
Therapeutic potential and mechanism of kinetin as a ... · Therapeutic potential and mechanism of...
13
ORIGINAL ARTICLE Therapeutic potential and mechanism of kinetin as a treatment for the human splicing disease familial dysautonomia Matthew M. Hims & El Chérif Ibrahim & Maire Leyne & James Mull & Lijuan Liu & Conxi Lazaro & Ranjit S. Shetty & Sandra Gill & James F. Gusella & Robin Reed & Susan A. Slaugenhaupt Received: 18 September 2006 / Revised: 24 October 2006 / Accepted: 26 October 2006 / Published online: 6 January 2007 # Springer-Verlag 2007 Abstract Mutations that affect the splicing of pre-mRNA are a major cause of human disease. Familial dysautonomia (FD) is a recessive neurodegenerative disease caused by a T to C transition at base pair 6 of IKBKAP intron 20. This mutation results in variable tissue-specific skipping of exon 20. Previously, we reported that the plant cytokinin kinetin dramatically increases exon 20 inclusion in RNA isolated from cultured FD cells. The goal of the current study was to investigate the nature of the FD splicing defect and the mechanism by which kinetin improves exon inclusion, as such knowledge will facilitate the development of future therapeutics aimed at regulating mRNA splicing. In this study, we demonstrate that treatment of FD lymphoblast cell lines with kinetin increases IKBKAP mRNA and IKAP protein to normal levels. Using a series of minigene constructs, we show that deletion of a region at the end of IKBKAP exon 20 disrupts the ability of kinetin to improve exon inclusion, pinpointing a kinetin responsive sequence J Mol Med (2007) 85:149–161 DOI 10.1007/s00109-006-0137-2 M. M. Hims : M. Leyne : J. Mull : L. Liu : C. Lazaro : R. S. Shetty : S. Gill : J. F. Gusella : S. A. Slaugenhaupt Center for Human Genetic Research, Massachusetts General Hospital and Harvard Medical School, Boston, MA 02114, USA E. C. Ibrahim : R. Reed Department of Cell Biology, Harvard Medical School, Boston, MA 02115, USA C. Lazaro Translational Research Laboratory, Institut Català d’Oncologia, L ’Hospitalet de Llobregat, Barcelona, Spain Present address: E. C. Ibrahim NICN-UMR 6184 CNRS, Faculté de Médecine Nord-IFR Jean Roche, Marseilles, France S. A. Slaugenhaupt Center for Human Genetic Research, Massachusetts General Hospital, 185 Cambridge Street, CPZN-5254, Boston, MA 02114, USA e-mail: [email protected] (*) SUSAN A. SLAUGENHAUPT received her Ph.D. in Human Genetics from the University of Pittsburgh in Pittsburgh, PA, USA. She is presently an Associate Professor of Neurology in the Center for Human Genetic Research at Massachusetts General Hospital and Harvard Medical School. Her research interests include the discovery and characteriza- tion of human disease genes and the role of mRNA splicing in human disease. MATTHEW M. HIMS received his Ph.D. in human genetics from the University of Leeds, England. He is currently a postdoctoral research fellow in the Center for Human Genetic Research at Massachusetts General Hospital. His research interests include the role of RNA splicing in human disease and the development of accurate murine models of human splicing defects.
Transcript of Therapeutic potential and mechanism of kinetin as a ... · Therapeutic potential and mechanism of...

ORIGINAL ARTICLE
Therapeutic potential and mechanism of kinetinas a treatment for the human splicing diseasefamilial dysautonomia
Matthew M. Hims & El Chérif Ibrahim & Maire Leyne &
James Mull & Lijuan Liu & Conxi Lazaro &
Ranjit S. Shetty & Sandra Gill & James F. Gusella &
Robin Reed & Susan A. Slaugenhaupt
Received: 18 September 2006 /Revised: 24 October 2006 /Accepted: 26 October 2006 / Published online: 6 January 2007# Springer-Verlag 2007
Abstract Mutations that affect the splicing of pre-mRNAare a major cause of human disease. Familial dysautonomia(FD) is a recessive neurodegenerative disease caused by a Tto C transition at base pair 6 of IKBKAP intron 20. Thismutation results in variable tissue-specific skipping of exon20. Previously, we reported that the plant cytokinin kinetindramatically increases exon 20 inclusion in RNA isolatedfrom cultured FD cells. The goal of the current study was toinvestigate the nature of the FD splicing defect and themechanism by which kinetin improves exon inclusion, as
such knowledge will facilitate the development of futuretherapeutics aimed at regulating mRNA splicing. In thisstudy, we demonstrate that treatment of FD lymphoblastcell lines with kinetin increases IKBKAP mRNA and IKAPprotein to normal levels. Using a series of minigeneconstructs, we show that deletion of a region at the end ofIKBKAP exon 20 disrupts the ability of kinetin to improveexon inclusion, pinpointing a kinetin responsive sequence
J Mol Med (2007) 85:149–161DOI 10.1007/s00109-006-0137-2
M. M. Hims :M. Leyne : J. Mull : L. Liu : C. Lazaro :R. S. Shetty : S. Gill : J. F. Gusella : S. A. SlaugenhauptCenter for Human Genetic Research, Massachusetts GeneralHospital and Harvard Medical School,Boston, MA 02114, USA
E. C. Ibrahim : R. ReedDepartment of Cell Biology, Harvard Medical School,Boston, MA 02115, USA
C. LazaroTranslational Research Laboratory, Institut Català d’Oncologia,L’Hospitalet de Llobregat,Barcelona, Spain
Present address:E. C. IbrahimNICN-UMR 6184 CNRS,Faculté de Médecine Nord-IFR Jean Roche,Marseilles, France
S. A. SlaugenhauptCenter for Human Genetic Research,Massachusetts General Hospital,185 Cambridge Street, CPZN-5254,Boston, MA 02114, USAe-mail: [email protected]
(*)
SUSAN A. SLAUGENHAUPTreceived her Ph.D. in HumanGenetics from the University ofPittsburgh in Pittsburgh, PA,USA. She is presently anAssociate Professor ofNeurology in the Center forHuman Genetic Research atMassachusetts General Hospitaland Harvard Medical School.Her research interests includethe discovery and characteriza-tion of human disease genesand the role of mRNA splicingin human disease.
MATTHEW M. HIMS
received his Ph.D. in humangenetics from the University ofLeeds, England. He is currentlya postdoctoral research fellow inthe Center for Human GeneticResearch at MassachusettsGeneral Hospital. His researchinterests include the role ofRNA splicing in human diseaseand the development of accuratemurine models of humansplicing defects.

element. We next performed a screen of endogenouslyexpressed genes with multiple isoforms resulting from exonskipping events and show that kinetin’s ability to improveexon inclusion is not limited to IKBKAP. Lastly, wehighlight the potential of kinetin for the treatment of otherhuman splicing disorders by showing correction of asplicing defect in neurofibromatosis.
Keywords mRNA splicing . Dysautonomia . Kinetin
Introduction
It has become increasingly clear in recent years thatalternative splicing contributes significantly to transcriptdiversity. Estimates of the proportion of human genes thatare alternatively spliced range from 35% to as high as 74%[1–3]. The study of human genetic disease also highlightsthe importance of mRNA splicing, as greater than 15% ofdisease-causing mutations result in splicing defects [4].Mutations that disrupt RNA splicing have been foundwithin the canonical splice sites and within regulatory cis-acting exonic and intronic sequences, reviewed in the studyof Cartegni et al. (2002) [5]. Unlike genes that harbordeletions, insertions, or missense mutations, genes withsplice mutations may still retain the ability to code forreduced levels of normal protein if the gene is occasionallyspliced correctly. Such splicing mutations are sometimesreferred to as ‘leaky’ as they produce both mutant and wild-type transcripts from the same allele [6, 7]. It has beennoted that subtle differences in the level of mis-splicing,and therefore, in the amount of normal protein produced,can lead to striking differences in disease phenotype andseverity [8]. For example, mutations in ATP7A areresponsible for both Menkes disease (MD), a lethal disorderof copper metabolism, and occipital horn syndrome (OHS),a milder disorder characterized by connective tissueabnormalities. MD is caused by mutations in the invariantdonor splice site of exon 6 that lead to complete exonskipping, while OHS is the result of a mutation atnucleotide 6 of the same donor splice site that leads toincomplete exon skipping, resulting in the milder pheno-type [9]. These observations have made splicing defects
attractive candidates for the development of therapeutics assmall shifts in splicing efficiency may lead to drasticphenotypic improvement. Targeting splicing defects as ameans of treating genetic disease is a young field that hasshown some initial promise. A variety of strategies havebeen used to alter splicing in human disease-causing genes,including oligonucleotide based technologies, RNA medi-ated mechanisms and pharmacologic agents, reviewed inthe studies of Garcia-Blanco (2003), Garcia-Blanco et al.(2004), and Yeo GW (2005) [10–12].
The human neurodegenerative disease, familial dysauto-nomia (FD), is an example of a disorder that is caused by a‘leaky’ splice defect. As FD patients produce detectablelevels of wild-type transcript and protein, this disorder maybe amenable to therapeutic approaches aimed at improvingexon inclusion. FD, or Riley–Day syndrome, (OMIM#223900) is the best known and most frequent of a groupof congenital sensory neuropathies characterized by wide-spread sensory and autonomic dysfunction. Developmental-ly, FD is caused by the poor development and progressivedegeneration of unmyelinated sensory and autonomicneurons [13, 14]. FD is a recessive genetic defect with aremarkably high carrier frequency in Ashkenazi Jewsranging from 1 in 18 (Polish descent) [15] to 1 in 32 [16].The clinical spectrum of the disease includes gastrointesti-nal dysfunction, abnormal respiratory responses to hypoxicand hypercarbic states, gastroesophageal reflux, vomitingcrises, lack of overflow teas, profuse sweating, and posturalhypertension [14]. Three FD-causing mutations have beenidentified to date in the IKBKAP gene: an intronicnoncoding point mutation, IVS20+6T>C (c.2204+6T>C,NM_003640.2), which leads to variable skipping of exon20, and two missense mutations, R696P (four patients) andP914L (one non-Jewish patient) [17–19].
Importantly, all FD patients possess at least one copy ofthe IVS20+6T>C mutation; 99.5% are homozygous, andfive patients are compound heterozygotes for the missensemutations [17–19]. This suggests that a treatment based onmodification of splicing efficiency will have the potential tobenefit all patients with FD. The major mutation results invariable skipping of exon 20 in the IKBKAP transcript(Fig. 1a). We have previously shown that despite the factthat FD is a recessive disease, homozygous mutant cells
Fig. 1 a Schematic diagramshowing the unspliced IKBKAPpre-mRNA, the wild-type (WT)and mutant (MU) spliced IKBKAP isoforms. Also indicated isthe location of the major FDmutation (IVS20+6T>C) at basepair 6 of intron 20. b Chemicalstructure of the plant cytokininkinetin (6-furfurylaminopurine)
150 J Mol Med (2007) 85:149–161

express both wild-type (WT) and mutant (MU) IKBKAPisoforms, and are therefore, capable of producing full-length functional IKAP protein [19]. Thus, the mutationweakens but does not completely inactivate the 5′ splicesite of exon 20.
We have used both densitometric analysis of reversetranscriptase-polymerase chain reaction (RT-PCR) prod-ucts and quantitative PCR to show that the relativeamount of MU and WT IKBKAP transcripts variesbetween tissues, with the lowest levels of wild-typeIKBKAP production in tissues from the central andperipheral nervous system [20]. These observations suggestthat cellular levels of IKAP protein in neurons fall belowthe threshold level required for normal development andmaintenance. The removal of exon 20 from the IKBKAPtranscript results in a frameshift and the creation of apremature termination codon in exon 21. Consequently, themutant transcript is predicted to be targeted for destructionvia the nonsense mediated decay (NMD) pathway [21].This prediction is consistent with our observations thattreatment of cultured FD cells with cycloheximide, aninhibitor of NMD, increases the level of the MU isoform[22] and the absence of a truncated protein in FD patienttissue and cell lines [19, 23]. Using computational analysiscombined with experimental validation, we recentlyreported that IKBKAP exon 20 definition is inherentlyweak even in the absence of the FD mutation and that exonskipping results from the additive effect of multiple weaksplicing signals in the exon 20 environment [24].
The IKBKAP gene encodes IKAP, which was originallyidentified as an IκB kinase (IKK) complex-associatedprotein [25]. However, this name is now a misnomer assubsequent work has disproved the role of IKAP in thispathway [26]. IKAP is a subunit of the highly conservedcomplex, Elongator, which is involved in transcriptionalelongation [27]. Recently, RNA interference studies haveshown that depletion of IKAP, and therefore Elongator,results in reduced transcriptional elongation of severaltarget genes via histone H3 hypoacetylation. A subset ofthese target genes are required for cell motility, and FDpatient cells were shown to be defective in cell migrationassays, suggesting that defective cellular motility mayunderlie the developmental neuropathology of FD [23].IKAP has also been implicated in a variety of cellularfunctions in addition to its proven role in transcription. Datain yeast suggest that the Elongator complex is involved inexocytosis and tRNA modification [28, 29], while studiesin mammalian cells implicate IKAP as a scaffold proteininvolved in cytoplasmic JNK activation in response toextracellular stress [30]. IKAP’s role in these processes, andhow they relate to the FD phenotype, is not yet understood.
Our characterization of the IKBKAP splice defect in FDsuggests that this disease is potentially treatable using
strategies that would improve exon 20 inclusion andincrease the amount of normal IKAP protein in FD patients.Although FD is a developmental disorder, patients showcontinued neuronal degeneration throughout life, whichleads to progressive ataxia and dementia in adulthood. Anincrease in IKAP at an early age might slow neuronal lossand reduce the symptoms that appear as patients mature.We participated in the NINDS sponsored Neurodegenera-tion Drug Screening Consortium, during which wescreened an extensive and diverse collection (the NINDSCustom Collection) of FDA-approved drugs and naturalproducts in FD cells [31]. The program was intended tobroadly evaluate compounds that have already demonstrat-ed safety and efficacy as human drugs, and therefore, couldface a less arduous regulatory process than novel com-pounds before testing in patients. During this screen of1,040 compounds, we identified the plant cytokinin kinetin(Fig. 1b) as a potent splicing enhancer for IKBKAP in bothFD lymphoblast and fibroblast cell lines [22]. We furthershowed the effect of kinetin to improve splicing in anIKBKAP minigene, but not on an additional splicing eventin MYO5A, suggesting that local sequence elementspresent in the IKBKAP exon 20 splicing environment arerequired in kinetin’s effect.
In the present study, we show for the first time thatkinetin is able to increase the level of both WT IKBKAPtranscript, and more importantly, IKAP protein to normallevels in FD cells. We then investigate the mechanism bywhich kinetin acts to improve exon 20 inclusion. Using anin vivo minigene model and a series of mutation, insertionand deletion constructs, we have determined that a motif atthe 3′ end of exon 20, most likely containing the 5′ splicesite, is necessary for kinetin’s action. Having demonstratedthat the effect of kinetin is sequence dependent, we thencarried out a screen of alternatively spliced exons andidentified two other genes that show a change in isoformratio after kinetin treatment. Finally, we demonstrate thepotential of kinetin to treat other splicing defects byshowing improved exon inclusion of NF1 exon 36 in aminigene model system of a splice mutation that causesneurofibromatosis type 1.
Materials and methods
Cell lines, tissue culture and kinetin treatment
Patient, carrier, and normal cell lines previously establishedin our laboratory by EBV transformation were utilized inthis study [32]. We have current institutional review boardapproval for the establishment and the use of these linesthrough New York University Medical Center and Massa-chusetts General Hospital. Lymphoblast lines were grown
J Mol Med (2007) 85:149–161 151

in RPMI-1640, supplemented with 2 mM L-glutamine and1% penicillin/streptomycin and with 10% fetal bovineserum. Where noted, lymphoblast cell lines were culturedwith kinetin solution (Sigma 1 mg/ml), at a final concen-tration of 100 μM for 72 h unless otherwise stated.Fibroblast and HEK cells were grown in Dulbecco’sModified Eagle’s Medium (DMEM) supplemented with2 mM L-glutamine and 1% penicillin/streptomycin and with10% fetal bovine serum.
WT IKBKAP quantitative PCR
Quantitative PCR analysis of WT IKBKAP was carried outusing the BIORAD iCylcer, Cyber Green supermix (BIORAD) a n d p r im e r s , F - 5 ′ - TTCACGGATTGTCACTGTTGTGCC-3′ and R-5′-TTCACGGATTGTCACTGTTGTGCC, specific to the WT spliced isoform.Human HPRT was used to normalize expression betweencell lines using primers, F-5′TGACACTGGCAAAACAATGCA, and R-5′-GGTCCTTTT CACCAGCAAGCT.
Western blot
Lymphoblast cell lines were treated with 100 μM kinetinfor 3 days, 1 week, and 2 weeks. Equal quantities ofextracted protein were run on a 6% acrylamide gel andtransferred to nitrocellulose membrane. IKAP was detectedusing a monoclonal antibody raised against amino acids796–1,008 of IKAP (BD Bioscience 117720), that detectsthe 150-kDa full length IKAP protein. The same blot wasprobed with antibodies to IQGAP (BD Bioscience 610611)as a loading control.
Minigene constructs, transfection, and splicing analysis
All IKBKAP constructs were derived from the IKBKAPminigene previously described [22], which includes clonedgenomic IKBKAP sequences from exon 19 to intron 21,including intervening introns. Nucleotide alterations anddeletions were introduced by site-directed mutagenesis,using a QuickChange Mutagenesis Kit (Stratagene).
Fragments of IKBKAP exon 20 (19 base pair oligonucleo-tides) were cloned into SXN (obtained from Dr. ChrisBurge) using SalI and BamHI restriction sites located withinwith SXN exon 2. The NF1 exon 36 minigene (NF1-EX36)containing genomic sequence from exons 35 to 37 wascreated by cloning an amplified fragment of genomic NF1into pcDNA3.1-TOPO (Invitrogen) using primers F-5′CCAGTGGACAGAACTAGCTCAA and R-5′TGATACCCAAAATGAATGCAC. The 6724C>T mutation was intro-duced into the NF1 minigene by site-directed mutagenesis.
Cells, 293-HEK, were incubated in 12-well plates andtransfected with 1 μg of plasmid by the use of Genejuice
(Novagen), 4 h post-transfection, where noted cells weretreated with 200 μM kinetin solution (Sigma). After 24 h,cells were harvested and RNA extracted using Tri-reagent(MRC). Reverse transcription was performed using 1 μgtotal RNA, oligo(dT) primer and Superscript III reversetranscriptase (Invitrogen). Semiquantitative PCR was per-formed using cDNA equivalent to 100 ng of starting RNAin a 40-ul reaction, by the use of Taq Polymerase (Roche)and 30 amplification cycles (94°C for 30 s, 58°C for 30 s,72°C for 30 s). Amplification of transcripts from NF1 andall IKBKAP based minigenes was carried out with T7 (5′TAATACGACTCACTATAGGG) and BGHR (5 ′TAGAAGGCACAGTCGAGG) primers. Amplification ofSXN spliced transcripts was carried out using the followingprimers: F 5′-AGTCAGGGCAGAGCCATCTA and R 5′-CGTGCAGCCTTTGACCTAGTA. NF1 and IKBKAP mi-nigene products were separated on 1.5% agarose gels, andSXN products were separated on 3% agarose gels andstained with ethidium bromide. The relative amount ofspliced isoforms in a single-PCR reaction were determinedusing Alpha 2000™ Imager Analyzer (BioRad) and Image-Quant QL software (Amersham), using the integrateddensity value (IDV) for each band [20], and the proportionof larger isoform detected was calculated as a percentage.
Semiquantitative RT-PCR of endogenous genes
Reverse transcription was performed using 1 μg total RNAfrom kinetin-treated and untreated lymphoblast cell lines,oligo(dT) primer, and Superscript III reverse transcriptase(Invitrogen). Primers to assay a skipping event were in theexons adjacent to skipped exon or used as described asnoted in the literature. Semiquantitative PCR was per-formed using cDNA equivalent of 40 ng of starting RNA,by the use of Taq Polymerase (Roche) and 30–35amplification cycles (94°C for 30 s, 58°C for 30 s, 72°Cfor 30 s). Products depending on size were separated on 1.5or 3% agarose gels and were stained with ethidiumbromide. The relative amount of spliced transcripts in asingle-PCR reaction were determined using Apha 2000™Imager Analyzer and Image Quant QL software, using theintegrated density value (IDV) for each band, as previouslydescribed in the study of Cuajungco et al. 2003 [20]. Thefollowing splice events and primers were used: EFNA5exon 4 (NM_001962) F-5′TGCAATCCCAGATAATGGAA, R-5′ATCGCCAGGAGGAACAGTAG; MYCBP2exon 19 (NM_015057) F-5′TGTCCCAGTGCCCGGG, R-5′GGTGAAATCCACAGCTGACTTGG [33]; HMGCR ex-on 13 (NM_000859) F-5 ′CCAGCCTACAAGTTGGAAACTC, R-5 ′CGAGCCAGGCTTTCACTT (1);MYO5A exon 35 (NM_000259) F-5′GAATACAATGACAGATTCCAC, R-5′CAGGCTGGCCTCAATTGC [34];SFRS10 exon 2 (NM_004593) F-5′AAGGAAGGTGCAA
152 J Mol Med (2007) 85:149–161

GAGGTTG, R-5′CGGCAATGGGACCATATTTA [35];BMP2K exon 14 (NM_198892) F-5′AACATCAGCAATCCACCTGA, R-5′GGTTTGCAGTGCCATTTTCT; ABI2exon 2 (U23435) F-5′CCGATTACTGCGAGAACAACT,R-5′CCCATCTTCATGTTCTGGGTA.
Results
IKBKAP exon 20 splicing efficiency in FD lymphoblastcell lines
Baseline IKBKAP levels were initially established usinglymphoblast cell lines from three FD patients, three carriers,and three normal controls. We used a specific quantitativePCR assay that amplifies only the WT isoform using aprimer within exon 20 (Fig. 2). The levels of WT IKBKAPin mRNA isolated from FD cell lines is approximately 30%of normal and that in carrier cell lines is 70% of normal,suggesting that the mutant allele is correctly splicedapproximately 30% of the time in transformed lymphoblastcell lines. A similar assay performed using FD and controlprimary fibroblast cell lines shows that in this cell type, theIVS20+6T>C allele is spliced correctly approximately 15%of the time (data not shown). We previously estimated thatthe mutant allele is spliced correctly only 5% of the time inneurons, illustrating that tissue-specific regulation of splic-ing can play a major role in the pathogenesis of humansplicing diseases [20].
Kinetin treatment restores normal IKAP levels in patientcells
FD is due to a dramatic, tissue-specific decrease in the levelof wild-type IKBKAP mRNA. Therefore, one of the goals
of the current study was to determine if treatment of FD celllines with kinetin could increase both IKBKAP mRNA andIKAP protein levels to those observed in FD carriers andcontrols. We first examined the percent of WT isoformusing a densitometric PCR assay that detects both spliceproducts. Figure 3a shows that kinetin dramaticallyimproves exon 20 inclusion and increases the relativepercentage of WT isoform in both FD and carrier cell lines.We next measured the total amount of WT IKBKAP mRNAin the same cell lines using quantitative PCR and primersthat are specific to the WT transcript (Fig. 3b). We foundthat in both the FD and carrier lymphoblast cell lines treatedwith kinetin for 3 days, the level of WT IKBKAP isincreased above normal untreated levels, confirming thatthe observed change in isoform ratio leads to increasedcellular levels of the WT IKBKAP transcript.
To confirm that the observed increase in IKBKAPmRNA after kinetin treatment leads to a direct increase inIKAP protein, we treated the nine cell lines used above with100 μM kinetin for 2 weeks and determined IKAP proteinlevels at three time points using an IKAP monoclonalantibody (612282 BD Bioscienes) (Fig. 3c). A clearincrease in IKAP protein expression can be seen progres-sively from 3 days to 1 week, and continued treatment overa period of 2 weeks leads to accumulation of IKAP proteinand restoration of IKAP levels to those observed in controlcell lines (Fig. 3c). These results are very encouraging asthey suggest that kinetin may be a potent therapeutic agentcapable of boosting cellular IKAP levels into the normalrange.
The FD mutation is not required for kinetin activity
Previously, we reported the development of a minigenesystem that models the mis-splicing seen in FD patientscells. These minigenes contain the complete IKBKAPgenomic sequence from the start of exon 19 through thefirst 16 nucleotides of intron 21, and the wild-type controland FD construct differ only in the IVS20+6 position [22,24]. Kinetin improves splicing and increases exon 20inclusion in the minigene transcripts, suggesting that localsequence elements are required for activity. In the currentstudy, we examined the splicing of transcripts fromminigene constructs with either an A or G (FD=C,WT=T) at position 6 of intron 20 to determine if kinetinactivity depended upon the specific FD mutation. Aspredicted computationally by 5′ splice site strength, thepresence of a C, a G, or an A at position 6 of intron 20 allled to weakened exon 20 inclusion when compared to theWT sequence (Fig. 4). Our in vivo-splicing assay showedthat kinetin improves splicing in constructs FD-MG andalso in 6A-MG, demonstrating that the FD mutation itself(IVS20+6C) is not required for kinetin activity.
Fig. 2 Analysis of WT IKBKAP levels in FD, carrier, and controllymphoblast cell lines. Expression levels are the average of threeindependent cell lines assayed in triplicate. Control normal cells wereconsidered to have 100% WT IKBKAP expression, and expression inFD (30%) and carrier (73%) cell lines are shown as a percentage ofnormal expression
J Mol Med (2007) 85:149–161 153

Kinetin improves splicing in a variety of modified IKBKAPminigenes
In our previous studies, we created a large series ofIKBKAP minigene constructs that show altered exon 20
inclusion in mRNA as a consequence of targeted sequencechanges in and around exon 20 [24]. Many of theseconstructs contain nucleotide substitutions that alter pre-dicted exonic splice silencer (ESS) or exonic spliceenhancer (ESE) motifs. As one of the goals of this study
Fig. 4 The effect of kinetin on in vivo splicing of IKBKAP minigenetranscripts with sequence alterations at exon 20 5′ splice site +6position. a A schematic representation of the exon/intron structure ofIKBKAP 19-21 minigene construct and sequence alterations made tothe 5′ splice site of exon 20. The splice site strengths for the respective5′ splice sites are shown, calculated using a modified Sapiro andSenapathy matrix method (http://ast.bioinfo.tau.ac.il/SpliceSiteFrame.htm) [50]. b RT-PCR analysis of ethidium stained agarose gel of invivo spliced transcripts from four IKBKAP minigene constructs
varying only at base pair 6 of intron 20. A relative increase in WTisoform in response to kinetin treatment is indicated by a YES, in the‘kinetin response’ column. Each construct and treatment is shown induplicate and represents independent transfections. Minigene con-structs FD-MG (IVS20+6C) and 6A-MG (IVS20+6A) both show aresponse to kinetin treatment with a relative increase in WT isoform.Constructs WT-MG and 6G-MG produce only one IKBKAP isoformand were therefore uninformative for kinetin
Fig. 3 The effect of kinetin treatment on relative MU:WT isoformlevels, WT IKBKAP expression, and IKAP protein levels in FD,carrier, and control lymphoblast cell lines. a Analysis of RT-PCRproducts on an ethidium stained agarose gel. Below each lane is therelative amount of WT:MU isoform, presented as WT percentage.b Absolute level of WT IKBKAP mRNA in kinetin-treated vsuntreated lymphoblast cell lines. Expression values shown are theaverage of three cell lines, assayed in triplicate, and normalized to
untreated control cells which are considered to have 100% expression.c Western blot probed with an IKAP monoclonal antibody showingincreasing levels of full length IKAP protein in FD lymphoblast cellsfollowing kinetin treatment. FD cells were treated with kinetin for3 days, 1 week, and 2 weeks and are shown compared to untreatedFD, control, and carrier cell lines. The lower panel shows the sameblot probed with IQGAP as a protein loading control. Results areshown for two independent FD, carrier, and control cell lines
154 J Mol Med (2007) 85:149–161

was to identify the sequences required for kinetin respon-siveness, we assayed splicing of these constructs todetermine if alteration of these cis-acting control elementsreduced or eliminated kinetin-induced splicing improve-ment. Data comparing the in vivo splicing of six of theseconstructs expressed in untreated and kinetin-treated HEKcells is shown in Fig. 5. Kinetin increased exon 20inclusion in all cases, suggesting that these specific cis-
acting control elements are not involved in kinetinsensitivity.
Insertion of IKBKAP exon 20 sequence fragmentsdoes not confer kinetin sensitivity
As kinetin improved splicing in all of the ESS/ESEmodified constructs, we created a series of minigeneconstructs to systematically test all of exon 20 for cis-acting target elements that kinetin may be operating on,either directly or indirectly. First, we tested the ability ofkinetin to effect the splicing of a second transientlyexpressed minigene construct, SXN. The SXN construct isa four-exon β-globin derived minigene [36]. It has beenpreviously shown that the inclusion or exclusion of SXNexon 2 is delicately balanced when SXN is transientlyexpressed. SXN exon 2 inclusion can be improved whenthe exon is lengthened, when an enhancer element ispresent, or when the 5′ or 3′ canonical splice sites areimproved [36–39]. As shown in Fig. 6, kinetin treatmenthad no effect on splicing of the SXN control construct,supporting our previous findings that kinetin does not affectall splicing events.
The goal of this experiment was to determine if we couldconfer sensitivity to kinetin in the SXN minigene bycloning IKBKAP exon 20 sequence elements into SXNexon 2. We cloned seven overlapping 19-bp sections ofIKBKAP exon 20 into the middle of SXN exon 2, creatingan exon of 34 bp (SXN20-1 to SXN20-7) and tested theseconstructs using our in vivo splicing assay. Examination ofFig. 6 shows that SXN20-2, SXN20-3, SXN20-4, andSXN20-7 minigenes all produce both splice isoforms, yetshow no difference in their levels due to kinetin treatment.We conclude, therefore, that these fragments of exon 20 inthe context of the SXN minigene, do not contain thesequences necessary to confer sensitivity to kinetin.Elements within constructs SXN20-1, SXN20-5, andSXN20-6 severely impact splicing and result in productionof only the exon skipped transcript. In these constructs, wecannot determine if a kinetin control element is indeedpresent but not strong enough to overcome the negativeeffect on splicing conferred by the inserted element.
Deletion of an exon 20 CAA element disrupts the abilityof kinetin to improve splicing
As the insertion constructs did not identify a specificsequence element that conferred sensitivity to kinetin, wenext created a series of deletion constructs using theoriginal control FD-MG minigene (see Fig. 7a). Wehypothesized that deletion of exon 20 fragments in thecontext of the entire exon might pinpoint the controlelement. We initially divided exon 20 into four nonover-
Fig. 5 Analysis of modified IKBKAP minigenes using an in vivosplicing assay. Targeted alterations of exon 20 sequences can alterexon 20 inclusion, while not disrupting kinetin’s effect to improveinclusion. a Analysis of RT-PCR products on ethidium stained agaroseof in vivo spliced transcripts from modified FD-MG constructs. Theconstructs shown are all modifications of FD-MG with targetedalterations of exon 20 sequences, aimed at either strengtheningpredicted ESE content or disrupting predicted ESS (TAGG) motifs[24]. All alterations shown improve the efficiency of exon 20inclusion relative to the FD-MG construct. Despite these sequencemodifications, all constructs responded to kinetin treatment withincreased efficiency of exon 20 inclusion. A relative increase in WTisoform in response to kinetin treatment is indicated by a YES, in the‘kinetin response’ column. Each construct and treatment is shown induplicate from independent transfections. b Shows the targetedsequence alterations made to exon 20. The targeted motif for eachconstruct is shown in bold, and the altered nucleotide(s) are under-lined. The complete unmodified exon 20 sequence of the FD-MGconstruct is also shown for comparison
J Mol Med (2007) 85:149–161 155

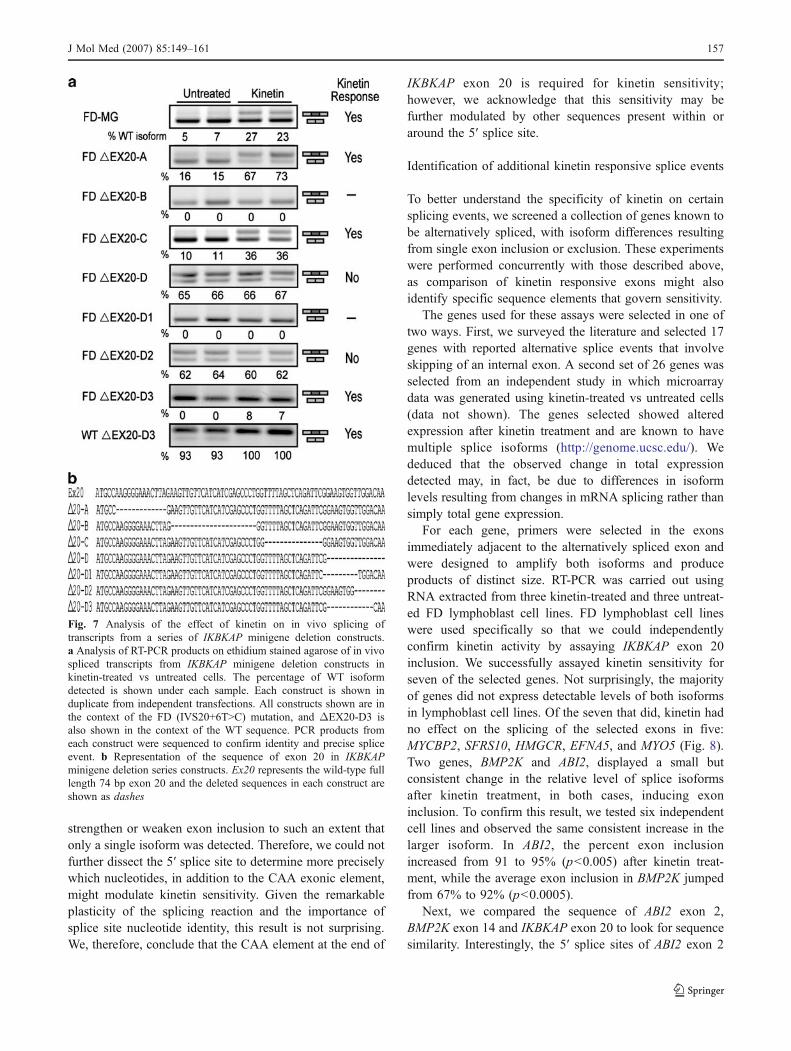
lapping sections (A–D) and deleted 14–22 base pairsegments. We tested these constructs for changes in therelative amounts of MU to WT isoforms produced afterkinetin treatment of transfected HEK cells. ConstructsΔEX20-A andΔEX20-C both respond to kinetin treatment.Splicing was completely disrupted in construct ΔEX20-B,and therefore, uninformative; however, construct ΔEX20-Dproduced both splice isoforms in equal amounts regardlessof kinetin treatment. This was the first IKBKAP exon 20construct that did not positively respond to treatment withkinetin, suggesting that deletion of the last 15 base pairs ofexon 20 disrupts the ability of kinetin to improve exon 20inclusion. Therefore, we further dissected the EX20-Dregion to pinpoint the required sequences.
The deletion of EX20-D1 resulted in complete exonskipping, suggesting the presence of a splice enhancer inthis region. Construct ΔEX20-D3 was responsive to kinetintreatment; however, deletion of this element also weakenedexon inclusion so it was difficult to detect the kinetinresponse. We, therefore, tested this deletion in both the FDand WT constructs and confirmed the presence of the
sequence required for kinetin sensitivity (Fig. 7). Examina-tion of Fig. 7 shows that construct ΔEX20-D2, likeconstruct ΔEX20-D described above, does not respond tokinetin. This suggests that the last seven base pairs of exon20, which are deleted in both ΔEX20-D2 and ΔEX20-Dare required for kinetin to improve splicing. These deletionschange the exonic contribution to the 5′ splice site fromCAA-intron to TCG/TGG-intron. The sequence differencebetween the nonresponsive ΔEX20-D construct and theresponsive ΔEX20-D3 is limited to the last three nucleo-tides of exon 20 at the 5′ splice site itself, stronglysuggesting that these three nucleotides are involved in themechanism and specificity by which kinetin improvesIKBKAP exon 20 inclusion.
To determine if kinetin sensitivity is governed solely bythe presence of the CAA motif at the end of the exon, or ifrather the entire 5′ splice donor site is involved, weexamined several constructs with single nucleotide alter-ations in the 5′ splice site [24]. As expected, alteringnucleotides within the canonical 5′ splice site changes thesplicing efficiency dramatically; in this case, acting to either
Fig. 6 Analysis of the effect of kinetin on the splicing of the SXNminigene, containing cloned IKBKAP exon 20 sequences. a Schematicdiagram showing the exonic/intronic structure of the SXN minigeneand the seven insert (19 mer) sequences of IKBKAP exon 20 clonedinto the context of the SXN minigene. b Analysis of RT-PCR productson ethidium stained agarose of in vivo spliced transcripts of transientlyexpressed FD-MG and SXN constructs in kinetin-treated and untreated
HEK cells. In FD-MG control sample, an increase in exon 20 inclusioncan be observed in kinetin-treated cells; however, there is noobservable change in any SXN construct in the inclusion of exon 2in between treated and untreated samples. An increase in exon 2containing transcripts in response to kinetin treatment is indicated by aYES, in the ‘kinetin response’ column. Each construct and treatment isshown in duplicate from independent transfections
156 J Mol Med (2007) 85:149–161
strengthen or weaken exon inclusion to such an extent thatonly a single isoform was detected. Therefore, we could notfurther dissect the 5′ splice site to determine more preciselywhich nucleotides, in addition to the CAA exonic element,might modulate kinetin sensitivity. Given the remarkableplasticity of the splicing reaction and the importance ofsplice site nucleotide identity, this result is not surprising.We, therefore, conclude that the CAA element at the end of
IKBKAP exon 20 is required for kinetin sensitivity;however, we acknowledge that this sensitivity may befurther modulated by other sequences present within oraround the 5′ splice site.
Identification of additional kinetin responsive splice events
To better understand the specificity of kinetin on certainsplicing events, we screened a collection of genes known tobe alternatively spliced, with isoform differences resultingfrom single exon inclusion or exclusion. These experimentswere performed concurrently with those described above,as comparison of kinetin responsive exons might alsoidentify specific sequence elements that govern sensitivity.
The genes used for these assays were selected in one oftwo ways. First, we surveyed the literature and selected 17genes with reported alternative splice events that involveskipping of an internal exon. A second set of 26 genes wasselected from an independent study in which microarraydata was generated using kinetin-treated vs untreated cells(data not shown). The genes selected showed alteredexpression after kinetin treatment and are known to havemultiple splice isoforms (http://genome.ucsc.edu/). Wededuced that the observed change in total expressiondetected may, in fact, be due to differences in isoformlevels resulting from changes in mRNA splicing rather thansimply total gene expression.
For each gene, primers were selected in the exonsimmediately adjacent to the alternatively spliced exon andwere designed to amplify both isoforms and produceproducts of distinct size. RT-PCR was carried out usingRNA extracted from three kinetin-treated and three untreat-ed FD lymphoblast cell lines. FD lymphoblast cell lineswere used specifically so that we could independentlyconfirm kinetin activity by assaying IKBKAP exon 20inclusion. We successfully assayed kinetin sensitivity forseven of the selected genes. Not surprisingly, the majorityof genes did not express detectable levels of both isoformsin lymphoblast cell lines. Of the seven that did, kinetin hadno effect on the splicing of the selected exons in five:MYCBP2, SFRS10, HMGCR, EFNA5, and MYO5 (Fig. 8).Two genes, BMP2K and ABI2, displayed a small butconsistent change in the relative level of splice isoformsafter kinetin treatment, in both cases, inducing exoninclusion. To confirm this result, we tested six independentcell lines and observed the same consistent increase in thelarger isoform. In ABI2, the percent exon inclusionincreased from 91 to 95% (p<0.005) after kinetin treat-ment, while the average exon inclusion in BMP2K jumpedfrom 67% to 92% (p<0.0005).
Next, we compared the sequence of ABI2 exon 2,BMP2K exon 14 and IKBKAP exon 20 to look for sequencesimilarity. Interestingly, the 5′ splice sites of ABI2 exon 2
Fig. 7 Analysis of the effect of kinetin on in vivo splicing oftranscripts from a series of IKBKAP minigene deletion constructs.a Analysis of RT-PCR products on ethidium stained agarose of in vivospliced transcripts from IKBKAP minigene deletion constructs inkinetin-treated vs untreated cells. The percentage of WT isoformdetected is shown under each sample. Each construct is shown induplicate from independent transfections. All constructs shown are inthe context of the FD (IVS20+6T>C) mutation, and ΔEX20-D3 isalso shown in the context of the WT sequence. PCR products fromeach construct were sequenced to confirm identity and precise spliceevent. b Representation of the sequence of exon 20 in IKBKAPminigene deletion series constructs. Ex20 represents the wild-type fulllength 74 bp exon 20 and the deleted sequences in each construct areshown as dashes
J Mol Med (2007) 85:149–161 157

(CAA-GTGAGA) and BMP2K exon 14 (CAA-GTAAGG),like that of IKBKAP exon 20 (CAA-GTAAGT) contain thesequence CAA as the exonic contribution to the splice site(Fig. 9b). This sequence is not present in the 5′ splice sitesof the genes that did not show kinetin sensitivity: EFNA5exon 4 (CAG-GTTAGT), HMGCR exon 13 (GGT-GTAAGT), MYO5A exon 31 (CAG-GTTATA), SFRS10exon 2 (TAG-GTAAGA), and MYCBP2 exon 19 (AAG-GTATTT).
These results illustrate, for the first time, that kinetin iscapable of altering the splicing of an exon other thanIKBKAP exon 20. Combined with the results obtainedusing the deletion constructs described above, it also argues
strongly for sequence specificity that is at least partiallygoverned by the presence of a CAA element at the 5′ splicesite.
Identification of an NF1 mutation that responds to kinetin
Neurofibromatosis type 1 (NF1, MIN# 162000) is anautosomal dominant disease caused by mutations in theNF1 gene, which is one of the most commonly mutateddisease-causing human genes. Furthermore, it has beenestimated that between 28 and 50% of mutations in NF1alter pre-mRNA splicing. Exon skipping events have beenreported for many NF1 exons [40, 41]. To determine ifkinetin might prove efficacious in another human mRNAsplicing disease, we created NF1 minigene construct pairsusing the wild-type sequence and six NF1 mutations thatinduce skipping. One construct, NF1-EX36, successfullymodeled the human splicing defect and was tested forkinetin sensitivity. The remainder of the NF1 constructs didnot model endogenous NF1 splicing, and were therefore,discarded (data not shown).
Fig. 9 Kinetin improves in vivo splicing of NF1 exon 36 in aminigene construct model. a Schematic representation of NF1 exon 36minigene (NF1-EX36, 6724C>T including exons 35 to 37) andanalysis of RT-PCR products on ethidium stained agarose of in vivospliced transcripts from this construct. Untreated and treated samplesare show in duplicate from independent transfections. The relativepercentage of the larger isoform (containing exon 36) is shown foreach sample. An increase in exon 36 containing isoform can be seenin kinetin-treated samples. Sequencing of the spliced productsconfirmed that the 372-bp product contains exon 36 and the 257 bpdoes not and revealed in both transcripts that an alternative crypticsplice site (C) downstream of exon 37 was used. b Shows thecomparison of the 5′ splice site of IKBKAP exon 20, ABI2 exon 2,BMP2K exon 14, and NF1 exon 36. Indicted are the location of theCAAG motifs
Fig. 8 Analysis of the effect of kinetin on splicing events in sevenendogenously expressed genes in three treated and untreated FDlymphoblast cell lines. In each event, the upper PCR productrepresents the exon included isoform, and the lower product representsthe exon skipped isoform. Product sizes are indicated on the right ofeach gel. All products were sequenced to confirm identity. The relativeamount of the larger isoform in each sample was calculated as apercentage using IDV analysis of the PCR products. As a control forthe kinetin effect, an increase in WT IKBKAP isoform can be seenwith kinetin treatment in all three cell lines. A change in relativeisoform ratios in response to kinetin treatment is indicated by a YES,in the ‘kinetin response’ column. A detectable increase in the relativelevels of isoforms containing ABI2 exon 2 and BMP2K exon 14 wasobserved with kinetin treatment
158 J Mol Med (2007) 85:149–161

The NF1-EX36 minigene construct contains the completegenomic sequence from exon 35 through exon 37. Skippingof exon 36 is caused by the mutation c.6724C>T [42]. RT-PCR analysis of in vivo-spliced RNA from HEK cellstransfected with the wild-type and mutant constructs yieldedtwo splice isoforms, differing only in the incorporation ofexon 36, as expected. As shown in Fig. 9a, inclusion of exon36 was improved after kinetin treatment, illustrating thepotential of this compound for generalized applicability.Interestingly, examination of the 5′ splice site of NF1 exon36 reveals that the CAA sequence motif is present but offsetby a single nucleotide CAAG-GTACCT (Fig. 9b).
Discussion
Familial dysautonomia is an interesting and unusualrecessive disease in that all patients produce normal IKAP.The nature of the primary splicing mutation results in IKAPlevels that vary in different tissues, with the expression inneurons falling below a threshold required for properdevelopment and maintenance. Current knowledge of IKAPprotein function suggests that it is required for transcrip-tional elongation of a subset of genes [23], suggesting thatthe developmental neuropathy and continued neurodegen-eration seen in FD is caused by reduced expression of anumber of genes required for neuronal development andmaintenance. Therefore, FD can be thought of as a diseaseof transcription and a splicing disorder.
Treatment of cultured FD cells with kinetin results in adramatic shift in splicing, and the data presented in the currentstudy show that the observed splicing shift is sufficient toboost IKAP expression above normal levels. Analysis ofmRNA levels using quantitative PCR shows that the level ofwild-type IKBKAP message reaches normal levels after only8 h in culture [22], while western blot analysis shows thatnormal IKAP protein levels are achieved in FD cells by1 week. It is important to note that FD carriers arephenotypically normal, proving that their IKAP expressionlevel is above the pathogenic threshold. Kinetin actuallyincreases the level of IKAP in FD lymphoblast cells beyondthat seen in carriers to the normal range, demonstrating itspotential as a therapy for FD.
An advantage of targeting splicing defects for pharma-cologic treatment is that unlike other types of mutations, thecapacity of the cell to code for a functional protein remains.Furthermore, studies of other splicing disorders show thatthe balance of correct vs incorrect splice transcripts isvariable and can often be correlated to disease severity. Wehypothesize that in the case of FD, the balance ofantagonizing splicing factors is favorable towards exoninclusion in some tissues, which leads to IKAP levels thatare above that required for normal function. In neurons,
however, negative regulating factors have the upper handand exon 20 is skipped in the majority of transcripts,leading to IKAP levels that fall below the requiredthreshold. Thus, it is possible that a small change in thebalance of the splicing reaction may be sufficient to bringlevels of cellular IKAP above threshold levels, alleviatingthe physiological effects of aging in FD patients. As all FDpatients have the splice mutation, the added advantage oftargeting this particular type of defect is that every patientwill benefit from this.
Kinetin, or 6-furfurylaminopurine, has been shown todelay the onset and decrease the extent of aging character-istics in cultured human skin fibroblasts [43]. The molecularmechanism for the anti-aging properties is unknown,although kinetin has been reported to protect againstoxidative damage to both DNA and protein [44, 45]. It iswidely marketed today in a variety of skin-care products andis reportedly effective in improving skin roughness, mottling,and fine wrinkling [46]. Given that kinetin is currently usedonly for topical applications, toxicity studies are currentlyunderway to assess its potential as a treatment for FD.
The precise mechanism by which kinetin improvesIKBKAP exon 20 inclusion is currently unknown. In thisstudy, we begin to address this question, showing furtherevidence that kinetin’s activity is sequence specific. Weidentify four splice events that show increased exoninclusion after kinetin treatment. We also show that aCAA element at the end of IKBKAP exon 20 is required forkinetin activity. A survey of 5,000 5′ splice sites fromcontiguously spliced exons using the Hollywood splicedatabase reveals that 8.8% of internal exons contain thesequence CAA-GT or CAAG-GT at the 5′ splice site [47].If the CAA element in the context of the 5′ splice site is thebasis of kinetin sensitivity, we predict that kinetin willmodify splicing of only a small proportion of exons. Thisspecificity also suggests that kinetin is not acting on amajor component of the spliceosome required for constitu-tive splicing, but rather on a regulatory splicing factorrequired for the proper splicing of a subset of exons. Suchan effect is not unprecedented; indole derivatives haverecently been identified that interact directly and selectivelywith certain SR proteins, specifically inhibiting ESE-dependent splicing events [48].
The response to kinetin in the four splice events that arealtered as a result of treatment is variable, with increases inexon inclusion ranging from a subtle 5% (ABI2) to a dramatic50% (NF1-EX36). While some of this variability may be dueto experimental conditions, the range of differences suggeststhat there is splice event specific variation in the degree ofkinetin responsiveness. This is not surprising given that thecontrol of alternative splicing is believed to involve amultiple component regulatory mechanism with a highdegree of redundancy among the RNA binding proteins
J Mol Med (2007) 85:149–161 159

[49]. For example, a particular trans-acting splicing factormay play a role in the exon recognition and inclusion ofmany different exons; however, the extent of its role in anyone event probably varies widely.
The presence of a CAA motif in four kinetin responsivesplice events, coupled with the fact that deletion of thiselement in IKBKAP exon 20 eliminates kinetin sensitivity,suggest that kinetin is interacting with or modifying asplicing factor that binds preferentially to CAA sequencesvery near or adjacent to the 5′ splice donor site. DuringmRNA splicing, the U1 snRNA is known to bind to the 5′splice site. Given the close proximity of the CAA motif tothe U1 binding site, perhaps kinetin is indirectly boostingexon inclusion by enhancing U1 binding.
Regulation of alternative splicing is a complicated,multilayered process, and despite recent progress in thefield the ‘splicing code’ that dictates when an exon isskipped or included in the final transcript, is still poorlyunderstood. Future discovery of the factors that govern thetissue-specificity of the FD splice defect will lead to a betterunderstanding of tissue-specific alternative splicing. Thecurrent study illustrates, for the first time, that kinetin canboost IKAP levels into the normal range in FD and also thatkinetin can alter exon choice in other genes. These resultsare extremely encouraging as we continue to pursue kinetinas a potential therapeutic agent for the treatment of FD andother human splicing disorders.
Acknowledgements We wish to thank all FD patients and theirfamilies for their continued participation in our studies. We thank Dr.Felicia Axelrod and her staff at the Dysautonomia Treatment andEvaluation Center at New York University Medical School for herlong-standing contributions to this work. We also thank Dr. ChrisBurge for generously providing us with the SXN minigene construct.This work was supported by grants from the DysautonomiaFoundation Inc, the National Institute for Neurological Disordersand Stroke, and the Massachusetts General Hospital-Tosteson Fundfor Medical discovery. C. Lazaro was supported by Generalitat deCatalunya (2003BEAI4000094, 2004BE00368, 2005SGR00018) andby the Spanish Government (SAF2005-00833, SAF2006-05399,ISCIII C03/07).
References
1. Johnson JM, Castle J, Garrett-Engele P, Kan Z, Loerch PM,Armour CD, Santos R, Schadt EE, Stoughton R, Shoemaker DD(2003) Genome-wide survey of human alternative pre-mRNAsplicing with exon junction microarrays. Science 302:2141–2144
2. Sorek R, Shamir R, Ast G (2004) How prevalent is functionalalternative splicing in the human genome? Trends Genet 20:68–71
3. Modrek B, Resch A, Grasso C, Lee C (2001) Genome-widedetection of alternative splicing in expressed sequences of humangenes. Nucleic Acids Res 29:2850–2859
4. Faustino NA, Cooper TA (2003) Pre-mRNA splicing and humandisease. Genes Dev 17:419–437
5. Cartegni L, Chew SL, Krainer AR (2002) Listening to silence andunderstanding nonsense: exonic mutations that affect splicing. NatRev Genet 3:285–298
6. Svenson IK, Ashley-Koch AE, Gaskell PC, Riney TJ, CummingWJ, Kingston HM, Hogan EL, Boustany RM, Vance JM, NanceMA et al (2001) Identification and expression analysis of spastingene mutations in hereditary spastic paraplegia. Am J Hum Genet68:1077–1085
7. Beck S, Penque D, Garcia S, Gomes A, Farinha C, Mata L,Gulbenkian S, Gil-Ferreira K, Duarte A, Pacheco P et al (1999)Cystic fibrosis patients with the 3272-26A->G mutation have milddisease, leaky alternative mRNA splicing, and CFTR protein atthe cell membrane. Hum Mutat 14:133–144
8. Nissim-Rafinia M, Kerem B (2005) The splicing machinery is agenetic modifier of disease severity. Trends Genet 21:480–483
9. Moller LB, Tumer Z, Lund C, Petersen C, Cole T, Hanusch R, SeidelJ, Jensen LR, Horn N (2000) Similar splice-site mutations of theATP7A gene lead to different phenotypes: classical Menkes diseaseor occipital horn syndrome. Am J Hum Genet 66:1211–1220
10. Garcia-Blanco MA (2003) Mending the message. Nat Biotechnol21:1448–1449
11. Garcia-Blanco MA, Baraniak AP, Lasda EL (2004) Alternativesplicing in disease and therapy. Nat Biotechnol 22:535–546
12. Yeo GW (2005) Splicing regulators: targets and drugs. GenomeBiol 6:240
13. Pearson J (1979) Familial dysautonomia (a brief review). J AutonNerv Syst 1:119–126
14. Axelrod FB (1995) Familial Dysautonomia. Harwood Academic,Luxembourg
15. Lehavi O, Aizenstein O, Bercovich D, Pavzner D, Shomrat R, Orr-Urtreger A, Yaron Y (2003) Screening for familial dysautonomia inIsrael: evidence for higher carrier rate among Polish Ashkenazi Jews.Genet Test 7:139–142
16. Maayan C, Kaplan E, Shachar S, Peleg O, Godfrey S (1987)Incidence of familial dysautonomia in Israel 1977–1981. ClinGenet 32:106–108
17. Anderson SL, Coli R, Daly IW, Kichula EA, Rork MJ, Volpi SA,Ekstein J, Rubin BY (2001) Familial dysautonomia is caused bymutations of the IKAP gene. Am J Hum Genet 68:753–758
18. Leyne M, Mull J, Gill SP, Cuajungco MP, Oddoux C, BlumenfeldA, Maayan C, Gusella JF, Axelrod FB, Slaugenhaupt SA (2003)Identification of the first non-Jewish mutation in familialdysautonomia. Am J Med Genet A 118:305–308
19. Slaugenhaupt SA, Blumenfeld A, Gill SP, Leyne M, Mull J,Cuajungco MP, Liebert CB, Chadwick B, Idelson M, Reznik L etal (2001) Tissue-specific expression of a splicing mutation in theIKBKAP gene causes familial dysautonomia. Am J Hum Genet68:598–605
20. Cuajungco MP, Leyne M, Mull J, Gill SP, Lu W, Zagzag D,Axelrod FB, Maayan C, Gusella JF, Slaugenhaupt SA (2003)Tissue-specific reduction in splicing efficiency of IKBKAP due tothe major mutation associated with familial dysautonomia. Am JHum Genet 72:749–758
21. Byers PH (2002) Killing the messenger: new insights intononsense-mediated mRNA decay. J Clin Invest 109:3–6
22. Slaugenhaupt SA, Mull J, Leyne M, Cuajungco MP, Gill SP, HimsMM, Quintero F, Axelrod FB, Gusella JF (2004) Rescue of ahuman mRNA splicing defect by the plant cytokinin kinetin. HumMol Genet 13:429–436
23. Close P, Hawkes N, Cornez I, Creppe C, Lambert CA, Rogister B,Siebenlist U, Merville MP, Slaugenhaupt SA, Bours V et al (2006)Transcription impairment and cell migration defects in elongator-depleted cells: implication for familial dysautonomia. Mol Cell22:521–531
24. Ibrahim EC, Hims MM, Shomron N, Burge CB, SlaugenhauptSA, Reed R (2006) Weak definition of IKBKAP exon 20 leads
160 J Mol Med (2007) 85:149–161

to aberrant splicing in familial dysautonomia. Hum Mutat 2006Sep 8 [Epub ahead of print]
25. Cohen L, Henzel WJ, Baeuerle PA (1998) IKAP is a scaffoldprotein of the IkappaB kinase complex. Nature 395:292–296
26. Krappmann D, Hatada EN, Tegethoff S, Li J, Klippel A, Giese K,Baeuerle PA, Scheidereit C (2000) The I kappa B kinase (IKK)complex is tripartite and contains IKK gamma but not IKAP as aregular component. J Biol Chem 275:29779–29787
27. Hawkes NA, Otero G, Winkler GS, Marshall N, Dahmus ME,Krappmann D, Scheidereit C, Thomas CL, Schiavo G,Erdjument-Bromage H et al (2002) Purification and character-ization of the human elongator complex. J Biol Chem277:3047–3052
28. Jablonowski D, Zink S, Mehlgarten C, Daum G, Schaffrath R(2006) tRNAGlu wobble uridine methylation by Trm9 identifiesElongator’s key role for zymocin-induced cell death in yeast. MolMicrobiol 59:677–688
29. Rahl PB, Chen CZ, Collins RN (2005) Elp1p, the yeast homologof the FD disease syndrome protein, negatively regulatesexocytosis independently of transcriptional elongation. Mol Cell17:841–853
30. Holmberg C, Katz S, Lerdrup M, Herdegen T, Jaattela M,Aronheim A, Kallunki T (2002) A novel specific role for I-kappaB kinase complex-associated protein in cytosolic stress signaling.J Biol Chem 10:10
31. Heemskerk J, Tobin AJ, Bain LJ (2002) Teaching old drugs newtricks. Meeting of the Neurodegeneration Drug Screening Con-sortium, 7–8 April 2002, Washington, DC, USA. Trends Neurosci25:494–496
32. Blumenfeld A, Slaugenhaupt SA, Axelrod FB, Lucente DE,Maayan C, Liebert CB, Ozelius LJ, Trofatter JA, Haines JL,Breakefield XO et al (1993) Localization of the gene for familialdysautonomia on chromosome 9 and definition of DNA markersfor genetic diagnosis. Nat Genet 4:160–164
33. Sorek R, Shemesh R, Cohen Y, Basechess O, Ast G, Shamir R(2004) A non-EST-based method for exon-skipping prediction.Genome Res 14:1617–1623
34. Lambert J, Naeyaert JM, Callens T, De Paepe A, Messiaen L(1998) Human myosin V gene produces different transcripts in acell type-specific manner. Biochem Biophys Res Commun252:329–333
35. Glatz DC, Rujescu D, Tang Y, Berendt FJ, Hartmann AM, FaltracoF, Rosenberg C, Hulette C, Jellinger K, Hampel H et al (2006) Thealternative splicing of tau exon 10 and its regulatory proteins CLK2and TRA2-BETA1 changes in sporadic Alzheimer’s disease.J Neurochem 96:635–644
36. Coulter LR, Landree MA, Cooper TA (1997) Identification of anew class of exonic splicing enhancers by in vivo selection. MolCell Biol 17:2143–2150
37. Fairbrother WG, Yeh RF, Sharp PA, Burge CB (2002) Predictiveidentification of exonic splicing enhancers in human genes.Science 297:1007–1013
38. Dominski Z, Kole R (1991) Selection of splice sites in pre-mRNAs with short internal exons. Mol Cell Biol 11:6075–6083
39. Xu R, Teng J, Cooper TA (1993) The cardiac troponin Talternative exon contains a novel purine-rich positive splicingelement. Mol Cell Biol 13:3660–3674
40. Messiaen LM, Callens T, Mortier G, Beysen D, Vandenbroucke I, VanRoy N, Speleman F, Paepe AD (2000) Exhaustive mutation analysis ofthe NF1 gene allows identification of 95% of mutations and reveals ahigh frequency of unusual splicing defects. Hum Mutat 15:541–555
41. Ars E, Serra E, Garcia J, Kruyer H, Gaona A, Lazaro C, Estivill X(2000) Mutations affecting mRNA splicing are the most commonmolecular defects in patients with neurofibromatosis type 1. HumMol Genet 9:237–247
42. Ars E, Kruyer H,Morell M, Pros E, Serra E, Ravella A, Estivill X andLazaro C (2003) Recurrent mutations in the NF1 gene are commonamong neurofibromatosis type 1 patients. J Med Genet 40:e82
43. Rattan SI, Clark BF (1994) Kinetin delays the onset of ageingcharacteristics in human fibroblasts. Biochem Biophys ResCommun 201:665–672
44. Olsen A, Siboska GE, Clark BF, Rattan SI (1999) N(6)-Furfuryla-denine, kinetin, protects against Fenton reaction-mediated oxidativedamage to DNA. Biochem Biophys Res Commun 265:499–502
45. Verbeke P, Siboska GE, Clark BF, Rattan SI (2000) Kinetininhibits protein oxidation and glycoxidation in vitro. BiochemBiophys Res Commun 276:1265–1270
46. McCullough JK (2002) Clinical study of safety and efficacy ofusing topical kinetin 0.1% (Kinerase) to treat photodamaged skin.Cosmet Dermatol 15:29
47. Holste D, Huo G, Tung V, Burge CB (2006) HOLLYWOOD: acomparative relational database of alternative splicing. NucleicAcids Res 34:D56–D62
48. Soret J, Bakkour N, Maire S, Durand S, Zekri L, Gabut M, Fic W,Divita G, Rivalle C, Dauzonne D et al (2005) Selectivemodification of alternative splicing by indole derivatives thattarget serine–arginine-rich protein splicing factors. Proc NatlAcad Sci U S A 102:8764–8769
49. Singh R, Valcarcel J (2005) Building specificity with nonspecificRNA-binding proteins. Nat Struct Mol Biol 12:645–653
50. Carmel I, Tal S, Vig I, Ast G (2004) Comparative analysis detectsdependencies among the 5′ splice-site positions. RNA 10:828–840
J Mol Med (2007) 85:149–161 161


















