Exploration of Using Cyclodextrins as Novel Additives and ...
description

Available online at www.sciencedirect.com
Journal of Controlled Release 123 (2007) 78–99www.elsevier.com/locate/jconrel
Review
The utility of cyclodextrins for enhancing oral bioavailability
Rebecca L. Carrier a,⁎, Lee A. Miller b,1, Imran Ahmed c,2
a Department of Chemical Engineering, Northeastern University, 457 Snell Engineering Center, Boston, Massachusetts 02115, United Statesb Pfizer, Inc., 2800 Plymouth Road, Ann Arbor, Michigan 48105, United Statesc Pfizer, Inc., Eastern Point Road, Groton, Connecticut 06340, United States
Received 18 April 2007; accepted 30 July 2007Available online 16 August 2007
Abstract
Cyclodextrins (CD) have been utilized extensively in pharmaceutical formulations to enhance oral bioavailability. A critical review of theliterature in which cyclodextrins were utilized for this purpose was conducted. The goal of this review was to determine if quantitative guidelinesfor drug and cyclodextrin properties necessary for bioavailability enhancement using cyclodextrins could be extracted. Twenty-eight studies wereexamined in which the focus was on the use of cyclodextrins as solubilizers to enhance bioavailability. Commonly observed factors included:utilization of pre-formed complex rather than physical mixtures, drug hydrophobicity (logP N 2.5), low drug solubility (typicallyb 1 mg/ml),moderate binding constant (b 5000 M−1), low dose (b 100 mg), and low CD:drug ratio (b 2:1). These general guidelines, however, did not applyto all studies. Quantitative guidelines useful to a formulation scientist considering the use of cyclodextrins were difficult to develop due to missinginformation and the complicated manner in which drug and cyclodextrin properties interact to influence key drug delivery processes (e.g.,dissolution, absorption). The mechanisms by which cyclodextrins influence these processes, again emphasizing solubilization capabilities, arediscussed to provide further insight into why cyclodextrins will increase bioavailability in certain cases but not influence or possibly decreasebioavailability in others.© 2007 Elsevier B.V. All rights reserved.
Keywords: Cyclodextrins; Solubilization; Bioavailability; Modeling; Formulation
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 792. Characteristics of studies utilizing cyclodextrins to enhance oral bioavailability . . . . . . . . . . . . . . . . . . . . . . . . . . . 80
2.1. Reported influence of cyclodextrins . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 802.2. Properties of compounds whose bioavailability is enhanced using cyclodextrins. . . . . . . . . . . . . . . . . . . . . . . 812.3. Use of complex vs. physical mixture of drug and cyclodextrin . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 812.4. Complex formation methodology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 862.5. Immediate vs. controlled release . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 872.6. Ionized vs. neutral drugs . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 882.7. Dose and molar CD:drug ratio . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 882.8. Type of CD used . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 892.9. Binding constant magnitude . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 90
2.10. Interaction with polymers and other formulation components . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 90
⁎ Corresponding author. Tel.: +617 373 7126; fax: +617 373 2209.E-mail addresses: [email protected] (R.L. Carrier), [email protected] (L.A. Miller), [email protected] (I. Ahmed).
1 Tel.: +734 622 3628; fax: +860 686 6209.2 Tel.: +860 441 4281; fax: +860 715 9575.
0168-3659/$ - see front matter © 2007 Elsevier B.V. All rights reserved.doi:10.1016/j.jconrel.2007.07.018

79R.L. Carrier et al. / Journal of Controlled Release 123 (2007) 78–99
3. Explanations for ability of cyclodextrins to enhance bioavailability . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 913.1. Significance . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 913.2. Enhancement in dissolution kinetics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 913.3. Increase in solubility . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 923.4. Decrease in degradation kinetics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 933.5. Change in intestinal membrane properties . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 933.6. Shuttling and enhancement of drug concentration at the intestinal wall . . . . . . . . . . . . . . . . . . . . . . . . . . . . 94
4. When cyclodextrins do not enhance bioavailability . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 944.1. Binding constant magnitude and amount of dosed cyclodextrin . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 944.2. Degradation of cyclodextrins in the intestinal environment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 94
5. Conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 95Nomenclature . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 96References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 96
1. Introduction
Cyclodextrins have been used extensively in pharmaceuticalresearch and development, and there are currently over 30marketed cyclodextrin-containing pharmaceutical productsworldwide [1,2]. Cyclodextrins possess a special ability tocomplex with drugs enabling them to increase solubility, reducebitterness, enhance stability, and decrease tissue irritation upondosing [3]. One of the most common applications ofcyclodextrins cited in the pharmaceutical literature is theenhancement of bioavailability. When can cyclodextrins beused to enhance oral bioavailability of a given compound? Oneapproach to addressing this question, taken in the presentreview, is to seek guidance by examining the vast body ofliterature in which cyclodextrins have been utilized to enhancebioavailability. There are numerous excellent reviews on the useof cyclodextrins in oral dosage forms, and many whichspecifically address the effect of cyclodextrins on oralabsorption and/or bioavailability [1–11]. One recent reviewby Loftsson et al. examines over 80 publications on the effect ofcyclodextrins on oral bioavailability of 50 different drugs using17 different cyclodextrins in the context of the Biopharmaceu-tical Classification System [1]. The importance of drugsolubility and permeability is emphasized. Here, multipleaspects of studies in which cyclodextrins were utilized toenhance bioavailability were analyzed to gain further insightinto which physical and chemical properties of drug, cyclodex-trin, dosage form, and delivery environment are suitable toallow enhancement of bioavailability. The specific values ofdrug and cyclodextrin properties as well as experimentalparameters (e.g., drug to cyclodextrin ratio, animal speciesused) were studied for apparent trends.
As indicated by the large number of reviews on this topic, theliterature affords an abundance of references demonstrating theuse of cyclodextrins to enhance oral bioavailability of activecompounds. These studies have utilized a range of naturalcyclodextrins and cyclodextrin derivatives, numerous animalspecies (including human), and various dosing vehicles, doselevels, and cyclodextrin-to-drug ratios. The vast majority ofthese studies demonstrate a positive affect of inclusion ofcyclodextrin in a dosed formulation. Most of the studies
attribute the influence on bioavailability to the solubilizingcapabilities of cyclodextrins, although some also discuss othercyclodextrin effects, such as effects on physical or chemicalstability [12–15]. Typically, the complex or physical mixture ofdrug and cyclodextrin is dosed, and the resulting pharmacoki-netic parameters are compared to those resulting when the drugalone or in a commercial formulation is dosed. Given the widerange of experimental parameters utilized in these studies andthe fact that most of them report positive results, the questionarises: Is it possible to gain insight into the important parametersthat determine the success or failure of bioavailabilityenhancement with cyclodextrins from reviewing a finite numberof studies?
In this critical review, a survey of the literature reporting useof cyclodextrins to enhance oral bioavailability is conducted.Some of the important attributes of these studies are discussedto give insight into key physical and chemical properties of thedrug, cyclodextrin, and dosage form that allow bioavailabilityenhancement to occur. Physical mechanisms of bioavailabilityenhancement using cyclodextrins are then discussed to providefurther understanding of why these parameter values areimportant and how successful bioavailability enhancementusing cyclodextrins can be achieved. It should be noted thatwhile recent applications of cyclodextrins have included theiruse for stabilizing protein, peptide, and nucleic acid therapeu-tics [2,8,11], the focus in this review is on the exploitation ofthe solubilizing capacity of cyclodextrins for the delivery ofsmall molecular weight (typically b 500 Da) compounds.However, much of the discussion of the influence ofcyclodextrins on the bioavailability of low molecular weightcompounds generally applies to biomolecules, with certainadditional mechanisms of action on biomolecules (e.g.,prevention of protein aggregation or enhancement of endoso-mal membrane disruption in gene delivery) not emphasized inthis review [11]. In addition, cyclodextrins have been utilizedfor a number of different drug delivery routes, and there hasbeen a large amount of recent investigation into cyclodextrinpolymers and cyclodextrins conjugated to other deliveryvehicles (e.g., nanoparticles, liposomes) [9]. However, thecurrent discussion is focused on oral drug delivery usingcyclodextrin monomers.

80 R.L. Carrier et al. / Journal of Controlled Release 123 (2007) 78–99
2. Characteristics of studies utilizing cyclodextrins toenhance oral bioavailability
2.1. Reported influence of cyclodextrins
Most of the literature on bioavailability enhancement usingcyclodextrins includes similar data [5]. Phase-solubility dia-grams are often used to determine the stoichiometry of bindingand the equilibrium binding constant. NMR-spectra, X-raydiffraction patterns, and DSC thermograms are typically used tomeasure changes in the characteristic analytical features of adrug molecule upon complexation as an indication that acomplex has been formed. Dissolution profiles for the drug,physical mixture of drug and cyclodextrin, and/or complex ofdrug and cyclodextrin are often presented to demonstrate theinfluence of cyclodextrin on dissolution kinetics and the totalamount of drug in solution [16]. In addition, pharmacokineticparameters resulting from dosing a physical mixture of drug andcyclodextrin or a pre-formed complex in comparison to drugalone are often presented to demonstrate an overall improvementin bioavailability upon dosing with cyclodextrin. These studiesoften involve compounds with poor or variable bioavailabilityand cite low solubility or slow dissolution kinetics as reasons forbioavailability issues [16–24]. The variability of pharmacoki-netic and pharmacodynamic responses to drugs has beenreported to decrease with the inclusion of cyclodextrins indosage forms [25,26]. Pharmacokinetic responses to low-solubility compounds are characteristically highly variable inthe absence of a solubilizing agent [17], and the ability ofcyclodextrins to solubilize drugs probably contributes to lowerresponse variability. Some studies also include information ondegradation rate of the studied compound and how it isinfluenced by cyclodextrin. The reported increase in bioavail-ability is typically expressed as a change in an area under theplasma concentration vs. time curve (AUC) value, a change inthe time to reachmaximum plasma levels of the given compound(Tmax), and/or the maximum plasma level achieved (Cmax)[23,24,26–28]. In some studies, the pharmacodynamics arereported in addition to or in place of the pharmacokineticchanges brought about by inclusion of cyclodextrin in a dosageform, demonstrating that cyclodextrins can improve the efficacyof a given dose of a therapeutic agent [25,29,30].
For the current review, twenty-eight randomly selectedarticles from the literature in which cyclodextrins were utilizedto enhance bioavailability were examined in an effort to developa greater understanding of when cyclodextrins can be used forbioavailability enhancement [12,17,18,20,22–28,30–46]. Spe-cifically, the different properties of these studies were compared,including the properties of the drug compounds utilized, theproperties of the cyclodextrins, the design of the dosage forms,and the details of the experiment (e.g., animal species used,manner in which material was dosed). The studies were selectedbased on the information they provided and/or the ability toobtain missing information from other literature sources so thatall studies could be compared [5,15,16,19,21,35,47–62]. Table 1compares some of the key aspects of studies conducted in whichcyclodextrins were used to enhance bioavailability, and Table 2
summarizes these same factors for experiments where it wasindicated that cyclodextrins were not successful in enhancingbioavailability. The discussion below is focused on observationsresulting from the review of these articles, although many of thecomments apply to the cyclodextrin literature in general, andseveral articles in addition to the twenty-eight studied in detailare referenced. Again, it is emphasized that the articles examinedfocused mainly on the solubilizing capabilities of cyclodextrinsfor small molecular weight compounds. In other words, theirfocus was not on other possible mechanisms of bioavailabilityenhancement using cyclodextrins (discussed below) or the use ofcyclodextrins to influence delivery of peptides, proteins, ornucleic acids, as has been the focus of much recent literature.
The studied articles contained a total of 58 comparisons madebetween a dosed formulation containing cyclodextrins and onethat did not. Of these comparisons, 52 showed evidence ofbioavailability enhancement using cyclodextrins (as indicatedby a change in AUC or a similar parameter as noted in Table 1),while 6 showed no change with inclusion of cyclodextrins. Theprominence of studies showing bioavailability enhancementusing cyclodextrins may be related to the tendency for positiveresults to be reported more frequently than negative results. It isalso likely that drugs selected for studies with cyclodextrins tendto possess qualities which make them candidates for solubili-zation (i.e. low solubility).
As can be seen in Table 1, about half of the increases in AUCvalues were less than 100% increases. Of 47 studies where achange in AUC (or a similar parameter as noted in Table 1) wasreported, 24 of those studies resulted in a ratio of AUC withcyclodextrin to AUC without cyclodextrin between 1 and 2,while 22 resulted in a ratio of 2–8 and one resulted in a ratio of46. Increases in AUC brought about by utilizing cyclodextrinswith drug are accompanied by both increases and decreases inTmax and Cmax values [24,25,28]. This implies that when theoverall exposure to a compound is increased by inclusion ofcyclodextrin in a dosage form, the accompanying kinetics ofdrug absorption in the intestine may increase or decrease. InTable 1 there are 28 reported decreases in Tmax, 5 reportedincreases, and 6 reports of no change. Most of the increases inTmax were of less than 3h. The fact that most studies reported adecrease in Tmax with inclusion of cyclodextrin is logical inlight of the fact that cyclodextrin speeds up dissolution kinetics,as described in more detail later in this review. An increase inTmax could be due to precipitation of a low solubility dosedcomplex or decrease in free drug concentration in the intestinallumen because of binding to cyclodextrin. In Table 1 there are38 reported increases in Cmax and one reported decrease. Mostincreased Cmax values were less than double the control value,and all except for two reported increases were less than tentimes the control value. There was no clear correlation betweenmagnitude of increase in Cmax or change in Tmax and magnitudeof increase in AUC (data not shown). The increase in Cmax islogical as cyclodextrins speed up dissolution, and higher levelsof drug in solution in the intestine typically result in greater drugabsorption. It has been noted that when an increase in bloodplasma levels for a given compound is not desired, cyclodextrincan be used to decrease the required dose [63].

81R.L. Carrier et al. / Journal of Controlled Release 123 (2007) 78–99
2.2. Properties of compounds whose bioavailability isenhanced using cyclodextrins
An obvious requirement for cyclodextrins to be a suitabletechnology for bioavailability enhancement is the formation of acomplex between drug and cyclodextrin. Specific exceptionsinclude cases where cyclodextrins such as dimethyl beta-cyclodextrin (DM-β-CD) inhibit efflux by P-glycoprotein (P-gp) or metabolism by multi-resistant protein 2 (MRP2) orproteolytic enzymes [64], or caseswhere drug is covalently boundto cyclodextrin for site-specific delivery [65,66], but thesespecific effects were not discussed in any of the studies presentedin Table 1. General guidelines on what molecules will complexwith cyclodextrin based on molecular properties are given in theliterature [67]. Drug-cyclodextrin complexation usually involvesinteraction of hydrophobicmoieties on drugs and the pocket of thecyclic cyclodextrin molecule. Consideration of the calculatedoctanol–water partitioning coefficient (clogP) values of thecompounds in Table 1 and examination of their structures (Fig. 1)demonstrates the predominance of hydrophobic compoundsemployed in studies reporting enhanced oral bioavailabilityusing cyclodextrins. 18 of the 29 studies examined involvedcompounds with logP values greater than 2.5. In addition tohaving a greater likelihood of complex formation, hydrophobiccompounds generally have low solubility and are more likely tobe dissolution rate-limited (as opposed to absorption rate-limited)in overall absorption kinetics. The formulator should keep inmindthat if a factor other than dissolution kinetics is resulting in poorbioavailability (e.g., low permeability of the intestinal membraneto the compound being studied), it is unlikely that formulationwith cyclodextrins will result in bioavailability enhancement.
Most of the compounds listed in Tables 1 and 2, althoughthey are not salt forms, will be ionized during at least a portionof gastrointestinal (GI) transit, as indicated by their pKa values.This is important as the charge on the drug molecule caninfluence its binding with cyclodextrin. Thus, the cyclodextrinmay influence the dissolution and solubility of the compound todifferent extents in different areas of the GI tract. This factincreases the complexity of comparing studies as listed inTables 1 and 2. If two compounds were used in the exact samestudy and all properties of the compounds were identical exceptfor pKa values, they may achieve different bioavailability due tovariable binding with cyclodextrin during GI transit. The pKavalue will also influence the solubility of the compound at agiven pH, influencing the total amount of drug that can be insolution in both free and complexed forms. Thus, bothunbuffered water solubilities and solubilities at specific pHvalues, when available, are listed for the compounds in Tables 1and 2. Most of the compounds have water solubilities of lessthan 0.1 mg of drug/ml, indicating that dissolution may be alimiting factor in drug absorption, but greater than 1 μg/ml. Thecritical solubility for drugs to exhibit dissolution limited drugabsorption from the GI tract has been reported as 0.1 mg/ml[68]. The fact that some of the drugs listed in Table 1 havesolubilities greater than 0.1 mg/ml emphasizes the importanceof considering the complex interaction of multiple factors thatcould determine the influence of cyclodextrins (e.g., binding
constant, cyclodextrin:drug ratio, dose, possible influence ofcyclodextrin on intestinal permeability or efflux, etc.).
2.3. Use of complex vs. physical mixture of drug and cyclodextrin
As can be seen in Table 1, the vast majority of studies inwhich cyclodextrins are utilized to enhance oral bioavailabilityhave employed the complex rather than the physical mixture ofthe given drug with cyclodextrin. When the physical mixturewas used, it typically resulted in a significantly lower level orcomplete lack of bioavailability enhancement. Of the six studiesreviewed in which physical mixtures of drug and cyclodextrinwere dosed, two did not show bioavailability enhancement[26,46], and bioavailability enhancement was moderate (1.1× to1.5× increase in AUC) for the other studies [18,20,36,41]. AUCincreases were approximately doubled for complexes vs.physical mixtures of single compounds, and this is oftenaccompanied by greater decreases in Tmax and greater increasesin Cmax. This is likely related to decreased enhancement indissolution kinetics observed when the physical mixture ratherthan the complex is utilized (see “Explanations for the ability ofcyclodextrins to enhance bioavailability” below). Severalstudies have shown that a physical mixture of cyclodextrinand drug exhibits dissolution kinetics either similar to or onlyslightly greater than those of drug alone, and almost alwaysslower than those of the complex [23,69–71]. It has beendocumented that physical mixing of drug and cyclodextrin,especially with addition of energy (e.g. from grinding) canresult in some complex formation [72,73]. However, it is clearupon analysis (e.g., via DSC) that the majority of the mixedmaterial is still pure parent substances (rather than complex)[20,24,36]. Thus, there is still likely to be a difference betweenphysical mixtures and pre-formed complex formations.
The much more common use of complexes rather thanphysical mixtures indicates that it is generally expected thatformulations of physical mixtures will not enhance oralbioavailability to the same extent as formulations of complexes.An exception comes in the patent literature, where Stella et al.claim that sulfoalkyl ether cyclodextrins formulated as bothphysical mixtures with drug and complexes can be used toequivalently enhance dissolution, solubility, and/or bioavail-ability [74,75]. These patents as well as published papers [76–80] give several examples of controlled-release tablet formula-tions containing physical mixtures with dissolution kineticssimilar to those containing complexes. However, they do notpresent actual in vivo bioavailability data to support theequivalence of physical mixtures and complexes in vivo. Inaddition, it is stated in these papers and patents that anappropriate dosage form will allow hydration of the drug-cyclodextrin physical mixture within the dosage form to ensureadequate formation of the complex. It is possible that the highsolubilities of sulfoalkyl ether cyclodextrins allow substantialamounts of cyclodextrin to be in solution in the hydrated oralcontrolled-release drug delivery device (e.g., matrix or osmotictablet). If the hydrated cyclodextrin and drug are present atsufficiently high concentrations, there could be appreciablecomplex formation prior to release from the drug delivery

Table 1Summary of drug, cyclodextrin, and dosage form parameters for studies in which cyclodextrins were successfully utilized to enhance bioavailability
82R.L.Carrier
etal.
/Journal
ofControlled
Release
123(2007)
78–99

(continued on next page)
83R.L.Carrier
etal.
/Journal
ofControlled
Release
123(2007)
78–99

A = Acidic, B = basic, soln. = solution, clogP = calculated logP value, calculated using Advanced Chemistry Development (ACD/Labs) Software Solaris V4.67 (data from SciFinder®). * = Calculated using AdvancedChemistry Development (ACD/Labs) Software Solaris V4.67 (data from SciFinder®). ** = Apparent 1:1 binding constant. Unless otherwise noted, the comparison and test dosage forms were the same with thecomplex or physical mixture replaced by drug. UCD CD:drug is based on water solubility, unless otherwise specified, and on 1:1 complex formation and apparent 1:1 binding constants. Lines separating rows separatestudies. Shaded rows correspond to reports that explicitly mentioned the influence of CD on the stability of the compound.
Table 1 (continued )
84R.L.Carrier
etal.
/Journal
ofControlled
Release
123(2007)
78–99

Table 2Summary of drug, cyclodextrin, and dosage form parameters for studies in which cyclodextrins were not successfully utilized to enhance bioavailability
Drug (species) pKa clogPMW
Watersolubility(mg/mL)
Buffered solubility(mg/mL)
Dosageform
Complexformationmethod
Dose(mg)
DosedCD:Drug(molar)
UCD CD:Drug(molar)
CD type,CD:Drug
Bindingconstant(M−1)
Otherformationcomponents
Comparisondosage form
AUC increase(x AUCcontrol)
Tmax
change(hr)
Cmax
change(μg/ml)
Glibenclainide[26] (dog)
5.3 (A) 3.93494
6.18e−3 (pH 7.4);2.3−4 (pH 3.0)
Physicalmixture
– 3 29:1 β-CD1:1
827(pH 7.4)
Gelatincapsule,dosed withwater
Drug (incapsule,with water)
No change 4.5–3.5
0.084–0.12
Indomethacin[38] (rabbit)
4.2⁎(A) 3.11358
0069[49]
b3.578 (pH 1,4); N3.578,b35.78 (pH 7,8),N35.78,b357.8 (pH 10)⁎
Complex Freeze-drying
50 1:1 10.8(K=5300),100.1(K=523)
β-CD1:1[56]
5300[51],523 [57]
Dosed withwater
Freeze-dried drug(with water)
No change
Naproxen [19](human)
44⁎ (A) 3.0230
0.04(pH 4)
b2.30 (pH 1,4); N23.03,b230.3 (pH 7,8); N230.3(pH 10)⁎
Complex Freeze-drying
200 1:1 5.2 β-CD1:1
1378(pH=1,25 °C)
Gelatincapsule
Drug (ingelatin capsule)
No change
Freeze-drieddrug (in gelatincapsule)
No change
Rutin [12](dog)
6.8⁎(A) 2.23611
.045 [59] b6.11 (pH 1,4,7,8);N61.05,b610.5 (pH 10)⁎
Complex(tablet)
Slurry(ethanol–water)/kneading/drying
200 1:1 52.0 β-CD1:1
266 Starch Tablet(complexreplaced by drug)
No change
Tolbutamide[46] (rabbit)
2.34270
0.1053[49]
b2.70 (pH 1,4); N2,70,b27.04 (pH 7); N27.04,b270.4 (pH 8); N270.4(pH 10)⁎
Physicalmixture
– 100/kg
1:1 β-CD2:1 [45]
196 [45] Drug No change(serumglucosevariationcoefficient)
Notations are the same as those described for Table 1.
85R.L.Carrier
etal.
/Journal
ofControlled
Release
123(2007)
78–99

Fig. 1. Structures of compounds used in studies, summarized in Tables 1 and 2, where cyclodextrins were employed to enhance bioavailability.
86 R.L. Carrier et al. / Journal of Controlled Release 123 (2007) 78–99
device, and it would thus be likely that devices formulated withphysical mixtures of these highly soluble cyclodextrins wouldperform in vivo in a similar fashion to devices formulated withcomplexes. It should be noted that formulation with a physicalmixture rather than a complex is desirable from a processingviewpoint, since the steps involved in making the complexcould be skipped in the manufacturing process.
2.4. Complex formation methodology
While most studies utilizing cyclodextrins to enhancebioavailability employ a drug-cyclodextrin complex, themethod of preparation of the complex varies, as can be seenin Table 1. Investigators have used freeze-drying, spray-drying,and co-precipitation of a cyclodextrin/drug solution, as well as

87R.L. Carrier et al. / Journal of Controlled Release 123 (2007) 78–99
simple grinding with a mortar and pestle of a slurry of drug andcyclodextrin [81]. The method of preparation of the complexcan greatly influence the dissolution kinetics, and, presumably,the bioavailability enhancement obtained with a complex[23,39,40,71]. This is logical in light of the fact that certainmethods of preparation can result in more or less complexformation, a factor that is rarely quantified, as well as changes inthe particle size and degree of amorphous nature of the resultingmaterial, although the cyclodextrin-drug complex is oftenamorphous. Material with a smaller particle size (greater surfacearea per unit volume of material) and amorphous material willgenerally have faster dissolution kinetics. These differences incomplex formation methodology, therefore, make it somewhatdifficult to make clear comparisons between studies. In somestudies, the particulate matter resulting from complex formationhas been sieved so that only a specific particle size was used inthe study [12,38–40]. Care has been taken in some studies tosubject the comparator formulation (e.g., drug alone) to thesame processing as the complex, minimizing effects ofprocessing on any observed increases in dissolution kineticsor bioavailability [38].
2.5. Immediate vs. controlled release
All studies referenced in Tables 1 and 2 and most studiesemploying CD to enhance bioavailability in general haveinvolved immediate release dosage forms. There are severalexamples of the use of cyclodextrins in controlled-releasedosage forms in the literature, but unfortunately very littleinformation on their affect on bioavailability. Cyclodextrinshave been shown to both increase and decrease the rate of drugrelease from controlled-release devices. Increases in release ratecould be due to increase in solubility of the complex relative tothe drug alone and associated increase in drug in solution in thereleasing device. Decreases have been attributed to thedecreased diffusivity of the bulky complex relative to thedrug alone. Giunchedi et al. used complexation of the insolubledrug naftazone with beta-cyclodextrin (β-CD) and hydroxy-propyl beta-cyclodextrin (HP-β-CD) to enhance dissolutionkinetics from hypromellose matrix tablets [82]. The influence ofcyclodextrin on prednisolone and carbamazepine release fromhydroxypropylmethylcellulose (HPMC) matrix tablets has beeninvestigated [21,79], and it was found that cyclodextrinincreased drug dissolution rate, with the increase being greaterwhen the drug and cyclodextrin were formulated as a complexrather than a physical mixture. Quaglia et al. [83] reported thatinclusion of cyclodextrin in a formulation of nicardipine incrosslinked polyethylenglycol (PEG) hydrogels decreasedrelease rate. The authors attributed this result to the decreasein the diffusivity of drug when it is complexed to cyclodextrin(due to increase in effective molecular size), and quantitativetreatment of this phenomenon was presented. Similarly,Sangalli et al. [84] found that inclusion of β-CD hinderedrelease of poorly soluble drugs from hydrophilic matrices(HPMC) relative to matrices containing drug and lactose, whileit increased release rate from inert matrices (acrylic resins). Thisresult was attributed to the complex having difficulty diffusing
through the matrix of hydrophilic polymer chains in thehydrated HPMC tablet. In one study, the gel-forming propertiesof HP-β-CD were utilized to design a controlled-release matrixfor metoprorol [85].
Cyclodextrins have also been used in osmotic systems toenable delivery of low solubility compounds. In a patent ofStella et al., examples of controlled-release formulationscontaining cyclodextrins, including multilayer tablets andosmotic formulations, are presented [75]. This same patentprovides examples from the literature of the use of cyclodextrinsin controlled-release formulations. In a separate reference,Stella et al. discuss the relative importance of osmotic anddiffusional components of release kinetics in osmotic pumptablets containing cyclodextrins [86]. It has been demonstratedthat certain cyclodextrins, especially sulfobutyl ether cyclodex-trins, can have sufficient osmolality to act as osmotic agents inan osmotic tablet, and the factors affecting release incyclodextrin-containing osmotic tablets have been studied[76–78,87,88]. Hydrophobic cyclodextrins have been utilizedin controlled-release formulations mainly as the controlled-release agent, as they slow the release of soluble activecomponents [13,63,66]. Enteric type cyclodextrins have beenused to prevent drug release in the stomach [89]. Covalentlinkage with hydrophilic cyclodextrins (as opposed to non-covalent interactions typically involved in complex formation)has been used to provide site-specific release in the cecum andcolon, where the covalent cyclodextrin-drug link is broken bymicroflora enzymatic activity [66,90]. For example, covalentbonding of α-cyclodextrin has been utilized to target drugrelease to the colon [90].
Special consideration of the use of cyclodextrins in oralcontrolled-release dosage forms is warranted as they aretypically designed to release drug throughout a portion of GItransit, and the variable GI environment can alter the influencethat cyclodextrin ultimately has on drug solubility. As a dosageform travels through the GI tract, the changes in physiologicalenvironment (e.g., pH, water content, bile salt concentration,motility) can influence the dissolution kinetics and solubility ofdrugs, cyclodextrins, and complexes, especially, as mentionedabove, if the drug and/or cyclodextrin is likely to change itsionization state with the changes in physiological pH that occurin the GI tract. The stability constant of the complex is alsodependent on pH, especially if the drug is ionizable [26,30,63].A charge on a drug can offset the affinity of the hydrophobicportion of the molecule for the cyclodextrin cavity. Thus, thechange in pH during GI transit can influence the strength ofdrug interaction with cyclodextrin and ability of cyclodextrin tosolubilize the drug. It is therefore expected that a dosage formthat slowly delivers drug during GI transit may demonstratedifferent pharmacokinetic changes with the inclusion ofcyclodextrin than a dosage form that delivers all drugeffectively at one time to the upper GI tract. Supportingevidence for this statement is found in comparing bioavailabil-ity enhancement observed with dosing to different areas of theGI tract. When carmofur complexed with DM-β-CD, trimethylbeta-cyclodextrin (TM-β-CD), and β-CD was dosed orally torabbits, increases in AUC of 7.5, 3, and 3 times, respectively,

88 R.L. Carrier et al. / Journal of Controlled Release 123 (2007) 78–99
were seen over the AUC resulting from drug dosed alone.However, when the same complexes were dosed rectally, onlythe DM-β-CD showed a dramatic increase in AUC over drugalone (3.3, 1.4, and 1.2 times the control for DM-β-CD, TM-β-CD, and β-CD, respectively) [28]. The change in magnitude ofbioavailability enhancement could be related to the lower watercontent or higher pH in the rectum compared to the upperintestine altering the amount of complex formation. In adifferent study, indomethacin labeled with 14C was dosed aloneor as a complex with β-CD. When dosed to the small intestine,56% of a dose of indomethacin alone was absorbed in the smallintestine, while 6% was absorbed when dosed to the largeintestine. However, in the case of complexed indomethacin,absorption values were 68 and 66%, respectively, demonstrat-ing a more pronounced influence of complexation on absorptionin the lower GI tract [91]. In a study aimed at improving oralbioavailability of artemisinin through complexation with β- andγ-cyclodextrin, the statement was made that colonic absorptionwas “poor and negligible” regardless of whether or not thecompound was complexed [27]. It was clear in the cited studythat the comparator for the dosed complexes, the commercialformulation Artemisinin 250®, stopped being absorbed approx-imately at the time it reached the colon, with percent absorptionleveling off at 60% of the dose. However, in the cases of thecomplexes, nearly 100% of the dose was absorbed by the timethe dosage form reached the colon, making it difficult to drawany conclusions regarding the influence of cyclodextrin onabsorption in the colon. Several other studies have demonstrat-ed enhanced bioavailability using cyclodextrins of rectallydosed compounds [5,63,92]. It is evident from the studies citedabove that there is not a clear understanding of the relativeability of cyclodextrins to enhance bioavailability in the lowerGI compared to the upper GI. Such information, especially forcompounds that have very different solubilities at the pH of thelower and upper GI, would be particularly useful to theformulation scientist attempting to formulate controlled-releasedosage forms containing cyclodextrins.
2.6. Ionized vs. neutral drugs
As demonstrated in Table 1, most studies to date utilizingcyclodextrin to enhance oral bioavailability did not utilize saltforms of active compounds or consider the ionized state of thecompound upon dosing. This statement is based, however, onlack of mentioning in the references of the use of a salt form, andit is possible that specific information related to use of salt formsmay have been omitted from some references where they wereactually used. It is noted that all compounds listed in Table 2 willbe ionized in the small intestines (pH 5 to 7), while only a portionof those listed in Table 1 will be. As described above, the ionizedstate of the active compound and the presence of counterions arelikely to affect the drug's binding constant with cyclodextrin[93–95], and a decrease in binding constant with ionization ofdrug is often observed. An opposite effect can be observed,however, in cases where a charged cyclodextrin derivative (e.g.,anionically charged sulfobutyl ether beta-cyclodextrin (SBE-β-CD)) interacts with a drug of opposite charge [95]. It has also
been demonstrated that a salt form of a compound can exhibit agreater binding constant with cyclodextrin than the free basedrug, and it is believed this is due to the association of thecounterion with the charged drug in the complex [94]. In the caseof ziprasidone, the binding constant of the complex of theziprasidone mesylate ion pair with SBE-β-CD was 7892 M−1
compared to 957M−1 for the complex with the dissociated ioniccompound. A lower binding constant due to charge does notnecessarily mean that cyclodextrins cannot be used to solubilizea compound. In fact, a combination of pH adjustment (used todeliver drug in an ionized and more soluble state) andcomplexation with cyclodextrin has been used to successfullysolubilize compounds [96].
Quantitative consideration has been given to the influence ofthe ionized state of the drug on binding constant and utility ofcyclodextrin to solubilize the drug [93,96]. Rao and Stella [93]demonstrate theoretically that the decrease in binding constantassociated with charge on a compound relative to the bindingconstant with the neutral compound (ranging in the studiesconsidered from 40-fold to no appreciable decrease [95–99]) isoften outweighed by the accompanying increase in solubility ofthe ionized compound. Another consideration of the synergism ofionization and complexation is given by Li et al. [97]. The authorsderive the theoretical increase in total drug solubility with ion-ization and complexation and provide experimental validation.
2.7. Dose and molar CD:drug ratio
Examination of the typical drug and cyclodextrin propertiesand doses used in studies where cyclodextrins were shown toenhance bioavailability reveals that the majority of the dosesused were relatively low (b 100 mg in 25 out of 29 studies).Many of the studies dosed drug as a suspension or a powder withwater, enabling a greater dose than would be possible in aconventional oral dosage form such as a tablet or capsule. Theuse of cyclodextrins in solid oral dosage forms, in particular, islimited to low doses with relatively large stability constants dueto the relatively large size of cyclodextrin molecules and massand size limitations of oral dosing [5,6,67]. For example, in thecases of α-, β-, and γ-cyclodextrins (MW = 972, 1132, and1297 g/mol, respectively), 100 mg of 1:1 molar complexcontains only approximately 5–25mg of a drug with amolecularweight of 500. Most probably for similar reasons, the molar ratioof cyclodextrin:drug utilized was low in most of the formula-tions studied, with more than half of the comparisons involving amolar ratio of cyclodextrin to drug of 2:1 or less. The amount ofcyclodextrin necessary to create a desired increase in bioavail-ability for a given dose of drug is dependent on a number offactors including the binding constant and the physicochemicalproperties of the drug and cyclodextrin (e.g., solubility), all ofwhich influence the various processes occurring during deliveryof the drug in the GI environment (e.g., dissolution andabsorption), as described below (See “Section 3 Explanationsfor ability of cyclodextrins to enhance bioavailability”).
Most of the literature concerning the use of cyclodextrins toenhance bioavailability does not discuss the required amount ofcyclodextrin in quantitative terms. In the previously mentioned

89R.L. Carrier et al. / Journal of Controlled Release 123 (2007) 78–99
patents of Stella et al. [74,75], it is stated for the particular typesof cyclodextrins and drug delivery devices discussed that themolar ratio of CD:drug should be in the range of 1:1 to 20:1.Rao and Stella presented a theoretical consideration of theappropriateness of cyclodextrins as a solubilizing technology inwhich the ability of a given amount of cyclodextrin toadequately solubilize a given drug dose was determined bywhether or not a dimensionless parameter, “cyclodextrin utilitynumber,” (UCD) was greater than or less than one [93]. Thistreatment is based on the fact that a UCD number greater thanone indicates that the cyclodextrin amount is sufficient tosolubilize the entire dose of drug. In order for this condition tobe met, the dose per unit available volume of solution must beless than or equal to the total solubility of the drug in thepresence of the cyclodextrin. Here “solubility” refers to themaximum amount of drug that can be in solution at equilibrium,including both free and complexed drug. Therefore, thesolubility in the presence of cyclodextrin is the sum of thefree drug solubility and the maximum equilibrium concentrationof complex in solution. To determine an expression for thissolubility, first consider the definition of the binding constant(K). The binding constant describes the equilibrium betweendrug and cyclodextrin. For a 1:1 complex:
K ¼ com½ �CD½ �f drug½ �f
ð1Þ
The binding constant can also be expressed in terms of thetotal molar amount of both bound and free cyclodextrin, CDtotal,for a given volume V:
K ¼ com½ �CDtotal=V � com½ �ð Þ drug½ �f
ð2Þ
Rearranging and solving for [com],
com½ � ¼ K drug½ �f1þ K drug½ �f� �
CDtotal
Vð3Þ
The maximum complex concentration is present when thedrug concentration is equal to the free drug solubility, So.Making this substitution, the maximum solubility of a drug inthe presence of a given molar quantity of cyclodextrin is:
drug½ �total ¼ So þ KSo1þ KSo
CDtotal
Vð4Þ
Thus, the requirement described by Rao and Stella for agiven molar dose of drug (Dtotal) is:
Dtotal
VV So þ KSo
1þ KSo
CDtotal
Vð5Þ
This can be rearranged to:
SoVDtotal
þ KSo1þ KSo
CDtotal
Dtotalz1 ð6Þ
The first term is the inverse of the dose number, adimensionless number that has been used to assess the ability of
a given dose of drug to be delivered based on solubility. It can beassumed to bemuch less than one in caseswhere cyclodextrins arebeing used to enhance solubility and dissolution. The second termis the UCD defined by Rao and Stella. Thus, the ability of a givenamount of cyclodextrin to solubilize a dose of drug is dependenton the drug's solubility and the binding constant with cyclo-dextrin. A less obvious but still important factor is the solubility ofthe cyclodextrin, which is assumed in the analysis not to be alimiting factor.
It is interesting to compare the theoretical ratio of CD:drugrequired according to the UCD with what has actually been usedin the literature. In Table 1, the molar ratio of CD:drugnecessary for a UCD of one has been calculated for studies inwhich the necessary information was able to be obtained. Thewater solubility, when available, was used to calculate the UCD.If the water solubility was not available, the solubility at aspecific pH, as indicated in the table, was used. It is evident thatenhancement in bioavailability has been reported when a levelof cyclodextrin below the UCD-predicted amount has beenutilized. Of the studies in Table 1 about which enoughinformation was able to be obtained to compare a CD:drugmolar ratio necessary for a UCD of one and the dosed CD:drugmolar ratio, 20 utilized a CD:drug ratio less and 5 utilized a CD:drug ratio greater than that predicted to be necessary by theUCD. There appears to be no clear correlation of the differencebetween the utilized and UCD-predicted CD:drug molar ratiowith the magnitude of the AUC increase. It should be noted thatconsiderable error can be introduced into the UCD CD:drugmolar ratio calculation by the variation that is seen in reportedsolubility and binding constant values, making it possible thatthe values calculated are not exactly those relevant to the studyat hand. For example, the binding constants reported for β-CDand piroxicam in two different studies were 101 and28,000 M−1, leading to UCD-predicted necessary CD:drugmolar ratios of 1.9 and 103, respectively [23,41]. However, itappears that it is not always necessary for the cyclodextrinamount in a given formulation to be adequate to solubilize theentire dose for enhancement of bioavailability. A very high CD:drug molar ratio, in fact, can lead to a decrease in bioavailabilitydue to a decreased free drug concentration in the intestinallumen when a very large amount of drug is bound tocyclodextrin.
2.8. Type of CD used
Both natural cyclodextrins and cyclodextrin derivatives havebeen used to enhance bioavailability, as can be seen in Table 1.Cyclodextrin derivatives often have a higher solubility thannatural cyclodextrins, and they may have different bindingconstants with a given compound, as well. This can result indifferent levels of bioavailability enhancement using naturalcyclodextrins vs. derivatives [44,45]. For example, when the β-CD and HP-β-CD complexes of rutin were dosed, β-CD had noinfluence on bioavailability, while HP-β-CD resulted in a 2.9times increase in the AUC [12]. Similarly, when salbutamol wasdosed as the perbutanoyl-β-CD (TB-β-CD) complex, the AUCwas increased 4.6 times in comparison to dosing of drug alone,

90 R.L. Carrier et al. / Journal of Controlled Release 123 (2007) 78–99
while it was only increased 1.7 times when dosed as the β-CDcomplex [13].
2.9. Binding constant magnitude
A range of binding constant values of 0 to approximately100,000 M−1 have been reported for cyclodextrin complexes inthe literature, with 0 corresponding to absence of binding [6].Very weak binding is roughly characterized by a bindingconstant less than 500 M−1, while weak, moderate, strong, andvery strong binding are characterized by binding constants inthe ranges of 500–1000 M− 1, 1000–5000 M−1, 5000–20,000 M−1, and greater than 20,000 M−1, respectively. Themean binding constant values of pharmaceutical compoundsand α, β, and γ-CD were determined to be 129, 490, and355 M−1 when a large number of complexes were statisticallyanalyzed [93,100,101]. Of the 46 comparison for which bindingconstant magnitudes were able to be found (Table 1), 23 hadvery weak binding constants, while 5, 5, 10, and 3 had weak,moderate, strong, and very strong binding constants, respec-tively. It has been suggested in the literature that error may existin reported binding constants, for example if they are measuredassuming 1:1 binding when a different stoichiometry actuallyexists in the complex [101–103].
The AUC increase is plotted vs. the binding constant inFig. 2. It is clear that there is no correlation between bindingconstant and increase in AUC for the studies examined. Themajority of the studies surveyed involved lower binding constantvalues. It also appears that as the binding constant increases,there may be a decrease in the maximum AUC increase that canbe achieved. It has been reported in the literature that themagnitude of binding constants is similar to molar ratios of CD:drug in that if it is too big, a decrease in bioavailability over drugdosed alone can actually result, while if it is too small, there maynot be any effect of cyclodextrin [7]. A theoretical model of acyclodextrin-drug system developed by Szejtli predicts thatdosing a complex of cyclodextrin and drug at a 1:1 molar ratioshould result in increased blood plasma levels of the drug over areasonable range of binding constants (500–10,000 M−1). Themodel also predicts, however, that it is possible with a highbinding constant (e.g., greater than approximately 10,000 M−1)
Fig. 2. Plot of AUC increase vs. binding constant. The y-axis represents thefactor by which the AUC was increased over the AUC when cyclodextrins werenot used (i.e., the ratio of these two AUC values).
and a large molar excess of cyclodextrin to obtain a lowerbioavailability in a system containing cyclodextrin than if drugalone were dosed [5,104]. If a complex with a very high bindingconstant is dosed, the complex may not dissociate appreciably,and the complex itself is not absorbed [63]. Complexation withagents other than cyclodextrin is known to be able to decreaseabsorption if the complexed species is not able to be absorbed[105,106].
One strategy for displacing drug that is tightly bound tocyclodextrin is to co-dose a competitive binding agent. For ex-ample, complexation of cinnarizine with β-CD resulted in AUCvalues 8.0 and 1.4 times that of drugwhen dosedwith andwithoutphenylalanine, respectively [34,107]. Interestingly, dosing ofuncomplexed drug with phenylalanine resulted in a decrease inAUC and Cmax and an increase in Tmax relative to dosing drugalone. It has been demonstrated that drug can also be displacedfrom a complex by lipids in the rectum, mucus, and bile [63].
2.10. Interactionwith polymers and other formulation components
While most of the studies surveyed in Table 1 involved dosinga complex of drug and cyclodextrin as a powder alone or in agelatin capsule with water, some also included other excipients.As the presence of other excipients, including polymers, isknown to possibly influence the interaction between drug andcyclodextrins, it is important to take these factors intoconsideration when reviewing the literature in search of guide-lines for using cyclodextrins to enhance bioavailability. Theability of water-soluble polymers to enhance the solubilizingeffect of cyclodextrins and thus possibly reduce the amount ofcyclodextrin necessary in a given dosage form has beendemonstrated [14,26,108–110]. Formulations containing awater-soluble polymer (e.g., HPMC or polyvinylpyrrolidone,PVP) have been able to achieve bioavailability enhancementequivalent to formulations containing up to 80% less cyclodex-trin [26]. Such results are generally attributed to a synergisticsolubilizing effect of polymer and cyclodextrin believed to bedue to formation of ternary complexes or co-complexes betweendrug, cyclodextrin, and polymer [110]. Polymers such as water-soluble cellulose derivatives can form complexes with cyclo-dextrin that have different physicochemical properties than thoseof the cyclodextrin alone. For example, the solubility of thecyclodextrin and/or the apparent binding constant between drugand cyclodextrin can be changed in this manner [108].
It should be noted that formulations of drugs alone with thesepolymers also often lead to enhancement in bioavailability, andthese polymers are known to interact with and solubilize drugs.For example, when tacrolimus was dosed to rats in acommercial PROGRAF tablet containing HPMC and comparedto drug alone, it resulted in an AUC0–12 increase of 3.6 times, anincrease in Cmax from 1.6 to 11.2 ng/ml, and a decrease in Tmax
from 0.5 to 1.3h, effects comparable to those observed whentacrolimus was dosed with a 50:1 molar ratio of DM-β-CD [44].
Formulation of cyclodextrins with hydroxy acids or salts ofbasic drugs can also enhance their solubilizing effects [14,111].There is often a synergistic effect observed in dosing an acidwith a cyclodextrin, such that the total solubility enhancement

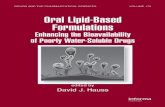
Fig. 3. Diagram of the processes in the intestinal drug delivery system when adrug is dosed either as a physical mixture or a complex with cyclodextrin.Processes occurring that are influenced by the presence of cyclodextrin includedissolution of drug and/or complex, precipitation of drug (if free drugconcentrations exceed equilibrium solubility), complexation of drug andcyclodextrin, and absorption of drug. These processes interact to determinethe change with time in amount of solid (drug or complex); drug, cyclodextrin,and complex in solution; and absorbed drug. The properties of the drug,cyclodextrin, and intestinal environment determine the kinetics of theseprocesses and their effects on overall component absorption.
91R.L. Carrier et al. / Journal of Controlled Release 123 (2007) 78–99
observed via dosing with both acid and cyclodextrin is greaterthan the predicted combined effect from dosing with each alone.There are several examples in the literature of using cyclo-dextrins together with acids to enhance solubility, dissolutionkinetics, and bioavailability, and several theories of possibleinteractions between drug, acid, and cyclodextrin have beenproposed [111]. Other formulation components, including salts,surfactants, preservatives, and organic solvents are known toinfluence and often reduce the efficiency of binding betweendrug and cyclodextrin. For example, the inclusion of non-ionicsurfactants has been shown to decrease binding of cyclodextrinto diazepam due to competitive binding of the surfactant to thecyclodextrin [112]. Formulation component effects can berelated to change in charge on the drug or cyclodextrin, asdescribed above, as well.
3. Explanations for ability of cyclodextrins to enhancebioavailability
3.1. Significance
What are the properties of drug, cyclodextrin, deliverydevice, and/or physiological environment necessary for cyclo-dextrins to enhance oral bioavailability? Answers to thisquestion in the form of general guidelines are found inreviewing the literature, as described above and demonstratedin Table 1 for cases where the solubilization properties ofcyclodextrins were specifically utilized. For example, it isevident that most studies in which cyclodextrins have been usedto enhance oral bioavailability involve hydrophobic (logP N2.5), low solubility (1 μg/ml–1 mg/ml) compounds with a doseof less than 100 mg and a CD:drug ratio of 2:1 or less. Similargeneral guidelines were outlined above for binding constantmagnitude and dosing of a physical mixture vs. a complex.However, these are rough guidelines true of most studies, but itis evident from the discussion above that there are manyexceptions to these general rules. In the limited range of studiesreviewed, there was no clear correlation between properties ofdrug (e.g., solubility, binding constant with cyclodextrin) orexperimental parameters (e.g., type of cyclodextrin used, dose)that could give definitive, quantitative guidance regarding whenand how cyclodextrins can be used for bioavailabilityenhancement. This is likely related to the lack of informationregarding failed attempts to use cyclodextrin to enhance oralbioavailability and the wide range of variables associated witheach study performed (method of preparation of complex, typeof cyclodextrin used, type of dosage form, animal species, etc.)that make it difficult to assign boundaries to key parametersbased on available data. In addition, the drug and cyclodextrinproperties and experimental parameters interact to simulta-neously influence processes in the intestinal drug deliveryenvironment, so that looking at one parameter of this system inisolation provides limited information.
Further insight can be found in consideration of whatphenomena in the drug delivery environment are affected by thepresence of cyclodextrin and how, ultimately, overall drugabsorption is influenced by these changes. These phenomena
are described below. The text is organized according to commonexplanations for bioavailability enhancement provided in theliterature followed by theoretical consideration of theseexplanations. This theoretical consideration could provide thebasis for quantitative analysis of the simultaneous influence ofthe properties of the cyclodextrin-drug-dosage form system onkey processes in the drug delivery environment that determinebioavailability enhancement.
3.2. Enhancement in dissolution kinetics
The main cited reasons for enhancement in bioavailabilitywith inclusion of cyclodextrins in a dosage form are increase indissolution kinetics and increase in solubility, and it is oftenstated that cyclodextrins will increase bioavailability when therate-limiting step in drug absorption is dissolution rather thanpermeation through the intestinal membrane [7,20,66]. Most ofthe compounds listed in Table 1 have low solubility, and, asdiscussed above, most of the studies cited specifically refer tothe low solubility and slow dissolution of the compound asmotivating factors for studying the influence of cyclodextrin onbioavailability. Many of the compounds listed in Table 1 arereported to have both low and variable absorption, character-istics associated with low solubility and slow dissolutionkinetics [18,22,26,37]. In many of the studies cited, theinfluence of cyclodextrin on the dissolution kinetics of thecompound is measured in vitro.
As depicted in Fig. 3, once solid drug is delivered to thegastrointestinal tract as either free drug, physical mixture withcyclodextrin, or complex with cyclodextrin, dissolution andpermeation across the intestinal membrane must occur in orderfor the drug to be absorbed. If the dissolution kinetics arelimiting in the overall absorption process, enhancement of

92 R.L. Carrier et al. / Journal of Controlled Release 123 (2007) 78–99
dissolution kinetics via dosing a physical mixture withcyclodextrin or dosing a complex will likely increasebioavailability. The enhancement in dissolution kineticsbrought about by dosing a physical mixture of drug andcyclodextrin is related to the fact that the dissolution of drug willinvolve the flux of both free drug and complexed drug awayfrom the drug particle surface if cyclodextrin is present in theimmediate environment [63]. In the classical Noyes–Whitneydissolution expression for a drug particle in the absence ofcyclodextrin, dissolution rate is proportional to the concentra-tion gradient across the unstirred boundary layer surrounding adissolving particle in a well-mixed compartment. For a neutralcompound:
ddrugfdt
¼ � kdis So � drug½ �f� �� � ð7Þ
kdis ¼ ADdrug
lblð8Þ
The concentration of drug at the drug particle surface is takenas its solubility (So), and the concentration at the edge of theboundary layer is taken as the concentration of drug in the well-stirred intestinal lumen ([drug]f). The rate constant is equal tothe ratio of the product of the diffusivity of the drug (Ddrug) andthe surface area (A) to the length of the unstirred boundary layer(lbl). When cyclodextrin is present in the environment of thedissolving drug particle, the rate of dissolution is nowproportional to an additional “driving force”: the difference incomplex concentration at the particle surface and in the bulkintestinal fluid [113]:
ddrugfdt
¼ � A
lblDdrug So � drug½ �f
� �þ Dcom com½ �surface � com½ �� �� �
ð9Þ
Dissolution kinetics of complex are usually enhanced overthose of both the drug alone and the physical mixture [70,71].For some drugs, the dissolution of drug alone or as a physicalmixture with β-CD is indistinguishable, while the complex ofdrug and β-CD demonstrate much faster dissolution kinetics(e.g., 90% vs. 25% dissolved in water in 10 min) [29,35,114].This is related to the physical properties of the complex. Thecomplex of a low solubility drug typically is more hydrophilicand has a higher solubility than the free drug itself. In addition,in the case of the derivatized cyclodextrins, the complex isusually amorphous. Water molecules break up amorphousmaterial with relative ease in comparison to crystalline drug[25]. Replacement of the first term in Eq. (7), So, with theenhanced solubility of the complex results in a much greaterdriving force for dissolution. It is possible that the method offormation of the complex will also result in an increased surfacearea in relation to the surface area of dissolving drug alone orphysical mixture, increasing the dissolution rate constant in Eq.(7). As a result of these various factors, the complex willdissolve faster than the drug alone or the physical mixture [63].There are reports of low solubility inclusion complexes that will
tend to precipitate, however, especially if formed from one ofthe parent cyclodextrins [14,24]. This type of behavior givesrise to what Higuchi defined as a B-type phase-solubilitydiagram [115].
Enhancement in dissolution kinetics is not always accom-panied by enhancement in bioavailability. For example, in astudy in which the β-CD and HP-β-CD complexes of rutin werestudied, both cyclodextrins had comparable affects on dissolu-tion kinetics and stability, but only HP-β-CD increasedbioavailability [12]. When indomethacin was processed as afreeze-dried complex with β-CD, it showed increased dissolu-tion kinetics over freeze-dried drug alone. However, when thecomplex and drug were dosed to rabbits, there was no increasein percent drug recovered in urine with dosing of the complex[38]. These results highlight the importance of gainingunderstanding of all the interconnecting factors influencingabsorption when a cyclodextrin-drug system is dosed. It isimportant to determine what the rate-limiting step is inabsorption of the compound when cyclodextrin is not presentand then assess the ability of cyclodextrin to influence this rate-limiting step.
3.3. Increase in solubility
Along with an increase in dissolution kinetics, increase insolubility is often cited as being responsible for enhancedbioavailability when dosing drug with cyclodextrins [24].Solubility can be a key factor in kinetics of dissolution (Eq.(7)) and can also influence permeation through the intestinalmembrane by influencing the concentration of drug in solutionin the intestinal lumen. Thus, low solubility is often blamed forlow bioavailability. It is useful to clarify what is meant by the“increase in solubility” brought about by cyclodextrins,however, in order to evaluate their ability to enhancebioavailability. In the presence of cyclodextrin, the total amountof drug in solution is equal to the sum of free drug and complexin solution. As described above in “Dose and molar CD:drugratio” in the discussion of the cyclodextrin utility number [93],the maximum value that this total amount of drug in solutioncan have is the sum of the solubility of the drug itself and theamount of complex formed when the free drug concentration insolution is the drug solubility. Thus, for a neutral compound:
drug½ �total ¼ drug½ �f þ com½ �f V So þ KSo1þ KSoð Þ
CDtotal
Vð10Þ
Similar expressions can be written for the total amount ofionizable compound in solution in the presence of cyclodextrinbased on the binding constant with ionized drug [96]. This totalamount of free drug and complex is typically referred to as“enhanced solubility.” For example, the solubility of prednis-olone in water at room temperature is 0.25 mg/ml, while thesolubilities in the presence of 15 mg/ml β-CD and DM-β-CDare 3.4 mg/ml and 3.3 mg/ml, respectively [5]. This enhancedsolubility forms the basis for the theoretical treatment of amountof cyclodextrin required in a formulation provided by Rao andStella [93]. It is important to note, however, that the value of the

93R.L. Carrier et al. / Journal of Controlled Release 123 (2007) 78–99
free drug concentration at equilibrium will not exceed thesolubility of the free drug. This is a key point as the rate ofpermeation through the intestinal membrane is dependent on thefree drug concentration in the intestinal lumen:
ddrugabsdt
¼ ka drug½ �fVlumen ð11Þ
Although there are studies in which transport of cyclodex-trins across the intestinal membrane has been reported [116], itis generally accepted that neither the complex nor freecyclodextrin are absorbed to an appreciable extent [7,66,117].Thus, based on the dependence of absorption on free drugconcentration (Eq. (11)), the equilibrium “enhanced solubility”brought about by cyclodextrins described by Eq. (10), on itsown, will not enhance rate of permeation through the intestinalmembrane. In fact, it is possible that complexation withcyclodextrin, especially in cases where the binding constant ishigh, will reduce the absorption rate due to the fact that thecomplex is not absorbed and the free drug concentration can bereduced by binding [34].
In spite of the apparent inability of cyclodextrins to increasethe equilibrium free drug solubility, there are ways thatcyclodextrins can result in free drug concentration greater thanthe solubility in the intestinal lumen for a transient period oftime. For example, if the complex is dosed, it will disassociate asit goes into solution to an extent determined by the bindingconstant and concentrations of drug, cyclodextrin, and complexin the intestinal lumen. Association and disassociation are oftenassumed to be instantaneous in comparison to the kinetics ofdissolution and permeation through the intestinal membrane,and free drug molecules can be considered to be in pseudo-equilibrium with molecules bound in the cyclodextrin cavity atall times [14,118]. Free drug and cyclodextrin will precipitate iftheir concentrations in solution, as dissolution and decomplexa-tion are taking place, are higher than their equilibriumsolubilities [119]. However, if dissolution of the complex anddisassociation are rapid enough relative to precipitation, dosingof a complex can result in free drug concentration higher than thesolubility of the drug for a period of time [5,7,63,104]. This canlead to increased drug absorption through the intestinalmembrane. Water soluble polymers (e.g., hydroxypropylcellulose (HPC) or PVP) have been used to prolong thesupersaturated state brought about by complex dissolution [7].A second way that cyclodextrins may enhance free drugconcentration is by slowing the precipitation of free drug [5].Precipitation kinetics are proportional to the drug concentrationand thus are reduced when some of the drug is bound bycyclodextrin. In addition to dosing a complex, dosing a salt formof the drug can result in transient concentrations of free drughigher than the equilibrium solubility.
Another cited method of using cyclodextrins to enhancebioavailability related to dissolution kinetics and solubility isthrough the formation of nanospheres. Amphiphilic CDs, suchas native CDs derivatized on secondary hydroxyl groups withalkyl chains, are capable of self-assembling into nanospheresthat can be loaded with drug [66,120]. The molecularly
dispersed drug is released rapidly from the nanospheres,enhancing dissolution rate for low-solubility compounds.
3.4. Decrease in degradation kinetics
Stability of many compounds has been enhanced viacomplexation with cyclodextrins, as has been extensivelyreviewed in the literature. Stability can be enhanced either inthe dosage form itself, by inhibiting polymorphic transitions, forexample [121], or once the drug is actually dosed. Of the studiespresented in Table 1, reports in which explicit mention wasmade of compound stability issues are highlighted. In thesehighlighted studies, the bioavailability of the drug molecule isgenerally known to be influenced by its degradation rate, and insome studies bioavailability enhancement using cyclodextrinswas at least partially attributed to the stabilizing effect ofcyclodextrin on the drug molecule. As many of these studiesinvolve low-solubility compounds, it is difficult to determine ifthe bioavailability enhancement is due to the effect ofcyclodextrins on dissolution, degradation, or both. Binding ofcyclodextrin can reduce the reactivity of a drug by shielding thedrug molecule from attack and/or changing the chemical andphysical stability of the molecule itself via conformationchanges, for example. Thus, if a compound is prone tohydrolysis at intestinal pH or intestinal enzymatic degradation,complexation with cyclodextrins can aid in maintainingintestinal drug concentrations and thus absorption through theintestinal membrane according to Eq. (11) [12–15]. Forexample, complexation of salbutamol with β-CD and TB-β-CD was used to increase the bioavailability relative to dosingdrug alone 1.7 and 4.6 times, respectively [13]. This wasattributed to decreased biotransformation (mainly glucuronida-tion) in the intestine. In vitro tests demonstrated thatcomplexation led to decreased dissolution rate for this highlysoluble drug, especially in the case of complexation with thehydrophobic cyclodextrin derivative TB-β-CD. Such protectionmay be particularly useful in oral delivery of peptides that areparticularly susceptible to physicochemical and enzymaticdegradation in the intestine [122]. It is also possible, however,that changes in physical or chemical drug properties broughtabout by complexation with cyclodextrins enhance thedegradation of a given drug molecule [123].
3.5. Change in intestinal membrane properties
The interaction of cyclodextrins with biological membranesand possible associated changes in permeability have beeninvestigated [8,9,11,124]. The nature and extent of interaction ofcyclodextrins with the intestinal membrane is not completelyunderstood, but appears to depend on the type of cyclodextrinpresent. Free cyclodextrin may remove membrane components.For example, in a rat intestinal model, α-CD was shown topreferentially release phospholipids, and β-CD selectively re-leased cholesterol. An influence of cyclodextrins on P-glycopro-tein (P-gp) and multidrug resistance-associated protein 2 (MRP2)has also been reported and investigated [11,64,125]. Certaincyclodextrins (e.g., DM-β-CD) inhibited these efflux proteins in

94 R.L. Carrier et al. / Journal of Controlled Release 123 (2007) 78–99
Caco-2 cell monolayers, while other cyclodextrins (e.g., HP-β-CD) had little effect. It was hypothesized that the P-gp inhibitionbrought about by DM-β-CD is due to its solubilizing effect oncholesterol, an abundant component of the caveolaewhere P-gp islocalized. It has been shown that methylated cyclodextrins canextract lipids from the nasal mucosa, possibly enhancingparacellular transport via this mechanism, and a similar mech-anism may apply to the GI tract [11]. Interaction of cyclodextrinswith calcium ions has also been implicated in loosening of tightjunctions [9]. Peracylated β-cyclodextrins have been shown tohave mucoadhesive properties [13,126]. Cyclodextrins can alsoreduce local irritation of the GI tract that would occur if the drugwere dosed alone [39], and thus possibly influence absorption inthis manner. In general, the possible interaction betweensolubilizing capabilities, degradation inhibition, and/or changesin intestinal properties make it difficult to develop quantitativeguidelines on the use of cyclodextrins to enhance bioavailabilitybased on reports in the literature, such as those summarized inTables 1 and 2.
3.6. Shuttling and enhancement of drug concentration at theintestinal wall
The intestine is often modeled as a well-mixed compartment(i.e., uniform concentrations of all species) [127]. However, inreality, there is an “unstirred” boundary layer near the intestinalwall as well as other solid species present, and there are con-centration gradients within these boundary layers. There may be adecreasing concentration of drug in the boundary layer adjacent tothe intestinal membrane due to the fact that drug is being depletedby absorption and may not be replenished quickly enough bydiffusion through the boundary layer. It is possible that com-plexing agents diminish this effect. As free drug is depleted in thevicinity of the intestinal wall, disassociation of complex occurs tore-establish equilibrium, potentially replenishing free drugconcentration faster than it can be replenished via diffusion.This phenomenon could be aided by the use of amphiphilicderivatives of natural cyclodextrins formed by grafting aliphaticchains to the glucopyranose units. These hydrophobic moietiesmay aid in intimate contact of cyclodextrins with biologicalmembranes [120,128]. It has also been hypothesized thatcomponents of the intestinal wall (mucus, lipids) displace thedrug from the complex, leading to an elevated drug concentrationat the intestinal wall [63,92].
4. When cyclodextrins do not enhance bioavailability
4.1. Binding constant magnitude and amount of dosedcyclodextrin
The majority of the literature deals with successful use ofcyclodextrins to enhance bioavailability, but there are reports ofno improvement or decreases in bioavailability with use ofcyclodextrins, as well. There are no clear differences betweenparameters of studies in Table 2, where cyclodextrins were notsuccessful in increasing bioavailability, and those in Table 1. Asmentioned above, all of the compounds listed in Table 2 will be
ionized to a certain extent at the pH of the small intestines, whichcan lead to a decreased binding constant. However, some of thecompounds listed in Table 1 will also be ionized at the pH of thesmall intestines, yet still experienced enhanced bioavailabilityusing CD. In some studies, the lack of bioavailability enhance-ment has been attributed to the magnitude of the binding constantwith cyclodextrin. The reasoning is that a binding constant that is“too small” does not lead to enough complexation for thedissolution kinetics or solubility to be influenced significantly,and a binding constant that is “too big”may lead to decreased freedrug concentration in the intestine, lowering overall absorption(Eq. (11) and Fig. 2) [5,63]. For example, the low level ofbioavailability enhancement observed when cinnarizine wasdosed with β-CD was attributed to a relatively high bindingconstant (6200 M−1) [34,129]. However, similar increases inbioavailability were seen when cinnarizine complexed with HP-β-CD and SBE-β-CDwas dosed in spite of very different bindingconstants with these two cyclodextrins (2242 and 4276 M−1,respectively) [33,129]. A clear method does not currently exist fordetermining the range of appropriate binding constant values for agiven compound due to the complexity of the interaction ofprocesses occurring in the intestinal drug delivery environmentand their dependence on the properties of the drug, drug deliverydevice, and cyclodextrin. These results again highlight theimportance of understanding the interacting processes involvedin dosing a drug to the intestinal environment with a complexingagent such as cyclodextrin as opposed to focusing on theinfluence of a single parameter, such as binding constant. Anexcess of cyclodextrin can have the same effect as a high bindingconstant with regards to potentially decreasing bioavailability.Both factors result in shifts in the equilibrium between drug,cyclodextrin, and complex toward complexation.
4.2. Degradation of cyclodextrins in the intestinal environment
While not explicitly mentioned in the studies presented inTable 2, one factor to consider when assessing the utility ofcyclodextrins to enhance bioavailability of orally deliveredcompounds, especially in the case of controlled-releaseformulations, is the stability of cyclodextrins in the intestinalenvironment. Cyclodextrins are resistant to the enzymes thathydrolyze starch. They are completely resistant to β-amylaseattack, in fact. α-amylases attack the inside of the cyclodextrinmolecule at a relatively slow rate [130]. γ-CD is metabolized byenzymes in the saliva, while α-CD and β-CD are not [3]. α-CDand β-CD are not believed to be hydrolyzed during transitthrough the small intestine, but are degraded by colonic flora.Cyclodextrin metabolism was investigated by Anderson et al. byorally administering 14C-labeled β-CD to rats [131]. The ratsexhaled approximately 55% of the radioactivity within 24 h,with maximum radioactivity observed at 4–8 h. In a similarstudy, Gerloczy et al. administered 14C-labeled cyclodextrin andglucose to rats [132]. Radioactivity was apparent in the respiredair from rats administered glucose only 2 h after feeding, while itappeared 4–8 h after feeding in rats administered cyclodextrin.In both cases, approximately 60% of the administeredradioactivity was accounted for in respired air. These results

95R.L. Carrier et al. / Journal of Controlled Release 123 (2007) 78–99
indicate that cyclodextrins are metabolized in the rat. It has beensuggested based on these and similar studies that absorption ofcyclodextrin does not occur in the small intestine, but rather inthe colon where cyclodextrin is metabolized by colonic bacteria.In fact, as described above, the use of cyclodextrins as pro-drugsfor colon-targeted delivery of compounds has been investigated[65,66,90]. The kinetics of degradation of α- and β-CDs byhuman colon anaerobes was studied by Antenucci et al. [133]. Itwas found that degradation is well under way in as little as 1–2 h,and most of the Bacteroides strains studied were shown todegrade the cyclodextrins. Extensive degradation was observedwithin 18 h, suggesting that colonic transit time may be adequateto cause extensive deterioration of dosed cyclodextrins. Thedegradation observed is attributed mainly to cyclomaltodex-trinase (CDase), an enzyme that hydrolyzes cyclic dextrins andlinear maltodextrins [134,135]. CDase is known to rapidlyhydrolyze cyclodextrins. Characterization of the influence ofsuch degradation on the performance of a controlled-releasedosage form is important for formulation development.
5. Conclusions
A survey of the literature related to use of cyclodextrins forenhancing oral bioavailability was conducted in order to gainunderstanding ofwhen cyclodextrins can be used for this purpose.The focus of the literature reviewed was on the solubilizingcapabilities of cyclodextrins and their contribution to bioavail-ability enhancement, as is the focus ofmost literature on the use ofcyclodextrins in oral pharmaceutical formulations. Generalguidelines were evident from examining the studies, includinginformation related to “typical” affect on bioavailability. Forexample, most studies report successful improvement in bioavail-ability. Of these studies, the majority report an increase in AUCbetween 0 and 100% (1 to 2 times). Most studies (72% of thoseexamined) report a decrease in Tmax of less than 3 h, while the vastmajority (98%) report an increase in Cmax, most often to a valueless than double that when drug is dosed alone. Regarding theproperties of the compounds utilized in these studies, they weregenerally hydrophobic (18 out of 29 studies involved compoundswith logPN2.5) and poorly soluble (most with a solubility of 1μg/ml–1 mg/ml). This is expected, as cyclodextrins enhance overallabsorption by influencing dissolution kinetics. The complex of thedrug rather than a physical mixture is typically dosed, and incomparing studies in which both complex and physical mixturewere used, the AUC approximately doubled with the complexcompared to the physical mixture. This phenomenon is related tothe high solubility of most cyclodextrin complexes. Most studiesinvolved low doses (b100mg in 25 out of 29 studies) and lowCD:drug ratios (more than half with 2:1 or less), with very weak tomoderate binding constants (b5000 M−1 in 33 out of 46 studiesreporting the constant values). Low doses are required forpractical use of cyclodextrins in traditional oral dosage forms(tablets, capsules). CD:drug ratios are also limited by practicaldosage form sizes. Low to moderate CD:drug ratios and bindingconstants are also important as a negative affect of cyclodextrin onbioavailability can be related to a high percentage of bound druglimiting the free drug in solution available for absorption.
In spite of these general guidelines, many studies reportedparameters outside of these guidelines, and it was difficult todistinguish between parameters of studies in which success orlack thereof in bioavailability enhancement was reported. There-fore, it was not possible to develop clear quantitative guidelinesfor what drug and cyclodextrin properties are key to enabling oralbioavailability enhancement using cyclodextrins. This is likelypartially due to complicating factors (method of complex form-ation, charge of drug during GI transit) and variability in reportedparameters (e.g., binding constant). It is also partially due to theother effects of cyclodextrins in certain dosage forms, such asdecreasing degradation kinetics or inhibiting compound efflux,which were not taken into consideration in comparing studies.However, even in cases where adequate information regardingexperimental parameters are supplied and other effects ofcyclodextrin in addition to solubilization are not believed toplay a role, it is difficult to correlate a single parameter to theability of cyclodextrins to enhance bioavailability. The mechan-isms of bioavailability enhancement using cyclodextrins weretherefore discussed to provide further insight. The influence ofcyclodextrins on the dissolution of drug in the intestinal lumen aswell as the absorption of drug, a process proportional to the freedrug concentration in the intestinal lumen, were considered. It isevident that the physical and chemical properties of a given drug,cyclodextrin, and dosage form interact to influence kinetics of keyprocesses of oral drug delivery, including dissolution andabsorption. These interactions create difficulty in preciselyspecifying one range of values for one parameter (e.g., bindingconstant, solubility) that will result in successful bioavailabilityenhancement using cyclodextrins. A more comprehensivetheoretical analysis of the influence of cyclodextrins on thekinetics of simultaneous processes occurring in the drug deliveryenvironment may provide further guidance.
NomenclatureA Surface area of dissolving particle, dm2
CDtotal Total molar amount of free and bound cyclodextrin,moles
Dcom Complex diffusivity, dm2/sDdrug Drug diffusivity, dm2/sDtotal Molar dose of drug, molesK Cyclodextrin complexation constant, M−1, assuming
1:1 bindingSo Free drug solubility, MV Total volume, LVlumen Volume of the intestinal lumen, Ldrugabs Moles of drug absorbed, molesdrugf Moles of free drug in solution, moleska Absorption rate constant, min−1
kdis Dissolution rate constant, Ms−1
kpre Precipitation rate constant, units depend on specifickinetics
lbl Boundary layer thickness, dm[drug]f Molar concentration of free drug in solution, M[drug]total Total molar concentration of free and bound drug in
solution, M[com] Molar concentration of complex in solution, M

96 R.L. Carrier et al. / Journal of Controlled Release 123 (2007) 78–99
[com]surface Concentration of complex at dissolving drugparticle surface, M
[CD]f Molar concentration of free cyclodextrin in solution,
MReferences
[1] T. Loftsson, M.E. Brewster, M. Masson, Role of cyclodextrins inimproving oral drug delivery, Am. J. Drug Del. 2 (4) (2004) 175–261.
[2] M.E. Davis, M.E. Brewster, Cyclodextrin-based pharmaceutics: past,present and future, Nat. Rev. Drug Discovery 3 (2004) 1023–1035.
[3] G.L. Mosher, D.O. Thompson, in: J. Swarbrick (Ed.), Encyclopedia ofPharmaceutical Technology, 2nd Edition, Marcel Dekker, 2002.
[4] J. Szejtli, Cyclodextrin Technology, Kluwer Academic Publishers,Dordrecht, 1988.
[5] J. Szejtli, Medicinal applications of cyclodextrins, Med. Res. Rev. 14(1994) 353–386.
[6] R.A. Rajewski, V.J. Stella, Pharmaceutical applications of cyclodextrins. 2.In vivo drug delivery, J. Pharm. Sci. 85 (1996) 1142–1169.
[7] K. Uekama, M. Otagiri, Cyclodextrins in drug carrier systems, Crit. Rev.Ther. Drug Carr. Syst. 3 (1) (1987) 1–40.
[8] R. Challa, A. Ahuja, J. Ali, R.K. Khar, Cyclodextrins in drug delivery: anupdated review, AAPS PharmSciTech 6 (2) (2005) E329–E357.
[9] H. Arima, F. Hirayama, C.T. Okamoto, K. Uekama, Recent aspects ofcyclodextrin-based pharmaceutical formulations, Recent Res. Devel.Chem. Pharm. Sciences 2 (2002) 155–193.
[10] D.O. Thompson, Cyclodextrins-enabling excipients: their present and futureuse in pharmaceuticals, Crit. Rev. Ther. Drug Carr. Syst. 14 (1) (1997) 1–104.
[11] K. Uekama, Design and evaluation of cyclodextrin-based drugformulation, Chem. Pharm. Bull. (Tokyo). 52 (8) (2004) 900–915.
[12] K. Miyake, H. Arima, F. Hirayama, M. Yamamoto, T. Horikawa, H.Sumiyoshi, S. Noda, K. Uekama, Improvement of solubility and oralbioavailability of rutin by complexation with 2-hydroxypropyl-β-cyclodextrin, Pharm. Dev. Technol. 5 (3) (2000) 399–407.
[13] F. Hirayama, T. Horikawa, M. Yamanaka, K. Uekama, Enhancedbioavailability and reduced metabolism of salbutamol by perbutanoyl-b-cyclodextrin after oral administration in dogs, Pharm. Sci. 1 (11) (1995)517–520.
[14] T. Loftsson, M.E. Brewster, Pharmaceutical applications of cyclodex-trins. 1. Drug solubilization and stabilization, J. Pharm. Sci. 85 (10)(1996) 1017–1025.
[15] M. Usuda, T. Endo, H. Nagase, K. Tomono, H. Ueda, Interaction ofantimalarial agent artemisinin with cyclodextrins, Drug Dev. Ind. Pharm.vol. 26 (2000) 613–619.
[16] K. Uekama, T. Fujinaga, F. Hirayama, M. Otagiri, M. Yamasaki, H. Seo,T. Hashimoto, M. Tsuruoka, Improvement of the oral bioavailability ofdigitalis glycosides by cyclodextrin complexation, J. Pharm. Sci. 72 (11)(1983) 1338–134141.
[17] K. Uekama, T. Fujinaga, M. Otagiri, H. Seo, M. Tsuruoka, Enhancedbioavailability of digoxin by γ-cyclodextrin complexation, J. Pharmaco-bio-dyn. 4 (1981) 735–737.
[18] J.L. Vila-Jato, J. Blanco, A. Vilar, Spironolactone/β-cyclodextrin complex:oral bioavailability in humans, Pharm. Technol. 32 (2) (1986) 82–85.
[19] F.J. Otero-Espinar, S. Anguiano-Igea, N. Garcia-Gonzalez, J.L. Vila-Jato,J. Blanco-Mendez, Oral bioavailability of naproxen-β-cyclodextrininclusion compound, Int. J. Pharm. vol. 75 (1991) 37–44.
[20] S. Choudhury, K.F. Nelson, Improvement of oral bioavailability ofcarbamazepine by inclusion in 2-hydroxypropyl-b-cyclodextrin, Int. J.Pharm. 85 (1–3) (1992) 175–180.
[21] L.S. Koester, P. Mayorga, V.L. Bassani, Carbamazepine/βCD/HPMCsolid dispersions. I. Influence of the spray-drying process and bCD/HPMC on the drug dissolution profile, Drug Dev. Ind. Pharm. 29 (2)(2003) 139–144.
[22] M.D. Dhanaraju, K.S. Kumaran, T. Baskaran, M. Sree Rama Moorthy,Enhancement of bioavailability of griseofulvin by its complexation withβ-cyclodextrin, Drug Dev. Ind. Pharm. 24 (6) (1998) 583–587.
[23] S.A. Elkheshen, S.M. Ahmed, B.T. Al-Quadeib, Inclusion complexes ofpiroxicam with b-cyclodextrin derivatives in comparison with the naturalβ-cyclodextrin, Pharm. Ind. 64 (7) (2002) 708–715.
[24] O.A.E. Soliman, K. Kimura, F. Hirayama, K. Uekama, H.M. El-Sabbagh, A.E.-G.H. El-Gawad, F.M. Hashim, Amorphous spirono-lactone-hydroxypropylated cyclodextrin complexes with superiordissolution and oral bioavailability, Int. J. Pharm. 149 (1997) 73–83.
[25] J. Geczy, J. Bruhwyler, J. Scuvee-Moreau, V. Seutin, H. Masset, J.C. VanHeugen, A. Dresse, C. Lejeune, E. Decamp, L. Szente, J. Szejtli, J.-F.Liegeois, The inclusion of fluoxetine into γ-cyclodextrin increases itsbioavailability: behavioural, electrophysiological and pharmacokineticstudies, Psychopharmacology (Berl). 151 (2000) 328–334.
[26] J. Savolainen, K. Jarvinen, H. Taipale, P. Jarho, T. Loftsson, T. Jarvinen, Co-administration of a water-soluble polymer increases the usefulness of cyclo-dextrins in solid oral dosage forms, Pharm. Res. 15 (11) (1998) 1696–1701.
[27] J.W. Wong, K.H. Yuen, Improved oral bioavailability of artemisininthrough inclusion complexation with β- and γ-cyclodextrin, Int. J. Pharm.227 (2001) 177–185.
[28] M. Kikuchi, F. Hirayama, K. Uekama, Improvement of oral and rectalbioavailabilities of carmofur by methylated β-cyclodextrin complexa-tions, Int. J. Pharm. 38 (1987) 191–198.
[29] J.L. Vila-Jato, J. Blanco, J.J. Torres, Biopharmaceutical aspects ofglibornuride-b-cyclodextrin inclusion compound, S.T.P. Pharma 3 (1)(1987) 28–32.
[30] H.-G. Choi, B.-J. Lee, J.-H. Han, M.-K. Lee, K.-M. Park, C.S. Yong, J.-D.Rhee, Y.-B. Kim, C.-K. Kim, Terfenadine-b-cyclodextrin inclusioncomplex with antihistaminic activity enhancement, Drug Dev. Ind.Pharm. 27 (8) (2001) 857–862.
[31] J. Luengo, T. Aranguiz, J. Sepulveda, L. Hernandez, C. Von Plessing,Preliminary pharmacokinetic study of different preparations of acyclovirwith β-cyclodextrin, J. Pharm. Sci. 91 (12) (2002) 2593–2598.
[32] B. Evrard, P. Chiap, P. DeTullio, F. Ghalmi, G. Piel, T. Van Hees, J.Crommen, B. Losson, L. Delattre, Oral bioavailability in sheep ofalbendazole from a suspension and from a solution containing hydro-xypropyl-β-cyclodextrin, J. Control. Release 85 (1–3) (2002) 45–50.
[33] T. Jarvinen, K. Jarvinen, N. Schwarting, V.J. Stella, β-Cyclodextrinderivatives, SBE4-β-CD and HP-b-CD, increase the oral bioavailabilityof cinnarizine in beagle dogs, J. Pharm. Sci. 84 (3) (1995) 295–299.
[34] T. Tokumura, M. Namba, Y. Tsushima, K. Tatsuishi, M. Kayano, Y.Machida, T. Nagai, Enhancement of bioavailability of cinnarizine from itsβ-cyclodextrin complex on oral administration with DL-phenylalanine asa competing agent, J. Pharm. Sci. 75 (1986) 391–394.
[35] K. Uekama, S. Narisawa, F. Hirayama, M. Otagiri, Improvement ofdissolution and absorption characteristics of benzodiazepines bycyclodextrin complexation, Int. J. Pharm. 16 (3) (1983) 327–338.
[36] H.P.R. Bootsma, H.W. Frijlink, A. Eissens, J.H. Proost, H. Van Doorne,C.F. Lerk, β-Cyclodextrin as an excipient in solid oral dosage forms: invitro and in vivo evaluation of spray-dried diazepam-β-cyclodextrinproducts, Int. J. Pharm. 51 (3) (1989) 213–223.
[37] G.L. Stracciari, J. Malvisi, P. Anfossi, G.B. Fregnan, Pharmacokinetics ofdipyridamole-β-cyclodextrin complex in dogs, Arch. Int. Pharmacodyn.Ther. 300 (1989) 7–13.
[38] N. Nambu, M. Shimoda, Y. Takahashi, H. Ueda, T. Nagai, Bioavailabilityof powdered inclusion compounds of nonsteroidal anti-inflamatory drugswith β-cyclodextrin in rabbits and dogs, Chem. Pharm. Bull. (Tokyo). 26(10) (1978) 2952–2956.
[39] G. Ramprakash, M.S. Nagarsenker, Cyclodextrin based oral delivery offlurbiprofen: effect of method of preparation on drug release and studieson in-vivo performance, 28th International Symposium on ControlledRelease of Bioactive Materials and 4th Consumer & Diversified ProductsConference, vol. 28, Controlled Release Society, Inc., San Diego, CA,2001, pp. 772–773.
[40] L.H. Emara, R.M. Badr, A.A. Elbary, Improving the dissolution andbioavailability of nifedipine using solid dispersions and solubilizers,Drug Dev. Ind. Pharm. 28 (7) (2002) 795–807.
[41] D.N. Reddy, U.V. Singh, S. Pandey, N. Udupa, Evaluation of piroxicamoral and transdermal preparations, Indian J. Pharm. Sci. 54 (4) (1992)152–154.

97R.L. Carrier et al. / Journal of Controlled Release 123 (2007) 78–99
[42] K. Uekama, M. Otagiri, Y. Uemura, T. Fujinaga, K. Arimori, N. Matsuo,K. Tasaki, A. Sugii, Improvement in oral bioavailability of prednisoloneby β-cyclodextrin complexation in humans, J. Pharmacobio-dyn. 6(1983) 124–127.
[43] F. Hirayama, T. Horikawa, M. Yamanaka, K. Uekama, Enhancedbioavailability and reduced metabolism of salbutamol by perbutanoyl-β-cyclodextrin after oral administration in dogs, Pharm. Sci. 1 (11)(1995) 517–520.
[44] H. Arima, K. Yunomae, K. Miyake, T. Irie, F. Hirayama, Comparativestudies of the enhancing effects of cyclodextrins on the solubility and oralbioavailability of tacrolimus in rats, J. Pharm. Sci. 90 (2001) 690–701.
[45] F. Veiga, C. Fernandes, F. Teixeira, Oral bioavailability and hypoglycemicactivity of tolbutamide/cyclodextrin inclusion complexes, Int. J. Pharm.vol. 202 (2000) 165–171.
[46] J.L. Vila-Jato, Biopharmaceutical aspects of the tolbutamide-beta-cyclodextrin inclusion compound, Il Farmaco 43 (1988) 37–45.
[47] C. Von Plessing Rossel, J. Sepulveda Carreno, M. Rodriguez-Baeza, J.B.Alderete, Inclusion complex of the antiviral drug acyclovir withcyclodextrin in aqueous solution and in solid phase, Quim. Nova 23(6) (2000) 749–752.
[48] T. Tokumura, H. Ueda, Y. Tsushima, M. Kasai, M. Kayano, I. Amada, Y.Machida, T. Nagai, Inclusion complex of cinnarizine with β-cyclodextrinin aqueous solution and in solid state, J. Incl. Phenom. vol. 2 (1984)511–521.
[49] H. Ueda, D. Ou, T. Endo, H. Nagase, K. Tomono, T. Nagai, Evaluation ofa sulfobutyl ether β-cyclodextrin as a solubilizing/stabilizing agent forseveral drugs, Drug Dev. Ind. Pharm. 24 (9) (1998) 863–867.
[50] E.S. Kostewicz, U. Brauns, R. Becker, J.B. Dressman, Forecasting theoral absorption behavior of poorly soluble weak bases using solubilityand dissolution studies in biorelevant media, Pharm. Res. 19 (3) (2002)345–349.
[51] Y. Hamada, N. Nambu, T. Nagai, Pharmaceutical interactions in dosageforms and processing. III. Interactions of α- and β-cyclodextrin withseveral nonsteroidal antiinflammatory drugs in aqueous solution, Chem.Pharm. Bull. (Tokyo). 23 (6) (1975) 1205–1211.
[52] K. Ikeda, K. Uekama, M. Otagiri, Inclusion complexes of β-cyclodextrinwith antiinflammatory drugs fenamates in aqueous solution, Chem.Pharm. Bull. (Tokyo). 23 (1) (1975) 201–208.
[53] M.D. Veiga, P.J. Diaz, F. Ahsan, Interactions of griseofulvin withcyclodextrins in solid binary systems, J. Pharm. Sci. 87 (7) (1998)891–900.
[54] M. Platzer, M.A. Schwarz, R.H.H. Neubert, Determination of formationconstants of cyclodextrin inclusion complexes using affinity capillaryelectrophoresis, J. Microcolumn Sep. 11 (3) (1999) 215–222.
[55] K.P.R. Chowdary, R.G. Kamalakara, Controlled release of nifedipinefrom mucoadhesive tablets of its inclusion complexes with β-cyclodex-trin, Pharmazie 58 (10) (2003) 721–724.
[56] Y.L. Loukas, Multiple complex formation of unstable compounds withcyclodextrins: efficient determination and evaluation of the bindingconstant with improved kinetic studies, Analyst 122 (4) (1997) 377–381.
[57] S. Lee, C. Kwon, Y. Choi, D.-H. Seo, B.-W. Kim, S. Jung, Inclusioncomplexation of a family of cyclosophoraoses with indomethacin,J. Microbiol. Biotechnol. 11 (3) (2001) 463–468.
[58] X. Guo, Y. Yu, G. Zhao, G. Zhang, J. Chao, S. Shaomin, Study oninclusion interaction of piroxicam with β-cyclodextrin derivatives,Spectrochim. Acta A. Mol. Biomol. Spectrosc. 59A (14) (2003)3379–3386.
[59] M.R. Lauro, M.L. Torre, L. Maggi, F. De Simone, U. Conte, R.P. Aquino,Fast- and slow-release tablets for oral administration of flavonoids: rutinand quercetin, Drug Dev. Ind. Pharm. 28 (4) (2002) 371–379.
[60] V. Lemesle-Lamache, M. Taverna, D. Wouessidjewe, D. Duchene, D.Ferrier, Determination of the binding constant of salbutamol tounmodified and ethylated cyclodextrins by affinity capillary electropho-resis, J. Chromatogr. A 735 (1+2) (1996) 321–331.
[61] H. Seo, M. Tsuruoka, T. Hashimoto, T. Fujinaga, M. Otagiri, K. Uekama,Enhancement of oral bioavailability of spironolactone by β- and γ-cyclodextrin complexations, Chem. Pharm. Bull. (Tokyo). 31 (1) (1983)286–291.
[62] Y. Namiki, A. Fujiwara, N. Kihara, S. Koda, K. Hane, T. Yasuda, Factorsaffecting tautomeric phenomenon of a novel potent immunosuppressant(FK506) on the design for injectable formulation, Drug Dev. Ind. Pharm.21 (7) (1995) 809–822.
[63] O. Bekers, E.V. Uijtendaal, J.H. Beijnen, A. Buit, W.J.M. Underberg,Cyclodextrins in the pharmaceutical field, Drug Dev. Ind. Pharm. 17(1991) 1503–1549.
[64] K. Yunomae, H. Arima, F. Hirayama, K. Uekama, Involvementof cholesterol in the inhibitory effect of dimethyl-β-cyclodextrinon P-glycoprotein and MRP2 function in Caco-2 cells, FEBS Lett. 536(2003) 225–231.
[65] H. Yano, F. Hirayama, H. Arima, K. Uekama, Preparation of prednisolone-appended alpha-, beta- and gamma-cyclodextrins: substitution at secondaryhydroxyl groups and in vitro hydrolysis behavior, J. Pharm. Sci. 90 (4)(2001) 493–503.
[66] F. Hirayama, K. Uekama, Cyclodextrin-based controlled drug releasesystem, Adv. Drug Delivery Rev. 36 (1999) 125–141.
[67] J. Szejtli, Cyclodextrins in drug formulations: part II, Pharm. Technol. Int.3 (3) (1991) 16–24.
[68] J.B. Dressman, J. Butler, J. Hempenstall, C. Reppas, The BCS: where dowe go from here? Pharm, Technol. N. Am. 25 (7) (2001) 68–76.
[69] S.Y. Lin, Y.H. Kao, Studies on drug interaction in pharmaceuticalformulations. Part XII. Solid particulates of drug-β-cyclodextrininclusion complexes directly prepared by a spray-drying technique, Int.J. Pharm. 56 (3) (1989) 249–259.
[70] M.S. Islam, M.M. Narurkar, The effect of 2-hydroxypropyl-β-cyclodextrinon the solubility, stability, and dissolution rate of famotidine, DrugDev. Ind.Pharm. 17 (9) (1991) 1229–1239.
[71] S.-Z. Lin, D. Wouessidjewe, M.-C. Poelman, D. Duchene, Indomethacinand cyclodextrin complexes, Int. J. Pharm. 69 (1991) 211–219.
[72] S. Baboota, M. Dhaliwal, K. Kohli, Physicochemical characterization, invitro dissolution behavior, and pharmacodynamic studies of rofecoxib-cyclodextrin inclusion compounds. Preparation and properties ofrofecoxib hydroxypropyl β-cyclodextrin inclusion complex: a technicalnote, AAPS PharmSciTech. 6 (1) (2005) E83–E90.
[73] J.M. Ginés, M.J. Arias, C. Novák, P.J. Sánchez-Soto, A. Ruiz-Conde, E.Morillo, Thermal study of complex formation of triamterene withβ-cyclodextrin by spray-drying and co-grinding, J. Therm. Anal. Calorim.45 (4) (1995) 659–666.
[74] V. Stella, R.A. Rajewski, J.W. McGinity, Sulfoalkyl ether cyclodextrinbased solid pharmaceutical formulations and their use, United StatesPatent 5,874,418, February 23, 1999.
[75] V.J. Stella, R.A. Rajewski, V.M. Rao, J.W. McGinity, G.L. Mosher,Sulfoalkyl ether cyclodextrin based controlled release solid pharmaceu-tical formulations, United States Patent 6,046,177, April 4, 2000.
[76] V.J. Stella, R.A. Rajewski, K. Okimoto, K. Uekama, T. Irie, S. Shiraishi,E.A. Zannou, V. Rao, Oral controlled release of poorly water solubledrugs utilizing Captisol as both a solubilizer and osmotic agent, Int.Symp. Control. Release Bioact. Mater. (2000) 145–146.
[77] K. Okimoto, M. Miyake, N. Ohnishi, R.A. Rajewski, V.J. Stella, T. Irie,K. Uekama, Design and evaluation of an osmotic pump tablet (OPT) forprednisolone, a poorly water soluble drug, using (SBE)7M-β-CD, Pharm.Res. 15 (10) (1998) 1562–1568.
[78] K. Okimoto, A. Ohike, R. Ibuki, O. Aoki, N. Ohnishi, R.A. Rajewski, V.J.Stella, T. Irie, K. Uekama, Factors affecting membrane-controlled drugrelease for an osmotic pump tablet (OPT) utilizing (SBE)7M-β-CD asboth a solubilizer and osmotic agent, J. Control. Release 60 (2–3) (1999)311–319.
[79] V.M. Rao, J.L. Haslam, V.J. Stella, Controlled and complete release of amodel poorly water-soluble drug, prednisolone, from hydroxypropymethylcellulose matrix tablets using (SBE)7M-β-cyclodextrin as asolubilizing agent, J. Pharm. Sci. 90 (7) (2001) 807–816.
[80] K. Okimoto, Y. Tokunaga, R. Ibuki, T. Irie, K. Uekama, R.A. Rajewski,V.J. Stella, Abblicability of (SBE)7M-beta-CD in controlled-porosityosmotic pump tablets (OPT)s, Int. J. Pharm. 286 (2004) 81–88.
[81] L.A. Miller, R.L. Carrier, I. Ahmed, Practical considerations indevelopment of solid dosage forms that contain cyclodextrin, J. Pharm.Sci. 96 (7) (2007) 1691–1707.

98 R.L. Carrier et al. / Journal of Controlled Release 123 (2007) 78–99
[82] P. Giunchedi, L. Maggi, A. LaManna, U. Conte, Modification of thedissolution behavior of a water-insoluble drug, naftazone, for zero-orderrelease matrix preparation, J. Pharm. Pharmacol. 46 (6) (1994) 476–480.
[83] F. Quaglia, G. Varricchio, A. Miro, M.I. La Rotonda, D. Larobina, G.Mensitieri, Modulation of drug release from hydrogels by usingcyclodextrins: the case of nicardipine/β-cyclodextrin system in cross-linked polyethylenglycol, J. Control. Release 71 (2001) 329–337.
[84] M.E. Sangalli, L. Zema, A. Maroni, A. Foppoli, F. Giordano, A.Gazzaniga, Influence of betacyclodextrin on the release of poorly solubledrugs from inert hydrophilic heterogeneous polymeric matrices, Bioma-terials 22 (2001) 2647–2651.
[85] Y. Ikeda, K. Kimura, F. Hirayama, H. Arima, K. Uekama, Controlledrelease of a water-soluble drug, captopril, by a combination ofhydrophilic and hydrophobic cyclodextrin derivatives, J. Control.Release 66 (2) (2000) 271–280.
[86] V.J. Stella, V.M. Rao, E.A. Zannou, The pharmaceutical use of captisol:some surprising observations, J Incl. Phenom. Macro. 44 (2002) 29–33.
[87] E.A. Zannou,W.H. Streng, V.J. Stella,Osmotic properties of sulfobutyletherand hydroxypropyl cyclodextrins, Pharm. Res. 18 (8) (2001) 1226–1231.
[88] K. Okimoto, K. Miyake, O. Aoki, N. Ohnishi, T. Irie, Design andevaluation of a porosity-controlled osmotic pump tablet for chlorprom-azine using (SBE)7M-β-CD, in: J.J. Labandeira, J.L. Vila-Jato (Eds.), 9thInternational Symposium on Cyclodextrins, Kluwer Academic Publish-ers, Santiago de Comostela, Spain, 1999, pp. 285–288.
[89] T. Horikawa, R. Hirayama, K. Uekama, In-vivo and in-vitro correlationfor delayed-release behaviour of a molsidomine/O-carboxymethyl-O-ethyl-β-cyclodextrin complex in gastric acidity-controlled dogs,J. Pharm. Pharmacol. 47 (2) (1995) 124–127.
[90] M. Kamada, F. Hirayama, K. Udo, H. Yano, H. Arima, K. Uekama,Cyclodextrin conjugate-based controlled release system: repeated- andprolonged-releases of ketoprofen after oral administration in rats,J. Control. Release 82 (2002) 407–416.
[91] J. Szejtli, L. Szente, Interaction between indomethacin and β-cyclodex-trin, Pharmazie 36 (10) (1981) 694–698.
[92] H.W. Frijlink, A.J.M. Schoonen, C.F. Lerk, The effects of cyclodextrins ondrug absorption. I. In vitro observations, Int. J. Pharm. 49 (1989) 91–102.
[93] V.M. Rao, V.J. Stella, When can cyclodextrins be considered forsolubilization purposes? J. Pharm. Sci. 92 (5) (2003) 927–932.
[94] Y. Kim, D.E. Oksanen, W. Massefski, J.F. Blake, E.M. Duffy, B. Chrunyk,Inclusion complexation of ziprasidone mesylate with β-cyclodextrinsulfobutyl ether, J. Pharm. Sci. 87 (12) (1998) 1560–1567.
[95] K. Okimoto, R.A. Rajewski, K. Uekama, J.A. Jona, V.J. Stella, Theinteraction of charged and un-charged drugs with neutral (HP-β-CD) andanionically charged (SBE7-β-CD) β-cyclodextrins, Pharm. Res. 13(1996) 254–256.
[96] A.Y. Tinwalla, B.L. Hoesterey, T.X. Xiang, K. Lim, B.D. Anderson,Solubilization of thiazolobenzimidazole using a combination of pHadjustment and complexation with 2-hydroxypropyl-β-cyclodextrin,Pharm. Res. 10 (1993) 1136–1143.
[97] P. Li, E. Tabibi, S.H. Yalkowsky, Combination effect of complexation andpH on solubilization, J. Pharm. Sci. 87 (1998) 1535–1537.
[98] M.D. Johnson, B.L. Hoesterey, B.D. Anderson, Solubilization of atripeptide HIV protease inhibitor using a combination of ionization andcomplexation with chemically modified cyclodextrins, J. Pharm. Sci. 83(1994) 1142–1146.
[99] V. Zia, R.A. Rajewski, V.J. Stella, Effect of cyclodextrin charge oncomplexation of neutral and charged substrates: comparison of (SBE)7M-β-CD to HP-β-CD, Pharm. Res. 18 (2001) 667–673.
[100] K.A. Connors, Population characteristics of cyclodextrin complexstabilities in aqueous solution, J. Pharm. Sci. 84 (7) (1995) 843–848.
[101] K.A. Connors, The stability of cyclodextrin complexes in solution, Chem.Rev. 97 (5) (1997) 1325–1357 (Washington, D. C.).
[102] R.R. Burnette, K.A. Connors, Statistical properties of thermodynamicquantities for cyclodextrin complex formation, J. Pharm. Sci. 89 (11)(2000) 1389–1394.
[103] Y.L. Loukas, Understanding molecular association and isomers recogni-tion in isomer-cyclodextrin multiple complex formation by improvedliquid chromatographic studies, Anal. Chem. 70 (5) (1998) 966–970.
[104] J. Szejtli, in: J.E.D. Davies (Ed.), Cyclodextrin Technology, KluwerAcademic Publishers, Dordrecht, 1988, pp. 186–306.
[105] G. Levy, E.J. Mroszczak, Effect of complex formation on drug absorptionVI, J. Pharm. Sci. 57 (2) (1968) 235–239.
[106] R.E. Davis, C.W. Hartman, J.H. Fincher, Dialysis of ephedrine andpentobarbital from whole human saliva and simulated saliva, J. Pharm.Sci. 60 (3) (1971) 429–432.
[107] T. Tokumura, Y. Tsushima, M. Kayano, Y. Machida, T. Nagai,Enhancement of bioavailability of cinnarizine from its β-cyclodextrincomplex on oral administration with DL-phenylalanine as a competingagent, J. Pharm. Sci. 74 (4) (1985) 496–497.
[108] T. Loftsson, H. Fridriksdottir, A.M. Sigurdadottir, H. Ueda, The effect ofwater soluble polymers on drug-cyclodextrin complexation, Int. J. Pharm.110 (1994) 169–177.
[109] T. Loftsson, H. Fridriksdottir, T.K. Gudmundsdottir, The effect of water-soluble polymers on aqueous solubility of drugs, Int. J. Pharm. 127(1996) 293–296.
[110] M. Valero, B.I. Perez-Revuelta, L.J. Rodriguez, Effect of PVP K-25 onthe formation of the naproxen:β-cyclodextrin complex, Int. J. Pharm. 253(2003) 97–110.
[111] E. Redenti, L. Szente, J. Szejtli, Drug/cyclodextrin/hydroxy acidmulticomponent systems. Properties and pharmaceutical applications,J. Pharm. Sci. 89 (1) (2000) 1–8.
[112] C. Kraus, W. Mehnert, K.H. Froemming, Interactions of β-cyclodex-trin with Solutol HS 15 and their influence on diazepam solubiliza-tion, Pharmazeutische Zeitung-Wissenschaftsausgabe 4 (1) (1991)11–15.
[113] D.R. Olander, Simultaneous mass transfer and equilibrium chemicalreaction, AIChE J. 6 (1960) 233–239.
[114] C.D. Yu, S.A. Sweetana, N.I. Chu, G.J.L. Lee, I.J. Massey, Enhancementof solubility, dissolution rate, and oral bioavailability of RS-82856 bycomplex formation with cyclodextrins, Drug Dev. Ind. Pharm. 15 (4)(1989) 609–620.
[115] T. Higuchi, K.A. Connors, in: C.N. Reilly (Ed.), Advances in AnalyticalChemistry and Instrumentation, vol. 4, Wiley-Interscience, New York,1965, pp. 117–212.
[116] T. Irie, Y. Tsunenari, K. Uekama, J. Pitha, Effect of bile on the intestinalabsorption of a-cyclodextrin in rats, Int. J. Pharm. 43 (1988) 41–44.
[117] J. Szejtli, in: W.F. Smolen, L.A. Ball (Eds.), Controlled DrugBioavailability, vol. 3, Wiley, New York, 1985, p. 365.
[118] V.J. Stella, V.M. Rao, E.A. Zannou, V. Zia, Mechanisms of drug releasefrom cyclodextrin complexes, Adv. Drug Delivery Rev. 36 (1999)3–16.
[119] J. Szejtli, Cyclodextrins in drug formulations: part I, Pharm. Technol. Int.3 (2) (1991) 15–22.
[120] E. Memisoglu, A. Bochot, M. Oz alp, M. Sen, D. Duchene, A.A. Hincal,Direct formation of nanospheres from amphiphilic β-cyclodextrininclusion complexes, Pharm. Res. 20 (1) (2003) 117–125.
[121] K. Kimura, F. Hirayhama, H. Arima, K. Uekama, Effects of aging oncrystallization, dissolution and absorption characteristics of amorphoustolbutamide-2-hydroxypropyl-beta-cyclodextrin complex, Chem. Pharm.Bull. (Tokyo). 48 (5) (2000) 646–650.
[122] B. Haeberlin, T. Gengenbacher, A. Meinzer, G. Fricker, Cyclodextrins—useful excipients for oral peptide administration? Int. J Pharm. 137 (1996)103–110.
[123] K. Uekama, F. Hirayama, M. Daiguji, Effects of α- and β-cyclodextrinson base-catalyzed isomerization of prostaglandin A1 and prostaglandinA2, Chem. Lett. 4 (1978) 327–330.
[124] K. Nakanishi, T. Nadai, M. Masada, K. Miyajima, Effect of cyclodextrinson biological membrane. II. Mechanism of enhancement on the intestinalabsorption of non-absorbable drug by cyclodextrins, Chem. Pharm. Bull.(Tokyo). 40 (1992) 1252–1256.
[125] K. Yunomae, H. Arima, F. Hirayama, K. Uekama, Contribution of P-glycoprotein to enhancing effects of dimethyl β-cyclodextrin on oralbioavailability of tacrolimus in rats, 28th International Symposium onControlled Release of Bioactive Materials and 4th Consumer &Diversified Products Conference, Controlled Release Society, Minnea-polis, MN, San Diego, CA, United States, vol. 1, 2001, pp. 712–713.

99R.L. Carrier et al. / Journal of Controlled Release 123 (2007) 78–99
[126] K. Uekama, T. Horikawa, M. Yamanaka, F. Hirayama, Peracylatedβ-cyclodextrins as novel sustained-release carriers for a water-solubledrug, molsidomine, J. Pharm. Pharmacol. 46 (1994) 714–717.
[127] L.X. Yu, E. Lipka, J.R. Crison, G.L. Amidon, Transport approaches tothe biopharmaceutical design of oral drug delivery systems: predictionof intestinal absorption, Adv. Drug Delivery Rev. 19 (3) (1996)359–376.
[128] D. Duchene, D. Wouessidjewe, G. Ponchel, Cyclodextrins and carriersystems, J. Control. Release 62 (1999) 263–268.
[129] H. Ueda, J.H. Perrin, T. Nagai, A microcalorimetric investigation of thebinding of cinnarizine to cyclodextrins, J. Pharm. Biomed. Anal. 7 (1989)642–939.
[130] J. Szejtli, The significance of cyclodextrins: biological effects, J. DrugDev. 4 (Suppl. 1) (1991) 3–11.
[131] G.H. Anderson, F.M. Robbins, F.I. Dominigues, C.L. Long, Theutilization of Schardinger dextrins by the rat, Toxicol. Appl. Pharmacol.5 (1963) 257–266.
[132] A. Gerloczy, A. Fonagy, J. Szejtli, Absorption and metabolism ofβ-cyclodextrin by rats, First International Symposium on Cyclodextrins,Reidel Publishing, 1981, pp. 101–108.
[133] R.N. Antenucci, J.K. Palmer, Enzymatic degradation of α- andβ-cyclodextrins by Bacteroides of the human colon, J. Agric. FoodChem. 32 (1984) 1316–1321.
[134] B.C. Saha, J.G. Zeikus, Cyclodextrin degrading enzymes, Starch/Staerke44 (1992) 312–315.
[135] G. Schmid, in: J.L. Atwood, J.E.D. Davies, D.D.MacNicol, F. Vogtle, J.-M.Lehn (Eds.), Comprehensive Supramolecular Chemistry, vol. 3, Pergamon,2000, pp. 615–626.