The Unbearable Lightness of Being Eating Disorders in ...
58
+ The Unbearable Lightness of Being Eating Disorders in General Practice 2021 Dr Janet Bayley NQUEDS CHMHATODS With thanks to Dr Warren Ward Director Eating Disorders Service RBWH and Emma Coleman NQuEDS Dietitian
Transcript of The Unbearable Lightness of Being Eating Disorders in ...
+
The Unbearable Lightness of BeingEating Disorders in General Practice 2021Dr Janet Bayley NQUEDS CHMHATODS
With thanks to Dr Warren WardDirector Eating Disorders ServiceRBWH and Emma Coleman NQuEDS Dietitian
ACKNOWLEDGMENT OF OUR TRADITIONAL OWNERS
We acknowledge Aboriginal people and Torres Strait Islanders as this country’s First Nations people.
We recognise First Nation people and communities as traditional and cultural custodians of the lands on which we work to provide safe and quality health services.
We pay our respect to Elders past, present and emerging.
Artwork produced for Cairns and Hinterland Hospital and Health Service
by Jedess Hudson
+Definition
DSM V Classification
Anorexia Nervosa
Avoidant/Restrictive Food Intake Disorder
Binge Eating Disorder
Bulimia Nervosa
Other Specified Feeding or Eating Disorder
PICA
Rumination Disorder
Eating disorders are characterised by disturbances of eatingbehaviours and a core psychopathology centred on food, eating andbody image concerns (RANZCP Guidelines)
Overevaluation weight and body shape
+
Small Bites
BMI no longer as important for many patients
Most people with an eating disorder have an unremarkable body weight as restraint –binge/purge cancel each other out
Increasing numbers of people are presenting with significant malnutrition with “higher BMI” AKA Atypical AN (“The Biggest Loser” Effect)
Many are told by medical professionals they “are not thin enough to have an eating disorder”
+Eating Disorders are common, and increasing in prevalence 1 in 20 Australians has an eating disorder*
Approximately 15% of Australian women experience an eating disorder during their lifetime*
The number of people in Australia with purging behaviours has doubled in past 10 years^
*www.nedc.com.au
^Hay PJ, Mond J, Buttner P, Darby A (2008) Eating Disorder Behaviors Are Increasing: Findings from Two Sequential Community Surveys in South Australia. PLoS ONE 3(2)
+High Mortality Rates10-20% for Anorexia Nervosa
The highest mortality rate of any psychiatric illness
+Causes of Death
80% due to medical causes. Bloods can be totally normal at time of death. Fatal arrhythmias Hypotension Hypoglycemia Hypokalemia Hypophosphatemia
20% Suicide Suicide rates in those with
AN 32x more likely than those without
+A Lethal Combination
I’m fine’
‘There’s nothing wrong with me’
‘I’ll eat’
‘See my bloods are fine’
‘You worry too much’
‘I’m not dead yet’
‘Everyone in my family is thin’
‘She’s medically stable’
‘Her bloods are fine’
‘Everything’s pretty normal now’
‘We’ve corrected her potassium’
‘She looks fine’
‘She’s an athlete so you’d expect her pulse to be low’
Sufferer denial Doctor Ignorance
+ What causes eating disorders?
The causes of eating disorders are complex and include… Genetic Personality Early attachment problems (trauma/abuse/neglect) Obesity Bullying and teasing The culture and media/certain subcultures Stressors Dieting Starvation syndrome
No consistent evidence of an anorexogenic familyOften adverse events within family precede development
of ED
+
The Six Seductions of AnorexiaEmily T. Troscianko - A Hunger Artist
1. Anorexia as anaesthetic: Making everything else matter less
2. Anorexia as Rosetta Stone: Giving you ready made meaning
3. Anorexia as gold star: Giving you top marks in the little things .
4. Anorexia as halo: Making you feel special
5. Anorexia as hunger strike: Letting you be other than what you’re expected to be.
6. Anorexia as partial suicide: Letting you live.
+The Impact of TV on Teenage Girls
Within 3 years of introduction of TV to area in Fiji:
Eating Disorder symptoms increased 5-fold
Vomiting to control weight increased from 3% to 15%
74% felt “too big or fat”
62% dieting in past month
Favourite programs included Melrose Place, ER, Xena: Warrior Princess.
Becker et al (2002) British Journal of Psychiatry, 180, 509-514
This study done in 2002 BEFORE:
Facebook (2004)
The iPhone (2008)
Instagram (2010) Front-facing
Cameras And Selfies (2010)
Snapchat (2011)
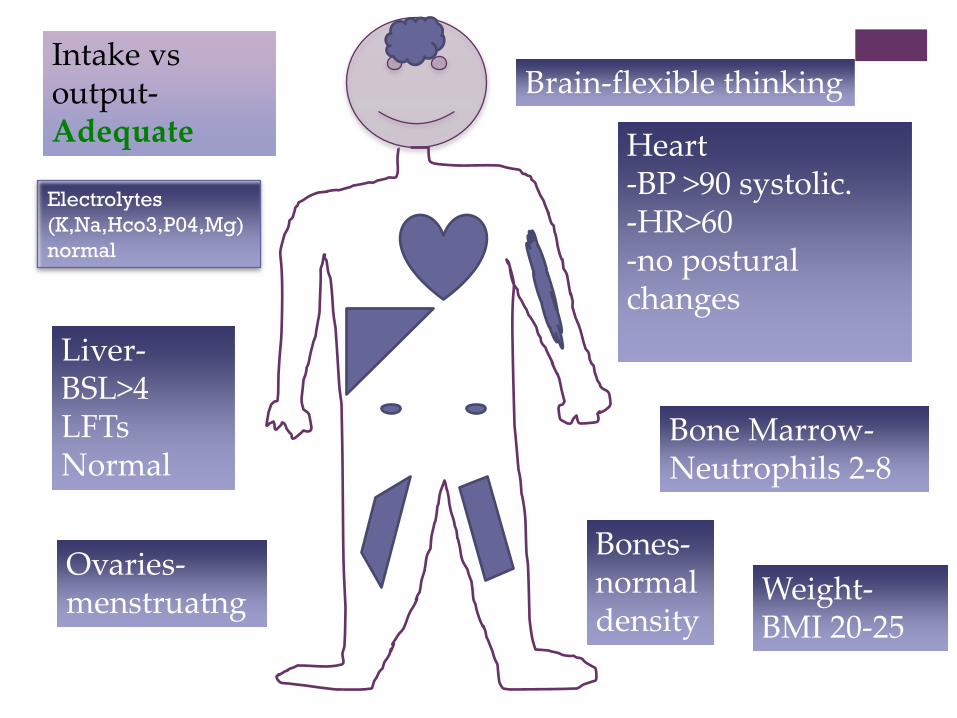
Brain-flexible thinking
Heart-BP >90 systolic.-HR>60 -no postural changes
Bone Marrow-Neutrophils 2-8
Liver-BSL>4LFTs Normal
Ovaries-menstruatng
Bones-normal density
Weight-BMI 20-25
Intake vs output-Adequate
Electrolytes (K,Na,Hco3,P04,Mg) normal
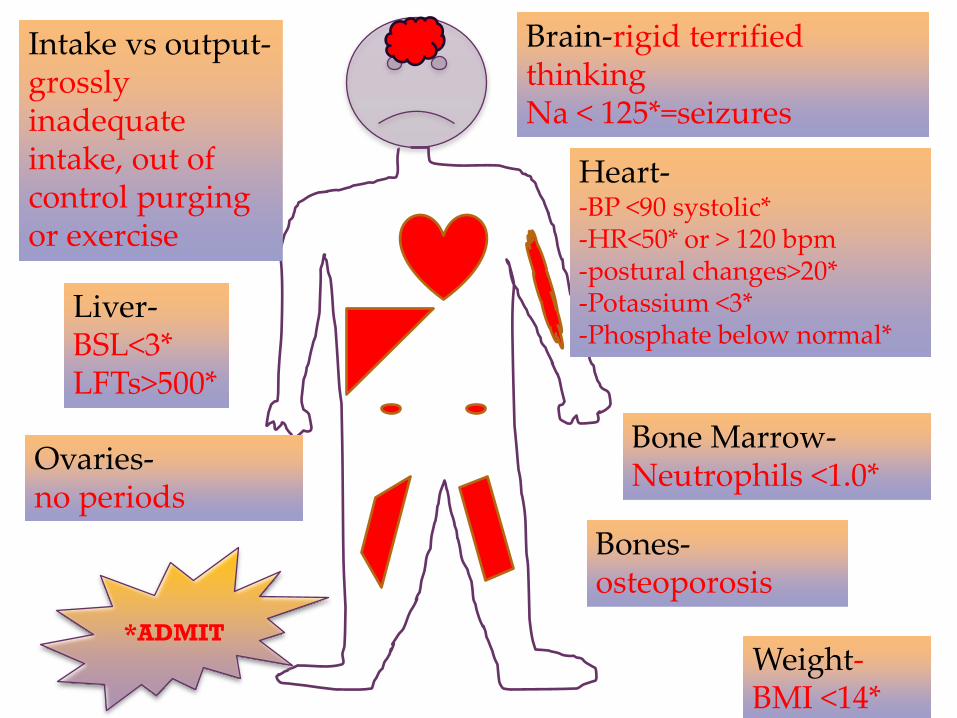
Brain-rigid terrified thinkingNa < 125*=seizures
Heart--BP <90 systolic*-HR<50* or > 120 bpm-postural changes>20*-Potassium <3*-Phosphate below normal*
Bone Marrow-Neutrophils <1.0*
Liver-BSL<3*LFTs>500*
Ovaries-no periods
Bones-osteoporosis
Weight-BMI <14*
Intake vs output-grossly inadequate intake, out of control purging or exercise
*ADMIT
+
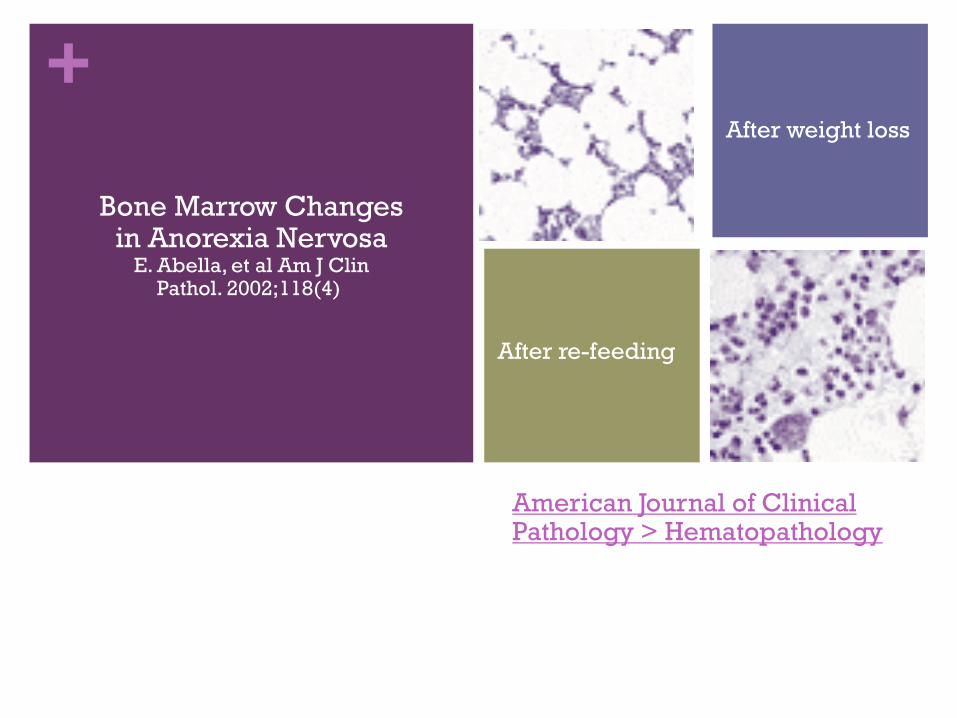
American Journal of Clinical Pathology > Hematopathology
Bone Marrow Changes in Anorexia Nervosa
E. Abella, et al Am J Clin Pathol. 2002;118(4)
After weight loss
After re-feeding
+
The Medical Assessment•History
•Examination
•Investigations
FNQ Health Pathways
+
Red Flags
High – risk patient, or medically unstable eg electrolyte disturbance
Pregnant with low BMI and failure to gain adequate weight
Extremely underweight (eg BMI <16) or rapid weight loss
Recurrent ketoacidosis in diabetic patients
Suicide risk
+History: Suggestive Features
Unexplained disturbances in physical observations or pathology eg bradycardia, neutropenia
Rapid or unexplained wt loss
Inadequate wt gain in pregnancy
Preoccupation with
Wt, body shape, Xs exercise
Diet or GIT symptoms + low BMI
Grossly inadequate nutritional intake
Suicidal ideation, alcohol + substance use, DSH
T1DM with unexplained poor glycaemic control
Suspected misuse of medications (eg laxatives, diuretics, wt loss pills)
Disturbed eating behaviours(purge, binge, fast)
Personal or Family Hx ED
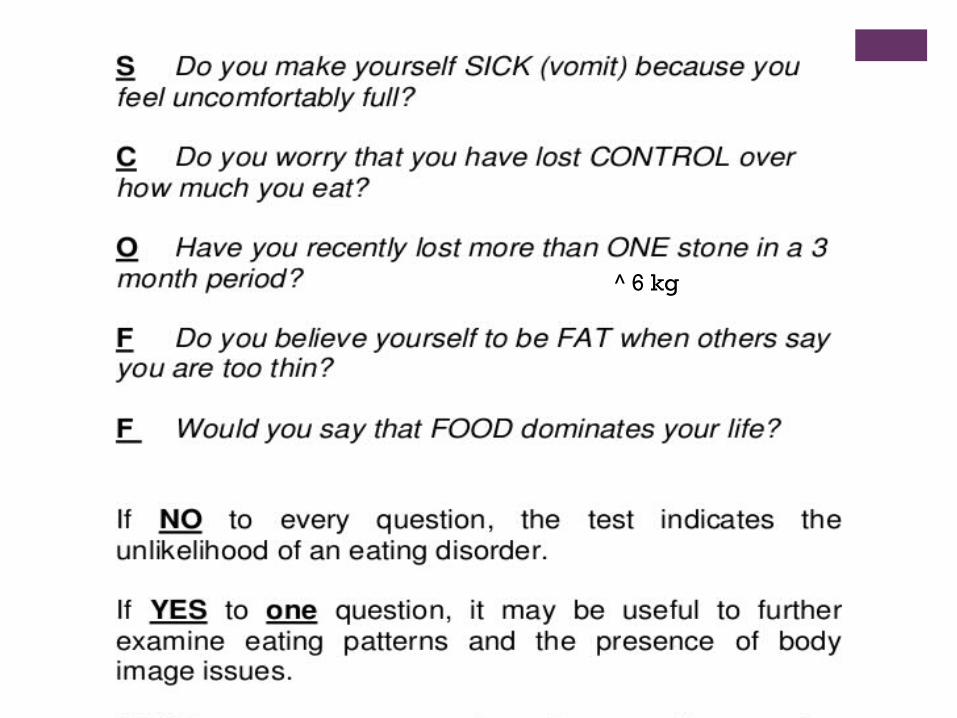
^ 6 kg
+
If you suspect an Eating Disorder, always ask what they have eaten in the last 24 hr for:Breakfast
Morning Tea
Lunch
Afternoon TeaDinner
Supper
+
Targeted History
Collateral information family etc
Weight history
Physical activity and food related behaviours
Signs and symptoms of severity
Physiological changes
Psychosocial factors
Co-morbidities and medications
+Physical examination
Weight*
Height*
BP/HR-lying and standing
Postural Tachycardia >20 BPM
Consider on spot BSL
*Body Mass Index(BMI)=Wt(kg)÷Ht(m)÷Ht(m)

+
Investigations
Serum biochemistry incl Ca2+, Mg, PO4, TSH
Full Blood Count
ECGIncreased PR, 1oHB,
Bradycardia, ST-T changes, QTC prolongation
+ If patient doesn’t meet criteria for medical admission…
Should really be admitted medically if has met any of criteria in last 24 hours e.g. at G.P. or outpatients
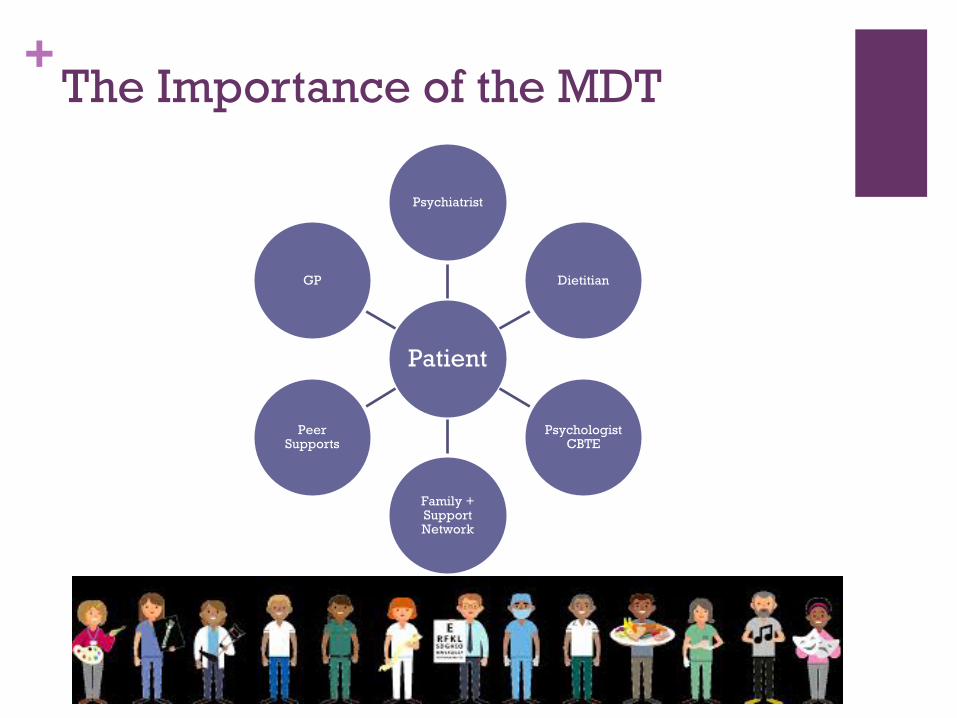
+The Importance of the MDT
Patient
Psychiatrist
Dietitian
Psychologist CBTE
Family + Support Network
Peer Supports
GP
+ Treating Eating Disorders
Establish a therapeutic alliance
Monitor and stabilise medically
Reverse cognitive & behavioural effects of starvation
• more adaptive ways to deal with emotions• to resist cultural pressures• To identify and challenge ED thoughts
Psychotherapy – help patient learn:
+The Art of Engagement
Find common goals
Clarify non-negotiables
Educate the patient
Enhance motivation
Externalise the disorder
Involve the family
Monitor countertransference
Interdisciplinary MDT approach
Consultation
Mental Health Act
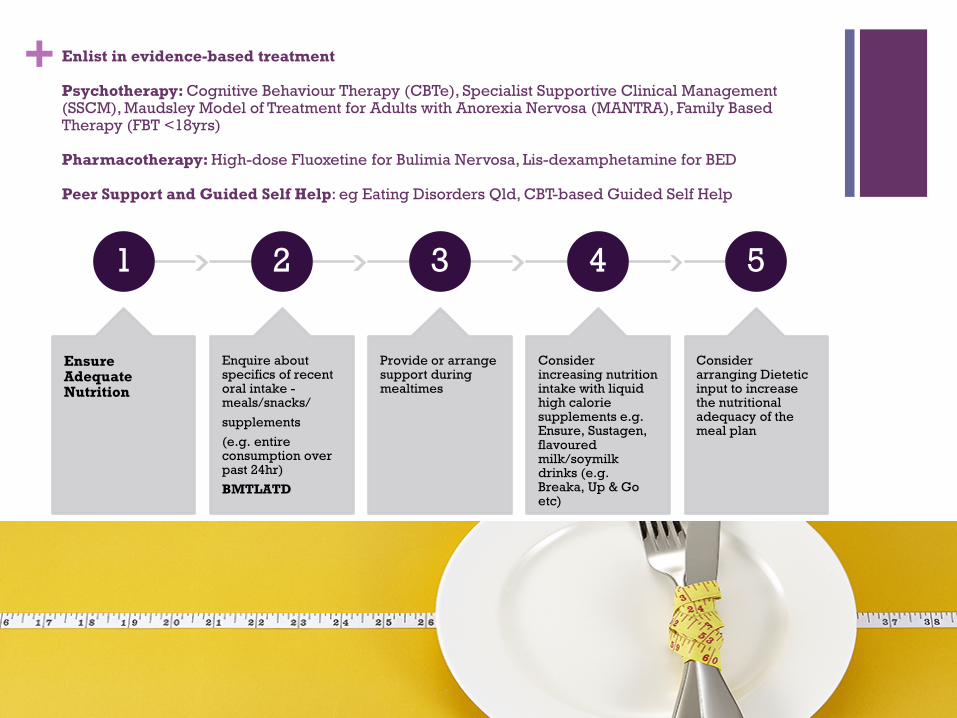
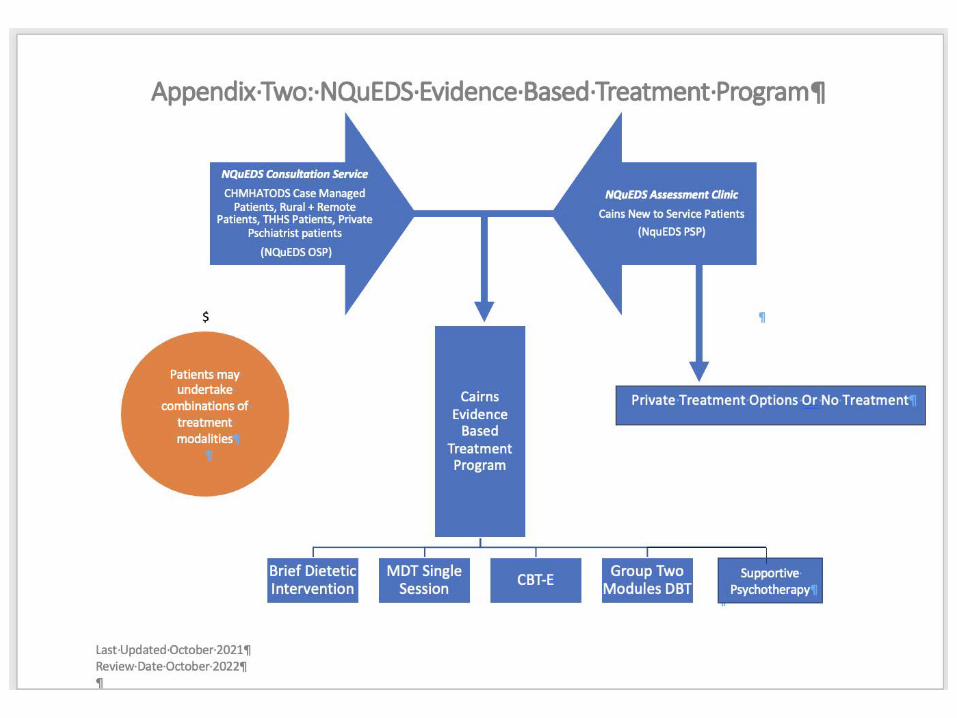
+ Enlist in evidence-based treatment
Psychotherapy: Cognitive Behaviour Therapy (CBTe), Specialist Supportive Clinical Management (SSCM), Maudsley Model of Treatment for Adults with Anorexia Nervosa (MANTRA), Family Based Therapy (FBT <18yrs)
Pharmacotherapy: High-dose Fluoxetine for Bulimia Nervosa, Lis-dexamphetamine for BED
Peer Support and Guided Self Help: eg Eating Disorders Qld, CBT-based Guided Self Help
1
Ensure Adequate Nutrition
2
Enquire about specifics of recent oral intake -meals/snacks/supplements (e.g. entire consumption over past 24hr)BMTLATD
3
Provide or arrange support during mealtimes
4
Consider increasing nutrition intake with liquid high calorie supplements e.g. Ensure, Sustagen, flavoured milk/soymilk drinks (e.g. Breaka, Up & Go etc)
5
Consider arranging Dietetic input to increase the nutritional adequacy of the meal plan
+GP Role
Medical Monitoring May be weekly if very unwell FBC ELFT Postural BP/HR Temp Weights ECG PRN Bone health
Referrals Dietitian, Psychology, Psychiatry
Patient Support, Education and Engagement
Family Support, Education and Engagement
+ MBS Eating Disorder Management Plan From 1 November 2019, a new suite of 64 Medicare Benefits Schedule (MBS) items will be introduced to
support a model of best practice evidence based care for patients with anorexia nervosa and other eligible patients with eating disorders.
· The listing of these new items is a result of recommendations in 2018 by the independent clinician-led Medical Benefits Schedule (MBS) Review Taskforce and the Australian Government’s response to those recommendations.
·This new item structure means eligible patients will be able to receive a Medicare rebate when eligible providers undertake the development of a Eating Disorder treatment and management plan or a review which will activate: a course of evidence based eating disorder psychological treatment services (up to a total of 40 psychological
services in a 12 month period); and
up to 20 dietetic services, in a 12 month period, depending on their treatment needs.
It is intended that the MBS services will be provided by practitioners with the knowledge, skills and experience in providing treatment to patients with eating disorders.
·Treatment provided under the Eating Disorder Psychological Treatment items are limited to the defined list of evidence based eating disorder specific treatments.
·Patients who do not fit the eligibility criteria for the MBS Eating Disorders Treatment Pathway may be eligible for treatment under the Better Access to Mental Health treatment pathway.
·There will be an evaluation of the new items after 12 months to assess if the items are operating as intended for patients, providers and the Government.

+
EDTP
Review
Before or at sessions, 10, 20, 30 psychological treatmentAfter session 1 or 2 of dietetics servicesAt EDTP completion
Psychiatrist or Paediatrician review by session 20 of psychological treatment (reviewing specialist must be able to claim relevant MBS item number)
Co-morbidities or pre-existing conditions, consider if another simultaneous MBS management plan advisable
Avoidant Restrictive Food Intake Disorder Consider GP MHTP instead as not eligible for EDTP
+
EDE-Q
+https://insideoutinstitute.org.au

+
Encourage contact with community-based support services
Some offer online services for patients and carers and clinicians

+
+Referrals NQUEDS
Routine Referral
Complete Referral Form
Contact CHMHATODS Centralised Intake Service
phone 1300 642 255 fax 07 4226 3149
Urgent need for advice
Contact NQUEDS Intake (Usually CNC or Psychiatry Registrar)
Phone 07 4226 3100
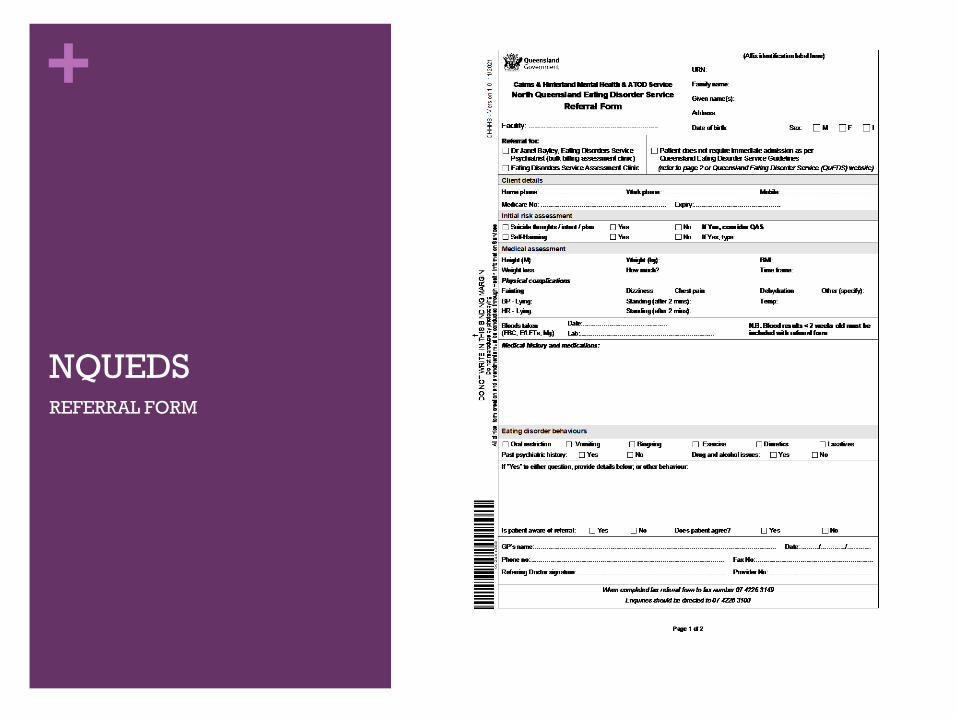
+
NQUEDS REFERRAL FORM
+Optional Extra Bits

+Effects of Starvation Syndrome
Physical changes• Heart rate reduced by 25%• Heart rate and blood pressure decreased• Basal metabolic rate slowed down• Feeling cold• Fluid retention • Loss of strength/fatigue• Hair loss and dry skin •Wt loss 25%
Attitudes and behaviour relating to eating• Thinking about food all the time•Meticulous planning on meals• Eating very fast of very slowly• Increased hunger, binge-eating• Unusual food routines and rituals • Tendency to hoard • Increased use of condiments for flavour
Emotional changes•Depression • Anxiety• Irritability• Increased mood fluctuations• Intense and negative emotional reactions• Reduced motivation• Loss of interest in life
Social changes•Withdrawal and isolation• Loss of sense of humour• Feelings of social inadequacy•Neglect of personal hygiene•More critical of others• Strained relationships
Changes in thinking• Impaired concentration, judgement and decision-making• Impaired comprehension• Increased rigidity and obsessional thinking• Reduced alertness
+
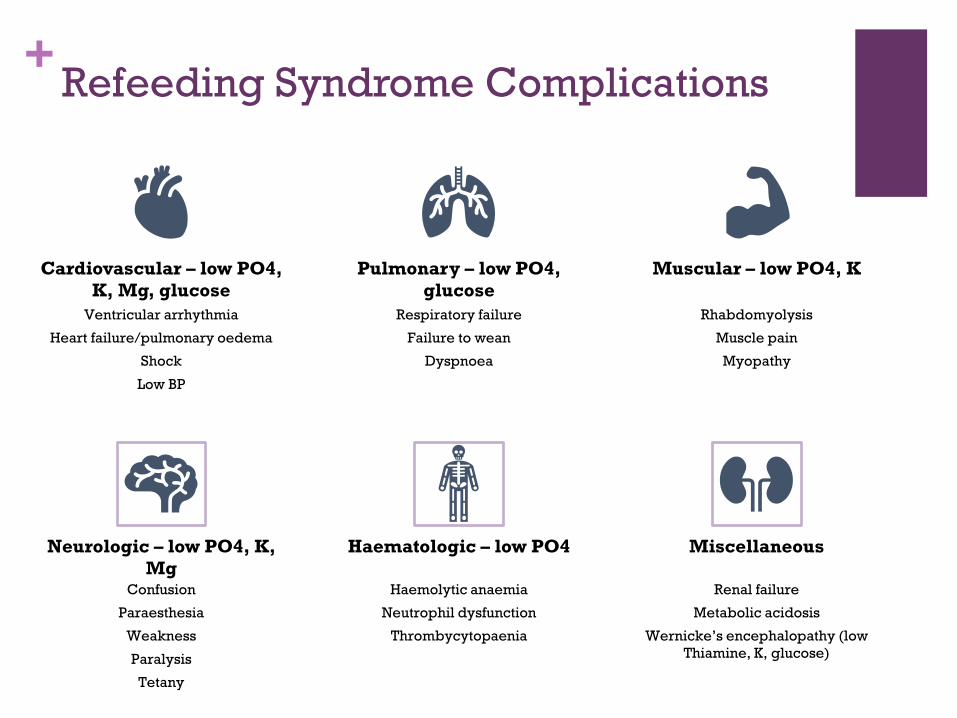
Cardiovascular – low PO4, K, Mg, glucose
Ventricular arrhythmia
Heart failure/pulmonary oedema
Shock
Low BP
Pulmonary – low PO4, glucose
Respiratory failure
Failure to wean
Dyspnoea
Muscular – low PO4, K
Rhabdomyolysis
Muscle pain
Myopathy
Neurologic – low PO4, K, Mg
Confusion
Paraesthesia
Weakness
Paralysis
Tetany
Haematologic – low PO4
Haemolytic anaemia
Neutrophil dysfunction
Thrombycytopaenia
Miscellaneous
Renal failure
Metabolic acidosis
Wernicke’s encephalopathy (low Thiamine, K, glucose)
Refeeding Syndrome Complications
+
Benefits of Nasogastric Refeeding
Prevents hypoglycaemia due to constant supply of carbohydrates
Reduces gastric discomfort
96% of ED patients report postprandial fullness
More controlled method of renourishment
Minimise electrolyte shifts in refeeding
Reach goal nutrition more timely (less chance of not receiving nutrition)
Ensures adequate hydration (only 17% ED patients consume recommended amount)
Shortens length of stay (one study showed LOS reduced by 17 days)
Can be a relief/break for a person
When placed at admission, less likely to be seen as a punishment for poor treatment compliance
Eating disorder patients will generally fall into low-risk group for NGT insertion with pH testing for confirmation avoiding the need for chest x-ray.
+
Ethical & Legal Considerations
Autonomy
Beneficence
Competence/decision-making capacity
Reversibility of starvation syndrome
Legal framework
+
Recovery
“Normal Eating”Flexible and regular
Diversity of foods
Not preoccupied with avoiding food
Enjoy food
Social Meals
Family Meals
No Compensatory Behaviours
“Normal Emotions”Tolerance of distress
Experience of emotional range
Life outside of eating disorder
Self esteem
Absence shame and guilt
Mentalization ability
Variety+
Regular+
Enough
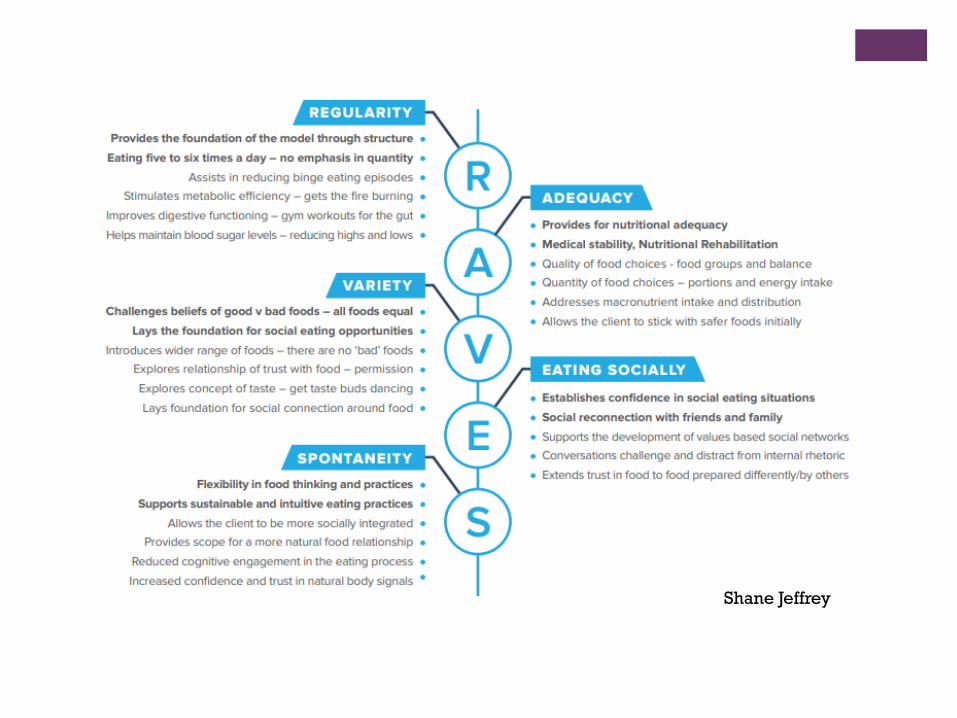
Shane Jeffrey
+
Bariatric Surgery
Eating disorders and disordered eating are prevalent in the bariatric population
Patients with BED show similar patterns of weight loss post surgery cf non-BED
Problems
• Loss of control: eating pathology and weight gain
• Too much control: Anorexia Nervosa• Alcohol abuse risk increases post
bariatric surgery
+Type 1 DM: 2.4 X risk of ED
Why?
Focus on food, weight and exercise
Weight loss at onset of DM
Weight gain with insulin treatment
Availability of extra weight loss technique (insulin restriction/omission)
Need to be like peers
Need to assert control/autonomy/independence
Goebel-Fabbri. Diabetes and Eating Disorders. J Diabetes Sci Technol. 2008 May; 2(3): 530–532.
Jones JM, Lawson ML, Daneman D, Olmsted MO, Rodin G. Eating disorders in adolescent females with and without type 1 diabetes: cross sectional study. BMJ. 2000 Jun 10; 320(7249): 1563–1566.
+
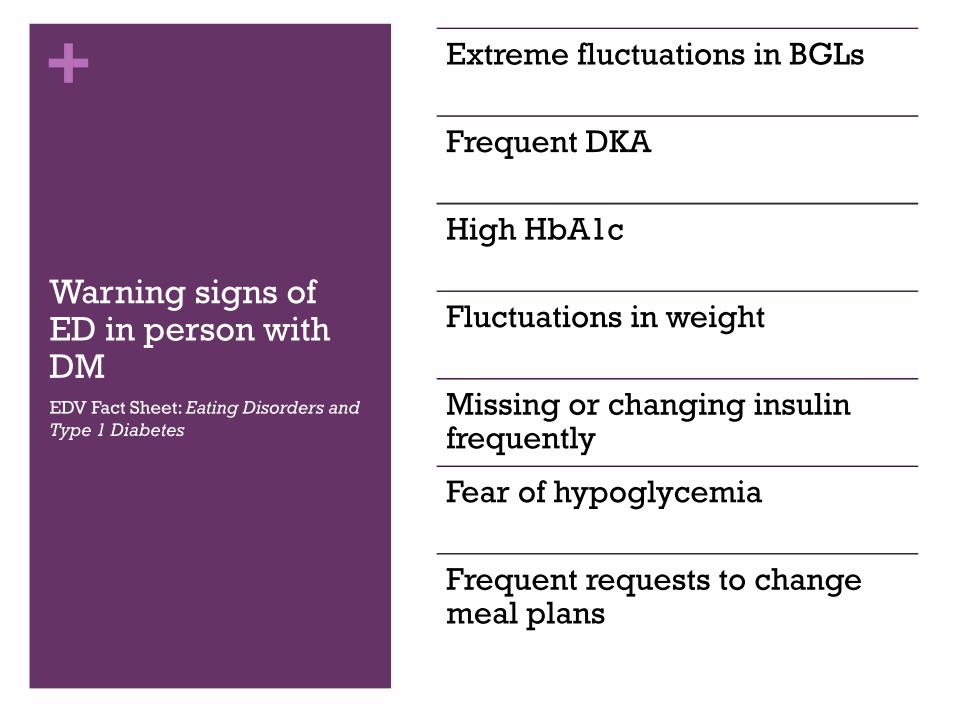
Warning signs of ED in person with DMEDV Fact Sheet: Eating Disorders and Type 1 Diabetes
Extreme fluctuations in BGLs
Frequent DKA
High HbA1c
Fluctuations in weight
Missing or changing insulin frequently
Fear of hypoglycemia
Frequent requests to change meal plans
+Diabetes and Binge Eating
Type II DM: 6.5-9% have binge eating
Type I DM: binge eating also common
• Depression (50%)• Self-medicating other negative feelings incl remorse• Dieting/restriction• Fluctuations in blood glucose
Causes of binge eating:
+
Eating Disorders in the Peripartum
Pregnancy is a time of enormous body transformation
Body and weight dissatisfaction are common in peripartum
Link between active eating disorder in pregnancy and poor maternal and neonatal outcomes Miscarriage Pre-eclampsia Postnatal depression Anaemia Low birth weight - particularly in
Anorexia Nervosa High birth weight - particularly In Binge
Eating Disorder (BED) Premature birth Poor infant attachment and maternal
bonding Feeding difficulties in infancy
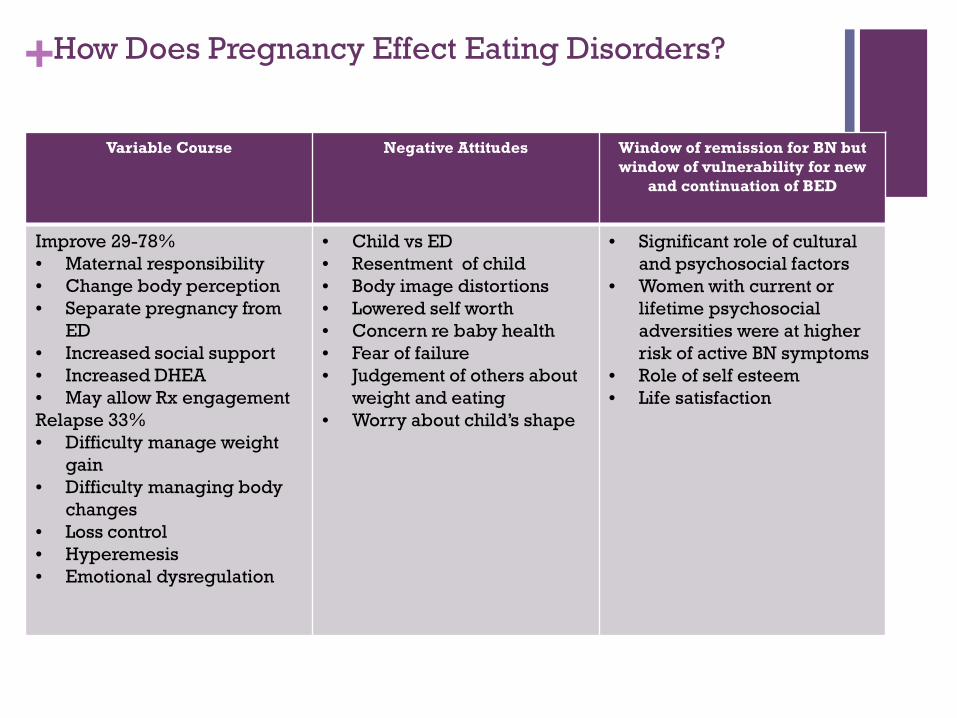
+How Does Pregnancy Effect Eating Disorders?
Variable Course Negative Attitudes Window of remission for BN but window of vulnerability for new
and continuation of BED
Improve 29-78%• Maternal responsibility• Change body perception• Separate pregnancy from
ED• Increased social support• Increased DHEA • May allow Rx engagement Relapse 33%• Difficulty manage weight
gain• Difficulty managing body
changes• Loss control• Hyperemesis• Emotional dysregulation
• Child vs ED• Resentment of child• Body image distortions • Lowered self worth• Concern re baby health• Fear of failure• Judgement of others about
weight and eating• Worry about child’s shape
• Significant role of cultural and psychosocial factors
• Women with current or lifetime psychosocial adversities were at higher risk of active BN symptoms
• Role of self esteem• Life satisfaction
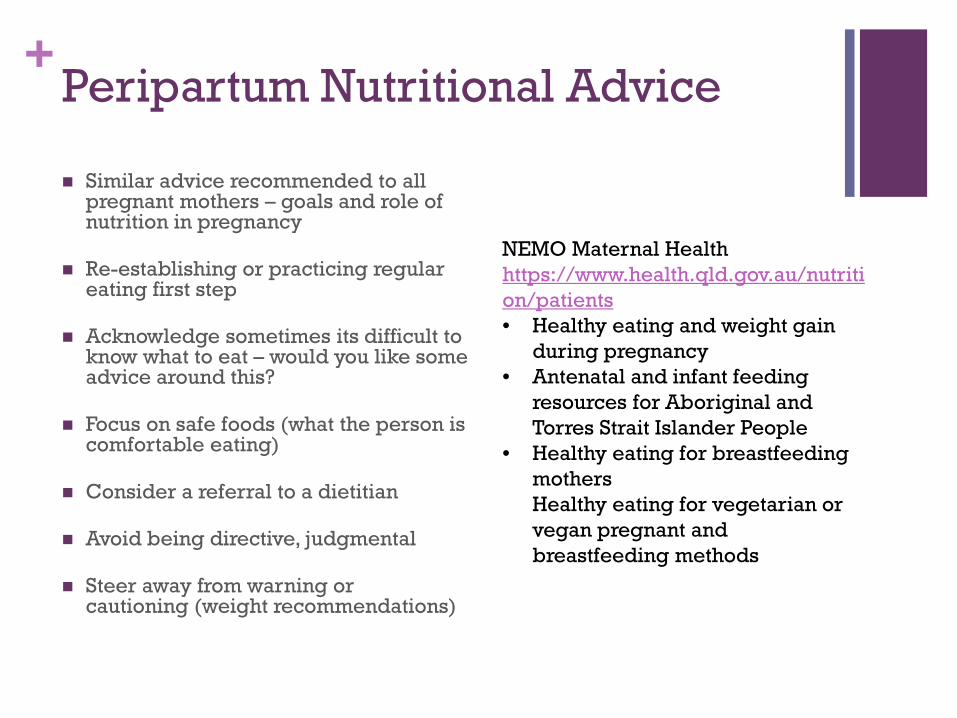
+Peripartum Nutritional Advice
Similar advice recommended to all pregnant mothers – goals and role of nutrition in pregnancy
Re-establishing or practicing regular eating first step
Acknowledge sometimes its difficult to know what to eat – would you like some advice around this?
Focus on safe foods (what the person is comfortable eating)
Consider a referral to a dietitian
Avoid being directive, judgmental
Steer away from warning or cautioning (weight recommendations)
NEMO Maternal Health https://www.health.qld.gov.au/nutrition/patients• Healthy eating and weight gain
during pregnancy• Antenatal and infant feeding
resources for Aboriginal and Torres Strait Islander People
• Healthy eating for breastfeeding mothersHealthy eating for vegetarian or vegan pregnant and breastfeeding methods
+Gestational diabetes
Can increase/exacerbate ED behaviours
Food monitoring
Carbohydrate counting
Treating hypo’s: sugary food and drink
Body changes during pregnancy
Consider individual treatment rather than group
Can better adjust for the eating disorder
Regular eating and general eating in pregnancy
Meal ideas vs. carbohydrate counting
‘safe’ hypo management plan
Strategies for bingeing/purging behaviours
Liaison Obstetrics + Endocrine + POSM/NQUEDS teams
+ Bone Health Assessment & Management North Queensland Eating Disorder Service Clinical Practice Guideline
DRAFT Referral Screening Investigations
General Practitioner and NQUEDS Intake to make relevant inquiries FBC, ELFT, B12, Folate, Iron, Vitamin D, TSH
Postural BP and HR Temp etc
NQUEDS Assessment
Psychiatry/Dietitian Investigate fracture history
Investigate dietary intake and evidence of malnutrition
Look for other signs high risk Osteoporosis
Fracture history
Amenorrhoea (duration)
Identification of low BMI and/or malnutrition
Restore weight and resumption of normal eating behaviours
Identification Inadequate Calcium dietary intake
Less than 1000-1200mg per day Recommend dietary enhancement of calcium
intake
Commence Calcium supplements 600mg tablets, i-ii Indefinite until adequate dietary calcium intake
Identification Vitamin D Deficiency Risk
Less than 75 nmol/L Commence Vitamin D Replacement tablets
Consider annual monitoring or more frequently if severe Vitamin D deficiency
If Vitamin D level does not increase with oral supplements
Consider IMI 600 000 units 3-6monthly.
Consider alternative causes for level not returning to normal (eg. pancreatic insufficiency)
+ Bone Health Assessment & Management 2 North Queensland Eating Disorder Service Clinical Practice Guideline
DRAFT Identification Amenorrhoea greater than
six months duration Baseline Dexa scan
Two yearly Dexa scan thereafter
Consider bone density 2-5 yearly or repeat at time of menopause.
Can consider ceasing ongoing routine surveillance if recovery eating disorder and normal bone density.
Consider hormone replacement therapy” Low BMI (<17) and amenorrhoea
Pubertal younger adult (peak bone mass is achieved in teens and this is important time to avoid hypogonadism)
Minimal trauma fracture (therefore higher risk of further minimal trauma fractures)
More severe osteoporosis (ie BMD Z score -2.5 or worse)
Poorer prognosis with eating disorder - ie chance of achieving healthy BMI is lower
Estalis Sequi patch - Until normal BMI and spontaneous recovery of hypogonadism - ienormal menses.
If topical HRT not an option second line option Oral Combined Contraceptive Pill if no contraindications"
Identification of established osteoporosis consider secondary screening Thyroid Test
Vitamin D,
Coeliac Screening (Ttg/Iga)
Parathyroid Hormone
Endocrinology Referral If minimal trauma fracture or established
osteoporosis CHHHS Medical Referral (MR Form) if Cat 1 or
external referral from GP
Yearly review of bone health for long term patients of NQUEDS