The Value of Routine Transthoracic Echocardiography in ... · cute cerebrovascular accident (CVA)...
5
www.jcomjournal.com Vol. 22, No. 9 September 2015 JCOM 407 ABSTRACT • Background: Acute stroke or cerebrovascular acci- dent (CVA) is a common indication for hospitalization and can have devastating consequences, particu- larly in the setting of recurrence. Cardiac sources are potentially remediable; thus, a transthoracic echocar- diogram (TTE) is frequently ordered to evaluate for a cardiac source of embolism. • Objective: To evaluate the utility of performing TTE on patients experiencing a CVA or transient ischemic at - tack (TIA) to evaluate for a cardiac source of embolism. • Methods: Retrospective review of TTE reports and patient electronic medical records at Anne Arun- del Medical Center, a 385-bed community hospital. Medical charts for all CVA patients receiving a TTE between February 2012 to April 2013 were reviewed for TTEs showing unequivocal cardiac sources of embolism as evaluated by the reviewing cardiologist. Patient information and clinical morbidities were also noted to construct a composite demographic of CVA patients. • Results: One TTE of 371 (0.270%) identified a clear cardiac embolus.Risk factors for stroke included hyper- tension (n = 302), cardiovascular disease (n = 204), cardiomyopathy (n = 131), and diabetes (n = 146). • Conclusion: In the setting of stroke, TTE is of limited value when determining the etiology of stroke and should be used provisionally rather than routinely in evaluating patients experiencing CVA or TIA. A cute cerebrovascular accident (CVA) is a com- mon indication for hospitalization and can have devastating clinical consequences, particularly in the setting of recurrence. Defining the etiology of CVA and transient ischemic attacks (TIA) when they occur is important so that appropriate therapy can be initiated. Transthoracic echocardiograms (TTEs) are frequently ordered to evaluate for a cardiac source of embolism. No consensus exists about the use of imaging strategies to identify potential cardiovascular sources of emboli in patients who have had strokes. A few published studies have investigated the yield of TTE in identifying cardiac sources of CVA. The yield has been reported to be between < 1% and as high as 37% [1–3]. However, some of the reported sources of CVA in- cluded mitral valve prolapse and patent foramen ovale [4,5], conditions for which the association with stroke has been questioned [6–8]. In addition, many of these studies were performed using clinical data from tertiary referral centers, which may have increased the yield of cardiac sources [9]. The purpose of this study was to evaluate the yield of TTE in evaluating for a clear cardiac source of embolism in a consecutive series of patients diagnosed with a CVA or TIA in a community hospital. METHODS Setting All data was collected from the echocardiography lab at Anne Arundel Medical Center, a 384-bed community hospital in Annapolis, MD. The medical center sees about 250 patients a day in its emergency department and admits about 30,000 patients annually. All echocardiograms are performed by a centralized laboratory accredited by the Intersocietal Commission for the Accreditation of Echo- cardiography Laboratories, which performs approximately 6000 echocardiograms annually. All TTEs done for the diagnosis of CVA or TIA between 1 February 2013 and 1 May 2013 were evalu- ated in consecutive fashion by report review. Reports were searched for any cardiac source of embolism to include The Value of Routine Transthoracic Echocardiography in Defining the Source of Stroke in a Community Hospital Richard H. Bellemare, Joseph Cheruserry, RDCS, Barry Meisenberg, MD, and William C. Maxted Jr, MD ORIGINAL RESEARCH From Anne Arundel Medical Center, Annapolis, MD.
Transcript of The Value of Routine Transthoracic Echocardiography in ... · cute cerebrovascular accident (CVA)...
![Page 1: The Value of Routine Transthoracic Echocardiography in ... · cute cerebrovascular accident (CVA) ... One study did associate cardiomyopathy with CVA [12]; ... clinical nuances of](https://reader043.fdocuments.in/reader043/viewer/2022030609/5b2f7fde7f8b9ac06e8d7411/html5/page/1.jpg)
www.jcomjournal.com Vol. 22, No. 9 September 2015 JCOM 407
AbstrAct• Background: Acute stroke or cerebrovascular acci-
dent(CVA)isacommonindicationforhospitalizationand can have devastating consequences, particu-larlyinthesettingofrecurrence.Cardiacsourcesarepotentiallyremediable;thus,atransthoracicechocar-diogram(TTE)isfrequentlyorderedtoevaluateforacardiacsourceofembolism.
• Objective:ToevaluatetheutilityofperformingTTEonpatientsexperiencingaCVAortransientischemicat-tack(TIA)toevaluateforacardiacsourceofembolism.
• Methods: Retrospective review of TTE reports andpatient electronic medical records at Anne Arun-del Medical Center, a 385-bed community hospital.Medicalcharts forallCVApatients receivingaTTEbetweenFebruary2012toApril2013werereviewedfor TTEs showing unequivocal cardiac sources ofembolismasevaluatedbythereviewingcardiologist.PatientinformationandclinicalmorbiditieswerealsonotedtoconstructacompositedemographicofCVApatients.
• Results:OneTTEof371(0.270%)identifiedaclearcardiacembolus.Riskfactorsforstrokeincludedhyper-tension(n=302),cardiovasculardisease(n=204),cardiomyopathy(n=131),anddiabetes(n=146).
• Conclusion:Inthesettingofstroke,TTEisoflimitedvalue when determining the etiology of stroke andshouldbeusedprovisionally rather thanroutinely inevaluatingpatientsexperiencingCVAorTIA.
Acute cerebrovascular accident (CVA) is a com-mon indication for hospitalization and can have devastating clinical consequences, particularly in
the setting of recurrence. Defining the etiology of CVA and transient ischemic attacks (TIA) when they occur is important so that appropriate therapy can be initiated.
Transthoracic echocardiograms (TTEs) are frequently ordered to evaluate for a cardiac source of embolism. No consensus exists about the use of imaging strategies to identify potential cardiovascular sources of emboli in patients who have had strokes.
A few published studies have investigated the yield of TTE in identifying cardiac sources of CVA. The yield has been reported to be between < 1% and as high as 37% [1–3]. However, some of the reported sources of CVA in-cluded mitral valve prolapse and patent foramen ovale [4,5], conditions for which the association with stroke has been questioned [6–8]. In addition, many of these studies were performed using clinical data from tertiary referral centers, which may have increased the yield of cardiac sources [9].
The purpose of this study was to evaluate the yield of TTE in evaluating for a clear cardiac source of embolism in a consecutive series of patients diagnosed with a CVA or TIA in a community hospital.
METHODSsettingAll data was collected from the echocardiography lab at Anne Arundel Medical Center, a 384-bed community hospital in Annapolis, MD. The medical center sees about 250 patients a day in its emergency department and admits about 30,000 patients annually. All echocardiograms are performed by a centralized laboratory accredited by the Intersocietal Commission for the Accreditation of Echo-cardiography Laboratories, which performs approximately 6000 echocardiograms annually.
All TTEs done for the diagnosis of CVA or TIA between 1 February 2013 and 1 May 2013 were evalu-ated in consecutive fashion by report review. Reports were searched for any cardiac source of embolism to include
The Value of Routine Transthoracic Echocardiography in Defining the Source of Stroke in a Community HospitalRichard H. Bellemare, Joseph Cheruserry, RDCS, Barry Meisenberg, MD, and William C. Maxted Jr, MD
Original research
From Anne Arundel Medical Center, Annapolis, MD.
![Page 2: The Value of Routine Transthoracic Echocardiography in ... · cute cerebrovascular accident (CVA) ... One study did associate cardiomyopathy with CVA [12]; ... clinical nuances of](https://reader043.fdocuments.in/reader043/viewer/2022030609/5b2f7fde7f8b9ac06e8d7411/html5/page/2.jpg)
408 JCOM September 2015 Vol. 22, No. 9 www.jcomjournal.com
TransThoracic Echocardiography
thrombus, tumor, vegetation, shunt, aortic atheroma, or any other finding that was felt to be a clear source of em-bolism by the interpreting cardiologist. We did not include entities such as mitral valve prolapse, patent foramen ovale, and isolated atrial septal aneurysms since their association with CVA/TIA has been questioned. Also not included was cardiomyopathy without aneurysm, apical wall motion abnormality, or intra-cavitary thrombus solely because the ejection fraction was less than 35%, as the literature does not support these conditions as clear causes of TIA or CVA.
In addition to reviewing echocardiogram reports, all patient records were evaluated for clinical variables including age, gender, presence of atrial fibrillation, hypertension, diabetes, past CVA, left atrial dilation by calculation of indexed direct left atrial volume, recent myocardial infarction, and known cardiovascular disease.
All echocardiograms were performed on Hewlet-Packard Vivid 7 or Vivid 9 (GE Healthcare, Wauwatosa, WI) by technicians who held registered diagnostic car-diac sonographer status. All TTEs contained the “stan-dard” views in accordance with published guidelines [10]. Saline contrast to look for shunts was not standard on these studies. Echocardiogram images were stored digitally and read from an EchoPac (GE Healthcare, Wauwatosa, WI) reading station. All echocardiograms were interpreted by one of 16 American Board of Internal Medicine–certified cardiologists, 5 of whom were tes-tamurs (physicians who have passed one of the examina-tions of special competence in echocardiography). These 5 interpreted 20% of the studies.
RESULTS
During the observation period, 867 patients with a diag-nosis of CVA or TIA were admitted to our institution. Among these patients, there were 417 TTEs performed as part of their evaluation, generally within 48 hours of the event or admission. Over 90% of the TTEs were ordered by hospitalists, who were responsible for admit-ting patients to the stroke unit at our institution. Forty-six of the patients were subsequently felt not to have had a CVA or TIA on clinical grounds by their treating physi-cians in conjunction with absence of brain imaging find-ings, and were excluded from further analysis. Hence, the remaining cohort was comprised of 371 consecutive TTE studies for CVA or TIA that was documented on clinical and imaging criteria The population contained 49.9% men and 50.1% women. The average age was 69.7 years (range, 23–96). The age distribution is further outlined in Figure 1. The remainder of the demographic and clinical variables are outlined in Figure 2. The mean CHADS-VASC score [11] was 4.2.
Of the 371 echocardiograms, only 1 showed an unequivocal source of embolism, specifically a left ven-tricular apical thrombus in a patient who had recently experienced an anterior myocardial infarction (Figure 3).
DISCUSSION
Our data are in keeping with those of others, though our yield was even lower than that reported in previous studies [1–3]. The low yield may be explained by a num-ber of factors. First, we did not include patent foramen
Figure 1. Agedistributionof371consecutivepatientswithCVAorTIAundergoingroutineTTE.
Nu
mb
er o
f P
atie
nts
Age (Years)
![Page 3: The Value of Routine Transthoracic Echocardiography in ... · cute cerebrovascular accident (CVA) ... One study did associate cardiomyopathy with CVA [12]; ... clinical nuances of](https://reader043.fdocuments.in/reader043/viewer/2022030609/5b2f7fde7f8b9ac06e8d7411/html5/page/3.jpg)
www.jcomjournal.com Vol. 22, No. 9 September 2015 JCOM 409
ovale or atrial septal aneurysms (which account for a high percentage of embolic sources in other publications) since there is not a clear consensus that any of those entities are associated with an increased risk of embolic events. The exclusion of cardiomyopathy as a cause of CVA or TIA is arguable, but its link to CVA or TIA is also unproven. One study did associate cardiomyopathy with CVA [12]; however, the mechanism is not clear, as the incidence of CVA in cardiomyopathy has been described as similar regardless of the severity of left ventricular dysfunction [13]. Many past reports have come from tertiary care centers, where there may be referral bias whereas our data come from consecutive patients at a single community hospital.
TTE is relatively quick to perform and interpret and carries no physical risk to a patient. However, our data suggest that ordering TTE routinely in the setting of CVA offers little value. With health care organizations turning their attention to reducing low-value care, which potentially wastes limited resources, considerations of value and effectiveness continue to be a priority. Our findings suggest TTE use in this setting conflicts with the current trajectory of value-based medical practice. As well, a prior Markov model decision analysis found that TTE is not cost-effective when used routinely to identify source of emboli in stroke [14].
Despite the low yield of TTE in evaluating for a cardiac source of CVA, TTEs continue to be frequently ordered. In our own institution, 48% of patients with a CVA or TIA underwent a TTE based on preferences and
habits of individual admitting physicians and without any structured criteria. Order sets for CVA admissions do not include this test; physicians are adding it but not for any particular patient characteristic or exam finding.
There are a number of reasons that echocardiograms may be ordered more frequently by some. A documented decline in ordering echocardiograms was seen follow-ing education at one center [15], suggesting that lack of knowledge about the limitations of TTE may be a factor. A second potential factor is fear of medicolegal consequences. Indeed, the current American Heart As-sociation/American Stroke Association guidelines for the early management of adults with ischemic stroke [16] offers no formal recommendations or clear indications.
Computerized decision support (CDS) that links the medical record to appropriateness criteria could poten-tially reduce the inappropriate use of TTE. CDS has been shown to be effective in reducing unnecessary ordering of tests in other settings [17–19].
Among the limitations in our analysis is the heteroge-neity in echocardiogram readers. However, this heteroge-neity may makes the study more relevant as it reflects the reality in most community hospitals. Another potential limitation is that saline contrast studies were not used routinely; however, this too is typical at community hos-pitals. Also, while all echocardiograms were interpreted by “board-certified” cardiologists, only 5 had passed the “examination of special competence” to be certified as a testamur of the National Board of Echocardiography, raising the question as to whether subtle findings could
Original research
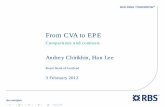
Figure 2. Comorbiditiesof371consecutivepatientswithCVAundergoingroutineTTE.CVdisease=structuralcardiovasculardisease;LA=leftatrium;MI=myocardialinfarction.
Per
cen
tag
e o
f P
atie
nts
![Page 4: The Value of Routine Transthoracic Echocardiography in ... · cute cerebrovascular accident (CVA) ... One study did associate cardiomyopathy with CVA [12]; ... clinical nuances of](https://reader043.fdocuments.in/reader043/viewer/2022030609/5b2f7fde7f8b9ac06e8d7411/html5/page/4.jpg)
410 JCOM September 2015 Vol. 22, No. 9 www.jcomjournal.com
TransThoracic Echocardiography
have been missed. However, there were no relevant find-ings in the 20% of studies interpreted by the testamurs, suggesting that the other echocardiographers were not missing diagnoses. Finally, we had only 10 patients younger than age 45 and so the study conclusions are less definitive for that age-group.
CONCLUSION
TTE was of limited utility in uncovering a cardiac source of embolism in a typical population with CVA or TIA.Based upon the data, we believe that TTE should not be used routinely in the setting of CVA; however, we do recognize that TTE may be of value in patients who have other comorbidities that would place them at increased risk of embolic CVA such as a recent anterior MI, those at risk for endocarditis, or those with brain imaging findings suggestive of embolic CVA [20]. Ordering a low-value test such as a TTE in the setting of TIA or CVA adds cost and does not often yield a clinically meaningful results. In addition, a “negative” TTE can be misinterpreted as a normal heart and forestall addi-tional workup such as transesophageal echocardiography and long-term rhythm analysis, which may be of higher value. We suggest that in a community hospital setting the determination of need for TTE be made based on the clinical nuances of the case rather than by habit or as part of standardized order sets.
Corresponding author: Barry Meisenberg, MD, DeCesaris Cancer Institute, 2001 Medical Parkway, Annapolis, MD 21146, [email protected].
Financial disclosures: None.
Author contributions: conception and design, BM, WCM; analysis and interpretation of data, BM, WCM; drafting of article, RHB, BM, WCM; critical revision of the article, BM, WCM; administrative or technical support, JC; collection and assembly of data, RHB, JC.
REfERENCES1. Rauh R, Fischereder M, Spengel FA. Transesophageal echo-
cardiography in patients with focal cerebral ischemia of un-known cause. Stroke 1996;27:691.
2. Khan MA, Khealanj B, Kamal, A. Diagnostic yield of trans-thoracic echocardiography for stroke patients in a developing country. J Pak Med Assoc 2008;58:375–7.
3. de Abreu T, Mateus S, José Correia J. Therapy implications of transthoracic echocardiography in acute ischemic stroke patients. Stroke 2005;36:1565–6.
4. de Bruijn SFTM, Agema WRP, Lammers GJ, et al. Trans-esophageal echocardiography is superior to transthoracic echocardiography in management of patients of any age with transient ischemic attack or stroke. Stroke 2006;37:2531–4.
5. Putaala J, Metso AJ, MD, Metso T. Analysis of 1008 con-secutive patients aged 15 to 49 with first-ever ischemic stroke. Stroke 2009;40:1195–203.
6. Lechat P, Mas JL, Lascault G, et al. Prevalence of patent fora- men ovale in patients with stroke. N Engl J Med 1988;318: 1148–52.
7. Di Tullio MR, Jin Z, Russo C, et al. Patent foramen ovale, subclinical cerebrovascular disease, and ischemic stroke in a population-based cohort. J Am Coll Cardiol 2013; 62:35–41.
8. Orencia AJ, Petty GW, Khandheria BK, et al. Risk of stroke with mitral valve prolapse in population-based cohort study; Stroke 1995;26:7–13.
9. Holmes M, Rathbone J, Littlewood C. Routine echocardiog-raphy in the management of stroke and transient ischaemic attack: a systematic review and economic evaluation. Health Technol Assess 2014;18:1–176.
10. Ryan T, Armstrong W. Feigenbaum’s echocardiography. 7th ed. Philadelphia: Lippincott Williams & Wilkins; 2009.
11. Lip GY, Nieuwlaat R, Pisters R, et al. Refining clinical risk strati-fication for predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor-based approach: the Euro Heart Survey on Atrial Fibrillation. Chest 2010;137:263–72.
12. Furie KL, Kasner SE, Adams RJ, et al. Guidelines for the prevention of stroke in patients with stroke or transient isch-emic attack: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2011;42:227–76.
13. Hays AG, Sacco RL, Rundek T. Left ventricular systolic dysfunction and the risk of ischemic stroke in a multiethnic population. Stroke 2006;37:1715–9.
14. McNamara RL, Lima JA, Whelton PK, Powe NR. Echocar-diographic identification of cardiovascular sources of emboli to guide clinical management of stroke: a cost-effectiveness analysis. Ann Intern Med 1997;127:775–87.
15. Alberts MJ, Bennett CA, Rutledge VR. Hospital charges for stroke patients. Stroke 1996;27:1825–8.
Figure 3. Transthoracic echocardiogram 2-chamber view.Notethelargethrombusintheapexoftheleftventricle.
![Page 5: The Value of Routine Transthoracic Echocardiography in ... · cute cerebrovascular accident (CVA) ... One study did associate cardiomyopathy with CVA [12]; ... clinical nuances of](https://reader043.fdocuments.in/reader043/viewer/2022030609/5b2f7fde7f8b9ac06e8d7411/html5/page/5.jpg)
www.jcomjournal.com Vol. 22, No. 9 September 2015 JCOM 411
16. Jauch EC, Saver JL, Adams HP, et al. Guidelines for the early management of patients with acute ischemic stroke: a guideline for healthcare professionals from the American Heart Associa-tion/American Stroke Association. Stroke 2013;44:870–947.
17. Levick DL, Stern G, Meyerhoefer CD, et al. Reducing un-necessary testing in a CPOE system through implementation of a targeted CDS intervention. BMC Med Inform Decis 2013;13:43.
18. Chen P, Tanasijevic MJ, Schoenenberger RA, et al. A computer-
based intervention for improving the appropriateness of anti-epileptic drug level monitoring. Am J Clin Pathol 2003;119: 432–8.
19. Solberg LI, Wei F, Butler JC, et al. Effects of electronic deci-sion support on high-tech diagnostic imaging orders and patients. Am J Manag Care 2010;16:102–6.
20. Menon BK, Coulter JI, Simerpret B, et al. Acute ischaemic stroke or transient ischaemic attack and the need for inpatient echocardiography. Postgrad Med J 2014;90:434–8.
Copyright 2015 by Turner White Communications Inc., Wayne, PA. All rights reserved.
Original research