Therapeutic Hypothermia ChillOut
38
Therapeutic Therapeutic Hypothermia Hypothermia Post Cardiac Post Cardiac Arrest Arrest Prepared and Presented by: Prepared and Presented by: Cameron Schmidt MS RN Cameron Schmidt MS RN Clinical Teacher Clinical Teacher Critical Care Education Critical Care Education
-
Upload
ryanfromhamilton -
Category
Documents
-
view
109 -
download
2
description
Good presentation on Therapeutic Hypothermia
Transcript of Therapeutic Hypothermia ChillOut

Therapeutic Therapeutic HypothermiaHypothermia Post Cardiac Post Cardiac
ArrestArrestPrepared and Presented by: Prepared and Presented by:
Cameron Schmidt MS RNCameron Schmidt MS RNClinical TeacherClinical Teacher
Critical Care EducationCritical Care Education

IntroductionIntroduction• Clinically induced hypothermia is an
evidence based intervention strategy that can improve the neurologic outcome of unconscious patients post sudden cardiac arrest

IntroductionIntroduction• Brain temperature during the first 24
hours after resuscitation from Cardiac Arrest may have significant effect on survival and neurologic recovery

GoalsGoals• The goal is to obtain a core temperature of
32-34 degrees C. Our Goal:33 degrees C (91.4 F) within 6 hours of the onset of cardiac arrest and to maintain core temperature of 32-34 degrees C for 24 hours, as this may decrease chances of death and increase chance of neurologic recovery

• Mild to moderate states of Hypothermia have been found to have a neuroprotective mechanism within the brain that can improve a patients outcome S/P Cardiac arrest

• Therapeutic Hypothermia provides several brain preserving effects, however it also has associated complications that require attentive Nursing Care and Interventions to prevent complications from therapy.

Pathophysiology and Pathophysiology and Adverse EffectsAdverse Effects
• Cardiac Arrest• Decreased perfusion (BP)• Decreased Cerebral Oxygen delivery
(causing neurological deficit)• Cerebral Hypoxia• Cerebral Edema• Ischemia (Brain releases enzymes and
experience intracellular ion changes that damage cellular mitochondria)

Pathophysiology Con’tPathophysiology Con’t• APOPTOSIS (pre-programmed cellular
death)• Anaerobic Metabolism occurs• Increased Calcium• Increased hyper excitability in the brain
cells• Exacerbation of Hypoxemic state• Cellular Death• Increased Cerebral edema

Pathophysiology Con’tPathophysiology Con’t• Blood Brain Barrier is Disrupted
during low perfusion states• Influx of fluid• Worsening of Cerebral Edema

• Hypothermia slows neuroexcitory processes, stabilizing the influx of Ca, limiting cellular death and reducing disruption in the blood Brain Barrier therefore decreasing cerebral edema

• Apoptosis can last up to 48 hours after initial insult, which may explain why Therapeutic hypothermia is Neuroprotective.

• Cooling patients limits the negative effects from hypoxemia
• Inducing mild hypothermia slows cerebral metabolism, decreasing Cerebral metabolic rate by 5-7%(20-28% reduction in cerebral metabolism when pt is cooled to 33C) for each degree Centigrade reduction in body temperature

Other PathophysiologyOther Pathophysiology• Therapeutic hypothermia suppresses
ischemia induced inflammatory reactions
• Neutrophil and macrophage function decrease at temperature <35 degrees C
• Therefore…. Decreased Cerebral edema.

Complications/Adverse Complications/Adverse EffectsEffects
• There is a risk of infection due to changes in WBC function
• Mild Hypothermia induces insulin resistance and hyperglycemia results which increases risk of infection (Pulmonary and wound infections are the most common)– VAP oral care will be implemented

Complications Con’tComplications Con’t
• Mild hypothermia causes mild bleeding from platelet dysfunction, may cause mild coagulopathies.
• Lab analysis of coagulation studies may not accurately report alterations in function because tests are usually performed on patients with body temps of 37 C therefore…..– Nurses must observe for alterations in
coagulation (delayed clotting)

ComplicationsComplications• Fluid and Electrolyte shifts occur during
induction of hypothermia• Mild Diuresis can occur with initiation of
cooling– U/O replacement will be ordered on admission.
Type and amount will be individualized on the order form
• Hypothermia decreases Cardiac Output by 25% causing mild acidosis and increased serum lactate levels.– Lactate levels are drawn on admission and will
be ordered prn.

ComplicationsComplications• Electrolytes shift because of changes
in cellular membranes with ischemia and states of cellular acidosis (decreased MG, K, Ca… Mg is Neuroprotective)– Labs will be drawn Q6hoursx24H– (BMP,PT/PTT, CA, Mg, Po4, CBC diff)

ShiveringShivering• The body’s natural response to cold• The goal of cooling is to decrease
VO2 therefore prevention of shivering is essential
• Use sedatives and NMBA’s– These will be ordered on the pre-printed
order form

ShiveringShivering
• Use shivering Scale• Shivering Increase VO2 40-100%• Early signs of shivering:
– Decreased SVO2– Increased RR– Facial Tensing– “Noise” on EKG– Palpation of muscle fasculations of face or
chest– Treat with sedatives and NMBA’s

Shivering ScaleShivering Scale
• 0- No Shivering• 1- One or more of the following
– Piloerection– Peripheral vasoconstriction– Peripheral cyanosis without other causes, but with
visible muscular activity2- Visible muscular activity confined to 1 muscle group3- Visible muscular activity confined to 2 muscle groups4- Gross Muscular activity involving the entire bodyIf score is >2 for >5 minutes….Notify MD

Nursing Care of the Nursing Care of the Hypothermic PatientHypothermic Patient
• RN’s must provide vigilant surveillance over the patients changing physical condition

Nursing Care Con’tNursing Care Con’t• The RN’s knowledge of Pathophysiology
will require assessment of the following:– Prevention of rewarming during the cooling
phase– Electrolyte imbalances– Arrhythmia recognition– Prevention of infection– Skin Care– Pain/ Sedation management

• Prior to initiating hypothermia:– Perform a complete skin assessment– Assess response to pain– Perform baseline Neurological exam:
This is essential to allow for comparison after therapies, as well as some patients wakeup prior to cooling thus Therapeutic Hypothermia would not be an option

• Once target temperature is reached, temperature needs to be maintained within target range (32-34 degrees C)
• Temperature must be constantly monitored.– Gaymar Mediterm III does this for you.– It becomes a big thermometer!!
• Ensure cool air is not lost when performing nursing functions that may require removal of garments(this should be avoided at all cost)
• Must remove ice packs so temperature does not fall below 33c (20-25 minutes of application according to ECMC orders)
• Excessive cooling or overshooting the target temperature(<33C) puts the patient at risk for Moderate Hypothermia with significant complications– Gaymar Mediterm III when set, will maintain set point temp

SedationSedation• Monitor for effective analgesia and
sedation without oversedating ( Pain Scale, SAS Scale)
• This maximizes patient comfort• Benzodiazepines are effective sedative
agents and inhibit neurotransmitters on the brain and decrease cerebral VO2– Lorazepam or midazolam drips
• Propofol

PainPain• Fentanyl and Morphine are preferred

Train of Four (TOF)Train of Four (TOF)• Must be established before initiating NMBA
therapy• Due to Peripheral Vasoconstriction during
hypothermia, it may be difficult for ongoing TOF monitoring– If this occurs titrate NMB to prevent shivering
• Hypothermia changes drug metabolism and pharmacokinetics
• Dosing of sedation, pain and NMBA’s may need to be decreased
• DC NMBA’s at the beginning of rewarming

Cardiac ComplicationsCardiac Complications• As temperature decreases, CO and
SV decrease. SVR and BP increase in response to vasoconstriction
• Sinus Bradycardia is a common finding with cooling related to hypothermic myocardial depression.
• It is refractory to Atropine• Risk of Dysrhythmias during
MODERATE cooling is higher (<32C)

Cardiac Complications Con’tCardiac Complications Con’t• Skin will be pale and Pedal Pulses are often
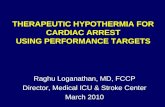
difficult to assess• Osborne waves are seen in lateral precordial
waves (V5, V6)• Osborne Wave- a positive deflection notch on the
down stroke of the QRS complex(at the junction between the QRS complex and the ST segment)
• Occurs due to delayed closing of the transient outward K current channels
• Not unique only to hypothermia, can also be seen with autonomic dysreflexia, hypercalcemia and cerebral injury

Osborne WaveOsborne Wave

Additional Cardiac ChangesAdditional Cardiac Changes• Wide QRS• ST elevations or depressions• T wave inversion• QT prolongation
• These are caused by ischemia or acidosis and can occur for days after rewarming

HyperglycemiaHyperglycemia• Due to insulin resistance• Associated with increased infection• Associated with increased incidence
of Renal failure• Insulin requirements are higher than
normal to maintain normal glucose levels.– Sliding Insulin scale will be ordered

ElectrolytesElectrolytes
• Alterations are due to extracellular ion shifts
• Fluxuations in K, Mg, Ca occur• Mg levels are treated to maintain normal
to high levels due to its role mitigating neurological injuries– If Mg <1.7, MD may order 2 grams Magnesium
Sulfate• K levels will drop during cooling and rise
during rewarming– K will not be replaced unless K is <3 during the
cooling phase

Immune Immune Response/HematologicResponse/Hematologic
• WBC decrease blood cultures may be ordered• Cooling masks normal response to fever• Platelets decrease
– MD may order platelets if platelets <30,000– MD may order FFP (Vitamin K if on Coumadin) to correct
INR>2
• Hemoconcentration occurs due to loss of plasma through changes in vascular permeability and cold Diuresis
• For every 1 C decrease in temperature, the HCT increases by about 2%.– MD may order PRC’s if hemoglobin is<10

RenalRenal• Cold induced Diuresis due to decreased
reabsorbtion of solute in the loop of henle• Resistance to ADH• If CO decreases too drastically, GFR will
decrease.– If GFR decreased<30 ml/min Cisatricurium will
be used as the NMB agent and Famotidine will be given Q24h instead of Q 12h

ConclusionConclusion• Hypothermia is evidenced-based practice proven
to improve neurological outcomes of some unconscious cardiac arrest patients.
• Early interventions with hypothermic therapy offers a realistic approach to preventing severe neurological deficits post cardiac arrest.
• Critical Care and ED nurses that are knowledgeable in the management of patients during clinically induced hypothermia therapy can positively impact patient care and prevent adverse neurologic complications from sudden cardiac arrest, as well as prevent complications associated with this therapy.