"What is Dysautonomia?" Brochure - Dysautonomia International

The Spectrum of Dysautonomia:
Primer in Diagnosis and Management
Emily H Caldwell, MSN ACNP-BCLos Angeles Cardiology AssociatesCedars Sinai Medical Foundation

Objectives• Define the Dysautonomia (DA) family of conditions• Identify the basic mechanism of POTS• Identify DA symptoms and etiologies• Understand the importance of the medical history
as a diagnostic tool in DA• Discuss at least three treatment strategies for DA

Dysautonomia
A disorder of the autonomic nervous system (ANS)that causes disturbances
in some or all autonomic functions.

The DysautonomiaFamily of Conditions
• Vasodepressor Syncope (VDS)• Neurogenic Orthostatic Hypotension (NOH)• Postural Orthostatic Tachycardic Syndrome
(POTS)• Familial Dysautonomia• Pure Autonomic Failure• Multiple Systems Atrophy

Epidemiology• >70 million people worldwide live with some form
of autonomic dysfunction• POTS:
» 500,000 (Robertson, D., Am J Med, 1999)» ~1-3 million Americans» Millions around the world (DA International)
• POTS: Prevalent in women 5:1 ratio
Why is this group growing?

Basic Mechanisms of Dysautonomia
• Induced tachycardia during orthostasis• Reduced venous return• Low plasma volume/Hypovolemia
» Venous pooling● Abnormal veins that stretch excessively● Altered capillary permeability
» Denervation● “slack” blood vessels● Hyperadrenergic state may result as the body attempts to
compensate

Dysautonomia
• PRIMARY:» Injury to the ANS as part of several different
degenerative neurologic disorders• SECONDARY:
» Non-neurologic systemic illness in which injury to the ANS may occur and become a predominant component
• IATROGENIC: » side effect of drugs

Dysautonomia: Symptoms• Palpitations
» When standing, with position changes» At inappropriate times
• Activity and exercise intolerance• Fatigue• Lightheadedness, near or true syncope• Tremor• Headache• Nausea

Dysautonomia: Symptoms• Increased sleep disturbance
» Daytime somnolence• Secondary features
» Muscle atrophy and deconditioning» Depression» Anxiety» “Brain Fog”, cognitive decline, memory loss» Inability to drive, work or stay in school

Vasodepressor Syncope
• Self-limited episode of pre-syncope or syncope in the presence of a drop of 30mmHg in SBP accompanied by bradycardia or asystole
• Also referred to as:» Neurocardiogenic syncope» Vasovagal syncope» Situational syncope» Neurally mediated hypotension


Orthostatic Hypotension
• A reduction in SBP of at least 20mmHg or DBP of at least 10mmHg within 3 minutes of standing
• NOH:» The above PLUS
● The use of patient’s medical history or clinical exam that suggests it is due to autonomic dysfunction, failure or neuropathy

POTS
• A heart rate increase of over 30 bpm or more, or over 120 bpm, within the first 10 minutes of standing, in the presence of symptoms of orthostatic intolerance» Neuropathic- more common» Hyperadrenergic

Subtypes of POTS
(Conner, Sheikh, & Grubb, 2012)

DA Patient Characteristics• Female predominance
» Neuropathic POTS: 5:1 female to male ratio (Connor, Sheikh, & Grubb, BJMP, 2012)
» Unpublished 5-year institutional data thru 8/17: ● 356 patients● 77% female
• Young age» 90% of POTS fell between ages 20-50
• Often precipitated by a trigger event• Remote history of orthostatic intolerance or
syncope

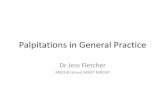
Characteristics and Ancillary Test Results of Patients with POTS
MayoClinProc 2007;82(3):308-313
Feature FindingNo. (%) of pts
(N=152)Mean ±SD age (y)
FemaleMaleTotal
30.8 ± 9.726.3 ±13.330.2 ±10.3
132 (86.8)20 (13.2)152 (100)
Mean ± SD symptom duration (y)FemaleMaleTotal
4.1 ± 5.04.0 ± 4.24.1 ± 4.9
128 (86.5)20 (13.5)148 (97.4)
Mean ± SD heart rate increase to head-up tilt (b/min)
44.2 ±13.2 152 (100)
Mean ± SD TST percent anhidrosis 8.2 ±18.1 78 (51.3)Median supine norepinephrine level (pg/mL) (IQR)
No. with supine norepinephrine level > 100 pg/ml219.5 (154.3-309)
898 (64.5)98 (8.2)


Dysautonomia: Diagnosis• Take a detailed history investigating
» Symptoms» Etiologies
● Connective tissue disorders● Joint hypermobility syndromes- Ehlers-Danlos Syndrome
● History of Central Nervous System Trauma● Viral Insult● Remote history of orthostatic intolerance● History of polypharmacy contributing to iatrogenic effect● Mast Cell Activation Disorder

Dysautonomia: Associated Conditions
• Gastroparesis• Migraine headaches• Skin rashes and hives• Multiple allergies to environmental factors and
foods

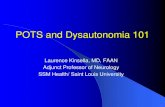
NEJM 2015;373:163-72
Clinically Relevant Mediators Released from Mast Cells and Putative Effects

Increased ReleaseNorepinephrine &Neuropeptide Y
MastCell
Histamine
Flushing
Vasodilation
SympatheticActivity
Vascular Resistance
OrthostaticTachycardia
MCAD and Mastocytosis


Dysautonomia: Diagnosis
• Physical exam should be methodical and directed» Obtain orthostatic vital signs with each visit
● In our practice: supine, standing, standing 5 min» Acrocyanosis may be the only physical signs in these
patients

Dysautonomia: Diagnosis
• If clinical history or physical exam suggest other cardiovascular abnormalities» Cardiodiagnostic testing first» TILT table test» Ambulatory monitoring

What is a Tilt Table test?

Dysautonomia: Diagnosis
• Labs» Serum and urine catecholamines» Cortisol
• Consultant referrals» GI symptoms- consider SIBO, bowel motility studies» Allergy/immunology- suspect MCAD» Neurology- migraines» Endocrine

Dysautonomia Prognosis
• Highly variable• No long term studies
» Longest at the Mayo Clinic: 2003-2010 ● (Kizilbash, Ahrens, Bhatia, Abstract Presentation at the Intl Symposium of
Autonomic Nervous System, 2013)
» Adolescents with POTS: 18.2% report total resolution while 52.8% reported persistent but improved symptoms
• Spectrum Disorder

Dysautonomia: Treatment
• There is no single treatment that addresses dysautonomia
• At present there is no cure for dysautonomia
The GOAL of treatment is to reduce symptoms and improve quality of life.

Dysautonomia: Treatment
• Differs based on subtype and concurrent diagnoses» Thoughtful provider history» Diagnostic studies:
● Tilt Table study● Ambulatory telemetry● Laboratory studies● Neurologic evaluation
» Primary versus secondary

Heart Rhythm Society, 2015

Dysautonomia: TreatmentLifestyle Interventions
» Hydration● electrolyte waters● avoid caffeine
» Increased sodium intake● Salt tabs
» Dietary modifications● Small, frequent meals● High sodium snacks● Avoid Histamine-rich foods

Dysautonomia: TreatmentLifestyle Interventions
» Position changes and postural training● Tilt Training (Verhaden, et al, Euro Heart J, 2008)● Recumbent exercise
» Compression● at least moderate grade● Abdominal binders

Dysautonomia: Treatment
Type of DA First Line Second Line Third Line and Beyond
POTSLifestyle
Intervention Beta Blockers (BB) Ivabradine
VDS
BB+/-
Fludrocortisone+/-
Midodrine
Pacemaker
NoH Florinef+/-
MidodrineDroxidopa
Mixed DAFlorinef
+/-Midodrine
Ivabradine
Droxidopa

Midodrine• Alpha1 receptor agonist• Objective effects: raises SBP
» both supine and standing» may result in supine hypertension
• Subjective effects» reduces dizziness, near and true syncope» reduces brain fog
• Side effects: » headache, vasodilation, dry mouth, nervousness,
piloerection

Ivabradine
• Used in Europe since 2005 and approved for use by FDA since 2015
• Selectively inhibits the I(f) currents in a dose-dependent manner» Most important for regulating pacemaker activity in the
heart• Indications for use in U.S.
» symptomatic management of stable chest pain and heart failure not fully managed by beta-blockers

Ivabradine
• Objective effects» Reduces heart rate
• Subjective effects» Reduces symptoms associated with the tachycardic
component of dysautonomia• Side effects
» bradycardia, hypertension, atrial fibrillation and luminous phenomena

Droxidopa
• Approved for use by FDA in fall 2014 to treat neurogenic orthostatic hypotension as a primary and secondary condition
• Prodrug of norepinephrine » used to increase concentrations of these
neurotransmitters in the body and brain

Droxidopa
• Objective effects» Raise SBP, both supine and standing» May result in supine hypertension
• Subjective effects» Reduce dizziness, near and true syncope» Reduce brain fog
• Side effects» headache, nausea, dizziness

Less obvious challenges in RX • Many pts are chronically ill
» Altered family dynamics• Great reliance on internet, websites, and social media
» Much doctor shopping
• Difficult to find collaborating providers• Use of opioids is excessive • Major medical centers have no interest in this patient
group• Major clinical trials of pharmacologic and treatment
strategies necessary

In ConclusionüConsider Dysautonomia in your differential dxüDetailed historyüOrthostatic vital signs üLifestyle modificationsüPrescriptions when lifestyle changes not enoughüMultidisciplinary approach
ü Referrals to collaborating consultants