
THE STEROID HORMONE CASCADE · from any online file that you purchased. Unlimited quizzes may be...
32
Authored by: Deborah L. Buckley Course Code - C018 Category - Chemistry Contact Hours - 2 ** CEUINC is approved as a provider of continuing education programs in the clinical laboratory sciences by the ASCLS P.A.C.E. ® Program. ** Level - Intermediate *This course meets the 1 hour Chemistry requirement for Florida license renewal* THE STEROID HORMONE CASCADE
Transcript of THE STEROID HORMONE CASCADE · from any online file that you purchased. Unlimited quizzes may be...

Authored by: Deborah L. Buckley
Course Code - C018 Category - Chemistry
Contact Hours - 2
** CEUINC is approved as a provider of continuing education programs in the clinical laboratory sciences by the ASCLS P.A.C.E.® Program. **
Level - Intermediate
*This course meets the 1 hour Chemistry requirement for Florida license renewal*
THE STEROID HORMONE CASCADE

i www.4CEUINC.com
COURSE OBJECTIVESAt the end of this course participants will be able to:
1.) Summarize how hormones ‘work’, including their synthesis, effects, elimination and receptor sites. 2.) Describe the role that cholesterol plays in the Steroid Hormone Pathway. 3.) List the five major Steroid Hormone Groups. 4.) Identify the different hormones associated with each of the major hormone groups. 5.) Explain the role that each hormone plays in the body. 6.) Identify the enzymes that act on each hormone to convert it into the next hormone in the cascade. 7.) Correlate a patient’s lab results to certain disease states associated with that hormone.
COPYRIGHT INFO:
RIGHTSHOLDER
Author: Deborah L. Buckley, MBA, MT (ASCP) © 2011 Continuing Education Unlimited ALL RIGHTS RESERVED
PERMISSIONS Permissions are currently unavailable.
ARTICLE REPRODUCTION This article may not be reproduced for any purpose in any medium. Please refer to the original source documents listed in the Reference section for additional information. Some reference documents are in the Public Domain and can be reproduced if necessary. If sharing this written document with colleagues, please share the original document. One copy may be printed from any online file that you purchased. Unlimited quizzes may be photocopied for sharing purposes only.
COURSE LICENSE INFO:
LABORATORY CA Dept. of Health Services (Agency #): 0001 FL Board Of Clinical Lab Personnel: 50-2256 ASCLS P.A.C.E.® : 511
Our courses are accepted by: AMTIE, ASCP, NCA, CA, FL, LA, ND, NV, MT, RI, TN, WV ** If you do not see your organization, state, or licensing agency listed above it does not mean that the credits will be unacceptable. Most licensing bodies accept credits, so please check directly with them for acceptance of our courses.**
PHLEBOTOMY Most licensing bodies accept credits. Please check with them directly for acceptance of our course credits.
OTHER MEDICAL DISCIPLINES Many medical licensing bodies will accept credits issued by valid licensed providers of other disciplines. Please check directly with the state, agency, or organization that issued your license for acceptance of our credits.

ii www.4CEUINC.com
TABLE OF CONTENTS READ BEFORE COMPLETING MATERIAL ................................................................ ivFREQUENTLY ASKED QUESTIONS ........................................................................ vQUIZ QUESTIONS ................................................................................................. vi INTRODUCTION ..................................................................................................... 1
Hormone Synthesis .............................................................................................. 1Effects ................................................................................................................ 1Steroidogenesis ................................................................................................... 3Steroid Elimination ............................................................................................... 3Steroid Hormone Receptors ................................................................................... 3Steroid Receptor Sites ........................................................................................... 4
CHOLESTEROL ....................................................................................................... 4
Conversion of Cholesterol To Pregnenolone .............................................................. 5Mechanism of action .......................................................................................... 5
STEROID HORMONE GROUPS ................................................................................. 6
Progestagens ....................................................................................................... 6Pregnenolone .................................................................................................... 617α -Hydroxpregnenolone .................................................................................. 7Progesterone .................................................................................................... 717-Hydroxyprogesterone .................................................................................... 9
Mineralocorticoids and Glucocorticoids ..................................................................... 9Corticosterone ................................................................................................. 10Aldosterone ..................................................................................................... 1011-Deoxycortisol .............................................................................................. 11Cortisol ........................................................................................................... 12
Androgens .......................................................................................................... 13Dihydroepiandrosterone .................................................................................... 14Androstenedione .............................................................................................. 14Testosterone .................................................................................................... 15Dihydrotestosterone ......................................................................................... 17
Estrogens ........................................................................................................... 18Estrone ........................................................................................................... 18Estradiol.......................................................................................................... 19Estriol ............................................................................................................. 20
APPENDIX ........................................................................................................... 22REFERENCES ........................................................................................................ 23

iii www.4CEUINC.com
*THIS PAGE INTENTIONALLY LEFT BLANK*

iv www.4CEUINC.com
Thanks for choosing CEUINC for your continuing education needs! We strive to offer you current course material at the most cost effective price. If you have comments or suggestions, be sure to add them to your evaluation – we appreciate them. If you like our courses pass them on to a coworker or friend.
READ BEFORE COMPLETING MATERIAL GENERAL:
1.) Check your reading material to make sure that it contains the correct course(s) you ordered.
2.) Carefully read the material before completing your quiz packet. All answers are within the reading material. With few exceptions, quiz questions typically follow in order of the reading.
3.) Courses must be completed within 1 year of purchase date, unless otherwise specified.
4.) All of your records are available to you on our website for 4 years. If you don’t have a login to access your records, please contact our office and we will give you that information. Please do not create a 2nd profile! 5.) When sharing your materials with a coworker, be sure to pass on both the reading material and the quiz. HOME STUDY COURSES:
1.) Each course should have a corresponding answer sheet(s), course evaluation, and an envelope.
2.) If you have ordered multiple courses, please make sure that you are using the correct answer sheet for that course or course section. The course code will be located on the label of your answer sheet.
3.) After you have completed reading the material, complete the quiz, then fill in the corresponding answer sheet.
4.) Upon completion, send in your answer sheet(s) to our office. Please make copies for your records before sending !
5.) Once we receive your answer sheet in our office we will grade it & mail you back a certificate of completion. Your certificate will arrive in the mail within 4 weeks from the date you mail your answer sheets us. ONLINE COURSES:
1.) Course materials are offered in Adobe pdf documents, which allow multiple options for accessing & saving the material. You can read the document online, print it out for reference, store it on your hard drive, or copy it to a disk. Please remember to save or print the document before completing your quiz. Once you complete your quiz you will be permanently locked out of that record. Per copyright law, you can print one copy of each online course.
2.) Quizzes can be printed out if you’d like to work offline. Once you are done, simply transfer your results to the active, online quiz and click “Score”. You will receive immediate feedback of your results. “SITE-BASED” GROUPS:
1.) Coordinators should mail all “Pay As You Go” answer sheets to our facility as a group once per month.
2.) We mail certificates once per month according to the schedule furnished to the educational coordinator.
3.) Be sure to fill in your course code on the Pay As You Go (PAYG) answer sheets.
4.) If you have the online login to your profile, you may purchase online quizzes rather than mail in an answer sheet. This will allow you to immediately print your certificate of completion and will save time & money.
****Please be sure to make a copy of your answer sheet for your records before mailing**** This safeguards you in the event that your answer sheet gets mishandled during mailing.
Continuing Education Unlimited 6231 PGA Blvd , Ste 104 / #306 Palm Beach Gardens, FL 33418 General Fax: 561-775-4933 / Answer Sheet Only Fax: 561-775-4933 Phone: 561-775-4944 / Web: www.4CEUINC.com
Last Revised 12/09/10

v www.4CEUINC.com
FREQUENTLY ASKED QUESTIONS
Q. What course completion date goes on my certificate? A. The date that we receive your answer sheet in our office. Q. I need my certificate dated on a certain day because of license renewals how can I be sure that this will happen? A. Since your certificate is dated on the day that we receive your answer sheet in the mail, you should always allow adequate mailing time, taking into consideration weekends and holidays when we are not in the office. If you need us to grade a certificate by a certain date you can overnight the answer sheet to us - please use a “trackable” service. Online courses will have the date the course was completed online on the certificate. Q. What score is considered passing? A. A score of 70% or higher is considered a passing grade. In the event that you do not pass on your first attempt, you are allowed a second attempt to score a passing grade. Q. Does your company allow me to fax my answer sheet to your office? A. YES, you may now fax your answer sheet to 561-775-4948. Include a cover sheet with your full name, license number and telephone number. Please only fax to the number listed above and NOT to our general fax #. Q. Can a course be shared with multiple users? A. Yes. If you are sharing materials, one person will buy the “complete course” package and each of the others will purchase an “answer sheet only” or “online quiz only” packet. Please be sure you have the reading material and quiz packet if you’re sharing the materials. Prices are subject to change, please check before ordering. **Combo courses MUST be ordered as a complete unit when ordering for extra people.** Q. How long will it take for my certificate to arrive if I’m sending my answers by mail? A. We can’t give you an exact date when it will arrive because of variations in mail delivery time, however, we ask that you allow 3-4 weeks from the time you mail it to us until your certificate to arrives in your mailbox. Q. May I print out an online course? A. Yes, you may print 1 copy of an online course. Copyright laws do not allow more than one copy to be printed.
Q. Where can I find additional information out about a course? A. Basic course information is located on the course cover. Additional information is located on the 2nd page of each course.
Q. Our facility participates in your educational program. When can we expect our certificates to be processed and mailed back to our site coordinator? A. We have sent a mailing schedule to your coordinator which lists mailing dates your certificates will be mailed back. It’s important that your answer sheets arrive in our office 5 business days prior to our mailing date.
Q. Does CEUINC offer group discounts or group packages? A. Yes. We require at least 5 participants and a person to act as the educational coordinator for the group. Discount amounts depend on the number of participants and the course or package chosen.
****Please be sure to make a copy of your answer sheet for your records before mailing****
This safeguards you in the event that your answer sheet gets mishandled or lost during mailing.
Continuing Education Unlimited 6231 PGA Blvd , Ste 104 / #306 Palm Beach Gardens, FL 33418 General Fax: 561-775-4933 / Answer Sheet Only Fax: 561-775-4933 Phone: 561-775-4944 / Web: www.4CEUINC.com
Last Revised 12/09/10

vi www.4CEUINC.com
QUIZ QUESTIONS
1.) Name the five major steroid hormone groups. A. cholesterol, glucocorticoids, androgens, estrogens, and progestagens B. glucocorticoids, Vitamin D, androgens, estrogens, and progestagens C. glucocorticoids, mineralocorticoids, androgens, estrogens, and progestagens
2.) Steroids are mainly oxidized by cytochrome _____ oxidase enzymes. A. C170 B. P450 C. X950
3.) __________ is the precursor to all other hormones downstream in the steroid hormone cascade. A. Cholesterol B. Progesterone C. DHEA
4.) Pregnenolone is converted directly to ___ other hormones. A. one B. two C. three
5.) On average up to ______ mg of progesterone is produced daily during pregnancy. A. 300-400 B. 550-600 C. 700-800
6.) A ____ sodium diet would cause a low aldosterone level. A. normal B. high C. low
7.) 11-deoxycortisol is converted to cortisol via the enzyme ______________. A. 21 α-hydroxylase B. aromatase C. 11-β-hydroxylase
8.) Plasma cortisol levels undergo a diurnal variation throughout the day, with peaks _______. A. at noon B. between midnight and 4am C. in the early morning around 8am
THE STEROID HORMONE CASCADE Category: Chemistry / Contact Hours: 2 / Course Code: C018
vii www.4CEUINC.com
9.) Normally only <1% of testosterone is free and circulating unbound.
A. True B. False
10.) DHT has a _____ times greater affinity for androgen receptors than testosterone. A. three B. five C. twenty
11.) Uterine fibroids are a symptom of low estradiol levels. A. True B. False
12.) Of the three major estrogen hormones, _____ exerts the weakest affect on the body. A. estrone B. estradiol C. estriol
****END OF QUIZ****
THE STEROID HORMONE CASCADE Quiz - PAGE 2

THE STEROID HORMONE CASCADE COURSE # - C018
1 www.4CEUINC.com
INTRODUCTION
steroid hormone is a steroid that functions as a hormone in the body. Steroid hormones can be placed into five groups based on the receptors to which they bind. The five groups are: glucocorticoids, mineralocorticoids, androgens, estrogens, and progestagens. Although not discussed in this course, it should be noted that Vitamin D derivatives are a sixth closely related hormone group, technically known as a sterols.
HORMONE SYNTHESIS
The natural steroid hormones are generally synthesized from cholesterol in various organs, including the gonads and adrenal glands. These hormone building blocks are known as lipids. Further conversions and catabolism occur in the liver, in other "peripheral" tissues, and in the target tissues and organs themselves. The synthesized hormones can pass through the cell membrane, as they are fat-soluble, and then bind to steroid hormone receptors to bring about rapid changes within the cell. Steroid hormones are generally carried in the blood bound to specific carrier proteins such as sex hormone-binding globulin or corticosteroid-binding globulin.
EFFECTS
Steroids exert a wide variety of effects mediated by slow genomic, as well as, by rapid nongenomic mechanisms. They bind to nuclear receptors in the cell nucleus for genomic actions. Membrane-associated steroid receptors activate intracellular signaling cascades involved in nongenomic actions.
Because steroids and sterols are lipid-soluble, in most cases they can diffuse freely from the bloodstream through the cell membrane and into the cytoplasm of target cells. Once in the cytoplasm, the steroid typically undergoes an enzyme-mediated alteration such as reduction, hydroxylation, or aromatization. Once in the cytoplasm, the steroid binds to its specific receptor, which is a large metalloprotein. Upon steroid binding, many types of steroid receptors dimerize, forming two receptor subunits joining together to form one functional DNA-binding unit. This DNA-binding unit can then enter into the cell nucleus. In some of the known hormone systems, the receptor is associated with a heat shock protein, which is released with the binding of the ligand1. Once in the nucleus, the steroid-receptor-ligand complex binds to specific DNA sequences and induces the transcription of its target genes, exerting its hormonal effect.
1 Ligand: A substance that forms a complex with a biomolecule to serve a biological purpose. In a narrower sense, it is a signal triggering molecule, binding to a site on a target protein.[29]
AA

THE STEROID HORMONE CASCADE COURSE # - C018
2 www.4CEUINC.com
FIGURE 1: Steroid Hormone Cascade
CHOLESTEROL
PREGNENOLONE
PROGESTERONE 17-HYDROXYPROGESTERONE
17-HYDROXYPREGNENOLONE
CORTICOSTERONE
ALDOSTERONE
11-DEOXYCORTISOL
CORTISOL
DHEA
ANDROSTENEDIONE
TESTOSTERONE
DHEA SULFATE (DHEAS)
ESTRONE (E1)
ESTRADIOL (E2)
DIHYDROTESTOSTERONE
ESTRIOL (E3) FIGURE 1 - COLOR KEY PROGESTAGENS:
CORTICOIDS:
ANDROGENS:
ESTROGENS:
It should be noted that there are several hormone cascade models available, each with their own configuration. It’s possible that others may show slightly different pathways and have additional hormones added to the tree. For this course, we are using a basic, straightforward model.
Because of space restriction, this course will focus on the basics of each hormone in the cascade, briefly touch on testing.

THE STEROID HORMONE CASCADE COURSE # - C018
3 www.4CEUINC.com
STEROIDOGENESIS
Steroidogenesis is the process whereby a desired steroid hormone is generated through the conversion of another steroid. The pathway of human steroidogenesis is shown in Figure 1. It should be noted that Figure 1 diagrams the basic, most direct pathways. Appendix A shows a more complex example, including intermediate and alternate pathways that can exist during the process. This course will focus on the basic pathways.
STEROID ELIMINATION
Steroids are mainly oxidized by cytochrome P450 oxidase enzymes. These reactions introduce oxygen into the steroid ring and allow the structure to be broken up by other enzymes to ultimately form bile acids as a final product in most cases. These bile acids can then be eliminated through secretion from the liver into the bile. The expression of this oxidase gene can be upregulated by the steroid sensor PXR when there is a high blood concentration of steroids.[26]
STEROID HORMONE RECEPTORS
Steroid hormone receptors are found on the plasma membrane, in the intracellular fluid known as the cytosol2, and also in the nucleus of target cells. They are generally intracellular receptors (typically cytoplasmic) and initiate signal transduction for steroid hormones which lead to changes in gene expression.
The steroid hormone receptors belong to the steroid and thyroid hormone receptor super-family of proteins. This includes not only the typical receptors for steroid hormones, such as androgen receptors (AR); progesterone receptors (PR); estrogen receptors (ER), but also for thyroid hormone (TR), vitamin D (VDR), retinoic acid (RAR), mineralocorticoids (MR), and glucocorticoids (GR). This large class of receptors is known as the nuclear receptors.
The steroid-family of receptors all have three distinct domains: a ligand-binding domain, a DNA-binding domain and a transcriptional regulatory domain. When these hormone receptors bind ligand they undergo a conformational change that renders them active to recognize and bind to specific nucleotide sequences. These specific nucleotide sequences in the DNA are referred to as hormone-response elements (HREs). When ligand-receptor complexes interact with DNA they alter the transcriptional level of the associated gene, resulting in either activation or repression. Although there is the commonly observed effect of altered transcriptional activity in
2 CYTOSOL: Part of the cytoplasm not held within the organelles

THE STEROID HORMONE CASCADE COURSE # - C018
4 www.4CEUINC.com
response to hormone-receptor interaction, there are family member-specific effects with ligand-receptor interaction.
STEROID PRODUCTION SITES TABLE 1: Hormone Production By Gland/Organ Type HORMONE PRODUCED GLAND/ORGAN Placenta Ovaries Testes Adrenal Progesterone + + + 17-Hydroxyprogesterone + + + + Aldosterone + Cortisol + DHEA + Testosterone + + Estradiol + Estrone + Estriol + +
CHOLESTEROL
*PLEASE NOTE: For purposes of this course, we will only briefly touch on the subject of cholesterol. Cholesterol is a waxy steroid metabolite which regulates the fluidity and permeability of cell membranes. In addition, it is also an important component for manufacturing bile acids, vitamin D, and other steroid hormones. Cholesterol is the principle sterol synthesized in the body.
Cholesterol is carried in the blood by special lipid carriers called lipoproteins. Although there are others, the following are the four main lipoproteins in the body:
• High-Density Lipoprotein (HDL) is known as the "good" cholesterol. Approximately 1/3 to 1/4 of the blood cholesterol in the body is carried by high-density lipoproteins. They are known as “good”
cholesterol because they are thought to carry cholesterol away from the arteries to the liver where the body can eliminate it or make it available to synthesize hormones. Some experts also believe that HDL removes excess cholesterol from arterial plaque, thereby slowing its buildup. Levels of HDL less than 40 mg/dl increase the risk of heart disease therefore HDL levels should be higher than 40 mg/dl to help prevent disease.
• Low-Density Lipoprotein (LDL) is known as "bad" cholesterol. Together with other substances, LDL can form plaque, which can restrict blood flow to your heart or brain. Plaque is a thick hard deposit that narrows the arteries, making them

THE STEROID HORMONE CASCADE COURSE # - C018
5 www.4CEUINC.com
inflexible. Too many low-density lipoproteins (LDL) will cause a build up in the arteries resulting in a condition known as atherosclerosis. For this reason, LDL levels should remain low.
• Very Low Density Lipoprotein (VLDL) molecules are produced by the liver and contain excess triacylglycerol and cholesterol that is not required by the liver for synthesis of bile acids. These molecules contain apolipoprotein B100 and apolipoprotein E in their shell. Increased levels of VLDL cholesterol are thought to reflect the presence of particles called lipoprotein remnants that are intermediate particles on the pathway of conversion of VLDL to LDL. When high levels of VLDL are present, the conversion of VLDL to LDL is slowed and the accumulation of intermediate particles is thought to contribute to the development of atherosclerosis and coronary heart disease.[30]
• Triglycerides are a type of fat in the blood. They're produced in the liver and can also come from certain foods that you eat. Obesity, physical inactivity, cigarette smoking, excess alcohol consumption, and a diet high in carbohydrates (≥60% of the total calories) also contribute to elevated triglycerides. High levels can contribute to the hardening and narrowing of arteries, making it harder for blood to flow. A high triglyceride level often goes hand in hand with a high LDL level and lower HDL level further contributing to heart disease.
One easy way to remember which is referred to as the “good” cholesterol and which is referred to as the “bad” cholesterol, is to remember the following:
• The “H” in HDL = Healthy • The “L” in LDL = Lousy
CONVERSION OF CHOLESTEROL TO PREGNENOLONE Cholesterol is the precursor to all other hormones downstream in the steroid hormone cascade. In order to convert cholesterol to pregnenolone, P450scc, also known as, 20,22-desmolase is needed. This protein is a mitochondrial enzyme. The presence of this enzyme defines whether a cell is steroidogenic or not. Consequently, P450scc is found in all steroid-producing cell types such as theca cells and luteal cells in the ovary, Leydig cells in the testis, and various cell types in the adrenal cortex.
MECHANISM OF ACTION
P450scc catalyzes the conversion of cholesterol to pregnenolone in three monooxygenase reactions. They involve 2 hydroxylations of the cholesterol side-chain, which generate, first, 22R-hydroxycholesterol and then 20α,22R-dihydroxycholesterol. The final step cleaves the bond between carbons 20 and 22, resulting in the production of pregnenolone and isocaproic acid.[31]

THE STEROID HORMONE CASCADE COURSE # - C018
6 www.4CEUINC.com
STEROID HORMONE GROUPS
There are five main hormone groups all derived initially from cholesterol. Each group has a different function within the body.
PROGESTAGENS The progestagens are a group of hormones made up of a 21carbon skeleton (C21), also called a pregnane skeleton. Although they are also present at other phases in the menstrual cycle, progestagens are named for their function in maintaining pregnancy meaning “pro-gestational”. In addition to maintaining pregnancy, they are also known for their antiestrogenic properties. After cholesterol, Progestagens are precursors to all other hormones groups downstream.
PREGNENOLONE
As mentioned earlier, pregnenolone is synthesized in the body directly from cholesterol through hydroxylation and is the first step in steroidogenesis. Cytochrome P450scc (scc - side chain cleavage), which is located in the mitochondria, performs this hydroxylation step.[9]
Pregnenolone is known as “The Mother Hormone”. (It should be noted here that some literature may refer to
DHEA as “The Mother Hormone”, although technically it’s pregnenolone.)
CONVERSION: Pregnenolone is converted to both progesterone via 3 β-hydroxysteroid dehydrogenase and to 17-hydroxypregnenolone via the enzyme 17 α-hydroxylase.[9]
Pregnenolone is considered to be a neurosteroid (or neurotransmitter) and is therefore found in high concentrations in the brain. Neurosteroids affect synaptic functioning, are neuroprotective, and help to enhance myelinization.[9] Supplementation with pregnenolone has been reported to increase brain function, promote better memory, give greater clarity, improve energy, improve vision, and increase libido. Currently, there have been limited trials and studies performed to understand the safety or scientific benefits of pregnenolone supplementation however.
TESTING: Although pregnenolone tests are available, levels are rarely ordered. Typically when testing is done many times it’s by physicians that prescribe bioidentical hormone therapy or practice alternative medicine.
LOW LEVELS: As with other hormones, ageing can cause a decrease in levels. Low levels of pregnenolone can also manifest as low levels of other hormones down the cascade.
HIGH LEVELS: Excessive supplementation can cause elevated pregnenolone levels.

THE STEROID HORMONE CASCADE COURSE # - C018
7 www.4CEUINC.com
17α ‐HYDROXPREGNENOLONE 17α-hydroxypregnenolone is a progestagen that is sythesized by the hydroxylation of pregnenolone. The hydroxylation occurs by the mitochondrial cytochrome P450 enzyme 17α-hydroxylase that is present in both the adrenal glands and the gonads. CONVERSION: 17α-hydroxypregnenolone can be further converted to both 17α-hydroxyprogesterone and DHEA. (Figure 1) It’s converted to 17α-hydroxyprogesterone by 3-β-hydroxysteroid dehydrogenase and to DHEA by 17,20 lyase. As previously stated, both of these enzyme activities are mediated by a cytochrome P450 complex.[11]
As with pregnenolone, there is some evidence that 17α-hydroxypregnenolone may have activity as a neurohormone. [10]
As a person ages, their levels tend to decline. Peak levels of are typically reached at the end of puberty and during pregnancy.
PROGESTERONE
Progesterone is produced by the ovaries of menstruating women during the second two weeks of the menstrual cycle, in small amounts by the adrenal glands, and by the placenta during pregnancy. After menopause, the majority of progesterone is produced by the adrenal glands. On average, about 20-25 mg of progesterone is produced per day during a woman's menstrual cycle and up to 300-400 mg is produced daily during pregnancy. After cholesterol and pregnenolone, progesterone is a precursor to most steroid hormones and performs a myriad of different functions in the body.
Progesterone’s main function is to stabilize the endometrial lining of the uterus in preparation for implantation of a fertilized egg. Elevated levels of progesterone help to maintain a healthy pregnancy. When pregnancy does not occur, the uterus is signaled to shed the lining through menstruation and the monthly cycle starts over again.
TESTING: Serum or Plasma. **TESTING INFORMATION GIVEN IN THIS DOCUMENT IS FOR GENERAL REFERENCE ONLY. PLEASE CHECK WITH YOUR LAB OR REFERENCE FACILITY FOR STORAGE AND TRANSPORT REQUIREMENTS FOR ALL TESTING LISTED IN THIS COURSE.**
DECREASED LEVELS: Levels can be suppressed with dexamethasone inhibition.
ELEVATED LEVELS: Elevated levels can be found in patients with idiopathic hirsutism, during the follicular phase of the menstrual cycle, external ACTH stimulation, 3-β-hydroxylase enzyme deficiency, and 17,20-lyase enzyme deficiency.

THE STEROID HORMONE CASCADE COURSE # - C018
8 www.4CEUINC.com
In addition to preparing the body for pregnancy, progesterone also plays a role in brain function through mood enhancing and antidepressant effects and for that reason is often called the “feel good hormone”. When levels are optimal in the body, a feeling of well being and calm can be felt. Recent studies have shown that progesterone may also play a role in the health of the nervous system.
CONVERSION: Progesterone is converted to both 17 α-hydroxyprogesterone and corticosterone downstream. Progesterone is converted to 17 α-hydroxyprogesterone by the enzyme 17 α-hydroxylase. Progesterone is also converted to corticosterone by first being converted to the intermediate product deoxycorticosterone via the enzyme 21 α-hydroxylase and then deoxycorticosterone is finally converted to corticosterone by 11 β-hydroxylase.
Symptoms of low progesterone: Symptoms of excess progesterone:
Allergy symptoms Arthritis symptoms Anxiety Autoimmune disorders can be triggered Irregular or heavy menstrual bleeding PMS, moods swings & irritability Bloating Cervical dysplasia Menstrual cramping Uterine fibroids and fibrocystic breasts Insomnia Weight gain
Dizziness Somnolence or sleepiness Bloating Increased yeast infections
Progesterone levels may be ordered to:
• Establish the presence of a functioning corpus lutem or luteal cell function • Help pinpoint ovulation • Help monitor placental function during pregnancy
TESTING: Serum is collected for Progesterone measurement in either a red top tube or a barrier gel tube. A Progesterone test should not be added to a barrier gel tube that was collected 24 hours or more prior, as Progesterone binds to the gel causing decreased values.
DECREASED LEVELS: Decreased levels are associated with amenorrhea, anovulatory menstrual cycles, fetal death, pending miscarriage, and gonadal agenesis.
ELEVATED LEVELS: Levels increase sharply during the luteal phase of the menstrual cycle. The level also increases from 9 to 32 weeks of pregnancy. Elevated levels are also seen in ovarian and adrenal tumors and hormone replacement therapy.

THE STEROID HORMONE CASCADE COURSE # - C018
9 www.4CEUINC.com
17‐HYDROXYPROGESTERONE
17-Hydroxyprogesterone (17-OHP) is a 21 carbon steroid hormone produced during the synthesis of glucocorticoids. It can be synthesized via two pathways in the hormone cascade. In the first pathway, 17-hydroxyprogesterone is synthesized from progesterone through the enzyme 17 α-hydroxylase and in the second pathway, it is synthesized from 17-hydroxypregnenolone via 3-β-hydroxysteroid dehydrogenase.
CONVERSION: 17-OHP is converted to 11-desoxycortisol via the enzyme 21 α-hydroxylase.
Low levels of 17-OHP fail to support healthy fetal development and growth and often cause preterm delivery and low birth weight. Elevated levels are seen in congenital adrenal hyperplasia.
17-Hydroxyprogesterone levels may be ordered to:
• Monitor cortisol replacement therapy • Test for congenital adrenal hyperplasia (CAH), when measured along with cortisol
and androstenedione[35] • Evaluate infertility and problem pregnancies • Evaluate females for hirsutism • Monitor ovarian or adrenal neoplasms
MINERALOCORTICOIDS AND GLUCOCORTICOIDS Mineralocorticoids regulate minerals such as sodium, potassium, and hydrogen. Mainly, these hormones balance mineral levels to maintain water balance in and around cells. Acting mostly in the kidney, colon and salivary glands, they direct cells to retain sodium while excreting potassium and hydrogen ions in the urine. When sodium is
TESTING: This test has several acceptable samples and testing methods available. Samples include serum collected in a non-barrier red top tube, plasma: lavender top (EDTA), green top (lithium or sodium heparin), and urine (24 hr collection or random sample).
DECREASED LEVELS: Decreased levels are associated miscarriage, preterm delivery, and low birth rate[34].
ELEVATED LEVELS: Serum levels are elevated in congenital adrenal hyperplasia (CAH), urine levels are seen in polycystic ovarian disease, idiopathic hirsutism, and 21-α-hydroxylase deficiency.

THE STEROID HORMONE CASCADE COURSE # - C018
10 www.4CEUINC.com
retained, water is also retained, increasing the total amount of circulating blood and raising blood pressure. Blood pressure sensors in the kidney help to switch mineralocorticoid release on or off so that the right balance is maintained.[3] In short, mineralocorticoids help to maintain blood volume and control renal excretion of electrolytes.[26]
Glucocorticoids are named for their role in releasing glucose. These hormones affect every system of the body and guide fundamental processes associated with converting sugar, fat, and protein stores to useable energy; inhibiting swelling and inflammation; and suppressing immune responses.[3] In short, glucocorticoids regulate many aspects of metabolism and immune function.
CORTICOSTERONE
Corticosterone is a 21 carbon hormone produced by the adrenal cortex via the progesterone pathway. Progesterone is converted to corticosterone first by conversion to the intermediate product deoxycorticosterone via the enzyme 21 α-hydroxylase and then on to corticosterone by 11 β-hydroxylase.
CONVERSION: Corticosterone is converted to aldosterone by aldosterone synthase.
Classed as a glucocorticoid, corticosterone helps to regulate the conversion of amino acids into carbohydrates, glycogen by the liver, and also helps to stimulate glycogen formation in the tissues.[42] It is produced in response to stimulation by pituitary ACTH.
When used in conjunction with 11-deoxycortisol it may be useful in the measurement of:
• 11 β-hydroxylase deficiency
ALDOSTERONE
Aldosterone is a mineralocorticoid that acts on the kidneys to regulate sodium and potassium levels in the body, which in turn help to regulate blood pressure and fluid balance in the body.
Aldosterone is synthesized in the adrenal cortex from the conversion of corticosterone via the enzyme aldosterone
TESTING: Methodology: Liquid Chromatography-Tandem Mass Spectrometry (LC-MS/MS). Specimen: Serum.
DECREASED LEVELS: No data available
ELEVATED LEVELS: No data available.

THE STEROID HORMONE CASCADE COURSE # - C018
11 www.4CEUINC.com
synthase. Its secretion is mediated mainly by angiotensin II but also by adrenocorticotrophic hormone (ACTH) and local potassium levels.
Renin normally stimulates the adrenal gland to release aldosterone. High levels of both renin and aldosterone can be found when the body is trying to conserve fluid and salt in the body, as seen in secondary hyperaldosteronism due to heart or kidney disease. In the event of an aldosterone producing tumor, the aldosterone levels will be high, while the renin levels low, as is seen in Conn’s syndrome.
Like cortisol, the secretion of aldosterone has a diurnal rhythm.
Aldosterone levels can be affected by positional changes. Serum aldosterone levels will typically be higher if you are standing or sitting up prior to testing[40]. Some labs may request that the patient to be ambulatory in the 30 minutes prior to testing if the patient is able. Serum reference ranges exist for both ambulatory and non-ambulatory patients. Dietary sodium also may have an effect on the results of the test. Some physicians prefer to order the 24 hour urine aldosterone because it’s not affected by diurnal and postural variations.
Symptoms of an elevated aldosterone level include high blood pressure, muscle cramps and weakness, low potassium levels, and numbness of tingling in the hands. Decreased aldosterone levels in the body will result in a drop in both blood volume and blood pressure[41].
11‐DEOXYCORTISOL
11-deoxycortisol, also referred to as Compound S, is the immediate precursor to cortisol and follows the same catabolic pathways[11]. It is synthesized from 17-
TESTING: Serum or 24 hour urine
LOW LEVELS: Low levels can be seen in Addison’s disease, congenital adrenal hyperplasia (CAH), a very high sodium diet, and hyporeninemic hypoaldosteronism which causes impaired renin release from the kidney[39]. Acquired hypoaldosteronism can be caused by heparin administration, as well as, persistently hypotensive or critically ill patients with sepsis, peritonitis, pneumonia, and liver failure where low aldosterone levels are seen with elevated plasma renin activity.
ELEVATED LEVELS: Elevated levels can be seen in primary aldosteronism, Bartter syndrome, secondary to heart, liver, or kidney disease, certain adrenal tumors (Conn’s syndrome), and a very low sodium diet[39]. Secondary hyperaldosteronism may be seen with cirrhosis, toxemia of pregnancy, and congestive heart failure[11].

THE STEROID HORMONE CASCADE COURSE # - C018
12 www.4CEUINC.com
hydroxyprogesterone by the enzyme 11-β-hydroxylase and is considered a glucocorticoid.
CONVERSION: 11-deoxycortisol is converted to cortisol via the enzyme 11-beta-hydroxylase[38].
Conversion of 11-deoxycortisol is inhibited by metyrapone, which acts on 11-β-hydroxylase (see test info below). 11-deoxycortisol is typically increased when ACTH levels are increased (Cushing disease or ACTH producing tumors) or in 11-β-hydroxylase deficiency.
11-deoxycortisol may be ordered to:
• Diagnose patients with 11-β-hydroxylase deficiency (causes congenital adrenal hyperplasia)
• Diagnose primary adrenal insufficiency from adrenal failure, as part of a metyrapone testing workup.
• Diagnose secondary adrenal insufficiency caused by a hypothalmic-pituitary ACTH deficiency
CORTISOL
Cortisol is a glucocorticoid that is produced by the adrenal glands in response to stress. Its primary functions are reducing inflammation, moderating or suppressing the immune system, and aiding in fat, protein, and carbohydrate metabolism. It also helps to increase glucose through gluconeogenesis and decrease bone formation (osteogenesis). During weeks 30-32 of pregnancy cortisol initiates production of fetal lung surfactant to help promote maturation of lung tissue[36].
TESTING: Methodology: Typically performed as Liquid Chromatography-Tandem Mass Spectrometry (LC-MS/MS). Specimen: Serum or plasma.
DECREASED LEVELS: Decreased levels seen after metyrapone testing indicate probable adrenal insufficiency.
ELEVATED LEVELS: Serum levels are elevated in congenital adrenal hyperplasia (CAH), 11-β-hydroxylase deficiency[38] and when ACTH levels are elevated.
METYRAPONE TEST: Metyrapone is a drug used in the diagnosis of adrenal insufficiency and occasionally in the treatment of Cushing's syndrome (hypercortisolism). Metyrapone blocks cortisol synthesis by inhibiting steroid 11β-hydroxylase. This stimulates ACTH secretion, which in turn increases plasma 11-deoxycortisol levels. When excess ACTH secretion is the cause of hypercortisolism, the metyrapone test helps clarify if the source of the ACTH is pituitary or ectopic (non-pituitary).

THE STEROID HORMONE CASCADE COURSE # - C018
13 www.4CEUINC.com
90-97% of circulating cortisol is bound to cortisol-binding globulin (CBG). Plasma cortisol levels undergo a diurnal variation throughout the day, with peaks in the early morning around 8am and reaching its lowest level typically between midnight and 4am (or 3-5 hours after the onset of sleep).
Changes in cortisol concentrations have been seen with abnormal ACTH levels, Cushing’s syndrome, clinical depression, temperature extremes, psychological stress, and physiological stressors, such as hypoglycemia, surgery, disease, fever, trauma, physical exertion, pain, and fear.
Symptoms of low cortisol: Symptoms of excess cortisol:
Joint or muscle pain Weakness Low blood pressure Changes in mood Inability to handle stress Shakiness Skin darkening (incl. beneath eyes) Change in sleep patterns
Fluid retention Immune suppression Thinning skin & bone loss
Symptoms of chronic elevations:
Weight gain, especially in the waist Fatigue Depression Anxiety
ANDROGENS The androgens are a group of hormones made up of a 19 carbon skeleton. Androgens are primarily known for masculine characteristics, although they are present in both males and females in varying degrees. Androgens are the precursors to all estrogen hormones in both males and females. The androgens synthesized in the adrenal cortex, such as DHEA and DHEAS, function as steroid precursors to the androgens and estrogens downstream including testosterone. All androgens play a role in the development of male characteristics (including sperm production), inhibition of fat deposition, muscle mass, and brain function.
TESTING: Specimens: 1.) Serum – 8AM & 4PM specimens should be collected to check diurnal variation, although random levels can be run 2.) 24 hour urine or 3.) Saliva testing can also be used to check levels throughout a 24 hour period (usually 4 specimens).
LOW LEVELS: Low levels of cortisol congenital adrenal hyperplasia due to 11-β-hydroxylase deficiency, Addison’s disease, and pituitary or hypothalamic insufficiency.
ELEVATED LEVELS: Elevated levels of cortisol are seen with severe stress, sepsis, Cushing’s syndrome, 21-hydroylase deficiency, pregnancy, oral contraceptives and prescription steroidal anti-inflammatory therapy (prednisone, methylprednisolone, etc).

THE STEROID HORMONE CASCADE COURSE # - C018
14 www.4CEUINC.com
DIHYDROEPIANDROSTERONE
Dihydroepiandrosterone, also known as DHEA, is secreted predominately by the adrenal glands. DHEA itself is produced from cholesterol by way of pregnenolone. Cholesterol is first converted to pregnenolone by the enzyme P450. CYP17A1 then converts pregnenolone to 17α-Hydroxypregnenolone and finally to DHEA.[7] DHEA serves as a direct precursor to androgens and estrogens.
In the body, DHEA levels peak naturally in the 20s and begins a gradual decline starting in the 30s. Because of this natural decline, there has been great interest in DHEA’s role in the ageing process. It’s been noted that by the time we reach 80 years of age, there is only 10%-20% of the levels that were present in our 20s. DHEA supplementation has been shown to be beneficial with boosting the immune system, adrenal insufficiency, depression, treating systemic lupus erythematosus, etc.
CONVERSION: DHEA is converted to androstenedione by the enzyme 3-β-hydroxysteroid. DHEA also has a sulfated form known as DHEAS. Conversion to DHEAS takes place by sulfotransferase primarily in the adrenal glands, the liver, and small intestine. In the blood, most DHEA is found as DHEAS, so DHEAS is measured during blood testing.
Symptoms of low DHEA: Symptoms of excess DHEA:
Decreased immune function Decreased libido Joint pain Depression Increase in autoimmune diseases
Aggressive behavior Oily skin Increased facial hair Adult acne Heart palpitations
ANDROSTENEDIONE
Androstenedione is a 19 carbon steroid hormone that is produced in the adrenal glands, ovaries, and testes. It’s an ‘intermediate’ hormone that converts downstream to the hormones testosterone and estrone.
TESTING: Serum is collected for DHEAS measurement.
LOW LEVELS: In addition to age, low DHEAS levels have also been seen in certain diseases states, such as, anorexia, end-stage kidney disease, Addison disease, type-2 diabetes, AIDS, adrenal insufficiency, cancer, etc. Low levels may also be seen in adrenal dysfunction or hypopituitarism.
ELEVATED LEVELS: Elevated levels of DHEAS have been seen in adrenocortical tumors, adrenal cancers, adrenal hyperplasia, hirsutism, athletes (exercise increases DHEA), newborns (drops shortly after birth), and excess supplementation.

THE STEROID HORMONE CASCADE COURSE # - C018
15 www.4CEUINC.com
Androstenedione is synthesized from dihydroepiandrosterone (DHEA) by the enzyme 3-β-hydroxysteroid. Some literature also shows a direct pathway of synthesis from 17-hydroxyprogesterone via the enzyme 17,20 lyase.
Although primarily thought of as a ‘male hormone’, in females androstenedione is released into the bloodstream by the theca cells of the ovary where they provide the building blocks needed for conversion to estrone by the granulosa cells. A marked diurnal variation exists, with a peak around 7 AM and a low around 4 PM. Levels rise sharply after puberty to peak at about age 20. An abrupt decline occurs after menopause[11].
Several years back, androstenedione was manufactured and used as a dietary supplement called Andro. Since it was a legal substance that helped to boost testosterone levels, many athletes used it for performance boosting. A side effect of this supplement was often excess estrogen production that often had to be blocked by taking aromatase inhibitors. In March of 2004 the Anabolic Steroid Control Act of 2004 was introduced and in April 11, 2004 the FDA banned the sale of Andro in the United States, citing that the drug poses significant health risks.
CONVERSION: Androstenedione can be converted to two other hormones downstream. First, androstenedione is converted via 17-β-hydroxysteroid dehydrogenase to testosterone. It can also be converted to estrone by aromatase.
TESTOSTERONE
Testosterone is an anabolic hormone that is synthesized from androstenedione via the enzyme 17-β-hydroxysteroid dehydrogenase.
Testosterone is essential for building and maintaining skin, muscles, and bone. It also plays a role in creating energy, maintaining brain function, and immune system regulation.
In men, over 95% of the testosterone is produced by the Leydig cells of the testes. It is also synthesized in much smaller quantities by the thecal cells of the ovaries, by the placenta, and in both sexes by the zona reticularis of the adrenal cortex. Like most
TESTING: Serum or plasma specimens are required for use in Liquid Chromatography/Tandem Mass Spectrometry (LC/MS-MS)
LOW LEVELS: Lower levels can be seen during ageing in menopause and andropause.
ELEVATED LEVELS: Elevated levels can be seen in approximately 60% of hirsutism cases (including Stein-Leventhal Syndrome), Cushing syndrome, ectopic ACTH-producing tumors, certain ovarian tumors, and very elevated levels are seen in congenital adrenal hyperplasia due to C21-hydroxylase deficiency.

THE STEROID HORMONE CASCADE COURSE # - C018
16 www.4CEUINC.com
hormones, testosterone is supplied to target tissues in the blood where much of it is transported bound to the plasma protein, sex hormone binding globulin (SHBG).
In general, testosterone circulates almost entirely bound to transport proteins, such as sex hormone binding globulin (SHBG). Normally only <1% is free and circulating unbound.
CONVERSION: Testosterone is converted to both estradiol and dihydrotestosterone. 5-α-reductase converts testosterone to dihydrotestosterone, while aromatase converts testosterone to estradiol.
There are currently drugs on the market that block the conversion of testosterone to estradiol and dihydrotestosterone. 5 α-reductase inhibitors, such as Propecia, Proscar, and Avodart are used to impair the conversion of testosterone to dihydrotestosterone. These medications are prescribed in cases of mild to moderate benign prostatic hyperplasia (BPH), androgenic alopecia, and prostate cancer. Saw Palmetto is an example of a natural 5 α-reductase inhibitor. Aromatase inhibitors for blocking conversion to estradiol include Arimidex and Femara and are prescribed for preventing and stalling postmenopausal breast and ovarian cancers.
Symptoms of low testosterone: Symptoms of excess testosterone:
Low libido Symptoms of chronically low levels:
Fatigue Erectile dysfunction Depression Problems with memory Vaginal dryness (also related to estrogen) Decreased muscle mass
Loss of hair on scalp Oily skin Increased body & facial hair Adult acne Increased muscle mass Irritability or aggression
Testosterone levels may be ordered to assess:
• Erectile dysfunction • Infertility • Hormone replacement therapy
TESTING: Specimen: Serum.
LOW LEVELS: Low levels can be seen during ageing, increased cortisol levels through the suppression of ovarian and testicular production, hypogonadism, and hypopituitarism.
ELEVATED LEVELS: Elevated levels can be seen in overproduction by the ovaries, testes, and adrenal glands, supplementation of testosterone or DHEA, and in polycystic ovarian syndrome (PCOS) in premenopausal women.

THE STEROID HORMONE CASCADE COURSE # - C018
17 www.4CEUINC.com
DIHYDROTESTOSTERONE
Dihydrotestosterone (DHT) is an androgen, synthesized primarily in the prostate gland, testes, hair follicles, and adrenal glands by the enzyme 5α-reductase by means of reducing the 4,5 double-bond of the hormone testosterone.
In men, approximately 5% of testosterone undergoes 5α-reduction to form the more potent androgen, dihydrotestosterone. DHT has a three times greater affinity for androgen receptors than testosterone and has 15-30 times greater affinity than adrenal androgens. During embryogenesis DHT has an essential role in the formation of the male external genitalia, and in the adult DHT acts as the primary androgen in the prostate and hair follicles.
An example illustrating the significance of DHT for the development of secondary sex characteristics is the congenital 5-α-reductase (5-AR) deficiency which can result in pseudohermaphroditism. This condition results in underdeveloped male genitalia and prostate. These individuals are often raised as girls due to their lack of conspicuous male genitalia. In the onset of puberty, although their DHT levels remain very low, their testosterone levels elevate normally. Their musculature develops like that of other adults. After puberty, men with this condition have a large deficiency of pubic and body hair, and no incidence of male pattern baldness.
Unlike other androgens such as testosterone, DHT cannot be converted by the enzyme aromatase to estradiol. Therefore, it is frequently used in research settings to distinguish between the effects of testosterone caused by binding to the androgen receptor and those caused by testosterone's conversion to estradiol and subsequent binding to estrogen receptors.
DHT is the primary contributing factor in male pattern baldness, however, female hair loss is more complex, and DHT is only one of several possible causes. Women with increased levels of DHT may develop certain androgynous male secondary sex characteristics, including a deepened voice and facial hair. In males, DHT plays a role in the development and exacerbation of benign prostatic hyperplasia, as well as prostate cancer, by enlarging the prostate gland. Prostate growth and differentiation are highly dependent on sex steroid hormones, particularly DHT.
TESTING: Specimen: Serum is the specimen of choice, although plasma is acceptable.
LOW LEVELS: Low levels can be seen in patients taking 5α-reductase inhibitors, and those with a 5α-reductase deficiency.
ELEVATED LEVELS: Elevated levels can be seen when there are elevations of other androgens up stream in the cascade, whether the elevation occurs naturally or through supplementation.

THE STEROID HORMONE CASCADE COURSE # - C018
18 www.4CEUINC.com
ESTROGENS Estrogens (or oestrogens) are a group of steroidal hormones with an 18 carbon structure. The estrogen hormone group is made up of the three major hormones estrone, estradiol, and estriol. Although estrogen is produced in both males and females, it is the primary hormone group found in females especially during the reproductive years. In the body estradiol is the most abundant making up 60-80% of the circulating estrogens, while estrone and estriol each make up between 10-20%.
In females, estrogens are produced primarily in the ovary by conversion of testosterone and androstenedione via the enzyme aromatase and by the placenta during pregnancy. Some estrogens are also produced in smaller amounts in other tissues of the body such as, adipose tissue (fat cells), the liver, adrenal glands, testes, and breast tissue. In males, estrogen is secreted in small amounts by the testes and the adrenals.
In women, estrogens promote the development of female reproductive characteristics, such as enlargement of the breasts, thickening of the endometrium and regulation of the menstrual cycle. In males, estrogen also plays a role in reproductive development of the testes and sperm, although testosterone still remains the primary male hormone. Since estrogen receptors are found throughout the body, in addition to reproductive characteristics, estrogen also plays a role in metabolism, muscle & fat development, maintenance of skin and blood vessel integrity, bone resorption, coagulation, lipid metabolism, etc.[16]
In females there should be a proper ratio of estrogens to progesterone. If the ratio is out of balance or too much estrogen exists in the body, a syndrome known as estrogen dominance can appear. Because hormones need to work in proper balance with one another, this syndrome can cause negative health effects for women, such as anxiety, weight gain, migraines, irregular bleeding, etc.[18]
Most of the estrogens are metabolized in the liver by cytochrome P-450 enzymes. Although the majority of estrogen metabolites are excreted from the body through bile, small amounts are excreted in the urine and some also get reabsorbed from the digestive tract back into the serum. Patients suffering from liver disease or other situations that cause a toxic liver will hinder clearance and metabolism of estrogen and estrogen metabolites.
ESTRONE
Estrone, written as E1 or oestrone, is an estrogenic hormone mainly secreted from the ovaries. Estrone is synthesized from androstenedione by aromatase. CONVERSION: Estrone is converted to estradiol (and back
again when necessary) by 17 α-hydroxylase. Estrone can also be converted to estriol by 16 α-hydroxylase.

THE STEROID HORMONE CASCADE COURSE # - C018
19 www.4CEUINC.com
In general, estrone is the least abundant of the three estrogen hormones in the body until a woman enters into menopause. In post-menopausal women, however, it is the primary estrogen in the body and is mainly stored in fat cells. When converted to its sulfated form, it serves as a reservoir for conversion to estradiol and estriol as needed.
Estrone levels may be ordered to:
• Evaluate postmenopausal vaginal bleeding due to peripheral conversion of androgenic steroids.[11]
ESTRADIOL
Estradiol, also written as E2 or oestradiol, is the most potent of the estrogen hormones. In women it is produced in the ovaries and to a lesser degree from the adrenal glands. In males it’s produced in small amounts in the testes and adrenal glands. Synthesis of estradiol takes place through the conversion of both testosterone and estrone.
Estradiol binds well to both estrogen receptors ERα, and Erβ throughout the body. In plasma, estradiol is largely bound to sex hormone-binding globulin (SHBG) and also albumin to a lesser extent[24], therefore only a fraction is freely available and biologically active.
Symptoms of low estradiol: * Symptoms of excess estradiol:
Hot flashes Bone loss Night Sweats Vaginal dryness Sleep disturbances Skin changes – thinning & dryness Cognitive changes including foggy
thinking, inability to concentrate Heart palpitations Irritability
Uterine fibroids & fibrocystic breasts Heavy menstrual bleeding Water retention Weight gain in the hips Irritability & anxiety
* Excess estradiol is usually present along with low progesterone levels and referred to as “estrogen dominance”.
TESTING: Specimen - Serum or plasma.
LOW LEVELS: Low levels can be indicative of aromatase deficiency, and hypogonadism.
ELEVATED LEVELS: Associated with increased levels of androgens and their peripheral conversion[11], obesity[12], menopause, pregnancy, luteal phase of menstrual cycle. An increase in the estrone to estradiol ratio may be indicative of menopause.[12]
THE STEROID HORMONE CASCADE COURSE # - C018
20 www.4CEUINC.com
ESTRIOL
Estriol, also known as E3, is produced from both estrone and estradiol conversion in non-pregnant females, although the majority comes from estradiol.[23]
Of the three major estrogen hormones, estriol exerts the weakest affect on the body, with some studies showing that its effects are 1000 times weaker on breast tissue than
estradiol.[33] In addition to conversion from estradiol and estrone, it is also produced in significant quantities during pregnancy from the placenta and helps to maintain a healthy pregnancy. In the placenta, it is synthesized from 16-α-hydroxydehydroepiandrosterone of fetal origin. During pregnancy, estriol is produced in much higher quantities than both estrone and estradiol. Estriol is excreted from the body through the kidneys.
In general, estriol is the least studied and least understood of the major estrogen hormones. One of only a few published studies came from H.M. Lemmon in 1966 who reported his findings in the Journal of the American Medical Association. In the study, Dr. Lemmon showed that women who had been diagnosed with breast cancer had lower levels of estriol as compared to women without breast cancer, who had naturally higher levels. Subsequent studies have yielded varying results on this theory.
In receptor binding studies, it’s been shown that estriol has a relatively low binding
TESTING: Specimen - serum. Estradiol levels fluctuate greatly during the monthly menstrual cycle in women of reproductive age. In menopausal women, estradiol levels typically remain consistently low. Levels are routinely monitored during IVF cycles.[11]
LOW LEVELS: Low levels of estradiol can be seen in several situations including menopause, anovulatory cycles (no ovulation), birth control supplementation, surgical removal of the ovaries (oophorectomy)[14] , and aromatase deficiency.
ELEVATED LEVELS: In women, elevated levels can occur due to excessive production of androgens (which are converted to estradiol), birth control supplementation or bioidentical hormone replacement therapy (HRT), slow clearance from the body due to a sluggish liver[14], primary or secondary ovarian hyperfunction, ovulation induction during IVF[12], and increased body fat (estradiol is formed from estrone though aromatase). In males, elevated levels are seen in gynecomastia (increased breast tissue), increased body fat, excessive use of alcohol, or use of certain prescription drugs, such as, spironolactone.[11]
Extremely elevated levels are seen in certain glandular tumors and germ cell tumors.[11]

THE STEROID HORMONE CASCADE COURSE # - C018
21 www.4CEUINC.com
affinity for endometrial estrogen receptors at approximately 10%, a normal binding affinity for estrogen receptors in the breast, and a high binding affinity for estrogen receptors in the vagina. It’s thought that estriol may exhibit anticancer affects by occupying the estrogen receptors in breast tissue, thereby blocking the carcinogenic effects that estradiol and estrone can exhibit. Since estriol has a high affinity for estrogen receptors in the vagina, it’s used most often in post menopausal women to treat vaginal dryness and tissue atrophy.
It should be noted that Asian women and women who eat a mainly vegetarian diets have higher levels of estriol, as well as a lower incident of breast cancer.
Estriol levels may be ordered:
• To establish a level in a healthy woman as part of a fractionated estrogen panel. • As a series to monitor a trend in a high risk pregnancy. • To evaluate fetal distress, or placental function when a patient is exhibiting pre-
eclampsia, diabetes, Rh immunization, or a hydatidiform mole.
TESTING: Serum or urine (check with your lab or reference lab).
LOW LEVELS: Unconjugated estriol is measured as part of a “quad” test for Down syndrome, neural tube defects, adrenal abnormalities, and in a living anencephalic fetus. Single values may be low in cases of placental sulfatase deficiency, patients living in high altitudes, anemia, severe liver disease, and a variety of medications.
ELEVATED LEVELS: Multiple pregnancy, hydrops fetalis, and with oxytocin use.

THE STEROID HORMONE CASCADE COURSE # - C018
22 www.4CEUINC.com
APPENDIX
APPENDIX 1: COMPLETE EXAMPLE OF STEROID HORMONE CASCADE INCLUDING INTERMEDIATE HORMONES AND ENZYMES
THE STEROID HORMONE CASCADE COURSE # - C018
23 www.4CEUINC.com
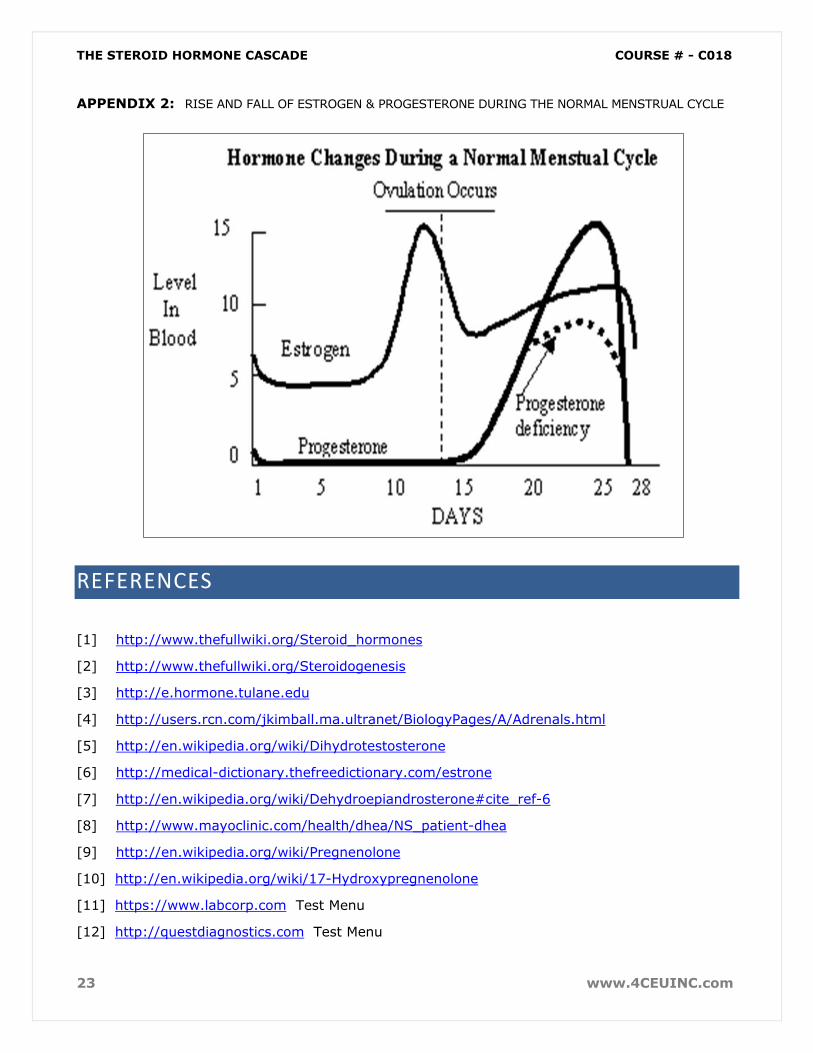
APPENDIX 2: RISE AND FALL OF ESTROGEN & PROGESTERONE DURING THE NORMAL MENSTRUAL CYCLE
REFERENCES
[1] http://www.thefullwiki.org/Steroid_hormones
[2] http://www.thefullwiki.org/Steroidogenesis
[3] http://e.hormone.tulane.edu
[4] http://users.rcn.com/jkimball.ma.ultranet/BiologyPages/A/Adrenals.html
[5] http://en.wikipedia.org/wiki/Dihydrotestosterone
[6] http://medical-dictionary.thefreedictionary.com/estrone
[7] http://en.wikipedia.org/wiki/Dehydroepiandrosterone#cite_ref-6
[8] http://www.mayoclinic.com/health/dhea/NS_patient-dhea
[9] http://en.wikipedia.org/wiki/Pregnenolone
[10] http://en.wikipedia.org/wiki/17-Hydroxypregnenolone
[11] https://www.labcorp.com Test Menu
[12] http://questdiagnostics.com Test Menu

THE STEROID HORMONE CASCADE COURSE # - C018
24 www.4CEUINC.com
[13] http://labtestsonline.org Test Menu
[14] www.zrtlabs.com “Understanding Hormone Highs and Lows”
[15] http://www.endotext.org/male/male17/maleframe17.htm
[16] http://en.wikipedia.org/wiki/Estrogen
[17] http://en.wikipedia.org/wiki/Estrone
[18] http://www.womentowomen.com/menopause/estrogendominance.aspx?id=1&campaignno =estrogendominance&adgroup=ag1estrodom&keywords=estrogen+dominance+symptoms
[19] http://www.aeron.com/estrone.htm
[20] http://solutionspharmacy.com/index.php?option=com_content&view=article&id=47&Itemid=18
[21] http://www.afboard.com/forum/showthread.php?136-Anafit-Ezine-Vol-3-Estrogen
[22] http://www.yourmenopausetype.com/menopausequestionsandanswers/04232000.html
[23] Tietz Fundamentals of Clinical Chemistry.
[24] http://en.wikipedia.org/wiki/Estradiol
[25] http://www.heart.org/HEARTORG/Conditions/Cholesterol/AboutCholesterol/Good-vs-Bad-Cholesterol_UCM_305561_Article.jsp
[26] http://en.wikipedia.org/wiki/Steroid
[27] http://en.wikipedia.org/wiki/Steroid_hormone_receptor
[28] http://themedicalbiochemistrypage.org/steroid-hormones.html
[29] http://en.wikipedia.org/wiki/Ligand_(biochemistry)
[30] http://labtestsonline.org/understanding/analytes/vldl/test.html
[31] http://en.wikipedia.org/wiki/Cholesterol_side-chain_cleavage_enzyme
[32] http://www.progesteronefaqs.com/
[33] http://www.yourgoddessroom.com/estriol.html
[34] http://www.livestrong.com/article/36688-signs-symptoms-low-hydroxyprogesterone/
[35] http://www.mayomedicallaboratories.com/test-catalog/Clinical+and+Interpretive/9231
[36] http://en.wikipedia.org/wiki/Cortisol
[37] http://en.wikipedia.org/wiki/Corticosterone
[38] http://www.mayomedicallaboratories.com/test-catalog/Clinical+and+Interpretive/8547
[39] http://www.nlm.nih.gov/medlineplus/ency/article/003704.htm
[40] http://www.webmd.com/a-to-z-guides/aldosterone?page=2
[41] http://endocrine.niddk.nih.gov/pubs/addison/addison.htm
[42] http://www.encyclopedia.com/topic/corticosterone.aspx#1







![7. NS STEROID NON RESPONSIF.ppt [Read-Only]ocw.usu.ac.id/...I/mk_nea_slide_7.sindroma_nefrotik_steroid_non... · SINDROMA NEFROTIK STEROID NON RESPOSIF (NS STEROID RESISTEN) Definisi](https://static.fdocuments.in/doc/165x107/5c892edf09d3f21d318c7e0a/7-ns-steroid-non-read-onlyocwusuacidimkneaslide7sindromanefrotiksteroidnon.jpg)










