The Use of Psychotropics in the Pediatric Population · Pulse, BP, prolactin, fasting BG, HbA1c,...
65
Ecology of the Wyoming big sagebrush alliance in the northern Great Basin: 2004 Progress Report Eastern Oregon Agricultural Research Center USDA Agricultural Research Service & Oregon State University 67826-A Hwy 205 Burns OR, 97720
Transcript of The Use of Psychotropics in the Pediatric Population · Pulse, BP, prolactin, fasting BG, HbA1c,...

12/21/2015
1
The Use of Psychotropics in the Pediatric
Population
Noor Daghistani
PGY2 Psychiatric Pharmacy Resident
Nova Southeastern University
Objectives
� Define psychotropics and discuss the different classes used in pediatrics
� Discuss barriers for the effective use of psychotropics in the pediatric population
� Understand the role that psychotropics play in the treatment of varying mental disorders
in the pediatric population
� Review the most commonly used psychotropics in pediatrics
� Describe important side effects and monitoring parameters for psychotropics used in the pediatric population
Introduction
� Psychotropic: a chemical substance that changes brain function and results in alteration of perception, mood, or consciousness
� Psychotropic Classes Utilized:� Antipsychotics
� Antidepressants
� Benzodiazepines
� Anticonvulsants
� Hypnotics
� Stimulants

12/21/2015
2
Barriers in Pediatric Psychopharmacology
� Limited research on existing medications for new indications
� Lack of adequately trained work force
�Consent
� Sets of knowledge and attitudes about
medications
� Competent to make the decision?
� Understanding changes with age
Barriers in Pediatric Psychopharmacology
�Compliance
� Network
� Attitude
� Ability to swallow
� Taste of the medication
� Adverse effects
Place of Medication in Therapeutic Planning
� Targets of Medication need to be:
� Clear enough to allow monitoring
� Practical enough to change
� Simple enough for explanation
� Targets:
� Symptoms
� Course of a condition

12/21/2015
3
Place of Medication in Therapeutic Planning
� Pharmacological versus Psychological interventions
� Advise patients on the best treatment for them
� Medication is not always a last resort
� Initial treatment based on each case
� Choice of intervention is not due to cause
Mental Illnesses in Pediatrics
� Attention Deficit Hyperactivity Disorder (ADHD): 8.4%
� Anxiety: 4.7%� Behavioral or conduct problems: 4.6%� Depression: 3.9%� Bipolar Disorder: 1.8%� Autism Spectrum Disorder: 1.1%
� Tourette's Syndrome: 0.3%� Schizophrenia: 0.23%� Substance Use Disorder
� Alcohol: 4.2%
� Illicit drug: 4.7%
� Cigarette 2.8%
SCHIZOPHRENIA

12/21/2015
4
Schizophrenia
�General principles:
• Antipsychotic drug regimens are the
cornerstone
• Require pharmacotherapy, family and
individual counseling
� Antipsychotics
• Safety and efficacy based on adult trials
• Young show greater sensitivity to adverse
events
Antipsychotics
�Recent randomized control trials on:
� Risperidone, olanzapine, aripiprazole,
paliperidone
�Choice of antipsychotic determined
primarily by side effect profile
� Atypicals preferred in young and
treatment naïve
� Start below the usual range for adults
and titrate slowly upwards to minimum effective dose
� First-Generation (aka typical):
� Haloperiodol (haldol): ≥3 years
� Trifluoperazine (Stelazine): ≥6 years
� Thiothixene (Navane): ≥12 years
� Second-Generation (aka atypical):
� Risperidone (Risperdal): ≥13 years
� Olanzapine (Zyprexa): ≥13 years
� Quetiapine (Seroquel):≥13 years
� Aripiprazole (Abilify): ≥13 years
� Paliperidone (Invega): ≥12 years
Antipsychotics

12/21/2015
5
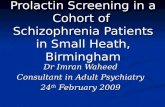
Schizophrenia: Recommended order of treatment
AtypicalAtypical
No response/ intolerable
No response/ intolerable
Different atypical or typical
Different atypical or typical
No Response/ intolerable
No Response/ intolerable
ClozapineClozapine
ResponseResponse
ResponseResponse
Continue for 2 yearsContinue
for 2 years
� First-Generation
� Extrapyramidal
motor symptoms (EPS)
•Dystonia
• Parkinsonism
•Akathesia
• Tardive Dyskinesia
� Second-Generation
� Obesity
� � triglycerides
� � Nonhigh-density
lipoprotiens
� � Cholesterol
� � Glucose
� Diabetes II
� Hyperprolactinemia
Antipsychotics: Adverse Events
�Weight gain� Greatest with Olanzapine
� Least with aripiprazole
�EPS� Greater with typicals (eg: haloperidol) and higher doses of risperidone
� Aripiprazole: akathisia
Antipsychotics: Adverse Events

12/21/2015
6
�Sedation� Greater with olanzapine, clozapine, quetiapine and haloperidol than with risperidone and aripiprazole
�Hyperprolactinaemia� Greatest with risperidone and haloperidol
� Least with quetiapine and aripiprazole
Antipsychotics: Adverse Events
Antipsychotics: Monitoring
�Baseline Monitoring
� Physical examination
•Height & weight (BMI)
•CV exam: pulse & BP
•Neurological exam: evidence of
abnormal movement
� Labs:
•CBC, LFTs, BMP, prolactin, fasting BG, HbA1c, plasma lipids
�Monitoring while on treatment
� Weight:
•Weekly 1st 6 wks
•At 12 wks
•Every 6 months thereafter
� Pulse, BP, prolactin, fasting BG, HbA1c,
lipids
•At 12 wks
•Every 6 months thereafter
Antipsychotics: Monitoring

12/21/2015
7
BIPOLAR DISORDER
Bipolar Disorder
�General Approaches
• Focus treatment on most disabling
aspects
• Later treatment can address other issues
• Must consider common issues affecting children and adolescents, such as
substance abuse and pregnancy
• Comprehensive treatment requires both psychotherapy and psychopharmacology
• Treatment must address the phase of the illness
Step 1: Initiate antimanic agent
1st-line: lithium, valproate, carbamazepine, risperidone, olanzapine, quetiapine
Step 1: Initiate antimanic agent
1st-line: lithium, valproate, carbamazepine, risperidone, olanzapine, quetiapine
Full Response: - Continue maintenance treatment (with side effect monitoring)- Proceed to Step 2
Full Response: - Continue maintenance treatment (with side effect monitoring)- Proceed to Step 2
Step 2: Assess and treat associated conditions- ADHD: consider stimulants- Depression/anxiety: consider SSRIs, lithium, lamotrigine, or atypical antipsychotic medication
Step 2: Assess and treat associated conditions- ADHD: consider stimulants- Depression/anxiety: consider SSRIs, lithium, lamotrigine, or atypical antipsychotic medication
Partial Response:- Consider augmentation with second antimanicagent- Consider how associated/comorbid conditions are affecting response
Partial Response:- Consider augmentation with second antimanicagent- Consider how associated/comorbid conditions are affecting response
Re-evaluate responseRe-evaluate response
Non Response or not tolerated:- Switch to other antimanicagent
Non Response or not tolerated:- Switch to other antimanicagent

12/21/2015
8
Bipolar Disorder: Mania
� Current available antimanic medications:
� Second-generation antipsychotics (SGA)
� Lithium
� Antiepileptic drugs (AED)
� Recent RCT support the following:
� SGA are effective and potentially superior
� Lithium’s role in pediatric BD is less clear
� AED may be less efficacious
� SGA
� Strongest efficacy data
� FDA-indications to treat mania or mixed states in 10-17 years:
• Risperidone, aripiprazole, quetiapine,
asenapine
� Lithium
� Mixed support for efficacy
� FDA-indicated to treat mania in 12 years and older
Bipolar Disorder: Mania
� Adverse Events:
� Early: fine tremor, polydipsia, polyuria,
nausea, malaise, weight gain, headache, diarrhea
� Late: continued hand tremor that may
worsen, polydipsia, polyuria, weight gain and edema, thyroid and renal
abnormalities, dermatologic abnormalities, fatigue, leukocytosis
Lithium: Adverse Events

12/21/2015
9
� Toxicity:
� Diarrhea, vomiting, mild ataxia, coarse
hand tremor, muscular weakness and fasciculations, drowsiness, sedation, slurred speech, and impaired
coordination
� Life-threatening toxic effects: cardiac
arrhythmias and severe central nervous system difficulties
Lithium: Adverse Events
� Serum Lithium Concentrations:
� Every 3-4 days during initiation
� 1-2 months once stabilized
� Obtain 8-12 hours post-dose
� Reference Range:
• Acute mania: 0.6-1.2 mEq/L
•Maintenance: 0.8-1 mEq/L
• Toxic: > 1.5 mEq/L
Lithium: Monitoring
� Baseline:
� CBC, urine analysis, pregnancy test,
thyroid function tests, ECG
� Serum Na, calcium, crieatinine, BUN
� EEG in children with seizures or known abnormalities in EEG
� Periodic Monitoring: thyroid, kidney,
and cardiac function
Lithium: Monitoring

12/21/2015
10
� AED:
� Weak evidence of efficacy
•Benefits seen in small open-label trials with carbamazepine, valproate, and
lamotrigine
� No placebo control group
� Safety data is stronger
Bipolar Disorder: Mania
Antiepileptics
� Valproic acid� Boxed Warnings:
•Hepatotoxicity and pancreatitis� More common in < 2 years old
•Mitochondrial disease
• Teratogenic
� Adverse effects:• Transient: nausea, vomiting, indigestion
• Psychiatric effects: emotional upset, depression, psychosis, aggression, hyperactivity, behavioral deterioration
• Thrombocytopenia
• Polycystic ovary syndrome
� Valproic acid
� Monitoring:
•Liver enzymes
� Especially during 1st 6 months
•CBC with platelets
� Prior to initiation and periodically
•Serum concentrations
� Trough: 50-125 mcg/mL
Antiepileptics

12/21/2015
11
�Carbamazepine
� Boxed Warnings
• Aplastic anemia/agranulocytosis
� Very rare
• Serious dermatologic reactions
� SJS/TEN
� HLA-B*1502 allele
� Adverse Effects: dizziness, drowsiness, unsteadiness, nausea, vomiting
� Monitoring:
• CBC with diff, LDL, LFTs, TSH, BUN, serum Na
• Serum levels: 4-12 mcg/mL
Antiepileptics
� Lamotrigine
� Boxed Warning: Serious skin rashes
• SJS/TEN
• Increased risk with age <12 or co-
administration of valproic acid
� Monitor:
• CBC with diff, kidney and liver function,
hypersensitivity reactions
Antiepileptics
� Lack of RCT to guide medication treatment of depression and anxiety in
BD
�Data suggests that:
� Youth spend considerable time struggling
with depression
� Youth often receive SSRIs with no induction to mania
� Risk of antidepressant-induced mania higher in prepubertal children
Bipolar Disorder: Depression

12/21/2015
12
DEPRESSION
Depression
� Type and intensity of treatment depends on severity
• Mild: assessment and education
• Moderate:
• NICE guidelines: CBT, IPT, or family therapy
first; then add medication if no response
• Never use antidepressants without psychotherapy
• AACAP guidelines:
• Combination therapy preferable
• Monotherapy acceptable in certain cases
• Persistent or Severe:
• SSRIs, CBT, IPT, or combination
� Progress should be reassessed in 4-6 weeks
� Tricyclic antidepressants:
� Not efficacious
� Selective Serotonin Reuptake Inhibitors:
� Fluoxetine (Prozac): first-line
•Only agent recommended for use in
adolescents by NICE guidelines
• FDA-approved for both preadolescent and
adolescent depression (≥ 8 years)
Depression

12/21/2015
13
� Selective Serotonin Reuptake Inhibitors:
� Escitalopram (Lexapro):
• FDA-approved for depression in 12-17 years
� Sertraline (Zoloft):
•Has been reported superior to placebo
•Not FDA approved for pediatric depression
� Citlaopram (Celexa):
• Found to be as efficacious as fluoxetine
• Not FDA approved for pediatric depression
� Paroxetine (Paxil):
• Not recommended
Depression
SSRIs: Adverse Effects & Monitoring
�Headache, N/V, diarrhea, sleep disturbance, weight gain/loss,
anxiety, SIADH
� Behavioral disinhibition
� Sexual dysfunction
� Serotonin Syndrome
�Discontinuation syndrome
SSRIs: Adverse Effects & Monitoring
� Suicidal ideation
� Incidence is rare
• Studies have shown attempts more
common prior to initiation of SSRI
� Occurs within first 3-5 wks
� Combination of meds and therapy
needed
�Monitoring: weight, CBC, LFTs,
Electrolytes, suicidality

12/21/2015
14
�Only two non-SSRIs with some support for efficacy in adolescents:
� Nefazodone (Serzone)
• Increased risk of hepatotoxicity
� Venlafaxine (Effexor)
• Post-hoc analysis of two clinical trials:
� Showed efficacy in adolescent, but not
preadolescent, depression
� As efficacious as fluoxetine in treatment resistant
depression
� Bupropion (Wellbutrin):
� Only open-label studies
Depression
Depression
� Treatment-resistant depression
� Non-response to SSRI: switch to
another SSRI and add CBT
� Non-response with two consecutive
trials of SSRIs: consider other classes
• Ex: Venlafaxine, bupropion
� If partial response: augment with an antipsychotic, bupropion, or lithium
• No empirical studies in the youth
ANXIETY

12/21/2015
15
Anxiety
� Several effective approaches, both psychotherapeutic and psychopharmacological, have been documented• Studies show additive effects of using combination over either alone
�SSRIs are highly effective• Sertraline, fluoxetine, paroxetine, fluvoxamine
• Efficacious for anxiety experienced while in the feared situation• Not as good for anticipatory anxiety
OBSESSIVE COMPULSIVE
DISORDER
Obsessive Compulsive Disorder
�Relative abundance of RCT demonstrating efficacy with:
� SSRIs: Sertraline, fluoxetine, paroxetine, fluvoxamine
• Fluvoxamine FDA-approved for ≥ 8 years
• Fluoxetine FDA-approved for ≥ 7 years
• Sertraline FDA-approved for ≥ 6 years
� Clomipramine
• FDA-approved for ≥ 10 years
•Meta-analysis showed superiority to SSRIs

12/21/2015
16
Clomipramine: Adverse Events
�Class: Tricyclic antidepressant
� Adverse Events:
� Anticholinergic effects
� CND depression
� Hematologic effects
� Orthostatic hypotension
� Seizures
� Sexual dysfunction
� Weight gain
� Conduction abnormalities
�Weight
� Pulse rate and BP
� Prior to and during therapy
� EEG and cardiac status
� LFTs
�CBC with diff
� In patients who develop fever and sore throat during treatment
Clomipramine: Monitoring
�Combination Treatment
� Studies show superiority of CBT with
medication than to medication or CBT alone
� While medications alone help, CBT is first-line
� Augmentation strategies
� In adults: SGA, clonazepam, morphine
• No controlled studies to guide clinicians for
child and adolescent treatment-resistance
Obsessive Compulsive Disorder

12/21/2015
17
AUTISM SPECTRUM DISORDER
Autism Spectrum Disorder
� Nonpharmacological interventions are first-line� Psychotropics for more severe cases
� Systematic reviews have demonstrated some evidence for use of antipsychotics� Disagreement in the field exists
• NICE guidelines do not recommend antipsychotics for core treatment of ASD
• AACAP guidelines recommend the use of pharmacotherapy when there is a specific target symptom or comorbid condition
� Pharmacotherapy used to allow child to better engage in treatment plans
ASD: Antipsychotics
�Management of maladaptive behaviors
�Haloperidol (Haldol)
� Not FDA approved, but most commonly studied prior the SGA
�Risperidone (Risperdal)
� FDA-approved for treatment of irritability associated with ASD in 5-15 years
� Aripiprazole (Abilify)
� FDA-approved for treatment of irritability
associated with ASD in 6-17 years

12/21/2015
18
ASD: Antipsychotics
�Other SGA researched in ASD:
� Olanzapine (Zyprexa)
• Placebo-controlled, double blind study
• Positive efficacy for aggression and irritability
� Agents with modest efficacy in reducing irritability
• Clozapine (Clozaril)
• Ziprasidone (Geodon)
•Quetiapine (Seroquel)
ASD: Antidepressants
� SSRIs studied and used in clinical practice for the repetitive behaviors in
ASD
� Overall efficacy appears inconsistent
• A systematic review in 2010 showed no data
supporting their use in ASD and strong data
recording incidence of ADE
� Antidepressants evaluated:
� Clomipramine
� Fluoxetine, sertraline, escitalopram, fluvoxamine
� Psychostimulants for the treatment of ADHD-like symptoms have been used
with mixed results
� Amphetamines have limited efficacy data, with no controlled studies since 1970s
� Results indicate minimal benefit and potential ADE, including worsening of ASD symptoms
� Clonidine and guanfacine: moderate
efficacy in reducing stereotypy, hyperactivity, and irritability
ASD: Psychostimulants

12/21/2015
19
OPPOSITIONAL DEFIANT
& CONDUCT DISORDERS
Oppositional and Conduct Disorders
� Differing views as to the usefulness of medications
� Prescribing medications is increasing� Modest evidence for effectiveness
� Antipsychotics: risperidone, aripiprazole• Clinical experience suggests they can reduce
aggression in some cases
� Mood stabilizers: lithium, carbamezapine
� Buspirone, clonidine
� Best studied pharmacological interventions in youth with ODD/CD and ADHD: psychostimulants
TIC DISORDERS

12/21/2015
20
Tic Disorders
�Decision on use of medications depends on clinical presentation and
level of symptoms
� Best to withhold medication use until tic become a significant source of impairment
� Many cases can be managed without medications
� Treat co-morbid conditions first
�Goal of pharmacotherapy: use as little medication as possible to render tics
more tolerable
� Typical antipsychotics remain most predictably effective tic-suppressing agents� Haloperidol, pimozide, fluphenazine
•Haloperidole FDA-approved for ≥3 years
• Pimozide FDA-approved for ≥ 2 years
� To avoid EPS, atypicals have been used to treat tic symptoms� Risperidone, olanzapine, ziprasidone, aripiprazole•Only aripiprazole FDA-approved for 6-18 years
� Botulinum toxin injections
Tic Disorders
Summary
�Greater barriers to the effective use of psychotropic medications exist in pediatric population
� Psychotropics are not always a last resort treatment
�Use of specific psychotropic agents should be guided by the best available evidence
�Monitoring patients for improvement and ADE should be part of the treatment plan

12/21/2015
21
True or False?
�One barrier to the effective use of psychotropic medications in pediatrics may be inadequate adult supervision.
� Psychotropics are a last resort treatment, only to be used after all other methods have failed.
� The second generation antipsychotics are the standard for treating the first episode of psychosis in pediatric patients with risperidone being the most widely used atypical.
References1. Brent D, Maalouf F. Chapter 63: Depressive disorders in childhood
and adolescence. In: Thapar, Pine, Leckman, Scott, Snowling, & Taylor, Eds. Rutter’s Child and Adolescent Psychiatry Sixth Edition. Oxford, UK: John Wiley & Sons, Ltd; 2015: 874-892.
2. Emslie GJ. Pediatric psychopharmacology trials: Beyond Efficacy. Am J Psychiatry. 2015; 172 (12): 1171-1172.
3. Green WH. Child and Adolescent Clinical Psychopharmacology Fourth Edition. Philadelphia, PA: Lippincott Williams & Wilkins; 2007.
4. Hollis C & Palaniyappan. Chapter 57: Schizophrenia and psychosis. In: Thapar, Pine, Leckman, Scott, Snowling, & Taylor, Eds. Rutter’s Child and Adolescent Psychiatry Sixth Edition. Oxford, UK: John Wiley & Sons, Ltd; 2015: 774-792.
5. Leckman JF, Bloch M. Chapter 56: Tic disorders. In: Thapar, Pine, Leckman, Scott, Snowling, & Taylor, Eds. Rutter’s Child and Adolescent Psychiatry Sixth Edition. Oxford, UK: John Wiley & Sons, Ltd; 2015: 757-773.
6. Leibenluft E, Dickstein DP. Chapter 62: Bipolar disorder in childhood. In: Thapar, Pine, Leckman, Scott, Snowling, & Taylor, Eds. Rutter’s Child and Adolescent Psychiatry Sixth Edition. Oxford, UK: John Wiley & Sons, Ltd; 2015: 858-873.
7. Merikangas KR, Nakamura EF, Kessler RC. Epidemiology of mental disorders in children and adolsecents. Dialogue in Clinical Neuroscience. 2009; 11 (1):7-20.
References8. Perou R, Bitsko RH, Blumberg SJ, et al. Mental health surveillance among children
– United States, 2005-2022. Centers for Disease Control and Prevention Morbidity and Mortality Weekly Report. 2013; 62 (2):1-36.
9. Pine DS, Klein RG. Chapter 60: Anxiety disorders. In: Thapar, Pine, Leckman, Scott, Snowling, & Taylor, Eds. Rutter’s Child and Adolescent Psychiatry Sixth Edition. Oxford, UK: John Wiley & Sons, Ltd; 2015: 882-840.
10. Rapoport JL. Shaw P. Chapter 61: Obsessive compulsive disorders. In: Thapar, Pine, Leckman, Scott, Snowling, & Taylor, Eds. Rutter’s Child and Adolescent Psychiatry Sixth Edition. Oxford, UK: John Wiley & Sons, Ltd; 2015: 841-857.
11. Rey JA. Chapter 28: Autism spectrum disorders. In: Benavides S & Nahata MC, Eds. Pediatric Pharmacotherapy. Lenexa, Kansas: American College of Clinical Pharmacy; 2013:409-422.
12. Scott S. Chapter 65: Oppositional and conduct disorders. In: Thapar, Pine, Leckman, Scott, Snowling, & Taylor, Eds. Rutter’s Child and Adolescent Psychiatry Sixth Edition. Oxford, UK: John Wiley & Sons, Ltd; 2015: 913-930.
13. Taylor E. Chapter 43: Pharmacological, medically-led and related treatments. In: Thapar, Pine, Leckman, Scott, Snowling, & Taylor, Eds. Rutter’s Child and Adolescent Psychiatry Sixth Edition. Oxford, UK: John Wiley & Sons, Ltd; 2015: 559-571.
14. Volkmar F, Siegel M, Woodbury-Smith M, et al. Practice parameter for the assessment and treatment of children and adolescents with autism spectrum disorder. Journal of the American Academy of Child and Adolescent Psychiatry. 2014; 53(2): 237-257.
15. Walkup J, et al. Practice parameter on the use of psychotropic medication in children and adolsecents. Journal of the American Academy of Child and Adolescent Psychiatry. 2009; 48(9): 961-973.