capacity and higher oxygen utilization compared with pika (5).
Microvessel densities, the numerical density of mitochondria, and the surface density of mitochondria in skeletal muscle of zokor are sig-nificantly higher than those of pika (6). The myoglobin content in skel-etal muscle of zokor is also notably higher than that of pika (6). In the skeletal muscle of pika, the expression of the gene encoding one sub-unit of heteromeric lactose dehydrogenase, Ldh-a, is markedly upregu-lated, and the main LDH isoenzymes found are LDH-A4, LDH-A3B, and LDH-A2B2. However, in skeletal muscle of zokor, the expression of Ldh-b, encoding a different LDH subunit, is upregulated, and the main LDH isoenzymes are LDH-A4, LDH-AB3 and LDH-B4. The activity of LDH in skeletal muscle of pika is significantly higher than that of zokor. Taken together, this suggests that even though zokor inhabits a hypoxic environment, its skeletal muscle can produce high energy lev-
Department of Biology, Qinghai University, Xining, Qinghai, China.*Corresponding author: [email protected]
Differences in Physiological Adaptive Strategies to Hypoxic Environments in Plateau Zokor and Plateau Pika Wei Deng-Bang*, Wang Duo-Wei, Wei Lian, Ma Ben-Yuan
els by aerobic oxidation, whereas pika skeletal muscle obtains energy by anaerobic glycolysis. Furthermore, we found that Ldh-c, originally thought to be expressed only in testis and spermatozoa in mammals (7), was expressed in skeletal muscle of pika, but not in that of zokor. LDH-C4 is a lactate dehydrogenase that catalyzes the interconversion of pyruvate to lactate. It has a low Km for pyruvate (~0.030 mM) and a high Km for lactate (~2.0 mM) compared with LDH-A4 (8). This find-ing implies that LDH-C4 has an affinity for pyruvate that is 60-fold higher than for lactate, suggesting that pyruvate turnover may be higher even at high concentrations of endogenous or extracellular lactate. This notion is supported by studies using a human spermatozoa incu-bation system in which the addition of excess lactate (50-fold excess in relation to pyruvate) did not influence ATP production in capacitat-ing spermatozoa (9). Therefore, skeletal muscle produces ATP mainly by aerobic glycolysis in zokor, and mainly by anaerobic glycolysis in pika.
In conclusion, plateau zokor and plateau pika adopt differ-ent strategies to adapt to hypoxic environments. Plateau zokor has an efficient system for energy production by aerobic oxida-tion even though they inhabit a hypoxic environment, whereas pla-teau pika has an efficient system for energy production by anaerobic glycolysis.
REFERENCES1. N.C.Fan,Y.Z.Shi,Acta Theriol. Sinica 2, 180 (1982). 2. J. X. Zeng, Z. W. Wang, Z. X. Shi, Acta Biol. Plateau Sinica 3, 163
(1984). 3. Z. J. Feng, C. L. Zheng, Acta Theriol. Sinica 5, 269 (1985). 4. X. J. Wang et al., Acta Zool. Sinica 54, 531 (2008).5. D. B. Wei, L. Wei, J. M. Zhang, H. Y. Yu, Comp. Biochem. Phys. A 145,
372 (2006). 6. S. Zhu et al., Sheng li xue bao:[Acta Physiol. Sinica] 61, 373 (2009). 7. A. Blanco, W. H. Zinkham, Science 139, 601 (1963). 8. C. E. Coronel, C. Burgos, N. M. Gerez de Burgos, L. E. Rovai, A.
Blanco, J. Exp. Zool. 225, 379 (1983). 9. T. H. Hereng et al., Hum. Reprod. 26, 3249 (2011).
ACKNOWLEDGMENTSThis work was supported by the National Natural Science Foundation of China (Grant No. C030302 and 30960054), and the Key Project of the Chinese Ministry of Education (Grant No. 209132).

Section Two: Hypoxic Physiology
CR
EDIT
: © IS
TOC
KPH
OTO
.CO
M/A
330P
ILO
T

38
Hypoxic Physiology
Ischemic heart disease is a leading cause of cardiovascular mortality in developed countries (1). Ischemia/reperfusion (I/R) injury is a common cardiovascular problem and has no satisfactory treatment. Thus, identifying new approaches that will reduce I/R injury is clini-
cally important. We have studied the protective use of chronic inter-mittent hypobaric hypoxia (CIHH) systemically since 1996 and have demonstrated that CIHH treatment has a significant cardioprotective effect against I/R injury.
In a previous study, adult male Sprague-Dawley rats were exposed to hypobaric hypoxia in a hypobaric chamber, simulating an altitude of 5,000 m (PO2= 84 mmHg) over 28 or 42 days, for six hours each day. CIHH-treated adult or neonate rats displayed cardiac protection against global and regional I/R, which lasted for two weeks after the end of CIHH treatment. CIHH treatment alleviated the inhibition of ventricular function, limited the infarct area, promoted the recovery of cardiac function, and prevented arrhythmia during I/R (2). In addi-tion, CIHH decreased the activity of lactate dehydrogenase, prevented mitochondrial structural damage and mtDNA deletion, and inhibited calcium overload during I/R (3). Furthermore, I/R-induced apoptosis in cardiomyocytes was significantly attenuated in CIHH-treated rats (4) (Figure 1).
Several mechanisms in the heart may be involved in CIHH-mediat-ed cardiac protection. Our electrophysiological studies suggested that CIHH treatment causes prolongation of the action potential (AP) dura-tion and effective refractory period in a time-dependent manner under normoxic conditions. Additionally, CIHH efficiently prevents the inhi-bition of AP in the ventricular papillary muscles during simulated isch-emia. Whole-cell patch clamp analysis demonstrated that CIHH did not alter the activity of the Ica-L channel in normal recording conditions, but resisted the decrease of Ica-L current and a positive shift of the steady-state inactivation curve under simulated ischemic conditions (5). Thus, the aforementioned effects of CIHH might determine the electrophysi-ological basis for CIHH antiarrhythmia.
Oxygen free radicals are a major cause of I/R-induced injury in car-diomyocytes (6). Endogeneous antioxygenation systems, such as super-oxide dismutase (SOD) and catalase, can block the cascade reactions of oxygen free radicals and activation of lipid peroxidation, resulting in cardiac protection. Our study showed that myocardial SOD activity was increased and malonaldehyde levels were decreased during I/R in CIHH-treated rats, suggesting that CIHH can improve myocardial an-tioxidation capacity (2).
Stress proteins or heat shock proteins (HSPs) can be induced by
various stress stimuli such as hypoxia or ischemia, and have an im-portant protective role in the body. A previous study demonstrated that CIHH induced the augmentation of cardiac HSP70 mRNA ex-pression, which was maintained for approximately two weeks af-ter CIHH treatment (7). The augmentation of cardiac HSP70 mRNA expression was inversely correlated with the incidence rate of arrhythmia, suggesting that HSP is important in CIHH cardiac protection (7).
Opening of the ATP-sensitive potassium channel (KATP) both in cell membranes and mitochondrial membranes is involved in the car-diac protection of ischemia preconditioning (IP). Additionally, glib-enclamide, an inhibitor of KATP in the cell membrane, and 5-HD, an inhibitor of KATP in the mitochondrial membrane, eliminated the im-provement of cardiac function caused by I/R and shortened the time-to-peak contracture of ischemic hearts in CIHH-treated rats compared with control animals. This suggests that KATP, especially KATP in mito-chondrial membranes, is involved in the cardiac protection rendered by CIHH (8).
CIHH was shown to promote the expression of particulate frac-tion PKC-a, -b and -d isozymes after I/R. In isolated rat heart, che-lerythrine, a PKC inhibitor, significantly inhibited the improvement of cardiac functional recovery from I/R in CIHH-treated rats, but had no effect on control heart function. Further research on the mecha-nism of PKC effects showed that chelerythrine treatment increased intracellular sodium ([Na+]i) and calium ([Ca2+]i) in cardiomyocytes, and aggravated the overloading of Na+ and Ca2+ caused by I/R in CIHH-treated rats. Additionally, CIHH inhibited ischemia-induced acidosis in a PKC-dependent manner (9). Together, these data sug-gest that PKC contributes to the cardiac protection afforded by CIHH against I/R.
Treatment with aminoguanidine, a specific inhibitor of inducible nitric oxide synthase, reversed the cardioprotective effect against I/R injury in CIHH-treated rats, but cardiac function in control rats was unchanged. This result suggested that nitric oxide might be involved in the cardiac protection of CIHH (10).
To study the role of mitochondria in cardiac protection with CIHH treatment, atractyloside (Atr), a specific agent that opens the mitochon-drial permeability transition pore (MPTP), was used in Langendorff isolated rat heart preparations. The results showed that CIHH reduced myocardial [Ca2+]i, delayed the time for myocardial MPTP to open and contract, and decreased mitochondrial cytochrome C leakage. The Atr pretreatment abolished the cardioprotective effect in CIHH-treated rats. In contrast, Atr aggravated myocardial [Ca2+]i overloading and contrac-ture in control rats. These results suggested that mitochondria play a pivotal role in cardiac protection of CIHH by inhibiting MPTP (11).
Proteomic studies of mitochondrial proteins in CIHH-treated and nor-moxic control rats showed that more than 14 protein spots were altered at least three-fold. Among the 11 proteins identified by mass spectrom-etry, nine were involved in energy metabolism, of which seven were increased and two were decreased after CIHH treatment. Biochemical tests of energy metabolism in mitochondria supported the proteomic
1Department of Physiology, Hebei Medical University and Hebei Key Labora-tory of Medical Biotechnology, Shijiazhuang, China;2Shanghai Institute for Biological Sciences, Chinese Academy of Sciences, Shanghai, China.*Corresponding authors: Zhang Yi ([email protected]) and Zhu Zhaonian ([email protected])
Cardioprotective Effect of Chronic Intermittent Hypobaric HypoxiaZhang Yi1,* and Zhou Zhaonian2,*

Sect ion Two
39
Section Two
results. CIHH also increases the expression of a molecular chaperone, HSP60 and an antioxidant protein, peroxiredoxin 5. This suggests that adaptive alterations of the expression of enzymes involved in material and energy metabolism in mitochondria play a role in the cardioprotec-tive effect of CIHH (12).
It is generally recognized that CIHH treatment offers cardiac protec-tion against I/R injury. Multiple mechanisms or pathways have been suggested to contribute to the cardioprotection of CIHH. In conclusion, CIHH treatment is useful because it is safe, simple and easy to apply, economical, and can be applied to a broad range of disorders. Thus, it has important clinical value.
REFERENCES 1. C. J. Murray, A. D. Lopez, Lancet 349, 1436 (1997).2. Y. Zhang, N. Zhong, H. F. Zhu, Z. N. Zhou, Acta. Physiol. Sin. 52, 89
(2000).3. W. Z. Zhu, J. W. Dong, H. L. Ding, H.T. Yang, Z. N. Zhou, Eur. J. Appl.
Physiol. 91, 716 (2004). 4. J. W. Dong, H. F. Zhu, W. Z. Zhu, H. L. Ding, Z. N. Zhou, Cell Res. 13,
385 (2003).
5. Y. Zhang, N. Zhong, Z. N. Zhou, High Alt. Med. Biol. 11, 61 (2010). 6. M. K. Ozer et al., Mol Cell Biochem. 273, 169 (2005).7. N. Zhong, Y. Zhang, Q. Z. Fang, Z. N. Zhou, Acta. Pharmacol. Sin. 21,
467 (2000). 8. H. F. Zhu, J. W. Dong, W. Z. Zhu, H. L. Ding, Z. N. Zhou, Life Sci. 73,
1275 (2003). 9. H. L. Ding, H. F. Zhu, J. W. Dong, W. Z. Zhu, Z. N. Zhou, Life Sci. 75,
2587 (2004).10. H. L. Ding et al., Acta. Pharmacol. Sin. 26, 315 (2005).11. W.Z.Zhu,Y.Xie,L.Chen, H.T.Yang, Z. N. Zhou, J. Mol. Cell. Cardiol.
40, 96 (2006).12. W.Z.Zhu,X.F.Wu,Y.Zhang,Z.N.Zhou,Eur. J. Appl. Physiol.
112,1037 (2012).
ACKNOWLEDGMENTSThis work was supported by grants from the National Basic Research Ò 973Ó Program (Grant No. 2006CB504106 and 2012CB518200), the National Natural Science Foundation of China (Grant No. 30572086, 31071002, and 31271223), and the Natural Science Foundation of Hebei Province (Grant No. C2012206001).
FigureÊ 1.Ê TheÊ protectiveÊ effectÊ ofÊ chronicÊ intermittentÊ hypobaricÊ hypoxiaÊ (CIHH)Ê onÊ theÊ heartÊagainstÊ ischemiaÊ andÊ reperfusionÊ (I/R)Ê injuryÊ inÊ rats.Ê DataÊ wereÊ expressedÊ asÊ mean±SD.Ê (A)ÊRepresentativeÊ recordingÊ ofÊ leftÊ ventricularÊ pressure.Ê (B)Ê RepresentativeÊ photosÊ ofÊ infarctÊ size.Ê (C)ÊRepresentativeÊ photomicrographsÊ showingÊ apoptoticÊ cardiomyocytes.Ê BrownÊ stainingÊ (TUNEL-positive)Ê indicatesÊ apoptoticÊ myocytesÊ (arrows).Ê (D)Ê RecoveryÊ ofÊ leftÊ ventricularÊ developingÊpressureÊ (LVDP),Ê maximalÊ differentialsÊ pressureÊ (±LVdp/dtmax)Ê afterÊ 30Ê minuteÊ ischemiaÊ andÊ 60ÊminuteÊ reperfusion.Ê N=8Ê forÊ eachÊ group,Ê *p<0.05,Ê **p<0.01Ê vsÊ Control.Ê (E)Ê ArrhythmiaÊ scoreÊ afterÊ30Ê minuteÊ ischemiaÊ andÊ 60Ê minuteÊ reperfusion.Ê N=8Ê forÊ eachÊ group,Ê **p<0.01Ê vsÊ Control.Ê (F)Ê InfarctÊsizeÊ ofÊ heartÊ afterÊ 30Ê minuteÊ ischemiaÊ andÊ 120Ê minuteÊ reperfusion.Ê N=5Ê forÊ eachÊ group,Ê **p<0.01ÊvsÊ Control.Ê (G)Ê MeanÊ numberÊ ofÊ cardiomyocytesÊ undergoingÊ apoptosisÊ perÊ slide.Ê N=6Ê slidesÊ forÊeachÊ group,Ê I/RÊ representsÊ 30Ê minuteÊ ischemiaÊ andÊ 60Ê minuteÊ reperfusion.Ê **p<0.01Ê vsÊ Control,Ê##p<0.01Ê vsÊ correspondingÊ I/R.Ê
D E F
G
B CA

40
Hypoxic Physiology
A pproximately 140 million people around the world live at altitudes above 2,500 m, including on the Qinghai-Tibet Plateau in China. The increasing ability to travel rapidly to high altitudes results in millions of people being exposed
to the risk of mountain sickness every year, but the underlying mecha-nism of this disorder is still not fully understood. The hypothalamo-pituitary-adrenal (HPA) axis is critical in maintaining homeostasis and in physiological, endocrine, and behavioral responses to stress (1–4). Our findings have shown that corticotropin-releasing factor (CRF) and CRF type-1 receptor (CRFR1) play a crucial role in hypoxia-induced brain-endocrine-immune network disorder (2, 3, 5). The mechanisms include activation of the HPA axis by CRF and CRFR1 signaling in the paraventricular nucleus (PVN); suppression of the growth hormone axis (6); inhibition of the reproductive and metabolic axis (7, 8); distur-bance of immune function; alteration of cognition (9, 10); and induc-tion of anxiety-like behavior (4), as well as reduced sensitivity of the HPA axis and a multimodal pattern of responses to severe hypoxic chal-lenge in mammals of the Tibetan Plateau (11). This minireview extends these findings.
Hypoxia Activates the HPA AxisHypoxia can acutely activate the HPA axis by CRF and endothelin-1 (ET-1) release. CRFR1 mRNA expression is upregulated in the PVN where CRF and ET-1 neurons are stimulated through an ultrashort (au-tocrine and/or paracrine) positive feedback loop to activate CRFR1 sig-naling. Morphologically, CRFR1 is co-localized with CRF and ET-1 (12). Moreover, CRF release is positively regulated by norepinephrine (NE) (13) and angiotensin II (AII) (14), and negatively regulated by arginine vasopressin (AVP) and β-endorphin (β-EP). In the pituitary, hypoxia, cold, and restraint stress, alone or in combination, trigger dif-ferential expression of CRFR1 and CRFR2 mRNA, suggesting that this may lead to distinct endocrine responses not only in the HPA axis but also in other endocrine systems. Interestingly, restraint stress boosts hy-poxia-induced responsiveness, but not in combination with cold stress (2). Hypoxia chronically induces a phase alteration of the HPA axis cascade amplification, including CRF expression in the PVN, as well as ACTH and corticosterone levels in plasma (Figure 1) (1, 3, 12).
Hypoxia Suppresses the Neuroendocrine Network In addition to activation of the HPA axis by hypoxia, a series of shifts
in physiological activity occurs. Hypoxia, particularly at very high al-titude, can acutely induce neuroendocrine network disorder and sig-nificantly suppress growth and development (6), reproduction (7), me-tabolism (8), and immunity, along with marked stimulation of prolactin (PRL) (3), oxytocin (OXT), dynorphin (DNY), and enkephalin (ENK) secretion (Figure 1). All of these effects are modulated by the central ac-tivation of CRF and CRFR1 in the PVN and by increased corticosteroid feedback due to stress. In support of this, morphological observations show that CRF and CRFR1 are present throughout the brain, endocrine organs, and immune tissues, and our findings show that their expres-sion is upregulated following hypoxia. Mimicking ascent to an altitude of 5,000 m in a hypobaric chamber not only activates the HPA axis but also causes a concomitant decline in body weight, reduced food intake, and decreased growth hormone release in adult male and female rats (6). These effects correlate with increased somatostatin gene expression and secretion in the periventricular nucleus and upregulated CRFR1 expression in the pituitary. Although CRFR1 can stimulate insulin-like growth factor 1 (IGF-1) mRNA expression in the liver, it did not alter the downregulated growth hormone (GH) response (6).
Hypobaric hypoxia chronically inhibits the normal development of the testes in neonatal rats, especially at the critical age for gonadal development. Notably, hypoxia reduces testosterone secretion and in-duces swelling of the testicular interstitium and enlargement of the mi-tochondria in Leydig cells at postnatal day 21 (7). CRF inhibits gonad-otropin-releasing hormone (GnRH) and testosterone levels. However, AVP coordinates the inhibition of GnRH by CRF. Moreover, β-EP can also suppress GnRH release, but NE and acetylcholine (Ach) stimulate GnRH release.
Interestingly, acute hypoxia stimulates thyrotropin-releasing hor-mone (TRH) release from the PVN and median eminence, enhancing plasma thyrotropin-stimulating hormone (TSH) levels. NE is also in-volved in TRH release via the α2 receptor (8), whereas chronic hypoxia suppresses TRH mRNA expression in the rat PVN (1), and β-EP modu-lates TRH release in rats.
Hypoxia inhibits T-lymphocyte proliferation, suppresses humoral immune function and alters initial antigen processing via CRF. Chronic hypoxia elicits a dose- and time course-dependent change in CRF and CRFR1 mRNA expression in the PVN, and in CRFR1 mRNA expres-sion in the pituitary (2, 12). During sustained hypoxia, CRF mRNA expression reaches a peak at day five and returns to normal levels at day 10. The peak of CRF and CRFR1 secretion inhibits the release of insulin, which can be blocked by a specific CRFR1 antagonist, sug-gesting CRFR1 is important in glucose metabolism in rats chronically exposed to hypoxia (Figure 2) (15). Hypoxia decreases insulin release, suggesting its potential use in organ transplantation and preservation.
Hypoxia Alters Cognitive Ability and Induces Anxiety Behavior Hypoxia can reduce cognitive ability. Hypoxic injury correlates to a
Corticotropin-Releasing Factor Type-1 Receptors Play a Crucial Role in the Brain-Endocrine Network Disorder Induced by High-Altitude HypoxiaDu Jizeng and Chen Xuequn
Division of Neurobiology and Physiology, Department of Basic Medical Sci-ences, School of Medicine, Zhejiang University, Hangzhou, China; Key Laboratory of Medical Neurobiology of The Ministry of Health, China;Key Laboratory of Medical Neurobiology of Zhejiang Province, Hangzhou, China. Corresponding authors: Du Jizeng ([email protected]) and Chen Xuequn ([email protected])
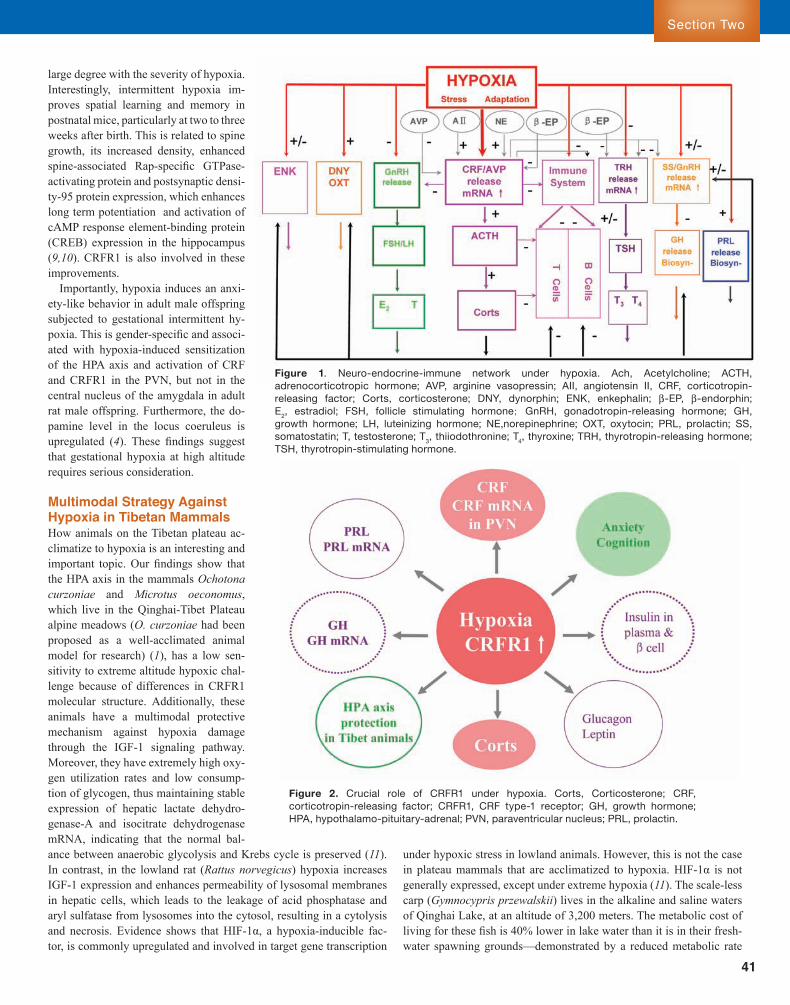
Sect ion Two
41
Section Two
large degree with the severity of hypoxia. Interestingly, intermittent hypoxia im-proves spatial learning and memory in postnatal mice, particularly at two to three weeks after birth. This is related to spine growth, its increased density, enhanced spine-associated Rap-specific GTPase-activating protein and postsynaptic densi-ty-95 protein expression, which enhances long term potentiation and activation of cAMP response element-binding protein (CREB) expression in the hippocampus (9,10). CRFR1 is also involved in these improvements.
Importantly, hypoxia induces an anxi-ety-like behavior in adult male offspring subjected to gestational intermittent hy-poxia. This is gender-specific and associ-ated with hypoxia-induced sensitization of the HPA axis and activation of CRF and CRFR1 in the PVN, but not in the central nucleus of the amygdala in adult rat male offspring. Furthermore, the do-pamine level in the locus coeruleus is upregulated (4). These findings suggest that gestational hypoxia at high altitude requires serious consideration.
Multimodal Strategy Against Hypoxia in Tibetan MammalsHow animals on the Tibetan plateau ac-climatize to hypoxia is an interesting and important topic. Our findings show that the HPA axis in the mammals Ochotona curzoniae and Microtus oeconomus, which live in the Qinghai-Tibet Plateau alpine meadows (O. curzoniae had been proposed as a well-acclimated animal model for research) (1), has a low sen-sitivity to extreme altitude hypoxic chal-lenge because of differences in CRFR1 molecular structure. Additionally, these animals have a multimodal protective mechanism against hypoxia damage through the IGF-1 signaling pathway. Moreover, they have extremely high oxy-gen utilization rates and low consump-tion of glycogen, thus maintaining stable expression of hepatic lactate dehydro-genase-A and isocitrate dehydrogenase mRNA, indicating that the normal bal-ance between anaerobic glycolysis and Krebs cycle is preserved (11). In contrast, in the lowland rat (Rattus norvegicus) hypoxia increases IGF-1 expression and enhances permeability of lysosomal membranes in hepatic cells, which leads to the leakage of acid phosphatase and aryl sulfatase from lysosomes into the cytosol, resulting in a cytolysis and necrosis. Evidence shows that HIF-1α, a hypoxia-inducible fac-tor, is commonly upregulated and involved in target gene transcription
under hypoxic stress in lowland animals. However, this is not the case in plateau mammals that are acclimatized to hypoxia. HIF-1α is not generally expressed, except under extreme hypoxia (11). The scale-less carp (Gymnocypris przewalskii) lives in the alkaline and saline waters of Qinghai Lake, at an altitude of 3,200 meters. The metabolic cost of living for these fish is 40% lower in lake water than it is in their fresh-water spawning grounds—demonstrated by a reduced metabolic rate
FigureÊ 1.Ê Neuro-endocrine-immuneÊ networkÊ underÊ hypoxia.Ê Ach,Ê Acetylcholine;Ê ACTH,ÊadrenocorticotropicÊ hormone;Ê AVP,Ê arginineÊ vasopressin;Ê AII,Ê angiotensinÊ II,Ê CRF,Ê corticotropin-releasingÊ factor;Ê Corts,Ê corticosterone;Ê DNY,Ê dynorphin;Ê ENK,Ê enkephalin;Ê b-EP,Ê b-endorphin;ÊÊE2,Ê estradiol;Ê FSH,Ê follicleÊ stimulatingÊ hormone;Ê GnRH,Ê gonadotropin-releasingÊ hormone;Ê GH,ÊgrowthÊ hormone;Ê LH,Ê luteinizingÊ hormone;Ê NE,norepinephrine;Ê OXT,Ê oxytocin;Ê PRL,Ê prolactin;Ê SS,Êsomatostatin;Ê T,Ê testosterone;Ê T3,Ê thiiodothronine;Ê T4,Ê thyroxine;Ê TRH,Ê thyrotropin-releasingÊ hormone;ÊTSH,Ê thyrotropin-stimulatingÊ hormone.
FigureÊ 2.Ê CrucialÊ roleÊ ofÊ CRFR1Ê underÊ hypoxia.Ê Corts,Ê Corticosterone;Ê CRF,Êcorticotropin-releasingÊ factor;Ê CRFR1,Ê CRFÊ type-1Ê receptor;Ê GH,Ê growthÊ hormone;ÊHPA,Ê hypothalamo-pituitary-adrenal;Ê PVN,Ê paraventricularÊ nucleus;Ê PRL,Ê prolactin.
42
Hypoxic Physiology
1Environmental Medicine Research Center, Institute of Health and Environmental Medicine, Academy of Military Medical Sciences, Tianjin, China; 2Thadweik Academy of Medicine, Beijing, China.*Corresponding author: [email protected]
The Key Role of Vascular Endothelial Dysfunction in Injuries Induced by Extreme Environmental Factors at High AltitudeLong Chaoliang1, Liu Jiaying1, Yin Zhaoyun1, Liu Wei1, Wang Hai1,2,*
leading to capillary leakage, activation of prothrombosis, and initiation of inflammation (1, 2).
Hypoxia and Endothelial DysfunctionWe previously demonstrated that hypoxia could induce structural and functional injury of ECs. When cultured pulmonary artery ECs (PAECs) were exposed to hypoxia, the rates of von Willebrand factor (vWF) and prostaglandin I2 (PGI2) release were significantly decreased, while endothelin-1 (ET-1) release was increased, suggesting that PAEC functionality as a permeability barrier was impaired (3). Vascular endo-thelial growth factor (VEGF), a potent and specific mitogen for ECs, can initiate angiogenesis and increase vascular permeability (2). Un-der hypoxic conditions, PAEC monolayer permeability to bovine se-rum albumin and human albumin was enhanced and VEGF levels were significantly increased, indicating that PAEC permeability may play an important role in the occurrence of high-altitude pulmonary edema (HAPE) (3). In vivo studies showed decreased levels of nitric oxide and nitric oxide synthase activity in the brain and lungs from rats exposed to hypoxia. High-altitude cerebral edema (HACE) in rats was induced by
F ar from being a passive lining of blood vessels as was initially thought, endothelium is a dynamic tissue with numerous func-tions, which include regulation of blood fluidity, formation of an active barrier between the vascular lumen and tissue,
modulation of local vascular tone, development of new vessels during angiogenesis, and propagation and amplification of the inflammatory response (1). Extreme environmental factors at high altitude such as hypoxia and cold can result in endothelial dysfunction, which plays key roles in the initiation and progression of high-altitude sickness and frostbite. Vascular endothelial cells (ECs) are the first to respond to low oxygen partial pressure (PO2) experienced at high altitudes. The en-dothelial response to hypoxic challenge induces a highly reproducible cascade of events, which includes modification of cellular phenotype
and O2 consumption—indicating that they are well adapted to hypoxic conditions and experience a “metabolic holiday” when in Qianghai Lake (16). Gill remodeling during hypoxia is a general characteristic of cold-water carp species. The reduced magnitude of the response to hy-poxia in G. przewalskii relative to goldfish and crucian carp may reflect a more active lifestyle and the fact that it lives in a hypoxic environ-ment at altitude. Low habitat temperatures have reduced the evolution-ary pressure for selection of HIF-1α in G. przewalskii, whereas the cold and hypoxic lake water has contributed to the evolution of the HIF-1α gene (17).
In summary, activation of CRF and CRFR1 by high-altitude hypoxia can result in activation of the HPA axis and a series of disorders of growth, reproduction, metabolism, immunity, and behavioral respons-es. CRFR1 antagonists may be used to treat and prevent disorders of the neuroendocrine network under hypoxic conditions.
REFERENCES 1. J. Z. Du, in Progress in Mountain Medicine and High Altitude
Physiology. H.Ohna et al., Eds. (Press committee of the 3rd world congress on mountain medicine and high altitude physiology, Japan, 1999), pp. 416-417.
2. T.Y.Wanget al., Neuroscience 128, 111 (2004). 3. J. F. Xu, X. Q. Chen, J. Z. Du, Horm. Behav. 49, 181 (2006). 4. J. M. Fan, X. Q. Chen, H. Jin, J. Z. Du, Neuroscience 159, 1363 (2009).
5. J. F. Xu, X. Q. Chen, J. Z. Du, T. Y. Wang, Peptides 26, 639 (2005). 6. X.Q.Chen,N.Y.Xu,J.Z.Du,Y.Wang,C.M.Duan,Mol. Cell.
Endocrinol. 242, 50 (2005). 7. J. X. Liu, J. Z. Du, Neuro. Endocrinol. Lett. 23, 231 (2002). 8. T. D. Hou, J. Z. Du, Neuro. Endocrinol. Lett. 26, 43 (2005). 9. X. J. Lu et al., Neuroscience 162, 404 (2009). 10. J. X. Zhang, X. Q. Chen, J. Z. Du, Q. M. Chen, C. Y. Zhu, J. Neurobiol.
65, 72 (2005). 11. X. Q. Chen, S. J. Wang, J. Z. Du, X. C. Chen, Am. J. Physiol. Regul.
Integr. Comp. Physiol. 292, R516 (2007).12. J. J. He, X. Q. Chen, L. Wang, J.F. Xu, J. Z. Du, Neuroscience 152,
1006 (2008). 13. X. Q. Chen, J. Z. Du, Y. S. Wang, Regul. Pept. 119, 221 (2004). 14. Y.Wu,J.Z.Du,Acta Pharmalogica Sin. 21,1035 (2000).15. X. Q. Chen, J. Dong, C. Y. Niu, J. M. Fan, J. Z. Du, Endocrinology 148,
3271 (2007). 16. C. M. Wood, Physiol. Biochem. Zool. 80, 59 (2007).17. Y.B.Cao,X.Q.Chen,S.Wang,Y.X.Wang,J.Z.Du,J. Mol. Evol. 67,
570 (2008).
ACKNOWLEDGMENTSThis work was supported by grants from the National Natural Science Foundation of China (Grant No. 30393130) and the National Basic Research Ò 973Ó Program (Grant No. 2006CB504100 and 2012CB518200).

Sect ion Two
43
Section Two
exposure to a simulated altitude of 8,000 m, and electron micrographs showed capillary endothelial cell swelling, irregular thickening of cap-illaries, and widening of the perivascular space in the blood–brain bar-rier (BBB). Gene expression and protein levels of VEGF, aquaporin-1, and aquaporin-4 in ECs were significantly increased (4, 5). Changes in ECs during cerebral edema caused by hypoxic exposure might induce BBB injury, and be involved in the pathogenesis of HACE. Based on
these findings, we proposed that management of endothelial dysfunc-tion could be an important strategy for the prevention and treatment of HAPE and HACE.
Cold and Endothelial DamageIn addition to hypoxia, cold is another extreme environmental fac-tor; frostbite is sometimes observed among individuals exposed to
FigureÊ 1.Ê TheÊ endothelialÊ dysfunctionÊ hypothesisÊ ofÊ frostbite.Ê ColdÊ exposureÊ inducesÊ endothelialÊ cellÊ (EC)Ê freezingÊ andÊischemia/reperfusionÊ (I/R)Ê injuries,Ê resultingÊ inÊ EC-Ê polymorphonuclearÊ leukocyteÊ (PMN)Ê adhesionÊ andÊ ECÊ dysfunction.ÊThe imbalance of vasoactive factors and inflammatory mediators released from damaged ECs induce coagulation disor-dersÊ includingÊ bloodÊ hemorheologicalÊ disorders,Ê vasomotorÊ dysfunction,Ê edema,Ê andÊ hypercoagulability.Ê TheseÊ eventsÊresultÊ inÊ microcirculationÊ disorderÊ andÊ thrombosis,Ê whichÊ leadÊ toÊ tissueÊ injuriesÊ suchÊ asÊ cellÊ necrosisÊ atÊ sitesÊ ofÊ frostbite.ÊNO,Ê nitricÊ oxide;Ê PGI2,Ê prostaglandinÊ I2;Ê vWF,Ê vonÊ WillebrandÊ factor;Ê ET-1,Ê endothelin-1;Ê ACE,Ê angiotensinÊ convertingÊ en-zyme;Ê TXA2,Ê thromboxaneÊ A2;Ê RBC,Ê redÊ bloodÊ cell.

44
Hypoxic Physiology
low temperatures at high altitude, caused by a combination of tissue freezing and hypoxia. Tissue freezing depends on environmental fac-tors including wind, duration of exposure, and air moisture, resulting in tissue necrosis (3, 6). Research over the past 20 years has led to a new understanding of the pathophysiology of cold injury. Elucidation of the roles of inflammatory mediators such as prostaglandin F2 (PGF2), thromboxane A2 (TXA2), platelet aggregation, and thrombosis has led to active medical regimens for the treatment for frostbite, such as the use of ibuprofen and aloe vera, heparin, low molecular weight dextran, and vasodilating agents, as well as the widespread acceptance of the importance of rapid rewarming (6).
Our previous studies demonstrated that exposure to cold could in-duce structural and functional damage, as the number of ECs in cir-culatory blood was significantly increased, suggesting they had been damaged and separated from the arterial wall lamina (7). Concurrently, the levels of TXA2, fibronectin, the TXA2:PGI2 ratio, and angiotensin converting enzyme activity in serum were increased, while PGI2 levels and antithrombin-III activity were significantly decreased. Histologi-cal examination showed that cold induced microvascular EC degen-eration, necrosis, and detachment. Platelet aggregation, bleeding, and thrombosis were also observed in microvessels. These data suggested that cold induced structural and functional damage to ECs, resulting in vasoconstriction, promotion of blood coagulation, circulation disor-ders, and tissue anoxia or necrosis (7, 8). Consistent with the in vivo results, in vitro experiments showed that ECs were sensitive to cold injury, which caused a decrease in the number of ECs and the PGI2 levels, while lactate dehydrogenase (LDH) activity and TXA2 levels in the culture media increased (3).
The characteristics of cold acclimation include enhanced tolerance to cold exposure and lower susceptibility to cold injury. To confirm the role of ECs in the pathogenesis of frostbite, the effects of cold acclimation on EC functions in rats affected by frostbite were inves-tigated. Frostbite caused damage to ECs, resulting in their detach-ment, as well as vasoconstriction, blood coagulation, and microcir-culation disorders, which could exacerbate the effects of frostbite. When cold acclimation was induced, these parameters were tem-porarily changed, and the area of tissue survival significantly in-creased. This suggested that adaptive changes after cold acclimation, such as increased metabolic turnover rate and improved function of ECs, were beneficial to enhancing repair responses and resistance to frostbite (9, 10).
We further investigated the molecular mechanisms of EC damage induced by cold and found that freezing/thawing of ECs and polymor-phonuclear leukocytes (PMNs) could elicit increased expression of in-tercellular adhesion molecule-1 (ICAM-1) on the surface of ECs and lymphocyte function-associated antigen-1 (LFA-l) on the surface of PMNs. This may trigger EC-PMN adherence and subsequently lead to EC damage. After freezing/thawing, tumor necrosis factor α (TNF-α) release from ECs was increased, which was promoted by EC-PMN in-teractions. TNF-α can promote the expression of LFA-l (on the surface of frozen/thawed PMNs) and ICAM-1 (on normal ECs), thus encourag-ing EC-PMN interactions and further induction of EC damage. TNF-α can also promote apoptosis or necrosis in normal ECs and frozen/thawed PMNs, causing further tissue damage. Monoclonal antibodies against LFA-1 and ICAM-1 could partly block EC-PMN adhesion and thereby attenuate EC damage (11–13).
During the frostbite process, hemagglutination is enhanced as the blood becomes hypercoagulable due to increased platelets and rising
plasma levels of TXA2, which could promote platelet aggregation and enhance vasoconstriction. Altered hemorheological behavior, such as increased levels of hematocrit and whole blood viscosity, and decreased red blood cell deformability, resulted in slower blood flow and throm-bosis, and led to microcirculation disorder. Ultrastructural analysis of frozen tissue showed that the most obvious change was characterized by vascular EC injury that was consistent with the degree of cold (9, 10). Thus, we proposed that dysfunctional ECs have a key role in the pathogenesis of frostbite (Figure 1). Indeed, our new medical regimen for treating frostbite, based on this hypothesis, was highly effective.
SummaryHypoxia and cold coexist at high altitudes. Tissue injuries induced by hypoxia and cold together were more serious than damage caused by ei-ther factor alone. Blood circulation disorders reduced tissue blood and oxygen supply, and the rate of tissue metabolism, which exacerbated tissue damage and delayed the repair of damaged tissue, causing exten-sive tissue necrosis. EC damage induced the synthesis and secretion of PGI2 and TXA2, which induced vasoconstriction, platelet aggregation, and exacerbated hemagglutination and thrombosis (10). However, we found that EC damage was more serious and the tissue survival area was reduced in frostbitten rats acclimated to hypoxia when compared to frostbite at normoxia or frostbite during acute hypoxia.
In summary, extreme environmental factors, such as hypoxia and cold, induced structural damage and dysfunction of ECs. Inflamma-tory responses from ECs further aggravated dysfunction, forming a feedback loop resulting in the imbalance of biologically active factors synthesized and released by ECs, causing high altitude pulmonary hy-pertension, HAPE, HACE, and frostbite. Endothelial dysfunction plays a key role in injuries induced by extreme environmental factors at high altitudes. Thus, ECs may be important targets for the prevention and treatment of high-altitude sickness.
REFERENCES 1. V. S. Ten, D. J. Pinsky, Curr. Opin. Crit. Care 8, 242 (2002). 2. D. Shweiki, A. Itin, D. Soffer, E. Keshet, Nature 359, 843 (1992). 3. H. Wang et al., Sci. Sin. (Vitae) 41, 822 (2011). 4. H. L. Zhu, W. Q. Luo, H. Wang, Neuroscience 157, 884 (2008).5. Y. M. Tian et al., Chin. J. Appl. Physiol. 27, 7 (2011).
6. C. Imray, A. Grieve, S. Dhillon, the Caudwell Xtreme Everest Research Group, Postgrad. Med. J. 85, 481 (2009).
7. F.Z.Li,P.H.Yan,Y.M.Liu,Z.R.Yang,S.J.Zhang,Chin. J. Trauma 10, 280 (1994).
8. F. Z. Li et al., Chin. J. Appl. Physiol. 16, 204 (1996).9. Z. R. Yang, J. Y. Liu, P. H. Yan, Clin. Hemorheol. Microcirc. 29, 103
(2003).10. Z. R. Yang et al., Clin. Hemorheol. Microcirc. 20, 189 (1999).11. J.Y.Liu,Q.L.Shan,Z.R.Yang,P.H.Yan,F.R.Sun,Chin. J. Appl.
Physiol. 22, 153 (2006).12. M.Wang,J.Y.Liu,Z.R.Yang,P.H.Yan,W.Cao,Chin. J. Appl.
Physiol. 19, 52 (2003).13. L.Y.Jin,J.Y.Liu,Z.R.Yang,P.H.Yan,Chin. J. Appl. Physiol. 21, 393
(2005).
ACKNOWLEDGMENTSThis work was supported by grants from the National Basic Research Ò 973Ó Program (Grant No. 2012CB518200) and the State Key Research Project of China (Grant No. AWS11J003).

Sect ion Two
45
Section Two
distinct subunits. KATP channels vary among different tissues, suggest-ing structurally and functionally distinct subtypes. In endothelial cells, KATP channels consist of SUR2B and Kir6.1 subunits and contribute to maintaining resting membrane potential (5, 6). Although activated KATPchannels regulate intracellular Ca2+ levels that affect the production of
T here are at least 140 million individuals living or working in high-altitude areas
worldwide who suffer from high-altitude illnesses (1). The limitations of available therapies against these diseas-es have been recognized and effective medications are ur-gently needed (2). A growing body of evidence suggests that endothelial cells play a critical role in the pathophysiological events related to the initiation and progression of high-alti-tude sickness (3). Hypoxia ex-posure rapidly induces energy metabolism abnormalities, activation of vascular endo-thelial cells, and subsequently results in endothelial dysfunc-tion. Dysfunctional endothe-lial cells secrete lower levels of nitric oxide (NO) and pros-taglandin I2 (PGI2), and higher levels of endothelin-1 (ET-1) compared with normal cells, and overexpress multiple ad-hesion molecules and vascular endothelial growth factor (3). This eventually leads to loss of vasomotor control, pro-motion of inflammation, and cardiovascular remodeling (2–4). Therefore, developing a therapeutic target that af-fords protection against endothelial dysfunction is of great value for the treatment of high-altitude sickness.
The Role of KATP Channels in EndotheliumAdenosine triphosphate-sensitive potassium (KATP) channels regulate cell energy metabolism by controlling membrane potentials and play important roles in modulating cell functions (5). KATP channels are formed from two dissimilar subunits. The pore-forming subunit is an inwardly rectifying potassium channel that has two subtypes: Kir6.1 and Kir6.2. The regulatory subunit is the sulfonylurea receptor (SUR) that has three subtypes: SUR1, SUR2A, and SUR2B. The KATP chan-nel is a hetero-octameric complex composed of four pairs of these two
1Cardiovascular Drug Research Center, Institute of Health and Environmental Medicine, Academy of Military Medical Sciences, Beijing, China; 2Thadweik Academy of Medicine, Beijing, China.*Corresponding author: wh9588@ yahoo.com.cn
Targeting Endothelial Dysfunction in High-Altitude Illness with a Novel Adenosine Triphosphate-Sensitive Potassium Channel OpenerPan Zhiyuan1, Cui Wenyu1, Zhang Yanfang1, Long Chaoliang1, Wang Hai1,2,*
FigureÊ 1. IptakalimÊ activatesÊ SUR2B/Kir6.1-typeÊ KATPÊ channelsÊ toÊ protectÊ againstÊ endothelialÊ dysfunctionÊ inducedÊbyÊ environmentalÊ factors.Ê ByÊ openingÊ endothelialÊ SUR2B/Kir6.1-typeÊ KATPÊ channels,Ê therebyÊ permittingÊ plasmaÊmembraneÊ K+ efflux, iptakalim induces hyperpolarization, increases Ca2+Ê entry,Ê andÊ consequentlyÊ producesÊ aÊseriesÊ ofÊ cellularÊ andÊ molecularÊ eventsÊ toÊ improveÊ endothelialÊ dysfunction:Ê (i)Ê AnÊ increaseÊ inÊ cytosolicÊ freeÊ Ca2+
activatesÊ cellularÊ phospholipaseÊ A2Ê (cPLA2)Ê andÊ promotesÊ arachidonicÊ acidÊ conversionÊ toÊ prostaglandinÊ I2Ê (PGI2);Ê(ii)Ê FreeÊ Ca2+Ê bindsÊ toÊ calmodulinÊ andÊ theÊ Ca2+Ð calmodulinÊ complexÊ activatesÊ endothelialÊ nitricÊ oxideÊ synthaseÊ(eNOS)Ê toÊ produceÊ nitricÊ oxideÊ (NO),Ê anÊ effectiveÊ vasodilatorÊ thatÊ canÊ synergizeÊ withÊ PGI2Ê toÊ relaxÊ resistanceÊofÊ vesselsÊ andÊ pulmonaryÊ arteries;Ê (iii)Ê IncreasedÊ NOÊ inducedÊ byÊ iptakalimÊ canÊ suppressÊ theÊ expressionÊ ofÊproinflammatory mediators by inhibiting the activation of the transcription factor nuclear factor-kBÊ (NF-kB);Ê(iv)Ê IptakalimÊ canÊ leadÊ toÊ secretionÊ ofÊ chemerinÊ andÊ enhancementÊ ofÊ theÊ chemerin/ChemR23Ê signalingÊ system;Ê(v)Ê IptakalimÊ inhibitsÊ theÊ expressionÊ ofÊ endothelin-1Ê (ET-1)Ê andÊ vascularÊ endothelialÊ growthÊ factorÊ (VEGF)Ê toÊpreventÊ cardiovascularÊ remodelingÊ andÊ increasedÊ capillaryÊ permeability.Ê COX,Ê cyclooxygenase;Ê cPLA2,Ê cytosolicÊphospholipaseÊ A2;Ê HIF,Ê hypoxiaÊ inducibleÊ factor;Ê MCP-1,Ê monocyteÊ chemotacticÊ protein-1;Ê ICAM-1,Ê intercellularÊadhesionÊ molecule-1;Ê VCAM-1,Ê vascularÊ cellÊ adhesionÊ molecule-1.

46
Hypoxic Physiology
endothelial autacoids, it is not clear whether the opening of endothelial KATP channels can modulate the process of endothelial dysfunction (4).
We showed that administration of a KATP channel opener (KCO) to cultured endothelial cells increased NO release and free intracellular Ca2+ levels. Additionally, KATP channel activation inhibited ET-1 syn-thesis and secretion that correlated with a reduction in gene expres-sion of ET-1 and endothelin-converting enzyme. Notably, our results demonstrated for the first time that KCO could reverse the imbal-ance between decreased NO release and increased ET-1 production in dysfunctional endothelial cells (7). ET-1, a potent vasoconstrictor and proliferative factor, is implicated in hypoxic pulmonary hyper-tension and cardiovascular remodeling, while NO, a potent vaso-dilator, can reduce the resistance of blood vessels. Reversing a NO/ET-1 imbalance by activation of endothelial KATP channels is the main factor protecting against endothelial dysfunction. Previously, it was shown that opening of KATP channels could modulate endothe-lial resting membrane potentials and increase intracellular Ca2+ lev-els to activate cellular phospholipase A2. This promoted arachidonic acid conversion to PGI2, and synergized with increased bioavailability of NO to reduce pulmonary hypertension and ameliorate endothelial function (3).
Interestingly, in endothelial cells under metabolic disturbances, we demonstrated that KCO inhibited the overexpression of monocyte che-motactic protein-1, intercellular adhesion molecule-1, and vascular cell adhesion molecule-1, which are proinflammatory proteins commonly controlled by the transcription factor nuclear factor-κB (NF-κB) (7). Because NO can inhibit the activity of NF-κB, increased NO by KCO may decrease the expression of proinflammatory proteins. Recently, we also reported that KCO upregulated endothelial chemerin secretion and receptor ChemR23 gene/protein expression to inhibit inflammation me-diated by endothelial cell activation (Figure 1) (8).
Treating High-Altitude Sickness Using KATP Channel OpenersBased on these investigations, we hypothesized that improving endo-thelial dysfunction with a KCO may be a useful way to prevent the development of high-altitude sickness. However, currently available KCOs, such as minoxidil, pinacidil, and diazoxide, cannot selectively activate the endothelial SUR2B/Kir6.1-type KATP channel, and induce many undesirable side effects that severely restrict their clinical utility (6). Therefore, we used a heterologous expression technique and patch clamp recordings to screen KCOs with selectivity for SUR2B/Kir6.1 channels. We discovered that iptakalim, a novel KCO, exhibited high selectivity for the SUR2B/Kir6.1 channel. Clinical trials of iptakalim in China have shown that in addition to its potent antihypertensive effica-cy, it has a favorable safety and tolerability profile (6). Interestingly, our previous studies indicated that iptakalim could potently protect against endothelial dysfunction by activating endothelial KATP channels (7). We further investigated the efficacy of iptakalim in treating high-altitude cerebral edema in rats in a simulated high-altitude (8,000 meters) en-vironment (9). As predicted, it prevented hypobaric hypoxia-induced brain injury in a dose-dependent manner, attenuated permeability of the blood brain barrier and resulting brain edema, reversed abnormali-ties in Na+ and Ca2+ levels, and normalized the activities of Na+/K+-ATPases, Ca2+-ATPases, and Mg2+-ATPases in the rat cerebral cortex. Furthermore, we found that iptakalim could increase cell survival and decrease lactate dehydrogenase release in cultured endothelial cells
under oxygen-and-glucose-deprived conditions (9). In hypoxic pulmo-nary hypertensive rats (10), iptakalim decreased blood pressure in the pulmonary circulation, and attenuated remodeling in the right ventricle and pulmonary arteries. In monocrotaline-induced pulmonary arterial hypertensive rats (11), iptakalim treatment reduced the high right ven-tricle systolic pressure and the increase in weight ratio of right ven-tricle to left ventricle plus septum, decreased the mean arterial pressure, and inhibited right ventricle myocardial tissue cell apoptosis. It also prevented pulmonary edema and inflammation, and reduced ET-1 and tumor necrosis factor-α levels in lung tissue (11). We also investigated the effects of iptakalim on the progression of cardiac hypertrophy fail-ure in a rat model of pressure overloading caused by abdominal aor-tic banding (AAB) (12). In AAB-treated rats, iptakalim attenuated left ventricular hypertrophy, lowered blood pressure, improved systolic and diastolic cardiac dysfunction, and prohibited the progression of heart failure. Because endothelial dysfunction is pivotal to cardiac hyper-trophy and failure induced by pressure overload, we further explored the effects of iptakalim on endothelial dysfunction in vivo. Following iptakalim administration, the downregulation of the NO signaling sys-tem was reversed, whereas the upregulation of the endothelin signaling system was inhibited, resulting in normalization of the balance between these two systems (12). Importantly, a clinical trial of iptakalim for the treatment of pulmonary hypertension is currently ongoing in China. The preliminary statistical analysis implies that iptakalim significantly ameliorates high-altitude heart disease by lowering pulmonary arterial pressure (unpublished data). Iptakalim also appears to have a favorable safety and tolerability in patients with high-altitude pulmonary hyper-tension and heart disease (unpublished data).
In summary, we have provided evidence to support the hypothesis that improvement in endothelial dysfunction by activation of endothe-lial KATP channels could be an important strategy for the treatment of high-altitude sickness. Iptakalim, a recently developed SUR2B/Kir6.1-type KCO, has been shown to be efficacious in patients with high-alti-tude sickness.
REFERENCES 1. D. Penaloza, J. Arias-Stella, Circulation 115,1132 (2007). 2. B. Basnyat, D. R. Murdoch, Lancet 361,1967 (2003). 3. C. Michiels, T. Arnould, J. Remacle, Biochim. Biophys. Acta. 1497, 1
(2000). 4. T. Minamino, M. Hori, Cardiovasc. Res. 73, 448 (2007). 5. C. G. Nichols, Nature 440, 470 (2006). 6. Z. Y. Pan et al., J. Cardiovasc. Pharmacol. 56, 215 (2010). 7. H. Wang et al., Cardiovasc. Res. 73, 497 (2007). 8. R. J. Zhao, H. Wang, Acta Pharmacol. Sin. 32, 573 (2011). 9. H. L. Zhu, W. Q. Luo, H. Wang, Neuroscience 157, 884 (2008).10. H. Wang, Y. Tang, Y. L. Zhang, Cardiovasc. Drug. Rev. 23, 293 (2005). 11. J.S.Li,C.L.Long,W.Y.Cui,H.Wang,J. Cardiovasc. Pharmacol.
Ther. (2012), doi:10.1177/1074248412458154.12. S. Gao, C. L. Long, R. H. Wang, H. Wang, Cardiovasc. Res. 83, 444
(2009).
ACKNOWLEDGMENTSThis work was supported by grants from the National New Drug Research and Development Key Project of China (Grant No. 2008ZX09101-006, 2008ZXJ09004-018, 2009ZX09301-002, and 2010ZX09401-307-1-9) and the National Basic Research Ò 973Ó Program (Grant No. 2012CB518200).
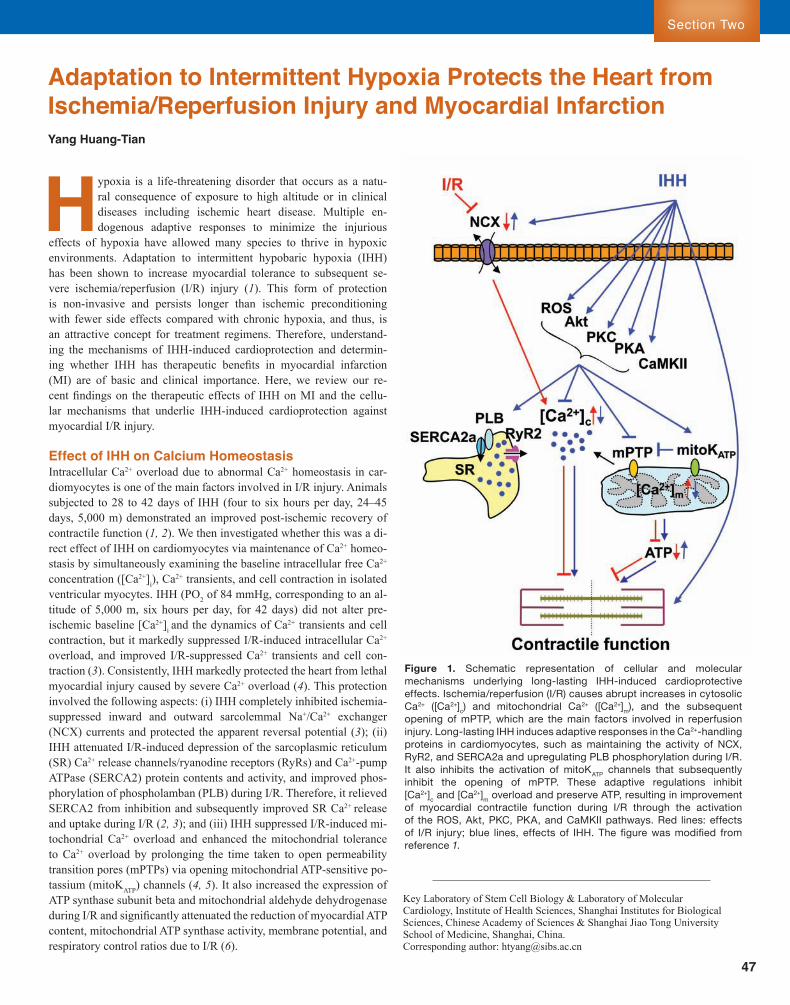
Sect ion Two
47
Section Two
Adaptation to Intermittent Hypoxia Protects the Heart from Ischemia/Reperfusion Injury and Myocardial InfarctionYang Huang-Tian
Key Laboratory of Stem Cell Biology & Laboratory of Molecular Cardiology, Institute of Health Sciences, Shanghai Institutes for Biological Sciences, Chinese Academy of Sciences & Shanghai Jiao Tong University School of Medicine, Shanghai, China.Corresponding author: [email protected]
Hypoxia is a life-threatening disorder that occurs as a natu-ral consequence of exposure to high altitude or in clinical diseases including ischemic heart disease. Multiple en-dogenous adaptive responses to minimize the injurious
effects of hypoxia have allowed many species to thrive in hypoxic environments. Adaptation to intermittent hypobaric hypoxia (IHH) has been shown to increase myocardial tolerance to subsequent se-vere ischemia/reperfusion (I/R) injury (1). This form of protection is non-invasive and persists longer than ischemic preconditioning with fewer side effects compared with chronic hypoxia, and thus, is an attractive concept for treatment regimens. Therefore, understand-ing the mechanisms of IHH-induced cardioprotection and determin-ing whether IHH has therapeutic benefits in myocardial infarction (MI) are of basic and clinical importance. Here, we review our re-cent findings on the therapeutic effects of IHH on MI and the cellu-lar mechanisms that underlie IHH-induced cardioprotection against myocardial I/R injury.
Effect of IHH on Calcium HomeostasisIntracellular Ca2+ overload due to abnormal Ca2+ homeostasis in car-diomyocytes is one of the main factors involved in I/R injury. Animals subjected to 28 to 42 days of IHH (four to six hours per day, 24–45 days, 5,000 m) demonstrated an improved post-ischemic recovery of contractile function (1, 2). We then investigated whether this was a di-rect effect of IHH on cardiomyocytes via maintenance of Ca2+ homeo-stasis by simultaneously examining the baseline intracellular free Ca2+
concentration ([Ca2+]i), Ca2+ transients, and cell contraction in isolated ventricular myocytes. IHH (PO2 of 84 mmHg, corresponding to an al-titude of 5,000 m, six hours per day, for 42 days) did not alter pre-ischemic baseline [Ca2+]i and the dynamics of Ca2+ transients and cell contraction, but it markedly suppressed I/R-induced intracellular Ca2+ overload, and improved I/R-suppressed Ca2+ transients and cell con-traction (3). Consistently, IHH markedly protected the heart from lethal myocardial injury caused by severe Ca2+ overload (4). This protection involved the following aspects: (i) IHH completely inhibited ischemia-suppressed inward and outward sarcolemmal Na+/Ca2+ exchanger (NCX) currents and protected the apparent reversal potential (3); (ii) IHH attenuated I/R-induced depression of the sarcoplasmic reticulum (SR) Ca2+ release channels/ryanodine receptors (RyRs) and Ca2+-pump ATPase (SERCA2) protein contents and activity, and improved phos-phorylation of phospholamban (PLB) during I/R. Therefore, it relieved SERCA2 from inhibition and subsequently improved SR Ca2+ release and uptake during I/R (2, 3); and (iii) IHH suppressed I/R-induced mi-tochondrial Ca2+ overload and enhanced the mitochondrial tolerance to Ca2+ overload by prolonging the time taken to open permeability transition pores (mPTPs) via opening mitochondrial ATP-sensitive po-tassium (mitoKATP) channels (4, 5). It also increased the expression of ATP synthase subunit beta and mitochondrial aldehyde dehydrogenase during I/R and significantly attenuated the reduction of myocardial ATP content, mitochondrial ATP synthase activity, membrane potential, and respiratory control ratios due to I/R (6).
FigureÊ 1.Ê SchematicÊ representationÊ ofÊ cellularÊ andÊ molecularÊmechanismsÊ underlyingÊ long-lastingÊ IHH-inducedÊ cardioprotectiveÊeffects.Ê Ischemia/reperfusionÊ (I/R)Ê causesÊ abruptÊ increasesÊ inÊ cytosolicÊCa2+Ê ([Ca2+]c)Ê andÊ mitochondrialÊ Ca2+Ê ([Ca2+]m),Ê andÊ theÊ subsequentÊopeningÊ ofÊ mPTP,Ê whichÊ areÊ theÊ mainÊ factorsÊ involvedÊ inÊ reperfusionÊinjury.Ê Long-lastingÊ IHHÊ inducesÊ adaptiveÊ responsesÊ inÊ theÊ Ca2+-handlingÊproteinsÊ inÊ cardiomyocytes,Ê suchÊ asÊ maintainingÊ theÊ activityÊ ofÊ NCX,ÊRyR2,Ê andÊ SERCA2aÊ andÊ upregulatingÊ PLBÊ phosphorylationÊ duringÊ I/R.ÊItÊ alsoÊ inhibitsÊ theÊ activationÊ ofÊ mitoKATPÊ channelsÊ thatÊ subsequentlyÊinhibitÊ theÊ openingÊ ofÊ mPTP.Ê TheseÊ adaptiveÊ regulationsÊ inhibitÊ[Ca2+]cÊ andÊ [Ca2+]mÊ overloadÊ andÊ preserveÊ ATP,Ê resultingÊ inÊ improvementÊofÊ myocardialÊ contractileÊ functionÊ duringÊ I/RÊ throughÊ theÊ activationÊofÊ theÊ ROS,Ê Akt,Ê PKC,Ê PKA,Ê andÊ CaMKIIÊ pathways.Ê RedÊ lines:Ê effectsÊof I/R injury; blue lines, effects of IHH. The figure was modified from referenceÊ 1.

48
Hypoxic Physiology
Effect of IHH on Kinase SignalingProtein kinases play important roles in mediating the transduction of stress signals from the plasma to various cellular organelles. Activation of protein kinase B (Akt/PKB), protein kinase Ce (PKCe), and protein kinase II (CaMKII) during reperfusion, and activation of protein kinase A (PKA) at the end of ischemia and early reperfusion, have been shown to contribute to IHH-induced cardioprotection in SR and/or mitochon-dria and subsequently to the maintenance of intracellular Ca2+ homeo-stasis and improvement of post-ischemic myocardial performance (1, 2, 4, 7). Recently, we observed that IHH further elevated mitochondrial reactive oxygen species (ROS) production during early reperfusion, which contributed to IHH-induced cardioprotection by activating the Akt and PKCe pathways and inactivating glycogen synthase kinase-3b(8). Thus, a moderate increase in ROS during early reperfusion may be required to efficiently activate pro-survival signaling pathways.
IHH as a TherapyTo date, most studies have focused on the preventative effects of IHH on myocardial I/R injury, but little is known regarding the therapeutic effect of IHH exposure after MI has occurred. We found that exposure to 14 or 28 days of IHH (PO2 of 84 mmHg, six hours per day) 7 days after the onset of MI significantly reduced the scar area and improved myocardial viability and left ventricular function (9). These results were associated in part with an anti-apoptotic effect, improved coro-nary flow by increased vascular endothelial growth factor expression and capillary density, and reduction of collagen content in the peri-in-farct region. These data raise the intriguing possibility that a relatively simple intervention—intermittent exposure to a simulated altitude initi-ated days after coronary artery occlusion—may offer profound benefits to patients with acute MI (10).
Published studies have indicated that long-lasting IHH might provide a unique and promising preventive and therapeutic approach for treat-ing ischemic heart disease (1, 2, 9, 10). IHH appears to protect the heart by activating an intrinsic defensive system and integrating multiple tar-gets to deal with injurious stimuli (Figure 1), but further studies are
required to dissect the mechanisms involved, especially those related to transcriptional, post-transcriptional, and post-translational regulation. More work is also required to confirm the therapeutic effect on MI and to identify a suitable cycle length, number of hypoxic episodes per day, degree and duration of IHH, and suitable MI candidates for IHH. The knowledge derived from these studies should provide new insights into understanding the intrinsic defensive mechanism and new therapeutic approaches for protecting the heart against ischemic diseases and other stresses.
REFERENCES1. H.-T.Yang,Y.Zhang,Z.H.Wang,Z.N.Zhou,in Intermittent Hypoxia
and Human Diseases, L. Xi, T. V. Serebrovskaya, Eds. (Springer, New York,2012),pp.47-58.
2. Y. Xie et al., Am. J. Physiol. Heart. Circ. Physiol. 288, H2594 (2005). 3. L. Chen et al., Am. J. Physiol. Cell. Physiol. 290, C1221 (2006).4. Y. Xie et al., Life Sci. 76, 559 (2004).5. W.Z.Zhu,Y.Xie,L.Chen,H.T.Yang,Z.N.Zhou,J. Mol. Cell. Cardiol.
40, 96 (2006). 6. Z. H. Wang et al., Exp. Physiol. 97, 1105 (2012).7. Z. Yu, Z. H. Wang, H. T. Yang, Am. J. Physiol. Heart. Circ. Physiol. 297,
H735 (2009). 8. Z. H. Wang et al., Am. J. Physiol. Heart. Circ. Physiol. 301, H1695
(2011). 9. W. Q. Xu et al., Basic. Res. Cardiol. 106, 329 (2011).10. K. Przyklenk, P. Whittaker, Basic. Res. Cardiol. 106, 325 (2011).
ACKNOWLEDGMENTSThese studies were supported by the Major State Basic Research Development Program of China (Grant No. 2012CB518203 and 2006CB504106), the National Science and Technology Major Project (Grant No. 2012ZX09501001), Major and General Programs of the National Natural Sciences Foundation of China (Grant No. 81170119, 30393133, and 30370536), and the Knowledge Innovation Program of the Chinese Academy of Sciences (Grant No. KSCX2-YW-R-75).

Sect ion Two
49
Section Two
Self-renewing neural stem cells (NSCs) are present
throughout the develop-ing and adult mammalian brain and can differenti-ate in vitro into neurons, astrocytes, or oligoden-drocytes (1). The prolif-eration of NSCs in vitro is regulated by various factors. However, studies using oxygen microelec-trodes have shown that the mammalian embryo develops in the uterus in a hypoxic environment and NSCs in the brain are in a hypoxic niche (2, 3). The mean oxygen concentration is approximately 1%–5% in tissues. Currently, standard in vitro culture studies using NSCs have primarily been performed under atmospheric conditions of 20% oxygen (4). This indicates that oxygen concentrations used in tra-ditional cell culture systems may form a hyperoxic environment, but not the conditions of “physiological hypoxia” that most cells are ex-posed to in situ. Herein, we describe a series of experiments that tested whether exogenous hypoxia could impact the growth, regulation, and function of NSCs and to identify the molecular mechanisms involved.
First, we compared the effect of different exogenous oxygen concen-trations on NSCs growth in vitro. Embryo-derived NSCs were cultured under 3%, 10%, or 20% oxygen concentrations for one, two, or three days (Figure 1). There was an approximately two- to five-fold increase in the number of NSCs cultured after exposure to hypoxia conditions (10% oxygen) compared with normal conditions (20%). Mild hypoxia dramatically promoted the proliferation of NSCs and decreased lev-els of apoptosis (5, 6). These results were confirmed using mouse and human-derived NSCs from embryos and adults, which revealed that the growth of NSCs in vitro is optimal in a culture environment of 1% to 10% oxygen. Additionally, mild hypoxia could also dramatically in-crease the in vitro proliferation of mesenchymal stem cells (MSCs) and myoblasts while inhibiting the proliferation of embryonic stem cells (ES) and P19 cell lines when grown in 3%, 5%, or 10% oxygen (3, 7). Thus, mild hypoxia (1%–10% oxygen) is a more potent trigger to pro-mote the proliferation of adult stem cells than normoxia (20% oxygen), suggesting that mild hypoxia could provide a novel methodology for the expansion of various adult stem cells in vitro.
We further examined the differentiation ability of NSCs expanded under hypoxia conditions in vitro (8). NSCs were cultured in a 3% oxygen environment for three days, and differentiated with 1% fetal bovine serum (FBS) for another five–seven days. The cell lineage was
Institute of Basic Medical Sciences, Academy of Military Medical Sciences, Beijing, China.*Corresponding author: [email protected]
Mild Hypoxia Regulates the Properties and Functions of Neural Stem Cells In VitroZhu Ling-Ling, Wu Li-Ying, Wu Kui-Wu, Fan Ming*
evaluated by immunohistochemistry, flow cytometry, and high-perfor-mance liquid chromatography. NSCs cultured in hypoxia (3% oxygen) displayed an increase in the percentage of neurons, especially the per-centage of tyrosine hydroxylase (TH)-positive neurons, compared with NSCs grown in normal conditions. Dopamine (DA) levels in the su-pernatant of the hypoxia culture group were two-fold higher than in the normoxia group (Figure 2). Mild hypoxia may also promote the differentiation of MSCs and P19 cells into dopaminergic neurons, as demonstrated by TH staining and DA measurement (3, 7). Thus, this study identified a new approach to yield DA neurons by manipulating the physical environment.
Taken together, we demonstrated that low oxygen conditions signifi-cantly promotes the proliferation of NSCs and supports self-renewal in vitro. However, the molecular mechanisms underlying hypoxia-driven proliferation are yet unknown. To address this question, a cDNA micro-array containing 5,704 rat genes was used to characterize gene expres-sion patterns during hypoxia-driven proliferation of NSCs (9). Of the 5,704 genes examined, 49 were downregulated less than 0.5-fold and 22 were upregulated more than two-fold at 24 hours. At 72 hours, 60 genes were upregulated and 11 were downregulated. The percentage of genes with altered expression at each time point was approximately 1.24%. A greater number of differentially expressed genes were down-regulated at 24 hours, while at 72 hours, more where upregulated. Of the 71 differentially expressed genes identified at 24 hours, the great-est number were involved in glycolysis and metabolism (36%), fol-lowed by transcriptional regulation (15%), and cell organization and
FigureÊ 1.Ê HypoxiaÊ promotedÊ theÊ proliferationÊ ofÊ embryonicÊ NSCs.Ê (A)Ê PhaseÊ contrastÊ imagesÊ ofÊ neurospheresÊ formedÊunderÊ normoxicÊ (20%Ê oxygen)Ê conditions.Ê (B)Ê PhaseÊ contrastÊ imagesÊ ofÊ neurospheresÊ formedÊ underÊ hypoxicÊ (10%Êoxygen)Ê conditions.Ê (C)Ê TheÊ numberÊ ofÊ neurospheresÊ producedÊ underÊ hypoxicÊ conditions,Ê especiallyÊ 10%Ê oxygen,Êincreased significantly compared with controls. The data represent the mean ± SD (n = 4). *p<0.05, **p<0.01, compared withÊ controlsÊ (20%Ê oxygen).Ê ScaleÊ barÊ =Ê 100Ê μm.

50
Hypoxic Physiology
biogenesis (10%). NSCs under low oxygen consumed more glucose and produced energy by glycolysis (9). This gene expression pattern indicates that although the expression of most genes does not change under conditions of hypoxia, NSCs are able to adapt quickly to low oxygen environments. The information gained from gene expression and metabolic changes of NSCs under low oxygen conditions will pro-vide new approaches for the evaluation of NSCs as potential in vivo cellular therapeutics.
Hypoxia-inducible factor (HIF)-1, a key transcription factor during hypoxia, is important in mediating a variety of adaptive cellular and systemic responses to hypoxia by regulating the expression of more than 50 genes. We also demonstrated that the effects of mild hypoxia on proliferation and differentiation of NSCs were mediated by the hy-poxia-inducible transcription factor-1 alpha (HIF-1α) pathway in vitro by overexpression and downregulation of HIF-1α in the cultured NSCs following hypoxia (5, 6). The above differentially expressed genes were regulated directly or indirectly by HIF-1. Additionally, hypoxia-induced small non-coding RNA (ncRNA) was shown to be involved in the regulation of NSC proliferation (10). The results of significance analysis of microarrays revealed that 15 small RNAs were upregulated at least three-fold and 11 were downregulated in NSCs after being sub-jected to hypoxic conditions. MiR-210 was highly expressed in NSCs in a time- and oxygen-dependent manner, and was directly regulated by HIF-1α (10). Hypoxia-induced expression of miR-210 may be involved in regulating apoptosis and proliferation of NSCs under hypoxia. How-ever, further study is required to understand the hypoxia-induced ex-pression of ncRNAs in NSCs.
In summary, our studies demonstrate that mild hypoxia not only
FigureÊ 2. Ê LoweredÊ oxygenÊ concentrationÊincreasedÊ theÊ yieldÊ ofÊ tyrosineÊ hydroxylaseÊ (TH)-positiveÊ neuronsÊ andÊ dopamineÊ (DA)Ê content.Ê (A)RepresentativeÊ imagesÊ ofÊ THÊ andÊ Tuj1Ê double-labeledÊ cellsÊ differentiatedÊ fromÊ NSCsÊ underÊnormalÊ conditions.Ê (B)Ê RepresentativeÊ imagesÊ ofÊTHÊ andÊ Tuj1Ê double-labeledÊ cellsÊ differentiatedÊfromÊ NSCsÊ underÊ 3%Ê oxygen.Ê ScaleÊ barÊ =Ê 25Êμm.Ê (C)Ê TheÊ numberÊ ofÊ TH-positiveÊ neurons.Ê (D)LoweredÊ oxygenÊ concentrationÊ increasedÊ DAÊyieldÊ inÊ supernatants,Ê asÊ detectedÊ byÊ HPLC.ÊEachÊ barÊ representsÊ theÊ meanÊ ±Ê SDÊ (nÊ =Ê 4).Ê**p≤0.01 compared with controls.
promotes the self-renewal ability of NSCs in vitro, but also increases their differentiation ability into neurons. Therefore, mild hypoxia could become a potential approach for allograft cell transplantation by induc-ing the expansion of NSCs in vitro or by modifying NSC properties in situ. We hope these findings will aid in the transplantation of NSCs to treat neurodegenerative diseases such as Parkinson’s disease and brain trauma.
REFERENCES 1. G. Kempermann, L. Wiskott, F. H. Gage, Curr. Opin. Neurobiol. 14, 186
(2004). 2. K. Zhang, L. L. Zhu, M. Fan, Front. Mol. Neurosci. 4, 1 (2011).3. L. L. Zhu, L. Y. Wu, D. T. Yew, M. Fan, Mol. Neurobiol. 31, 231 (2005).
4. A. Mohyeldin, T. Garz— n-Muvdil, A. Qui–ones-Hinojosa, Cell Stem Cell 7, 150 (2010).
5. T. Zhao et al., FEBS J. 275, 1824 (2008). 6. L. Xiong et al., Cell Stress and Chaperones 14, 183 (2009).7. L.Y.Wuet al., Neurochemical Res. 33, 2118 (2008). 8. C. Zhang, T. Zhao, L. Wu, L. L. Zhu, M. Fan, Neurosignals 15, 259
(2007). 9. L. L. Zhu et al., Cell Reprogram. 13, 113 (2011).10. Z. H. Liu et al., Cell. Mol. Neurobiol. 31, 1 (2011).
ACKNOWLEDGMENTSThis work was supported by grants from the National Basic Research Ò 973Ó Program (Grant No. 2011CB910800 and 2012CB518200) and the National Natural and Sciences Foundation of China (Grant No. 90919025 and 31271205).

Sect ion Two
51
Section Two
High-altitude exposure (HAE) brain and lung edema are com-mon problems among people who ascend to altitudes greater than 2,500 m (1). Currently, the most common method for preventing brain and lung edema is a gradual ascent, but
there are serious drawbacks to this process that make the need for alter-native methods quite urgent.
After hyperbaric oxygen therapy (HBO2T), the body experiences relative hypoxia as the oxygen levels return to a normal level of 21% (normoxia). Therefore, repeated HBO2T treatments may produce a cy-cle of hyperoxia/normoxia, contributing to the accumulation of hypoxia inducing factor (HIF)-1a (2).
Heat shock protein 70 (HSP-70) is upregulated during hypoxia and mediates cell protection and survival (3). Preinduction of HSP-70 pro-motes hypoxic tolerance and facilitates acclimatization to acute HAE in the mouse brain. Hyperbaric oxygen preconditioning (HBO2P), similar to hypobaric hypoxia, significantly reduces pulmonary edema in rats caused by HAE (4). Thus, it is likely that HBO2P or hypobaric hypoxia preconditioning (HHP) can reduce lung and brain edema, and cognitive dysfunction in HAE by upregulating HSP-70 expression.
In our study, rats were randomly assigned to one of three treatment groups as follows: (i) HHP (18.3% O2 at 0.66 atmosphere absolute (ATA) for five hours per day, five consecutive days for two weeks); (ii) non-HHP (21% O2 at 1.0 ATA for five hours per day, five consecutive days for two weeks); (iii) NBA (normobaric air; 21% O2 at 1.0 ATA). One week after HHP, the HHP group was subjected to simulated HAE. A neutralizing polyclonal rabbit anti-mouse HSP-70 antibody (Ab; 0.2 mg/kg of body weight) dissolved in non-pyrogenic sterile saline was intravenously administered to some HHP or non-HHP rats 24 hours be-fore simulation of HAE (6,000 m; 9.8% O2 at 0.47 ATA) in a hypobaric chamber for 24 hours (4, 5). Western blot analyses revealed that HSP-70 protein expression in lung tissue was significantly higher in the HHP group compared with the non-HHP group (6), and significantly lower in the HHP+HSP-70 Ab group compared with the HHP group (6). The injury scores, including edema, neutrophil infiltration and hemorrhage, were significantly higher in the non-HHP group than in NBA controls after 24 hours of HAE (Figure 1). However, the HHP group had signifi-cantly lower scores for acute lung injury than the non-HHP group (6). Additionally, HHP reduced acute pleurisy and decreased lung myelo-peroxidase activity and bronchoalveolar fluid levels of pro-inflammato-ry cytokines, glutamate, glycerol, 2,3-dihydroxybenzoic acid (DHBA), and nitric oxide metabolites after HAE (6). These protective effects of HHP were significantly reduced by administration of a neutralizing anti-HSP-70 Ab (Figure 1). Thus, HHP-induced upregulation of lung HSP-70 might attenuate HAE-induced acute lung injury or edema.
In a second experiment, groups of eight rats were randomly assigned to the following groups: non-HBO2P+non-HAE; HBO2P+non-HAE; non-HBO2P+HAE; HBO2P+HAE; and HBO2P+HSP-70Ab+HAE. The HBO2P groups were administered 100% O2 at 2.0 ATA for 1 hour daily for five consecutive days. The HAE groups were exposed to simulated HAE in a hypobaric chamber for 24 hours. Immediately after returning to NBA, the rats were given cognitive performance tests, overdosed
Department of Medical Research, Chi Mei Medical Center and Department of Biotechnology, Southern Taiwan University of Science and Technology, Tainan, Taiwan, China.*Corresponding author: [email protected]
FigureÊ 1. HistologicalÊ examinationÊ ofÊ lungÊ tissueÊ fromÊ normobaricÊairÊ (NBA),Ê non-hypobaricÊ hypoxiaÊ preconditioningÊ (HHP),Ê HHPÊ andÊHHP+HSP-70Ê AbÊ rats.Ê (A)Ê RepresentativeÊ imagesÊ ofÊ ratÊ lungÊ fromÊ NBAÊ(upperÊ leftÊ panel),Ê non-HHPÊ (upperÊ rightÊ panel),Ê HHPÊ (lowerÊ leftÊ panel)ÊandÊ HHP+HSP-70Ê AbÊ groupsÊ (lowerÊ rightÊ panel).Ê (B)Ê AcuteÊ histologicalÊscoreÊ forÊ NBAÊ (whiteÊ bar),Ê non-HHPÊ (stripedÊ bar),Ê HHPÊ (hatchedÊ bar),Ê andÊHHP+HSP-70Ê AbÊ groupsÊ (blackÊ bar).Ê TheÊ non-HHPÊ ratsÊ hadÊ interstitialÊedema,Ê neutrophilÊ accumulation,Ê andÊ hemorrhage.Ê TheÊ lungÊ pathologicalÊchanges caused by HAE were significantly attenuated by HHP (p<0.05). ResultsÊ areÊ meanÊ ±Ê S.D.Ê (nÊ =Ê 8).Ê *p<0.05,Ê comparedÊ withÊ theÊ NBAÊ group;Ê+p<0.05,Ê comparedÊ withÊ theÊ non-HHPÊ group;Ê ¤ p<0.05Ê comparedÊ withÊ theÊHHP+HSP-70Ê AbÊ group.
Hypobaric Hypoxia or Hyperbaric Oxygen Preconditioning Reduces High-Altitude Lung and Brain Injury in RatsLin Hung-Jung, Chang Ching-Ping, Niu Ko-Chi, Lin Mao-Tsun*
A
B

52
Hypoxic Physiology
with a general anesthetic, and then their brains were ex-cised for water content measurement and biochemical evaluation and analysis. Western blot analysis demon-strated that the HBO2P group had significantly higher hippocampal expression of HSP-70 than the non-HBO2P group (p<0.01) (7), and the HBO2P+HSP-70 Ab group had significantly lower hippocampal HSP-70 protein expression levels than the HBO2P group without HSP-70 Ab (p<0.05) (7). Behaviorally, the non-HBO2P+HAE group had a significantly lower latency in cognitive function tests than the non-HBO2P controls (Figure 2A). HAE-induced cognitive dysfunction was significantly attenuated in the HBO2P+HAE group, but HBO2P bene-fits were significantly attenuated in the HBO2P+HSP-70 Ab group. After three days of HAE, when the brain had developed edema, the brain weight was higher in the non-HBO2P+HAE group than in the non-HBO2P+NBA control group (Figure 2B). Brain weight was signifi-cantly lower in the HBO2P+HAE group than in the non-HBO2P+HAE group (p<0.05). Additionally, the HBO2P benefits were significantly attenuated (p<0.05) in the HBO2P+HSP-70 Ab pretreatment group. Oxidative stress markers including DHBA, mono-nitrogen oxides (NOx), and lipid peroxidation levels in the hippocam-pus of the non-HBO2P+HAE group were significantly increased (p<0.05) after 24 hours of HAE (Figure 2C, D, E) compared with the NBA control group. Hippocampal levels of DHBA, NOx, and lipid peroxidation were significantly lower (p<0.05) in the HBO2P+HAE group than in the non-HBO2P+HAE group. The HBO2P+HSP-70 Ab pretreatment group showed a reduc-tion in the benefit of HHP treatment (Figure 2), strongly indicating that the increased HSP-70 levels before HAE injury might be beneficial. This suggested that the HSP-70 Ab could cross the blood-brain-barrier and neutralize HSP-70 expressed in the brain before inhibiting anti-apoptosis (5).
These results confirm the findings from previous studies. For exam-ple, prolonged and intermittent normobaric hyperoxia preconditioning caused ischemic tolerance in rat brain tissue (8); preinduction of HSP-70 by geranylgeranylacetone improved survival rate of mice exposed to sublethal hypoxia for six hours, prevented acute hypoxic brain dam-age, and was involved in mediating these benefits (9); and hypobaric hypoxia preconditioning in rats attenuated experimental heatstroke syndromes by preinducing HSP-70 (10).
In conclusion, HHP or HBO2P might attenuate the occurrence of pul-monary edema, inflammation, ischemic and oxidative damage, brain edema and oxidative damage, and cognitive deficits caused by HAE partly by upregulating HSP-70 in the lungs and brain.
REFERENCES 1. P. BŠ rtsch, R. C. Roach, N. Engl. J. Med. 245, 107 (2001). 2. A. Qui–ones-Hinojosa et al., J. Com. Neurol. 494, 415 (2006). 3. D. K. Das, N. Maulik, I. I. Moraru, J. Mol. Cell Cardiol. 27, 181 (1995). 4. Z. Li et al., J. Trauma 71, 673 (2011). 5. B. Liebelt et al., Neuroscience 166, 1091 (2010). 6. H. J. Lin et al., Clinical Sci. 121, 223 (2011). 7. H. Lin, C. P. Chang, H. J. Lin, M. T. Lin, C. C. Tsai, J. Trauma 72, 1220
(2012). 8. M. R. Bigdeli et al., Brain Res. 1152, 228 (2007). 9. K. Zhang et al., Cell Stress Chaperones 14, 407 (2009).10. L. C. Wang et al., Am. J. Med. Sci. (2012).
Doi: 10.1097/MAJ.0b013e31824314fe (2012).
ACKNOWLEDGMENTSThis work was supported in part by the National Science Council of China (Grant No. NSC 99-2314-B-384-006-MY2, NSC 99-2314-B-384-004-MY3,andNSC98-2314-B-218-MY2)andtheDepartmentofHealthofChina(Grant No. DOH99-TD-B-111-003, the Center of Excellence for Clinical Trial and Research in Neuroscience).
FigureÊ 2.Ê EffectÊ ofÊ high-altitudeÊ exposureÊ onÊ cognition,Êedema,Ê andÊ serumÊ oxidativeÊ stressÊ molecules.Ê (A)ÊLatencyÊ periodÊ beforeÊ enteringÊ theÊ darkÊ compartmentÊ inÊaÊ passiveÊ avoidanceÊ test;Ê (B)Ê percentageÊ changeÊ ofÊ brainÊweight,Ê andÊ oxidativeÊ stressÊ markers;Ê (C)Ê 2,3-DHBA;Ê (D)ÊlipidÊ peroxidation;Ê andÊ (E)Ê nitricÊ oxideÊ metabolitesÊ (NOx)Êfor all five groups were measured. *p<0.05, compared withÊ theÊ non-HBO2P+NBAÊ group;Ê +p<0.05,Ê comparedÊ withÊtheÊ non-HBO2P+HAEÊ group;Ê ¤ p<0.05,Ê comparedÊ withÊ theÊHBO2P+HAEÊ group.Ê EachÊ barÊ representsÊ theÊ meanÊ ±Ê SEMÊofÊe ightÊr atsÊ perÊ group.

Sect ion Two
53
Section Two
Mitochondria: A Potential Target in High-Altitude Acclimatization/Adaptation and Mountain SicknessGao Wenxiang1,2, , Luo Yongjun1,2, , Cai Mingchun1,2, Liu Fuyu1,2, Jiang Chunhua1,2, Chen Jian1,2, Gao Yuqi1,2,*
1) (5). The activity of mitochondrial complexes I, II, and III; placental energy charge; and mitochondrial ATP/ADP ratios were higher in the native Tibetans than in the immigrant Han, probably because of higher AAC activity and MMP in the placental mitochondria of native Tibetans (Figure 1) (unpublished data). The differences between the two groups may result from dissimilar gene and protein expression, as a set of dif-ferentially expressed genes related to pathways of energy metabolism, signal transduction, cell proliferation, electron transport, cell adhesion, and nucleotide-excision repair were identified by cDNA array (6). Fur-thermore, differences in the mitochondrial proteomes of skeletal muscle were also observed between the plateau pika (5,000 m) and Wistar rats (5,000 m for 30 days).
We further analyzed mitochondrial DNA (mtDNA) sequences from native high altitude residents, including Tibetans, as well as the plateau pika and the Tibetan wild donkey. We found that the nt3010G-nt3970C haplotype was positively associated with high-altitude adaptation in Tibetans, while the D4 haplogroup was negatively associated (7). In the pika, there were 15 species of pika-specific amino acids in mtDNA encoded proteins, including two α-helix amino acid replacements (posi-tions 146 and 408), which caused a polarity switch from hydrophilic to hydrophobic amino acids in cyclooxygenase-1 (COX1), and an amino acid change at locus 47 in the mitochondrial matrix region. These amino acid substitutions can affect the generation of NO via modification of complex IV structure and alteration of cytochrome c oxidase activity (8). Moreover, 16 amino acid substitutions were found in mtDNA-en-coded proteins in the Tibetan wild donkey when compared with Equus asinus and Equus caballus, including three in NADH dehydrogenase subunit 4 (ND4) and ND5 (9).
To confirm the critical role of mitochondria in hypoxic responses, we analyzed the correlation of mtDNA variations and maladaptation at high altitude (i.e., mountain sicknesses). We found that the mtDNA 3397G and 3552A genotypes correlated with susceptibility to high altitude pul-monary edema (HAPE) (10), and a recently identified mtDNA genotype significantly decreased the risk of high altitude polycythemia (HAPC) in Han Chinese migrating to the plateau (unpublished data). This sug-gests that the mtDNA variations are involved in the pathogenesis of both acute (HAPE) and chronic (HAPC) mountain sickness.
In addition, there is also evidence for changes in mtDNA biogenesis during high altitude acclimatization. For example, low-altitude Han sperm mtDNA content reached a peak one month after ascent to a high altitude (5,300 m) (11), while liver mtDNA content was decreased in chronic hypoxia rats (5,000 m for 30 days) (12).
1College of High Altitude Military Medicine, Third Military Medical Univer-sity; 2Key Laboratory of High Altitude Medicine, Ministry of Education, Third Military Medical University, Chongqing, China.*Corresponding author: [email protected]†Contributed equally to this work.
Hypobaric hypoxia is a primary cause of pathophysiological changes at high altitude, and affects oxygen intake, transpor-tation, and utility. Mitochondria are critical organelles that consume high levels of oxygen and generate ATP via sub-
strate dehydrogenation and oxidation, as well as oxidation phosphoryla-tion (1). Therefore, we hypothesized that the mitochondrion may be at the center of hypoxic responses in high altitude acclimatization/adapta-tion and mountain sickness.
Effect of Hypoxia on MitochondriaFirst, we found that acute hypoxia could impair mitochondrial structure and function. In acute hypoxic rats (housed at the equivalent of 4,000 m for three days), cerebral cortex mitochondria increased in size with swelling, rupture, and lysis of cristae, but mitochondrial numbers were not affected. Oxygen consumption state 3 (ST3, with ADP), respiratory control rate (RCR), and the activities of inner membrane complexes were decreased, while state 4 (ST4, ADP depleted) and uncoupling protein (UCP) activity was elevated. ATP synthesis efficiency was impaired as shown by decreased phosphate-oxygen ratios (P/O), F0F1-ATPase activity, and ATP levels in cellular and mitochondrial adenine nucleotide pools (2). Furthermore, acute hypoxic exposure can depress mitochondrial ATP/ADP transportation, as shown by decreased ATP/ADP carrier (AAC) activity and mitochondrial membrane potential (MMP) (3). Mitochondrial RNA and protein synthesis was also impaired in isolated rat brain mitochondria under conditions of acute hypoxia (4).
During prolonged hypoxia, the organism acclimatizes to the hypoxic environment and mitochondria exhibit gradual acclimatization changes. Mitochondrial ultrastructure and numbers were not different compared with normal controls in chronic hypoxic rat brain (4,000 m for 30 days). In the heart (4,000 m for 30 days) and brain (5,000 m for 30 days) of rats, ST3 and RCR levels were still low, but ST4 returned to normal levels. Mitochondrial complex activity, P/O, ATP synthesis, the mito-chondrial adenine nucleotide pool, AAC activity, and MMP were higher in rats with chronic hypoxia than with acute hypoxia and lower than in normal rats (2, 3). Mitochondrial RNA and protein synthesis in isolated mitochondria from chronic hypoxic rats were also partially restored (4).
The Role of GeneticsConstant hypobaric hypoxia exposure over many generations has been hypothesized to induce long-term genetic adaptation to high altitude. Native Tibetans, who have resided at high altitude for thousand of years, are considered the population best adapted to high altitudes. We found placental mitochondria to be considerably swollen in unacclimatized Han Chinese individuals who migrated to high altitudes, while mito-chondria in native Tibetans who live at a similar high altitude were in-tact with only partial swelling and vacuolization (Figure 1). Measures of placental mitochondrial oxidative phosphorylation function, such as ST3, RCR, the oxidative phosphorylation ratio (OPR), and ATP synthe-sis were higher in native Tibetans than in the immigrant Han popula-tion, and only ST4 was not different between the two groups (Figure

54
Hypoxic Physiology
SummaryIn summary, mitochondrial structure, oxidative phosphorylation, and ATP synthesis efficiency are involved in the processes of acute impair-ment and chronic acclimatization of migrating (Han Chinese) lowland-ers, as well as genetic adaption of native (Tibetan) residents at high al-titudes. However, individuals with certain mtDNA variations are prone to show maladaptation to hypoxia and are susceptible to mountain sicknesses. Further research focusing on the mitochondrial genome and function is required, which may lead to new strategies for the prediction and treatment of mountain sickness.
REFERENCES 1. V. Donald et al., Fundamentals of Biochemistry, 2nd Edition, (John Wiley
and Sons, Inc. 2006), p. 547. 2. G. Luo, Z. Xie, F. Liu, G. Zhang, Acta. Pharmacol. Sin. 19, 351 (1998). 3. C. Li, J. Liu, L. Wu, B. Li, L. Chen, World J. Gastroenterol. 12, 2120
(2006). 4. J. Liu, et al., Sheng Li Xue Bao 54, 485 (2002).
5. X. Zhao, W. Gao, Y. Gao, L. Suo, J. Chen, Nat. Med. J. China 87, 894 (2007).
6. Y. Luo et al., J. Med. Coll. PLA. 24, 88 (2009).7. Y.Luo,W.Gao,F.Liu,Y.Gao,Mitochondr. DNA 22, 181 (2011).8. Y. Luo et al., Mitochondrion 8, 352 (2008).9. Y.Luo,Y.Chen,F.Liu,Y.Gao,Asia Life Sci. 21, 1 (2012).10. Y. Luo, W. Gao, Y. Chen, F. Liu, Y. Gao, Wild. Environ. Med. 23, 128
(2012).11. Y. Luo et al., J. Assist. Reprod. Genet. 28, 951 (2011).12. Y.Luoet al., Eur. J. Appl. Physiol. (2012). doi: 10.1007/s00421-012-
2414-9.
ACKNOWLEDGMENTSThis work was supported by the National Basic Research Ò 973Ó Programof China (Grant No. 2012CB518201), the National Natural Science Foundation of China (Grant No. 81071610 and 30971426), and the Key Project of National Science and Technology Ministry of China (Grant No. 2009BAI85B01).
FigureÊ 1.Ê DifferencesÊ inÊ placentalÊ mitochondrialÊ ultrastructureÊ andÊ functionÊ inÊ immigrantÊ HanÊ ChineseÊ andÊ nativeÊ TibetansÊ atÊ highÊ altitudeÊ (3,650Ê toÊ4,450Ê m).Ê (A)Ê RepresentativeÊ photographsÊ ofÊ placentalÊ ultrastructureÊ inÊ immigrantÊ HanÊ andÊ nativeÊ Tibetans.Ê (B Ð I)Ê TheÊ placentalÊ mitochondrialÊ ST3Ê (B),ÊRCRÊ (D),Ê OPRÊ (E),Ê energyÊ chargeÊ ofÊ placentalÊ adenylateÊ poolÊ (F),Ê ATP/ADPÊ ratiosÊ inÊ theÊ placentalÊ mitochondrialÊ adenylateÊ poolÊ (G),Ê MMPÊ (H),Ê andÊ AACÊactivity (I) were significantly higher in native Tibetans than in immigrant Han Chinese, while ST4 (C) was not statistically different. *p<0.05 relative to immigrantÊ Han,Ê **p<0.01Ê relativeÊ toÊ immigrantÊ Han.

Sect ion Two
55
Section Two
FigureÊ 1.Ê Expres-sionÊ ofÊ p-GSK,Êp-ERK/t-ERK,Ê HIF-1a,Ê andÊ EPO.Ê (A-D)Ê CellsÊ wereÊ pre-incubatedÊ withÊ orÊwithoutÊ 100Ê mmol/LÊofÊ PD98059Ê (aÊ spe-cific MEK inhibi-tor)Ê orÊ 50Ê mmol/LÊ ofÊLY294002 (a specific PI3KÊ inhibitor)Ê forÊoneÊ hourÊ andÊ thenÊadministeredÊ hy-poxiaÊ (0Ê orÊ 16Ê hours)Êor Ê ginkgolidesÊ(37.5Ê mg/mLÊ forÊ 24Êhours).Ê TheÊ expres-sionÊ ofÊ p-GSKÊ (A),Êp-ERK/t-ERKÊ (B),ÊHIF-1a Ê (C),Ê andÊ EPOÊ(D)Ê wasÊ analyzedÊbyÊ westernÊ blot.Ê 0h:ÊcontrolÊ group;Ê HP:Ê16-hourÊ hypoxiaÊp r e c o n d i t i o n i n g ;ÊGin:Ê ginkgolidesÊ forÊ24Ê hours;Ê PD/HP:ÊPD98059Ê oneÊ hourÊ +ÊHP;Ê LY/HP:Ê LY294002ÊoneÊ Ê hourÊ +Ê HP;Ê PD/Gin:Ê PD98059Ê oneÊhourÊ +Ê ginkgolidesÊforÊ 24Ê hours;Ê andÊ LY/Gin:Ê LY294002Ê oneÊhourÊ +Ê ginkgolidesÊforÊ 24Ê hours.Ê TheÊdataÊ areÊ presentedÊ asÊ meanÊ ±Ê SEMÊ (nÊ =Ê 3).Ê *p<0.005,Ê **p<0.001Ê versusÊ controls;Ê #p<0.005Ê versusÊ HP;Ê @p<0.005Ê versusÊ Gin.Ê (EÐ G)Ê LigustilideÊ (LIG)ÊprotectedÊ brainÊ fromÊ injuryÊ inducedÊ byÊ ischemia-reperfusionÊ inÊ rats.Ê (E) Neurological deficit score. (F)Ê RepresentativeÊ imagesÊ ofÊ brainÊ slicesÊ stainedÊwithÊ 2,3,5-triphenyltetrazoliumÊ chloride.Ê (G)Ê InfarctÊ volumeÊ expressedÊ asÊ theÊ percentageÊ ofÊ brainÊ volume.Ê AnimalsÊ wereÊ subjectedÊ toÊ shamÊ operationÊ(i),Ê administrationÊ ofÊ vehicleÊ onlyÊ (ii),Ê nimodipineÊ atÊ aÊ doseÊ ofÊ 12Ê mg/kgÊ (iii),Ê ligustilideÊ atÊ aÊ doseÊ ofÊ 20Ê (iv),Ê 40Ê (v),Ê orÊ 80Ê mg/kgÊ (vi)Ê atÊ threeÊ hoursÊ andÊ 0.5ÊhoursÊ beforeÊ undergoingÊ middleÊ cerebralÊ arteryÊ occlusionÊ forÊ twoÊ hoursÊ followedÊ byÊ 24Ê hourÊ reperfusion.Ê ParametricÊ dataÊ areÊ presentedÊ asÊ meanʱÊS EMÊ (nÊ =Ê 6)Ê andÊ non-parametricÊ dataÊ asÊ boxÊ andÊ whiskerÊ plotsÊ withÊ theÊ minimumÊ andÊ maximumÊ valuesÊ (nÊ =Ê 9).Ê *p<0.05,Ê **p<0.01Ê versusÊ vehicle.
Preconditioning was first described in a dog model of myocar-dial injury in which sublethal ischemia enabled cells to better tolerate subsequent induction of usually lethal ischemia (1). A number of studies have demonstrated that preconditioning
induced by ischemia or hypoxia can produce a significant protective ef-fect for neurons in experimental animals and humans (2). Ischemic tol-
nomenon of preconditioning has received much attention because of its potential therapeutic importance (4). However, hypoxic or ischemic preconditioning has not been used clinically because of safety concerns (1). Therefore, it is desirable to find a safe preconditioning stimulus that is both practical and effective, or a biological agent that can mimic preconditioning pharmacologically (4, 5).
Mimicking Hypoxic Preconditioning Using Chinese Medicinal Herb ExtractsQian Zhongming1 and Ke Ya2,*
1Department of Pharmacology, Fudan University School of Pharmacy, Shanghai, China;2School of Biomedical Sciences, Faculty of Medicine, The Chinese University of Hong Kong, Shatin, Hong Kong, China.*Corresponding author: [email protected]
erance induced by hypoxic preconditioning in rodent brains is at least in part due to the induction of hypoxia-inducible factor-1 (HIF-1) and its target genes (3). Indeed, it is now recognized that this phenomenon can be induced in the central nervous system not only by ischemia and hypoxia (1), but also by a number of other stimuli including hyper-thermia (2) and hypothermia (3). During the last few years, the phe-

56
Hypoxic Physiology
Ginkgolides are the main constituents of the nonflavone standard-ized extract (EGb 761) from Ginkgo biloba (Ginkgoaceae), which has been used as a Chinese herbal medicine for thousands of years and shown to exert a wide range of biological activities. There is substantial experimental evidence to support a role for EGb 761 in the neuropro-tective properties of the Ginkgo biloba leaf (6). Thus, we investigated whether ginkgolides can act as a safe preconditioning agent to protect ischemic/hypoxic brain cells. We found that ginkgolides could protect brain cells subject to lethal hypoxia or ischemia treatment (6–8). We hypothesized that this protective effect of ginkgolides, similar to that of hypoxic preconditioning, was due to changes in the content or transac-tivity of hypoxia-inducible factor-1 alpha (HIF-1a) and its downstream gene targets. Indeed, our experiments demonstrated that the protective effect of ginkgolides pre-treatment in hypoxic cells was accompanied by elevated levels of HIF-1a, HIF-1 DNA-binding activity, and eryth-ropoietin (EPO) (6–8).
Additional studies demonstrated that both pretreatment with ginkgolides and hypoxic preconditioning could increase the expression of phosphorylated glycogen synthase kinase (p-GSK) and phosphory-lated extracellular signal-regulated kinase (p-ERK) in brain cells (Fig-ure 1, A–D). These results suggested that ginkgolides upregulate HIF-1 transcriptional activity, leading to increased expression of EPO, via the MEK/ERK and PI3/AKT/GSK-3β pathways. We also showed that in-creased expression of these proteins and improved cell viability induced by ginkgolides and hypoxic preconditioning could be significantly in-hibited by PD98059, a specific inhibitor of mitogen-activated protein kinase (MAPK), or LY294002, a specific inhibitor of phosphatidylino-sitol 3’-kinase (PI3K) (Figure 1, A-D). Previous studies demonstrated that EPO, induced by HIF-1, plays a dominant role in neuroprotection after ischemic stroke. Thus, it is likely that EPO and other target genes of HIF-1 also mediate the preconditioning-like effect of ginkgolides.
In our search for more compounds present in traditional Chinese
medicinal herbs that can mimic preconditioning pharmacologically, we tested whether ligustilide has a protective effect against ischemia-reperfusion (I/R) injury in the cerebral circulation in I/R rats in vivo and I/R neurons in vitro (9, 10). Ligustilide is the main constituent of the oil fraction of Radix Angelicae Sinensise, and is the root of An-gelica Sinensis (Oliv.) Diels (Umbelliferae). Additionally, it is believed to be one of the main pharmacologically active compounds of Danggui (9), a popular traditional Chinese medicinal herb that has long been used as a medicinal plant and is included in a number of traditional Sino-Japanese herbal prescriptions. We found that pretreatment with ligustilide reduced the neurological deficit score and infarct volume in a dose-dependent manner in I/R rats in vivo (Figure 1, E-G). In neurons exposed to oxygen-glucose deprivation (OGD) in vitro, ligustilide pre-treatment also increased cell viability with a corresponding decrease in lactate dehydrogenase (LDH) release (9). These observations were accompanied by a significant increase in EPO in I/R rats in vivo, and EPO as well as p-ERK in cultured neurons exposed to OGD in vitro (9). These findings provide evidence for the preconditioning effect of ligustilide and imply that the ligustilide-induced increase in EPO may be mediated by the phosphorylation of ERK.
Together, these results suggest that ginkgolides and ligustilide can serve as pharmacological agents that mimic hypoxic preconditioning and protect brain cells from ischemic/hypoxic injury. These compounds and hypoxic preconditioning may operate through similar mechanisms. As illustrated in the model in Figure 2, these agents and hypoxic pre-conditioning promote the phosphorylation of ERK, leading to an in-crease in the phosphorylation of HIF-1a. The latter, in turn, increases the transcriptional activity of HIF-1 and hence EPO expression. How-ever, the mechanism by which ginkgolides and ligustilide increase the phosphorylation of ERK is unknown. These compounds may also have effects on the stability of HIF-1a. Further research is required to clarify these questions.
Our findings have demonstrated that compounds extracted from tra-ditional Chinese medicinal herbs can mimic hypoxic preconditioning pharmacologically, and have the potential to be developed into safe and effective preventive or therapeutic agents in high-risk conditions including ischemic disorders of the cardiovascular and cerebrovascu-lar systems. Clinical trials based on these findings are warranted. Our findings shed new light on the potential beneficial effects of these com-pounds on the nervous system.
REFERENCES1. L. Yang et al., Biochim. Biophys. Acta Mol. Basis Dis. 1822, 500 (2012).
2. F. Du et al., Biochim. Biophys. Acta Mol. Basis Dis. 1802, 1048 (2010). 3. F. Du et al., Neurochem. Int. 55, 181 (2009). 4. T. W. Stone, Brit. J. Pharmacol. 140, 229 (2003). 5. D. Ma et al., J. Cereb. Blood Flow Metab. 26, 199 (2006). 6. L. Zhu et al., J. Cell. Biochem. 103, 564 (2008). 7. W. He et al., Int. J. Biochem. Cell Biol. 40, 651 (2008). 8. X. M. Wu et al., J. Cell. Mol. Med. 13, 4474 (2009). 9. X. M. Wu et al., Brit. J. Pharmacol. 164, 332 (2011). 10. X. Kuang et al., Brain Res. 1102, 145 (2006).
ACKNOWLEDGMENTSThese studies were supported by the National Natural Science Foundation of China (NSFC) (Grant No. 31271132), the National Basic Research Program of China (Grant No. 2011CB510004) and the Joint Research Grant of the NSFC and the Hong Kong RGC (Grant No. N-CUHK433/08).
FigureÊ 2.Ê ProposedÊ mechanismsÊ forÊ theÊ neuroprotectiveÊ roleÊ ofÊginkgolidesÊ andÊ ligustilide.Ê TheÊ neuroprotectiveÊ effectÊ ofÊ ginkgolidesÊ andÊligustilideÊ againstÊ ischemia-reperfusionÊ injury,Ê similarÊ toÊ thatÊ ofÊ hypoxicÊpreconditioning,Ê isÊ hypothesizedÊ toÊ beÊ mediatedÊ byÊ theÊ upregulationÊofÊ erythropoietin Ê (EPO)Ê andÊ activationÊ ofÊ otherÊ targetÊ genesÊ ofÊ HIF-1.ÊGinkgolidesÊ andÊ ligustilideÊ promote Ê theÊ phosphorylationÊ ofÊ ERKÊ (p-ERK).ÊTheÊ increasedÊ p-ERKÊ thenÊ inducesÊ anÊ increaseÊ inÊ theÊ phosphorylationÊofÊ HIF-1a.Ê TheÊ latterÊ leadsÊ toÊ anÊ increaseÊ inÊ theÊ transcriptionalÊ activityÊofÊH IF-1Ê andÊ theÊ increasedÊ expressionÊ ofÊ EPOÊ andÊ otherÊ targetÊ genes.

Sect ion Two
57
Section Two
Hypoxia, which is the failure to effectively use and regulate oxygen, is involved in the onset of several ischemia/hypoxia-related diseases such as high-altitude sickness, myocardial
infarction, and stroke. Of these disorders, stroke has the highest morbidity and mortality rate, often causing death and disability. Although progress has been made in understanding the pathophysiology of stroke and the time window of thrombolysis has been increased to 4.5 hours, results of clinical trials of pharmacological neuro-protective agents have been disappointing (1, 2). Thus, novel directions such as those involving endogenous strategies are being considered. Ischemic/hypoxic pre-conditioning (I/HPC) is a series of sublethal ischemic/hypoxic exposures that can allow a specific tissue or or-gan to become resistant to subsequent severe ischemic/hypoxic insults (3). The protective mechanism induced by I/HPC is so profound that it has the potential to be a future target of clinical therapeutic approaches, but its molecular mechanism is still unclear (3, 4). Studies have indicated that ischemic/hypoxic exposure activates vari-ous intracellular signaling pathways followed by altered gene and protein expression, which may contribute to early and delayed I/HPC. To elucidate the signal trans-duction pathways activated during cerebral ischemic/hypoxic injury and I/HPC, we chose to investigate pro-tein kinase C (PKC), one of many protein kinases impli-cated, but also an important factor in several pathways that are likely to be involved during ischemic/hypoxic injury.
Determination of PKC-Isoforms and Downstream Members in Cerebral Ischemic/ Hypoxic Injury and I/HPC DevelopmentPKC has been suggested to be involved during cerebral ischemic/hy-poxic injury and I/HPC development. However, because of the biologi-cal complexity and dual characteristics of PKC isoforms, there is a lack of detailed information on individual PKC isoforms in relation to neural protection or damage. Using our established “auto-hypoxia”-induced I/HPC mouse model, and hypoxic neuronal cells, we found that among the 10 PKC isoforms, conventional PKC (cPKC) bII, g, and novel PKC epsilon (nPKCe) showed increased membrane translocation, even though protein expression levels were unchanged (4, 5).
Kinases downstream of PKC that may also be important in cerebral I/HPC include the mitogen-activated protein kinase (MAPK) family that consists of three groups: extracellular signal-regulated kinases (ERK), c-Jun N-terminal kinases (JNK), and p38 MAPK. During the early phase of I/HPC, ERK1/2 phosphorylation decreased in the hippocam-pus and frontal cortex of mice, while in the late phase, protein levels
Department of Neurobiology, Beijing Key Laboratory for Neural Regeneration and Repairing, and Beijing Institute for Brain Disorders, Capital Medical University, Beijing, China.*Corresponding author: [email protected]
Molecular Path Finding: Insight into Cerebral Ischemic/Hypoxic Injury and Preconditioning by Studying PKC-isoform Specific Signaling PathwaysZhang Nan, Li Yun, Li Junfa*
FigureÊ 1.Ê Proposed PKC-isoform–specific signaling pathways in cerebral ischemic/hypoxicÊ injuryÊ andÊ I/HPCÊ development.Ê AÊ seriesÊ ofÊ extracellularÊ signalsÊ andÊ intracellularÊsecondÊ messengersÊ induceÊ theÊ activationÊ ofÊ cPKCbII,Ê cPKCg,Ê andÊ nPKCe,Ê followedÊby phosphorylation of several downstream molecules. These PKC-isoform specific signalingÊ pathways,Ê especiallyÊ cPKCbII-CRMP-2Ê andÊ cPKCg-synapsinÊ pathways,ÊareÊ neuroprotectiveÊ duringÊ theÊ earlyÊ stagesÊ ofÊ cerebralÊ I/HPC.Ê NineteenÊ miRNAs,ÊnotablyÊ miR-615-3p,Ê mayÊ targetÊ genesÊ encodingÊ cPKCbII,Ê cPKCg,Ê nPKCeÊ andÊ theirÊinteractingÊ proteinsÊ duringÊ delayedÊ cerebralÊ ischemic/hypoxicÊ injuryÊ andÊ I/HPC.Ê PIP2,ÊphosphatidylinositolÊ 4,5-bisphosphate;Ê IP3,Ê inositolÊ trisphosphate;Ê DAG,Ê diacylglycerol;ÊPLC,Ê phospholipaseÊ C;Ê BDP,Ê breakdownÊ productÊ (ofÊ CRMP2).
decreased when compared with normoxic controls (6). While JNK pro-tein expression remained unchanged, its level of phosphorylation in-creased at Thr183 and Tyr185 in the hippocampus and frontal cortex of early and delayed I/HPC mice. Additionally, phospho-Thr183/Tyr185 JNK co-localized with a neuron-specific protein in I/HPC mouse brain (7). Regarding p38 MAPK, there was a significant increase in phos-phorylation at Thr180 and Tyr182 in the frontal cortex, hippocampus, and hypothalamus of I/HPC mice. Furthermore, p38 MAPK was acti-vated in specific cell types in I/HPC mice: microglia in the cortex and hippocampus, and neurons in the hypothalamus (8). We also observed the possible involvement of PKC and MAPK downstream molecules, such as p90 KD ribosomal S6 kinase (RSK) (9), mitogen- and stress-

58
Hypoxic Physiology
activated protein kinase 1 (MSK1), cyclic AMP (cAMP) response ele-ment binding protein (CREB), and Ets-like transcription factor-1 (Elk-1) (10).
To determine whether I/HPC could protect the brain against ischemic injury, we used a middle cerebral artery occlusion (MCAO)-induced focal cerebral ischemia mouse model. Evaluation of neurological defi-cits, terminal deoxynucleotidyl transferase (TdT)-mediated dUTP nick end labeling (TUNEL), and 2,3,5-triphenyltetrazolium chloride (TTC) staining were performed to determine the extent of neurological injury, cortical neuron apoptosis, and cerebral infarction, respectively in I/HPC preconditioned MCAO mice. Six hours after MCAO induction, mouse neurological functions were significantly impaired and showed symp-toms such as hypomobility, flattened posture, unidirectional circling, passivity, forelimb flexion, and motor incoordination. I/HPC treatment significantly attenuated MCAO-induced neurological deficits, reduced the percentage of apoptotic cells, and decreased the infarct volume and edema ratio of MCAO mice (11, 12). Taken together, we concluded that I/HPC mice were resistant to subsequent cerebral ischemic/hypoxic in-jury.
Determination of PKC-Isoform–Specific Signaling Molecules in Cerebral Ischemic/hypoxic Injury and I/HPC DevelopmentUsing a functional proteomics approach, we investigated the role of activated PKC isoforms and associated signaling molecules in cerebral ischemic/hypoxic injury and I/HPC development. First, we observed a reduction in ischemia-induced cPKCbII and g membrane translocation in the peri-infarction region of MCAO mice. Additionally, inhibition of cPKCbII or g activation could abolish I/HPC-induced neuroprotection (11, 12). Second, we separated and identified PKC-isoform–specific in-teracting proteins in the brain of I/HPC mice using proteomic analysis. A total of 49 cPKCbII-interacting proteins, of which 15 were cytosolic and 34 were from particulate fractions, were identified. Among these proteins, expression of four in the cytosol and eight in the particulate fraction changed significantly during I/HPC development (11). We identified 41 cPKCg-interacting proteins in I/HPC mouse brains that showed significantly altered expression, of which eight were cytosolic and 15 were in the particulate fraction (12). Third, we chose several proteins with the greatest variation to validate their PKC-isoform–spe-cific interactions and potential roles in cerebral ischemic/hypoxic in-jury and I/HPC development. We determined that cPKCbII-collapsin response mediator protein-2 (CRMP-2) and cPKCg-synapsin pathways were responsible for I/HPC-induced neuroprotection against initial ischemic injuries (11, 12).
We also investigated whether changes in protein levels in PKC isoform-specific signal pathways caused delayed cerebral ischemic/hypoxic injury and I/HPC development. Large-scale miRNA microarrays and bioinformatics analyses were used to determine
differentially expressed miRNAs and their PKC-isoform specific gene network in I/HPC and MCAO mouse brains. Nineteen miRNAs were differentially expressed in I/HPC and MCAO mouse brains, notably miR-615-3p, which may target genes encoding cPKCbII, g, and nPKCe-interacting proteins. All of these proteins could potentially be involved in I/HPC-induced neuroprotection. It should be noted that downregulation of miR-615-3p during I/HPC had a detrimental effect on oxygen-glucose deprivation (OGD)-induced N2A cell injury (13).
Proposed PKC-isoform Specific Signaling Pathways in Cerebral Ischemic/Hypoxic Injury and I/HPC DevelopmentFollowing the development of an I/HPC treatment modality that could protect mouse brains against subsequent ischemic/hypoxic injury, we proposed several PKC-isoform specific signaling pathways that may be involved in cerebral ischemic/hypoxic injury and I/HPC develop-ment. As shown in Figure 1, a series of signaling molecules, especially cPKCbII-CRMP-2 and cPKCg-synapsin pathways, have a neuropro-tective role during the initial stage of cerebral I/HPC, whereas the 19 miRNAs, notably miR-615-3p, might target genes encoding cPKCbII, g, and nPKCe-interacting proteins during delayed cerebral ischemic/hypoxic injury and I/HPC. These results have expanded our under-standing of the molecular mechanisms underlying cerebral ischemic/hypoxic injury and I/HPC, and may assist in identifying new molecu-lar targets for future clinical therapy of cerebral ischemic/hypoxic in-juries such as stroke.
REFERENCES 1. J. D. Marsh, S. G. Keyrouz, J. Am. Coll. Cardiol. 56, 683 (2010). 2. A. Stemer, P. Lyden, Curr. Neurol. Neurosci. Rep. 10, 29 (2010). 3. B. M. Tsai et al., Shock 21, 195 (2004). 4. J. Li et al., Brain Res. 1060, 62 (2005). 5. J. Li et al., Brain Res. 1093, 25 (2006). 6. C. Long et al., Neurosci. Lett. 397, 307 (2006). 7. N. Zhang et al., Neurosci. Lett. 423, 219 (2007). 8. X. Bu et al., Neurochem. Int. 51, 459 (2007). 9. Z. Qi et al., Neurochem. Res. 32, 1450 (2007).10. J. Jiang et al., Neurochem. Res. 34, 1443 (2009).11. X. Bu et al., J. Neurochem. 117, 346 (2011).12. N. Zhang et al., Neurochem. Int. 58, 684 (2011).13. C. Liu et al., J. Neurochem. 120, 830 (2012).
ACKNOWLEDGMENTSThis work was supported by grants from the National Natural Science Foundation of China (Grant No. 31071048 and 31171147), the National Basic Research Ò 973Ó Pre-Program (Grant No. 2011CB512109), and the National Basic Research Ò 973Ó Program (Grant No. 2012CB518200).

Sect ion Two
59
Section Two
FigureÊ 1.Ê NeuN-TUNELÊ doubleÊstainedÊ cellsÊ inÊ ischemicÊ brainÊ re-gions.Ê (A)Ê RepresentativeÊ NeuNÊ (red)ÊandÊ TUNELÊ (green)Ê doubleÊ stainingÊinÊ brainÊ sectionsÊ fromÊ aÊ sham-TBIÊratÊ (£),Ê aÊ TBI+Normoxia-CMÊ ratÊ(▨),Ê aÊ TBI+Normoxia-MSC-CMÊ ratÊ(▩),Ê andÊ aÊ TBI+Hypoxia-MSC-CMÊratÊ (▤).Ê Sham-TBI:Ê ratsÊ wereÊ givenÊ aÊshamÊ traumaticÊ brainÊ injuryÊ (TBI)Ê op-eration;Ê TBI+Normoxia-CM:Ê TBIÊ ratsÊtreatedÊ withÊ conditionedÊ mediumÊ(CM)Ê obtainedÊ underÊ normoxicÊ con-ditionÊ withoutÊ MSCÊ forÊ threeÊ daysÊ(n=6);Ê TBI+Normoxia-MSC-CM:Ê TBIÊratsÊ treatedÊ withÊ conditionedÊ me-diumÊ fromÊ MSCsÊ culturedÊ forÊ threeÊdaysÊ underÊ normoxicÊ conditionsÊ(n=6);Ê andÊ TBI+Hypoxia-MSC-CM:ÊTBIÊ ratsÊ treatedÊ withÊ conditionedÊ mediumÊ fromÊ MSCsÊ culturedÊ forÊ threeÊ daysÊ underÊ hypoxicÊ conditionsÊ (n=6).Ê TheÊ dataÊwereÊ obtainedÊ fourÊ daysÊ afterÊ injection.Ê (B)Ê MeanÊ ±Ê standardÊ deviationÊ valuesÊ ofÊ NeuN-TUNELÊ doubleÊ stainedÊ cellsÊ inÊtheÊ ischemicÊ brainÊ regions.Ê *p<0.05Ê comparedÊ withÊ theÊ sham+TBIÊ group;Ê +p<0.05Ê comparedÊ withÊ theÊ TBI+Normoxia-CMÊ group;Ê ¤ p<0.05Ê comparedÊ withÊ theÊ TBI+Normoxia-MSC-CMÊ group.Ê
T raumatic brain injury (TBI) is primarily caused by mechanical disruption, although secondary or delayed mechanisms may be involved (1–5). Mesenchymal stem cells (MSCs) derived from donor rats or humans can
improve dysfunction in a rat model of TBI (6), while paracrine mechanisms mediated by factors secreted from stem cells have been shown to be important for the repair of brain damage after stem cell mobilization (7, 8). Therefore, we examined whether the secretome from precultured MSCs prior to transplantation could improve their tissue regenerative potential in a TBI rat model.
Human MSCs were isolated from commercially available bone marrow aspirates. Conditioned medium (CM) was prepared by collecting serum-free medium after 24 hours of culturing of an optimal number of cells (2×106). Hypoxic cells subcultured 1:2 and cultured for three days until confluent were treated in a well-characterized, finely controlled ProOX-C-chamber system for 24 hours. The oxygen concentration in the chamber was maintained at 0.5% with a residual gas mixture constituting 5% carbon diox-ide and balanced nitrogen.
Under hypoxia, the expression levels of vas-cular endothelial growth factor (VEGF) and he-patocyte growth factor (HGF) in the MSC-CM or secretome were signifi-cantly higher than under normoxia (1). Cultured MSCs grown under nor-mal or hypoxic conditions and transplanted into TBI animals significantly re-duced (p<0.05) the brain volume and occurrence of brain damage compared with animals receiving culture medium alone (1). Normoxic or hypoxic MSC secretome-treated TBI animals had a re-duced incidence of brain damage compared with TBI animals receiv-ing control medium. Importantly, the protective effect was significantly greater in the hypoxic MSC secretome-treated animals compared with normoxic MSC secretome-treated animals (1).
Behaviorally, the normoxic or hypoxic MSC-CM treated TBI rats had significantly better motor and cognitive functions than control ani-mals treated with CM alone when evaluated 4 days after TBI induction. Additionally, the hypoxic MSC secretome-treated TBI rats performed significantly better in motor and cognitive functions than normoxic
1Department of Medical Research, Chi Mei Medical Center; 2Department of Biotechnology, Southern Taiwan University of Science and Technology, Tainan, Taiwan, China.*Corresponding author: [email protected]
Hypoxic Preconditioning Enhances the Potentially Therapeutic Secretome from Cultured Human Mesenchymal Stem Cells in Experimental Traumatic Brain InjuryChio Chung-Ching1, Chang Ching-Ping2, Lin Mao-Tsun1,*
MSC secretome-treated TBI rats (1).There were fewer NeuN-TUNEL double stained apoptotic neurons
in the peri-lesioned cortex of normoxic or hypoxic MSCs secretome-
A
B

60
Hypoxic Physiology
treated TBI rats than that of control vehicle solution-treated TBI rats (Figure 1). These neurons were also fewer in number in the peri-lesioned cortex of hypoxic MSCs secretome-treated TBI rats than that of normoxic MSCs secretome-treated TBI rats (Figure 1).
BrdU-NeuN-DAPI triple staining of newly formed neurons was greater in peri-lesions of the cortex in normoxic or hypoxic MSC sec-retome-treated TBI rats than in control vehicle solution-treated TBI rats (Figure 2). Also, the peri-lesioned cortex of hypoxic MSCs secretome-treated TBI rats had significantly greater BrdU-NeuN-DAPI triple stained neurons than normoxic MSC secretome-treated rats.
Thus, our study strongly supports a paracrine mechanism for neuro-protective repair, as administration of MSC secretomes recapitulated the beneficial effects observed after stem cell treatment of TBI. We demonstrated that systemically delivering normoxia- or hypoxia-pre-conditioned human MSC secretomes effectively and potently inhibited brain damage and functional impairment in TBI rats. Our results were relatively consistent with previous studies. For example, Wei et al., (9) demonstrated that the conditioned media of adipose stromal cells di-minished hypoxia/ischemia-induced brain damage in neonatal rats.
Adult stem cells, particularly MSCs, produce and secrete a wide
FigureÊ 2.Ê NeuN/BrdU/DAPIÊ tripleÊ stainedÊ cellsÊ inÊ peri-ischemicÊ brainÊregions.Ê (A)Ê RepresentativeÊ NeuNÊ (red)/BrdUÊ (green)/DAPIÊ (blue)Ê tripleÊstainingÊ inÊ brainÊ sectionsÊ fromÊ aÊ sham-TBIÊ ratÊ (£),Ê aÊ TBI+Normoxia-CMÊratÊ (£),Ê aÊ TBI+Normoxia-MSC-CMÊ ratÊ (▨),Ê andÊ aÊ TBI+Hypoxia-MSC-CMÊratÊ (▤).Ê (B)Ê MeanÊ ±Ê standardÊ deviationÊ valuesÊ ofÊ NeuN/BrdU/DAPIÊ tripleÊstainedÊ cellsÊ inÊ theÊ peri-ischemicÊ brainÊ regionsÊ (seeÊ FigureÊ 1Ê legendsÊforÊ groupÊ abbreviations).Ê *p<0.05Ê comparedÊ withÊ theÊ sham-TBIÊ group;Ê+p<0.05Ê comparedÊ withÊ theÊ TBI+normoxia-MSC-CMÊ groupÊ (n=6Ê forÊeachÊ group).Ê
variety of cytokines, chemokines, and growth factors that may potentially repair damaged tissues. Further-more, hypoxic stress increases the expression of several of these factors (8). Our study demonstrated that hy-poxic preconditioning enhanced the capacity of cultured human MSC secretomes to release several of these fac-tors, indicating the therapeutic potential of the cultured MSC secretome.
Generally, the adult mammalian brain retains neu-ral stem cells that continually generate new neurons within the subventricular zone (SVZ) of the lateral cerebral ventricle and the dentate gyrus subgranular zone (SGZ) of the hippocampus. We observed that hy-
poxia-cultured MSCs increased their rate of migration in vitro using the standard “scratch test” technique. Since HGF and HGF receptor/c-Met in adult human MSCs mobilize and are involved in repair of tissues, we propose that migration of neural stem cells from the SVZ and SGZ to the ischemic brain during TBI might be augmented by the HGF/c-Met signaling system, which might benefit tissue engi-neering and human MSC therapy. Moreover, the use of hypoxia en-hanced the capacity of cultured MSC secretomes to generate newly-formed neurons during TBI, which might aid in the restoration of damaged tissues.
After TBI, brain repair requires a continuous supply of blood pro-vided by enlarging pre-existing anastomotic channels or sprouting new capillaries from existing vascular cells (angiogenesis). Following the administration of human MSCs in rats to catalyze brain plasticity, brain VEGF levels significantly increased, indicating that new blood vessels may have been created to nourish the damaged area. VEGF is a key vasculogenic and angiogenic regulator. The hypoxia-cultured MSCs used in our study also had increased VEGF levels in the secretome and systemic delivery improved TBI. Thus, activating endogenous HGF and VEGF or administration of human HGF and VEGF might reduce behavioral deficits and cerebral damage in TBI.
In conclusion, we demonstrated that MSCs could secrete bioactive factors including HGF and VEGF that stimulate neurogenesis and im-prove behavioral deficits in a rat model of TBI. Hypoxic precondition-ing enhanced the secretion of MSCs-produced bioactive factors, indi-cating the therapeutic potential of hypoxic cultured MSC secretomes for treatment of TBI and other neurodegenerative diseases.
REFERENCES 1. C. P. Chang et al., Clinical Sci. (2012) doi: 10.1042/CS20120226. 2. S. H. Chen et al., Crit. Care Med. 37, 3097 (2009). 3. K. C. Lin et al., J. Trauma 72, 650 (2012). 4. C. C. Chio et al., J. Neurochem. 115, 921 (2010). 5. J. R. Kuo et al., J. Trauma 69, 1467 (2010). 6. A. Mahmood, D. Lu, M. Chopp, J. Neurotrauma 21, 33 (2004). 7. W. J. Kim, J. H. Lee, S. H. Kim, J. Neurotrauma 27, 131 (2010). 8. T. Kinnaird et al., Circ. Res. 94, 678 (2004). 9. X. Wei et al., Stem Cells 27, 478 (2009).
ACKNOWLEDGMENTSThis work was supported in part by the National Science Council of China (Grant No. NSC 99-2314-B-384-006-MY2, NSC 99-2314-B-384-004-MY3,andNSC98-2314-B-218-MY2)andtheDepartmentofHealthofChina(Grant No. DOH99-TD-B-111-003, the Center of Excellence for Clinical Trial and Research in Neuroscience).

Sect ion Two
61
Section Two
Hypoxic preconditioning (HP) can be induced by a brief, sub-lethal exposure to hypoxia. Adaptive hypoxia-protective re-sponses are the main characteristics of HP. Mitochondria are the cellular organelles most sensitive to hypoxia and their
dysfunction is the main cause of hypoxic injury. In contrast, adaptation of mitochondria to hypoxia improves the ability of a cell to survive se-vere hypoxia or anoxia (1). Here, we show that mitochondrial adaptive responses induced by HP are sufficient to stimulate protective mecha-nisms against severe hypoxic or anoxic injury. Over the past ten years, we found that HP could reduce the occurrence of apoptosis by regulat-ing the functions of mitochondria, and inhibit necrosis by regulating the volume of cells.
We first reported 12 years ago that HP decreased apoptosis in cul-tured hippocampal neurons in vitro after anoxia-reoxygenation and in-duced anoxic tolerance (2). The protective effect of HP against anoxia or severe hypoxia was further confirmed in vivo. Animals exposed to varying levels of HP displayed a delayed appearance of hypoxic in-jury potential and the disappearance of presynaptic volley when ex-posed to acute, lethal hypoxia, indicating that synaptic function was enhanced by HP (3). To reveal the potential mechanisms of protection afforded by HP against severe hypoxia or anoxia, we analyzed vari-ous mitochondrial functions to determine their unique roles in hypoxia (4, 5). Mitochondrial membrane potential (MMP) is the potential dif-ference across mitochondrial membranes and changes in MMP levels have been proposed as an index of mitochondrial function (6). MMP in acute anoxia was monitored in real-time under a laser-scanning in-verted confocal microscope after neurons were exposed to HP or nor-moxia. We found that HP enhanced the ability of hypoxia-sensitive hippocampal neurons or the less-sensitive hypothalamic neurons to maintain normal mitochondrial function under acute anoxia (7, 8). These results suggest that mitochondria are organelles with a strong self-regulating capacity.
Since HP decreased apoptosis induced by anoxia in cultured hippo-campal neurons, and Bcl-2 proteins, which respond to stress, are critical in the prevention of apoptosis, we examined the expression of Bcl-2
FigureÊ 1.Ê NecrosisÊ inducedÊ byÊ acuteÊ anoxiaÊ (AA)Ê andÊ theÊ preventionÊofÊ necrosisÊ byÊ hypoxicÊ preconditioningÊ (HP)Ê assessedÊ byÊ cellÊ volumeÊregulationÊ andÊ lactateÊ dehydrogenaseÊ (LDH)Ê releaseÊ fromÊ PC12Ê cells.Ê(A)Ê NecrosisÊ underÊ AAÊ exposure.Ê a, Ê 1%Ê agaroseÊ electrophoresisÊ gelÊ atÊindicatedÊ timesÊ afterÊ AA;Ê b,Ê FlowÊ cytometricÊ analysisÊ ofÊ cellsÊ treatedÊ withÊpropidiumÊ iodideÊ (PI);Ê c,Ê MorphologyÊ assessedÊ byÊ electronÊ microscopy.ÊUpperÊ imageÊ showsÊ aÊ cellÊ inÊ normoxiaÊ andÊ lowerÊ imageÊ showsÊ aÊ cellÊexposedÊ toÊ AAÊ forÊ 24Ê hours;Ê d,Ê PIÊ (blue)Ê andÊ HoechstÊ 33258Ê (red)Ê doubleÊstaining assessed by fluorescent microscopy. (B)Ê TheÊ processÊ ofÊ cellÊvolumeÊ regulationÊ duringÊ 24Ê hoursÊ ofÊ AAÊ exposure.Ê AA:Ê cellsÊ culturedÊinÊ normoxiaÊ wereÊ directlyÊ exposedÊ toÊ AA;Ê HP+AA:Ê cellsÊ treatedÊ withÊ HP,ÊfollowedÊ byÊ exposureÊ toÊ AA.Ê (C)Ê LDHÊ leakage.Ê Control:Ê cellsÊ wereÊ culturedÊinÊ normoxia.Ê AA:Ê cellsÊ wereÊ exposedÊ toÊ anoxiaÊ forÊ 24Ê hours.Ê HP+AA:Ê cellsÊwereÊ treatedÊ withÊ HP,Ê followedÊ byÊ 24Ê hoursÊ ofÊ anoxia.Ê HP+BB:Ê cellsÊ wereÊtreatedÊ withÊ HPÊ inÊ theÊ mediumÊ containingÊ 20Ê μg/mLÊ berberineÊ chlorideÊ(BB),Ê followedÊ byÊ AAÊ exposureÊ forÊ 24Ê hours.Ê *p<0.01Ê comparedÊ withÊ AAÊgroup;Ê #p<0.05Ê comparedÊ withÊ HP+AAÊ group.
Institute of Basic Medical Sciences, Academy of Military Medical Sciences, Beijing, China.*Corresponding author: [email protected]
B
C
Mitochondrial Adaptation and Cell Volume Regulation in Hypoxic Preconditioning Contribute to Anoxic ToleranceWu Li-Ying, Zhu Ling-Ling, Fan Ming*
A

62
Hypoxic Physiology
by immunocytochemical staining, assessing protein levels using an imaging analyzer or by flow cytometric analysis. The results demon-strated that HP increased Bcl-2 expression which, taken together with the previous results, suggest that higher levels of Bcl-2 induced by HP may maintain the higher levels of MMP during anoxia. However, we still lack direct evidence that these effects are caused by Bcl-2 over-expression induced by HP.
Necrosis is another mechanism of cell death and occurs more fre-quently in acute anoxia when energy metabolism is at a low level. Us-ing a hypoxia-sensitive PC12 cell line, we found that HP prevented the occurrence of necrosis induced by anoxia and delayed the regula-tory volume decrease (RVD) after cells were exposed to acute anoxia (9). Moreover, we demonstrated for the first time that this protection was related to the HP-induced increase in aldose reductase (AR) and sorbitol levels. AR catalyzes the conversion of glucose to sorbitol in the presence of nicotinamide adenine dinucleotide phosphate (NADP). Sorbitol synthesis is induced by increasing the amount and activity of AR. Changes in osmolarity cause sorbitol to leak rapidly into the ex-ternal medium through a sorbitol permease transport pathway, which prevents excessive cell swelling. The efflux of sorbitol was the primary mechanism for RVD, which protects the cells by minimizing cell swell-ing (10). In our study, we showed that acute anoxia caused cell necrosis (Figure 1A) and HP prevented this by inhibiting the increase in cell volume (Figure 1B) and lactate dehydrogenase (LDH) leakage, when the cells were exposed to acute anoxia. Additionally, berberine chloride (BB), an inhibitor of AR, completely reversed the protective effects of HP against LDH release (Figure 1C). This suggested that cell volume regulation could be a potential mechanism for the protection exerted by HP against acute anoxia. Sorbitol, synthesized from glucose and catalyzed by AR, is directly related to cell volume regulation (11). We demonstrated for the first time that HP significantly increased sorbitol levels, while treatment with BB, an inhibitor of AR, attenuated the in-crease in sorbitol content induced by HP (data not shown). Thus, we
speculated that HP increased the activity of AR. Quinidine, a stronger inhibitor of sorbitol, reversed the protection afforded by HP (data not shown), which indicated that sorbitol contributes to the protection by HP. Taken together, HP can prevent necrosis induced by anoxia, and the protective mechanism involves the regulation of cell volume medi-ated by the AR-sorbitol pathway. Thus, we propose that hypoxia causes changes in metabolic products that in turn enable cells to adapt to the hypoxic environment, a change in process from passive stress to active adaptation.
In conclusion, our studies have provided potential mechanisms for HP against severe hypoxia or anoxia. HP reduces the occur-rence of apoptosis by regulating the functions of mitochondria and inhibiting necrosis by regulating the volume of cells. In turn, these adaptive changes facilitated the formation of hypoxic or anoxic tolerance.
REFERENCES 1. L.C. Heather et al., Basic Res. Cardiol. 107, 3 (2012). 2. A. S. Ding et al., Chin. J. Neuroanat. 16, 1 (2000). 3. T. Zhao et al., Acta Phys. Sinica. 53, 1 (2001). 4. J. Wang et al., J. Neurochem. 77, 3 (2001). 5. E. Er et al., Biochim. Biophys. Acta.1757, 9 (2006). 6. O Cazzalini et al., Biochem. Pharmacol. 62, 7 (2001).7. L.Y.Wuet al., Brain Res. 999, 2 (2004).8. L. Y. Wu et al., Neurosignals 14, 3 (2005). 9. L.Y.Wuet al., Cell Stress Chaperon. 15, 4 (2010). 10. H. Garty et al., Am. J. Physiol. 260, 5 (1991).11. A. W. Siebens, K.R. Spring, Am. J. Physiol. 257, 6 (1989).
ACKNOWLEDGMENTSThis work was supported by grants from the National Basic Research Ò 973Ó Program (Grant No. 2012CB518200 and 2011CB910800) and the National Natural Science Foundation of China (Grant No. 31271211 and 81071066).
A lzheimer’s disease (AD) is a progressive neurodegenerative disease. Our early survey results indicated that a subpopula-tion of middle-aged residents living on the Tibetan plateau often suffers from sleep disorders and light memory loss, and
that these symptoms worsen with age. Additionally, β-amyloid peptide
The Effects of Ratanasampil, a Traditional Tibetan Medicine, on β-amyloid Pathology in a Transgenic Mouse Model and Clinical Trial of AlzheimerÕ s DiseaseZhu Aiqin1,*, Li Guofeng1, Zhong Xin1, Li Yinglan1, Liao Baoxia1, Zhang Jun2, Chu Yide1
1Department of Geriatrics, Qinghai Provincial Hospital, Xining, Qinghai, China; 2National Institute of Neurological Disorders and Strokes/NIH, Bethesda, MD, U.S.*Corresponding author: [email protected]
(Aβ) production was seen to increase following cardiac arrest, indicat-ing that a chronic hypoxia environment might be involved in the patho-genesis of AD (1, 2). We also studied hyperhomocysteinemia and cogni-tion disorders at high altitude (3). Although drugs for the treatment of AD exist, no current treatment is curative or permanently arrests the dis-ease course (4). Ratanasampil (RNSP), a compound formulation from traditional Tibetan medicine, has been widely used as an anti-aging and anti-hypoxic drug to treat cerebrovascular diseases and high-altitude sickness in China. Our research group conducted a series of investi-gations on the effects of RNSP on Aβ pathology in an AD transgenic

Sect ion Two
63
Section Two
1College of Ethnomedicine of Chengdu University of Traditional Chinese Medicine, Sichuan, China;
2Teaching Hospital of Chengdu University of Traditional Chinese Medicine, Sichuan, China.*Corresponding author: [email protected]
Duoxuekang, a Traditional Tibetan Medicine, Reduces Hypoxia-Induced High-Altitude Polycythemia in RatsZhang Yi1,*, Meng Xianli1, Wu Wenbin1,2, Lai Xianrong1, Wang Yujie1, Zhang Jing1, Wang Zhang1
mouse model (Tg2576) and in patients living at high altitudes.The Tg2576 mouse has been widely used to simulate features of hu-
man AD (5). Tg2576 mice were administered RNSP at 0.14 mg/day for eight weeks. Immunohistochemistry in RNSP-treated mice showed a marked reduction in amyloid plaques in the cortex and hippocampus. Consistently, both Western blot and ELISA analysis indicated signifi-cant decreases of Aβ40 and Aβ42 peptides in the brains of RNSP-treated Tg2576 mice. Furthermore, RNSP treatment dramatically reduced the level of Aβ in serum. Densitometric analysis of C-terminal fragments (CTFs) showed that α-CTF (also called p3, the product of amyloid precursor protein cleavage by α-secretase containing the C-terminal portion of Aβ but not releasing the damaging Aβ peptide) was signifi-cantly increased in the brains of the drug treatment group, resulting in a higher ratio of α-CTF/β-CTF than in the vehicle group (6). Since α-secretase activity does not release Aβ, the significant increase in α-CTF seen in our study suggests that RNSP treatment most likely in-creases α-secretase activity. Thus, a higher ratio of α-CTF/β-CTF may indicate reduced release of the Aβ peptide. Animal behavior experi-ments suggested an improvement in memory and decreased anxiety in RNSP-treated Tg2576 mice (7, 8).
We then conducted a clinical trial to further investigate whether RNSP improves cognitive function in AD patients living in Xining (2,000 to 3,000 m). 140 patients with mild-to-moderate AD were divid-ed into three groups: high-dose RNSP (1 g/day), low-dose RNSP (0.3 g/day), and control (placebo). All patients were assessed using the Mini Mental State Examination (MMSE), Alzheimer’s disease Assessment Scale cognitive subscale (ADAS-cog), and activity of daily living scale (ADL) at three time points: before treatment, after four weeks of treat-ment, and at the end of 16 weeks of treatment (9). MMSE, ADAS-cog, and ADL scores were significantly improved in the high-dose RNSP group compared to scores before treatment. Additionally, the serum concentrations of tumor necrosis factor (TNF)-α, interleukin (IL)-1β, and IL-6 were decreased at 16 weeks but only in the high-dose RNSP group. Significantly, Aβ42 positively correlated with the concentrations of TNF-α, IL-1β, and IL-6 in serum. Furthermore, we found the su-peroxide dismutase activity was increased whereas nitric oxide (NO) synthase activity was inhibited in the high-dose RNSP group (10). Since
AD incidence is thought to correlate with increased levels of oxygen radicals and NO (11), this result suggests that high-dose RNSP could be considered as an option for AD treatment. Side effects of RNSP were not evident. The protocol was approved by the Qinghai Provincial Med-ical Ethics Committee.
Our group initiated an investigation into the anti-aging and anti-hy-poxia mechanisms of RNSP for the treatment of AD at high altitude. Although the mechanism for RNSP therapeutic activity is not fully un-derstood, we postulate three putative modes of action: (i) Intervention in the amyloid precursor protein system―RNSP may selectively increase α-secretase activity and/or inhibit β-secretase activity, resulting in the reduction of Aβ; (ii) Anti-inflammatory effects―RNSP might reduce inflammatory factors by inhibiting inflammatory responses and microg-lia activation; and (iii) Anti-oxidative stress activity.
In summary, these potential multifunctional effects of RNSP suggest a novel mechanistic target for Alzheimer therapeutics. Currently, we are working on a large group of subjects to determine the consistency of RNSP effects on mild to moderate AD at high altitudes. We hope to identify a form of RNSP with enhanced therapeutic efficacy and re-duced side effects. Furthermore, to explore the prevalence and risk fac-tors of AD for the elderly in areas of high altitude, we will investigate populations over the age of 50 living on the Qinghai-Tibet plateau.
REFERENCES1. R. Yaari, J. Corey-Bloom. Semin. Neurol. 27, 32 (2007).
2. H. Zetterberg et al., PLoS One 6, e28263 (2011). 3. Q. X. Ma, A. Q. Zhu. High Alt. Med. 7, 230 (2009). 4. S. A. Jacobson, M. N. Sabbagh. Alzheimers Res. Ther. 4, 20 (2011). 5. S. Lesne et al., Nature 440, 352 (2006). 6. A. Q. Zhu et al., Chin. Pharmacol. Bull. 6, 720 (2009). 7. A. Q. Zhu, Y. D. Chu, C. L. Masters, Q. X. Li, Chin. J. Psych. 3, 69
(2010). 8. A. Q. Zhu, C. L. Masters, Q. X. Li, Chin. J. Geriatr. 11, 950 (2009). 9. A. Q. Zhu et al., J. Behav. Brain Sci. 2, 82 (2012).10. B. X. Liao, A. Q. Zhu, A. Q. Xi, Y. D. Chu, Chin. J. Geriatr. 19, 2437
(2009).11. D. Y. Choi, Y. J. Lee, J. T. Hong, H. J. Lee, Brain Res. Bull. 87, 144 (2012).
China has a wide area of plateaus, about 17% of which reach an altitude of more than 3,000 m. In typical plateaus such as Qinghai, Xinjiang, and Tibet, various physical ailments and organ damage caused by hypoxia can pose consider-
able, sometimes life-threatening, risks to people visiting these areas for the first time (1).
High-altitude polycythemia (HAPC), named “Plethora” in Tibetan medicine, is a chronic altitude-induced disease characterized by
hyperplasia of red blood cells due to hypoxia and can seriously jeopardize the health of high-altitude plateau residents. HAPC in
64
Hypoxic Physiology
k-opioid Receptor and Hypoxic Pulmonary HypertensionLi Juanà , Zhang Lijunà , Fan Rongà , Guo Haitao, Zhang Shumiao, Wang Yuemin, Pei Jianming*
Hypoxic pulmonary hypertension (HPH) is critical in the pathogenesis and development of many cardiovascular and pulmonary diseases such as chronic obstructive pulmonary disease, chronic plateau disease, and neonatal pneumonia
(1). The κ-opioid receptor (κ-OR) is the predominant opioid receptor isotype and is present in the heart and peripheral blood vessels (2). However, the role of κ-OR in HPH has not been previously studied. Therefore, we recently attempted to elucidate the role of κ-OR in HPH along with its underlying mechanisms. Here, we present a review of our studies on the role of κ-OR and its possible mechanisms of action.
China has an incidence rate of between 2.5% and 5% in the plateau areas, with a total of approximately 250,000 patients, but currently there is no effective cure (2). However, the symptoms are commonly alleviated by increasing the oxygen-carrying capacity of the blood, improving hypoxia, and reducing the number of red blood cells. Other methods have been adopted, such as dredging blood vessels to improve microcirculation, oxygen inhalation, administration of blood-thinning agents, migration to lower altitude areas, and treatment with traditional medicine. However, the lack of an effective treatment for HAPC has hindered the economic and political development of China’s plateau areas (3).
Traditional Tibetan medicinal plants are endowed with unique physi-ological activity owing to the specific environment in which they are grown and, therefore, has unique effects in the prevention and treat-ment of a variety of chronic altitude illnesses. Nevertheless, a poor un-derstanding of the bioactive chemical constituents and mechanisms of traditional Tibetan remedies for the treatment of altitude sickness has restricted the modern development of Tibetan medicine. In this study, we selected one traditional Tibetan medicine, Duoxuekang, and con-ducted a proof of concept study of its mechanism to provide scientific evidence for the treatment and prevention of chronic altitude sickness.
Duoxuekang is derived from a secret recipe owned by the famous Tibetan medicine master, Cuoru, and has been found to alleviate ex-haustion and increase tolerance to hypoxia, greatly alleviating blood stasis and hyperplasia of red blood cells. In this study, we first estab-lished a HAPC rat model by using a low pressure chamber to simulate the high altitude plateau environment. Treatment of HAPC rats with Duoxuekang reduced the red blood cell, hemoglobin, and serum eryth-
ropoietin (EPO) concentrations. It also reduced the fibrinogen concen-tration, inhibited erythrocyte costimulation, and improved erythrocyte deformation, which possibly explains its effect on promoting blood circulation and dissipating blood stasis (4). Additionally, it downreg-ulated hypoxia-inducible factor (HIF)-1α protein expression in brain tissue, decreased EPO mRNA expression in kidney tissues and se-rum, and inhibited erythroid hyperplasia in the peripheral blood (5). A high-performance liquid chromatography (HPLC) method to detect active compounds in Duoxuekang was developed for quality control. A serum pharmacochemical study of Duoxuekang revealed that the plants Phyllanthus emblica and Hippophae rhamnoides might provide the active compounds responsible for the efficacy in the treatment of HAPC.
This study is helpful for understanding the mechanisms of action of traditional Tibetan medicines used for the prevention and treatment of HAPC caused by hypoxia, and related chronic diseases. Duoxuekang and the identified compounds can be further developed as new thera-peutics for the prevention and treatment of HAPC.
REFERENCES 1. C. F. Merino, Blood 5, 1 (1950). 2. P. Li et al., Exp. Hematol. 39, 37 (2011).3. W. B. Wu, X. L. Meng, Y. Zhang, X. R. Lai, J. Guangzhou. Univ. TCM.
27, 492 (2010). 4. W. B. Wu, X. R. Lai, Q. M. Suolang, X. L. Meng, Tib. Sci. Technol. 33,
39 (2009).5. W. B. Wu, X. R. Lai, Q. M. Suolang, X. L. Meng, F. Y. Liu, Pharmacol.
Clin. Chin. Mate. Clin. Med. 25, 93 (2009).
In 1986, Seelhorst and Starke demonstrated that κ-OR is found in the pulmonary artery (PA) of rabbits (3). For the first time, we recently demonstrated that κ-OR is expressed in PAs of rats and its expression increases in hypoxic states (4). To explore the effect of κ-OR on PAs in rats, isolated PA rings were perfused and the tension of the vessel was measured. κ-OR stimulation with U50,488H [(trans)-3,4-dichlo-ro-N-methyl-N-[2-(1-pyrrolidinyl)-cyclohexyl]benzeneacetamide], a selective κ-OR agonist, induced relaxation of PAs in vitro in a dose-dependent manner (5). This effect was abolished by administration of nor-binaltorphimine (nor-BNI), a selective κ-OR antagonist. The relaxation effect of U50,488H in PAs was partially endothelium-de-pendent and was significantly attenuated in the presence of NG-nitro-L-arginine methyl ester (L-NAME), a nitric oxide synthase inhibitor. The relaxation effect of U50,488H was also significantly attenuated by KV channel blocker 4-aminopyridine (4-AP) but not by glibenclamide (an ATP-sensitive K+ channel blocker) or tetraethylammonium (TEA, a Ca2+-activated K+ channel blocker). Further study demonstrated that
Department of Physiology, National Key Discipline of Cell Biology, Fourth Military Medical University, Xi’an, China.*Corresponding author: [email protected]‡Contributed equally to this work.

Sect ion Two
65
Section Two
FigureÊ 2.Ê StimulationÊ ofÊ k-ORÐ initiatedÊ pulmonaryÊ circulationÊ protectionÊ (upperÊ panel)Ê andÊ initiationÊ ofÊ PI3K-Akt-eNOS-NOÊ survivalÊ signalingÊ (lowerÊpanel).Ê UpperÊ panel: Ê InÊ PAs,Ê U50,488HÊ bindsÊ toÊ k-OR,Ê thenÊ relaxesÊ PAsÊ byÊ twoÊ separateÊ pathways:Ê endothelium-derivedÊ nitricÊ oxideÊ andÊ KVÊ chan-nelsÊ inÊ PASMCs.Ê U50,488HÊ treatmentÊ inhibitsÊ remodelingÊ ofÊ PAsÊ duringÊ hypoxia.Ê InÊ PASMCs,Ê U50,488HÊ inhibitsÊ proliferationÊ ofÊ theseÊ cellsÊ duringÊ
hypoxia.Ê InÊ vivo,Ê U50,488HÊ decreasesÊmPAP,Ê RVP,Ê andÊ RVÊ hypertrophyÊ byÊ ac-tivatingÊ k-ORÊ duringÊ hypoxia.Ê Addition-ally,Ê U50,488HÊ balancesÊ theÊ concen-trationÊ ofÊ NO,Ê ET,Ê andÊ AIIÊ inÊ bloodÊ andÊlungÊ tissuesÊ inÊ HPHÊ rats.Ê LowerÊ panel:ÊU50,488HÊ bindsÊ toÊ k-OR,Ê leadingÊ toÊ theÊactivationÊ ofÊ theÊ PI3K-Akt-eNOS-NOÊpathwayÊ andÊ mayÊ elicitÊ pro-survivalÊ andÊpulmonaryÊ vascularÊ protectiveÊ effectsÊincluding vasodilatation, anti-inflamma-tion,Ê anti-oxidative/nitrativeÊ stress,Ê andÊanti-apoptosis.Ê Abbreviations:Ê k-OR,Êk-opioidÊ receptor;Ê PA,Ê pulmonaryÊ artery;ÊPASMC,Ê pulmonaryÊ arteryÊ smoothÊ cell;ÊPAEC,Ê pulmonaryÊ endothelialÊ cell;Ê MTT,Êmonotetrazolium;Ê 3H-TdR,Ê [3H]-thymidine;ÊmPAP,Ê meanÊ pulmonaryÊ arteryÊ pres-sure;Ê RVP,Ê rightÊ ventricularÊ pressure;Ê RV/(LV+S),Ê rightÊ ventricleÊ (RV)/leftÊ ventricleÊ(LV)Ê +Ê septumÊ (S);Ê RV/BW,Ê rightÊ ventricleÊ(RV)/bodyÊ weightÊ (BW);Ê NO,Ê nitricÊ oxide;ÊET,Ê endothelin;Ê AII,Ê angiotensinÊ II;Ê PI3K,ÊphosphatidylinositolÊ 3Õ -kinase;Ê Akt,Ê pro-teinÊ kinaseÊ B;Ê eNOS,Ê endothelialÊ nitricÊoxideÊ synthase;Ê PMN,Ê polymorphonucle-arÊ neutrophil;Ê NADPH,Ê nicotinamideÊ ad-enineÊ dinucleotideÊ 2Õ -phosphate;Ê ROS,ÊreactiveÊ oxygenÊ species.
FigureÊ 1.Ê EffectsÊ ofÊ U50,488HÊ onÊ pulmonaryÊ arteryÊ(PA) remodeling induced by hypoxia (magnification ×400;Ê fromÊ referenceÊ 3).Ê (A,Ê D)Ê control;Ê (B,Ê E):Ê hy-poxiaÊ forÊ twoÊ weeks;Ê (C,Ê F)Ê hypoxiaÊ forÊ twoÊ weeksÊ+Ê U50,488H.Ê (AÐ C)Ê HematoxylinÊ andÊ eosinÊ stain-ingÊ andÊ (DÐ F)Ê elastinÊ stainÊ detectedÊ byÊ lightÊ andÊtransmissionÊ electronÊ microscopy,Ê respectively.ÊTheÊ proliferationÊ andÊ migrationÊ ofÊ pulmonaryÊ arteryÊsmoothÊ muscleÊ cellsÊ andÊ theÊ thicknessÊ ofÊ theÊ PAÊwall were significantly reduced in the group with hypoxiaÊ forÊ twoÊ weeksÊ thatÊ receivedÊ intraperitonealÊadministrationÊ ofÊ U50,488HÊ (1.25Ê mg/kg).
endothelium denudation and 4-AP have an addi-tive inhibitory effect on PA relaxation induced by U50,488H. Additionally, dynorphin A 1-13 (an en-dogenous κ-OR agonist) at the same concentration as U50,488H also induced a significant relaxation effect in rat PA rings that was lower (47.5 ± 4.8 %) than for U50,488H (61.4 ± 4.2 %). The vaso-relaxant effect of dynorphin A 1-13 was abolished by nor-BNI. The above results suggest that κ-OR stimulation with U50,488H relaxes PAs through two separate pathways: (i) endothelium-derived nitric oxide, and (ii) KV channels in pulmonary artery smooth muscle cells (PASMCs).
Based on the above results, we further explored the role of κ-OR in HPH and its potential application for treatment of HPH. The HPH model was developed by exposing rats to hypobaric and hypoxic en-vironments with 10% oxygen and indices for hemodynamics and right ventricular (RV) hypertrophy were measured. We found that
intravenous U50,488H significantly lowered mean pulmonary artery pressure (mPAP) in normoxic control rats and this effect was abol-ished by administration of nor-BNI. Hypoxia for longer than two weeks induced severe HPH in rats and intraperitoneal administration of U50,488H during chronic hypoxia reduced mPAP and attenuated RV hypertrophy compared with the control group (6). Moreover, acute intravenous administration of U50,488H after rats were subjected to
66
Hypoxic Physiology
Changes in the chemical composition and pharmacological activity of substances in the bloodstream evoke reflexive re-sponses of the central autonomic nuclei via the glomus che-moreceptors in the carotid bodies bilaterally located at the
bifurcation of the common carotid artery. Physiological stimuli, notably
1Department of Physiology, The University of Hong Kong, Pokfulam, Hong Kong, China; 2Department of Anatomy, The University of Hong Kong, Pokfulam, Hong Kong, China; 3Research Centre of Heart, Brain, Hormone & Healthy Aging, Li Ka Shing Faculty of Medicine, The University of Hong Kong, Hong Kong, China; 4School of Biomedical Sciences, The Chinese University of Hong Kong, New Territories, Hong Kong, China.*Corresponding author: [email protected]
Paracrine-Autocrine Mechanisms in the Carotid Body Function at High Altitude and in DiseaseFung Man Lung1,3,*, George L. Tipoe2,3, Leung Po Sing4
chronic hypoxia for four weeks significantly lowered mPAP. Thus, U50,488H has a significant vasorelaxant effect in rat PAs and may have preventive and therapeutic applications for HPH.
To further investigate the underlying mechanism of the HPH protec-tive effect of κ-OR stimulation with U50,488H, we investigated the ef-fect of U50,488H on PA remodeling and proliferation of PASMCs and on vasomotor factors such as nitric oxide (NO), endothelin (ET), and angiotensin II (AII). We found that U50,488H inhibited PA remodeling compared with the hypoxic group (Figure 1). Moreover, U50,488H also dose-dependently inhibited proliferation of hypoxia-induced PASMCs. Compared with the hypoxic group, NO content was higher, whereas production of ET and AngII were lower in both blood and pulmonary tissue in the group treated with U50,488H. Our results suggest that in-hibition of PA remodeling, PASMC proliferation and beneficial regula-tion of vasomotor factors may be responsible for the depressive effect of U50,488H in HPH (7).
In conclusion, we provide for the first time evidence of the precise location of κ-OR expression in PAs of rats and that κ-OR expression is upregulated during hypoxia. Further studies demonstrated that κ-OR stimulation plays an important role in inhibiting remodeling of PAs in adaptation to chronic hypoxia and inhibits the proliferation of PASMCs. Additionally, κ-OR stimulation with U50,488H balances the concentra-tion of NO, ET, and AngII in blood and lung tissues, which indirectly prevents the development of HPH. These findings suggest a potential preventive and therapeutic effect for κ-OR in a HPH rat model.
Studies suggest that HPH is initiated by hypoxia-induced endothelial injury of the pulmonary arteriole followed by an imbalance of various vasomotor factors, PA contraction, and remodeling of pulmonary ves-sels. NO and NO synthase (NOS) are involved in the occurrence and development of HPH. We previously found that U50,488H effectively
relaxes the PA ring and depresses mPAP in HPH rats. Moreover, ac-tivation of κ-OR reduces myocardial ischemia-induced cell apoptosis and inhibits inflammation (8, 9). All of these effects are associated with NO pathways. On the basis of previous studies, we intend to further investigate the signaling mechanisms underlying the κ-OR-induced improvement of endothelial function and to confirm the possible role of NO signaling pathways in the anti-HPH effect mediated by κ-OR. These experimental results will provide a novel prospective of HPH and will present evidence for new clinical strategies for the prevention and treatment of HPH. Based on our studies, we generated a schematic diagram indicating the κ-OR signaling pathway (Figure 2, upper panel) and areas of further study (Figure 2, lower panel).
REFERENCES 1. T. S. GŸ ven• et al., Heart, Lung and Circ. (2012) doi: 10.1016/j.
hlc.2012.08.004. 2. K. K. Tai et al., J. Mol. Cell. Cardiol. 23, 1297 (1991). 3. A. Seelhorst, K. Starke, Arch. Int. Pharmacodyn. Ther. 281, 298 (1986). 4. P. Peng et al., Anat. Rec. 292, 1062 (2009). 5. X. Sun et al., Life Sci. 78, 2516 (2006). 6. J. M. Pei et al., J. Cardiol. Pharmacol. 47, 594 (2006). 7. J. Li et al., Vasc. Pharmacol. 51, 72 (2009). 8. G. Tong et al., Life Sci. 88, 31 (2010). 9. X. D. Wu et al., Cytokine. 56, 503 (2011).
ACKNOWLEDGMENTSThis work was supported by the National Natural Science Foundation of China (Grant No. 30900535, 30971060, 31100827, 81270402, and 31200875) and Shaanxi Province (Grant Nos. 2010K01195 and 2011JM4001). We thank Professor Sharon Morey for editing input.
hypoxia, hypercapnea, or acidosis, in addition to circulating chemicals, stimulate reflexogenic chemoreceptors that trigger afferent impulses transmitted by the carotid sinus nerve to brainstem nuclei to induce ven-tilatory and circulatory responses. In addition to these stimuli, recent data suggest that a number of vasoactive peptides, such as cytokines and their ligand-binding receptors locally expressed in the carotid body, could function in a paracrine-autocrine manner to modulate the excit-ability and activity of carotid chemoreceptors. Additionally, hypoxia regulates the expression of paracrine-autocrine signaling molecules via the activation of hypoxia-inducible factors, suggesting that these local responses play an important role in the functional modulation of the ca-rotid body under chronically hypoxic conditions (1). Thus, these local regulatory mechanisms may have functional implications with respect to ventilatory acclimation at high altitudes and the cardiopulmonary responses to chronic hypoxemia in disease.

Sect ion Two
67
Section Two
Carotid Body Function at High Altitude and in DiseaseMinute ventilation increases at high altitude and the hy-poxic ventilatory response gradually increases over hours and days at high altitudes. This ventilatory acclimation is an important physiological adaptive response to chronic hypoxia. It has been shown to be mediated by the carotid body, since the response is abolished by the resection or denervation of this structure. A number of mechanisms can modulate carotid chemoreceptor activity under hypoxic conditions, including but not limited to: (i) hypoxia-induc-ible factor (HIF) pathways responsible for the structural and functional changes of the carotid body (1); (ii) changes in circulating or locally produced vasoactive peptides or factors that alter carotid chemoreceptor activity; (iii) the multiplicative effects of combined stimuli relevant to sleep apnea, which occurs in subjects at high altitude or in dis-ease conditions; and (iv) overproduction of reactive oxy-gen species (ROS) leading to oxidative stress induced by intermittent hypoxia or sleep apnea in disease conditions (1).
HIF-1 Pathway in the Carotid Body at High AltitudeThe carotid body enlarges and changes in sensitivity in response to hypoxic conditions in humans and animals living at high altitudes, and in subjects exposed to chronic hypoxemia associated with cardiopulmonary diseases or hematological disorders. In the carotid body, chronic hypoxemia can modulate the excitability and sensitiv-ity of the chemosensitive glomus cells to chemical signals as well as stimulate their proliferation and induce remodeling of the vasculature. HIFs―heterodimeric transcriptional factors―are directly induced by cellular or tissue hypoxia and regulate HIF-target gene expression in response. Some of the targeted gene products, including endothelin-1 (ET-1), type II nitric oxide synthase (iNOS), and vascular endothelial growth factor (VEGF) have important physiological roles in the control of vascular tone and angiogenesis (1).
HIF-1 target genes expressed in the carotid body are modulated by chronic hypoxemia, suggesting an active role for HIF-1 during moder-ate levels of hypoxic stress (2, 3). We have examined the role of HIF-1 and its target genes in the vascular and physiological changes in the carotid body of rats exposed to chronic hypoxia (inspired normobaric 10% oxygen or an altitude of 5,000 m, for four weeks). In chronic hy-poxia, the majority of cells in the carotid body increased protein expres-sion of HIF-1α, a heterodimeric partner of HIF-1 induced by hypoxia (2, 3). The increased level of HIF-1 activated the transcriptional ex-pression of genes encoding VEGF and VEGF receptors in the carotid body (2, 3). These changes may mediate angiogenesis for vascular re-modeling in the carotid body, which is important for limiting the dif-fusion distance between the capillary and the chemosensitive glomic tissue. Additionally, we showed that intracellular calcium responses to ET-1 were augmented in the chemosensitive glomus cells of the carotid body with increased ET-1 protein expression during chronic hypoxia (4). This suggested an enhancement of the paracrine-autocrine effects of ET-1 on the excitability and mitotic activities of the chemosensitive glomus cells during chronic hypoxia (4). Moreover, iNOS protein was localized in glomic clusters in the carotid body. Nitric oxide (NO) con-centration in the carotid body was significantly higher in hypoxia than
that under normoxic conditions. Hypoxia-induced NO production was attenuated by NOS inhibitor L-NAME and by S-methylisothiourea, a specific inhibitor of iNOS. Increased NO levels potentiated the in-hibitory effect of NO on carotid chemoreceptor activity, and therefore negatively modulated the chemoreflex response to hypoxia (5). Thus, our results suggest that chronic hypoxemia induces the transcriptional activity of HIF-1 and regulates the expression of target genes for the structural remodeling and physiological adaptation of the carotid body.
Local Renin-Angiotensin System Regulated by Hypoxia in the Carotid BodyAngiotensin receptors are localized in chemosensitive glomus cells in the carotid body and angiotensin II (AII) can stimulate chemorecep-tor activity (Figure 1). The carotid chemoreceptor response to AII is enhanced in chronically hypoxic rats, which can be explained by in-creased expression of the AII type 1 receptor in glomic clusters of the carotid body during chronic hypoxia (6, 7). Interestingly, in addition to its presence in the blood, AII is also locally produced by the renin-angiotensin system (RAS) in the carotid body (7). The RAS component genes encoding angiotensinogen (an angiotensin precursor) and Ang receptors are upregulated by hypoxia (7), which might represent an adaptive response of the carotid body to chronic hypoxia.
Moreover, AII and ROS expressed in the carotid body are involved in the pathophysiological response to intermittent hypoxia under disease conditions. We examined the expression of AII type 1 receptor and the by-products of oxidative stress in the carotid body of rats exposed to intermittent hypoxia mimicking a severe, obstructive sleep apnea con-dition (i.e., inspired oxygen levels alternating between 5%–21% per minute, eight hours per day for up to four weeks). The expression of AII type 1 receptors was markedly elevated in the glomic clusters of the carotid body in intermittent hypoxia. Additionally, intracellular cal-cium responses to AII were significantly enhanced in chemosensitive glomus cells, which could be abolished by administration of the AII
FigureÊ 1.Ê ExpressionÊ ofÊ angiotensinÊ IIÊ (AII)Ê typeÊ 11Ê receptorsÊ (A,Ê red)Ê inÊ theÊ glomicÊclustersÊ expressingÊ tyrosineÊ hydroxylaseÊ (TH,Ê B,Ê blue)Ê ofÊ theÊ ratÊ carotidÊ bodyÊ duringÊchronicÊ hypoxia.Ê (C)Ê MergedÊ imageÊ showsÊ localizationÊ ofÊ theÊ AIIÊ typeÊ 11Ê receptorÊ inÊtheÊ chemosensitiveÊ glomusÊ cellsÊ (circles).Ê (D)Ê NegativeÊ control.
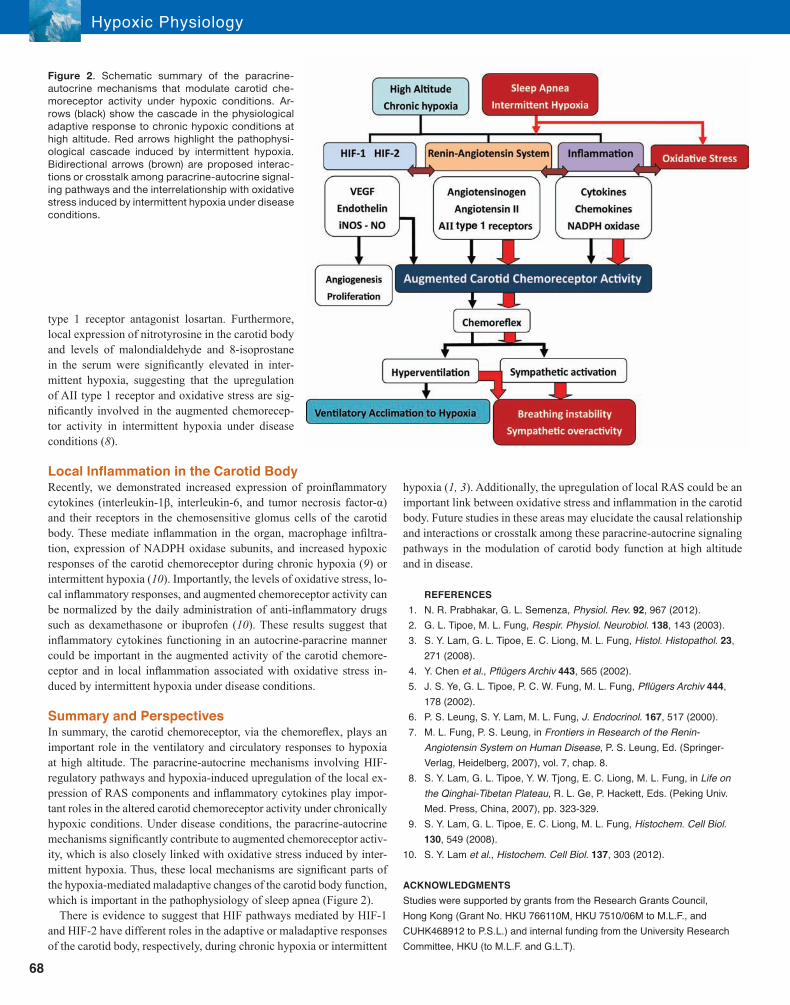
68
type 1 receptor antagonist losartan. Furthermore, local expression of nitrotyrosine in the carotid body and levels of malondialdehyde and 8-isoprostane in the serum were significantly elevated in inter-mittent hypoxia, suggesting that the upregulation of AII type 1 receptor and oxidative stress are sig-nificantly involved in the augmented chemorecep-tor activity in intermittent hypoxia under disease conditions (8).
Local Inflammation in the Carotid BodyRecently, we demonstrated increased expression of proinflammatory cytokines (interleukin-1β, interleukin-6, and tumor necrosis factor-α) and their receptors in the chemosensitive glomus cells of the carotid body. These mediate inflammation in the organ, macrophage infiltra-tion, expression of NADPH oxidase subunits, and increased hypoxic responses of the carotid chemoreceptor during chronic hypoxia (9) or intermittent hypoxia (10). Importantly, the levels of oxidative stress, lo-cal inflammatory responses, and augmented chemoreceptor activity can be normalized by the daily administration of anti-inflammatory drugs such as dexamethasone or ibuprofen (10). These results suggest that inflammatory cytokines functioning in an autocrine-paracrine manner could be important in the augmented activity of the carotid chemore-ceptor and in local inflammation associated with oxidative stress in-duced by intermittent hypoxia under disease conditions.
Summary and PerspectivesIn summary, the carotid chemoreceptor, via the chemoreflex, plays an important role in the ventilatory and circulatory responses to hypoxia at high altitude. The paracrine-autocrine mechanisms involving HIF-regulatory pathways and hypoxia-induced upregulation of the local ex-pression of RAS components and inflammatory cytokines play impor-tant roles in the altered carotid chemoreceptor activity under chronically hypoxic conditions. Under disease conditions, the paracrine-autocrine mechanisms significantly contribute to augmented chemoreceptor activ-ity, which is also closely linked with oxidative stress induced by inter-mittent hypoxia. Thus, these local mechanisms are significant parts of the hypoxia-mediated maladaptive changes of the carotid body function, which is important in the pathophysiology of sleep apnea (Figure 2).
There is evidence to suggest that HIF pathways mediated by HIF-1 and HIF-2 have different roles in the adaptive or maladaptive responses of the carotid body, respectively, during chronic hypoxia or intermittent
hypoxia (1, 3). Additionally, the upregulation of local RAS could be an important link between oxidative stress and inflammation in the carotid body. Future studies in these areas may elucidate the causal relationship and interactions or crosstalk among these paracrine-autocrine signaling pathways in the modulation of carotid body function at high altitude and in disease.
REFERENCES 1. N. R. Prabhakar, G. L. Semenza, Physiol. Rev. 92, 967 (2012). 2. G. L. Tipoe, M. L. Fung, Respir. Physiol. Neurobiol. 138, 143 (2003).3. S.Y.Lam,G.L.Tipoe,E.C.Liong,M.L.Fung,Histol. Histopathol. 23,
271 (2008).4. Y.Chenet al., Pflügers Archiv 443, 565 (2002).5. J. S. Ye, G. L. Tipoe, P. C. W. Fung, M. L. Fung, Pflügers Archiv 444,
178 (2002).6. P. S. Leung, S. Y. Lam, M. L. Fung, J. Endocrinol. 167, 517 (2000).
7. M. L. Fung, P. S. Leung, in Frontiers in Research of the Renin-Angiotensin System on Human Disease, P. S. Leung, Ed. (Springer-Verlag, Heidelberg, 2007), vol. 7, chap. 8.
8. S. Y. Lam, G. L. Tipoe, Y. W. Tjong, E. C. Liong, M. L. Fung, in Life on the Qinghai-Tibetan Plateau, R. L. Ge, P. Hackett, Eds. (Peking Univ. Med. Press, China, 2007), pp. 323-329.
9. S.Y.Lam,G.L.Tipoe,E.C.Liong,M.L.Fung,Histochem. Cell Biol. 130, 549 (2008).
10. S.Y.Lamet al., Histochem. Cell Biol. 137, 303 (2012).
ACKNOWLEDGMENTSStudies were supported by grants from the Research Grants Council, Hong Kong (Grant No. HKU 766110M, HKU 7510/06M to M.L.F., and CUHK468912 to P.S.L.) and internal funding from the University Research Committee, HKU (to M.L.F. and G.L.T).
FigureÊ 2.Ê SchematicÊ summaryÊ ofÊ theÊ paracrine-autocrineÊ mechanismsÊ thatÊ modulateÊ carotidÊ che-moreceptorÊ activityÊ underÊ hypoxicÊ conditions.Ê Ar-rowsÊ (black)Ê showÊ theÊ cascadeÊ inÊ theÊ physiologicalÊadaptiveÊ responseÊ toÊ chronicÊ hypoxicÊ conditionsÊ atÊhighÊ altitude.Ê RedÊ arrowsÊ highlightÊ theÊ pathophysi-ologicalÊ cascadeÊ inducedÊ byÊ intermittentÊ hypoxia.ÊBidirectionalÊ arrowsÊ (brown)Ê areÊ proposedÊ interac-tionsÊ orÊ crosstalkÊ amongÊ paracrine-autocrineÊ signal-ingÊ pathwaysÊ andÊ theÊ interrelationshipÊ withÊ oxidativeÊstressÊ inducedÊ byÊ intermittentÊ hypoxiaÊ underÊ diseaseÊconditions.
Hypoxic Physiology

The Beijing Institute for Brain Disorders (BIBD) at Capital Medical University (CMU), funded by the Beijing Munici-pal Government, is a research center aimed at understanding the mechanisms underlying brain disorders, and at translating results from the laboratory bench to the patientÕ s bedside, in order to reduce the burdens that the disor-ders impose on patients, families, and society.
CMU is one of the largest medical schools in the world, con-sisting of 10 schools, 18 affiliated hospitals, and 10 teach-ing hospitals with over 24,000 open hospital beds and
more than 10 million outpatient visits per year. The university and itsaffiliatedhospitalshaveastaffof~20,000,among themover1,000 professors and over 2,000 associate professors. CMU has more than 10,000 enrolled graduate and postgraduate students on campus and provides a wide range of educational programs forDoctorate,Master’s,andBachelor’sdegrees,aswellascertifi-cates. Translational neuroscience research is a particular strength of CMU, with experienced research teams that have access to a large and diverse patient population. Research programs and
clinicalservicesinneuroscienceandrelatedfieldsareattheforefrontinChinawithhighlyspecializedhospitalsin neurology (Xuanwu Hospital), neurosurgery (Tiantan and Sanbo Brain Hospitals), psychiatry (Anding Hospi-tal), and rehabilitation (Boai Hospital). The Department of Neurology of Xuanwu Hospital and the Department of Neurosurgery at Tiantan Hospital have both been ranked as number one in China in their respective disciplines. In addition, research centers on stroke, ParkinsonÕ s disease, AlzheimerÕ s disease, epilepsy, brain tumors, and psychiatric diseases are the best in China, boasting large clinical databases and tissue banks. These centers also host National Key Laboratories and have been coordination centers for awards from the National Key Initiatives and Programs. CMU is number one in China with respect to publications in the field of neuroscience in both clinic andbasic research over the past two years. The creation of BIBD represents a meaningful step forward in term of collaboration and productivity, drawing together leading neuroscientists from various disciplines and institutions, inside and outside of CMU, to develop better treatments for a range of neurological and psychiatric conditions. A number of research themes covering various brain disorders―including Parkinson’s disease,Alzheimer’s disease, stroke, epilepsy, cancer, and psychiatricdisorders―arebeingpursuedusingtechniquesrangingfrommolecularbiologytoadvancedinvivostudies.BIBDhasestablishedbeneficialinteractionswithmanyinternationallyrecognizedinstitutionsinthefieldofneuroscience.In fact, BIBD is a founding member of The International Alliance for Translational Neuroscience (IATN) together with Department of Neuroscience at Karolinska Institutet, Massachusetts General Hospital, the McGovern Institute for Brain Research at the Massachusetts Institute of Technology, the Brain Research Center at the University of British Columbia, and the Florey Institute of Neuroscience at the University of Melbourne. IATN aims to achieve decisiveadvancementsinneuroscienceandassociatedfieldsbydevelopinginteractionsbetweenBIBDandtheseprestigious international institutions. BIBD is currently the host institution for IATN. BIBD is recruiting outstanding faculty members at full professor level in the research areas outlined above. We invite candidates who are committed to the highest standards of scholarship and professional activities to apply. BIBD provides a dynamic research environment with faculty actively engaged in translational research in neuroscience. Applicants should have an established research program that can be expected to continue with a high productivity, andastrongrecordofextramuralfunding.BIBDoffersoutstandingoffice,laboratory,andresearchfacilities.
If interested, please e-mail [email protected].
Beijing Institute for Brain Disorders

OVERVIEWFounded in 1927, Qinghai Provincial PeopleÕ s Hospital is a hospital of Western medicine on the Qinghai-TibetPlateau.Withalonghistoryofofferingthefullspectrumoffirst-aidinadditiontoinpa-tient /outpatient healthcare and rehabilitation services, the staff is dedicated to teaching and scien-tificresearch.Ofthe2,089permanentstaff,1,892arehealthcareprofessionals,313areprofessorsand assistant professors, 12 are academic leaders in natural sciences and engineering, and 27 are outstanding specialists awarded a Governmental Special Allowance by the State Council. The hospital has 56 clinical and medical technology departments, four specialized state-level clinical sections, 10 provincial key multidisciplinary healthcare centers, and 32 state/provincial diagnostic centersandmedicalresearch/trainingbases.Theclinicallaboratorycenteristhefirststandardizedlaboratory inQinghai province certified according to ISO 15189 international standards.Qing-hai Provincial PeopleÕ s Hospital has been committed to the advancement of medical techniques to provide the best health care to the diverse ethnic communities on the Qinghai-Tibet Plateau. The researchers at the hospital are dedicated to the exploration of the unique characteristics of high-altitude medicine. With the application of teleconsultation systems, computerized medical informationsystems,and refinedmanagementmechanisms, theyhavebuilt thehospital intoawell-functioning comprehensive public service.
ADVANTAGES AND STRENGTHS Taking full advantage of its unique geographic location, the primary focus of the hospital is clinical research on the diagnosis and treatment of mountain sickness, endemic disease, and critical care inaharshenvironment(lowpressure,oxygendeficiency,andcoldtemperatures).Impressivead-vances have been made in the study of the pathophysiological changes stemming from these en-vironmental challenges. Many publications have come out of this work, including the introduction of the Ò Qinghai CriteriaÓ as the new standard of diagnostic criteria for chronic mountain diseases.
The hospital holds a leadership position in delivering the best quality health care services on the Qinghai-Tibet Plateau and has long been a pioneer in the application of advanced medical tech-nologies and techniques.
The hospital has always been active in providing medical assistance for local communities. Fol-lowingtheearthquakeinYushuprefecture,Qinghaiprovince,onApril14,2010,medicalrescuestaff fromthehospitaldeliveredtimelyandefficientmedical relief toearthquake-strickenareas.Notably, there were no injuries from transportation and no deaths from infections after emergency treatment.
Making full use of the professional knowledge and skills of its specialists and capacity of its multi-disciplinary care centers, the hospital regularly offers professional guidance and medical training for local hospitals in agricultural and pastoral areas, and provides professional health care for a va-riety of large and medium scale events both within and outside of the country, including two scien-tificexpeditionstotheSouthPoleandtenInternationalRoadCyclingRacesaroundQinghaiLake.
SCIENTIFIC RESEARCH ACHIEVEMENTSResearchers at the hospital study a broad range of ailments, including high-altitude pulmonary edema, cerebral edema and functional failure, polycythemia, and other high-altitudeÐ related heart andkidneydiseases.Consistentandunswervingefforthas led tosignificant researchachieve-ments, including the publication of over 3,300 journal articles. Thus far, 1,473 hospital-based re-search programs associated with new services, new technologies, and new surgical advances havebeenconducted.Thesestudieshavebeenawardedonefirstprizeand twosecondprizeNationalScienceandTechnologyProgressAwards,aswellassevenfirstprize,ninesecondprize,and 26 third and fourth prize provincial Science and Technology Progress Awards.
ACADEMIC EXCHANGESQinghai Provincial PeopleÕ s Hospital is committed to training and mentoring medical students from Qinghai, Lanzhou, Suzhou, and Ningxia Medical Universities in order to further enhance aca-demic cooperation and communication with other national and international medical institutions. The hospital currently has a long-term cooperative agreement with the Medical Center of Harvard University in United States, Klinikum Bamberg in Germany, and McMaster University Hospital in Canada. Within China, it also cooperates with Peking Union Medical College Hospital, Peking Uni-versity PeopleÕ s Hospital, China-Japan Friendship Hospital, Beijing Tiantan Hospital, and Beijing Jishuitan Hospital.
Qinghai Provincial PeopleÕ s Hospital continues to strive to build itself into one of the best clinical, research-oriented hospitals in the world.
Qinghai Provincial PeopleÕ s Hospital, ChinaA modern comprehensive public hospital ranked first among hospitals on the Qinghai-Tibet PlateauThird grade A-level general hospital
• Named one of the 100 best hospitals in China• International Research Base for Anoxia Medicine • National Clinical Research Center for High Altitude Medicine• Regional Center for Healthcare on the Qinghai-Tibet Plateau