
The Use of Atypical Antipsychotics in Borderline...
20
The Use of Atypical Antipsychotics in Borderline Personality Disorder (BPD): Black, White or Gray? Sarah Norman, PharmD PGY2 Psychiatric Pharmacy Resident The University of Texas at Austin College of Pharmacy Austin, Texas October 17, 2014 Learning Objectives: 1. Review the epidemiology, pathophysiology, and treatment of BPD 2. Review the mechanism of action and potential role for atypical antipsychotics in managing BPD 3. Evaluate the literature for atypical antipsychotic use in the treatment of BPD 4. Formulate evidence based conclusions regarding place of atypical antipsychotics in the treatment of BPD
-
Upload
truongkhanh -
Category
Documents
-
view
222 -
download
4
Transcript of The Use of Atypical Antipsychotics in Borderline...

The Use of Atypical Antipsychotics in Borderline Personality Disorder (BPD): Black, White or Gray?
Sarah Norman, PharmD PGY2 Psychiatric Pharmacy Resident
The University of Texas at Austin College of Pharmacy Austin, Texas
October 17, 2014
Learning Objectives: 1. Review the epidemiology, pathophysiology, and treatment of BPD 2. Review the mechanism of action and potential role for atypical antipsychotics in managing BPD 3. Evaluate the literature for atypical antipsychotic use in the treatment of BPD 4. Formulate evidence based conclusions regarding place of atypical antipsychotics in the treatment of BPD
Norman 2
1. Epidemiology A. Prevalence1-3
i. Lifetime – 6% ii. Inpatient mental health treatment – 20%
iii. Outpatient mental health treatment – 10% iv. Outpatient primary care treatment – 6% v. Female vs. Male - 4:1
B. Risk Factors4-6 i. Environmental
1. Separation from parent(s) at an early age 2. Abuse – physical, emotional or sexual 3. Unsupportive or inconsistent care
ii. Biological 1. First degree relative – 10 x increased incidence 2. No specific gene link
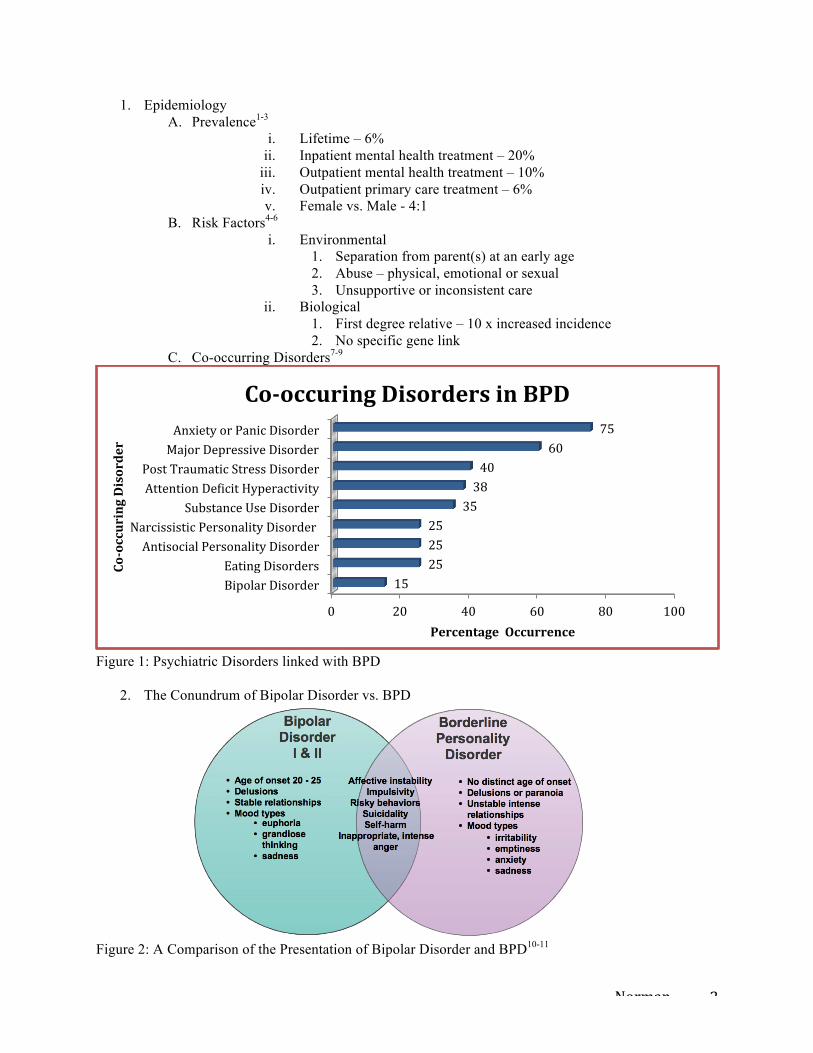
C. Co-occurring Disorders7-9
Figure 1: Psychiatric Disorders linked with BPD
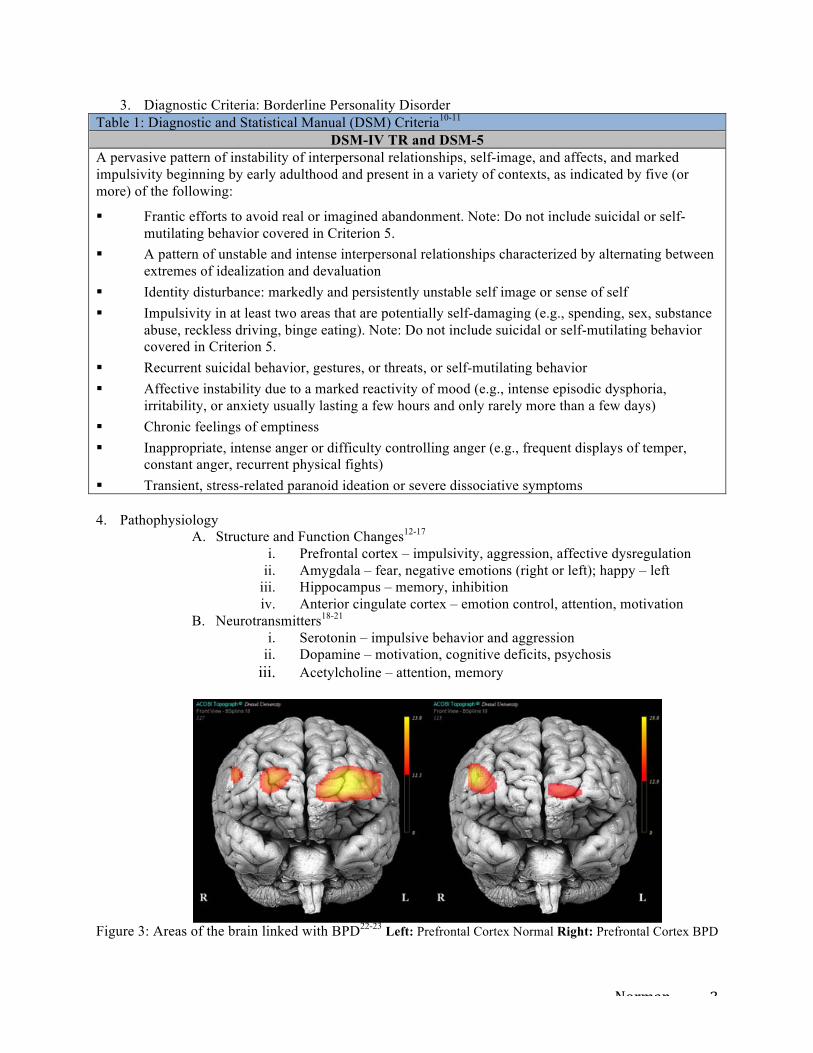
2. The Conundrum of Bipolar Disorder vs. BPD
Figure 2: A Comparison of the Presentation of Bipolar Disorder and BPD10-11
0 20 40 60 80 100
Bipolar Disorder Eating Disorders
Antisocial Personality Disorder Narcissistic Personality Disorder
Substance Use Disorder Attention DeAicit Hyperactivity Post Traumatic Stress Disorder
Major Depressive Disorder Anxiety or Panic Disorder
15 25 25 25
35 38 40
60 75
Percentage Occurrence
Co-‐occuring Disorder
Co-‐occuring Disorders in BPD
Norman 3
3. Diagnostic Criteria: Borderline Personality Disorder Table 1: Diagnostic and Statistical Manual (DSM) Criteria10-11
DSM-IV TR and DSM-5 A pervasive pattern of instability of interpersonal relationships, self-image, and affects, and marked impulsivity beginning by early adulthood and present in a variety of contexts, as indicated by five (or more) of the following: § Frantic efforts to avoid real or imagined abandonment. Note: Do not include suicidal or self-
mutilating behavior covered in Criterion 5. § A pattern of unstable and intense interpersonal relationships characterized by alternating between
extremes of idealization and devaluation § Identity disturbance: markedly and persistently unstable self image or sense of self § Impulsivity in at least two areas that are potentially self-damaging (e.g., spending, sex, substance
abuse, reckless driving, binge eating). Note: Do not include suicidal or self-mutilating behavior covered in Criterion 5.
§ Recurrent suicidal behavior, gestures, or threats, or self-mutilating behavior § Affective instability due to a marked reactivity of mood (e.g., intense episodic dysphoria,
irritability, or anxiety usually lasting a few hours and only rarely more than a few days) § Chronic feelings of emptiness § Inappropriate, intense anger or difficulty controlling anger (e.g., frequent displays of temper,
constant anger, recurrent physical fights) § Transient, stress-related paranoid ideation or severe dissociative symptoms 4. Pathophysiology
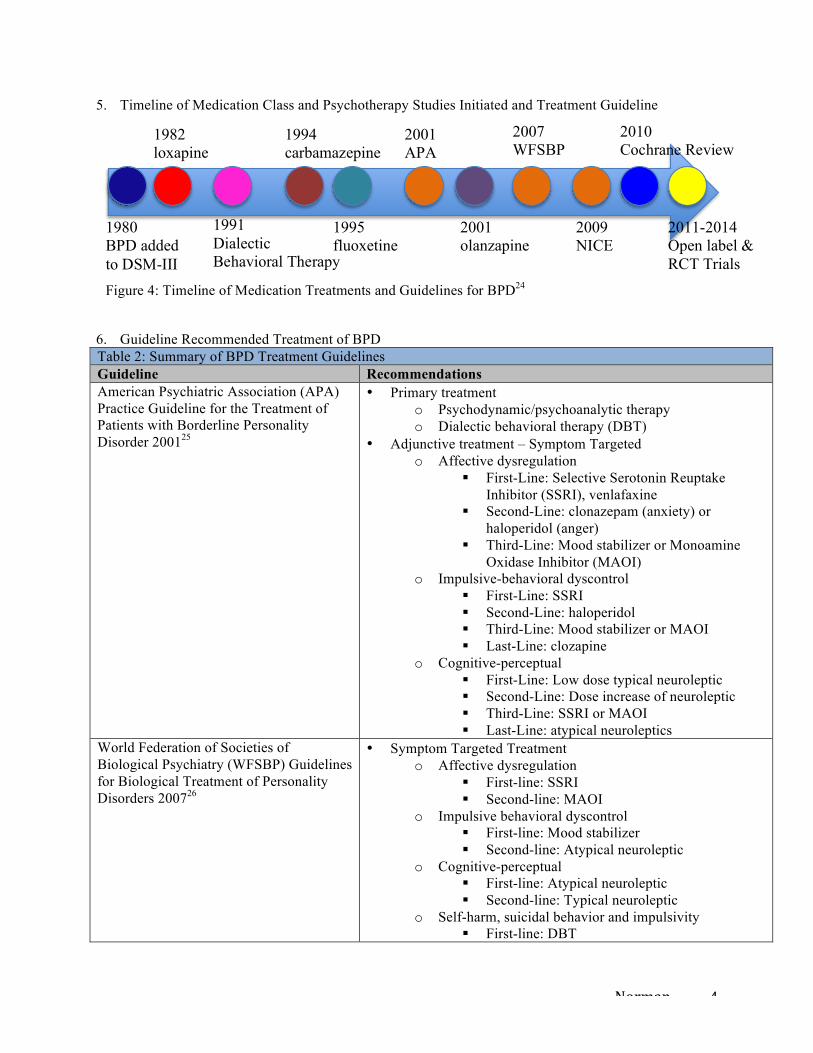
A. Structure and Function Changes12-17 i. Prefrontal cortex – impulsivity, aggression, affective dysregulation
ii. Amygdala – fear, negative emotions (right or left); happy – left iii. Hippocampus – memory, inhibition iv. Anterior cingulate cortex – emotion control, attention, motivation
B. Neurotransmitters18-21 i. Serotonin – impulsive behavior and aggression
ii. Dopamine – motivation, cognitive deficits, psychosis iii. Acetylcholine – attention, memory
Figure 3: Areas of the brain linked with BPD22-23 Left: Prefrontal Cortex Normal Right: Prefrontal Cortex BPD
Norman 4
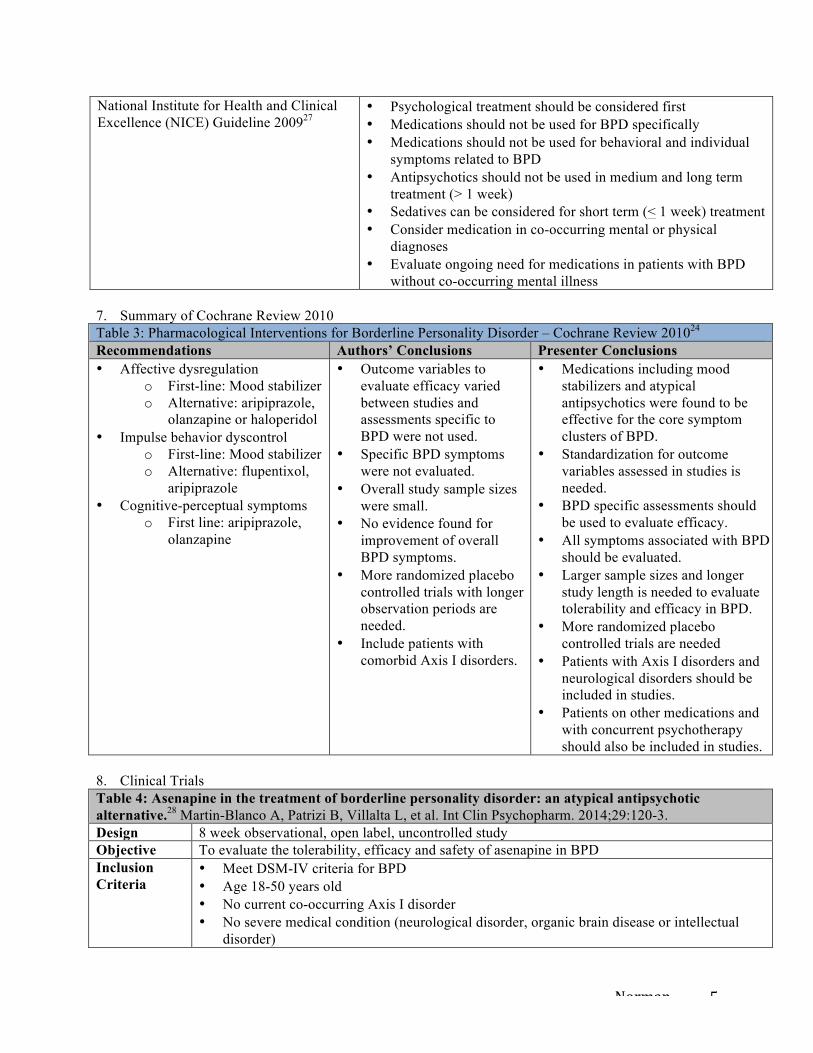
5. Timeline of Medication Class and Psychotherapy Studies Initiated and Treatment Guideline
6. Guideline Recommended Treatment of BPD Table 2: Summary of BPD Treatment Guidelines
Guideline Recommendations American Psychiatric Association (APA) Practice Guideline for the Treatment of Patients with Borderline Personality Disorder 200125
• Primary treatment o Psychodynamic/psychoanalytic therapy o Dialectic behavioral therapy (DBT)
• Adjunctive treatment – Symptom Targeted o Affective dysregulation
§ First-Line: Selective Serotonin Reuptake Inhibitor (SSRI), venlafaxine
§ Second-Line: clonazepam (anxiety) or haloperidol (anger)
§ Third-Line: Mood stabilizer or Monoamine Oxidase Inhibitor (MAOI)
o Impulsive-behavioral dyscontrol § First-Line: SSRI § Second-Line: haloperidol § Third-Line: Mood stabilizer or MAOI § Last-Line: clozapine
o Cognitive-perceptual § First-Line: Low dose typical neuroleptic § Second-Line: Dose increase of neuroleptic § Third-Line: SSRI or MAOI § Last-Line: atypical neuroleptics
World Federation of Societies of Biological Psychiatry (WFSBP) Guidelines for Biological Treatment of Personality Disorders 200726
• Symptom Targeted Treatment o Affective dysregulation
§ First-line: SSRI § Second-line: MAOI
o Impulsive behavioral dyscontrol § First-line: Mood stabilizer § Second-line: Atypical neuroleptic
o Cognitive-perceptual § First-line: Atypical neuroleptic § Second-line: Typical neuroleptic
o Self-harm, suicidal behavior and impulsivity § First-line: DBT
1980 BPD added to DSM-III
2001 APA
2007 WFSBP
2009 NICE
2010 Cochrane Review
2011-2014 Open label & RCT Trials
1982 loxapine
1994 carbamazepine
1995 fluoxetine
2001 olanzapine
1991 Dialectic Behavioral Therapy
Figure 4: Timeline of Medication Treatments and Guidelines for BPD24
Norman 5
National Institute for Health and Clinical Excellence (NICE) Guideline 200927
• Psychological treatment should be considered first • Medications should not be used for BPD specifically • Medications should not be used for behavioral and individual
symptoms related to BPD • Antipsychotics should not be used in medium and long term
treatment (> 1 week) • Sedatives can be considered for short term (< 1 week) treatment • Consider medication in co-occurring mental or physical
diagnoses • Evaluate ongoing need for medications in patients with BPD
without co-occurring mental illness 7. Summary of Cochrane Review 2010 Table 3: Pharmacological Interventions for Borderline Personality Disorder – Cochrane Review 201024 Recommendations Authors’ Conclusions Presenter Conclusions • Affective dysregulation
o First-line: Mood stabilizer o Alternative: aripiprazole,
olanzapine or haloperidol • Impulse behavior dyscontrol
o First-line: Mood stabilizer o Alternative: flupentixol,
aripiprazole • Cognitive-perceptual symptoms
o First line: aripiprazole, olanzapine
• Outcome variables to evaluate efficacy varied between studies and assessments specific to BPD were not used.
• Specific BPD symptoms were not evaluated.
• Overall study sample sizes were small.
• No evidence found for improvement of overall BPD symptoms.
• More randomized placebo controlled trials with longer observation periods are needed.
• Include patients with comorbid Axis I disorders.
• Medications including mood stabilizers and atypical antipsychotics were found to be effective for the core symptom clusters of BPD.
• Standardization for outcome variables assessed in studies is needed.
• BPD specific assessments should be used to evaluate efficacy.
• All symptoms associated with BPD should be evaluated.
• Larger sample sizes and longer study length is needed to evaluate tolerability and efficacy in BPD.
• More randomized placebo controlled trials are needed
• Patients with Axis I disorders and neurological disorders should be included in studies.
• Patients on other medications and with concurrent psychotherapy should also be included in studies.
8. Clinical Trials Table 4: Asenapine in the treatment of borderline personality disorder: an atypical antipsychotic alternative.28 Martin-Blanco A, Patrizi B, Villalta L, et al. Int Clin Psychopharm. 2014;29:120-3. Design 8 week observational, open label, uncontrolled study Objective To evaluate the tolerability, efficacy and safety of asenapine in BPD Inclusion Criteria
• Meet DSM-IV criteria for BPD • Age 18-50 years old • No current co-occurring Axis I disorder • No severe medical condition (neurological disorder, organic brain disease or intellectual
disorder)
Norman 6
• CGI-BPD score of > 4 • Current use of adequate birth control if female
Exclusion Criteria
None listed
Intervention asenapine 5-20 mg/d using variable dosing for 8 weeks Assessment • Symptoms at baseline and every 2 weeks using both patient rated and clinician rated scales.
• Safety assessed for emerging side effects and EPS using the modified Udvalg for Kliniske Undersogelser (UKU) Side Effect Rating Scale.
Endpoints • Primary endpoint: CGI-BPD and BSL-23 score change from baseline to study end • Secondary endpoints: HAM-D and BPRS score change from baseline to study end • Safety: UKU at 2 week assessment visits
Statistical Analysis
• Baseline and demographics data o ANOVA for quantitative measures o Chi-square for qualitative measures
• Safety and efficacy data o ANOVA for repeated measures o Last observation carried forward (LOCF) for endpoint
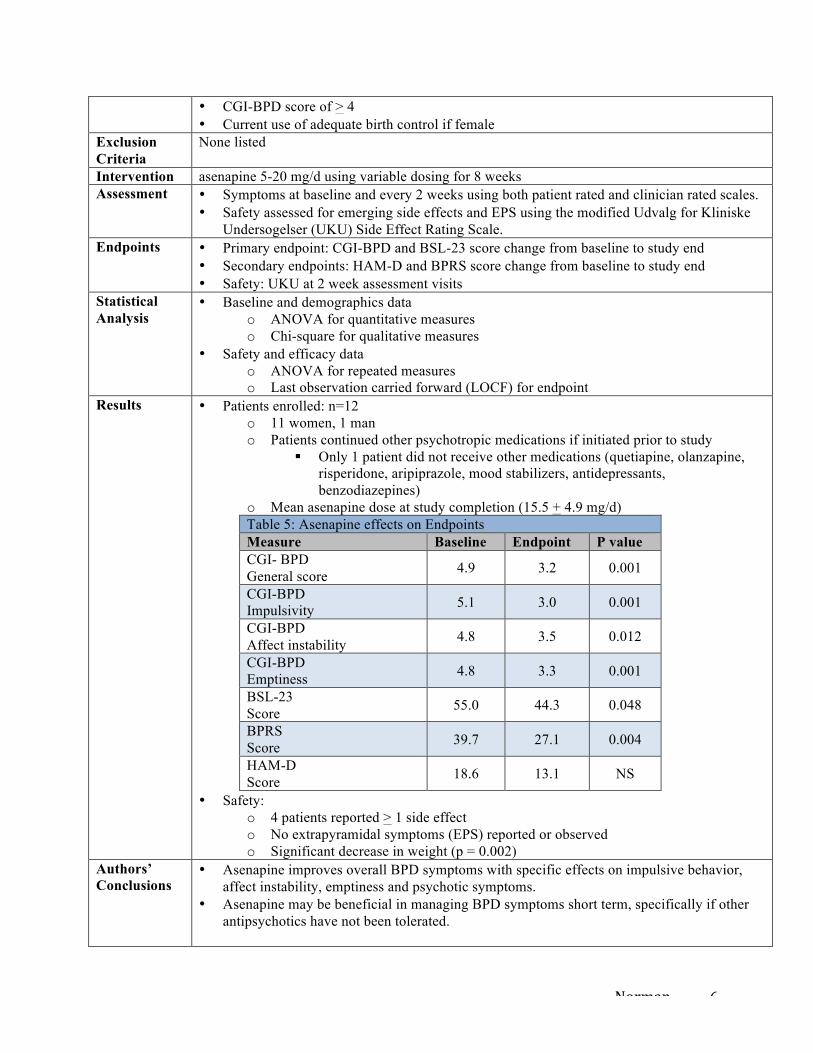
Results • Patients enrolled: n=12 o 11 women, 1 man o Patients continued other psychotropic medications if initiated prior to study
§ Only 1 patient did not receive other medications (quetiapine, olanzapine, risperidone, aripiprazole, mood stabilizers, antidepressants, benzodiazepines)
o Mean asenapine dose at study completion (15.5 + 4.9 mg/d) Table 5: Asenapine effects on Endpoints Measure Baseline Endpoint P value CGI- BPD General score 4.9 3.2 0.001
CGI-BPD Impulsivity 5.1 3.0 0.001
CGI-BPD Affect instability 4.8 3.5 0.012
CGI-BPD Emptiness 4.8 3.3 0.001
BSL-23 Score 55.0 44.3 0.048
BPRS Score 39.7 27.1 0.004
HAM-D Score 18.6 13.1 NS
• Safety: o 4 patients reported > 1 side effect o No extrapyramidal symptoms (EPS) reported or observed o Significant decrease in weight (p = 0.002)
Authors’ Conclusions
• Asenapine improves overall BPD symptoms with specific effects on impulsive behavior, affect instability, emptiness and psychotic symptoms.
• Asenapine may be beneficial in managing BPD symptoms short term, specifically if other antipsychotics have not been tolerated.
Norman 7
Presenter Comments and Conclusions
• Strengths: o Use of validated rating scales o No co-occurring psychiatric disorders were allowed o No conflicts of interest o Used BPD specific assessments
• Weaknesses: o Open label study design, small sample size, short duration of study o LOCF limits evaluation of treatment effect o Concurrent medications, doses, adjustments and duration used by each patient in
addition to asenapine during the study unknown o Initial and final dose reported as range and mean o Unknown if patients received concurrent or previous psychotherapy o Results not generalizable to current practice o No report on use or exclusion of alcohol or other substances
• Conclusions: o Asenapine doses of 10-20 mg/d appear effective in reducing overall symptoms of
BPD with noticeable improvements specifically in impulsivity, affect instability, feelings of emptiness and psychosis when used short term.
o The potential effects of concurrent medications on observed symptom improvement cannot be ignored.
o No serious side effects were observed during the study. o More research with large sample size randomized, double blind, placebo-controlled
trials with long-term evaluation is needed. Table 6: Paliperidone ER in the treatment of borderline personality disorder: a pilot study of efficacy and tolerability.29 Bellino S, Bozzatello P, Rinaldi C, et al. Depress Res Treat. 2011;doi:10.1155/2011/680194 Design 12 week open label, observational, uncontrolled study Objective To evaluate the tolerability and efficacy of paliperidone ER in patients with BPD Inclusion Criteria
• Meet DSM-IV criteria for BPD • Age 18-60 years old
Exclusion Criteria
• Diagnosis of delirium, dementia, other cognitive disorder, schizophrenia, other psychotic disorder, bipolar disorders, co-occurring major depressive disorder, substance abuse in previous 6 months
• Presence of hyperprolactinemia • Use of psychotropic medications or psychotherapy in previous 3 months • Females of childbearing age not using adequate contraception
Intervention paliperidone ER 3-6 mg/d for 12 weeks Assessment • Symptoms at baseline, 4 and 12 weeks using both patient rated and clinician rated scales.
• Safety assessed using serum prolactin level at baseline, 4 and 12 weeks, weight at baseline and 12 weeks, and emerging side effects using the Dosage Record and Treatment Emergent Symptoms Scale (DOTES), prolactin level and weight.
Endpoints Primary endpoints: CGI-S, BPRS, HAM-A, HAM-D, SOFAS, BIS-11, BPDSI mean score change from baseline to 4 weeks to study end
Statistical Analysis
ANOVA for repeated measures with Bonferroni correction to calculate changes in rating scale scores
Results • Patients enrolled: n=18 o 13 women and 5 men o Mean daily paliperidone dose (4.8 + 1.5 mg/d)
Norman 8
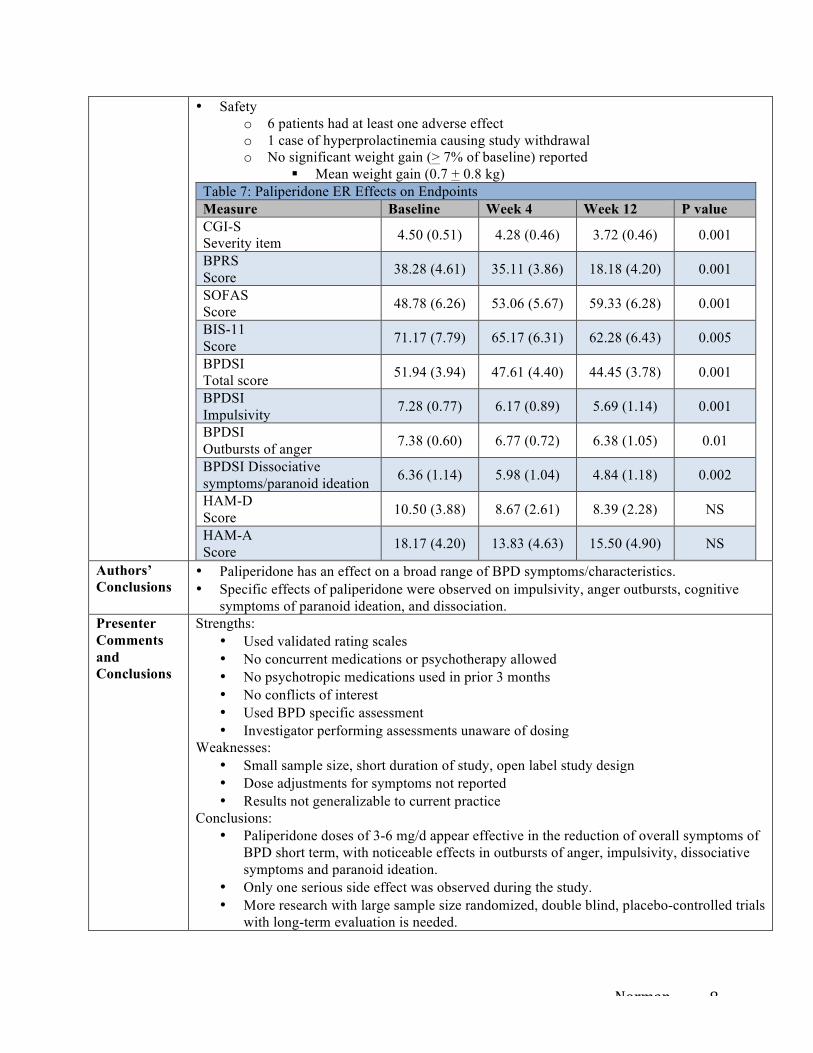
• Safety o 6 patients had at least one adverse effect o 1 case of hyperprolactinemia causing study withdrawal o No significant weight gain (> 7% of baseline) reported
§ Mean weight gain (0.7 + 0.8 kg) Table 7: Paliperidone ER Effects on Endpoints Measure Baseline Week 4 Week 12 P value CGI-S Severity item 4.50 (0.51) 4.28 (0.46) 3.72 (0.46) 0.001
BPRS Score 38.28 (4.61) 35.11 (3.86) 18.18 (4.20) 0.001
SOFAS Score 48.78 (6.26) 53.06 (5.67) 59.33 (6.28) 0.001
BIS-11 Score 71.17 (7.79) 65.17 (6.31) 62.28 (6.43) 0.005
BPDSI Total score 51.94 (3.94) 47.61 (4.40) 44.45 (3.78) 0.001
BPDSI Impulsivity 7.28 (0.77) 6.17 (0.89) 5.69 (1.14) 0.001
BPDSI Outbursts of anger 7.38 (0.60) 6.77 (0.72) 6.38 (1.05) 0.01
BPDSI Dissociative symptoms/paranoid ideation 6.36 (1.14) 5.98 (1.04) 4.84 (1.18) 0.002
HAM-D Score 10.50 (3.88) 8.67 (2.61) 8.39 (2.28) NS
HAM-A Score 18.17 (4.20) 13.83 (4.63) 15.50 (4.90) NS
Authors’ Conclusions
• Paliperidone has an effect on a broad range of BPD symptoms/characteristics. • Specific effects of paliperidone were observed on impulsivity, anger outbursts, cognitive
symptoms of paranoid ideation, and dissociation. Presenter Comments and Conclusions
Strengths: • Used validated rating scales • No concurrent medications or psychotherapy allowed • No psychotropic medications used in prior 3 months • No conflicts of interest • Used BPD specific assessment • Investigator performing assessments unaware of dosing
Weaknesses: • Small sample size, short duration of study, open label study design • Dose adjustments for symptoms not reported • Results not generalizable to current practice
Conclusions: • Paliperidone doses of 3-6 mg/d appear effective in the reduction of overall symptoms of
BPD short term, with noticeable effects in outbursts of anger, impulsivity, dissociative symptoms and paranoid ideation.
• Only one serious side effect was observed during the study. • More research with large sample size randomized, double blind, placebo-controlled trials
with long-term evaluation is needed.
Norman 9
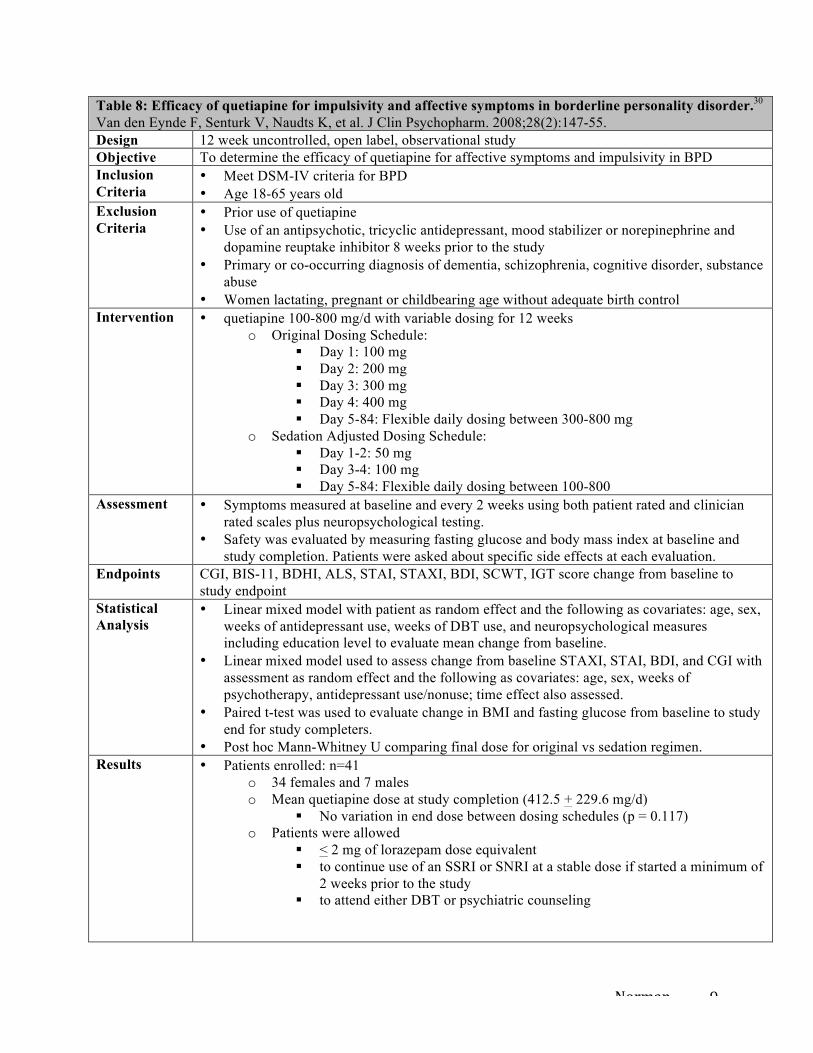
Table 8: Efficacy of quetiapine for impulsivity and affective symptoms in borderline personality disorder.30 Van den Eynde F, Senturk V, Naudts K, et al. J Clin Psychopharm. 2008;28(2):147-55. Design 12 week uncontrolled, open label, observational study Objective To determine the efficacy of quetiapine for affective symptoms and impulsivity in BPD Inclusion Criteria
• Meet DSM-IV criteria for BPD • Age 18-65 years old
Exclusion Criteria
• Prior use of quetiapine • Use of an antipsychotic, tricyclic antidepressant, mood stabilizer or norepinephrine and
dopamine reuptake inhibitor 8 weeks prior to the study • Primary or co-occurring diagnosis of dementia, schizophrenia, cognitive disorder, substance
abuse • Women lactating, pregnant or childbearing age without adequate birth control
Intervention • quetiapine 100-800 mg/d with variable dosing for 12 weeks o Original Dosing Schedule:
§ Day 1: 100 mg § Day 2: 200 mg § Day 3: 300 mg § Day 4: 400 mg § Day 5-84: Flexible daily dosing between 300-800 mg
o Sedation Adjusted Dosing Schedule: § Day 1-2: 50 mg § Day 3-4: 100 mg § Day 5-84: Flexible daily dosing between 100-800
Assessment • Symptoms measured at baseline and every 2 weeks using both patient rated and clinician rated scales plus neuropsychological testing.
• Safety was evaluated by measuring fasting glucose and body mass index at baseline and study completion. Patients were asked about specific side effects at each evaluation.
Endpoints CGI, BIS-11, BDHI, ALS, STAI, STAXI, BDI, SCWT, IGT score change from baseline to study endpoint
Statistical Analysis
• Linear mixed model with patient as random effect and the following as covariates: age, sex, weeks of antidepressant use, weeks of DBT use, and neuropsychological measures including education level to evaluate mean change from baseline.
• Linear mixed model used to assess change from baseline STAXI, STAI, BDI, and CGI with assessment as random effect and the following as covariates: age, sex, weeks of psychotherapy, antidepressant use/nonuse; time effect also assessed.
• Paired t-test was used to evaluate change in BMI and fasting glucose from baseline to study end for study completers.
• Post hoc Mann-Whitney U comparing final dose for original vs sedation regimen. Results • Patients enrolled: n=41
o 34 females and 7 males o Mean quetiapine dose at study completion (412.5 + 229.6 mg/d)
§ No variation in end dose between dosing schedules (p = 0.117) o Patients were allowed
§ < 2 mg of lorazepam dose equivalent § to continue use of an SSRI or SNRI at a stable dose if started a minimum of
2 weeks prior to the study § to attend either DBT or psychiatric counseling
Norman 10
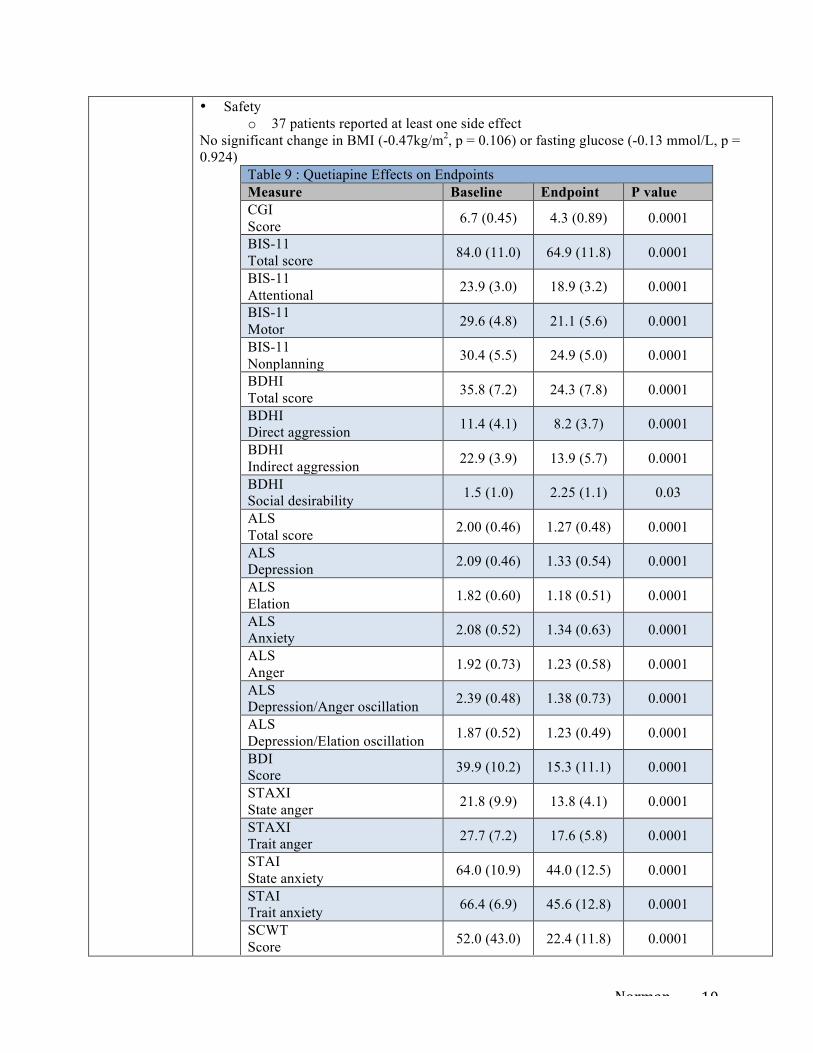
• Safety o 37 patients reported at least one side effect
No significant change in BMI (-0.47kg/m2, p = 0.106) or fasting glucose (-0.13 mmol/L, p = 0.924)
Table 9 : Quetiapine Effects on Endpoints Measure Baseline Endpoint P value CGI Score 6.7 (0.45) 4.3 (0.89) 0.0001
BIS-11 Total score 84.0 (11.0) 64.9 (11.8) 0.0001
BIS-11 Attentional 23.9 (3.0) 18.9 (3.2) 0.0001
BIS-11 Motor 29.6 (4.8) 21.1 (5.6) 0.0001
BIS-11 Nonplanning 30.4 (5.5) 24.9 (5.0) 0.0001
BDHI Total score 35.8 (7.2) 24.3 (7.8) 0.0001
BDHI Direct aggression 11.4 (4.1) 8.2 (3.7) 0.0001
BDHI Indirect aggression 22.9 (3.9) 13.9 (5.7) 0.0001
BDHI Social desirability 1.5 (1.0) 2.25 (1.1) 0.03
ALS Total score 2.00 (0.46) 1.27 (0.48) 0.0001
ALS Depression 2.09 (0.46) 1.33 (0.54) 0.0001
ALS Elation 1.82 (0.60) 1.18 (0.51) 0.0001
ALS Anxiety 2.08 (0.52) 1.34 (0.63) 0.0001
ALS Anger 1.92 (0.73) 1.23 (0.58) 0.0001
ALS Depression/Anger oscillation 2.39 (0.48) 1.38 (0.73) 0.0001
ALS Depression/Elation oscillation 1.87 (0.52) 1.23 (0.49) 0.0001
BDI Score 39.9 (10.2) 15.3 (11.1) 0.0001
STAXI State anger 21.8 (9.9) 13.8 (4.1) 0.0001
STAXI Trait anger 27.7 (7.2) 17.6 (5.8) 0.0001
STAI State anxiety 64.0 (10.9) 44.0 (12.5) 0.0001
STAI Trait anxiety 66.4 (6.9) 45.6 (12.8) 0.0001
SCWT Score 52.0 (43.0) 22.4 (11.8) 0.0001
Norman 11
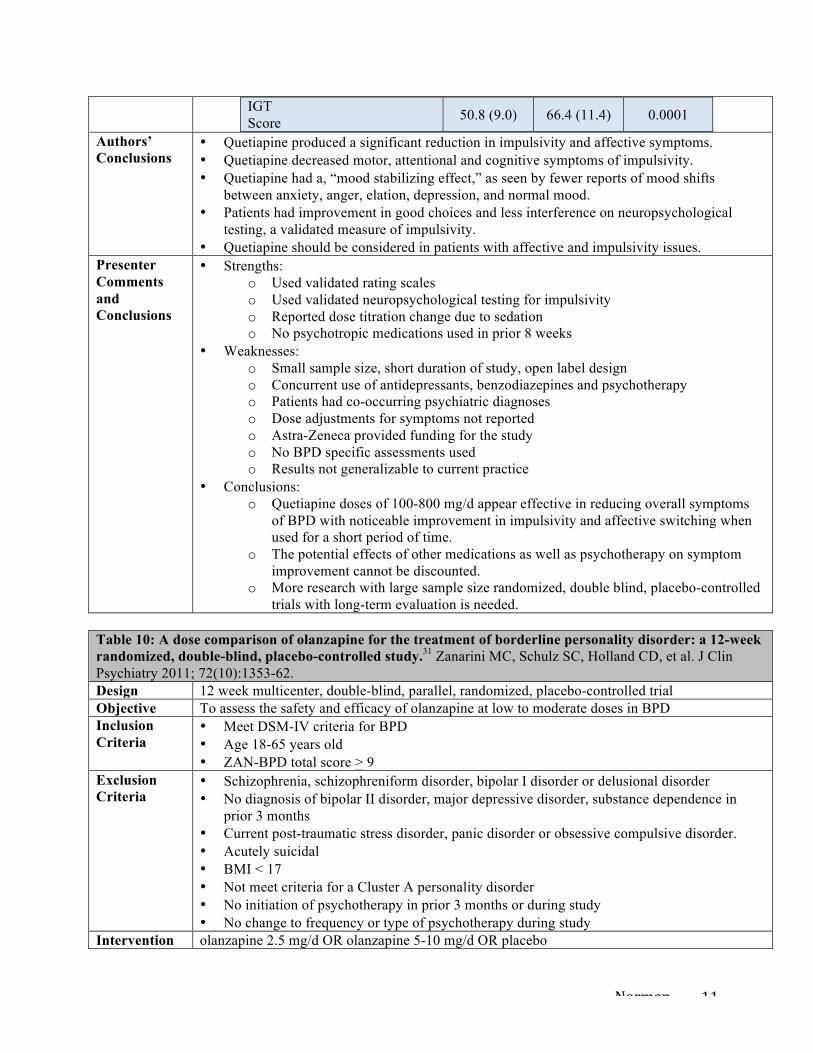
IGT Score 50.8 (9.0) 66.4 (11.4) 0.0001
Authors’ Conclusions
• Quetiapine produced a significant reduction in impulsivity and affective symptoms. • Quetiapine decreased motor, attentional and cognitive symptoms of impulsivity. • Quetiapine had a, “mood stabilizing effect,” as seen by fewer reports of mood shifts
between anxiety, anger, elation, depression, and normal mood. • Patients had improvement in good choices and less interference on neuropsychological
testing, a validated measure of impulsivity. • Quetiapine should be considered in patients with affective and impulsivity issues.
Presenter Comments and Conclusions
• Strengths: o Used validated rating scales o Used validated neuropsychological testing for impulsivity o Reported dose titration change due to sedation o No psychotropic medications used in prior 8 weeks
• Weaknesses: o Small sample size, short duration of study, open label design o Concurrent use of antidepressants, benzodiazepines and psychotherapy o Patients had co-occurring psychiatric diagnoses o Dose adjustments for symptoms not reported o Astra-Zeneca provided funding for the study o No BPD specific assessments used o Results not generalizable to current practice
• Conclusions: o Quetiapine doses of 100-800 mg/d appear effective in reducing overall symptoms
of BPD with noticeable improvement in impulsivity and affective switching when used for a short period of time.
o The potential effects of other medications as well as psychotherapy on symptom improvement cannot be discounted.
o More research with large sample size randomized, double blind, placebo-controlled trials with long-term evaluation is needed.
Table 10: A dose comparison of olanzapine for the treatment of borderline personality disorder: a 12-week randomized, double-blind, placebo-controlled study.31 Zanarini MC, Schulz SC, Holland CD, et al. J Clin Psychiatry 2011; 72(10):1353-62. Design 12 week multicenter, double-blind, parallel, randomized, placebo-controlled trial Objective To assess the safety and efficacy of olanzapine at low to moderate doses in BPD Inclusion Criteria
• Meet DSM-IV criteria for BPD • Age 18-65 years old • ZAN-BPD total score > 9
Exclusion Criteria
• Schizophrenia, schizophreniform disorder, bipolar I disorder or delusional disorder • No diagnosis of bipolar II disorder, major depressive disorder, substance dependence in
prior 3 months • Current post-traumatic stress disorder, panic disorder or obsessive compulsive disorder. • Acutely suicidal • BMI < 17 • Not meet criteria for a Cluster A personality disorder • No initiation of psychotherapy in prior 3 months or during study • No change to frequency or type of psychotherapy during study
Intervention olanzapine 2.5 mg/d OR olanzapine 5-10 mg/d OR placebo
Norman 12
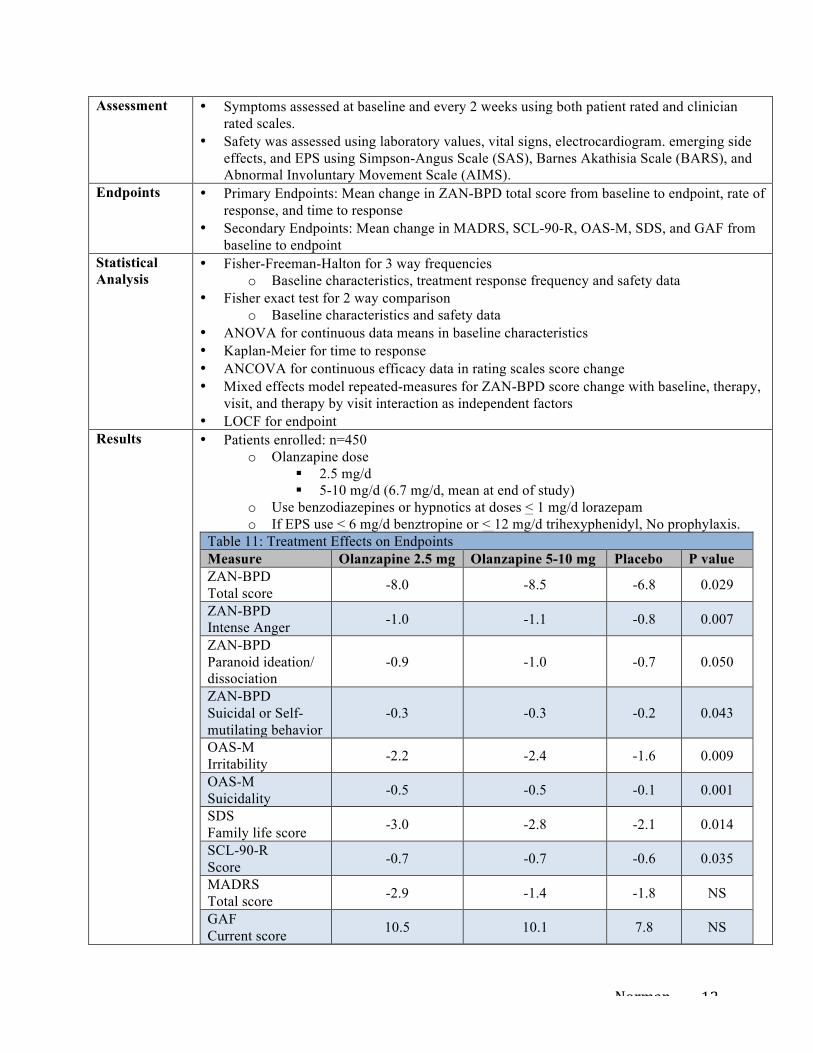
Assessment • Symptoms assessed at baseline and every 2 weeks using both patient rated and clinician rated scales.
• Safety was assessed using laboratory values, vital signs, electrocardiogram. emerging side effects, and EPS using Simpson-Angus Scale (SAS), Barnes Akathisia Scale (BARS), and Abnormal Involuntary Movement Scale (AIMS).
Endpoints • Primary Endpoints: Mean change in ZAN-BPD total score from baseline to endpoint, rate of response, and time to response
• Secondary Endpoints: Mean change in MADRS, SCL-90-R, OAS-M, SDS, and GAF from baseline to endpoint
Statistical Analysis
• Fisher-Freeman-Halton for 3 way frequencies o Baseline characteristics, treatment response frequency and safety data
• Fisher exact test for 2 way comparison o Baseline characteristics and safety data
• ANOVA for continuous data means in baseline characteristics • Kaplan-Meier for time to response • ANCOVA for continuous efficacy data in rating scales score change • Mixed effects model repeated-measures for ZAN-BPD score change with baseline, therapy,
visit, and therapy by visit interaction as independent factors • LOCF for endpoint
Results • Patients enrolled: n=450 o Olanzapine dose
§ 2.5 mg/d § 5-10 mg/d (6.7 mg/d, mean at end of study)
o Use benzodiazepines or hypnotics at doses < 1 mg/d lorazepam o If EPS use < 6 mg/d benztropine or < 12 mg/d trihexyphenidyl, No prophylaxis.
Table 11: Treatment Effects on Endpoints Measure Olanzapine 2.5 mg Olanzapine 5-10 mg Placebo P value ZAN-BPD Total score -8.0 -8.5 -6.8 0.029
ZAN-BPD Intense Anger -1.0 -1.1 -0.8 0.007
ZAN-BPD Paranoid ideation/ dissociation
-0.9 -1.0 -0.7 0.050
ZAN-BPD Suicidal or Self-mutilating behavior
-0.3 -0.3 -0.2 0.043
OAS-M Irritability -2.2 -2.4 -1.6 0.009
OAS-M Suicidality -0.5 -0.5 -0.1 0.001
SDS Family life score -3.0 -2.8 -2.1 0.014
SCL-90-R Score -0.7 -0.7 -0.6 0.035
MADRS Total score -2.9 -1.4 -1.8 NS
GAF Current score 10.5 10.1 7.8 NS
Norman 13
• ZAN-BPD o Rate of response significantly greater
§ 5-10 mg: 73.6% > 2.5 mg: 60.1% (p = 0.018) > placebo: 57.8% (p=0.006) o Time to first response significantly shorter
§ 5-10 mg < placebo (p = 0.028) • Safety
o Patients reporting > 1 side effect § 2.5 mg: 98 vs 5-10 mg: 99
o Mean change in weight was significant § 2.5 mg: 2.09 + 2.93 kg vs placebo: 0.02 + 2.47 kg (p < 0.001) § 5-10 mg: 3.17 + 3.28 kg vs placebo: 0.02 + 2.47 kg (p < 0.001)
o Significant increase in fasting triglycerides § 2.5 mg: 0.20 + 0.79 mmol/L vs placebo: -0.06 + 0.66 (p = 0.018) § 5-10 mg: 0.21 + 0.80 mmol/L vs placebo: -0.06 + 0.66 (p = 0.014) § No significant difference in fasting glucose, fasting lipids, ECG or EPS
Authors’ Conclusions
• Moderate (5-10 mg/d) dose olanzapine was better than placebo at reducing overall symptoms in BPD as well as improving school and work functioning.
• Both low (2.5 mg/d) and moderate dose olanzapine lessened irritability and suicidality symptoms in BPD and improved family function.
• Adverse effects were not different than those seen in previous studies evaluating olanzapine use in various patient populations.
Presenter Comments and Conclusions
• Strengths: o Used validated rating scales o Randomized, placebo-controlled, double blinded with large sample size o Used BPD specific assessment
• Weaknesses: o Strict exclusion criteria o Concurrent psychotherapy o Dose adjustments for symptom management not stated o Results not generalizable to current practice o Eli Lilly funded the study and multiple researchers were affiliated with Eli Lilly o Medication use prior to the study was not reported
• Conclusions: o Olanzapine 5-10 mg/d appears effective in reducing overall symptoms of BPD in
short-term use. o Olanzapine 2.5-10 mg/d appears effective in reducing specific symptoms of
irritability, intense anger, and paranoid ideation/dissociation when used short term. o The potential effects of concurrent psychotherapy, benzodiazepines and hypnotics
on symptom improvement cannot be discounted. o Patients may experience significant changes in weight and triglycerides with short-
term use of olanzapine.
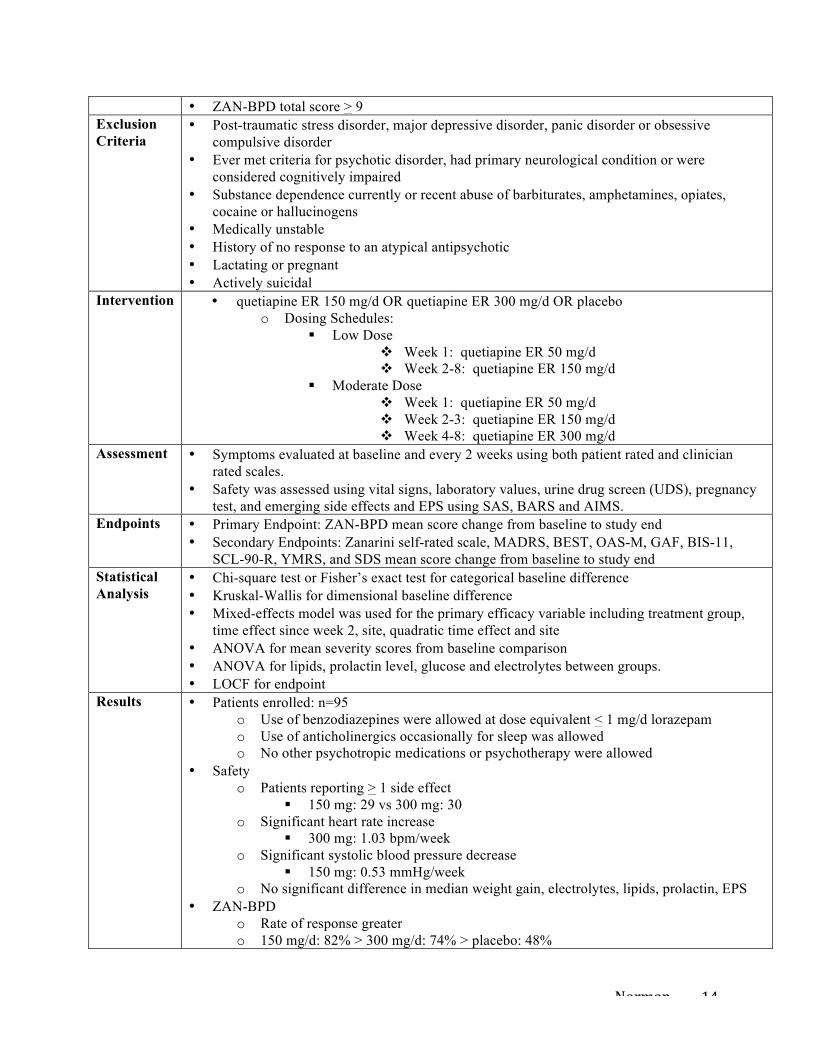
Table 12: Comparison of low and moderated dosages of extended-release quetiapine in borderline personality disorder: a randomized, double-blind, placebo-controlled trial.32
Black DW, Zanarini MC, Rominie A, et al. Am J Psychiatry 2014; AIA:1-9. Design 8 week multicenter, randomized, double-blind, placebo-controlled trial Objective To compare tolerability and efficacy of low and moderate doses of extended-release (ER)
quetiapine in BPD Inclusion Criteria
• Meet DSM-IV criteria for BPD • Age 18-45 years old
Norman 14
• ZAN-BPD total score > 9 Exclusion Criteria
• Post-traumatic stress disorder, major depressive disorder, panic disorder or obsessive compulsive disorder
• Ever met criteria for psychotic disorder, had primary neurological condition or were considered cognitively impaired
• Substance dependence currently or recent abuse of barbiturates, amphetamines, opiates, cocaine or hallucinogens
• Medically unstable • History of no response to an atypical antipsychotic • Lactating or pregnant • Actively suicidal
Intervention • quetiapine ER 150 mg/d OR quetiapine ER 300 mg/d OR placebo o Dosing Schedules:
§ Low Dose v Week 1: quetiapine ER 50 mg/d v Week 2-8: quetiapine ER 150 mg/d
§ Moderate Dose v Week 1: quetiapine ER 50 mg/d v Week 2-3: quetiapine ER 150 mg/d v Week 4-8: quetiapine ER 300 mg/d
Assessment • Symptoms evaluated at baseline and every 2 weeks using both patient rated and clinician rated scales.
• Safety was assessed using vital signs, laboratory values, urine drug screen (UDS), pregnancy test, and emerging side effects and EPS using SAS, BARS and AIMS.
Endpoints • Primary Endpoint: ZAN-BPD mean score change from baseline to study end • Secondary Endpoints: Zanarini self-rated scale, MADRS, BEST, OAS-M, GAF, BIS-11,
SCL-90-R, YMRS, and SDS mean score change from baseline to study end Statistical Analysis
• Chi-square test or Fisher’s exact test for categorical baseline difference • Kruskal-Wallis for dimensional baseline difference • Mixed-effects model was used for the primary efficacy variable including treatment group,
time effect since week 2, site, quadratic time effect and site • ANOVA for mean severity scores from baseline comparison • ANOVA for lipids, prolactin level, glucose and electrolytes between groups. • LOCF for endpoint
Results • Patients enrolled: n=95 o Use of benzodiazepines were allowed at dose equivalent < 1 mg/d lorazepam o Use of anticholinergics occasionally for sleep was allowed o No other psychotropic medications or psychotherapy were allowed
• Safety o Patients reporting > 1 side effect
§ 150 mg: 29 vs 300 mg: 30 o Significant heart rate increase
§ 300 mg: 1.03 bpm/week o Significant systolic blood pressure decrease
§ 150 mg: 0.53 mmHg/week o No significant difference in median weight gain, electrolytes, lipids, prolactin, EPS
• ZAN-BPD o Rate of response greater o 150 mg/d: 82% > 300 mg/d: 74% > placebo: 48%
Norman 15
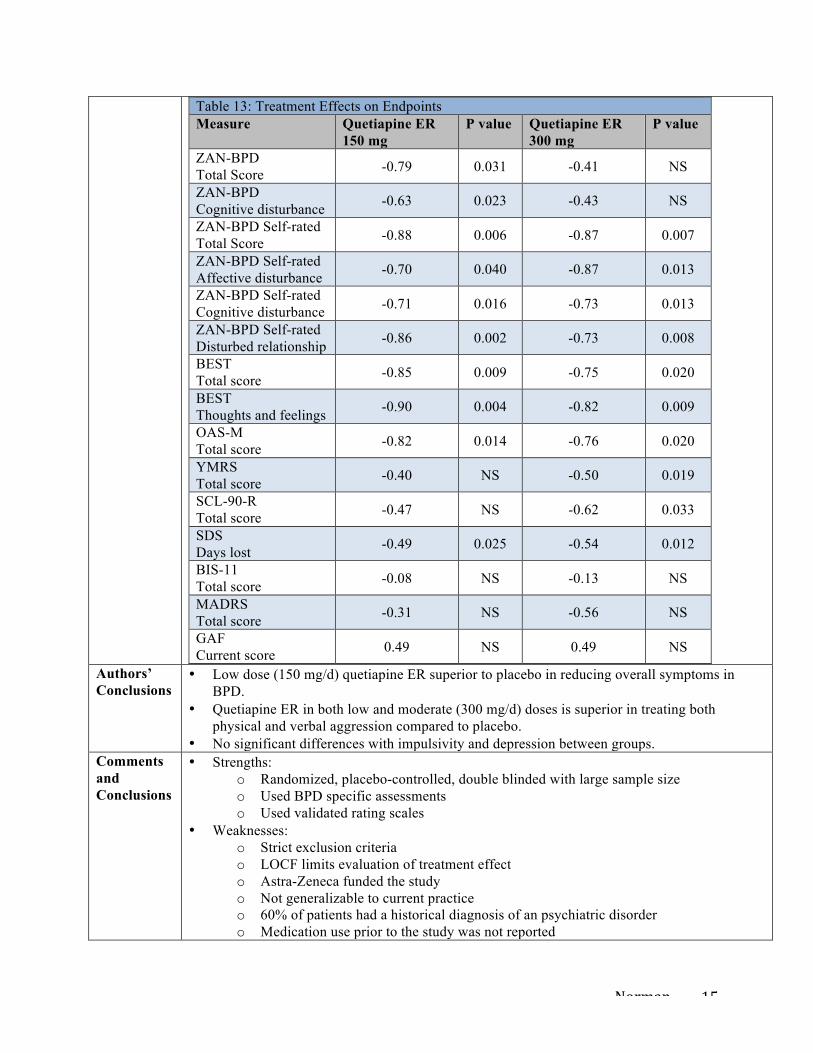
Table 13: Treatment Effects on Endpoints Measure Quetiapine ER
150 mg P value Quetiapine ER
300 mg P value
ZAN-BPD Total Score -0.79 0.031 -0.41 NS
ZAN-BPD Cognitive disturbance -0.63 0.023 -0.43 NS
ZAN-BPD Self-rated Total Score -0.88 0.006 -0.87 0.007
ZAN-BPD Self-rated Affective disturbance -0.70 0.040 -0.87 0.013
ZAN-BPD Self-rated Cognitive disturbance -0.71 0.016 -0.73 0.013
ZAN-BPD Self-rated Disturbed relationship -0.86 0.002 -0.73 0.008
BEST Total score -0.85 0.009 -0.75 0.020
BEST Thoughts and feelings -0.90 0.004 -0.82 0.009
OAS-M Total score -0.82 0.014 -0.76 0.020
YMRS Total score -0.40 NS -0.50 0.019
SCL-90-R Total score -0.47 NS -0.62 0.033
SDS Days lost -0.49 0.025 -0.54 0.012
BIS-11 Total score -0.08 NS -0.13 NS
MADRS Total score -0.31 NS -0.56 NS
GAF Current score 0.49 NS 0.49 NS
Authors’ Conclusions
• Low dose (150 mg/d) quetiapine ER superior to placebo in reducing overall symptoms in BPD.
• Quetiapine ER in both low and moderate (300 mg/d) doses is superior in treating both physical and verbal aggression compared to placebo.
• No significant differences with impulsivity and depression between groups. Comments and Conclusions
• Strengths: o Randomized, placebo-controlled, double blinded with large sample size o Used BPD specific assessments o Used validated rating scales
• Weaknesses: o Strict exclusion criteria o LOCF limits evaluation of treatment effect o Astra-Zeneca funded the study o Not generalizable to current practice o 60% of patients had a historical diagnosis of an psychiatric disorder o Medication use prior to the study was not reported
Norman 16
• Conclusions: o Quetiapine ER 150 mg/d appears to improve overall symptoms in BPD short term. o Quetiapine ER 150-300 mg/d appears to decrease affective and cognitive disturbance,
aggression, relationship problems and days lost from work as well as overall severity of symptoms when used for a short period of time.
o Quetiapine ER 300 mg/d appears to improve irritability, aggression and verbal outbursts.
9. Conclusions
A. There is some weak evidence for use of atypical antipsychotics in the short-term (8-12 weeks) management of BPD.
B. Atypical antipsychotics appear effective in reducing specific behavioral symptoms of BPD that lead to problems with personal relationships, legal trouble and most often hospitalization in short-term use.
C. The risk of side effects versus the benefit of symptom management is critical to determine whether atypical antipsychotics should be used in the short term for BPD.
D. More research using specific BPD symptom assessments along with standardized outcome measures is needed.
E. More research is needed in order to evaluate the benefits and risks associated with the long-term use of atypical antipsychotics in BPD.
10. References 1. Lenzenweger MF, Lane MC, Loranger AW, et al. DSM-IV personality disorders in the National
Comorbidity Survey Replication. Biol Psychiatry. 2007;62(6): 553–64. 2. Nasiri H, Abedi A, Ebrahimi A, et al. Personality profile of women affected with borderline personality
disorder. Mater Sociomed. 2013;25(1):60-3. 3. Gross R, Olfson M, Gameroff M, et al. Borderline personality disorder in primary care. Arch Intern Med.
2002;162:53-60. 4. Friedel RO. Borderline Personality Disorder Demystified. New York, Marlowe & Company, 2004, 45-61. 5. Kendler KS, Myers J, Reichborn-Kjennerud T. Borderline personality traits and their relationship with
dimensions of normative personality: a web-based cohort and twin study. Acta Psychiatrica Scandanavica. 2011;123:349-59.
6. Torgersen S, Myers J, Reichborn-Kjennerud T, et al. The heritability of cluster B personality disorders assessed both by personal interview and questionnaire. J Pers Disord. 2012;26(6):848-66.
7. National Alliance on Mental Illness [www.nami.org]. Arlington: NAMI; c1996-2014 [updated November 2012]. Borderline Personality Disorder; [about 2 screens]. Available at :http://www.nami.org/Template.cfm?Section=By_Illness&Template=/ContentManagement/ContentDisplay.cfm&ContentID=44780 Accessed 2014, Sept 10.
8. Ferrer M, Andion O, Matali J, et al. Comorbid attention-deficit/hyperactivity disorder in borderline patients defines an impulsive subtype of borderline personality disorder. J Pers Disord. 2012;24(6):812–22.
9. Grant BF, Chou SP, Goldstein RB, et al. Prevalence, correlates, disability, and comorbidity of DSM-IV borderline personality disorder: results from the Wave 2 National Epidemiologic Survey on Alcohol and Related Conditions. J Clin Psychiatry. 2008;69(4):533–45.
10. American Psychiatric Association. The Diagnostic and Statistical Manual of Mental Disorders: DSM 5 Text. Washington, DC, American Psychiatric Association, 2013.
11. American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision. Washington, DC, American Psychiatric Association, 2000.
12. Emotion-Regulating Circuit Weakened in Borderline Personality Disorder. Available at: www.nimh.nih.gov/science-news/2008/emotion-regulating-circuit-weakened-in-borderline-personality-disorder.shtml. Accessed 2014, Sept 10.
13. Kernberg OF, Michels MD. Borderline Personality Disorder. Am J Psychiatry. 2009;166:505-08.
Norman 17
14. Lis E, Greenfield B, Henry M, et al. Neuroimaging and genetics of borderline personality disorder: a review. J Psychiatry Neurosci. 2007;32(3):162–73.
15. Silbersweig D, Clarkin JF, Goldstein M, et al. Failure of frontolimbic inhibitory function in the context of negative emotion in borderline personality disorder. Am J Psychiatry. 2007;164(12):1832–41.
16. Koenigsberg HW, Siever LJ, Lee H, et al. Neural correlates of emotion processing in borderline personality disorder. Psychiatry Res. 2009;172(3):192–9.
17. Frankle WG, Lombardo I, New AS, et al. Brain serotonin transporter distribution in subjects with impulsive aggressivity: a positron emission study with [11C]McN 5652. Am J Psychiatry. 2005;162(5):915–23.
18. Schmahl C, Herpertz SC, Bertsch K, et al. Mechanisms of disturbed emotion processing and social interaction in borderline personality disorder: state of knowledge and research agenda of the German clinical research unit. Bord Personal Disord Emot Dysregul. 2014;1(12):1-17.
19. Friedel RO. Dopamine dysfunction in borderline personality disorder: a hypothesis. Neuropsychopharmacology. 2004;29(6):1029–39.
20. Gurvits IG, Koenigsberg HW, Siever LJ. Neurotransmitter dysfunction in patients with borderline personality disorder. Psychiatr Clin North Am. 2000;23(1):27–40.
21. Ruocco AC, Amirthavasagam S, Choi-Kain L, et al. Neural correlates of negative emotionality in borderline personality disorder: an activation likelihood-meta analysis. Biol Psychiatry. 2012;73(2);153-60.
22. Ruocco AC, Amirthavasagam S, Zakzanis KK. Amygdala and hippocampal volume reductions as candidate endophenotypes for borderline personality disorder: a meta-analysis of magnetic resonance imaging studies. Psychiatry Res. 2012;201:245-52.
23. Kleiner K. Understanding borderline personality disorder. University of Toronto News. 2013 Jan 17. Available at: http://www.news.utoronto.ca/understanding-borderline-personality-disorder. Accessed 2014, Sept 10.
24. Stoffers J, Vollm BA, Rucker G, et al. Pharmacological interventions for borderline personality disorder. Cochrane Database of Systematic Reviews 2010;Issue 6:Art. No.: CD005653.
25. American Psychiatric Association: Practice guideline for the treatment of patients with borderline personality disorder. Am J Psychiatry. 2001;158: (October supplement).
26. Herpertz SC, Zanarini M, Schulz CS, Siever L, Lieb K, Moller K, WFSBP Task Force on Personality Disorders. World Federation of Societies of Biological Psychiatry (WFSBP) guidelines for biological treatment of personality disorders. World J Biol Psychiatry. 2007;8(4):212-44.
27. NCCMH (2009) Borderline Personality Disorder: Treatment and Management. Leicester and London: The British Psychological Society and the Royal College of Psychiatrists.
28. Martin-Blanco A, Patrizi B, Villalta L, et al. Asenapine in the treatment of borderline personality disorder: an atypical antipsychotic alternative. Int Clin Psychopharm. 2014;29:120-3.
29. Bellino S, Bozzatello P, Rinaldi C, et al. Paliperidone ER in the treatment of borderline personality disorder: a pilot study of efficacy and tolerability. Depress Res Treat. 2011;Article ID 680194:doi:10.1155/2011/680194.
30. Van den Eynde F, Senturk V, Naudts K, et al. Efficacy of quetiapine for impulsivity and affective symptoms in borderline personality disorder. J Clin Psychopharm. 2008;28(2):147-55.
31. Zanarini MC, Schulz SC, Holland CD, et al. A dose comparison of olanzapine for the treatment of borderline personality disorder: a 12-week randomized, double-blind, placebo-controlled study. J Clin Psychiatry. 2011;72(10):1353-62.
32. Black DW, Zanarini MC, Rominie A, et al. Comparison of low and moderated dosages of extended-release quetiapine in borderline personality disorder: a randomized, double-blind, placebo-controlled trial. Am J Psychiatry. 2014; AIA:1-9.
33. Perez V, Barrachina J, Soler J, et al. Modification of the Clinical Global Impression (CGI) scale for use in borderline personality disorder patients (CGI-BPD). Actas Esp Psiquiatr. 2007;35:229-35.
34. Busner J, Targum SD. The Clinical Global Impressions Scale. Psychiatry. 2007;4(7):28-37. 35. Bohus M, Kleindienst, Limberger MF, et al. The short version of the Borderline Symptom List (BSL-23):
development and initial data on psychometric properties. Psychopathology. 2009;42(1):32-9.
Norman 18
36. Ventura J, Green M, Shaner A, et al. Training and quality assurance with the Brief Psychiatry Rating Scale. “the drift busters”, Int J Psychiatr Res. 1993;3:221.
37. Hamilton M. A rating scale for depression. J Neuro Neurosurg Psychiatry. 1960;23:56-62. 38. Goldman HH, Skodol AE, Lave TR. Revising Axis V for DSM-IV: a review of measures of social
functioning. Am J Psychiatr. 1992;149(9):1148-56. 39. Barratt ES. Factor analysis of some psychometric measures of impulsiveness and anxiety. Psychol Rep.
1965;16:547-54. 40. Arntz A, Van den Hoorn M, Cornelis J, et al. Reliability and validity of the borderline personality disorder
severity index. J Pers Disord. 2003;17(1):45-59. 41. Hamilton M. The assessment of anxiety states by rating. Brit J Med Psychol. 1959;32(1):50-5. 42. Buss AH, Durkee A. An inventory for assessing different kinds of hostility. J Consult Psychol.
1957;21:343-49. 43. Harvey PD, Greenberg BR, Serper MR. The Affective Liability Scales: development, reliability and
validity. J Clin Psychol. 1989;45:786-93. 44. Sielberger CD. Manual for the State-Trait Anxiety Inventory (Form Y) “Self Evaluation Questionnaire”.
Palo Alto, CA: Consulting Psychiatrists Press; 1983. 45. Spielberge C. State-Trait Anger Expression Inventory: Professional Manual. Odessa, FL: Psychological
Assessment Resources; 1991. 46. Beck AT, Steer RA. Manual for the Beck Depression Inventory. San Antonio, TX: The Psychological
Corp: 1987. 47. Stroop JR. Studies of interference in serial verbal reactions. J Exp Psychol. 1935;18:643-61. 48. Bechara A, Demasio AR, Damasio H, et al. Insensitivity to future consequences following damage to
human prefrontal cortex. Cognition. 1994;50:7-15. 49. Zanarini MC, Vujanovic AA, Parachini EA, et al. Zanarini Rating Scale for Borderline Personality
Disorder (ZAN-BPD): a continuous measure of DSM-IV borderline psychopathology. J Pers Disord. 2003;17(3):233-42.
50. Montgomery SA, Asberg M. A new depression scale designed to be sensitive to change. Br J Psychiatry. 1979;134(4):382-9.
51. Derogatis LR. SCL-90-R, brief symptom inventory, and matching clinical rating scales. The use of psychological testing for treatment planning and outcome assessment. New York, NY: Lawrence Erlbaum;1994:41-80.
52. Coccaro EF, Harvey PD, Kupsaw-Lawrence E, et al. Development of neuropharmacologically based behavioral assessments of impulsive aggressive behavior. J Neuropsychiatry Clin Neurosci. 1991;3(2):S44-S51.
53. Jones SH, Thomicroft G, Dunn G. A brief mental health outcome scale-reliability and validity of the Global Assessment of Functioning (GAF). Br J Psychiatry. 1995;166(5):654-9.
54. Sheehan DV, Harnett-Sheehan K, Raj BA. The measurement of disability. J Clin Psychopharm. 1996;11(S3):89-95.
55. Zanarini MC, Frankenburg FR. Self-Report Version of the Zanarini Rating Scale for Borderline Personality Disorder. Belmont, Mass, McLean Hospital, 2008.
56. Young RC, Biggs JT, Ziegler VE, et al. A rating scale for mania: reliability, validity and sensitivity. Br J Psychiatry. 1978;133:429-35.
57. Pfohl B, Blum N, McCormick B, et al. Reliability and validity of the Borderline Evaluation of Severity Over Time (BEST): a self-rated scale to measure severity and change in persons with borderline personality disorder. J Pers Disord. 2009;23:281-93.
58. Simpson GM, Angus JW. A rating scale for extrapyramidal side effects. Acta Psychiatr Scand. 1970;45(S212):11-9.
59. Barnes TR. A rating scale for drug-induced akathisia. Br J Psychiatry. 1989;154(5):672-6. 60. Guy W: ECDEU Assessment Manual for Psychopharmacology: Publication ADM 76-338. Washington,
DC, US Department of Health, Education and Welfare.1976:534-7. 61. Guy W. Dosage Record and Treatment Emergent Symptoms Scale (DOTES): ECDEU Assessment
Manual for Psychopharmacology-Revised, US Department of Health, Education and Welfare, Public Health Service, Alcohol, Drug Abuse, and Mental Health Administration, NIMH Psychopharmacology
Norman 19
Research Branch, Division of Extramural Research Programs. National Institute of Mental Health, Rockville, Md. 1976: 223-44.
62. Lingiaerde O, Ahifors UG, Bech P. The UKU Side Effect Rating Scale: a new comprehensive rating scale for psychotropic drugs and a cross-sectional study of side effects in neuroleptic treated patients. Acta Psychiatr Scand. 1987;25:349-55.
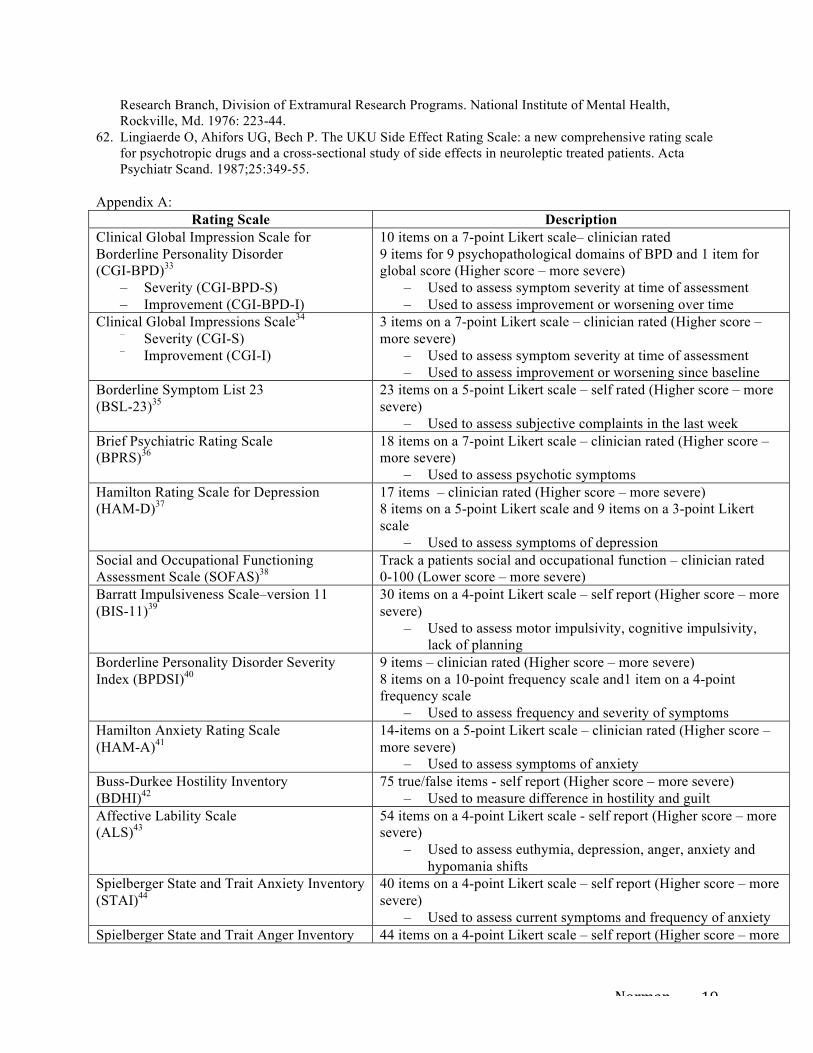
Appendix A: Rating Scale Description
Clinical Global Impression Scale for Borderline Personality Disorder (CGI-BPD)33
– Severity (CGI-BPD-S) – Improvement (CGI-BPD-I)
10 items on a 7-point Likert scale– clinician rated 9 items for 9 psychopathological domains of BPD and 1 item for global score (Higher score – more severe)
– Used to assess symptom severity at time of assessment – Used to assess improvement or worsening over time
Clinical Global Impressions Scale34
– Severity (CGI-S)
– Improvement (CGI-I)
3 items on a 7-point Likert scale – clinician rated (Higher score – more severe)
– Used to assess symptom severity at time of assessment – Used to assess improvement or worsening since baseline
Borderline Symptom List 23 (BSL-23)35
23 items on a 5-point Likert scale – self rated (Higher score – more severe)
– Used to assess subjective complaints in the last week Brief Psychiatric Rating Scale (BPRS)36
18 items on a 7-point Likert scale – clinician rated (Higher score – more severe)
– Used to assess psychotic symptoms Hamilton Rating Scale for Depression (HAM-D)37
17 items – clinician rated (Higher score – more severe) 8 items on a 5-point Likert scale and 9 items on a 3-point Likert scale
– Used to assess symptoms of depression Social and Occupational Functioning Assessment Scale (SOFAS)38
Track a patients social and occupational function – clinician rated 0-100 (Lower score – more severe)
Barratt Impulsiveness Scale–version 11 (BIS-11)39
30 items on a 4-point Likert scale – self report (Higher score – more severe)
– Used to assess motor impulsivity, cognitive impulsivity, lack of planning
Borderline Personality Disorder Severity Index (BPDSI)40
9 items – clinician rated (Higher score – more severe) 8 items on a 10-point frequency scale and1 item on a 4-point frequency scale
– Used to assess frequency and severity of symptoms Hamilton Anxiety Rating Scale (HAM-A)41
14-items on a 5-point Likert scale – clinician rated (Higher score – more severe)
– Used to assess symptoms of anxiety Buss-Durkee Hostility Inventory (BDHI)42
75 true/false items - self report (Higher score – more severe) – Used to measure difference in hostility and guilt
Affective Lability Scale (ALS)43
54 items on a 4-point Likert scale - self report (Higher score – more severe)
– Used to assess euthymia, depression, anger, anxiety and hypomania shifts
Spielberger State and Trait Anxiety Inventory (STAI)44
40 items on a 4-point Likert scale – self report (Higher score – more severe)
– Used to assess current symptoms and frequency of anxiety Spielberger State and Trait Anger Inventory 44 items on a 4-point Likert scale – self report (Higher score – more
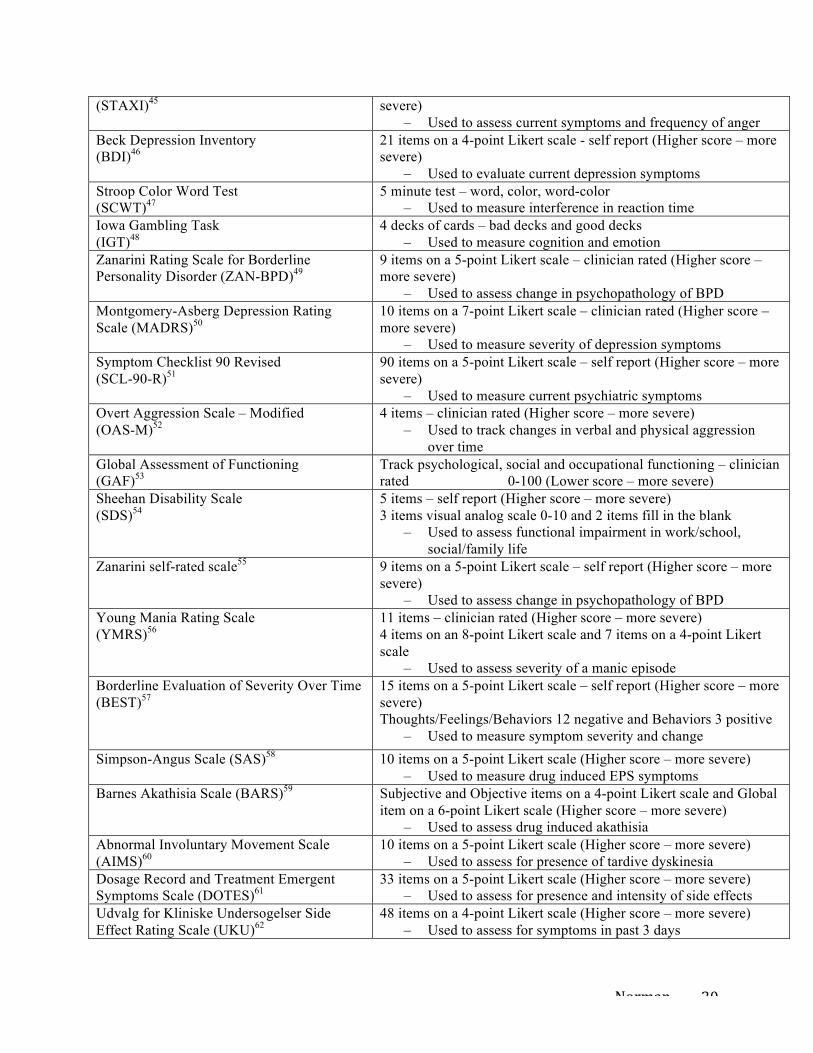
Norman 20
(STAXI)45 severe) – Used to assess current symptoms and frequency of anger
Beck Depression Inventory (BDI)46
21 items on a 4-point Likert scale - self report (Higher score – more severe)
– Used to evaluate current depression symptoms Stroop Color Word Test (SCWT)47
5 minute test – word, color, word-color – Used to measure interference in reaction time
Iowa Gambling Task (IGT)48
4 decks of cards – bad decks and good decks – Used to measure cognition and emotion
Zanarini Rating Scale for Borderline Personality Disorder (ZAN-BPD)49
9 items on a 5-point Likert scale – clinician rated (Higher score – more severe)
– Used to assess change in psychopathology of BPD Montgomery-Asberg Depression Rating Scale (MADRS)50
10 items on a 7-point Likert scale – clinician rated (Higher score – more severe)
– Used to measure severity of depression symptoms Symptom Checklist 90 Revised (SCL-90-R)51
90 items on a 5-point Likert scale – self report (Higher score – more severe)
– Used to measure current psychiatric symptoms Overt Aggression Scale – Modified (OAS-M)52
4 items – clinician rated (Higher score – more severe) – Used to track changes in verbal and physical aggression
over time Global Assessment of Functioning (GAF)53
Track psychological, social and occupational functioning – clinician rated 0-100 (Lower score – more severe)
Sheehan Disability Scale (SDS)54
5 items – self report (Higher score – more severe) 3 items visual analog scale 0-10 and 2 items fill in the blank
– Used to assess functional impairment in work/school, social/family life
Zanarini self-rated scale55
9 items on a 5-point Likert scale – self report (Higher score – more severe)
– Used to assess change in psychopathology of BPD Young Mania Rating Scale (YMRS)56
11 items – clinician rated (Higher score – more severe) 4 items on an 8-point Likert scale and 7 items on a 4-point Likert scale
– Used to assess severity of a manic episode Borderline Evaluation of Severity Over Time (BEST)57
15 items on a 5-point Likert scale – self report (Higher score – more severe) Thoughts/Feelings/Behaviors 12 negative and Behaviors 3 positive
– Used to measure symptom severity and change Simpson-Angus Scale (SAS)58 10 items on a 5-point Likert scale (Higher score – more severe)
– Used to measure drug induced EPS symptoms Barnes Akathisia Scale (BARS)59 Subjective and Objective items on a 4-point Likert scale and Global
item on a 6-point Likert scale (Higher score – more severe) – Used to assess drug induced akathisia
Abnormal Involuntary Movement Scale (AIMS)60
10 items on a 5-point Likert scale (Higher score – more severe) – Used to assess for presence of tardive dyskinesia
Dosage Record and Treatment Emergent Symptoms Scale (DOTES)61
33 items on a 5-point Likert scale (Higher score – more severe) – Used to assess for presence and intensity of side effects
Udvalg for Kliniske Undersogelser Side Effect Rating Scale (UKU)62
48 items on a 4-point Likert scale (Higher score – more severe) – Used to assess for symptoms in past 3 days


















