Therapeutic strategies to overcome crizotinib resistance ... · Therapeutic strategies to overcome...
6
Therapeutic strategies to overcome crizotinib resistance in non-small cell lung cancers harboring the fusion oncogene EML4-ALK Ryohei Katayama a,b , Tahsin M. Khan a,c , Cyril Benes a,b , Eugene Lifshits a , Hiromichi Ebi a,b , Victor M. Rivera d , William C. Shakespeare d , A. John Iafrate b,e , Jeffrey A. Engelman a,b,1 , and Alice T. Shaw a,b,c,1 a Massachusetts General Hospital Cancer Center, Boston, MA 02129; b Department of Medicine, Harvard Medical School, Boston, MA 02115; c Koch Institute for Integrative Cancer Research, Massachusetts Institute of Technology, Cambridge, MA 02139; d ARIAD Pharmaceuticals, Cambridge, MA 02139; and e Department of Pathology, Massachusetts General Hospital, Boston, MA 02114 Edited by Peter K. Vogt, The Scripps Research Institute, La Jolla, CA, and approved March 23, 2011 (received for review December 27, 2010) The echinoderm microtubule-associated protein-like 4 (EML4)- anaplastic lymphoma kinase (ALK) fusion oncogene represents a molecular target in a small subset of non-small cell lung cancers (NSCLCs). This fusion leads to constitutive ALK activation with potent transforming activity. In a pivotal phase 1 clinical trial, the ALK tyrosine kinase inhibitor (TKI) crizotinib (PF-02341066) demon- strated impressive antitumor activity in the majority of patients with NSCLC harboring ALK fusions. However, despite these remark- able initial responses, cancers eventually develop resistance to cri- zotinib, usually within 1 y, thereby limiting the potential clinical benefit. To determine how cancers acquire resistance to ALK inhib- itors, we established a model of acquired resistance to crizotinib by exposing a highly sensitive EML4-ALK–positive NSCLC cell line to increasing doses of crizotinib until resistance emerged. We found that cells resistant to intermediate doses of crizotinib developed amplification of the EML4-ALK gene. Cells resistant to higher doses (1 μM) also developed a gatekeeper mutation, L1196M, within the kinase domain, rendering EML4-ALK insensitive to crizotinib. This gatekeeper mutation was readily detected using a unique and highly sensitive allele-specific PCR assay. Although crizotinib was ineffectual against EML4-ALK harboring the gatekeeper mutation, we observed that two structurally different ALK inhibitors, NVP- TAE684 and AP26113, were highly active against the resistant can- cer cells in vitro and in vivo. Furthermore, these resistant cells remained highly sensitive to the Hsp90 inhibitor 17-AAG. Thus, we have developed a model of acquired resistance to ALK inhibitors and have shown that second-generation ALK TKIs or Hsp90 inhib- itors are effective in treating crizotinib-resistant tumors harboring secondary gatekeeper mutations. F irst described in 2007, the oncogenic fusion kinase echinoderm microtubule-associated protein-like 4-anaplastic lymphoma kinase (EML4-ALK) is present in ∼4% of patients with non-small cell lung cancer (NSCLC) (1). Chromosomal translocations in- volving ALK also occur in other cancers, including anaplastic large cell lymphomas and inflammatory myofibroblastic tumors. In all cases, the fusion partner (e.g., EML4) is believed to mediate ligand-independent oligomerization of ALK, resulting in consti- tutive ALK kinase activation (2–4). In cell line and genetically engineered mouse models, EML4-ALK serves as a potent onco- genic “driver,” and cancers with this translocation are highly sensitive to ALK kinase inhibition (5, 6). Recently, a tyrosine kinase inhibitor (TKI) targeting ALK, crizotinib (PF-02341066), was examined in a phase 1 trial (7). Among 105 patients with EML4-ALK–positive NSCLC, crizotinib showed remarkable ac- tivity, with an objective response rate of 56% and a median pro- gression-free survival of 9.2 mo (7, 8). These results support the notion that lung cancers harboring EML4-ALK are highly sus- ceptible to ALK-targeted therapies and demonstrate the prop- erties of “oncogene addiction” to ALK. Although many patients derive substantial clinical benefit, the development of drug resistance has curbed the impact of crizo- tinib in this disease. The paradigm of acquired TKI resistance has been seen with other targeted therapy successes, including epi- dermal growth factor receptor (EGFR) mutant lung cancers and v-raf murine sarcoma viral oncogene homolog B1 (BRAF) mutant melanomas (9–16). Similar to the experience with crizotinib, sensitive cancers ultimately develop resistance, usually within 1 y. For example, most patients with EGFR-mutant NSCLC will have disease progression after 9–12 mo of EGFR TKI monotherapy. In about one-half of cases, resistance arises due to the acquisition of a secondary gatekeeper mutation (T790M) within the EGFR (13, 15, 16). This mutation leads to substitution of a threonine in the ATP-binding pocket with a bulky methionine residue, which hinders drug binding. In about 10–20% of cases, resistance arises as a result of focal amplification of the MET proto-oncogene (9, 16, 17). Importantly, preclinical modeling of acquired resistance to EGFR TKIs has proven invaluable, not only for accurately pre- dicting the resistance mechanisms that emerge in the clinic, but also for assessing new therapeutic strategies to overcome re- sistance (12, 16–22). Recently, one NSCLC patient with acquired resistance to cri- zotinib was described (23). In this patient who relapsed after 5 mo of treatment, molecular analyses revealed that the resistant tumor cells harbored two secondary mutations within the kinase domain of EML4-ALK, C1156Y, and the gatekeeper mutation L1196M. These mutations occurred independently in distinct subclones of the resistant tumor. Studies of Ba/F3 cells engineered to express EML4-ALK harboring either mutation suggested that these mutants were resistant to crizotinib as well as resistant to a more potent ALK TKI, termed 2,4-pyrimidinediamine derivative (PDD). Thus, strategies to overcome this type of resistance have not yet been established. In addition, because there are no lab- oratory models of acquired resistance via this mechanism, it remains unknown if cancers that develop these resistance muta- tions remain addicted to ALK kinase activity and will be highly sensitive to other therapeutics targeting ALK. In this study, we have explored resistance to crizotinib by gen- erating and characterizing a unique cell line model of acquired resistance. In this model of acquired resistance, EML4-ALK is amplified and harbors the L1196M gatekeeper mutation. We show that cells expressing the L1196M mutant form of EML4- ALK are resistant to crizotinib, remain addicted to ALK signaling, Author contributions: R.K., J.A.E., and A.T.S. designed research; R.K., T.M.K., E.L., H.E., V.M.R., W.C.S., and A.J.I. performed research; R.K., C.B., V.M.R., W.C.S., and A.J.I. contrib- uted new reagents/analytic tools; R.K., T.M.K., C.B., A.J.I., J.A.E., and A.T.S. analyzed data; and R.K., J.A.E., and A.T.S. wrote the paper. The authors declare no conflict of interest. This article is a PNAS Direct Submission. 1 To whom correspondence may be addressed. E-mail: [email protected] or [email protected]. This article contains supporting information online at www.pnas.org/lookup/suppl/doi:10. 1073/pnas.1019559108/-/DCSupplemental. www.pnas.org/cgi/doi/10.1073/pnas.1019559108 PNAS | May 3, 2011 | vol. 108 | no. 18 | 7535–7540 MEDICAL SCIENCES Downloaded by guest on July 12, 2020
Transcript of Therapeutic strategies to overcome crizotinib resistance ... · Therapeutic strategies to overcome...

Therapeutic strategies to overcome crizotinibresistance in non-small cell lung cancers harboringthe fusion oncogene EML4-ALKRyohei Katayamaa,b, Tahsin M. Khana,c, Cyril Benesa,b, Eugene Lifshitsa, Hiromichi Ebia,b, Victor M. Riverad,William C. Shakespeared, A. John Iafrateb,e, Jeffrey A. Engelmana,b,1, and Alice T. Shawa,b,c,1
aMassachusetts General Hospital Cancer Center, Boston, MA 02129; bDepartment of Medicine, Harvard Medical School, Boston, MA 02115; cKoch Institute forIntegrative Cancer Research, Massachusetts Institute of Technology, Cambridge, MA 02139; dARIAD Pharmaceuticals, Cambridge, MA 02139; andeDepartment of Pathology, Massachusetts General Hospital, Boston, MA 02114
Edited by Peter K. Vogt, The Scripps Research Institute, La Jolla, CA, and approved March 23, 2011 (received for review December 27, 2010)
The echinoderm microtubule-associated protein-like 4 (EML4)-anaplastic lymphoma kinase (ALK) fusion oncogene representsa molecular target in a small subset of non-small cell lung cancers(NSCLCs). This fusion leads to constitutive ALK activation withpotent transforming activity. In a pivotal phase 1 clinical trial, theALK tyrosine kinase inhibitor (TKI) crizotinib (PF-02341066) demon-strated impressive antitumor activity in the majority of patientswithNSCLC harboringALK fusions. However, despite these remark-able initial responses, cancers eventually develop resistance to cri-zotinib, usually within 1 y, thereby limiting the potential clinicalbenefit. To determine how cancers acquire resistance to ALK inhib-itors, we established amodel of acquired resistance to crizotinib byexposing a highly sensitive EML4-ALK–positive NSCLC cell line toincreasing doses of crizotinib until resistance emerged. We foundthat cells resistant to intermediate doses of crizotinib developedamplification of the EML4-ALK gene. Cells resistant to higher doses(1 μM) also developed a gatekeeper mutation, L1196M, within thekinase domain, rendering EML4-ALK insensitive to crizotinib. Thisgatekeeper mutation was readily detected using a unique andhighly sensitive allele-specific PCR assay. Although crizotinib wasineffectual against EML4-ALK harboring the gatekeeper mutation,we observed that two structurally different ALK inhibitors, NVP-TAE684 and AP26113, were highly active against the resistant can-cer cells in vitro and in vivo. Furthermore, these resistant cellsremained highly sensitive to the Hsp90 inhibitor 17-AAG. Thus,we have developed amodel of acquired resistance to ALK inhibitorsand have shown that second-generation ALK TKIs or Hsp90 inhib-itors are effective in treating crizotinib-resistant tumors harboringsecondary gatekeeper mutations.
First described in 2007, the oncogenic fusion kinase echinodermmicrotubule-associated protein-like 4-anaplastic lymphoma
kinase (EML4-ALK) is present in∼4% of patients with non-smallcell lung cancer (NSCLC) (1). Chromosomal translocations in-volving ALK also occur in other cancers, including anaplasticlarge cell lymphomas and inflammatory myofibroblastic tumors.In all cases, the fusion partner (e.g., EML4) is believed to mediateligand-independent oligomerization of ALK, resulting in consti-tutive ALK kinase activation (2–4). In cell line and geneticallyengineered mouse models, EML4-ALK serves as a potent onco-genic “driver,” and cancers with this translocation are highlysensitive to ALK kinase inhibition (5, 6). Recently, a tyrosinekinase inhibitor (TKI) targeting ALK, crizotinib (PF-02341066),was examined in a phase 1 trial (7). Among 105 patients withEML4-ALK–positive NSCLC, crizotinib showed remarkable ac-tivity, with an objective response rate of 56% and a median pro-gression-free survival of 9.2 mo (7, 8). These results support thenotion that lung cancers harboring EML4-ALK are highly sus-ceptible to ALK-targeted therapies and demonstrate the prop-erties of “oncogene addiction” to ALK.Although many patients derive substantial clinical benefit, the
development of drug resistance has curbed the impact of crizo-
tinib in this disease. The paradigm of acquired TKI resistance hasbeen seen with other targeted therapy successes, including epi-dermal growth factor receptor (EGFR) mutant lung cancers andv-raf murine sarcoma viral oncogene homolog B1 (BRAF) mutantmelanomas (9–16). Similar to the experience with crizotinib,sensitive cancers ultimately develop resistance, usually within 1 y.For example, most patients with EGFR-mutant NSCLC will havedisease progression after 9–12 mo of EGFR TKI monotherapy.In about one-half of cases, resistance arises due to the acquisitionof a secondary gatekeeper mutation (T790M) within the EGFR(13, 15, 16). This mutation leads to substitution of a threonine inthe ATP-binding pocket with a bulky methionine residue, whichhinders drug binding. In about 10–20% of cases, resistance arisesas a result of focal amplification of the MET proto-oncogene (9,16, 17). Importantly, preclinical modeling of acquired resistance toEGFR TKIs has proven invaluable, not only for accurately pre-dicting the resistance mechanisms that emerge in the clinic, butalso for assessing new therapeutic strategies to overcome re-sistance (12, 16–22).Recently, one NSCLC patient with acquired resistance to cri-
zotinib was described (23). In this patient who relapsed after 5 moof treatment, molecular analyses revealed that the resistant tumorcells harbored two secondary mutations within the kinase domainof EML4-ALK, C1156Y, and the gatekeeper mutation L1196M.These mutations occurred independently in distinct subclonesof the resistant tumor. Studies of Ba/F3 cells engineered toexpress EML4-ALK harboring either mutation suggested thatthese mutants were resistant to crizotinib as well as resistant to amore potent ALK TKI, termed 2,4-pyrimidinediamine derivative(PDD). Thus, strategies to overcome this type of resistance havenot yet been established. In addition, because there are no lab-oratory models of acquired resistance via this mechanism, itremains unknown if cancers that develop these resistance muta-tions remain addicted to ALK kinase activity and will be highlysensitive to other therapeutics targeting ALK.In this study, we have explored resistance to crizotinib by gen-
erating and characterizing a unique cell line model of acquiredresistance. In this model of acquired resistance, EML4-ALK isamplified and harbors the L1196M gatekeeper mutation. Weshow that cells expressing the L1196M mutant form of EML4-ALK are resistant to crizotinib, remain addicted to ALK signaling,
Author contributions: R.K., J.A.E., and A.T.S. designed research; R.K., T.M.K., E.L., H.E.,V.M.R., W.C.S., and A.J.I. performed research; R.K., C.B., V.M.R., W.C.S., and A.J.I. contrib-uted new reagents/analytic tools; R.K., T.M.K., C.B., A.J.I., J.A.E., and A.T.S. analyzed data;and R.K., J.A.E., and A.T.S. wrote the paper.
The authors declare no conflict of interest.
This article is a PNAS Direct Submission.1To whom correspondence may be addressed. E-mail: [email protected] [email protected].
This article contains supporting information online at www.pnas.org/lookup/suppl/doi:10.1073/pnas.1019559108/-/DCSupplemental.
www.pnas.org/cgi/doi/10.1073/pnas.1019559108 PNAS | May 3, 2011 | vol. 108 | no. 18 | 7535–7540
MED
ICALSC
IENCE
S
Dow
nloa
ded
by g
uest
on
July
12,
202
0

and are highly sensitive to other structurally distinct ALK TKIsas well as to Hsp90 inhibition. On the basis of these results, wepropose two therapeutic strategies for overcoming acquired re-sistance to crizotinib, particularly when mediated by secondarymutations within the ALK TK domain.
ResultsGeneration and Biochemical Characterization of Crizotinib-ResistantCells. The NSCLC cell line H3122 expresses EML4-ALK variant 1and is highly sensitive to treatment with crizotinib. To exploremechanisms of crizotinib resistance, we generated resistantH3122 clones by exposing the sensitive parental cells to increasingconcentrations of crizotinib for 4 mo. We maintained cells withintermediate crizotinib resistance, referred to as H3122 CR0.6, in600 nM of crizotinib. The fully resultant cells, H3122 crizotinib-resistant (H3122 CR) cells, were maintained in 1 μMof crizotinib.H3122 CR cells were as resistant to crizotinib as other cancer
cell lines that did not harbor ALK gene rearrangements (IC50 > 1μM; Fig. 1A and SI Appendix, Fig. S1A). In addition, we assessed704 established cancer cell lines derived from a wide variety oftumor types for sensitivity to crizotinib as part of our automatedplatform to examine drug sensitivity across multiple cell lines(24). Whereas H3122 parental cells segregated with the mostsensitive cell lines, the H3122 CR cells segregated with the highlyresistant cell lines (Fig. 1B). Unlike the parental H3122 cells, theH3122 CR cells maintained ALK phosphorylation in the presenceof crizotinib (Fig. 1C). Accordingly, AKT and ERK phosphory-lation were not suppressed by crizotinib in the resistant cells.Notably, H3122 CR cells also contained higher total proteinlevels of EML4-ALK compared with the parental line (Fig. 1C).
EML4-ALK Gene Is Amplified and Mutated in H3122 CR Cells. To de-terminewhether gene amplification underlies the elevated proteinlevel of EML4-ALK in H3122 CR cells, we performed fluores-cence in situ hybridization (FISH) analysis. Relative to parentalH3122 cells, H3122 CR cells showed an increase in the number ofrearranged EML4-ALK genes per cell (Fig. 2A).Because the phosphorylation of EML4-ALK in H3122 CR cells
is not impacted by 1 μM crizotinib (Fig. 1C), we hypothesizedthat resistant cells might also harbor a mutation within ALK. Weprepared cDNA and examined the entire coding sequence ofEML4-ALK in H3122 parental and resistant cells. In the resistant
cells, we detected a C → A substitution at nucleotide 3586 ofEML4-ALK variant 1 (Fig. 2B) that was not detected in the pa-rental cells. This 3586C → A substitution results in a leucine →methionine change within the ALK TK domain, corresponding tothe L1196M gatekeeper mutation previously reported in a patientwith acquired resistance to crizotinib (23). We did not detect anyother TKmutations including the C1156Y substitution, which wasalso reported in the same patient (23). Consistent with the notionthat this L1196Mmutation confers resistance to crizotinib, Ba/F3cells engineered to express this mutant were also resistant tocrizotinib, whereas cells expressing wild-type EML4-ALK weresensitive (SI Appendix, Fig. S2). Notably, in the DNA sequencetracings, the peak corresponding to the mutation is approximatelyone-half to one-third as high as the wild-type peak (Fig. 2B). Thissuggests that only a fraction of the amplified EML4-ALK fusiongenes acquire the secondary resistance mutation.These resistant models were developed by stepwise increases
in drug concentration until fully resistant cells emerged. Becauseboth amplification andmutation were identified inH3122CR cells,we sought to investigate the temporal relationship between geneamplification and secondary mutation in acquired crizotinib re-sistance. Thus, we analyzed H3122 CR0.6 cells, the intermediate,partially resistant predecessors of H3122 CR cells that were re-sistant to 600 nM crizotinib. By Western blotting analysis, ALKprotein level and p-ALK were up-regulated in H3122 CR0.6 cells(SI Appendix, Fig. S3). FISH analysis demonstrated amplificationof the EML4-ALK fusion gene in the H3122 CR0.6 cells (Fig. 2A).However, they did not harbor a secondary ALK resistance muta-tion (Fig. 2B). To determine whether L1196M is present at a lowlevel in a subpopulation of H3122 CR0.6 cells, we developed ahighly sensitive gatekeeper mutation-specific PCR assay that candetect the L1196M mutation when it represents at least 1% of themutated ALK alleles (SI Appendix, Fig. S4). Using this assay, wedetected L1196M in H3122 CR cells and in all 11 clones derivedfrom single H3122 CR cells (SI Appendix, Fig. S5), but not in theH3122 CR0.6 cells, the parental H3122 cells, or the other NSCLCcell lines harboringEML4-ALK (Fig. 2C and SIAppendix, Fig. S5).These results suggest that the L1196Mmutation is present in eachcell of the resistant H3122 CR cells and that there is a stepwisemodel of acquired resistance involving amplification of the target,which confers resistance to 600 nM crizotinib, followed by sec-
A
of c
ontr
ol) 100 crizotinib (200nM), n=704
cell
num
ber (
%
501%
< 0 20
H31
22
A54
9
H12
99
SKB
R3
H31
22 C
R
BT4
74
< 0.20.2 - 0.50.5 - 0.75> 0.75
H52
2
H46
0
M
crizotinib (6hr) crizotinib(6hr)H3122 H3122 CR
MC
pALK(pY1604)
ALK
non
30 n
M10
0 nM
300
nM10
00 n
Mno
n30
nM
100
nM30
0 nM
1000
nM
pAKT(pS473)
pERK
panAKT
ERKERK
Actin
B
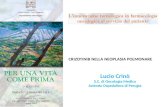
Fig. 1. H3122 CR cells are resistant to crizotinib. (A) Cell lines were seeded in 96-well plates and treated with 1 μM of crizotinib for 72 h. Cell survival wasanalyzed using the CellTiter-Glo viability assay. In contrast to the parental H3122 cells, which are highly sensitive to crizotinib (red bar), H3122 CR cells (bluebar) are as insensitive to crizotinib as non-ALK rearranged cell lines. (B) Pie chart representation of the sensitivity of H3122 and H3122 CR cells compared with704 other human cancer cell lines assessed by an automated cell viability assay to 200 nM crizotinib. Viability at 72 h was calculated as a ratio of viablecrizotinib-exposed cells to viable DMSO-treated cells. The color scheme corresponds to the relative inhibitory effect of treatment. The chart depicts the mostsensitive cell lines in order of decreasing sensitivity (from top to bottom). (C) H3122 parental and H3122 CR cells were treated with crizotinib at the indicatedconcentration for 6 h. Cell extracts were immunoblotted to detect the indicated proteins.
7536 | www.pnas.org/cgi/doi/10.1073/pnas.1019559108 Katayama et al.
Dow
nloa
ded
by g
uest
on
July
12,
202
0

ondary gatekeeper mutation that renders cells resistant to 1 μMcrizotinib.
H3122 CR Cells Are Addicted to ALK. To determine if H3122 CR cellscontinue to require EML4-ALK for their viability, we used siRNAstargeting ALK to knock down EML4-ALK. In both H3122 pa-rental and H3122 CR cell lines,ALK-specific siRNA decreased ex-pression of EML4-ALK and potently suppressed cell growth (Fig.3 A and B). As expected, the ALK siRNA had no effect on thegrowth of KRASmutant A549 cells (Fig. 3 A and B). These resultsdemonstrate that resistant H3122 CR cells expressing EML4-ALKL1196M remain addicted to ALK signaling.
NVP-TAE684 and AP26113 Overcome Crizotinib Resistance in H3122 CRCells. Based on the crystal structure of the kinase domain of ALK,the gatekeeper L1196M mutation causes resistance by steric in-terference with crizotinib binding (23). Thus, although resistant tocrizotinib, this mutant ALK may be sensitive to structurally dis-tinct ALK kinase inhibitors. To address this hypothesis, we testedthe activity of the ALK inhibitor NVP-TAE684, a 5-chloro-2,4-diaminophenylpyrimidine, in parental and resistant H3122 cells.As shown in Fig. 4, NVP-TAE684 markedly reduced cell survivalin both sensitive H3122 and H3122 CR cells, but had little to noeffect on the viability of other, non-ALK–dependent cancer celllines (Fig.4A and SI Appendixx, Fig. S1B). Within the panel of 704established cancer cell lines assessed in the automated platform(24), the vast majority were largely insensitive to 200 nM NVP-TAE684; however, 1% of lines displayed marked sensitivity toNVP-TAE684. Both the H3122 and the H3122 CR cell linessegregate with the highly sensitive cell lines (Fig. 4B). This is insharp contrast to the resistance of H3122 CR cells to crizotinib
(Fig. 1B). In contrast to crizotinib, NVP-TAE684 treatment ofH3122 CR cells suppressed phosphorylation of ALK, AKT, andERK and induced marked apoptosis (Fig. 4C and SI Appendix,Fig. S6). Similarly, NVP-TAE684 potently suppressed the survivalof Ba/F3 cells expressing the EML4-ALK L1196M mutant (SIAppendix, Fig. S7A). However, in this system, the potency ofNVP-TAE684 against mutant EML4-ALK was slightly reducedrelative to native EML4-ALK, with IC50 values of 2.7 versus 1.2nM, respectively.
A
H3122 H3122 CR0.6 H3122 CR
B Forward Reverse C
H3122
H3122 CR0.6 H31
22
22 C
R0.
6
3122
CR
H22
28
MG
H00
6
wat
er
H3122 CR
H31
2 H3 M
Leu (CTG) Met (ATG)
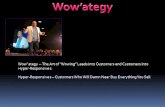
Fig. 2. EML4-ALK is both amplified and mutated in resistant H3122 CR cells. (A) Dual-color FISH [ALK-N-terminal (green)/ALK-C-terminal (red)] analysis wasperformed on H3122 parental, H3122 CR0.6, and H3122 CR cells. Arrows indicate the split ALK C-terminal region (EML4-ALK). Both H3122 CR0.6 and H3122 CRcells demonstrate amplification of EML4-ALK. (B) Secondary L1196M (gatekeeper) mutation in resistant H3122 CR cells. Shown are electrophoretograms ofEML4-ALK cDNA from H3122 parental, H3122 CR0.6, and H3122 CR cells. The 1903C → A mutation within exon 23 results in a L635M substitution thatcorresponds to the L1196M gatekeeper mutation of ALK. (C) Detection of the gatekeeper mutation using an L1196M mutation-specific PCR assay. Shown isthe amplified 160-bp product in H3122 CR cells after 35 PCR cycles. This product is not detected in parental H3122 or H3122 CR0.6 cells or in other EML4-ALK–positive cell lines (H2228, MGH006).
A B
100 ol
H3122
ol ol
H3122CR A549
50pALK
(pY1604)
si-c
ontr
o
si-A
LK
si-c
ontr
o
si-A
LK
si-c
ontr
si-A
LK
cntl
cntl
ALK
ALK cn
tl
ALK
cell
num
ber (
% o
f con
trol
)
0
ALK
Actin
H3122 H3122 CR
si-c
si-c
si-A
si-A
A549
si-c
si-A
Fig. 3. Resistant H3122 CR cells are oncogene-addicted. (A) The indicatedcell lines were transfected with small interfering RNA (siRNA) against ALK(siALK) or control siRNA, and cell viability was measured after 72 h. (B) Im-munoblotting of protein lysates 72 h after knockdown showing reducedlevels of phosphorylated ALK and total ALK in siALK-transfected cells.
Katayama et al. PNAS | May 3, 2011 | vol. 108 | no. 18 | 7537
MED
ICALSC
IENCE
S
Dow
nloa
ded
by g
uest
on
July
12,
202
0

We also tested a second, structurally distinct ALK kinase in-hibitor AP26113. A new highly selective small molecule inhibitorof ALK, AP26113 exhibits about fivefold greater potency in vitrocompared with crizotinib (SI Appendix, Table S1A). Like NVP-TAE684, AP26113 was highly active against both sensitive andresistant H3122 cells, decreasing cell growth (Fig. 4D and SI Ap-pendix, Fig. S1C), suppressing ALK phosphorylation (Fig. 4E), andinducing apoptosis (SIAppendix, Fig. S6).Higher doses ofAP26113were required to completely suppress ALK in the resistant cellsbecause there were greater levels ofALK/p-ALKas a result of geneamplification. AP26113 was also active in Ba/F3 cells expressingeither native or mutant EML4-ALK (IC50’s were 10 and 24 nM,respectively) (SI Appendix, Fig. S7B). Consistent with the Ba/F3data, the potency of AP26113 against mutant EML4-ALK wasslightly reduced relative to native EML4-ALK as determined by itscapacity to decrease p-ALK in theH3122 andH3122CR cells, withIC50 values of 7.4 versus 16.8 nM, respectively (SI Appendix, Fig.S8). These results suggest that AP26113 can overcome crizotinibresistance mediated by the gatekeeper L1196M mutation. Indeed,
we observed impressive in vivo activity of both NVP-TAE684 andAP26113, but not of crizotinib, against theH3122CRcells grown asxenograft tumors in vivo (SI Appendix, Fig. S9).
Hsp90 Inhibitor 17-AAG Overcomes Crizotinib Resistance in H3122 CRCells. In a recent phase 2 study, the Hsp90 inhibitor IPI-504demonstrated clinical activity in three of three patients with ALK-positive NSCLC and induced rapid degradation of EML4-ALK invitro (25). Hsp90 inhibitors also induced tumor regression in agenetically engineered mouse model of lung cancer driven byEML4-ALK (5). Therefore,we evaluated the efficacy of the Hsp90inhibitor 17-AAG in EML4-ALK L1196M-expressing cells. Asshown in Fig. 5A, 17-AAG potently suppressed cell growth in bothparental H3122 and H3122 CR cells, but not in other non-ALK–dependent lung cancer lines (SI Appendix, Fig. S1D). However, incontrast to NVP-TAE684 and AP26113, 17-AAG also inhibitedthe viability of SKBR3 and BT474 cell lines, both of which harborHER2 amplification and are known to be sensitive to Hsp90 in-hibition (26, 27). In Ba/F3 cells, 17-AAG was active against both
A Bon
trol
)
100TAE684 (200nM), n=704
ell n
umbe
r (%
of c
o
50
Cce 0
H3122 H3122 CR
H31
22
A54
9
H12
99
H31
22 C
R
SKB
R3
BT4
74
H52
2
H46
0< 0.20.2 - 0.50.5 - 0.75> 0.75
pALK(pY1604)
ALK
non
10 n
M30
nM
100
nM30
0 nM
3 nM
TAE684 (6hr)
non
10 n
M30
nM
100
nM30
0 nM
3 nM
TAE684 (6hr)
0.75
pAKT(pS473)
pERK
ERK
panAKT
Actin
D
) 100
non
10 n
M30
nM
100
nM30
0 nM
3 nM
AP26113 (6hr)
H3122 CR
criz
otin
ib (1
uM)
non
10 n
M30
nM
100
nM30
0 nM
3 nM
AP26113 (6hr)
H3122
criz
otin
ib (1
uM)E
(% o
f con
trol
50
100
pAKT(pS473)
pALK(pY1604)
AKT
ALK
cell
0
H31
22
A54
9
H12
99
BT4
74
H31
22 C
R
SKB
R3
H52
2
H46
0 pERK
panAKT
ERK
Actin
num
ber
Fig. 4. Two different ALK kinase inhibitors, NVP-TAE684 and AP26113, overcome crizotinib resistance in H3122 CR cells. (A) Cell lines were seeded in 96-wellplates and treated with 100 nM of TAE684 for 72 h. Cell survival was analyzed using the CellTiter-Glo viability assay. Both parental H3122 cells (red bar) andH3122 CR cells (blue bar) show marked sensitivity to TAE684. Non-ALK rearranged cell lines (A549, H1299, SKBR3, H522, H460, and BT474 cells) show minimalgrowth inhibition with TAE684. (B) Pie chart representation of the sensitivity of H3122 and H3122 CR cells compared with 704 other human cancer cell linesassessed by an automated cell viability assay to 200 nM TAE684. Viability at 72 h was calculated as a ratio of viable crizotinib-exposed cells to viable DMSO-treated cells. The chart depicts the most sensitive cell lines in order of decreasing sensitivity (from top to bottom). Both parental H3122 and H3122 CR cells areamong the 1% of the most sensitive cell lines to TAE684. (C) Suppression of ALK signaling by TAE684 in resistant H3122 CR cells. H3122 parental and resistantcells were exposed to increasing concentrations of TAE684 for 6 h. Cell lysates were immunoblotted to detect the indicated proteins. (D) Sensitivity of H3122CR cells to AP26113. Cell lines were seeded in 96-well plates and treated with 300 nM of AP26113 for 72 h. Cell survival was analyzed using the CellTiter-Gloviability assay. Both parental H3122 cells (red bar) and H3122 CR cells (blue bar) show marked sensitivity to AP26113, compared with non-ALK rearranged celllines. (E) Suppression of ALK signaling by AP26113 in resistant H3122 CR cells. H3122 parental and resistant cells were exposed to increasing concentrations ofAP26113 for 6 h. Cell lysates were immunoblotted to detect the indicated proteins.
7538 | www.pnas.org/cgi/doi/10.1073/pnas.1019559108 Katayama et al.
Dow
nloa
ded
by g
uest
on
July
12,
202
0

native and mutant EML4-ALK to a similar extent, but showed noactivity in parental Ba/F3 cells (SI Appendix, Fig. S7C). 17-AAGtreatment decreased both p-ALK level and ALK protein expres-sion with similar potencies in the parental and resistant cells (Fig.5B). These results suggest that Hsp90 inhibition might representan alternative therapeutic strategy for overcoming acquired re-sistance to crizotinib due to acquisition of a resistance mutation.
DiscussionIn tumors dependent on a driver kinase such as BCR-ABL ormutant EGFR, secondary mutation within the kinase domain isa common mechanism of acquired drug resistance. The mostfrequent resistance mutation involves the gatekeeper residue.Amino acid substitutions at this position hinder drug binding andthereby confer high-level resistance to many tyrosine kinaseinhibitors. Other mechanisms of acquired drug resistance involvegene amplification of the kinase target or activation of alterna-tive signaling pathways to bypass the need for kinase activation(10, 28). Identification of the genetic alterations underlying ac-quired drug resistance has fostered the development of targetedagents for patients with TKI resistance. For example, two second-generation TKIs—dasatinib and nilotinib—have efficacy againstmost of the known imatinib-resistant mutations and are approvedfor patients with imatinib-resistant chronic myeloid leukemia(CML) (29, 30). However, these drugs are not active against thegatekeeper T315I mutation within ABL (31). Similarly in EGFR-mutant lung cancer, second-generation, irreversible EGFRinhibitors are being explored to treat cancers that develop re-sistance via the gatekeeper T790M mutation (22, 32).EML4-ALK–positive NSCLC represents another tyrosine kinase-
driven cancer that is highly responsive to TKI therapy. Recently,two studies have reported the identification of secondary re-sistance mutations within the ALK TK domain in patients whorelapsed on crizotinib (23, 33). One of the mutations identifiedwas the gatekeeper L1196M substitution, analogous to T315I inABL and T790M in EGFR (23). In this study, we generated a cellline model of acquired crizotinib resistance by exposing sensitive,EML4-ALK–positive H3122 cells to increasing concentrationsof crizotinib. The resistant cells harbor both amplification ofEML4-ALK and the same L1196M gatekeeper mutation that wasidentified in a patient with acquired resistance. Notably, we didnot identify any other ALK mutations in this cell line, includingC1156Y. Because we did not use more sensitive technologies suchas deep sequencing, we cannot exclude the possibility that a smallfraction of resistant cells harbor distinct secondary mutations such
as C1156Y.However, this seems unlikely because we observed theL1196M mutation and not the C1156Y mutation in all of theclones derived from single cells from the H3122 CR cell line.Although amplification of ALK is a known oncogenic event
in pediatric neuroblastoma (34), amplification of ALK fusiononcogenes has not been reported. Analysis of partially resistantH3122 cells (H3122 CR0.6) that harborEML4-ALK amplification(but no gatekeeper mutation) suggests a step-wise evolution ofacquired resistance involving gene amplification followed by pointmutation. This model is also supported by the observation thatonly a fraction of the amplifiedALK fusion genes (per cell) harborL1196M (Fig. 2C). In other TKI-resistant cancers, target ampli-fication preceding acquisition of secondary mutations has notbeen reported in vitro or in vivo. It remains unknown if this two-step mechanism is unique to EML4-ALK–positive NSCLC or ifit is a product of the methodology used to develop resistance inthe laboratory.The detection of gatekeeper and other acquired mutations in
resistant tumor samples is clinically important, but can be tech-nically challenging. The EGFR T790M resistance mutation, forexample, is often difficult to detect on standard sequence trac-ings and may require more sensitive techniques such as deepsequencing for detection (19, 35, 36). This problem may be dueto contamination of the tumor specimen with noncancerous cells(e.g., stromal or inflammatory cells). Alternatively, for sometumors, only a small percentage of the EGFR alleles per cell mayharbor the T790M mutation (termed “allelic dilution”), or onlya small percentage of resistant cells in the tumor specimen mighthave T790M-mediated resistance. Notably, the finding of bothEML4-ALK amplification and L1196M mutation in the CR cellssuggests that allelic dilution also could ultimately contribute todifficulty in detecting resistance mutations in cancers with ac-quired resistance to crizotinib. In this study, we developed anL1196M-mutation specific PCR assay to detect potentially lowlevels of the gatekeeper L1196M mutation in partially resistantH3122 CR0.6 cells. This assay is highly sensitive with a detectionlimit of 1% or less (SI Appendix, Fig. S4) and requires only 30 nggenomic DNA. Thus, this assay might serve as the basis fora clinical diagnostic test for L1196M in biopsy samples fromcrizotinib-resistant patients.In both CML and EGFR-mutant lung cancer, resistant tumors
with gatekeeper mutations have proven refractory to second-generation, more potent TKIs. One recent report suggests thatthe gatekeeper mutation in ALK might behave similarly; com-pared with control Ba/F3 cells expressing native EML4-ALK, cellsexpressing mutant EML4-ALK L1196M were markedly less sen-sitive to a potent PDD (23). In contrast, we have found that cri-zotinib resistance mediated by the gatekeeper L1196M mutationcan be effectively overcome by two different ALK TKIs. Impor-tantly, one of these—AP26113—is under clinical developmentand is scheduled to begin clinical testing within the year. In H3122CR cells, the improved cellular activity of AP26113 comparedwith crizotinib is likely based on both its enhanced potency againstALK and its increased activity against L1196M-mutated ALK.In vitro kinase assays revealed that wild-type and L1196M-mutated ALK showed similar Km values for ATP binding (30.7and 27.2 μM, respectively). However, crizotinib was about 10-foldless potent against L1196M ALK compared with wild-type ALK(Ki of 8.2 and 0.7 nM, respectively), consistent with its diminishedefficacy against the L1196MALK in cell lines (SI Appendix, TableS1B). In contrast, AP26113 was ∼10-fold more potent againstALK than crizotinib in vitro, and unlike crizotinib, it was similarlypotent against the L1196M mutant (Ki of 0.09 and 0.08 nM,respectively).In addition to studying ALK TKIs, we have shown that EML4-
ALK harboring the gatekeeper mutation is an Hsp90 clientprotein similar to wild-type EML4-ALK and sensitive to Hsp90inhibition. Notably, cell lines expressing either native EML4-
A B H3122 CRH3122
100
pALK(pY1604)
non
10 n
M30
nM
100
nM30
0 nM
3 nM
17AAG (24hr)H3122 CR
non
10 n
M30
nM
100
nM30
0 nM
3 nM
17AAG (24hr)H3122
ell n
umbe
r (%
of c
ontr
ol)
50pAKT
(pS473)
panAkt
ALK
ce 0 pERK
ERK
ActinH31
22
BT4
74
SKB
R3
A54
9
H12
99
H31
22 C
R
H52
2
H46
0
Fig. 5. The Hsp90 inhibitor 17-AAG can overcome crizotinib resistance inH3122 CR cells. (A) Cell lines were seeded in 96-well plates and treated with10 nM of 17-AAG for 72 h. Cell survival was analyzed using CellTiter-Glo.Both parental H3122 cells (red bar) and H3122 CR cells (blue bar) showsensitivity to 17-AAG. (B) Suppression of ALK signaling by 17-AAG in re-sistant H3122 CR cells. H3122 parental and resistant cells were exposed toincreasing concentrations of 17-AAG for 6 h. Cell lysates were immuno-blotted to detect the indicated proteins.
Katayama et al. PNAS | May 3, 2011 | vol. 108 | no. 18 | 7539
MED
ICALSC
IENCE
S
Dow
nloa
ded
by g
uest
on
July
12,
202
0

ALK or EML4-ALK L1196M were even more sensitive to 17-AAG than two Hsp90-dependent, HER2-amplified breast cancerlines (Fig. 5A). Therefore, patients with crizotinib resistance dueto an acquired L1196M mutation may derive benefit from twodifferent ALK-targeted strategies: more potent ALK TKIs suchas AP26113 or any of a number of Hsp90 inhibitors already inclinical trials. Notably, although gatekeeper mutations are par-ticularly common in EGFR-mutant lung cancer, the frequency ofL1196M in EML4-ALK–positive NSCLC has yet to be estab-lished. Because secondary mutations such as the gatekeepermutation may not represent the predominant mechanism of ac-quired crizotinib resistance, additional studies are needed toelucidate other mechanisms of resistance. The results of thesestudies will be critical to selecting the best therapeutic strategiesfor targeting TKI resistance in the clinic.
Materials and MethodsSee SI Appendix for the description of the cell culture conditions, generationof H3122 CR cells, survival assays, fluorescence in situ hybridization, immu-noblotting, apoptosis assay retroviral infection, quantitative RT-PCR (qPCR),siRNA transfection, xenograft study, and statistical analyses.
Reagents. Crizotinib and NVP-TAE684 were purchased from ChemieTek and17-AAG was purchased from Selleck. AP26113 was provided by ARIADPharmaceuticals that makes AP26113 available to qualified academic labo-ratories free of charge for verification and reproduction of the resultsreported in this paper. Each compound was dissolved in DMSO for cell cultureexperiments. Control or ALK siRNA was from Invitrogen, and HiPerfect re-agent was from Qiagen.
Isolation of Genomic DNA Preparation and L1196M Mutation-Specific PCR.Genomic DNA was isolated from cell pellets with a DNeasy kit (QIAGEN)according to the manufacturer’s protocol. Exon 23 of ALK was PCR-amplifiedfrom genomic DNA using Pfu Ultra II (Agilent Technologies) and sequencedbidirectionally by Sanger dideoxynucleotide sequencing with the primersdescribed in SI Appendix. ALK-Exon23 or L1196M mutation-specific qPCRwas performed by a LightCycler 480 (Roche Diagnostics) with CYBR GreenMaster Mix (Roche). Primer sequences are provided in SI Appendix.
ACKNOWLEDGMENTS. This study was supported in part by a V Foundationfor Cancer Research Translational Grant (to J.A.E. and A.T.S.), by the CharlesW. and Jennifer C. Johnson Koch Institute Clinical Investigator Award (toA.T.S.), by National Institutes of Health K08 Grant CA120060-01 (to J.A.E.), bythe Sig Adler Lung Cancer Research Fund, by the Massachusetts GeneralHospital Thoracic Oncology Fund, and by a Japan Society for the Promotionof Science Postdoctoral Fellowship for Research Abroad from the Ministry ofEducation, Culture, Sports, Science, and Technology of Japan (to R.K.).
1. Soda M, et al. (2007) Identification of the transforming EML4-ALK fusion gene in non-small-cell lung cancer. Nature 448:561–566.
2. Mano H (2008) Non-solid oncogenes in solid tumors: EML4-ALK fusion genes in lungcancer. Cancer Sci 99:2349–2355.
3. Shinmura K, et al. (2008) EML4-ALK fusion transcripts, but no NPM-, TPM3-, CLTC-,ATIC-, or TFG-ALK fusion transcripts, in non-small cell lung carcinomas. Lung Cancer61:163–169.
4. Takeuchi K, et al. (2009) KIF5B-ALK, a novel fusion oncokinase identified by animmunohistochemistry-based diagnostic system for ALK-positive lung cancer. ClinCancer Res 15:3143–3149.
5. Chen Z, et al. (2010) Inhibition of ALK, PI3K/MEK, and HSP90 in murine lungadenocarcinoma induced by EML4-ALK fusion oncogene. Cancer Res 70:9827–9836.
6. Soda M, et al. (2008) A mouse model for EML4-ALK-positive lung cancer. Proc NatlAcad Sci USA 105:19893–19897.
7. Kwak EL, et al. (2010) Anaplastic lymphoma kinase inhibition in non-small-cell lungcancer. N Engl J Med 363:1693–1703.
8. Camidge DR, et al. (2010) Clinical activity of crizotinib (PF-02341066), in ALK-positivepatients with advanced non-small cell lung cancer. Ann Oncol 21(Suppl 8):viii123,mdq518.
9. Bean J, et al. (2007) MET amplification occurs with or without T790M mutations inEGFR mutant lung tumors with acquired resistance to gefitinib or erlotinib. Proc NatlAcad Sci USA 104:20932–20937.
10. Engelman JA, Jänne PA (2008) Mechanisms of acquired resistance to epidermalgrowth factor receptor tyrosine kinase inhibitors in non-small cell lung cancer. ClinCancer Res 14:2895–2899.
11. Flaherty KT, et al. (2010) Inhibition of mutated, activated BRAF in metastaticmelanoma. N Engl J Med 363:809–819.
12. Johannessen CM, et al. (2010) COT drives resistance to RAF inhibition through MAPkinase pathway reactivation. Nature 468:968–972.
13. Kobayashi S, et al. (2005) EGFR mutation and resistance of non-small-cell lung cancerto gefitinib. N Engl J Med 352:786–792.
14. Mok TS, et al. (2009) Gefitinib or carboplatin-paclitaxel in pulmonary adenocarcinoma.N Engl J Med 361:947–957.
15. Pao W, et al. (2005) Acquired resistance of lung adenocarcinomas to gefitinib orerlotinib is associated with a second mutation in the EGFR kinase domain. PLoS Med2:e73.
16. Turke AB, et al. (2010) Preexistence and clonal selection of MET amplification in EGFRmutant NSCLC. Cancer Cell 17:77–88.
17. Engelman JA, et al. (2007) MET amplification leads to gefitinib resistance in lungcancer by activating ERBB3 signaling. Science 316:1039–1043.
18. Corcoran RB, et al. (2010) BRAF gene amplification can promote acquired resistanceto MEK inhibitors in cancer cells harboring the BRAF V600E mutation. Sci Signal 3:ra84.
19. Engelman JA, et al. (2006) Allelic dilution obscures detection of a biologically
significant resistance mutation in EGFR-amplified lung cancer. J Clin Invest 116:
2695–2706.20. Faber AC, et al. (2009) Differential induction of apoptosis in HER2 and EGFR addicted
cancers following PI3K inhibition. Proc Natl Acad Sci USA 106:19503–19508.21. Guix M, et al. (2008) Acquired resistance to EGFR tyrosine kinase inhibitors in cancer
cells is mediated by loss of IGF-binding proteins. J Clin Invest 118:2609–2619.22. Zhou W, et al. (2009) Novel mutant-selective EGFR kinase inhibitors against EGFR
T790M. Nature 462:1070–1074.23. Choi YL, et al.; ALK Lung Cancer Study Group (2010) EML4-ALK mutations in lung
cancer that confer resistance to ALK inhibitors. N Engl J Med 363:1734–1739.24. McDermott U, et al. (2008) Genomic alterations of anaplastic lymphoma kinase may
sensitize tumors to anaplastic lymphoma kinase inhibitors. Cancer Res 68:3389–3395.25. Sequist LV, et al. (2010) Activity of IPI-504, a novel heat-shock protein 90 inhibitor, in
patients with molecularly defined non-small-cell lung cancer. J Clin Oncol 28:4953–4960.26. Chandarlapaty S, et al. (2010) Inhibitors of HSP90 block p95-HER2 signaling in
Trastuzumab-resistant tumors and suppress their growth. Oncogene 29:325–334.27. Zheng FF, et al. (2000) Identification of a geldanamycin dimer that induces the
selective degradation of HER-family tyrosine kinases. Cancer Res 60:2090–2094.28. Engelman JA, Settleman J (2008) Acquired resistance to tyrosine kinase inhibitors
during cancer therapy. Curr Opin Genet Dev 18:73–79.29. Kantarjian H, et al. (2010) Dasatinib versus imatinib in newly diagnosed chronic-phase
chronic myeloid leukemia. N Engl J Med 362:2260–2270.30. Saglio G, et al.; ENESTnd Investigators (2010) Nilotinib versus imatinib for newly
diagnosed chronic myeloid leukemia. N Engl J Med 362:2251–2259.31. O’Hare T, et al. (2005) In vitro activity of Bcr-Abl inhibitors AMN107 and BMS-354825
against clinically relevant imatinib-resistant Abl kinase domain mutants. Cancer Res
65:4500–4505.32. Yap TA, et al. (2010) Phase I trial of the irreversible EGFR and HER2 kinase inhibitor
BIBW 2992 in patients with advanced solid tumors. J Clin Oncol 28:3965–3972.33. Sasaki T, et al. (2010) The neuroblastoma associated F1174L ALK mutation causes
resistance to an ALK kinase inhibitor in ALK translocated cancers. Cancer Res 70:
10038–10043.34. Chiarle R, Voena C, Ambrogio C, Piva R, Inghirami G (2008) The anaplastic lymphoma
kinase in the pathogenesis of cancer. Nat Rev Cancer 8:11–23.35. Kosaka T, et al. (2006) Analysis of epidermal growth factor receptor gene mutation in
patients with non-small cell lung cancer and acquired resistance to gefitinib. Clin
Cancer Res 12:5764–5769.36. Kwak EL, et al. (2005) Irreversible inhibitors of the EGF receptor may circumvent
acquired resistance to gefitinib. Proc Natl Acad Sci USA 102:7665–7670.
7540 | www.pnas.org/cgi/doi/10.1073/pnas.1019559108 Katayama et al.
Dow
nloa
ded
by g
uest
on
July
12,
202
0