Theory and Method to Enhance Computer-Integrated Surgical Systems
16
Theory and Method to Enhance Computer-Integrated Surgical Systems Tam ´ as Haidegger Department of Control Engineering and Information Technology, Laboratory of Biomedical Engineering Budapest University of Technology and Economics Ph.D. Thesis Booklet Supervisor: Prof. Zolt´ an Beny´ o (BME – IIT) Advisors: Prof. J´ ozsef S´ andor (Semmelweis University) Prof. Imre Rudas ( ´ Obuda University) Budapest, 2011
Transcript of Theory and Method to Enhance Computer-Integrated Surgical Systems

Theory and Method to EnhanceComputer-Integrated Surgical Systems
Tamas Haidegger
Department of Control Engineering and Information Technology,Laboratory of Biomedical Engineering
Budapest University of Technology and Economics
Ph.D. Thesis Booklet
Supervisor: Prof. Zoltan Benyo (BME – IIT)Advisors: Prof. Jozsef Sandor (Semmelweis University)
Prof. Imre Rudas (Obuda University)
Budapest, 2011

2
I. THE EMERGING FIELD OF COMPUTER-INTEGRATED SURGERY
Computer-Integrated Surgery (CIS) is the most commonly used term to cover the emergingfield of interventional technologies in medicine, from image processing and augmentedreality applications to automated tissue ablation. CIS also incorporates surgical CAD/CAM(Computer Aided Design and Manufacturing)—analogous to industrial CAD/CAM—wheredigital information is used to create accurate patient models and surgical plans, whiletechnology also improves treatment delivery.
Robotic surgery is defined as “a surgical procedure or technology that adds a computer-technology-enhanced device to the interaction between the surgeon and the patient duringa surgical operation, and assumes some degree of freedom of control heretofore completelyreserved for the surgeon” [1].
Minimally Invasive Surgery (MIS) originally referred to laparoscopic procedures (keyholesurgery), where the abdominal cavity is accessed through 3–5 small incisions (0.5–3 cmin size). Today, it is generic term for the alternatives to open procedures reducing patienttrauma and operation risk. On the other hand, MIS requires a highly skilled surgeon witha significant amount of practice [2]. Robot-assisted MIS is often used to characterize thecomplete teleoperated systems, where the robot basically serves as a replacement of thehuman operator’s hand by manipulating endoscopic tools.
Telesurgery (also referred to as remote surgery or telepresence surgery) enables physiciansto invasively treat patients spatially separated from themselves. Unlimited bandwith andreal-time remote access to the medical site means that the surgeon is actually capable ofperforming operations through robots and other teleoperated devices. When the communi-cation link is not reliable enough or the technical tools are not given, a remote surgeoncan direct the local one based on semi-real-time (slightly delayed) video and voice feedfrom the Operating Room (OR). This technique is called telementoring (also referred toas teleproctoring), which is the spatial extension of classical mentoring and professionalguiding—the monitoring and evaluation of surgical trainees from a distance. When lowcommunication quality or latency does not even allow semi-real-time connection, consultancytelemedicine (or telehealth consultancy) can still be used. It only requires limited bandwidthaccess to the remote site, however, as a consequence, the distant group cannot use real-timeservices or information updates. Virtual presence and remote delivery of services has greatscientific and commercial potential in health care.
Image-Guided Surgery (IGS) means the accurate correlation and mapping of the operativefield to a pre-operative image or intra-operative (e.g., ultrasound, fluoroscopy) data set ofthe patient, providing freehand navigation, positioning accuracy of equipment or guidancefor mechatronic systems [3]. IGS has been primarily used in neurosurgery, pediatrics, ortho-pedics and also had a major impact in ear, nose, throat and maxio-facillary reconstructionsurgery.
Registration is a key element of medical imaging and robotics, it means the spatialalignment of different modalities to determine the position and orientation of the patient inthe operating field relative to a virtual data set of the anatomy, e.g., a pre-operative image.The registration should provide a homogeneous transformation (or similar representation)that allows the conversion of locations and control signals between different devices, i.e.,mapping between the control frames [4].
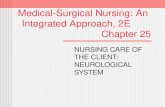
A generic robot-integrated IGS system’s schematic diagram is shown in Fig. 1, where thenodes represent control frames and the lines mean homogeneous transformations connectingthose. The navigation system (e.g., a camera) is able to track at least two markers. First,

3
Fig. 1. General control concept of image-guided robotic systems. The nodes represent control frames and the solid linesare homogeneous transformations.
the position of the Dynamic Reference Base (DRB), (i.e., a fiducial anchored to the patient)and second, the Tool Rigid Body (TRB). The navigation system is also used to register thepre-operative image of the patient to the DRB with the help of e.g., a hand-held probe andskin-mounted fiducials. Then the surgical plan can be mapped from the pre-operative imagespace to the robot coordinates through the chain of homogeneous transformations.
In the terms of accurate treatment delivery, it is most important to get a precise andrealistic transformation between the patient anatomy and the robot end effector. While theabove described registration and calibration procedures could theoretically allow for a perfectmapping, in reality, several issues arise, such as the finite accuracy of the fitting algorithms,communication latencies, the limited computational resources available and above all, thechanging medical environment, most often referred to as patient motion.
A. Surgical robotic conceptsRobots can be involved in medical procedures with various level of autonomy [5]. Some
of them serve as a robust tool holding equipment once directed to the desired position,while others are able to perform fully automated procedures, such as CT-based biopsy orbone cutting. The later ones are called autonomous or supervisory controlled devices, as ahuman supervisor would always be present to intervene if deviations from the surgical planare noticed. This can be combined with the classic tools of IGS, when the surgeons areonly using the images to gain additional information to better position their tools. Whenthe planning is completed, the physicians have to match the robot’s coordinates with thepatient’s anatomical points, registering the physical space to the robot’s working frame. Onceappropriately registered, the robot can autonomously perform the desired task by exactlyfollowing the pre-programmed plan.
On the other hand, if the robot is entirely teleoperated or remote-controlled (robotictelesurgery system) the surgeon is absolutely in charge of its motion. These complex systems(such as the da Vinci) consist of three parts: one or more slave manipulators, a mastercontroller and a vision system providing feedback to the user. Based on the gathered visual

4
(and sometimes haptic) information, the surgeon guides the arm by moving the controllerand closely watching its effect. In most of the cases, mechatronic systems and cameras arethe remote hands and eyes of the surgeon, and therefore key elements of the operation.
Modifying the teleoperation control paradigm we can introduce cooperative control (alsocalled shared control or hands-on surgery). It means that the surgeon is directly giving thecontrol signals to the machine through a force sensor. It is possible to read and process thesesignals in real-time to create the robot’s motion. The human is always in contact with therobot, as the master and the slave devices are physically identical. In this case, the robotis the extension of the doctor’s hand, equipped with special features and effectors. Thisapproach keeps the human in the control loop, and still allows the surgeons to use theirsenses throughout the procedure. It is often employed in the case of micro-manipulationoperations, such as vascular, urologic, eye or brain operations.
B. Advantages of surgical robotsRobot-assisted procedures offer remarkable advantages both for the patients and the
physicians [6]. The main features of robotic surgery systems are the following:• superior 3D spatial accuracy provided by the robot,• stabilization of the instruments within the surgical field,• improvement of manual dexterity, motion scaling,• physiological tremor filtering,• integrated 3D vision system with high resolution,• specific design for maximum performance (including miniature robots),• advanced ergonomics supporting long procedures,• high-fidelity information integration,• stable performance,• invulnerability to environmental hazards,• patient advantages (reduced blood loss, less trauma, shorter recovery time),• decreased costs (per treatment) due to shorter hospitalization,• possibility to provide better and more realistic training to physicians.
C. Further improvements for CISDespite their success in various applications, there are some concerns that prevent CIS
technologies from becoming omnipresent in health care. While there is a clear need foraccuracy and robust operation for many procedures, the associated high expenses are notwelcomed. Technology can only conquer the OR gradually, as it takes a long time and asignificant amount of training to change the way procedures are performed. Many surgeonsare reluctant to use novel devices or protocols that they do not completely understand orcontrol.
Image guidance at the same time is a steadily emerging field; physicians recognize thevalue of better imaging, more precise tools and smarter devices. Currently, the leadingdirection of development is to provide incremental updates to existing protocols and in-struments. This means the enhancements of already deployed navigation devices, bettersimulation, accurate modeling, information coupling and error-resistant control. The workingenvironment of a surgical robot is not entirely predictable and cannot be modeled completely,therefore complete automation of the procedures is extremely hard. Safety concerns delayedor prevented the approval of many automated interventional systems, and streamed the

5
Fig. 2. The NeuroMate-based IGS system at the Johns Hopkins University. (a) The NeuroMate robot in action: bonecutting on the skull base in a cadaver experiment at Johns Hopkins Medical Institute. (b) The integrated robotic systemmoved to the R. A. Swirnow Mock Operating Room at JHU.
research community towards human-integrated control solutions, such as telesurgery andhands-on surgery. Cooperative control is a promising way to provide highly integrated roboticsupport for procedures while applying all the necessary safety standards. It is believed thatthis method provides the highest effectiveness according to the criteria hierarchy for surgicalrobots [7].
D. The JHU image-guided neurosurgical systemI was given the unique chance to be involved in a neurosurgical project as a visiting scholar
at the Center for Computer-Integrated Surgical Systems and Technology (CISST ERC), JohnsHopkins University (JHU, Baltimore, MD) in 2007/08. We have developed an integratedsurgical robotic system to support skull base drilling. The system consists of a modifiedNeuroMate robot (Integrated Surgical Systems Inc., Sacramento, CA; currently owned byRenishaw plc., Wotton-under-Edge, UK), a StealthStation (SS) surgical navigation device(Medtronic Navigation Inc., Louisville, CO) and adequate network and control equipment.The goal of the project was to improve the safety and quality of neurosurgery while reducingthe operating time. The robotized solution is only used for the removal of bone tissue, togain access to the anatomical region affected by a tumor or other lesions. Our technicalapproach was to rely on pre-operative imaging, allowing the medical professional to identifythe region of the skull base that could be safely drilled. We chose a cooperative controlimplementation, in which the surgeon applies forces to move the robot and the robot enforcessafety boundaries [8].
The JHU system has three major advantages. First, it offers advanced visualization featurestypical used in stereotactic surgery; the tool’s position can be followed on the 3D model ofthe patient, acquired from pre-operative CT scans. Second, the surgical tool is mounted onthe rigid robot, thereby improving its stability. The surgeons still hold the classic drill anddirects its movement, but they can release the tool any time. Finally, the most importantadvantage—and the novelty of the application—is that the physicians can define virtualboundaries on the patient’s model prior to the operation. This spatial constraint is calledVirtual Fixture (VF), and once registered to the robot, it is strictly enforced, thus preventingthe tip of the tool from going beyond the defined safe area. These features together can

6
greatly increase the safety and the reliability of the procedure, facilitate task execution andpotentially reduce operating time.
The JHU setup was an excellent platform to prototype and test my results, and to performrealistic simulations along with phantom and cadaver trials to acquire relevant data.
II. METHODS OF THE RESERACH
The goal of my research was to create new methods and algorithms to support image-guided systems, to increase their accuracy and safety with intra-operative tracking, developerror reduction and advanced control. Three specific areas have been targeted for improve-ment, each addressed with a research project.
Within the areas of my work, I conducted profound literature review to assess the state ofthe art, and the results are thoroughly reported in my Thesis, incorporating over 280 refer-ences. Next, long discussions and planning phase proceeded, followed by the invention, im-plementation and verification of new models. Classical mathematical apparatus was deployedincluding linear algebra, statistics and classical control theory. New ideas were prototypedand tested on a physical setup and in a simulation environment under MATLAB (MathworksInc., Natick, MA). Extensive data collection was performed to acquire relevant input data setfor the algorithms. Further, the results connected to patient motion compensation and errormodeling in integrated IGS systems were verified on the JHU system through laboratorytrials and tests on actual data derived from the neurosurgical robot. Telesurgery controlexperiments were simulated based on previously verified models and properly identifiedsystem parameters.
III. RESEARCH PROBLEM STATEMENT
There is a clear trend in medicine to shift towards less invasive treatment solutions. Inthe case of robot-assisted IGS or radiation therapy, accuracy is paramount, therefore precisepositioning of the surgical tools is required. Typical practice is the rigid and invasive fixationof the patient, and the employment of additional hardware to ensure safety. Beyond theinherent precision of the system components, accuracy of treatment delivery can also beaffected by the many changing factors in the OR. There are several people in the roommoving around the numerous medical devices surrounding the patient. Further problemsarise with teleoperation. Long distance telesurgical applications require adequate controlalgorithms to support the operator and to handle latency. Effective emergency medical carein space requires additional considerations and innovative solutions.
Three specific problem descriptions have been formulated and grouped around outstandingchallenges in the field of CIS.
Problem 1: Patient motion in the Operating Room
There is an urgent clinical need to improve treatment delivery precision and to reduceinvasiveness solely relying on the existing hardware in the OR, as further costs and complex-ity should be avoided. Integrated IGS systems must provide increased safety and accuracyfeatures.
Image-guided surgery requires trackable markers used as references (or perfect immobi-lization of the body), as it is based on the principle that the real-world setup does not changeunpredictably over time; therefore the registration to the pre-operative image space remains

7
valid. IGS is sensitive to spatial changes, when the patient is unintentionally moved relativeto the marker that tracks their motion. The event of external patient motion occurs whenthe body’s position moves relative to the base frame of the device executing the surgicalplan. (Physiological tissue motion is not addressed here, as its tracking requires differenttechniques and methods.) The fundamental problem with patient motion is that withoutproper identification and compensation, the whole surgical plan may become obsolete, andthe treatment potentially harmful. From the clinical point of view, a few millimeters oferror could be tolerated at the most. Depending on the speed of the tool, this translatesto a maximum of a second of latency. If it is noticed in time, re-registration is demandedto avoid damaging the patient. However, re-registration is usually time consuming, thusit should be avoided, whenever possible. From the technical point of view, many sourcesof errors can be handled as patient motion, having the same degrading effect on performance.
Problem 2: Inadequate modeling of system error propagation
On the way towards having more robotic technology involved in the OR, a major problemis the proper modeling of system noises and their propagation. Even a semi-autonomouslyguided machine with a misaligned image-overlay can become the source of malpractice.Effective mapping of spatial error based on a priori information is necessary to supportthe operation of integrated medical tools. Currently, the experience of the medical staffdetermines the use of a system under different conditions, and typically generalized errorvalues are applied. As a consequence, worst case safety margins have to be applied all alongthe procedure, while more thorough analysis of the distribution of spatial error would allowfor optimized approach, leading to better treatment delivery and faster execution.
Surgical procedures and integrated medical devices relying on patient-imaging shouldprovide a clear indication of the system’s error at the Point of Interest (POI) and theexpectable distribution of it (point spread function). Widely accepted metrics should beapplied to make systems comparable. Deterministic spatial accuracy analysis of imageregistration and surgical robot systems was performed by many research groups [9, 10,11]. However, stochastic analysis has mostly been avoided due to the fact that it is compu-tationally demanding and can lead to extremely complex solutions [12]. Without effectiveand easy means of assessment, it is utterly difficult to verify IGS systems’ accuracy. Eventoday, the most successful surgical robot system (the da Vinci) relies on the direct controlof the surgeon. The human-in-the-loop control strategy allows for more flexible (and lessautonomous) hardware solutions, where the surgeon is entirely responsible for patient safety.It is believed that development is towards improved machine intelligence and automation,and as a major step forward, the inherent precision of future systems has to be improved.
Most of the previous methods developed for error assessment do not deal with theorientation error at a target, and do not provide any information about the error distributioneither. Originally, the concept of coordinate frame registration handled accuracy as a norm ofthe deviation in x, y, z from the target point—entirely disregarding the orientation uncertainty.In several applications, such as an IG interventional robot employing a Virtual Fixture, it iscritical to consider angular errors.
Problem 3: Difficulty of telesurgery over large distances
While pilot experiments have been conducted for long distance telesurgery around theglobe and between continents, regularly performed remote operations have many practical

8
obstacles and limitations. Primarily, these systems need robust and stable controllers todeal with technological issues deriving from the latency in the communication, and also toincorporate an adequate model of human–machine teleoperation.
Space application of telerobotic surgery has been a major focus of the research communitysince the early days of the field. While advanced internet-based communication theoreticallyenables terrestrial telesurgery, serious technological problems arise in the case of longdistance operations or space exploration missions. These days, it seems inevitable to havea flight surgeon on board of a spacecraft for long duration missions, as robots do not haveenough autonomy to adapt to unpredictable events.
A realistic teleoperation system suffers from communication delays between the master(controller) and slave side (effector system). Unless the process is significantly slower thanthe latency, the control lag time can cause the deterioration of control quality, and instabilitycan occur due to unwanted power generation in the communications. Time-varying delayposes further difficulties to classical PID controllers, while model predictive control isextremely hard to apply due to the human operator’s complex behavior. Scalable empiricalmethods, such as Kessler’s Extended Symmetrical Optimum (ESO) method could providebetter solution to these problems [13].
Beyond these points, there are many other challenges within the field of CIS, and researchersare exerting a great effort to tackle these, resulting in the continuous flow of technicalbreakthroughs and theoretical achievements. The problems identified above summarize threeareas covering an important set of interconnected issues, and addresses scientific problemsrelevant to the clinical practice.
IV. NEW RESULTS
1. Thesis Group: Algorithm for Patient Motion Detection and CompensationI have developed a new tracking-based Minimally Invasive concept for patient motion com-pensation. It supports systems with a less rigid fixation setup or limited surgical navigationcapabilities.
Related publications: [HT-1, HT-2, HT-3, HT-4, HT-5, HT-6, HT-7, HT-8, HT-9, HT-10,HT-11, HT-12, HT-13].
1.1 Optimal determination of Surgical CasesI developed a general framework for patient motion tracking that is applicable to various
Image-Guided Surgery setups. I proposed a decision-tree based event recognition algorithmthat allows to choose the best control option for any pre-defined Surgical Case. IGS eventshave been categorized and defined as patient motion, camera motion, robot motion and thearbitrary combination of these. The control sequences can be transformed to any arbitraryframe to ensure safe operation even during patient motion. A measurement-based methodwas constructed to identify the actual Surgical Case, and to perform the desired action toenhance patient safety.
1.2 Extending window adaptive filteringI proposed extending window averaging to be applied to compensate for the inaccuracies
in the control frames and transformations of an integrated IGS system. This ensures more re-liable and accurate estimation of the surgical tool, thus increases the safety of the operation.

9
Discussion of the thesis: The new approach uses the intra-operative navigation devices’internal coordinate base frame to better estimate the possible changes in the environment.The base frame for the computations can be chosen arbitrarily as long as it is registeredto the robot frame (and possibly to other control frames, such as the navigation systems)through known homogeneous transformations. The advantage of the method is that it isscalable to fit various surgical setups without additional hardware requirements. The generalnomenclature and definitions of the subfield were founded.
2. Thesis Group: Probabilistic Method to Improve Accuracy in Computer-IntegratedSurgeryI developed a stochastic approach for the assessment of spatial errors of an integratedIGS system. It can determine the probability density function of the location of the Pointof Interest. By combining computation and simulation, the error distribution for a givensetup can be derived. Once the spatial constraints are set and transformed into the POI’scoordinate system, it is possible to derive the exact probability of the tool entering the VirtualFixture, or other safety boundaries.
Related publications: [HT-14, HT-15, HT-16].
2.1 Better expression of transformation errorsI demonstrated that since the overall homogenous transformation connecting the patient’s
space and the robot can be expressed as the function of the ideal and noise terms:PATPOIT = f (t)+ f (∆t), where t = [x, y, z, φ , θ , ψ], (1)
the probability P(POI /∈ VF) means that the POI is in the forbidden region can be analyti-cally calculated as:
P(POI /∈ VF) =∫
t/∈VF
f (t)dt. (2)
Then stochastic approach can be applied to determine the location of the tooltip. This is asimple and effective way to represent f (∆t), the error of the transformation.
2.2 Describing a scalable solution for enhanced safetyWith the help of differently chosen VF segments and w weighting factors, any complex
penalty function can be built and applied to the IGS system in real-time during the executionof an operation. Critical errors occurring with lower probability are considered in the form:
η = w1P(POI /∈ VF1)+w2P(POI /∈ VF2) , (3)
where w1 > w2, if VF1 is more limiting than VF2. This enables faster and safer task ex-ecution for any integrated systems using a pre-operative surgical plan combined with anintra-operative interventional tool.
2.3 Improving treatment delivery precision in the Operating RoomThe new approach allows for the a priori estimation of the POI’s distribution. Based
solely on the devices’ known intrinsic accuracy parameters and the registration (acquiredbefore the surgical procedure), proper error distribution estimation can be performed. Thissimulation leads to better approximation of the surgical tool’s position.

10
Discussion of the thesis: I formulated the general extension of Wiles’ approach [14], takinginto consideration rotational uncertainties as well. The angular error distribution can alsoprovide information about the probability that the POI is moving toward the VF, which is acrucial in the case of certain surgical tasks. The method does not overload current hardwaresetups computationally, as the most recent devices allow for the handling of these functions.It is able to manage a previously challenging case: critical errors with low probability, andthe method can be extended and arbitrarily scaled to incorporate more regions. The exactcalculation of the probability of the error gives a much stricter control over the motionof the tool, resulting in higher accuracy and safety. With known error distribution, it ispossible to determine which directions are more dangerous from the application point ofview. The robot can be allowed to move faster towards directions with lower error deviation.
3. Thesis Group: Control Method for Long Distance TelesurgeryI proposed a three-layered space mission architecture to achieve the highest degree ofperformance by combining robotic and human surgery. A suitable teleoperation controlarchitecture was defined, and its limitations presented. I proved the effectiveness of Kessler’sExtended Symmetrical Optimum method in telesurgical applications and drawn conclusionson the optimal parameters to be chosen.
Related publications: [HT-17, HT-18, HT-19, HT-20, HT-21, HT-22, HT-23, HT-24, HT-25,HT-26, HT-27, HT-28].
3.1 Framework to design controllers for telesurgeryI presented the limitations of different telemedicine technologies, and developed a concept
for the application of telesurgery, enabling the support of a future space exploration missions.It contains the simplified human and machine representations derived to accommodate longdistance telesurgical applications. I proposed a method of control that relies on the adaptiveand continuously updated modeling and identification of the communication system, and onempirical controller design.
3.2 Cascade control structure with empirical design methodI proposed a cascade control structure employing empirical controller design in both
loops to address the challenges of a system with large and probably varying latencies. Ifocused on Kessler’s Extended Symmetrical Optimum method and showed the feasibility touse it embedded in the broader domain of robotics. I demonstrated the capability of themethod to deal with latencies up to 2 seconds. Optimal β design parameter settings werederived based on the requirements and assumptions for an effective space telesurgery system.
Discussion of the thesis: Different telepresence technologies combined may provide thebest performance in space medicine. The effectiveness of real-time control strategies andcommunication techniques decreases significantly with the increase of latency. Consideringthe challenges, I defined the pre-control context for telesurgery, based on what an adequatecontrol method was formulated. I focused on classical control options to provide a simple,universal and scalable solution. The use of empirical design methods is justified with the needfor simple and quick algorithms in cases when model predictive control may be cumbersometo apply.

11
V. APPLICATION OF THE RESULTS
A. First Thesis GroupThe Surgical Case identification concept was tested on the neurosurgical robot system
developed at the Johns Hopkins University. The setup serves as a testbed for various tech-nologies that can be prototyped and tested under realistic circumstances. The patient motionalgorithm has the universality and applicability to be employed beyond laboratory conditions.One of the future target applications is patient immobilization at ion therapy, a solutionthat the Austrian Center for Medical Innovation and Technology (ACMIT) is investigating.Negotiations for future applications with Renishaw plc. (current developer and distributor ofthe NeuroMate robot) are also scheduled.
B. Second Thesis GroupThe proposed stochastic approach has several advantages, as it can be applied to IGS
systems during the setup phase to verify the performance of the devices in the actual ORarrangement. It could easily be incorporated into commercially available navigation systems,fitting into the surgical workflow. At the beginning of the procedure—when the devices areroughly positioned around the patient—simple readings of the actual position information canserve as the input for the simulation. The stochastic method provides the error distributionbased on the Monte Carlo simulation within a few seconds, and with that knowledge, thesurgeon may decide to re-arrange the setup or to proceed with the operation.
C. Third Thesis GroupThe simulation results derived for delayed teleoperation may help to better understand
human adaptation to visual feedback latency, and new experiments are proposed to beconducted on our laparoscopic training box setup for that purpose.
VI. GRANTS SUPPORTING THE PH.D. WORK
The research was partially supported by the National Office for Research and Technology(NKTH), Hungarian National Scientific Research Foundation grant OTKA T69055, OTKACK80316 and the U.S. NSF EEC 9731748 grants. I am thankful for the generous scholarshipof the Hungarian–American Enterprise Scholarship Fund (HAESF) that made it possible tospend two semesters in the United States and to join the CISST ERC at the Johns HopkinsUniversity.

12
VII. REFERENCES
[1] D. M. Herron, M. Marohn and the SAGES–MIRA Robotic Surgery Consensus Group,“A consensus document on robotic surgery,” Surgical Endoscopy, vol. 22, no. 2, pp.313–325, 2007.
[2] J. Sandor, B. Lengyel, T. Haidegger, Gy. Saftics, G. Papp, A. Nagy and Gy. Weber,“Minimally invasive surgical technologies: Challenges in education and training,” AsianJ. of Endoscopic Surgery, vol. 3, no. 3, pp. 101–108, 2010.
[3] K. H. Wong, “Imaging Modalities,” in Lecture Notes in Computer Science (LNCS),Proc. of the 1st Intl. Conf. on Information Processing in Computer-Assisted Interven-tions (IPCAI), Geneva, 2010, pp. 241–273.
[4] J. Maintz and M. Viergever, “A survey of medical image registration,” Medical ImageAnalysis, vol. 2, no. 1, pp. 1–37, 1998.
[5] N. Nathoo, M. C. Cavusoglu, M. A. Vogelbaum and G. H. Barnett, “In Touch withRobotics: Neurosurgery for the Future,” Neurosurgery, vol. 56, no. 3, pp. 421–433,2005.
[6] C. S. Karas and E. A. Chiocca, “Neurosurgical robotics: a review of brain and spineapplications,” J. of Robotic Surgery, vol. 1, no. 1, pp. 39–43, 2007.
[7] M. D. O’Toole, K. Bouazza-Marouf, D. Kerr, M. Gooroochurn and M. Vloeberghs, “Amethodology for design and appraisal of surgical robotic systems,” Robotica, vol. 28,no. 2, pp. 297–310, 2010.
[8] T. Xia, C. Baird, G. Jallo, K. Hayes, N. Nakajima, N. Hata and P. Kazanzides, “Anintegrated system for planning, navigation and robotic assistance for skull base surgery,”Intl. J. of Medical Robotics and Computer Assisted Surgery, vol. 4, no. 4, pp. 321–330,2008.
[9] D. M. Kwartowitz, S. D. Herrell and R. L. Galloway, “Toward image-guided roboticsurgery: determining intrinsic accuracy of the da Vinci robot,” Intl. J. of ComputerAssisted Radiology and Surgery, vol. 1, no. 3, pp. 157–165, 2006.
[10] R. Taylor and P. Kazanzides, “Medical Robotics and Computer-Integrated InterventionalMedicine,” Advances in Computers: Emerging Technologies, vol. 73, pp. 219–258,2008.
[11] J. M. Fitzpatrick, “The role of registration in accurate surgical guidance,” Proc. of theInstitution of Mechanical Engineers, Part H: J. of Engineering in Medicine, vol. 224,no. 5, pp. 607–622, 2010.
[12] K. O. Arras, “An Introduction To Error Propagation: Derivation, Meaning and Examplesof Equation CY = FXCX FT
X ,” Lausanne, pp. 1–14, 1998[13] S. Preitl and R. Precup, “Extended Symmetrical Optimum (ESO) Method: A New
Tuning Strategy for PI/PID Controllers”, Proc. of the IFAC Workshop on DigitalControl: Past, Present and Future of PID Control, 2000, pp. 421–426.
[14] A. D. Wiles, D. G. Thompsona and D. D. Frantz, “Accuracy assessment andinterpretation for optical tracking systems,” in Proc. of SPIE Medical Imaging, vol.5367, San Diego, 2004, pp. 421–432.

13
VIII. PUBLICATIONS
[HT-1] T. Haidegger, T. Xia and P. Kazanzides, “Accuracy improvement of a neurosurgicalrobot system,” in Proc. of the 2nd IEEE RAS/EMBS Intl. Conf. on Biomedical Roboticsand Biomechatronics (BioRob), Scottsdale, 2008, pp. 836–841.
[HT-2] T. Haidegger, L. Kovacs, G. Fordos, Z. Benyo and P. Kazanzides, “Future Trendsin Robotic Neurosurgery,” in Proc. of the 14th Nordic-Baltic Conf. on BiomedicalEngineering and Medical Physics, Riga, 2008, pp. 229–233.
[HT-3] T. Haidegger, P. Kazanzides and Z. Benyo, “Integrated robotic system to assistskull base surgery (in Hungarian),” in Proc. of the Conf. for Biomedical and ClinicalEngineers (BUDAMED08), Budapest, 2008, pp. 1–5.
[HT-4] T. Xia, T. Haidegger, K. Hayes, N. Hata and P. Kazanzides, “Integration of OpenSource and Commercial Software for a Neurosurgical Robot System,” Workshop onSystems & Architecture for Computer Assisted Intervention at MICCAI (electronic fullversion), 2008.
[HT-5] T. Haidegger, L. Kovacs, B. Benyo and Z. Benyo, “Spatial Accuracy of SurgicalRobots,” in Proc. of the 5th Intl. Symp. on Applied Computational Intelligence andInformatics (SACI), Timisoara, 2009, pp. 133–138.
[HT-6] T. Haidegger, Z. Benyo and P. Kazanzides, “Sensor fusion for patient motioncompensation,” in Proc. of the Workshop on Advanced Sensing and Sensor Integrationin Medical Robotics at IEEE ICRA, Kobe, 2009, pp. 19–24.
[HT-7] T. Haidegger and Z. Benyo, “Surgical robotics in neurosurgery (in Hungarian),”Orvosi Hetilap, vol. 150, no. 39, pp. 1701–1711, 2009.
[HT-8] T. Haidegger, Z. Benyo and P. Kazanzides, “Patient motion tracking in the presenceof measurement errors,” in Proc. of the Annual Intl. Conf. of the IEEE Engineering inMedicine and Biology Society (EMBC), Minneapolis, 2009, pp. 5563–5567.
[HT-9] T. Haidegger, Z. Benyo and P. Kazanzides, “Manufacturing the Human Body—theEra of Surgical Robots,” J. of Machine Manufacturing, vol. XLIX, no. E2, pp. 18–24,2009.
[HT-10] T. Haidegger, B. Benyo, L. Kovacs and Z. Benyo, “Force Sensing and Force Controlfor Surgical Robots,” in Proc. of the 7th IFAC Symp. on Modelling and Control inBiomedical Systems, Aalborg, 2009, pp. 413–418.
[HT-11] T. Haidegger, P. Kazanzides, B. Benyo, L. Kovacs and Z. Benyo, “Surgical caseidentification for an image-guided interventional system,” in Proc. of the IEEE/RSJIntl. Conf. on Intelligent Robots and Systems (IROS), Taipei, 2010.
[HT-12] T. Haidegger, P. Kazanzides, J. Sandor, and Z. Benyo, “Technological challengesof image-guided robotic surgery—abrupt changes in the operating room,” in Proc. ofthe 4th Scientific Meeting of the Japan-Hungary Surgical Society (JHSS), Yokohama,2010.
[HT-13] T. Haidegger, Z. Benyo and P. Kazanzides, “Machines for Humans—the dawn ofrobot surgery (in Hungarian),” Gepgyartas (in press), 2011.
[HT-14] T. Haidegger and Z. Benyo, “Accuracy of CIS systems (in Hungarian),” in Proc.of the BME–MATE CIS Mini-Symp. I–II., Budapest, 2009, pp. 33–34.
[HT-15] T. Haidegger, P. Kazanzides, I. Rudas, B. Benyo and Z. Benyo, “The Importanceof Accuracy Measurement Standards for Computer-Integrated Interventional Systems,”in Proc. of the EURON GEM Sig Workshop on The Role of Experiments in RoboticsResearch at IEEE ICRA, Anchorage, 2010, pp. 19–24.

14
[HT-16] T. Haidegger, S. Gyori, B. Benyo and Z. Benyo, “Stochastic approach to errorestimation for image-guided robotic systems,” in Proc. of the Annual Intl. Conf. ofthe IEEE Engineering in Medicine and Biology Society (EMBC), Buenos Aires, 2010,pp. 984–987.
[HT-17] T. Haidegger and Z. Benyo, “Surgical robotic support for long duration spacemissions (electronic full version),” in Proc. of the 16th IAA Humans in Space Symp.,Beijing, 2007, pp. 234–234.
[HT-18] T. Haidegger, “Surgical Robots in Space: Long Distance Telesurgery,” 3rd SEU onSurgical Robotics (electronic version), Montpellier, pp. 1–15, 2007.
[HT-19] T. Haidegger and Z. Benyo, “Future of Surgical Robots in Space,” in Proc. of the58th Intl. Astronautical Congress (IAC), Hyderabad, 2007, pp. 1461–1471.
[HT-20] T. Haidegger and Z. Benyo, “Surgical robotic support for long duration spacemissions,” Acta Astronautica, vol. 63, no. 7-10, pp. 996–1005, IF: 0.374, 2008.
[HT-21] T. Haidegger and Z. Benyo, “Extreme telemedicine: feasibility of telesurgery andtelementoring in space (electronic full version),” J. of Telemedicine and e-Health,Proc. of the 13th Annual Intl. Meeting and Exposition of the American TelemedicineAssociation, IF: 0.97, vol. 14, no. S1, pp. 75–75, 2008.
[HT-22] T. Haidegger, “In-space surgery: impact of robotic technology on future explorationmissions,” in Proc. of the 9th Intl. Symp. on Artificial Intelligence, Robotics andAutomation in Space (i-SAIRAS08), Los Angeles, 2008, pp. 135–141.
[HT-23] T. Haidegger, L. Kovacs, S. Preitl, R.-E. Precup, A. Kovacs, B. Benyo and Z. Benyo,“Modeling and Control Aspects of Long Distance Telesurgical Applications,” in Proc.of the IEEE Intl. Joint Conf. on Computational Cybernetics and Technical Informatics(ICCC–CONTI), Timisoara, 2010, pp. 197–202.
[HT-24] T. Haidegger, J. Sandor and Z. Benyo, “Surgery in space: the future of robotictelesurgery,” Surgical Endoscopy, vol. 25, issue: 3, pp.681-690, IF: 3.304, 2011.
[HT-25] T. Haidegger and Z. Benyo, Extreme Telesurgery, ch. 2. in S. H. Baik, Ed. RobotSurgery, IN-TECH, Vienna, 2010, pp. 25–44.
[HT-26] T. Haidegger, L. Kovacs, S. Preitl, R.-E. Precup, B. Benyo and Z. Benyo, “CascadeControl for Telehealth Applications,” Scientific Bulletin “Politehnica” University ofTimisoara, Romania, Transactions on Automatic Control and Computer Science , vol.55(69), no. 4, 2010, pp. 99–108.
[HT-27] T. Haidegger, L. Kovacs, S. Preitl, R.-E. Precup, B. Benyo and Z. Benyo,“Controller Design Solutions for Long Distance Telesurgical Applications,” Intl. J.of Artificial Intelligence (IJAI), vol. 6, no. S11, pp. 48–71, 2011
[HT-28] T. Haidegger, L. Kovacs, S. Preitl, R.-E. Precup, B. Benyo and Z. Benyo, “CascadeControl for Telerobotic Systems Serving Space Medicine,” 18th IFAC World Congress,accepted, 2011

15
IX. FURTHER SELECTED PUBLICATIONS
[HT-28] T. Haidegger, “Advanced Robotic Arms in Space,” in Proc. of the 55th Intl.Astronautical Congress (IAC), Vancouver, 2004, vol. 4, pp. 2584–2594.
[HT-29] T. Haidegger, “Medical robots and teleoperation—surgery of tomorrow (in Hun-garian),” IME – Inforamtika es Menedzsment az Egeszsegugyben, vol. 5, no. 3, pp.49–52, 2006.
[HT-30] T. Haidegger and Z. Benyo, “Industrial Robotic Solutions for InterventionalMedicine,” in Proc. of the Intl. GTE Conference MANUFACTURING, Budapest, 2008,pp. 125–130.
[HT-31] T. Haidegger and Z. Benyo, “Introduction to surgical robotics (in Hungarian),” inProc. of the BME–MATE Surgical Robotics Mini-Symp. (electronic version), Budapest,2008, pp. 1–16.
[HT-32] Z. Benyo, L. Kovacs, G. Fordos, B. Benyo, I. Bosznai, L. Szabo, T. Haidegger andG. Varallyay, “Monitoring of driver’s physiological signals (in Hungarian),” A JovoJarmuve, vol. 3, no. 1-2, pp. 13–15, 2008.
[HT-33] T. Haidegger, L. Kovacs, B. Benyo and Z. Benyo, “Industrial Concepts Appliedto Surgical Robotics,” in Proc. of the 9th Intl. Conf. on Modern Technologies inManufacturing (MTeM), Cluj-Napoca, 2009, pp. 115–118.
[HT-34] T. Haidegger, B. Lengyel, P. Lenyu, Z. Benyo and J. Sandor, “The new Apollosurgical training system (electronic full version),” in Proc. of the 21th Intl. Conf. ofSociety for Medical Innovation and Technology (SMIT), 2009, pp. 97–98.
[HT-35] T. Haidegger and Z. Benyo, “Present and Future of CIS systems (in Hungarian),”in Proc. of the BME–MATE CIS Mini-Symp. I-II., Budapest, 2009, pp. 8–8.
[HT-36] T. Haidegger, “Robotic NOTES (in Hungarian),” in Proc. of the II. Magyar NOTESKongresszus, P. Lukovics, Ed., Budapest, 2009, pp. 1–8.
[HT-37] A. Gyorgy, L. Kovacs, T. Haidegger and B. Benyo, “Investigating a Novel Modelof Human Blood Glucose System at Molecular Levels from Control Theory Point ofView,” Acta Universitatis Sapientiae, Electrical and Mechanical Engineering, vol. 1,no. 1, pp. 77–92, 2009.
[HT-38] T. Haidegger, “Simulation of biomedical systems,” Course materials I-II. forVIFO5132, TE14AF06, VIFO2OBG, BME, pp. 1–26, 2009.
[HT-39] T. Haidegger, “Identification of biomedical systems,” Course materials I-II. forVIFO5132, TE14AF06, VIFO2OBG, BME, pp. 1–32, 2009.
[HT-40] L. Szilagyi, A. Lehotsky, M. Nagy, T. Haidegger, B. Benyo and Z. Benyo, “Stery-Hand: a New Device to Support Hand Disinfection,” in Proc. of the Annual Intl. Conf.of the IEEE Engineering in Medicine and Biology Society (EMBC), Buenos Aires,2010, pp. 4756–4759.
[HT-41] M. Nagy, T. Haidegger, L. Szilagyi, A. Lehotsky, L. Kovacs and B. Benyo, “ImagingTechnology to Prevent Hospital Acquired Infections,” in Proc. of the 8th Student ScienceConf. (SSC). Wroclaw, Wydawnictwo Politechniki Wroclawskiej, 2010, pp. 451–456.
[HT-42] A. Lehotsky, M. Nagy and T. Haidegger, “Towards the Objective Evaluation ofHand Disinfection,” in Proc. of the 16th Southern Biomedical Engineering Conf.(SBEC), College Park, SessionID: 7.4, 2010.
[HT-43] A. Lasso, M. Kelemen, T. Haidegger, C. Kirisits and G. Fichtinger, “Gynecologybrachytherapy applicator pose reconstruction in MR images,” Intl. Congress Series,

16
Proc. of the 24th Intl. Congress and Exhibition on Computer Assisted Radiology andSurgery (CARS), no. S1, pp. 324–325, 2010.
[HT-44] T. Haidegger, “The advancement of robotic surgery successes, failures, challenges(in Hungarian),” Orvosi Hetilap, vol. 151, no. 41, pp. 1688–1694, 2010.
[HT-45] T. Haidegger, G. Fenyvesi, L. Kovacs, B. Benyo and Z. Benyo, “Methods andTechniques to Assess Electromagnetic Tracking Systems,” in Proc. of the 1st Intl. Conf.on Applied Bionics and Biomechanics (ICABB), R. V. Mayorga, Ed., Venice, 2010.
[HT-46] J. Sandor, B. Lengyel, T. Haidegger, G. Saftics, G. Papp, A. Nagy and G. Weber,“Minimally invasive surgical technologies: Challenges in education and training,” AsianJ. of Endoscopic Surgery, vol. 3, no. 3, pp. 101–108, 2010.
[HT-47] M. Nagy, L. Szilagyi, A. Lehotsky, T. Haidegger and B. Benyo, “An Image-GuidedTool to Prevent Hospital Acquired Infections,” in Proc. of SPIE Medical Imaging, vol.7962-142, Orlando, 2011, pp. 1–4.
[HT-48] T. Haidegger, M. Nagy, A. Lehotsky and L. Szilagyi, “Method and apparatus forhand disinfection quality control,” Hungarian Patent Office (BME patent pending), 2010
Summary of publishing activity:
• Total number of publications: 53• Peer reviewed publications: 28• Patent: 1 (pending)• All known citations (including self-citation): 38• All known independent citations: 6• Independent recensions: 1• Total Impact Factor: 3.681
Summary of advisory activity:
• Total number of students supervised: 16• Student’s Scientific Circle (TDK) papers: 3• Successful B.Sc. defenses: 2• Successful M.Sc. defenses: 3; 3 in progress
Contact:
• E-mail: [email protected]• Professional blog on surgical robotics: http://surgrob.blogspot.com