The sooner, the better: temporal patterns in brief treatment of depression and their role in...
12
This article was downloaded by: [University of Regina] On: 18 November 2014, At: 09:51 Publisher: Routledge Informa Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK Psychotherapy Research Publication details, including instructions for authors and subscription information: http://www.tandfonline.com/loi/tpsr20 The sooner, the better: temporal patterns in brief treatment of depression and their role in long-term outcome Eva Gilboa-Schechtman a & Golan Shahar b a Department of Psychology , Bar-Ilan University , Ramat Gan, Israel b Ben-Gurion University, Department of Psychiatry , Yale University School of Medicine , Beer-Sheva, Israel Published online: 22 Feb 2007. To cite this article: Eva Gilboa-Schechtman & Golan Shahar (2006) The sooner, the better: temporal patterns in brief treatment of depression and their role in long-term outcome, Psychotherapy Research, 16:03, 374-384, DOI: 10.1080/10503300500485425 To link to this article: http://dx.doi.org/10.1080/10503300500485425 PLEASE SCROLL DOWN FOR ARTICLE Taylor & Francis makes every effort to ensure the accuracy of all the information (the “Content”) contained in the publications on our platform. However, Taylor & Francis, our agents, and our licensors make no representations or warranties whatsoever as to the accuracy, completeness, or suitability for any purpose of the Content. Any opinions and views expressed in this publication are the opinions and views of the authors, and are not the views of or endorsed by Taylor & Francis. The accuracy of the Content should not be relied upon and should be independently verified with primary sources of information. Taylor and Francis shall not be liable for any losses, actions, claims, proceedings, demands, costs, expenses, damages, and other liabilities whatsoever or howsoever caused arising directly or indirectly in connection with, in relation to or arising out of the use of the Content. This article may be used for research, teaching, and private study purposes. Any substantial or systematic reproduction, redistribution, reselling, loan, sub-licensing, systematic supply, or distribution in any form to anyone is expressly forbidden. Terms & Conditions of access and use can be found at http:// www.tandfonline.com/page/terms-and-conditions
Transcript of The sooner, the better: temporal patterns in brief treatment of depression and their role in...

This article was downloaded by: [University of Regina]On: 18 November 2014, At: 09:51Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House,37-41 Mortimer Street, London W1T 3JH, UK
Psychotherapy ResearchPublication details, including instructions for authors and subscription information:http://www.tandfonline.com/loi/tpsr20
The sooner, the better: temporal patterns in brieftreatment of depression and their role in long-termoutcomeEva Gilboa-Schechtman a & Golan Shahar ba Department of Psychology , Bar-Ilan University , Ramat Gan, Israelb Ben-Gurion University, Department of Psychiatry , Yale University School of Medicine ,Beer-Sheva, IsraelPublished online: 22 Feb 2007.
To cite this article: Eva Gilboa-Schechtman & Golan Shahar (2006) The sooner, the better: temporal patterns inbrief treatment of depression and their role in long-term outcome, Psychotherapy Research, 16:03, 374-384, DOI:10.1080/10503300500485425
To link to this article: http://dx.doi.org/10.1080/10503300500485425
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all the information (the “Content”) containedin the publications on our platform. However, Taylor & Francis, our agents, and our licensors make norepresentations or warranties whatsoever as to the accuracy, completeness, or suitability for any purpose of theContent. Any opinions and views expressed in this publication are the opinions and views of the authors, andare not the views of or endorsed by Taylor & Francis. The accuracy of the Content should not be relied upon andshould be independently verified with primary sources of information. Taylor and Francis shall not be liable forany losses, actions, claims, proceedings, demands, costs, expenses, damages, and other liabilities whatsoeveror howsoever caused arising directly or indirectly in connection with, in relation to or arising out of the use ofthe Content.
This article may be used for research, teaching, and private study purposes. Any substantial or systematicreproduction, redistribution, reselling, loan, sub-licensing, systematic supply, or distribution in anyform to anyone is expressly forbidden. Terms & Conditions of access and use can be found at http://www.tandfonline.com/page/terms-and-conditions

The sooner, the better: Temporal patterns in brief treatmentof depression and their role in long-term outcome
EVA GILBOA-SCHECHTMAN1 & GOLAN SHAHAR2
1Department of Psychology, Bar-Ilan University, Ramat Gan, Israel and 2Ben-Gurion University, Beer-Sheva, Israel, and
Department of Psychiatry, Yale University School of Medicine
(Received 26 August 2003; revised 6 June 2005; accepted 14 September 2005)
AbstractTo examine whether temporal patterns of change in brief treatment for depression are predictive of outcome at 18 monthsposttreatment, the authors used data from the National Institute of Mental Health-sponsored Treatment of DepressionCollaborative Research Program. In accordance with their hypotheses, they found that (a) individuals whose level of distressdoes not decrease between intake and Week 4 of therapy (slow remoralizers) exhibited a more severe symptom pattern atfollow-up assessments than those exhibiting immediate relief (rapid remoralizers); (b) rate of symptom reduction duringtreatment is predictive of 12- and 18-month outcomes beyond initial symptom severity; and (c) rate of symptom reduction ismore predictive of 12- and 18 month outcomes in psychotherapy than in nonpsychological treatments. Findings encouragefurther research and clinical attention to temporal patterns of response in brief treatments of depression.
Despite successful treatment, relapse and recurrence
are the rule rather than the exception in the long-
term course of major depressive disorder (MDD).
Thus, the risk of repeated episodes of depression is
estimated to be as high as 80% (e.g., Judd, 1997; see
also Joiner, 2000). Accordingly, understanding the
underpinnings of depression’s chronicity is one of
the most important challenges facing contemporary
research. So far, estimating the risk of relapse and
recurrence of depression has focused on psychiatric
history (e.g., Belsher & Costello, 1988; Hammen,
Mayol, deMayo, & Marks, 1986; Lewinsohn, Zeiss,
& Duncan, 1989; Hart, Craighead & Craighead,
2001), life events (e.g., Billings & Moos, 1984;
Brown & Harris, 1978; Mazure, Bruce, Maciejewski,
& Jacobs, 2000), and dysfunctional cognitions (e.g.,
Segal, Shaw, Vella, & Katz, 1992). As important as
these factors are, they all share the characteristic of
being unrelated to the treatment process. In con-
trast, only few studies have examined how patterns
of response to treatment of depression contribute to
the prediction of the recurrence of depressive symp-
toms. This gap in the literature paves the way to the
present investigation.
Most studies predicting the course of depression
after treatment have examined either posttreatment
depressive symptomatology or the change in this
symptomatology from pre- to posttreatment. All
these measures are aggregates across individuals.
Thus, the precise manner in which an individual
responds to treatment between the initial (pretreat-
ment) time point and the final session is overlooked.
However, it has been observed that the temporal
patterns of patients’ response often differ substan-
tially from the pattern of the average (i.e., aggregate)
group response (cf. Gilboa-Schechtman & Foa,
2001; Tang & DeRubeis, 1999a, 1999b). In parti-
cular, it is possible that although some individuals
exhibit a monotonically decreasing pattern of symp-
tomatology from the beginning to the end of treat-
ment, others show an initial increase, reaching a
peak at idiosyncratic times, again followed by a
decrease. Indeed, Gilboa-Schechtman and Foa
(2001) examined 3-month patterns of natural re-
covery after sexual and nonsexual assault. They
found that the timing of peak distress, which varied
between individuals, was ‘‘washed away’’ by group
aggregation. However, this parameter, together with
rate of symptom reduction, was an important pre-
dictor of long-term posttrauma pathology. In sum,
aggregating over idiosyncratic patterns of response
obscures the predictive importance of individual
patterns of change.
Another individual difference parameter that can
be washed away by group aggregation is a sudden
(yet individually spaced) decrease in symptom
Correspondence: Eva Gilboa-Schechtman, Department of Psychology, Bar-Ilan University, Ramat-Gan 52900, Israel. E-mail:
Psychotherapy Research, May 2006; 16(3): 374�/384
ISSN 1050-3307 print/ISSN 1468-4381 online # 2006 Society for Psychotherapy Research
DOI: 10.1080/10503300500485425
Dow
nloa
ded
by [
Uni
vers
ity o
f R
egin
a] a
t 09:
51 1
8 N
ovem
ber
2014

severity that occurs between session intervals, or the
‘‘sudden gains’’ phenomenon. Tang and DeRubeis
(1999b) found that individuals receiving cognitive�/
behavioral therapy (CBT) for depression and ex-
periencing such sudden gains were more likely to
evidence significantly lower levels of depressive
symptomatology at the end of therapy than those
who did not experience such gains. Moreover, this
enhanced recovery held through most of the follow-
up period. Tang and DeRubeis concluded that, by
investigating the time course of individual patients,
meaningful patterns that are shared by many in-
dividual patients might be detected, even if these
patterns are not revealed in the group mean time
course. As has been convincingly argued by Krause,
Howard, and Lutz (1998), ‘‘in order to maximize
relevance for clinical practice, the results of treat-
ment research should always be reported at this most
disaggregated or individual change level.’’ (p. 838).
Given the significance of temporal patterns of
change during treatment for the prediction of long-
term outcome, we sought to examine the relation-
ship between temporal patterns of change and
ensuing outcome using data from the National
Institute of Mental Health-sponsored Treatment of
Depression Collaborative Research Program
(TDCRP; Elkin, 1994). Several features render
these data appropriate for such an investigation.
First, the TDCRP is the single most important
controlled trial juxtaposing several treatment mod-
alities (Elkin, 1994; Elkin et al., 1989). Second, the
TDCRP involved follow-up assessments at signifi-
cantly distant time intervals after initial treatments
(at 12 and 18 months). Third, the TDCRP offers
multiple converging measures of symptom severity,
which were collected at several time points.
Theoretically, we were motivated by the phase
model of treatment (Howard, Lueger, Maling, &
Martinovich, 1993). This model postulates that
patients undergo three distinct phases in treatment:
remoralization (enhancement of the patient’s sense
of subjective well-being), remediation (symptom
reduction), and rehabilitation (recovery of life func-
tioning). Viewing TDCRP as providing information
on the first two phases of treatment, remoralization
and remediation, we sought to examine how para-
meters of temporal response during these two phases
would relate to ensuing outcome.
The first goal of the present study was to examine
whether symptom reduction in the early phases of
treatment is predictive of ensuing outcome. So far,
only a few studies addressed this issue. Fennel and
Teasdale (1987) examined the relationship between
early symptom reduction during brief psychological
treatment for depression and symptom return after
treatment. In their study, 15 individuals receiving
CBT were identified as either rapid (more than 50%
symptom reduction) or slow (less than 50% symp-
tom reduction) responders based on the amount of
symptom reduction observed on the Beck Depres-
sion Inventory (BDI) after the first two initial
sessions. Fennel and Teasdale found that slow
responders reported being more distressed than
rapid responders 12 months after treatment termi-
nation. Similarly, early versus delayed improvement
in symptoms of posttraumatic stress disorder
(PTSD) was predictive of long-term recovery (Gil-
boa-Schechtman & Foa, 2001). More recently,
Santor and Segal (2001) examined in 76 outpatients
with MDD the relationship between symptom re-
turn 3 and 6 months after CBT and pattern of
symptom reduction during treatment. They did not
find a relationship between early symptom reduction
(defined as change score between pretreatment BDI
score and BDI score at Week 3) and symptoms at 3-
and 6-months follow-up. Given the inconsistent
pattern of results emerging from the studies con-
cerning the prognostic value of early improvement,
we sought to reexamine the association between
symptom reduction early in the therapeutic process
and ensuing outcome in the TDCRP data. Specifi-
cally, we examined whether the intrapersonal change
in level of symptom severity (rather than absolute
level of change in the first weeks of treatment) is
indicative of better ensuing outcome.
We predicted that individuals who are slow to
engage in the first, remoralization, phase of treat-
ment (slow remoralizers [SRs]) would exhibit a more
severe symptom pattern at follow-up assessments
than would those who are faster to warm up to
treatment (rapid remoralizers [RRs]). We defined
SRs as those individuals who do not experience a
significant reduction in symptoms over the first 4
weeks of treatment and RRs as those who do
experience some relief. Our choice of 4 weeks of
treatment as the critical period was driven by
theoretical as well as practical considerations. On
the theoretical side, the remoralization phase is
supposed to commence even before the first formal
therapy session, as individuals begin to ‘‘do some-
thing’’ about their problems (such as setting up an
appointment). This phase is purported to be non-
modality specific, because it exerts its influence by
the virtue of establishing a proper context for
therapeutic work. Consistent with previous research,
we assumed that the remoralization phase occurs
between intake and Week 4 of treatment (Ilardi &
Craighead, 1994). On the practical side, the assess-
ment points in the TDCRP were given every 4
weeks; therefore, the critical period coincides with
the first two assessment points (i.e., pretreatment
and first treatment).
Temporal patterns in brief treatment for depression 375
Dow
nloa
ded
by [
Uni
vers
ity o
f R
egin
a] a
t 09:
51 1
8 N
ovem
ber
2014

The second goal of the present research was to
examine whether the rate of symptom reduction
during the remediation phase of treatment (after the
4-week assessment and continuing until treatment
termination) was predictive of long-term outcome as
indicated by symptom severity at 12- and 18-months
follow-up. To the best of our knowledge, only Santor
and Segal (2001) examined whether the rate of
symptom reduction during treatment was associated
with symptoms at follow-up. Using hierarchical
linear modeling, they found that the rate of symptom
reduction during the first 10 weeks of treatment was
negatively associated with symptoms at 3- and 6-
month follow-up assessments, even after controlling
for initial depression severity. In the present study,
we sought to replicate and extend these results in a
number of ways. First, we examined 12- and 18-
month outcomes, because a more prolonged follow-
up period increases the likelihood of relapse. Second,
we examined the relationship between rate of
symptom reduction during the remediation phase
as measured by self-report as well as by clinician
measures, whereas in Santor and Segal’s study the
examination was limited to self-reports only. In
addition, thus far the study of the relationship
between pattern of change (as indicated by both
rapid and SRs and rate of symptom change) and
long-term outcome has been limited to the examina-
tion of the outcome of CBT. The present study
extends previous investigations by examining tem-
poral patterns of response to treatment modalities
included in the TDCRP (i.e., CBT, interpersonal
therapy [IPT], imipramine plus clinical management
[IMI-CM], inactive placebo plus clinical manage-
ment [PLA-CM]) condition. Specifically, we postu-
lated that the rate of symptom reduction during
treatment, as assessed by self-report as well as
clinician-rated scales, would be predictive of ensuing
outcome beyond initial symptom severity.
A third goal of the current study was to examine
whether the rate of symptom reduction is differen-
tially related to long-term outcome depending on the
modality of treatment. In doing so, we sought to
replicate and extend the findings of Watkins et al.
(1993) study, which compares the temporal course
of response to psychotherapy and pharmacotherapy
in the TDCRP data. Watkins et al. examined group
differences in active pharmacological treatment ver-
sus psychological treatments at discrete time inter-
vals (i.e., 4, 8, and 12 weeks). Although Watkins et
al. have examined the differential effects of modality
during the course of treatment (up to 16 weeks), we
studied ensuing outcome (up to 18 months). Indeed,
previous research has already shown that treatment
modality predicts long-term outcome over and above
the overall success of treatment. For example, after a
successful treatment of depression using CBT, out-
patients show less relapse than those who recover
with antidepressant medication and are then with-
drawn from pharmacotherapy (e.g., Blackburn,
Funson, & Bishop, 1986; Shea et al., 1992). In
line with these findings, we reasoned that rapid
improvement in psychological treatments is likely
to indicate some insight, successful cognitive proces-
sing (Beck, Rush, Shaw, & Emery, 1979), or ‘‘work-
ing through’’ (Freud, 1958) of a painful issue and
thus is likely indicative of future ability to deal with
stress. In contrast, because pharmacological and
placebo treatments are not specifically geared toward
the acquisition of psychological skills (e.g., emotion
regulation, psychological insight), gains made with
the assistance of such treatments, even if rapid, are
likely to be of limited prognostic importance. Thus,
we hypothesized that the nature of the relationship
between rate of symptom recovery and long-term
outcome would vary between psychotherapy and
nonpsychological treatments. Specifically, we ex-
pected that the rate of recovery in therapy would
be a better predictor of long-term outcome than it
would be for pharmacological and placebo treatment
conditions.
Method
Participants and Procedure
The design and procedures of the TDCRP have
been described in detail elsewhere (e.g., Elkin et al.,
1989). In brief, patients were assigned randomly, at
each of three sites, to one of four treatment condi-
tions: IPT, CBT, IMI-CM, or PLA-CM. All treat-
ments were 16 weeks long (range �/ 16�/20
sessions).
Participants were outpatients between the ages of
21 and 60 who met research diagnostic criteria for
MDD. Eligible patients scored a minimum of 14 on
a modified Hamilton Rating Scale for Depression
(HRSD; Hamilton, 1967) both at an initial screen-
ing and at a rescreening 1 to 2 weeks later. A total of
250 patients met study entry criteria and were
randomly assigned; of these, 239 actually entered
treatment. According to Elkin et al.’s definition, a
‘‘completer’’ is an individual who has participated in
at least 12 sessions and 15 weeks of treatment.
Following earlier studies, we have focused on 162
completers (see Elkin et al., 1989, or Watkins et al.,
1993, for the use of the same inclusion criteria and
completer sample).
Measures
To assess outcome, we focused on two widely used
measures of depression severity: the Beck Depres-
376 E. Gilboa-Schechtman and G. Shahar
Dow
nloa
ded
by [
Uni
vers
ity o
f R
egin
a] a
t 09:
51 1
8 N
ovem
ber
2014

sion Inventory (BDI; Beck, Ward, Mendelson,
Mock, & Erbaugh, 1961) and the HRSD (Hamilton,
1960). In addition to these widely used measures of
depression, we also used a composite clinical out-
come variable (Blatt, Zuroff, Quinlan, & Pilkonis,
1996) based on the five primary outcome measures
of the TDCRP: BDI, HRSD, the total score on the
Hopkins Symptom Checklist-90 (SCL-90; Deroga-
tis, Lipman, & Covi, 1973), Global Assessment
Scale (GAS; Endicott, Spitzer, Fleiss, & Cohen,
1976), and the sum of the global ratings from the
Social Adjustment Scale (SAS; Weissman & Paykel,
1974). The BDI and SCL-90 are self-report mea-
sures, and the HRSD, GAS and SAS are interview-
based measures completed by clinical evaluators.
Higher scores on the composite outcome measure
indicated better relative improvement.1
Results
Modeling Individual Change Patterns
As mentioned, we viewed TDCRP as providing
information on the first two phases of treatment:
remoralization (Weeks 0�/4) and remediation (Week
4 to end of treatment). For the remoralization phase,
we defined SRs as those individuals who experience
only a mild (B/ 15%) decrease in distress between
intake and Week 4 of treatment2 and RRs as those
with a more significant distress decrease.
For the remediation phase, we assumed that the
process of symptom reduction proceeds in an
exponential decay fashion, because it is the simplest
and most commonly used model of temporal change
(e.g., Howard et al., 1993; Willett & Sayer, 1994).
This form of the recovery function is assumed
because many studies have found that a more rapid
change in symptoms is being made at early stages
compared with later stages of treatment. This
phenomenon consistently produces a curvilinear
growth curve that is best normalized by a log-linear
transformation of session number (see Howard,
Moras, Brill, Martinovich, & Lutz, 1996; Lambert,
Hansen, & Finch, 2001, for similar discussions and
procedures).
In an exponential decay function, the severity of
the symptoms at a given time point decreases by a
constant proportion over any time interval of a given
length. For example, if the severity of depression
decreased from 27 to 18 from Week 4 to Week 8,
then it is expected to decrease to 12 and 8 for Weeks
12 and 16, respectively (the decay rate being 33%
per month). We are assuming only that the recovery
function is exponential in form; we are not making
any assumption about the parameters of decay (i.e.,
33% or 50%), because this variable is a part of the
individual growth function parameters. Inspection of
the data at the individual level indicated that, for
most patients, exponential decay function was in-
deed a reasonable approximation. The explicit
functional form we estimate is as follows: Distress
(t)�/a*exp(�/b*t). The trajectory of the symptom
reduction depends on the values of parameters a and
b , which vary across individuals. Parameters a and b
determine the magnitude of peak distress and rate of
recovery. Specifically, according to this model, the
magnitude of peak reaction is EXP(a) and the rate of
recovery is 1�/EXP(b). Thus, when time is mea-
sured in months, the model predicts that the degree
of distress is multiplied by EXP(b) every month, and
1�/EXP(b) is the monthly percentage of decrease.
Mathematically, an exponential decay of a distress
reaction is equivalent to its logarithm being a linear
function of time; that is, log(distress(t))�/log(a)�/
b*t. To allow linear modeling of growth curves, we
first transformed them using a log-linear transforma-
tion by session number and then computed the
individual difference parameters.
Rapid Versus Slow Remoralizers
To address our first, early remoralization,
hypothesis*/that SR individuals, who are slow to
engage in the first, remoralization, phase of treat-
ment, would exhibit a more severe symptom pattern
at follow-up assessments than would RR individuals,
who are faster to warm up to treatment*/we
contrasted the parameters of response of these two
groups. Table I presents means and standard devia-
tions of symptoms at intake, end of treatment, and
12- and 18-month follow-up periods and the
monthly rate of symptom reduction for fast and
slow remoralizers.
Results indicate that RRs do not differ from SRs in
their initial levels of distress on composite measures,
whereas on the BDI and the HRSD the RRs were
more distressed than the SRs. However, SRs ex-
hibited a more severe symptomatology at the end of
treatment on all three measures. At 12- and 18-
month follow-up assessments, SRs were more dis-
tressed than RRs on two of the three outcome
measures (the BDI and composite measures but
not HRSD). To ascertain that the end-point and
follow-up differences between SRs and RRs were not
attributable to differences in the initial levels of
distress, we examined the difference between these
groups, controlling for the initial (pretreatment)
level of distress on the corresponding measure
(e.g., we regressed BDI at 12 months on pretreat-
ment BDI and type of remoralizer). The pattern of
results was identical to that presented in Table I.
Finally, the data also indicate that SRs and RRs do
Temporal patterns in brief treatment for depression 377
Dow
nloa
ded
by [
Uni
vers
ity o
f R
egin
a] a
t 09:
51 1
8 N
ovem
ber
2014

not differ significantly in their rate of symptom
reduction during treatment.
Rate of Symptom Reduction During
Remediation Phase
To examine our second, rapid remediation,
hypothesis*/that the rate of symptom reduction
during treatment would predict ensuing outcome
beyond initial symptom severity*/we conducted
regression analyses. Specifically, we regressed 12-
and 18-month follow-up scores on pretreatment
scores alone, rate of symptom reduction alone,
pretreatment scores and rates of symptom reduction
combined, and finally pretreatment scores, rates
of symptom reduction, and type of remoralizer
(slow vs. rapid) combined. Results are presented in
Table II.
The results of regressions A1�/A3 presented in
Table II, including a single predictor each, indicated
that, for BDI and composite but not HRSD scores,
pretreatment severity predicted long-term outcome;
higher pretreatment scores were associated with
higher scores at follow-up. Results further suggested
that rate of recovery alone predicted 12- and 18-
month outcomes on all three measures. Finally, type
of remoralizer predicted 12- and 18-month out-
comes on the BDI measures and on the composite
measure.
The results of the regression B presented in
Table II, involving pretreatment scores and rate of
symptom reduction as predictors, indicated that, for
BDI, HRSD, and the composite scores for both 12-
and 18-month outcomes, rates of symptom reduc-
tion independently contributed to the prediction of
long-term symptom severity over and above initial
distress.
Finally, the results of simultaneous regression C
presented in Table II, using all variables as predic-
tors, indicated that the rate of symptom reduction is
a significant predictor of 12- and 18-month out-
comes, controlling for initial symptoms and for type
of remoralizers for all outcome measures. Type of
remoralizer was a significant predictor of outcome
over and above pretreatment symptoms and rate of
recovery on two of our three measures (i.e., the BDI
and composite).
Treatment Modality
To test our third, treatment modality, hypothesis*/
that the rate of recovery in talk therapy (i.e., CBT
and IPT) would be a better predictor of 12- and
18-month outcomes than it would be for pharma-
cological and placebo treatment conditions*/we
conducted additional regression analyses with treat-
ment modality as a binary variable. Specifically, we
examined whether the rate of symptom reduction
was differentially predictive of treatment outcome
depending on whether the patient participated in a
treatment involving therapy (i.e., IPT or CBT
interventions) or medications (placebo or imipra-
mine interventions). To this end, we regressed
measures of 12- and 18-month outcomes on pre-
treatment severity, rate of symptom reduction,
therapy, a Therapy�/Rate of Reduction interaction,
and a Therapy�/Type of Remoralization interaction
using simultaneous regression. The results of this
analysis are shown in Table III.
Consistent with our hypothesis, inspection of
Table III reveals a significant Therapy �/ Rate of
Reduction interaction when the BDI and the com-
posite score were considered as outcomes. The
examination of the rates of recovery in the psycho-
logical treatments and in the nontalk therapy treat-
ments revealed that rate of recovery was more
predictive of ensuing outcome if the patient was
engaged in active psychological treatment and less
predictive if the patient received pharmacological or
placebo treatment. Further, we also found that
therapy modality interacted with type of remoraliza-
tion on most measures. This lends further indirect
support to the treatment modality hypothesis.
Table I. Means and standard deviations of symptoms at pretreat-
ment (intake), end of treatment, 12- and 18- month follow-up
assessments, and of rate of symptom reduction for fast and slow
remoralizers.
Measure
RRs
(N�/122)
SRs
(N�/40) F (1, 147�/161)
Pretreatment
BDI 27.719/7.37 24.489/8.72 4.72*
HRSD 19.149/4.19 18.999/3.96 .06
Comp 1.159/0.57 1.019/0.50 .19
End of treatment
BDI 7.859/7.56 15.009/11.18 18.17**
HRSD 6.509/5.05 11.759/6.75 22.59**
Comp �/0.869/0.83 0.019/1.11 27.17**
12-Month follow-up
BDI 8.189/8.32 12.039/13.18 3.91*
HRSD 7.309/6.93 9.809/8.64 2.81*
Comp �/0.779/0.96 �/0.209/1.31 6.94**
18-Month follow-up
BDI 7.759/7.60 11.129/12.03 3.52*
HRSD 6.849/5.60 9.639/6.96 5.66**
Comp �/0.859/0.83 �/0.369/1.13 7.09**
Reduction rate (%)
BDI 239/0.29 249/0.31 0.19
HRSD 179/0.25 199/0.24 0.14
Comp 139/0.13 159/0.14 0.71
Note. RRs�/rapid remoralizers; SRs�/slow remoralizers; BDI�/
Beck Depression Inventory; HRSD�/Hamilton Rating Scale for
Depression.; Comp�/composite.
*p B/.05. **p B/.01, one-tailed.
378 E. Gilboa-Schechtman and G. Shahar
Dow
nloa
ded
by [
Uni
vers
ity o
f R
egin
a] a
t 09:
51 1
8 N
ovem
ber
2014
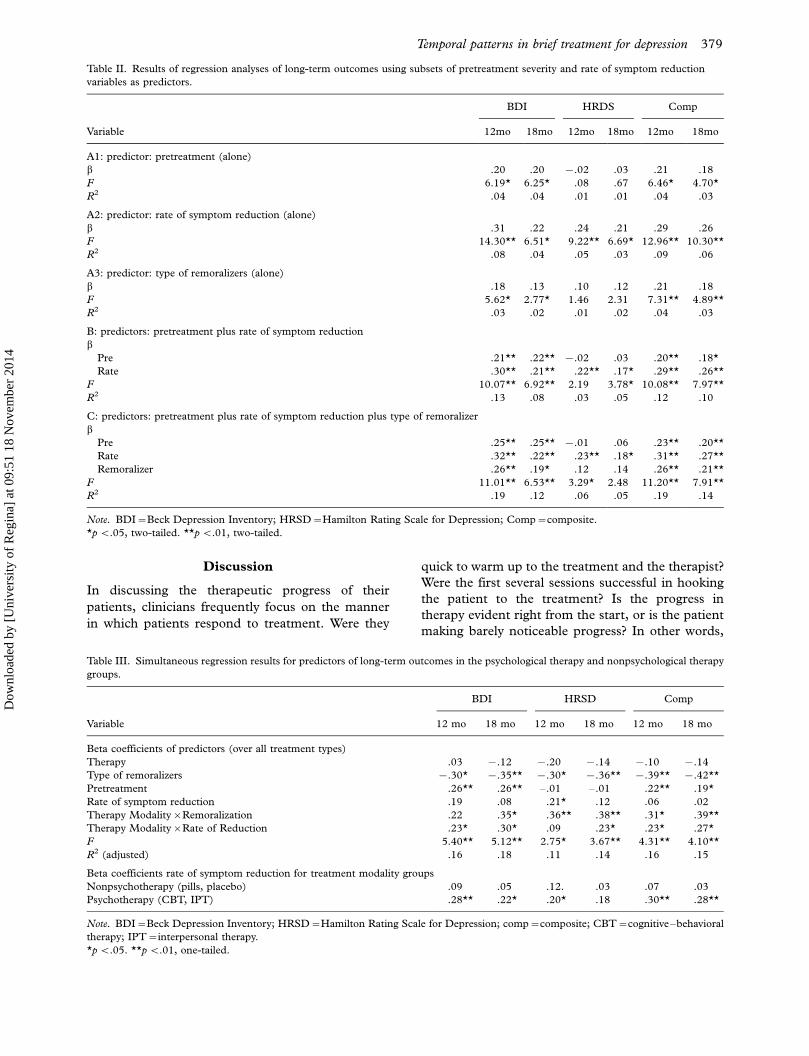
Discussion
In discussing the therapeutic progress of their
patients, clinicians frequently focus on the manner
in which patients respond to treatment. Were they
quick to warm up to the treatment and the therapist?
Were the first several sessions successful in hooking
the patient to the treatment? Is the progress in
therapy evident right from the start, or is the patient
making barely noticeable progress? In other words,
Table II. Results of regression analyses of long-term outcomes using subsets of pretreatment severity and rate of symptom reduction
variables as predictors.
BDI HRDS Comp
Variable 12mo 18mo 12mo 18mo 12mo 18mo
A1: predictor: pretreatment (alone)
b .20 .20 �/.02 .03 .21 .18
F 6.19* 6.25* .08 .67 6.46* 4.70*
R2 .04 .04 .01 .01 .04 .03
A2: predictor: rate of symptom reduction (alone)
b .31 .22 .24 .21 .29 .26
F 14.30** 6.51* 9.22** 6.69* 12.96** 10.30**
R2 .08 .04 .05 .03 .09 .06
A3: predictor: type of remoralizers (alone)
b .18 .13 .10 .12 .21 .18
F 5.62* 2.77* 1.46 2.31 7.31** 4.89**
R2 .03 .02 .01 .02 .04 .03
B: predictors: pretreatment plus rate of symptom reduction
bPre .21** .22** �/.02 .03 .20** .18*
Rate .30** .21** .22** .17* .29** .26**
F 10.07** 6.92** 2.19 3.78* 10.08** 7.97**
R2 .13 .08 .03 .05 .12 .10
C: predictors: pretreatment plus rate of symptom reduction plus type of remoralizer
bPre .25** .25** �/.01 .06 .23** .20**
Rate .32** .22** .23** .18* .31** .27**
Remoralizer .26** .19* .12 .14 .26** .21**
F 11.01** 6.53** 3.29* 2.48 11.20** 7.91**
R2 .19 .12 .06 .05 .19 .14
Note. BDI�/Beck Depression Inventory; HRSD�/Hamilton Rating Scale for Depression; Comp�/composite.
*p B/.05, two-tailed. **p B/.01, two-tailed.
Table III. Simultaneous regression results for predictors of long-term outcomes in the psychological therapy and nonpsychological therapy
groups.
BDI HRSD Comp
Variable 12 mo 18 mo 12 mo 18 mo 12 mo 18 mo
Beta coefficients of predictors (over all treatment types)
Therapy .03 �/.12 �/.20 �/.14 �/.10 �/.14
Type of remoralizers �/.30* �/.35** �/.30* �/.36** �/.39** �/.42**
Pretreatment .26** .26** �/.01 �/.01 .22** .19*
Rate of symptom reduction .19 .08 .21* .12 .06 .02
Therapy Modality�/Remoralization .22 .35* .36** .38** .31* .39**
Therapy Modality�/Rate of Reduction .23* .30* .09 .23* .23* .27*
F 5.40** 5.12** 2.75* 3.67** 4.31** 4.10**
R2 (adjusted) .16 .18 .11 .14 .16 .15
Beta coefficients rate of symptom reduction for treatment modality groups
Nonpsychotherapy (pills, placebo) .09 .05 .12. .03 .07 .03
Psychotherapy (CBT, IPT) .28** .22* .20* .18 .30** .28**
Note. BDI�/Beck Depression Inventory; HRSD�/Hamilton Rating Scale for Depression; comp�/composite; CBT�/cognitive�/behavioral
therapy; IPT�/interpersonal therapy.
*p B/.05. **p B/.01, one-tailed.
Temporal patterns in brief treatment for depression 379
Dow
nloa
ded
by [
Uni
vers
ity o
f R
egin
a] a
t 09:
51 1
8 N
ovem
ber
2014

clinicians experience and discuss their patients as
individuals rather than as prototypical examples of a
certain group. Thus, the questions posed by the
practitioner are typically not about a treatment’s
effectiveness or efficacy but about treatment effec-
tiveness for a particular patient (patient-focused
research; Howard et al., 1996). Patient-focused
questions must be answered by focusing on an
individual and his or her pattern of change rather
than on the changes observed in a group of different
individuals.
So far, the examination of TDCRP data focused
solely on questions pertaining to treatment efficacy,
investigating the average response of a group of
patients. In an effort to assess patient-focused
questions, all of which deal with patterns of change
within the treatment process, we examined the
temporal pattern of responding to brief therapy of
depression as it relates to 12 and 18-month out-
comes. We have found that, controlling for initial
depression severity, individuals who exhibited im-
mediate gains between intake and Week 4 of treat-
ment fared better during the follow-up period than
those who exhibited very mild, if any, relief during
this interval. Our results are consistent with those of
Fennel and Teasdale (1987) in that RRs exhibited a
less severe long-term symptomatology than SRs.
Moreover, our results strengthen those of Fennel
and Teasdale in that we used a less stringent criterion
of improvement (15% vs. 50%). Findings obtained
here indicated that early response to treatment is a
simple predictor of therapy outcome. Psychophar-
macological research has already begun investigating
criteria for treatment discontinuation by analyzing
the patterns of change with certain drug regimens
(e.g., Thase & Kupfer, 1996). Similar criteria might
need to be developed for other treatment modalities,
with the practical implication that if, after an
identifiable number of sessions, a patient has not
improved at least to some degree, the treatment
modality might be reconsidered (see also Lueger et
al., 2001).
Timing of remoralization, whether it occurs at the
onset of treatment (as in rapid remoralization) or at a
later stage (slow remoralization), is an important
predictor of both short-term (i.e., treatment effec-
tiveness) and long-term outcome. Several different,
although not necessarily incompatible, explanations
are possible for this finding. During the first several
weeks of a successful treatment, patients need to
accomplish several important goals to feel remor-
alized (Howard et al., 1993). For example, patients
need to be socialized to the treatment, they need to
formulate (with the help of the health care profes-
sional) a plausible rationale for their distress (Gold-
fried, 1980), they need to gather some hope that
their condition is treatable, and they need to come to
trust their own abilities to obtain such a relief (self-
efficacy; Bandura, 1977). Because an outcome-
relevant, constructive, therapeutic alliance has
shown to be formed early in the treatment process
(Shahar, Blatt, Zuroff, Krupnick, & Sotsky, 2004),
difficulties in establishing such an alliance might
result in a ‘‘false start’’ of a therapeutic process, a
worse outcome of therapy, and, therefore, poorer
prognosis.
Consistent with our second hypothesis, we have
found that faster rate of symptom reduction is
related to better ensuing outcome over and above
initial levels of distress and nature of the initial
response (slow or rapid response). Again, multiple
interpretations are consistent with this finding. First,
it is possible that fast rate of symptom reduction is
related to sudden gains in treatment, which have
been associated with better prognosis (Stiles et al.,
2003; Tang, Luborsky, & Andrusyna, 2002). Alter-
natively, it is also possible that such rapid sympto-
matic improvement is related to patients’ greater
self-efficacy (Bandura, 1977), which, in turn, can
lead to greater compliance with therapeutic proce-
dures. This may assist in modifying patients’ belief in
their ability to handle their symptoms (e.g., have less
difficulty concentrating, ruminate less) and cope
more effectively with the precipitating life situation.
Such greater efficacy may be translated to enhanced
future ability to cope more effectively with stressful
life events. Another explanation focuses on the
interpersonal nature of depression, namely, the fact
that depressive symptoms in general, and MDD in
particular, bring about interpersonal stress and
erode patients’ close relationships (Coyne, 1976a,b;
Hammen, 1991, 1998; Joiner, 2000; Shahar, 2001;
Zuroff, 1992). In that sense, the sooner that
patients’ depression is alleviated, the less likely it is
that their depression will be exacerbated by generat-
ing socially malignant conditions.
Consistent with our third hypothesis, we found
that the rate of symptom reduction is more impor-
tant for long-term outcome prediction in active
psychological therapy than in other treatments
(i.e., active pharmacological treatment and placebo
and clinical management treatment). This finding is
consistent with differential mechanisms related to
symptom reduction in the two treatment modalities.
To benefit from an active psychological intervention,
patients must implement in day-to-day life the
methods and strategies learned in therapy. As men-
tioned, rapid rate of symptom reduction may be
related to a successful integration of new cognitive,
interpersonal, and behavioral habits into one’s daily
routine. Those who successfully acquire such skills
may benefit from a ‘‘protective shield’’ that such
380 E. Gilboa-Schechtman and G. Shahar
Dow
nloa
ded
by [
Uni
vers
ity o
f R
egin
a] a
t 09:
51 1
8 N
ovem
ber
2014

skills provide when faced with life demands in the
long term. In contrast, the speed of improvement in
pharmacological treatment or in naturalistic recov-
ery is likely to exert its effect through a different
mechanism not under the patient’s conscious con-
trol. Given the high relapse rate after the disconti-
nuation of pharmacological treatment of depression,
we might speculate that the rate of symptom reduc-
tion in the therapeutic stage is unrelated to patients’
future ability to regulate their emotions.
Although the treatment modality effect was mod-
est in size, the findings regarding the differential
association between rate of symptom reduction and
long-term outcome suggest that studying patterns of
individual change allows the examination of the
mechanism of various therapeutic modalities. In-
deed, studies have begun to investigate the patterns
of symptom reduction across different disorders and
treatments (e.g., Nishith, Resick, & Griffin, 2002,
for PTSD; Wilson, Fairburn, Agras, Walsh, &
Kraemer, 2002, for bulimia nervosa). For example,
using session by session ratings of PTSD symptom
clusters, Nishith et al. (2002) suggested that the
exposure components of treatments for PTSD form
the active ingredients of both prolonged exposure
and cognitive processing therapy techniques.
In closing, we should mention several limitations
of the present research. First, in the TDCRP data,
symptom measures were obtained every 4 weeks,
resulting in only five data points for each individual.
This paucity of data points limits the sophistication
of the functional forms of change that can be used to
model the recovery process. Specifically, the avail-
ability of additional data points would have allowed
us to adopt more realistic change trajectories, allow-
ing, for example, the modeling of a trajectory in
which deterioration in treatment is experienced
before improvement is achieved. It is possible that
infrequent assessment distorted the actual shape of
the response pattern. However, this latter interpreta-
tion is unlikely, because our results largely parallel
those of Santor and Segal, in which assessments were
made every week. It should also be noted that our
exclusive reliance on linear regression procedures is
limited in that rate of improvement in treatment
might exert some nonlinear effects on outcome
during follow-up.
Second, our assessment period was limited to 18
months. Whereas this is a considerable time interval,
longer follow-up periods might reveal other patterns
of recovery. For example, Hollon, Thase, and
Markowitz (2002) have begun to conduct follow-
up intervals of up to 3 years. Clearly, such intervals
are better suited to discover the variables that govern
the recovery from depression. Third, we focused
only on patterns of symptom change. It is possible
that the inclusion of other measures (e.g., overall
well-being, interpersonal functioning) would have
shown a different pattern of results (see footnote 1).
Fourth, the long-term data of TDCRP were natur-
alistic (see Shea et al., 1992). Thus, patients might
have received additional treatment after the main
study treatment has ended or might still have been in
treatment when the assessments were being per-
formed. It is possible that such naturalistic design
affects the nature of the relationships examined in
the study.
Fifth, remoralization is typically defined as an
enhancement in a sense of well-being. In the present
research, remoralization was operationalized as a
decrease in distress rather than an increase on non-
symptom-related measures (e.g., in well-being, opti-
mism, or hopelessness). In particular, this implies
that the remoralization and remediation phases were
measured by the same variables observed at different
times. Future research would benefit from the
inclusion of well-being and optimism measures,
which will more directly assess remoralization and
will also provide a clearer conceptual distinction
between the remoralization and the remediation
phases.
Finally, in interpreting the present results, it is
important to note that a significant percentage of
patients who have completed the treatments offered
in this study have not experienced a complete
remission of their symptoms. This suggests that in
treating depression we need to look beyond symp-
tom reduction to the reduction of vulnerability.
Future studies should attempt to relate pattern of
symptom reduction to the reduction in vulnerability.
Despite these important limitations, our study
confirms and extends previous, albeit relatively
scarce, reports as to the important role of temporal
patterns in the treatment of depression and anxiety.
It is our hope that these findings will encourage
further investigation of the role of temporal patterns
in other samples, disorders, and treatment modal-
ities.
Acknowledgements
The authors thank Sidney J. Blatt and David C.
Zuroff for their helpful comments on earlier versions
of this article. Eva Gilboa-Schechtman thanks the
Department of Psychology at Yale University for its
hospitality.
Notes1 Blatt, Zuroff, and their colleagues (Blatt, Zuroff, Bondi, &
Sanislow, 2000; Zuroff, Blatt, Krupnick, & Sotsky, 2003) have
shown that patients’ enhanced adaptive capacity (EAC), a
TDCRP composite that assesses patients’ ability to cope with
Temporal patterns in brief treatment for depression 381
Dow
nloa
ded
by [
Uni
vers
ity o
f R
egin
a] a
t 09:
51 1
8 N
ovem
ber
2014

their symptoms and with life stress after treatment (a) is
independent of symptoms, (b) increases during the follow-up
period among patients in psychotherapy (i.e., CBT and IPT)
but not in pharmacotherapy (i.e., imipramine and placebo), and
(c) serves to buffer against life stress during the follow-up
period. To extend our analyses to nonsymptom measures of
functioning, we have regressed the EAC on type of remoralizer
and rate of symptom reduction. Results indicated that EAC at
both 12- and 18-month follow-up assessments were significantly
related (b�/�/.40, p B/.01, and b�/.44, p B/.01, respectively) to
rate of symptom reduction but not to type of remoralizer (bs�/
�/.078 and �/.084, respectively, ns ). However, no significant
interactions between therapy and rate of symptom reduction
were found in predicting EAC.2 Although any cutoff differentiating the two groups would be
arbitrary, we have chosen the 15% cutoff because this change is
distinctly above that expected by daily variations and measure-
ment errors. Specifically, given that the initial severity of
depression as measured by the BDI is approximately 25, 15%
reduction is more than the 3 points, which, in turn, is more than
BDI’s error of measurement. It is of note, however, that we
experimented with various cutoff points in conducting our
analyses. We have obtained an identical pattern of results with
all cutoffs.
References
Bandura, A. (1977). Self-efficacy: Toward a unifying theory of
behavioral change. Psychological Review, 84 , 191�/215.
Beck, A. T., Rush, A. J., Shaw, B. F., & Emery, G. (1979).
Cognitive therapy of depression . New York: Guilford Press.
Beck, A. T., Ward, C. H., Mendelson, M., Mock, J., & Erbaugh, J.
(1961). An inventory for measuring depression. Archives of
General Psychiatry, 4 , 561�/571.
Belsher, G., & Costello, C. G. (1988). Relapse after recovery from
unipolar depression: A critical review. Psychological Bulletin ,
104 , 84�/96.
Billings, A. G., & Moos, R. H. (1984). Coping, stress, and social
resources among adults with unipolar depression. Journal of
Personality and Social Psychology, 46 , 877�/891.
Blackburn, I. M., Funson, K. M., & Bishop, S. (1986). A two-year
naturalistic follow-up of depressed patients treated with cogni-
tive therapy, pharmacotherapy and a combination of both.
Journal of Affective Disorders , 10 , 67�/75.
Blatt, S. J., Zuroff, D. C., Quinlan, D. M., & Pilkonis, P. A.
(1996). Interpersonal factors in brief treatment of depression:
Further analyses of the National Institute of Mental Health
Treatment of Depression Collaborative Research Program.
Journal of Consulting and Clinical Psychology, 64 , 162�/171.
Brown, G. W., & Harris, T. (1978). Social origins of depression: A
reply. Psychological Medicine , 8 , 577�/588.
Coyne, J. C. (1976a). Depression and the response of others.
Journal of Abnormal Psychology, 85 , 186�/193.
Coyne, J. C. (1976b). Towards an interactional description of
depression. Psychiatry: Interpersonal and Biological Processes , 39 ,
28�/40.
Derogatis, L. R., Lipman, R. S., & Covi, L. (1973). SCL-90: An
outpatient psychiatric rating scale�/Preliminary report. Psycho-
pharmacology Bulletin , 9 , 13�/28.
Elkin, I. (1994). The NIMH Treatment of Depression Collabora-
tive Research Program: Where we began and where we are now.
In A. E. Bergin & S. L. Garfield (Eds.), Handbook of
psychotherapy and behavior change (4th ed., pp. 114�/135).
New York: Wiley.
Elkin, I., Shea, M. T., Watkins, J. T., Imber, S. D., Sotsky, S. M.,
Collins, J. F., et al. (1989). National Institute of Mental Health
Treatment of Depression Collaborative Research Program:
General effectiveness of treatments. Archives of General
Psychiatry, 46 , 971�/982.
Endicott, J., Spitzer, R. L., Fleiss, J. L., & Cohen, J. (1976).
The Global Assessment Scale: A procedure for measuring
overall severity of psychiatric disturbance. Archives of General
Psychiatry, 33 , 766�/771.
Fennell, M. J., & Teasdale, J. D. (1987). Cognitive therapy for
depression: Individual differences and the process of change.
Cognitive Therapy & Research , 11 , 253�/271.
Freud, S. (1958). Remembering, Repeating, and Working
Through: (Further recommendations on the technique of
psychoanalysis), Standard Edition (Vol. 12). London: Hogarth
Press and the Institute of Psychoanalysis.
Gilboa-Schechtman, E., & Foa, E. B. (2001). Patterns of recovery
after trauma: Individual differences and trauma characteristics.
Journal of Abnormal Psychology, 110 , 392�/400.
Goldfried, M. R. (1980). Toward the delineation of therapeutic
change principles. American Psychologist , 35 , 991�/999.
Hamilton, M. A. (1960). A rating scale for depression. Journal of
Neurology, Neurosurgery and Psychiatry, 6 , 56�/62.
Hamilton, M. A. (1967). Development of a rating scale for
primary depressive illness. British Journal of Social and Clinical
Psychology, 6 , 278�/296.
Hammen, C. (1991). Generation of stress in the course of
unipolar depression. Journal of Abnormal Psychology, 100 ,
555�/561.
Hammen, C. (1998). The emergence of interpersonal approaches
to depression. In T. Joiner & J. C. Coyne (Eds), The
interpersonal nature of depression (pp. 21�/35). Washington DC:
American Psychological Association.
Hammen, C., Mayol, A., deMayo, R., & Marks, T. (1986). Initial
symptom levels and the life-event-depression relationship.
Journal of Abnormal Psychology, 95 , 114�/122.
Hart, A. B., Craighead, W. E., & Craighead, L. W. (2001).
Predicting recurrence of major depressive disorder in young
adults: A prospective study. Journal of Abnormal Psychology,
110 , 633�/643.
Hollon, S. D., Thase, M. E., Markowitz, J. C. (2002). Treatment
and prevention of depression. Psychological Science in the Public
Interest , 3 , 39�/77.
Howard, K. I., Lueger, R. J., Maling, M. S., & Martinovich, Z.
(1993). A phase model of psychotherapy outcome: Causal
mediation of change. Journal of Consulting and Clinical Psychol-
ogy, 61 , 678�/685.
Howard, K. I., Moras, K., Brill, P. L., Martinovich, Z., & Lutz, W.
(1996). Evaluation of psychotherapy: Efficacy, effective-
ness, and patient progress. American Psychologist , 51 , 1059�/
1064.
Ilardi, S. S., & Craighead, W. E. (1994). The role of nonspecific
factors in cognitive-behavior therapy for depression. Clinical
Psychology: Science and Practice , 1 , 138�/156.
Joiner, T. E., JR. (2000). Depression’s vicious scree: Self
propagatory and erosive factors in depression chronicity.
Clinical Psychology: Science and Practice , 7 , 203�/218.
Judd, L. J. (1997). The clinical course of unipolar major
depressive disorders. Archives of General Psychiatry, 54 , 989�/
991.
Krause, M. S., Howard, K. I., & Lutz, W. (1998). Exploring
individual change. Journal of Consulting and Clinical Psychology,
66 , 838�/845.
Lambert, M. J., Hansen, N. B., Finch, A. E. (2001). Patient-
focused research: Using patient outcome data to enhance
382 E. Gilboa-Schechtman and G. Shahar
Dow
nloa
ded
by [
Uni
vers
ity o
f R
egin
a] a
t 09:
51 1
8 N
ovem
ber
2014

treatment effects. Journal of Consulting and Clinical Psychology,
69 , 159�/172.
Lewinsohn, P. M., Zeiss, A. M., & Duncan, E. M. (1989).
Probability of relapse after recovery from an episode of
depression. Journal of Abnormal Psychology, 98 , 107�/116.
Lueger, R. J., Howard, K., Martinovich, Z., Lutz, W., Anderson,
E. E., & Grissom, G. (2001). Assessing treatment progress
of individual patients using expected treatment response
models. Journal of Consulting and Clinical Psychology, 69 ,
150�/158.
Mazure, C. M., Bruce, M. L., Maciejewski, P. K., & Jacobs, S. C.
(2000). Adverse life events and cognitive-personality character-
istics in the prediction of major depression and antidepressant
response. American Journal of Psychiatry, 157 , 896�/903.
Nishith, P., Resick, P. A., & Griffin, M. G. (2002). Pattern
of change in prolonged exposure and cognitive-processing
therapy for female rape victims with posttraumatic stress
disorder. Journal of Consulting and Clinical Psychology, 70 ,
880�/886.
Santor, D. A., & Segal, Z. V. (2001). Predicting symptom
return from rate of symptom reduction in cognitive-behavior
therapy for depression. Cognitive Therapy and Research , 25 ,
117�/135.
Segal, Z. V., Shaw, B. F., Vella, D. D., & Katz, R. (1992).
Cognitive and life stress predictors of relapse in remitted
unipolar depressed patients: Test of the congruency hypothesis.
Journal of Abnormal Psychology, 101 , 26�/36.
Shahar, G. (2001). Personality, shame, and the breakdown of
social ties: The voice of quantitative depression research.
Psychiatry: Interpersonal and Biological Processes , 64 , 228�/239.
Shahar, G., Blatt, S. J., Zuroff, D. C., Krupnick, J. L., & Sotsky, S.
M. (2004). Perfectionism impedes social relations and response
to brief treatment for depression. Journal of Social and Clinical
Psychology, 23 , 140�/154.
Shea, M. T., Elkin, I., Imber, S. D., Sotsky, S. M., Watkins, J. T.,
Collins, J. F., et al. (1992). Course of depressive symptoms over
follow-up: Findings from the National Institute of Mental
Health Treatment of Depression Collaborative Research Pro-
gram. Archives of General Psychiatry, 49 , 782�/787.
Stiles, W. B., Leach, C., Barkham, M., Lucock, M., Iveson, S.,
Shapiro, D. A., et al. (2003). Early sudden gains in psychother-
apy under routine clinic conditions: Practice-based evidence.
Journal of Consulting and Clinical Psychology, 71 , 14�/21.
Tang, T. Z., & DeRubeis, R. J. (1999a). Reconsidering rapid early
response in cognitive behavioral therapy for depression. Clinical
Psychology: Science and Practice , 6 , 283�/288.
Tang, T. Z., & DeRubeis, R. J. (1999b). Sudden gains and critical
sessions in cognitive�/behavioral therapy for depression. Journal
of Consulting and Clinical Psychology, 67 , 894�/904.
Tang, T. Z., Luborsky, L., & Andrusyna, T. (2002). Sudden gains
in recovering from depression: Are they also found in psy-
chotherapies other than cognitive-behavioral therapy? Journal of
Consulting and Clinical Psychology, 70 , 444�/447.
Thase, M. E., & Kupfer, D. J. (1996). Recent developments in the
pharmacotherapy of mood disorders. Journal of Consulting and
Clinical Psychology, 64 , 646�/659.
Watkins, J. T., Leber, W. R., Imber, S. D., Collins, J. F., Elkin, I.,
Pilkonis, P. A., et al. (1993). Temporal course of change of
depression. Journal of Consulting and Clinical Psychology, 61 ,
858�/864.
Weissman, M. M., & Paykel, E. S. (1974). The depressed woman:
Study of social relationships . Chicago: University of Chicago
Press.
Willett, J. B., & Sayer, A. G. (1994). Using covariance structure
analysis to detect correlates and predictors of individual change
over time. Psychological Bulletin , 116 , 363�/381.
Wilson, G. T., Fairburn, C. C., Agras, W. S., Walsh, B. T., &
Kraemer, H. (2002). Cognitive-behavioral therapy for bulimia
nervosa: Time course and mechanisms of change. Journal of
Consulting and Clinical Psychology, 70 , 267�/274.
Zuroff, D. C. (1992). New directions for cognitive models of
depression. Psychological Inquiry, 3 , 274�/277.
Zusammenfassung
Je eher, desto besser: Zeitmuster in der kurzenBehandlung von Depression und ihre Rollefur Langzeitkatamnesen
Um zu untersuchen, ob zeitliche Veranderungsmuster inkurzer Behandlung von Depression den Behandlungser-folg bei einer Katamnese nach 18 Monaten voraussagenkonnen, benutzten die Autoren Daten des ‘NationalInstitute of Mental Health Treatment of DepressionCollaborative Research Program’. In Ubereinstimmungmit ihren Hypothesen fanden sie, dass a) Patienten, derenStressniveau nicht zwischen der Aufnahme und der viertenTherapiewoche abnahm (Patienten mit langsamer Verbes-serung) bei der Katamnese eine schlechteres Symptombildzeigten als Patienten mit unmittelbarer Stresserleichterung(Patienten mit schneller Verbesserung), b) die Hohe derSymptomreduktion wahrend der Behandlung den Zustandzu den Zeitpunkten von 12 und 18 Monaten nach derBehandlung, uber den anfanglichen Schweregrad derSymptome hinaus, vorherzusagen kann und c) dass dieHohe der Symptomreduktion fur die Zeitraume von 12und 18 Monaten nach der Behandlung bei Psychotherapiebesser als bei nicht-psychologischen Behandlungenvorhergesagt werden kann. Die Ergebnisse ermutigen zuweiterer Forschung und zu einer erhohten klinischenAufmerksamkeit fur zeitliche Veranderungsmuster beikurzen Behandlungen von Depression.
Resume
Plus c’est vite, et mieux c’est : patterns temporelsdans le traitement bref de la depression et leurrole pour les resultats a long terme
Pour examiner si des patterns temporels de changementdans le traitement bref de la depression predisent leresultat 18 mois apres la fin du traitement, les auteursont utilise les donnees du Programme de RechercheCollaborative du Traitement de la Depression, sponsorisepar l’Institut National de Sante Mentale. En accord avecleurs hypotheses, ils ont trouve que (a) les individus dont leniveau de detresse ne diminue pas entre l’entree et lasemaine 4 de la therapie (ceux qui retrouvent le morallentement) font preuve d’un pattern de symptomes plussevere a l’evaluation catamnestique que ceux qui montrentun soulagement immediat (qui retrouvent le moral rapide-ment) ; (b) le taux de diminution des symptomes au coursdu traitement predit les resultats a 12 et a 18 moisindependamment de la severite initiale des symptomes ;et (c), le taux de diminution des symptomes preditdavantage les resultats a 12 et 18 mois pour la psychother-apie que pour les traitements non psychologiques. Ces
Temporal patterns in brief treatment for depression 383
Dow
nloa
ded
by [
Uni
vers
ity o
f R
egin
a] a
t 09:
51 1
8 N
ovem
ber
2014

resultats devraient encourager des recherches ulterieures etune attention clinique pour les patterns temporels dereponse dans le traitement bref de la depression.
Resumen
Cuanto antes, mejor. Pautas temporales para laterapia breve de la depresion y su rol en losresultados a largo plazo
Para estudiar si las pautas temporales de cambio en laterapia breve de la depresion pueden predecir el resultadoa los dieciocho meses de terminado el tratamiento, losautores utilizaron datos del Programa de investigacion delTratamiento Colaborativo de la depresion patrocinado porel Instituto Nacional de Salud Mental (National Instituteof Mental Health-sponsored Treatment of DepressionCollaborative Research Program): De acuerdo con suhipotesis, encontraron que a) los individuos en los cualesel nivel de distres no disminuye entre la admision y lacuarta semana de terapia (recicladores (recicladores ) lentos)exhibieron una pauta de sıntomas mas severa en lasestimaciones de seguimiento que los que mostraron unalivio inmediato (recicladores (remoralizers) rapidos); b) latasa de reduccion de sıntomas durante el tratamientopredice resultados a los doce y dieciocho meses posterioresa los sıntomas iniciales; y c) la tasa de reduccion desıntomas es mas predictiva de los resultados a los doce y losdieciocho meses en tratamientos psicoterapeuticos que enotros tipos de tratamientos. Los hallazgos estimulan aproseguir investigaciones y observaciones clınicas depautas temporales de respuesta para las terapias brevesde la depresion.
Resumo
Quanto mais cedo melhor: Padroes Temporais noTratamento Breve da Depressao e o seu Papelno Resultado a longo prazo
Para examinar se os padroes temporais de mudanca emtratamentos breves para a depressao sao preditivos doresultado terapeutico aos 18 meses pos-tratamento, osautores usaram dados do Programa Colaborativo deInvestigacao do Tratamento da Depressao do InstititutoNacional de Saude Mental dos Estados Unidos. De acordocom as hipoteses, verificaram que (a) os indivıduos cujosnıveis de sintomatologia nao diminiuiam entre a admissaoe a 4a semana de terapia (re-moralizadores lentos) exibiampadroes mais severos de sintomas nas avaliacoes deseguimento (follow-up) que os que mostravam melhoriasimediatas nesse perıodo (re-moralizadores rapidos); (b) o
ritmo de reducao sintomatica durante o tratamento epreditor do resultado terapeutico entre os 12 e os 18 mesesindependentemente da gravidade sintomatica inicial; e (c)o ritmo de reducao sintomatica e mais preditivo doresultado terapeutico, entre os 12 e os 18 meses, notratamento psicoterapeutico que nos tratamentos naopsicologicos. Os resultados encorajam futuras investiga-coes e a atencao clınica aos padroes temporais da respostaao tratamento breve da depressao.
Sommario
Quanto prima, tanto meglio: modelli temporali neltrattamento breve della depressione ed il lororuolo nell’esito a lungo termine
Nell’esaminare se i modelli temporali di cambiamento neltrattamento breve della depressione sono predittivi dell’e-sito a 18 mesi dal trattamento, gli autori hanno usato i datidell’Istituto Nazionale di Salute Mentale, responsabile delProgramma di Ricerca d’equipe sul Trattamento dellaDepressione.
In accordo con le loro ipotesi, hanno trovato che:
a. gli individui i cui livelli di disagio non decresce-
vano tra immissione e 4 settimane di terapia
(lento ) manifestarono un tipo di sintomi piu
gravi alle valutazioni di follow-up rispetto a quelli
che avevano mostrato sollievo immediato;
b. il tasso di riduzione dei sintomi durante il
trattamento e predittivo degli esiti a 12 e 18
mesi indipendentemente dalla gravita iniziale dei
sintomi;
c. il tasso di riduzione dei sintomi e piu predittivo
degli esiti a 12 e 18 mesi nella psicoterapia
rispetto ai trattamenti non psicologici.
I risultati incoraggiano ulteriori ricerche e attenzioneclinica ai modelli temporali di risposta nel trattamentobreve della depressione.
384 E. Gilboa-Schechtman and G. Shahar
Dow
nloa
ded
by [
Uni
vers
ity o
f R
egin
a] a
t 09:
51 1
8 N
ovem
ber
2014