
Therapeutics II TH4002 Spring 2004 Pharmacotherapy of ... · Pharmacotherapy of Diabetes Mellitus...
23
1 Therapeutics II TH4002 Spring 2004 Pharmacotherapy of Diabetes Mellitus John M. Burke, Pharm.D., BCPS Required Reading: Pharmacotherapy: A Pathophysiologic Approach. 5 edition. Diabetes Mellitus. pp. 1335-1358 th Recommended Readings: Diabetes Control and Complications Trial Research Group: The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med 1993; 329: 977-86. UK Prospective Diabetes Study Group: Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes. (UKPDS 33) Lancet 1998; 352: 837- 53. UK Prospective Diabetes Study Group: Effect of intensive blood glucose control with metformin on complications in overweight patients with type 2 diabetes (UKPDS 34). Lancet 1998; 352: 854-65. OUTCOMES: Topic-specific Abilities 1. The student should be able to ASSESS a patient with Diabetes This includes: Assessment and classification of the problem (Type 1 DM, Type 2 DM, IFG, IGT, normal glucose tolerance); assessment of severity of hyperglycemia and level of overall glucose control; identification of any drug-induced causes of hyperglycemia; identification of acute or chronic complications related to diabetes; justifying assessment based on analysis of data; appropriately interpreting data; description of pathophysiology of diabetes and relating the mechanism of disease and the clinical manifestations present in the patient. 2. The student should be able to EVALUATE therapy for a patient with diabetes This includes: evaluation of appropriateness of choice of agent (indication and no contraindication), appropriateness of dose and evaluation of adequacy of current dose in relationship to efficacy (based on BS readings and HbA1c) in controlling diabetes; identification of adverse effects related to medications used for the treatment of diabetes; identification of significant drug interactions; identification of factors likely influencing patient adherence to therapy; supporting evaluation with drug and patient-specific data; using literature (DCCT, UKPDS) to support evaluation 3. The student should be able to SELECT/RECOMMEND therapy for a patient with diabetes. This includes: Discontinuing inappropriate or ineffective medications or those causing unmanageable adverse effects; titrating doses for medications to achieve optimal glucose control; initiating therapy for patients requiring the addition of new agents; adding other therapies which are necessary for managing commonly co- existing conditions in diabetes (aspirin for MI prophylaxis; antihypertensives; antihyperlipidemic therapies); non-pharmacologic therapies; justifying decisions based on patient-specific, disease-specific, and drug-specific information; using literature to support drug therapy decisions, when appropriate; upon questioning, explaining why other agents were not chosen; using literature to support drug therapy decisions, when appropriate.
-
Upload
nguyenminh -
Category
Documents
-
view
218 -
download
1
Transcript of Therapeutics II TH4002 Spring 2004 Pharmacotherapy of ... · Pharmacotherapy of Diabetes Mellitus...

1
Therapeutics II TH4002 Spring 2004Pharmacotherapy of Diabetes Mellitus
John M. Burke, Pharm.D., BCPS
Required Reading:
Pharmacotherapy: A Pathophysiologic Approach. 5 edition. Diabetes Mellitus. pp. 1335-1358th
Recommended Readings:
Diabetes Control and Complications Trial Research Group: The effect of intensive treatment of diabetes on thedevelopment and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med 1993;329: 977-86.
UK Prospective Diabetes Study Group: Intensive blood-glucose control with sulphonylureas or insulin compared withconventional treatment and risk of complications in patients with type 2 diabetes. (UKPDS 33) Lancet 1998; 352: 837-53.
UK Prospective Diabetes Study Group: Effect of intensive blood glucose control with metformin on complications inoverweight patients with type 2 diabetes (UKPDS 34). Lancet 1998; 352: 854-65.
OUTCOMES:
Topic-specific Abilities
1. The student should be able to ASSESS a patient with DiabetesThis includes: Assessment and classification of the problem (Type 1 DM, Type 2 DM, IFG, IGT, normalglucose tolerance); assessment of severity of hyperglycemia and level of overall glucose control; identificationof any drug-induced causes of hyperglycemia; identification of acute or chronic complications related todiabetes; justifying assessment based on analysis of data; appropriately interpreting data; description ofpathophysiology of diabetes and relating the mechanism of disease and the clinical manifestations present inthe patient.
2. The student should be able to EVALUATE therapy for a patient with diabetesThis includes: evaluation of appropriateness of choice of agent (indication and no contraindication),appropriateness of dose and evaluation of adequacy of current dose in relationship to efficacy (based on BSreadings and HbA1c) in controlling diabetes; identification of adverse effects related to medications used forthe treatment of diabetes; identification of significant drug interactions; identification of factors likelyinfluencing patient adherence to therapy; supporting evaluation with drug and patient-specific data; usingliterature (DCCT, UKPDS) to support evaluation
3. The student should be able to SELECT/RECOMMEND therapy for a patient with diabetes.This includes: Discontinuing inappropriate or ineffective medications or those causing unmanageable adverseeffects; titrating doses for medications to achieve optimal glucose control; initiating therapy for patientsrequiring the addition of new agents; adding other therapies which are necessary for managing commonly co-existing conditions in diabetes (aspirin for MI prophylaxis; antihypertensives; antihyperlipidemic therapies);non-pharmacologic therapies; justifying decisions based on patient-specific, disease-specific, and drug-specificinformation; using literature to support drug therapy decisions, when appropriate; upon questioning, explainingwhy other agents were not chosen; using literature to support drug therapy decisions, when appropriate.

2
4. The student should be able to MONITOR therapy for a patient with diabetesThis includes: identification of symptoms, physical findings, and laboratory or other tests which can helpyou assess or re-assess the patient’s diabetes and glycemic control; identification of symptoms, physicalfindings, and laboratory parameters which can help identify or detect the presence of adverse effects totherapy, particularly drug-induced hypoglycemia; Each parameter must be specific and justifiable based onthe value in detecting efficacy or adverse effects from a specific medication
5. The student should be able to EDUCATE the patient about diabetes and therapies:This includes: explanations about diabetes, its symptoms, and complications; discussion about therapies fordiabetes, how they work, adverse effects, and proper administration; detection and management of drug-induced hypoglycemia.
CONTENT QUESTIONS
1. Identify risk factors associated with the development of diabetes mellitus
2. List symptoms commonly associated with diabetes mellitus
3. Define the criteria necessary for the diagnosis of diabetes and use them to determine whether a patient hasdiabetes, impaired glucose tolerance, impaired fasting glucose, or normal glucose tolerance.
4. Distinguish characteristics of Type 1 and Type 2 diabetes mellitus based upon: age of onset, C-peptidelevels, symptomatology, body habitus, and treatment options available.
5. Identify drug-induced causes of hyperglycemia and explain the mechanisms responsible for hyperglycemia
6. Define the goals of therapy of diabetes for pre-prandial BS, bedtime BS, and HbA1c.
7. Given a HbA1c value, determine the corresponding mean glucose concentration.
8. Explain the rationale for achieving tight-glycemic control and define the expected outcomes.
9. List the complications associated with long-standing diabetes and the criteria for assessing their presence.
10. Describe the components of non-drug therapy for diabetes
11. What is considered an adequate trial of non-pharmacologic therapy before the addition of drug therapy?
12. Describe the mechanism of action of sulfonylureas, repaglinide, nateglinide, metformin, α-glucosidaseinhibitors, thiazolidinediones, and insulin in the management of diabetes.
13. Describe the common side effects associated with each of the therapies used in the management o fdiabetes..
14. List risk factors associated with the development of metformin-induced lactic acidosis.
15. Describe the proper management of metformin therapy for a patient who is to receive radiocontrast dye.
16. Define the onset, peak, and duration of action of: lispro, insulin aspart, regular, NPH, PZI, and Ultra-lenteinsulins and insulin glargine.
3
17. Based on the time course of insulin activity, define the insulin dose to target based on the time of bloodglucose testing (fasting, noon, pre-dinner, bedtime, or 3am).
18. Describe the symptoms associated with hypoglycemia
19. List potential causes of hypoglycemia in a patient with diabetes
20. List the advantages and disadvantages of urine glucose testing, home blood glucose testing, monitoring ofhemoglobin A1c, urine ketones, and urine protein.
21. How often should hemoglobin A1c be monitored?

4
I. Introduction/Definition
A. DIABETES MELLITUS: a heterogenous disorder characterized by abnormal carbohydratemetabolism secondary to an absolute deficiency of insulin (Type 1) or a relative deficiency ofinsulin (Type 2) resulting in hyperglycemia.
II. ASSESSMENT OF DIABETES MELLITUS
A. Screening Identify Risk Factors
What are 8 Risk factors associated with the development of diabetes mellitus?1.
2.
3.
4.
5.
6.
7.
8.
B. Patient AssessmentList Symptoms commonly associated with diabetes mellitus
1.2.3.4.5.6.7. Others:
C. HyperglycemiaWhat is normal fasting blood glucose concentration?
D. Diagnosis of Diabetes MellitusList the 3 diagnostic criteria for Diabetes Mellitus(Diabetes Care 2004; 27(Suppl 1) or DiPiro’s, 5 edition, pp. 1337)th
1.
2.
3.
5
E. Classification of Diabetes Mellitus
Compare/Contrast the 2 major types of diabetes mellitus for each of the followingType 1 Type 2
Incidence
Age at onset
Pancreatic function
Symptoms
Body Habitus
Treatment
F. Complete Assessment of a Patient with Diabetes should include:
1. Severity of Hyperglycemia2. Type/classification of diabetes3. Etiology for secondary causes (see pp. 1343 for discussion of drug-induced causes)4. Complications present in the patient
III. Establishing Goals of Therapy
A. Normalization of Blood Glucose Concentrations
B. Normalization of glycosylated hemoglobin
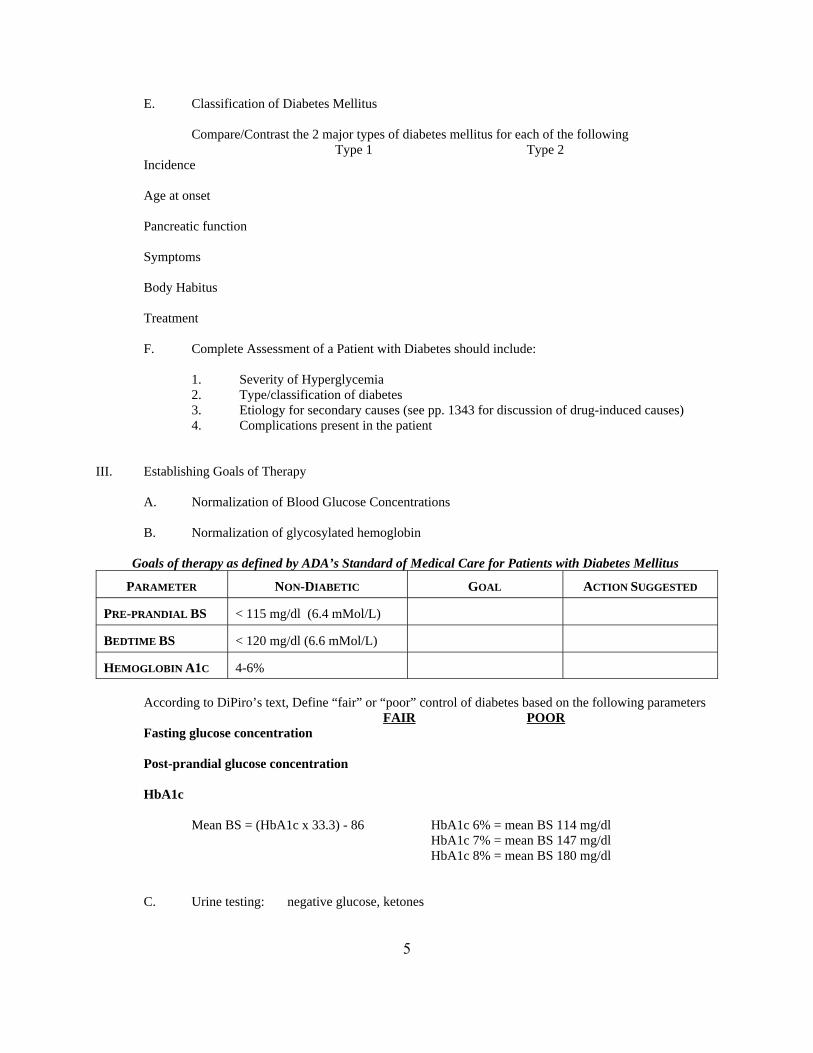
Goals of therapy as defined by ADA’s Standard of Medical Care for Patients with Diabetes Mellitus
PARAMETER NON-DIABETIC GOAL ACTION SUGGESTED
PRE-PRANDIAL BS < 115 mg/dl (6.4 mMol/L)
BEDTIME BS < 120 mg/dl (6.6 mMol/L)
HEMOGLOBIN A1C 4-6%
According to DiPiro’s text, Define “fair” or “poor” control of diabetes based on the following parametersFAIR POOR
Fasting glucose concentration
Post-prandial glucose concentration
HbA1c
Mean BS = (HbA1c x 33.3) - 86 HbA1c 6% = mean BS 114 mg/dlHbA1c 7% = mean BS 147 mg/dlHbA1c 8% = mean BS 180 mg/dl
C. Urine testing: negative glucose, ketones

6
D. Symptomatic Improvement: hyperglycemic symptomshypoglycemic symptoms
E. Normalize nutrition: achieve ideal body weightmaintain normal growth & development
F. Normal/Flexible Lifestyle
G. Avoid/Prevent/Minimize Complications
Diabetes Control and Complications Trial (N Engl J Med 1993)Compared the rate of complications in patients with type 1 diabetes who received intensive insulin therapy vs thosewho received “conventional therapy”
UKPDS StudyPatients with Type 2 diabetes
Outcomes:Intensive glycemic control reduces the risk of retinopathy/nephropathy by 25%Every 1% point reduces the risk of microvascular disease by 35% and the risk of diabetes-related death by25%

Diagnosis of Type 2 Diabetes
Insulin
Severe HyperglycemiaPregnancy
Ketosis
Diet/Exercise
Oral Monotherapyoral hypoglycemic
or metformin
Combination Oral therapyoral hypoglycemic + metformin
Add "-glucosidase inhibitor
Add thiazolidinedione
Add Bedtime NPH
7
IV. General Approach to Therapy for Type 2 Diabetes
A 57 year-old male (height 6'0", Weight 225 lbs) who presented to the clinical was found to have a fastingplasma glucose of 180 mg/dl on routine screening. It was subsequently repeated and found to be 170 mg/dl. Hedenies any symptoms of diabetes.FH: [+] diabetes in an older brother and father SH:[+] tobacco, occasional ethanolMedications: none PE: unremarkable Lab: otherwise wnl
1. Provide an ASSESSMENT of this patient’s hyperglycemia
2. How should this patient be initially treated?
V. Non-Drug Therapy
A. Dietary Management1. Sufficient caloric intake to achieve ideal body weight2. Regularly scheduled meals- to prevent hypoglycemia3. Nutritional content
a. carbohydrates: 55-60% of total caloriesb. fats: < 30% of total calories (avoid saturated fats)

GLUT-2Glucose Glucose
Na-KATPase
K+
Na+
Gluc-6-PO4
Glucokinase
ATP
[+]
[-]
K+
Ca++
insulin
Pancreatic β cells
[+]
Pro-insulin insulin
GLUT-2Glucose Glucose
Na-KATPase
K+
Na+
Gluc-6-PO4
Glucokinase
ATP
[+]
[-]
K+
Ca++
insulin
Pancreatic β cells
[+]GLUT-2
Glucose GlucoseGLUT-2
Glucose GlucoseGlucose Glucose
Na-KATPase
K+
Na+
Gluc-6-PO4
Glucokinase
ATP
[+]
[-]
K+
Ca++
insulin
Pancreatic β cells
[+]
Pro-insulin insulin
8
c. cholesterol: less than 300 mg/dayd. protein: 10-20% of total calories (0.8 gm/kg/day)
4. Alcohol:CAUTIONS: hypoglycemia--alcohol suppresses gluconeogenesis
hyperglycemia-excessive, chronic usereactions with sulfonylureas
B. Exercise1. Benefits: improves blood glucose control
increases peripheral circulationkeeps the patient fitimproves sense of well-beingreduces cardiovascular risk
2. cautions: avoid hypoglycemiamay increase the rate of insulin absorption
What is considered an adequate trial of non drug therapy before the addition of drug therapy?
The patient returns to follow-up after the initial intervention. He remains asymptomatic, but hisfasting blood glucose remains from 180-200 mg/dl.
What pharmacologic treatment options are available?
How should he be treated (drug, dose, route, frequency, rationale)
VI. Sulfonylureas
A. Pharmacology

9
B. Indications: Type 2 diabetes mellitusCharacteristics which favor positive response
1. Type 2 diabetes mellitus2. new onset disease3. mild hyperglycemia
-FBS < 200 mg/dl (< 11mmol/l)-insulin requirements < 40-50 units/day
4. obesity at initial presentation
C. Contraindications1. Type 1 diabetes mellitus2. pregnancy3. documented hypersensitivity reactions4. severe hepatic/renal dysfunction5. during severe illness, surgery, or stress
D. Adverse Effects1. Hypoglycemia: may be more severe, more prolonged than with insulin2. Gastrointestinal: nausea, fullness, indigestion
-management: take agent with food reduce the dose
3. Hematologic: eosinophilia, leukopenia, anemia, agranulocytosis, pancytopenia
4. Disulfiram-like reactionsManifestations: alcohol-related flush
headachelightheadedness, nauseavomiting, hypotension (v. rarely)
-most commonly occurs with chlorpropamide-management-if necessary, switch to another agent
5. Hyponatremia/SIADHa. mechanism-enhanced release and increased renal response to ADHb. Risk factors: elderly; diuretic therapy
CHF increase water intakechlorpropamide (high doses); tolbutamide
c. Onset: days to weeks after an increase in dose
6. Hepatotoxicity-Rare: hypersensitivity reactions-mild intrahepatic cholestasis
-mild increase in LFT's; rash; fever; eosinophilia
7. Dermatologicrash: maculopapular, erythematous
on face, neck, trunk, or upper armscross-sensitivity with other sulfonylureas, sulfonamides
8. Cardiovascular EffectsNot significant based on UKPDS results

10
E. Dosing/Administration
1. General Principlesa. Depending upon BS level, begin with low to moderate dosesb. Re-evaluate and adjust doses no more often than weeklyc. Average reduction in BS expected approximately 60 mg/dl; may be greater with
weight loss and exercise
DRUG AVAILABILITY IN U.S. DOSING
Tolbutamide 250, 500 mg tabs (scored) 0.5-3 g/day in 2-3 divided dosesadminister 30 minutes before meals
chlorpropamide 100, 250 mg tabs (scored) 100-500 mg/day in single dose
acetohexamide 250, 500 mg tabs (scored) 250-1500 mg/day in 1-2 divided doses
tolazamide 100, 250, 500 mg tabs (scored) 100-1000 mg/day in 1-2 divided doses
glipizide 5, 10 mg tabs (scored) 2.5-40 mg/day in 1-2 divided doses 5, 10 mg SR tabs If > 15 mg/day divide or use XL
administer 30 minutes before meals
glyburide 1.25, 2.5, 5 mg tabs (scored) 1.25-20 mg/day in 1-2 divided doses
glyburide (micronized) 3, 6 mg tabs 0.75-12 mg/day in 1-2 divided dosesdivide if > 6 mg/day
glimepiride 1, 2 mg tabs 1-8 mg/day in single daily dose
1. tolbutamide: short duration may make it useful in patients prone to hypoglycemiaMultiple daily doses may decrease compliance
2. chlorpropamide Convenient once daily dosingvariable renal excretionlong half-life/duration of actionincreased incidence of adverse effectshypoglycemia may be prolongednot recommended in elderly/renal disease patients
3. acetohexamide intermediate duration with convenient dosingactive metabolite is excreted renallyavoid in elderly/renal disease patients
4. tolazamide metabolized to inactive metabolitesintermediate duration with convenient dosing
5. glipizide intermediate duration with convenient dosingmetabolized to inactive metabolitesabsorption is impaired by food
6. glyburide intermediate duration with convenient dosing absorption is not affected by food

11
VII. Meglitinides
A. Mechanism of Action: stimulates rapid release of insulin from the pancreas; does not stimulatethe sulfonylurea receptor. Average decrease in FBS 60 mg/dl (3.3 mmol/l)
B. Pharmacokinetics: Rapidly absorbed after oral administrationHepatically metabolized via oxidation & conjugation; involves CYT 3A4Mean t ½ : 1-1.4 hrs
C. Dosing and Administration: repaglinide (Prandin) 0.5, 1, 2 mg tabletsOne tablet before/at the time of each mealDoses should be skipped when a meal is skipped
D. Adverse Effects Hypoglycemia
VIII. Nateglinide (Starlix)
A. Mechanism of Action: Stimulates ATP-sensitive K+ channels in pancreatic beta cells, therebystimulating rapid release of insulin; rapid dissociation from binding sites
B. Clinical efficacy: decreases HbA1c by 0.6-0.8%Greater reduction when combined with metformin or glitazones
C. Dosing/Administration:Availability: 60, 120 mg tabletsDose: 60-120 mg PO TID taken within 30 minutes prior to meals
The patient returns for follow-up evaluation with blood glucose concentrations of 200-234 mg/dl. He states thathe is compliant with the regimen previously prescribed (details available in class).
What is your EVALUATION of his current therapy?
Provide recommendations for changes in his therapy. (Plan for existing therapy, additional Drug, dose, route,frequency, rationale)
VIII. MetforminA. Chemistry: Biguanide
B. Pharmacology: Antihyperglycemic effects
12
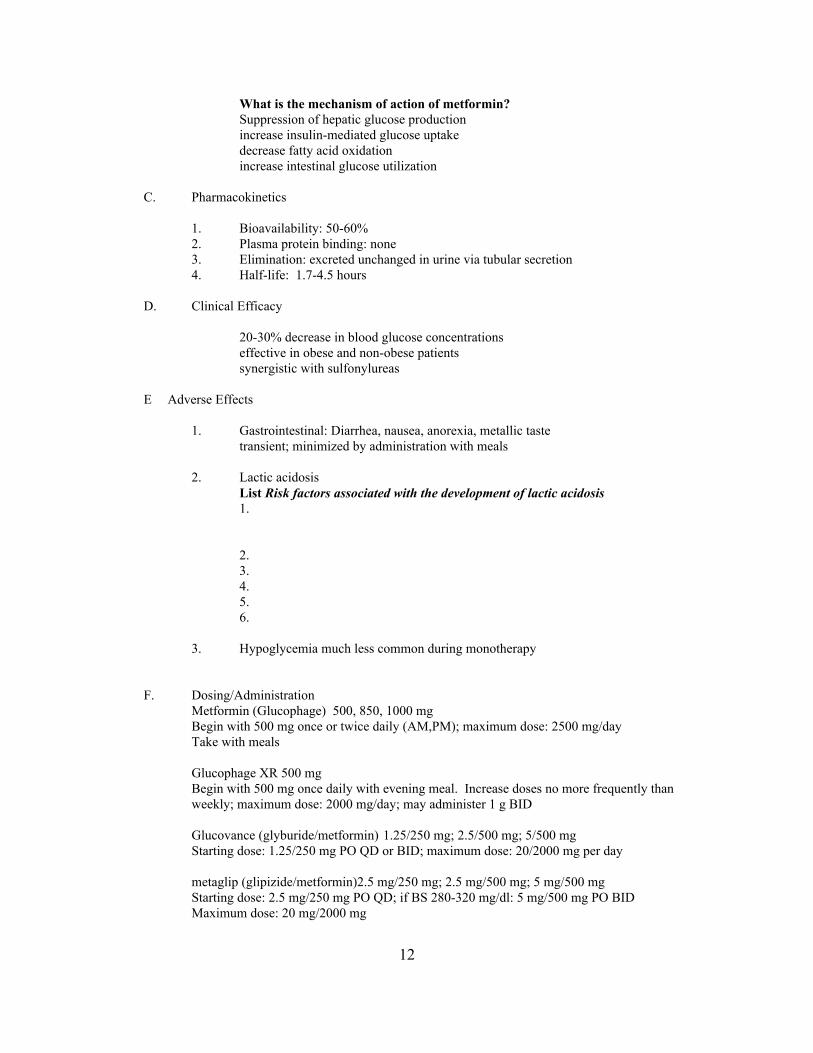
What is the mechanism of action of metformin?Suppression of hepatic glucose productionincrease insulin-mediated glucose uptakedecrease fatty acid oxidationincrease intestinal glucose utilization
C. Pharmacokinetics
1. Bioavailability: 50-60%2. Plasma protein binding: none3. Elimination: excreted unchanged in urine via tubular secretion4. Half-life: 1.7-4.5 hours
D. Clinical Efficacy
20-30% decrease in blood glucose concentrationseffective in obese and non-obese patientssynergistic with sulfonylureas
E Adverse Effects
1. Gastrointestinal: Diarrhea, nausea, anorexia, metallic tastetransient; minimized by administration with meals
2. Lactic acidosisList Risk factors associated with the development of lactic acidosis1. 2. 3. 4. 5. 6.
3. Hypoglycemia much less common during monotherapy
F. Dosing/AdministrationMetformin (Glucophage) 500, 850, 1000 mg Begin with 500 mg once or twice daily (AM,PM); maximum dose: 2500 mg/dayTake with meals
Glucophage XR 500 mgBegin with 500 mg once daily with evening meal. Increase doses no more frequently thanweekly; maximum dose: 2000 mg/day; may administer 1 g BID
Glucovance (glyburide/metformin) 1.25/250 mg; 2.5/500 mg; 5/500 mgStarting dose: 1.25/250 mg PO QD or BID; maximum dose: 20/2000 mg per day
metaglip (glipizide/metformin)2.5 mg/250 mg; 2.5 mg/500 mg; 5 mg/500 mgStarting dose: 2.5 mg/250 mg PO QD; if BS 280-320 mg/dl: 5 mg/500 mg PO BIDMaximum dose: 20 mg/2000 mg

GlucoseFructose
GlucoseGalactose
ABSORPTION
Starch DisaccharidesSucrose Lactose
MonosaccharidesFructoseGlucose
MaltoseMaltotrioseDextrins
Glucose
α-amylase
α-glucosidases
α-glucosidases Lactase
13
IX. Alpha-glucosidase Inhibitors
A. Mechanism of Action
Describe the mechanism of action of acarbose in the management of diabetes.
B. Therapeutic Responseattenuation of post-prandial hyperglycemiaaverage blood glucose decrease: 40-50 mg/dLaverage decrease in hgb A : 0.65-1.4%1c
C. Adverse EffectsWhat are the adverse effects associated with alpha-glucosidase inhibitors?
Based on your understanding of the mechanism of action, how would you treat hypoglycemia in apatient receiving an alpha-glucosidase inhibitor?
D. Dosing/Administrationacarbose (Precose) miglitol (Glyset)Week 1-2 25 mg once daily with dinnerWeek 3-4 25 mg twice daily with breakfast and dinnerWeek 5-12 25 mg three times daily with mealsMaintenance 50 mg three times daily with mealsMaximum 100 mg three times daily with meals

GLUCOKINASEPROMOTER
GLUCOSE
Peroxisome Proliferator-Activated Receptor-gamma
Adipose tissueskeletal muscleLiver
Thiazolidinediones
14
X. Thiazolidinedione
A. Chemistry: thiazolidinedione
B. Mechanism of Action: binds to activated receptors in the nucleus of the cell which stimulates DNAtranscription and enhances the action of glucose.
Activation of glucokinase promoter increases glucose transport into the cell. Enhances insulin sensitivity in skeletal muscle, liver, and adipose tissue
C. Pharmacokinetics1. Pioglitazone
Bioavailability not affected by food; absorption somewhat slowedMetabolized by hydroxylation and oxidation; CYP 3A4elimination t ½ : 3-7 hours
2. RosiglitazoneBioavailability: 99%Food decreases peak concentration and delays peak but no change in bioavailabilityHighly bound to plasma proteins (99.8%)Metabolized by N-demethylation and hydroxylation followed by conjugationPrimarily metabolized via CYP 2C8; CYP 2C9 is a minor pathwayelimination t ½ : 3-4 hours
D. Role in therapyLowers fasting and post-prandial blood glucose concentrationsRosiglitazone reduces hemoglobin A1c: 1-1.5% ptsMay be used in combination with sulfonylureas, metformin, and insulin

15
E. Dosage/Administrationtroglitazone (Rezulin) off the market
rosiglitazone (Avandia)Availability: 2, 4, 8 mg May be used as monotherapy or in combinationDosage: Initial dose: 4 mg once daily or 2 mg BID
May be increased to 8 mg/day after 12 weeks if neededMay take with or without food
Pioglitazone (Actos)Availability: 15, 30, 45 mgDosage: 15-45 mg/day as a single daily dose
May take with or without food
F. Precautions/Adverse Effects
1. Hepatotoxicity: idiosyncratic hepatocellular injury
Monitoring for rosiglitazone; pioglitazoneObtain baseline serum transaminases, do not start if ALT > 2.5 times ULNMonitor every 2 months for the first 12 months and periodically thereafterpatients with mild elevations at baseline (1-2.5 x ULN) should be monitored morefrequently
2. Hypoglycemia
3. Gastrointestinal
4. Hematologic
5. Congestive Heart Failure
XI. Insulin
A Factors to be considered in developing an insulin regimen
1. type(s) of insulin to be used
2. dose(s) of insulin to be used
3. time(s) of insulin administration
16
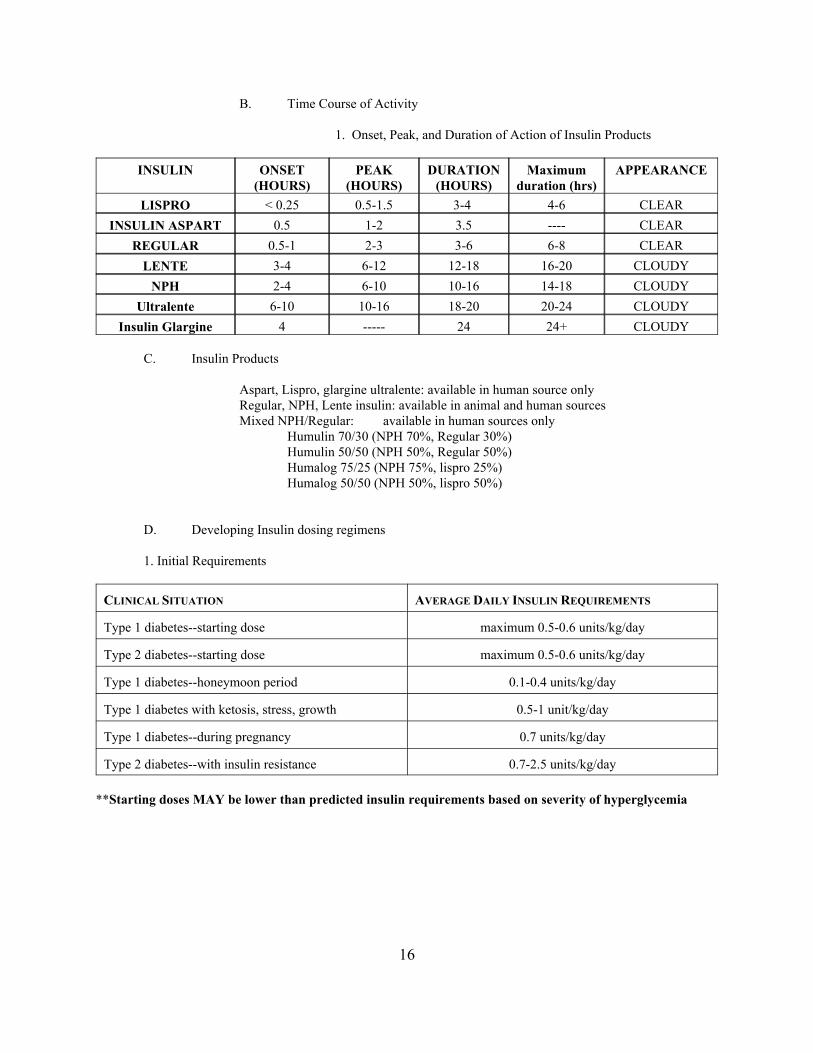
B. Time Course of Activity
1. Onset, Peak, and Duration of Action of Insulin Products
INSULIN ONSET PEAK DURATION Maximum APPEARANCE(HOURS) (HOURS) (HOURS) duration (hrs)
LISPRO < 0.25 0.5-1.5 3-4 4-6 CLEARINSULIN ASPART 0.5 1-2 3.5 ---- CLEAR
REGULAR 0.5-1 2-3 3-6 6-8 CLEARLENTE 3-4 6-12 12-18 16-20 CLOUDY
NPH 2-4 6-10 10-16 14-18 CLOUDYUltralente 6-10 10-16 18-20 20-24 CLOUDY
Insulin Glargine 4 ----- 24 24+ CLOUDY
C. Insulin Products
Aspart, Lispro, glargine ultralente: available in human source onlyRegular, NPH, Lente insulin: available in animal and human sourcesMixed NPH/Regular: available in human sources only
Humulin 70/30 (NPH 70%, Regular 30%)Humulin 50/50 (NPH 50%, Regular 50%)Humalog 75/25 (NPH 75%, lispro 25%)Humalog 50/50 (NPH 50%, lispro 50%)
D. Developing Insulin dosing regimens
1. Initial Requirements
CLINICAL SITUATION AVERAGE DAILY INSULIN REQUIREMENTS
Type 1 diabetes--starting dose maximum 0.5-0.6 units/kg/day
Type 2 diabetes--starting dose maximum 0.5-0.6 units/kg/day
Type 1 diabetes--honeymoon period 0.1-0.4 units/kg/day
Type 1 diabetes with ketosis, stress, growth 0.5-1 unit/kg/day
Type 1 diabetes--during pregnancy 0.7 units/kg/day
Type 2 diabetes--with insulin resistance 0.7-2.5 units/kg/day
**Starting doses MAY be lower than predicted insulin requirements based on severity of hyperglycemia
5pm12N7am 10pm 7am5pm12N7am 10pm 7am
17
For each of the following insulin regimens, draw the approximate time course of activity based on the onset, peak,and duration of the insulins used.
a. Mixed Split Regimen7 am (before breakfast) NPH + Reg (2/3 daily dose)5 pm (before supper) NPH + Reg (1/3 daily dose)
b. Three Daily Injections7am (before breakfast) NPH + Reg (2/3 daily dose)5pm (before supper) Reg (1/6 daily dose)10pm (HS) NPH (1/6 daily dose)

5pm12N7am 10pm 7am5pm12N7am 10pm 7am
18
c. Long-acting insulin + bolus doses of Regular(Complex; reserve for difficult to control patients7 am: Ultra-lente or PZI (2/5 of daily dose)7 am, 12noon, 5pm (AC): Pre-prandial regular or lispro (each 1/5 of daily dose)
d. Bedtime NPH insulin combined with day-time sulfonylureasBedtime: NPH insulin

19
e. Insulin glargine
Based on the above time courses of insulin activity, which insulin doses should be targeted for each of thefollowing blood sugars monitored:
TESTING TIME INSULIN DOSE TO TARGET MEAL/SNACK TO TARGET
Fasting Glucose Evening or bedtime NPH bedtime snack
Pre-lunch Glucose AM regular insulin breakfast or AM snack
Pre-dinner Glucose AM NPH insulin lunch or PM snack
Bedtime Glucose PM regular insulin dinner
3 AM or later PM NPH insulin dinner or bedtime snack
b. Supplemental insulin doses-additional doses of Regular insulin administered in response to an elevated bloodglucose concentration-for outpatients: 1-2 units/50 mg/dl elevation above normal
c. Sliding scale insulin: a scale designed to provide supplementary short-acting(regular) insulin in varied amounts based on the degree of elevation in blood sugarmeasured.
Example 1 Example 2BS < 70 mg/dl: call physician BS < 70 mg/dl: call M.D.BS 70-200mg/dl: 0 units BS 70-300 mg/dl: 0 unitsBS 201-300 mg/dl:2 units BS 300-400 mg/dl; 4 unitsBS 301-400 mg/dl:4 units BS > 400 mg/dl call M.D.BS 401-500 mg/dl:6 unitsBS > 500 mg/dl: call physician

20
d. Anticipatory dosing-increasing/decreasing dosing based on changes in diet or
physical activity
1. Diet-increase Reg insulin dose by 1-2 units for each additional 20 gm CHO (80 kcal)
2. Exercise-Check BS before, during, and after exercise-with Moderate exercise, dec REG by 30-50%-if BS is low/normal, supplemental snack
e. Sick Day Management1. Patients should continue to take insulin2. Monitor blood sugars more closely3. Try to drink/eat as regularly as possible
H. Administration of Insulin1. Describe step by steps procedure for measuring and administering a
subcutaneous insulin dose.Wipe insulin vial and injection site with alcohol swabRoll insulin vial to mixDraw up air equal to the amount of insulin needed and inject into insulin vialInvert the insulin vial and draw up the desired amount of insulinRemove air from syringePinch skin at the injection site and inject the needle at a 45 degree angleInject the insulin and remove needle
When mixing NPH and Regular insulin in the same syringe, which insulin should bedrawn into the syringe first? Why?
3. Injection sites:Identify possible and optimal injection sites for SQ insulin administration.

HYPOGLYCEMIA SUSPECTED
CHECK BLOOD SUGAR
BS < 70 mg/dl
SEVERE SYMPTOMS
RE-EVALUATEIV DEXTROSESQ GLUCAGON
ORAL GLUCOSE
CONSIDEROTHERCAUSES
NO
YES
YES NO
21
I. Storage of Insulin
How long can insulin be safely stored at controlled room temperature?
How long can it be safely stored in a refrigerator?
J. Adverse Effects
1. Hypoglycemia
Defined as Blood Glucose Concentration < __________
A. Clinical Manifestations:List the clinical manifestations of hypoglycemia.
B. Causes: List 5 potential causes of hypoglycemia in a patient with diabetes.
1.
2.3.4.5.
C. Management
What doses are recommended for IV dextrose and SQ glucagon to treat severe hypoglycemia?

22
XII. Monitoring of the patient with Diabetes
A. Blood glucose monitoringvisual method: Chemstrips; Glucostix, Visidex (visual only)
reflectance meters:List advantages and disadvantages of blood glucose monitoring for the patient with diabetes
1. Advantages:
2. Disadvantages:
3. Monitoring times:
At What times in the day should blood glucose be monitored in a patient with diabetes
C. Hemoglobin A (glycosylated Hgb)1c
Why does hemoglobin A1c reflect long-term control of diabetes mellitus?How often should hemoglobin A1c be monitored?
D. Urine Ketone Testing: Acetest; Ketostix; Chemstrip-K
What information is obtained by urine ketone testing?
Which patients should be monitored in this manner?
E. Monitoring for proteinuria and progression of renal disease (refer to Therapeutics I)24-hour urine collectionUrine albumin:creatinine ratioSpot microalbumin

23
XIII. Areas of Patient Education
1. Diabetes: describe pathogenesis and complications2. Hyperglycemia signs and symptoms3. Ketoacidosis: sign/symptoms; significance of urine ketones4. Hypoglycemia: signs/symptoms
treatment5. Diet/Exercise: effect on blood glucose concentration and insulin dose6. Insulin
a. Typesb. injection techniquec. onset/peak actionsd. storagee. stability
7. Monitoring: urine/blood glucose testinginterpretation of results
8. Foot care: inspect feet dailywear well-fitted shoesavoid self-care of ingrown toenails, corns and athlete's foot
9. Sick Day Management10. Cardiovascular risk factors
-Hypertension (goal BP < 130/80 or < 125/75 if proteinuria > 1 g/day)-Smoking-Obesity-Hyperlipidemia (goal LDL < 100 mg/dl)Prophylactic aspirin use is recommended
11. Annual eye examinations
XIV. Conclusions/Summary


















