
The use of electrical stimulation to guide epidural and intrathecal needle advancement at the L 5 -L...
5
SHORT COMMUNICATION The use of electrical stimulation to guide epidural and intrathecal needle advancement at the L 5 -L 6 intervertebral space in dogs Pablo E Otero*, Natali Verdier*, Martin R Ceballos*, Lisa Tarragona*, Myriam Flores* & Diego A Portela† *Anaesthesiology Department, College of Veterinary Medicine, University of Buenos Aires, Buenos Aires, Argentina †Department of Clinical Sciences, College of Veterinary Medicine, Cornell University, Ithaca, NY, USA Correspondence: Pablo E Otero, Anaesthesiology Department, College of Veterinary Medicine, University of Buenos Aires, Av. Chorroar ın 280, C1427CWO Buenos Aires, Argentina. E-mail: [email protected] Abstract Objective To determine the minimal electrical threshold (MET) necessary to elicit appropriate muscle contraction when the tip of an insulated needle is positioned epidurally or intrathecally at the L 5-6 intervertebral space (phase-I) and to determine whether the application of a fixed electrical current during its advancement could indicate needle entry into the intrathecal space (phase-II) in dogs. Study design Prospective, blinded study. Animals Thirteen (phase-I) and seventeen (phase- II) dogs, scheduled for a surgical procedure where L 5-6 intrathecal administration was indicated. Methods Under general anesthesia, an insulated needle was first inserted into the L 5-6 epidural space and secondly into the intrathecal space and the MET necessary to obtain a muscular contraction of the pelvic limb or tail at each site was determined (phase- I). Under similar conditions, in dogs of phase-II an insulated needle was inserted through the L 5-6 intervertebral space guided by the use of a fixed electrical current (0.8 mA) until muscular contrac- tion of the pelvic limb or tail was obtained. Intrathe- cal needle placement was confirmed by either free flow of cerebrospinal fluid (CSF) or myelography. Results The current required to elicit a motor response was significantly lower (p < 0.0001) when the tip of the needle was in the intrathecal space (0.48 0.10 mA) than when it was located epi- durally (2.56 0.57). The use of a fixed electrical stimulation current of 0.8 mA resulted in correct prediction of intrathecal injection, corroborated by either free flow of CSF (n = 12) or iohexol distribu- tion pattern (n = 5), in 100% of the cases. Conclusion and clinical relevance Nerve stimula- tion may be employed as a tool to distinguish epidural from intrathecal insulated needle position at the L 5-6 intervertebral space in dogs. This study demonstrates the feasibility of using an electrical stimulation test to confirm intrathecal needle position in dogs. Keywords dog, electrical threshold, epidural, intra- thecal, nerve stimulation test. Introduction Intrathecal anesthesia has some advantages over epidural anesthesia, including faster onset and offset of action, lower systemic absorption of drugs and the possibility to use different weight solutions to target the metameric region to be blocked (Sarotti et al. 2013). However, the difficulty in performing the technique may be compounded by the lack of a free flow of cerebrospinal fluid (CSF) that can be used to confirm correct needle placement. In dogs, Sarotti et al. (2011) reported a failure rate of 26% during the first stage of learning curve, which improved to 10% in experienced hands. 1 Veterinary Anaesthesia and Analgesia, 2014 doi:10.1111/vaa.12137
Transcript of The use of electrical stimulation to guide epidural and intrathecal needle advancement at the L 5 -L...

SHORT COMMUNICAT ION
The use of electrical stimulation to guide epidural and
intrathecal needle advancement at the L5-L6 intervertebral
space in dogs
Pablo E Otero*, Natali Verdier*, Martin R Ceballos*, Lisa Tarragona*, Myriam Flores* & Diego A Portela†
*Anaesthesiology Department, College of Veterinary Medicine, University of Buenos Aires, Buenos Aires, Argentina
†Department of Clinical Sciences, College of Veterinary Medicine, Cornell University, Ithaca, NY, USA
Correspondence: Pablo E Otero, Anaesthesiology Department, College of Veterinary Medicine, University of Buenos Aires, Av. Chorroar�ın
280, C1427CWO Buenos Aires, Argentina. E-mail: [email protected]
Abstract
Objective To determine the minimal electrical
threshold (MET) necessary to elicit appropriate
muscle contraction when the tip of an insulated
needle is positioned epidurally or intrathecally at the
L5-6 intervertebral space (phase-I) and to determine
whether the application of a fixed electrical current
during its advancement could indicate needle entry
into the intrathecal space (phase-II) in dogs.
Study design Prospective, blinded study.
Animals Thirteen (phase-I) and seventeen (phase-
II) dogs, scheduled for a surgical procedure where
L5-6 intrathecal administration was indicated.
Methods Under general anesthesia, an insulated
needle was first inserted into the L5-6 epidural space
and secondly into the intrathecal space and the MET
necessary to obtain a muscular contraction of the
pelvic limb or tail at each site was determined (phase-
I). Under similar conditions, in dogs of phase-II an
insulated needle was inserted through the L5-6intervertebral space guided by the use of a fixed
electrical current (0.8 mA) until muscular contrac-
tion of the pelvic limb or tail was obtained. Intrathe-
cal needle placement was confirmed by either free
flow of cerebrospinal fluid (CSF) or myelography.
Results The current required to elicit a motor
response was significantly lower (p < 0.0001) when
the tip of the needle was in the intrathecal space
(0.48 � 0.10 mA) than when it was located epi-
durally (2.56 � 0.57). The use of a fixed electrical
stimulation current of 0.8 mA resulted in correct
prediction of intrathecal injection, corroborated by
either free flow of CSF (n = 12) or iohexol distribu-
tion pattern (n = 5), in 100% of the cases.
Conclusion and clinical relevance Nerve stimula-
tionmay be employed as a tool to distinguish epidural
from intrathecal insulated needle position at the L5-6intervertebral space in dogs. This study demonstrates
the feasibility of using an electrical stimulation test to
confirm intrathecal needle position in dogs.
Keywords dog, electrical threshold, epidural, intra-
thecal, nerve stimulation test.
Introduction
Intrathecal anesthesia has some advantages over
epidural anesthesia, including faster onset and offset
of action, lower systemic absorption of drugs and the
possibility to use different weight solutions to target
the metameric region to be blocked (Sarotti et al.
2013). However, the difficulty in performing the
technique may be compounded by the lack of a free
flow of cerebrospinal fluid (CSF) that can be used to
confirm correct needle placement. In dogs, Sarotti
et al. (2011) reported a failure rate of 26% during
the first stage of learning curve, which improved to
10% in experienced hands.
1
Veterinary Anaesthesia and Analgesia, 2014 doi:10.1111/vaa.12137

Nerve stimulation has been used to confirm
epidural or intrathecal needle placement in humans,
pigs (Tsui et al. 2004, 2005), rabbits, cats (Otero
et al. 2012, 2013) and dogs (Garcia-Pereira et al.
2010). Moreover, it has been proposed to confirm
intrathecal injection in the absence of CSF in the
needle hub (Tsui 2006; Otero et al. 2012). Although
the minimal electrical threshold (MET) necessary to
elicit pelvic limb or tail muscle contraction when the
tip of an insulated needle is located in the epidural
space at the lumbosacral region has been reported in
dogs (Garcia-Pereira et al. 2010), to our knowledge
approach through a lumbar intervertebral space has
not been studied.
The purpose of the two stage study reported here
was to determine the MET necessary to elicit
appropriate muscle contraction when the tip of an
insulated needle is positioned epidurally and intra-
thecally at the L5-6 intervertebral space (phase I) and
to determine whether the application of a fixed
electrical current during the advancement of an
insulated needle could be used to confirm the needle
tip introduction into the intrathecal space (phase II)
in dogs.
Materials and methods
Animals
This study was approved by the Institutional Animal
Care and Use Committee, College of Veterinary
Medicine, University of Buenos Aires (Project num-
ber 2012/14). Thirteen (phase I) and seventeen
(phase II) dogs, admitted to the Veterinary Teaching
Hospital for different surgical procedures during
which intrathecal anesthesia was scheduled as part
of the analgesic protocol, were enrolled. Written
informed consent was obtained from the owners
prior to participation in the study.
Anesthesia and preparation of animals
Dogs were premedicated with acepromazine (0.02
mg kg�1; Inadrin; Laboratorios Richmond, Argen-
tina) plus morphine (0.3 mg kg�1; Analmorph; Dr.
Gray S.A.C.I., Argentina) by intramuscular (IM)
injection. Fifteen minutes after premedication, a
cannula was placed in a cephalic vein and anesthesia
was induced with propofol (1–5 mg kg�1; Propovet;
Laboratorios Richmond) administered intravenously
to effect, followed by tracheal intubation. Anesthesia
was maintained with isoflurane (Forane; Abbott
Laboratories, Argentina) in oxygen using a circle
breathing system allowing spontaneous breathing.
Throughout anesthesia, heart rate, respiratory rate,
non-invasive arterial blood pressure, end-tidal car-
bon dioxide concentration, end-tidal isoflurane con-
centration, esophageal temperature, hemoglobin
oxygen saturation and lead II electrocardiogram
were continuously monitored (VET 420F; Goldway
US, NY, USA). When anesthesia was stable, the hair
over L3-S1 vertebrae was clipped and the skin
aseptically prepared. Animals were placed in sternal
recumbency, with the pelvic limbs flexed at the hips.
The use of a cradle allowed flexion of the lumbar spine
to facilitate epidural and intrathecal access through a
paramedian approach at the L5-6 intervertebral
space, as previously described (Otero & Campoy
2013).
Phase-I (Epidural and intrathecal MET
determination)
A 30° short bevel 22-gauge, 50 mm insulated
needle without its extension line (SonoPlex Stim
cannula; Pajunk GmbH, Germany) was inserted into
the epidural space, using the loss of resistance
technique with air (limited to 0.03 mL kg�1). When
the epidural space was identified, the needle hub was
observed for 60 seconds for absence of CSF. Then, a
second investigator connected the needle to a
peripheral nerve stimulator (NS) (MultiStim
SWITCH, Pajunk, Dyna Medical Corp, UK). The
negative lead of the NS was attached to the insulated
needle, while the positive lead was placed on the skin
over the caudal aspect of the thigh. The NS was set to
a frequency of 2 Hz, pulse width of 0.1 ms, and the
current was gradually increased from 0 mA and by
0.01 mA until pelvic limb or tail motor response was
elicited. When these muscle twitches were evident,
the delivered stimulating current was recorded as
METepi. The NS was then turned off and the needle
was advanced until CSF was obtained. A separate
investigator turned on the NS for MET determina-
tion. The procedure was abandoned if CSF was not
present. The delivered stimulating current necessary
to elicit pelvic limb or tail motor response was
recorded as METint as described above. Before needle
withdrawal, a solution of 0.5% hyperbaric bupiva-
caine (Caina-G Hiperb�arica; Dr. Gray S.A.C.I.) con-
taining 0.1 mg mL�1 of morphine (Duramorph; Dr.
Gray S.A.C.I.) in a total volume of 0.05 mL kg�1
was administered intrathecally to all dogs in prep-
aration for the surgical procedure.
© 2014 Association of Veterinary Anaesthetists and the American College of Veterinary Anesthesia and Analgesia2
Neuraxial electrical stimulation in dogs PE Otero et al.
Phase-II (Electrical stimulation test)
After analyzing the results of phase I, a new group of
seventeen dogs was enrolled. Anesthesia and instru-
mentation were performed as in phase I. For this
group a 30° short bevel 24-gauge 25 mm or a
22-gauge 50 mm insulated needle without their
extension lines were used. After the needle pene-
trated the skin, a separate investigator connected the
NS which, based on the phase I results, was set to a
fixed current of 0.8 mA, frequency of 2 Hz and pulse
width of 0.1 ms. The needle was advanced into the
intrathecal space. As soon as muscle twitching was
detected, needle advancement was stopped and the
current was lowered by 0.01 mA to determine the
threshold for motor activity (METphase-II). The NS
was then turned off and if CSF was present in the hub
of the needle, 0.05 mL kg�1 of the same bupiva-
caine and morphine solution used in phase I was
injected. If CSF was absent (dry tap), the anesthetic
solution was injected followed by 1–2 mL of iohexol
and a radiograph of the lumbar area was obtained to
confirm intrathecal injection.
Complications such as prolonged neural deficit or
pain around the injection site were noted until
the dogs were discharged from the hospital
24–48 hours after surgery.
Statistical analysis
After the normality distribution of data was con-
firmed (Shapiro-Wilk test), statistical significance
between METepi and METint was determined using a
paired t-test. Differences were judged to be signifi-
cant when p < 0.05. Data distributed normally are
presented as mean � SD values.
Accuracy of the electrical stimulation test was
measured by positive predictive value (PPV). PPV
were calculated as the number of times the intra-
thecal space was reached within two SD of the
METint divided by the total number of accesses
performed. Confidence limits (95%) were calculated
according to the Clopper–Pearson method.
Results
Thirteen dogs ASA I-III (9 non-spayed females and 4
non-neutered males) weighing 16.4 � 8.4 kg and
aged 4.0 � 2.4 years and seventeen non-spayed
females dogs ASA I-II weighing 12.6 � 8.8 kg and
aged 4.4 � 3.8 years were included in phase I and
II, respectively.
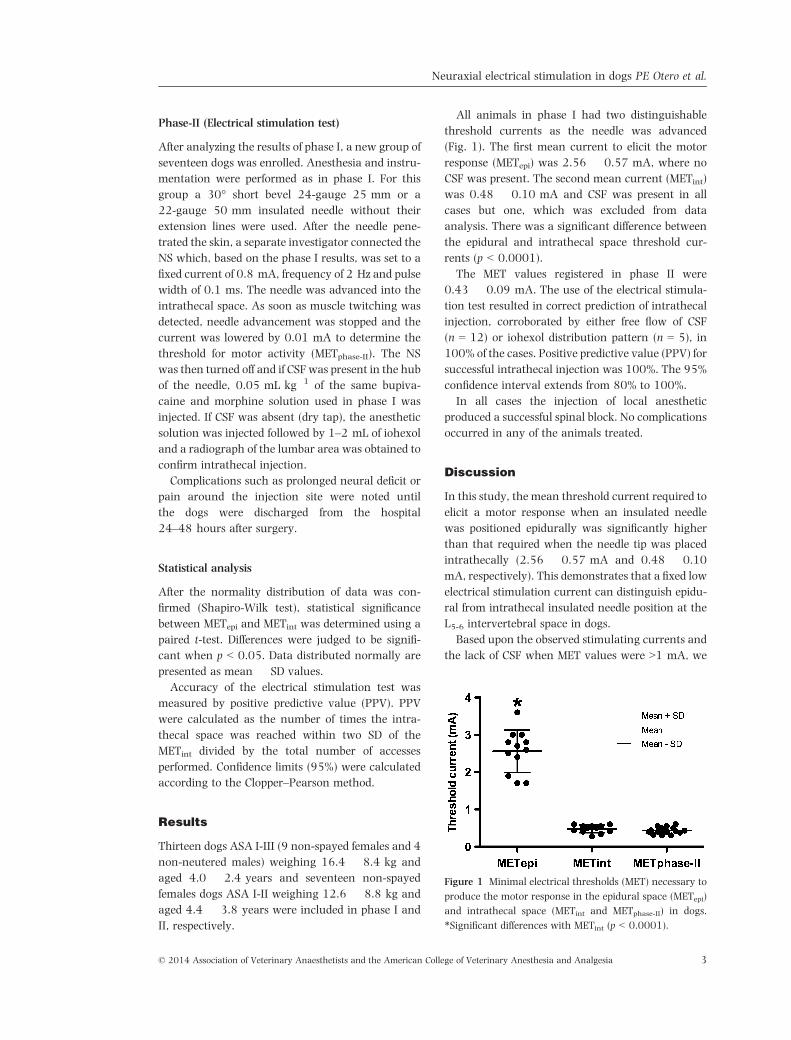
All animals in phase I had two distinguishable
threshold currents as the needle was advanced
(Fig. 1). The first mean current to elicit the motor
response (METepi) was 2.56 � 0.57 mA, where no
CSF was present. The second mean current (METint)
was 0.48 � 0.10 mA and CSF was present in all
cases but one, which was excluded from data
analysis. There was a significant difference between
the epidural and intrathecal space threshold cur-
rents (p < 0.0001).
The MET values registered in phase II were
0.43 � 0.09 mA. The use of the electrical stimula-
tion test resulted in correct prediction of intrathecal
injection, corroborated by either free flow of CSF
(n = 12) or iohexol distribution pattern (n = 5), in
100% of the cases. Positive predictive value (PPV) for
successful intrathecal injection was 100%. The 95%
confidence interval extends from 80% to 100%.
In all cases the injection of local anesthetic
produced a successful spinal block. No complications
occurred in any of the animals treated.
Discussion
In this study, the mean threshold current required to
elicit a motor response when an insulated needle
was positioned epidurally was significantly higher
than that required when the needle tip was placed
intrathecally (2.56 � 0.57 mA and 0.48 � 0.10
mA, respectively). This demonstrates that a fixed low
electrical stimulation current can distinguish epidu-
ral from intrathecal insulated needle position at the
L5-6 intervertebral space in dogs.
Based upon the observed stimulating currents and
the lack of CSF when MET values were >1 mA, we
Figure 1 Minimal electrical thresholds (MET) necessary to
produce the motor response in the epidural space (METepi)
and intrathecal space (METint and METphase-II) in dogs.
*Significant differences with METint (p < 0.0001).
© 2014 Association of Veterinary Anaesthetists and the American College of Veterinary Anesthesia and Analgesia 3
Neuraxial electrical stimulation in dogs PE Otero et al.

concluded that, if loss of resistance was present,
these needles were most likely in the epidural space.
Confirmation of intrathecal injections was per-
formed by obtaining CSF in the hub of the needle
or by typical iohexol distribution pattern within the
subarachnoid space.
The results of this study are in agreement with
those reported in other species. In pigs (Tsui et al.
2004) and humans (Tsui et al. 2005) the METs
tested in lumbar segments of the spinal cord are
>1 mA in the epidural space and <1 mA in the
intrathecal space. Garcia-Pereira et al. (2010)
reported in dogs a MET value of 0.3 mA when the
needle was placed in the lumbosacral epidural space.
In contrast, METepi in this study was 2.56 � 0.57
mA. Based on the fact that the lesser the distance
between the nerve and the tip of the stimulating
device, the lower the MET needed to stimulate it
(Ford et al. 1984), the difference found between
these epidural MET values could be explained by
closeness of the needle to the centrally running
nerve roots at the lumbosacral level.
Air was preferred over saline when performing
loss of resistance for this study to avoid confusion
between injected saline and CSF. The amount of air
injected was limited to 0.03 mL kg�1 to minimize
hindrance to electrical conduction.
In this study, the METint was 0.48 � 0.10 mA
and did not overlap the METepi (2.56 � 0.57 mA).
Our METint values were similar to those reported in
humans (Tsui et al. 2005), pigs (Tsui et al. 2004),
rabbits (Otero et al. 2012) and cats (Otero et al.
2013). The information on needle tip position and
the different thresholds registered provided the
framework for applying a current of fixed frequency
and intensity (2 Hz, and 0.8 mA) during intrathecal
needle insertion. Based on these results, with 95%
confidence, the intensity of the electrical current
needed to perform the technique should be between
the lower METepi [1.42 mA (mean �2SD)] and the
higher METint [0.68 mA (mean +2SD)]. In this
study, every motor response obtained with 0.8 mA
during needle insertion indicated that the stimulat-
ing needle was inside the intrathecal space. More-
over, the use of the electrical stimulation test
resulted in 100% of intrathecal injections. However,
since the observed values were given under the
specific settings for the small sample studied, the
lower 95% confidence limit for the 100% PPV
reported here can still be as low as 80%. Further
studies with a larger sample size are needed to
determine the advantages of nerve stimulation when
used to confirm intrathecal needle placement.
Although the prevalence of dry tap has not been
reported in dogs, Sarotti et al. (2011, 2013) referred
a procedural failure rate, defined as absence of CSF in
the needle for unspecified cause, of 10% and 7%,
respectively. It should be noted that the occurrence
of dry tap in this study was 29.4%. Possible causes of
dry taps in this study are sternal recumbency
position with the lumbar spine curved dorsally and
the needle positioned vertically that may have acted
in opposition to CSF spontaneous free flow. Addi-
tionally, the lack of stylet could have resulted in a
blocked needle.
In summary, at the L5-6 intervertebral space in
dogs, significantly lower electrical currents are
required to elicit a muscular response when the tip
of an insulated needle is located in the intrathecal
space than when it is placed epidurally. Additionally,
the present study demonstrated the feasibility of
using an electrical stimulation test with a fixed
current of 0.8 mA to confirm intrathecal needle
position in dogs.
Acknowledgements
This work was financed by UBACyT program,
University of Buenos Aires.
References
Ford DJ, Pither C, Raj PP (1984) Comparison of insulated
and uninsulated needles for locating peripheral nerves
with a peripheral nerve stimulator. Anesth Analg 63,
925–928.
Garcia-Pereira FL, Hauptman J, Shih AC et al. (2010)
Evaluation of electric neurostimulation to confirm
correct placement of lumbosacral epidural injections in
dogs. Am J Vet Res 71, 157–160.
Otero PE, Campoy L (2013) Epidural and spinal anesthesia.
In: Small Animals Regional Anesthesia and Analgesia.
Campoy L, Read M (eds). Wiley-Blackwell, New York,
USA. pp. 227–260.
Otero PE, Portela DA, Brinkyer JA et al. (2012) Use of
electrical stimulation to monitor lumbosacral epidural
and intrathecal needle placement in rabbits. Am J Vet
Res 73, 1137–1141.
Otero PE, Zaccagnini AS, Fuensalida SE et al. (2013) Use of
electrical nerve stimulation to monitor lumbosacral
epidural needle placement in cats. Vet Anaesth Analg
doi:10.1111/vaa.12107.
Sarotti D, Rabozzi R, Corletto F (2011) Efficacy and side
effects of intraoperative analgesia with intrathecal
© 2014 Association of Veterinary Anaesthetists and the American College of Veterinary Anesthesia and Analgesia4
Neuraxial electrical stimulation in dogs PE Otero et al.

bupivacaine and levobupivacaine: a retrospective study
in 82 dogs. Vet Anaesth Analg 38, 240–251.
Sarotti D, Rabozzi R, Franci P (2013) A retrospective study
of efficacy and side effects of intrathecal administration of
hyperbaric bupivacaine and morphine solution in 39
dogs undergoing hind limb orthopaedic surgery. Vet
Anaesth Analg 40, 220–224.
Tsui BC (2006) Verifying spinal needle location in the
presence of a “dry tap”. Can J Anaesth 53, 424–425.
Tsui BC, Wagner A, Finucane B (2004) The threshold
current in the intrathecal space to elicit motor response is
lower and does not overlap that in the epidural space: a
porcine model. Can J Anaesth 51, 690–695.
Tsui BC, Wagner AM, Cunningham K et al. (2005) Can
continuous low current electrical stimulation distinguish
insulated needle position in the epidural and intrathecal
spaces in pediatric patients? Paediatr Anaesth 15, 959–
963.
Received 5 August 2013; accepted 30 October 2013.
© 2014 Association of Veterinary Anaesthetists and the American College of Veterinary Anesthesia and Analgesia 5
Neuraxial electrical stimulation in dogs PE Otero et al.


















